Crossing borders: the need for empirical evidence of real-world evidence transportability in oncology
Publication: Journal of Comparative Effectiveness Research
Plain language summary
What is this article about?
This article discusses the challenges of using non local real-world evidence (RWE) in health technology assessments (HTA) when local data are unavailable, insufficient, or inappropriate. HTA organizations often prefer data collected locally or regionally, but the lack of suitable data in many markets has increased interest in understanding data ‘transportability’ – whether data from one country or population can be used to predict outcomes in another. Established in 2024, the Flatiron Fostering Oncology RWE Use Cases and Methods (FORUM) research consortium is exploring when and how non-local RWE can be effectively applied, with initial work focused on lung cancer, breast cancer and multiple myeloma.
What does the evidence suggest so far?
Initial studies suggest RWE from the US could predict outcomes in other countries with proper adjustment for population and treatment differences. Recent research in advanced non-small cell lung cancer demonstrated that adjusted US data provided comparable survival to real observed outcomes in Canada and the UK. This limited evidence base indicates that non-local RWE can help inform decision-making when local data is unavailable.
What studies are needed next?
The FORUM consortium is expanding research to other cancer types and countries to better understand RWE transportability. Future studies will focus on comparing outcomes across diverse healthcare systems, identifying key variables for adjustment and developing guidelines for when and how non-local data can be used. These efforts aim to create a framework for the use of global RWE in oncology HTA decision-making.
Real-world evidence (RWE) can be a valuable component of health technology assessment (HTA) dossiers. It provides insight into how a medicine evaluated under the controlled setting of a clinical trial performs, or is likely to perform, in a real-world population. The label-indicated population will usually be broader than the trial population across myriad factors, including age, health status, ethnicity, socioeconomic status, local screening practices and time to access treatment [1].
Guidance on the use of RWE has been issued by HTA and supporting bodies globally, including Canada’s Drug Agency, the National Institute for Health and Care Excellence (NICE) in the UK, the Institute for Quality and Efficiency in HealthCare (IQWiG) in Germany, the Haute Autorité de Santé in France and the European Network for HTA (EUnetHTA), which supports collaboration between HTA organizations across Europe [2]. When using RWE to inform decisions, HTA bodies largely prefer that the data was generated in their jurisdiction. A 2022 survey across EUnetHTA countries found non-local real-world data (RWD) – defined as data generated outside the respondent’s region – to be less preferred [3]. Differences in healthcare systems, healthcare practice, treatment access and patient characteristics between countries or regions can drive variation in outcomes, meaning inferences drawn from data in one population may not be applicable to another population.
This preference for local data, however, is often at odds with the reality that such data may not exist or may lack key variables needed for robust analysis. In this scenario, decision makers face a critical question: should they rely on the most suitable data, even if it comes from another country, or prioritize locally collected data, even if it has limitations? For example, an HTA body may want to assess the real-world comparative effectiveness of a new drug, but the drug has not yet launched in their market. Drugs are often launched earlier in the US compared with other geographies, meaning extensive US RWD may be available at time of launch in other markets [4]. But is this data appropriate for decision-making elsewhere? This conundrum highlights the need to better understand a key question of evidence transportability: can evidence generated from data in one population, the ‘source’ population, be used to infer outcomes for a different, separate ‘target’ population?
Recognizing these challenges – and despite the preference for local data – there is evidence of a growing shift in the HTA mindset [5]. This shift is reflected in updates to the NICE RWE framework, published in 2024, which incorporates new methodologies for enhancing the external validity and transportability of RWD [6]. A 2022 publication from IQWiG also referred to the need to appropriately adjust for differences in mortality or risk between the source and target populations when using non-local data [7]. While there appears to be willingness to consider non-local data sources, uncertainty remains and little empirical evidence exists to demonstrate the transportability of non-local data. There is also a lack of agreement on what data are most appropriate, and what are the best methods and variables to adjust for systemic differences between countries, populations and healthcare settings. Therefore, it is important to address these evidence gaps by executing studies that robustly test methods of evidence transportability.
FORUM rises to the challenge
To tackle this challenge, Flatiron Health formed a consortium of life science companies alongside academic experts and representatives from HTA bodies for Fostering RWE Use Cases and Methods (FORUM) [8]. The FORUM is exploring the transportability of RWE across borders for a series of cancer types, including metastatic breast cancer (mBC), advanced non-small cell lung cancer (aNSCLC) and multiple myeloma.
Learnings from our portfolio of work will be compared, contrasted and synthesized to draw collective insights about the transportability of real-world health outcomes in oncology, including addressing the following questions:
•
Can outcomes (overall survival [OS], progression-free survival, time to treatment discontinuation, etc.) in the US be transported to other international markets?
•
What variables are necessary to transport RWE across borders?
•
When is patient-level data required, and when is aggregated data sufficient?
•
Does country of origin still matter if you adjust for key transportability variables?
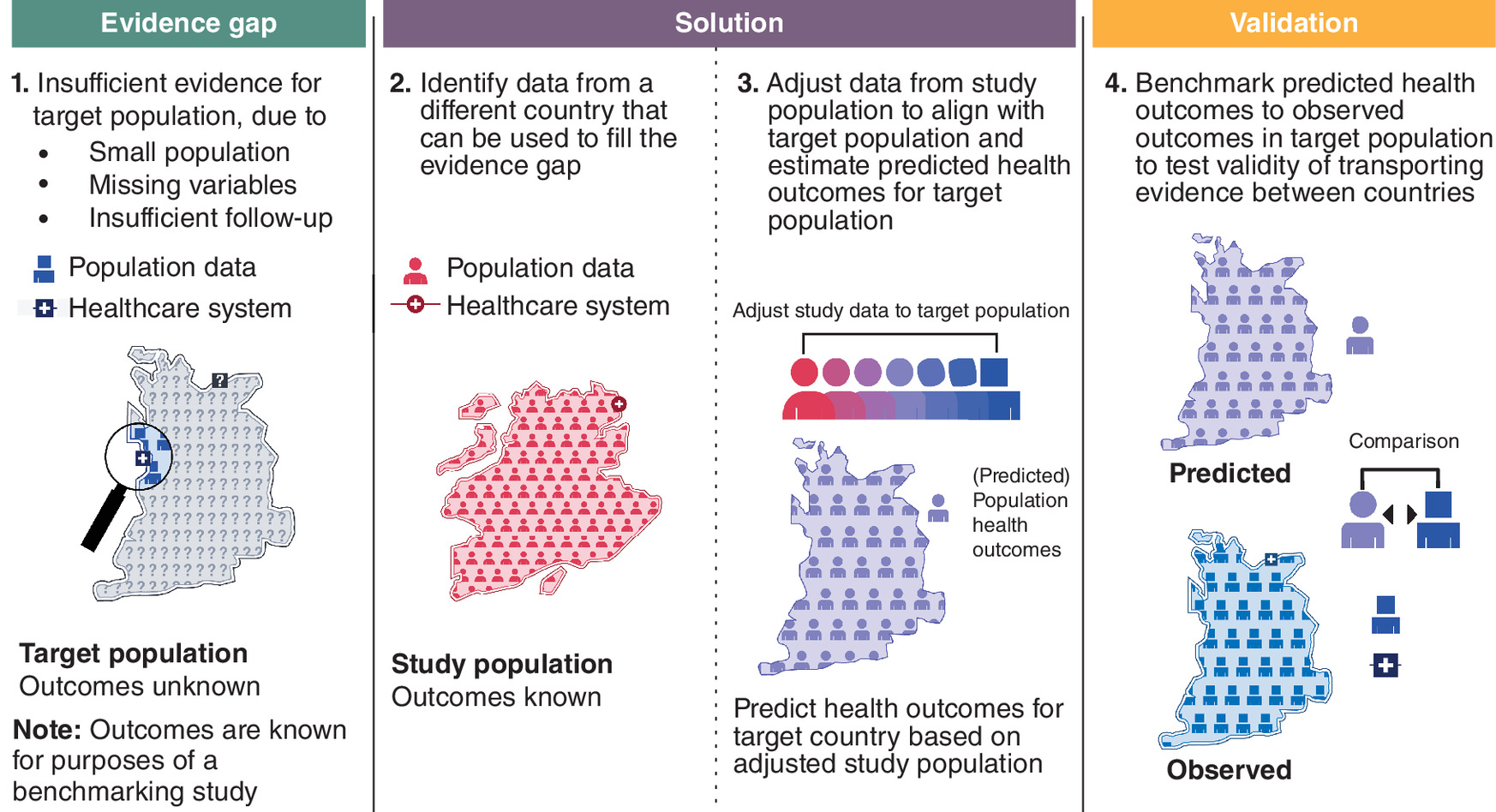
To answer these questions, the FORUM is conducting benchmarking studies (Figure 1) where the real-world health outcomes are known in both the source and target populations. This approach will validate whether data from a source population can accurately predict outcomes in a target population.
To conduct these benchmarking studies and assess external validity, data must be obtained from each of the countries being compared for each of the cancer types being evaluated. To enable transparency, all study protocols are being prespecified and published on The Professional Society for Health Economics and Outcomes Research (ISPOR) Real-World Evidence Registry before outcomes analysis [9].
The evidence so far
A recent scoping review was conducted to identify and describe studies applying transportability methods using RWD [10]. Of the seven identified studies, only two transported estimates from one real-world population to another [10,11], and only one of those transported estimates from one country to another [11]. That study reviewed the transportability of OS estimates in patients with aNSCLC between the US and Canada using patient-level data from each country, for two exposure-based cohorts: one exposed to first-line chemotherapy, and another to pembrolizumab. To account for population differences, known prognostic factors in the US data were adjusted to match the Canadian population. The study found that OS was similar for the exposure-based cohorts between the two countries after adjusting for baseline characteristics (age, sex, cancer stage, Eastern Cooperative Oncology Group performance status, tumor histology, smoking history and time since aNSCLC diagnosis). These findings suggest that adjusted OS estimates from US data could be used as a proxy for OS in Canada for patients with aNSCLC. In a subsequent transportability study conducted by Flatiron Health and NICE, published estimates of real-world OS in UK patients with aNSCLC who were exposed to chemotherapy, immunotherapy or targeted therapy were used as a benchmark [12]. When US survival outcomes were adjusted using matching-adjusted indirect comparison to align with UK patient characteristics, the study reported similar OS outcomes in all three exposure groups, suggesting that adjusted US data could effectively estimate survival in the UK had local data been unavailable [13]. Most recently, a FORUM study exploring the transportability of outcomes between patients in the US and England diagnosed with de novo mBC suggested that observed real-world OS may be transportable from the US to England [14]. These observations are further supported by two additional transportability studies in mBC subgroups: one examining transportability of OS estimates in patients with human epidermal growth factor receptor 2-positive mBC from the US to the UK, and the other in patients with triple negative breast cancer from the US to France [15,16].
A growing number of studies support the theory that real-world health outcomes in patients with solid tumors may be transportable between countries, such as the US, Canada and the UK. However, this small body of evidence illustrates the importance of extending the research to include other countries and cancer types (Figure 2). Expanding this research will improve our understanding of when and how evidence is transportable in oncology, and whether there are circumstances in which underlying differences in healthcare systems necessitate the use of local data.
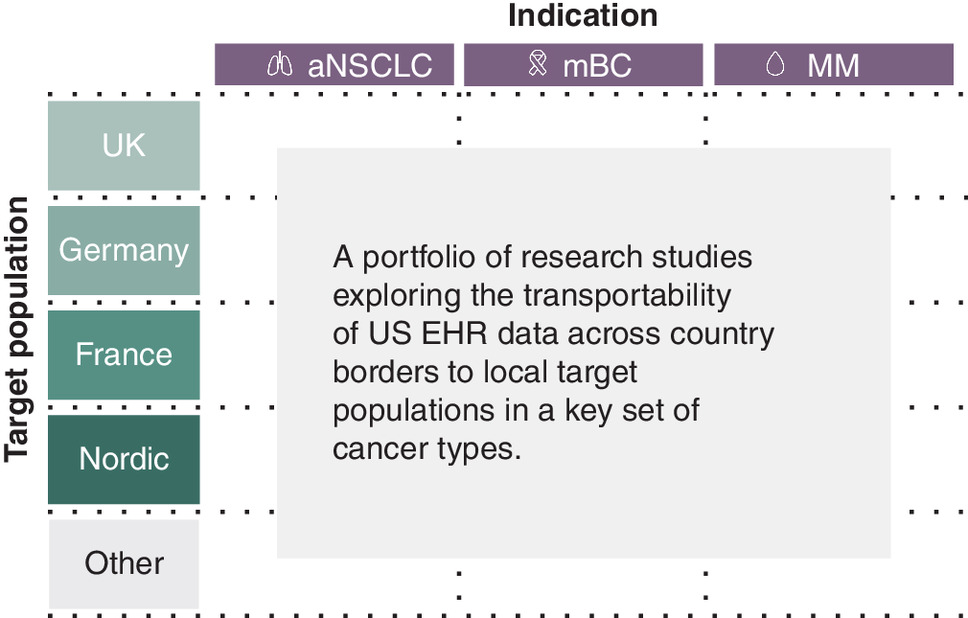
Figure 2. Flatiron FORUM will conduct and synthesize insights from a matrix of studies in different cancer types with different target populations.
aNSCLC: Advanced non-small cell lung cancer; EHR: Electronic health record; mBC: Metastatic breast cancer; MM: Multiple myeloma.
What will the impact be?
As the FORUM consortium designs and conducts a collection of research studies, it will be critical to synthesize learnings across individual countries and across each cancer type. Drawing insights from several studies with a single target population can help us identify challenges, patterns and nuances of when and how the validity of RWE transportability may be modified in specific healthcare settings. Consolidating learnings from multiple studies in the same cancer type will help us better understand oncology-specific transportability and help discern the relevance of study findings between different regions. Furthermore, we believe that the synthesis of these cross-study learnings can help shape a core set of principles for RWE transportability. By fostering discussion across industry, academia, and HTA stakeholders, Flatiron FORUM can help drive consensus around these principles to collectively define the appropriate situations, standardized methodology and interpretation of evidence transportability. We hope that these findings can serve as references to guide assumptions of RWE transportability between countries.
Author contributions
All authors were responsible for conception, administration, drafting and revision of the editorial.
Acknowledgments
The authors thank the Flatiron FORUM for its active engagement with HTA stakeholders and for incorporating their insights and preferences, which have meaningfully informed the development of this manuscript. The authors also thank Elsebeth Horne, Qianyi Zhang, Harlan Pittell of Flatiron Health for their support with writing review and editing; Madeline Morenberg of Flatiron Health for the visual design of figures; and Hashem Meriesh of Flatiron Health for editorial support.
Financial disclosure
This article and collection of studies were funded by the Flatiron FORUM members including Pfizer, Gilead, Roche and Daiichi Sankyo.
Competing interests disclosure
C Clunie-O'Connor, P Mpofu and B Adamson are employees of Flatiron Health, Inc. (an independent member of the Roche Group) and own stock in Roche. A Taylor is an employee of Gilead Sciences Europe LTD and owns stock in Gilead Sciences. M Rosenlund is an employee of Daiichi Sankyo Europe GmbH and owns stocks in GSK. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No funded writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Turner AJ, Sammon C, Latimer N et al. Transporting comparative effectiveness evidence between countries: considerations for health technology assessments. PharmacoEconomics 42(2), 165–176 (2024).
2.
Sarri G, Hernandez LG. The maze of real-world evidence frameworks: from a desert to a jungle! An environmental scan and comparison across regulatory and health technology assessment agencies. J. Comp. Eff. Res. 13(9), e240061 (2024).
3.
Hogervorst MA, Pontén J, Vreman RA, Mantel-Teeuwisse AK, Goettsch WG. Real world data in health technology assessment of complex health technologies. Front. Pharmacol. 13, 837302 (2022).
4.
Mpofu P, Kent S, Jónsson P et al. Evaluation of US oncology electronic health record real-world data to reduce uncertainty in health technology appraisals: a retrospective cohort study. BMJ Open 13(10), e074559 (2023).
5.
Jaksa A, Arena PJ, Chan KKW, Ben-Joseph RH, Jónsson P, Campbell UB. Transferability of real-world data across borders for regulatory and health technology assessment decision-making. Front. Med. 9, 1073678 (2022).
6.
Walker J. NICE updates real-world evidence framework to address new approaches in external validity and transportability of real-world data. (2024). Available at: https://becarispublishing.com/digital-content/blog-post/nice-updates-real-world-evidence-framework-address-new-approaches-external-validity-and
7.
Institute for Quality and Efficiency in Health Care (IQWiG). Routine practice data in manufacturer dossiers: things are not yet running smoothly. (2022). Available at: https://www.iqwig.de/en/presse/press-releases/press-releases-detailpage_67103.html
8.
Flatiron Health. Unlock critical evidence to accelerate access to cancer treatments worldwide. Available at: https://flatiron.com/real-world-evidence/value-access-hta
9.
Real World Evidence Registry | Search. Available at: https://osf.io/registries/rwe/discover
10.
Wang H, Tikhonovsky N, Gupta VA, Thompson A, Ramagopalan S, Duffield S. RWD30 applying transportability methods to real-world data: a scoping review. Value Health. 26(12), S510 (2023).
11.
Ramagopalan SV, Popat S, Gupta A et al. Transportability of overall survival estimates from US to Canadian patients with advanced non–small cell lung cancer with implications for regulatory and health technology assessment. JAMA Netw. Open 5(11), e2239874 (2022).
12.
Lester J, Escriu C, Khan S et al. Retrospective analysis of real-world treatment patterns and clinical outcomes in patients with advanced non-small cell lung cancer starting first-line systemic therapy in the United Kingdom. BMC Cancer 21(1), 515 (2021).
13.
Kent S, Mpofu P, Duffield S et al. Evaluating transportability of overall survival estimates from US to UK populations receiving first-line treatment for advanced non-small cell lung cancer: a retrospective cohort study. BMJ Open 14(12), e085722 (2024).
14.
Pittell H, Horne E, Mpofu P et al. HTA359 Transportability of overall survival estimates from the US to England in metastatic breast cancer using nationally representative data sources. Value Health. 27(12), S426 (2024).
15.
Mpofu P, Thuresson P, Sanglier T et al. HTA219 Transporting real-world evidence: is it possible to transport OS estimates in HER2+ mBC from US to UK? Value Health. 27(12), S397 (2024).
16.
Mbowen LS, Machuron V, Machuron G, Jegou R, Esnault C. MSR54 Anticipating the real-world impact of therapeutic innovations in France by transporting evidence from the United States (US): a case study in metastatic triple-negative breast cancer (mTNBC) based on the Flatiron Health Database. Value Health. 27(12), S448 (2024).
Information & Authors
Information
Published In
Copyright
© 2025 Flatiron Health, Inc. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 April 2024
Accepted: 5 June 2025
Published online: 10 July 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Crossing borders: the need for empirical evidence of real-world evidence transportability in oncology. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2025-0053
Export citation
Select the citation format you wish to export for this article or chapter.