Matching-adjusted indirect comparison between garadacimab and lanadelumab for the long-term prophylactic treatment of patients with hereditary angioedema
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study aimed to estimate the relative efficacy between garadacimab 200 mg once monthly (200 QM) and two dosing regimens of lanadelumab (300 mg once every 2 weeks [300 Q2W] and 300 mg once every 4 weeks [300 Q4W]) in adolescent/adult patients with hereditary angioedema (HAE) using matching-adjusted indirect comparisons (MAICs), in the absence of head-to-head randomized controlled trials. Materials & methods: Individual patient data were available from the phase II (NCT03712228) and the phase III VANGUARD (NCT04656418) trials investigating garadacimab, and published summary-level data from the phase III HELP trial investigating lanadelumab (NCT02586805). The primary outcome was time-normalized number of HAE attacks. Secondary efficacy outcomes included time-normalized number of HAE attacks requiring on-demand treatment, time-normalized number of moderate and/or severe HAE attacks, and proportion of attack-free patients. Quality of life (QoL) was also assessed via change from baseline in AE-QoL total score. Results: Compared with lanadelumab 300 Q2W, garadacimab 200 QM statistically significantly reduced number of moderate and/or severe HAE attacks (rate ratio [RR]; 95% confidence interval: 0.25; 0.07, 0.84) and improved AE-QoL score (mean difference: -17.38; -33.67, -1.08). Compared with lanadelumab 300 Q4W, garadacimab 200 QM showed statistically significant improvements in all outcomes: HAE attacks (RR: 0.29; 0.13, 0.63), attacks requiring on-demand treatment (RR: 0.29; 0.13, 0.66), moderate and/or severe HAE attacks (RR: 0.15; 0.05, 0.49), proportion of attack-free patients (hazard ratio: 3.25; 1.45, 7.29), and AE-QoL score (mean difference: -21.29; -37.39, -5.18). Conclusion: These MAICs showed improved efficacy and QoL with garadacimab compared with lanadelumab across multiple endpoints. These findings demonstrate that garadacimab may provide improved therapeutic benefit compared with lanadelumab in the long-term prophylactic treatment of patients with HAE.
Hereditary angioedema (HAE) is a rare genetic disorder characterized by recurrent episodes of severe swelling, most commonly affecting the limbs, abdomen and larynx [1]. Patients with HAE often experience poor quality of life (QoL) and a reduced ability to perform daily activities [2,3].
Treatments for HAE attacks can be administered for on-demand treatment of acute attacks, for short-term prophylaxis, or for long-term prophylaxis (LTP). LTP treatments aim to prevent the occurrence of HAE attacks and improve QoL in patients with HAE. Garadacimab is a novel, fully human, monoclonal antibody that inhibits factor XIIa, which initiates bradykinin formation in HAE, and has shown improved efficacy in preventing HAE attacks with a favorable safety profile [4–7]. Garadacimab’s long-term safety and efficacy is being evaluated in an ongoing phase III open label extension study (NCT04739059) [8]. Garadacimab was granted market authorization by the European Medicine Agency in February 2025, and is currently awaiting market authorization by the US FDA [9].
Lanadelumab (TAKHZYRO®) is a monoclonal antibody that prevents HAE attacks by inhibiting plasma kallikrein, which is a mediator of bradykinin formation downstream to factor XIIa [7]. The safety and efficacy of lanadelumab has been investigated in the phase III HELP (NCT02586805) trial, where it demonstrated a reduced HAE attack rate compared with placebo [10]. Lanadelumab is an established first-line therapy for LTP of HAE attacks, having been approved in various regions globally since 2018 [11–14].
In the absence of comparative randomized controlled trials (RCTs), indirect treatment comparison methods such as matching-adjusted indirect comparisons (MAICs) can be used to estimate the relative efficacy between treatments. Comparative efficacy estimates from these analyses can provide researchers, clinicians and policymakers involved in healthcare decision-making with valuable insight to inform decisions on optimal treatment choice. Traditional indirect treatment comparison methods (e.g., Bucher pairwise comparisons) rely on summary-level data (SLD) to estimate treatment effect, but these methods cannot always account for inherent differences in patient populations which can lead to biased estimates [15,16]. MAIC is a population-adjusted method that leverages individual patient data (IPD) from the target treatment of interest to adjust its population to the SLD of the comparator population. Consequently, MAICs can effectively correct some of the observed cross-trial imbalances in patient and study characteristics to produce a less biased comparison of two medical interventions than traditional methods [17].
The present study used MAICs to compare garadacimab to two dosing regimens of lanadelumab in the treatment of patients with HAE. By using IPD from the RCTs with garadacimab (the phase II trial, NCT03712228, and pivotal phase III VANGUARD, NCT04656418), and SLD for the pivotal phase III lanadelumab trial (HELP, NCT02020889), MAICs were used to estimate the relative efficacy and impact on QoL of garadacimab versus lanadelumab.
Materials & methods
Systematic literature search & feasibility assessment
The purpose of this MAIC is to assess the comparative efficacy of garadacimab and lanadelumab as LTP in adolescences and adults with HAE. To minimize the risk of missing studies, a systematic literature review (SLR) following established best practices [18,19] was conducted on 11 August 2022 to broadly identify relevant RCTs evaluating patients (≥12 years old) with HAE. Details of SLR materials and methods are provided in Supplementary Appendix A. The evidence base informed by this SLR for LTP in patients with HAE identified eight RCTs. The RCTs identified by the SLR were further filtered to isolate trials evaluating only garadacimab and lanadelumab to fulfil the objective of this current analysis. Of these, two RCTs investigated garadacimab (VANGUARD and a phase II trial) and one trial investigated lanadelumab (HELP), which were the focus for this analysis (Table 1). The studies were of good quality as assessed using the Centre for Reviews and Dissemination RCT checklist (2008) (Supplementary Appendix A7) [20].
| Trial; NCT | Phase | Setting | Blinding | Treatment period | Treatment arms |
|---|---|---|---|---|---|
| VANGUARD (NCT04656418) | III | Multicenter | Double-blind | 26 weeks | Garadacimab 400 mg SC once (loading dose) Garadacimab 200 mg SC once monthly |
| Placebo | |||||
| NA (NCT03712228) | II | Multicenter | Double-blind | 12 weeks | Garadacimab 100 mg IV once (loading dose) Garadacimab 200 mg SC once monthly |
| Placebo | |||||
| HELP (NCT02586805) | III | Multicenter | Double-blind | 26 weeks | Lanadelumab 300 SC every 2 weeks |
| Lanadelumab 300 SC mg every 4 weeks | |||||
| Placebo |
IV: Intravenously; NA: Not applicable/available; SC: Subcutaneously.
While there were some differences in trial duration, patient baseline characteristics, and trial enrollment criteria, clinical opinion (IJ, MD; and IP, DVM, PhD) deemed the three trials sufficiently similar in terms of trial design, eligibility criteria, baseline patient characteristics and outcome assessments as to be appropriate for assessing comparative efficacy via MAICs (Supplementary Appendix B). Notably, there were slight differences in the treatment plans between the trials. Firstly, the VANGUARD and phase II trials administered a single loading dose of garadacimab (400 mg subcutaneously [SC] in VANGUARD trial, and 100 mg intravenously in the phase II trial) in the first month of treatment, whereas the HELP trial did not administer a loading dose. Treatments schedules were administered as follows: at a dose of 200 mg SC once monthly in VANGUARD (garadacimab 200 QM); 300 mg SC once every 2 weeks (lanadelumab 300 Q2W) or once every 4 weeks (lanadelumab 300 Q4W) in HELP; and once every 4 weeks in the phase II trial (garadacimab 200 Q4W). Based on clinical opinion, the doses used in VANGUARD and phase II trials of garadacimab were considered equivalent and referred to as QM going forward for the purposes of these analyses.
Eligibility criteria
Eligibility criteria from VANGUARD, the phase II trial for garadacimab, and HELP are available in Supplementary Appendix C. Overall, the eligibility criteria among the trials were either similar or unable to be adjusted for due to HELP having broader criteria.
Outcomes of interest
Outcomes of interest were determined by investigating the pivotal trials for reported outcomes, which were then narrowed down using a feasibility assessment (Supplementary Appendix B). Outcomes assessed in this analysis included four efficacy outcomes and one QoL outcome. The primary outcome assessed in this analysis was time-normalized number of HAE attacks. Secondary efficacy outcomes included time-normalized number of HAE attacks requiring on-demand treatment, time-normalized number of moderate and/or severe HAE attacks and proportion of attack-free patients. The QoL outcome was change from baseline to day 182 in total Angioedema Quality of Life (AE-QoL) score. The aforementioned outcomes were reported in VANGUARD, the phase II trial for garadacimab, and HELP, except for change from baseline in total AE-QoL score, which was not reported in the phase II garadacimab trial.
Outcome definitions from all three trials are available in Supplementary Appendix D. The outcomes were defined similarly across trials where reported, with the only difference being that the phase II garadacimab trial had a shorter treatment period (12 weeks) than VANGUARD and HELP (26 weeks).
Data sources
VANGUARD was a double-blind, parallel arm, phase III randomized placebo controlled clinical trial conducted to characterize efficacy and safety of garadacimab in adolescent and adult patients aged 12 years and older with HAE [21]. The intention-to-treat (ITT) population consisted of 64 patients who were randomized to receive 200 mg garadacimab SC once monthly (QM; n = 39) or placebo (PBO; n = 25) [22]. Patients received either garadacimab or placebo for 26 weeks.
The phase II trial for garadacimab was a double-blind, parallel arm, randomized placebo controlled clinical trial conducted to characterize efficacy and safety of garadacimab in adult patients with HAE [23]. The ITT population consisted of 32 patients who were randomized to receive garadacimab SC at 75 mg every 4 weeks (Q4W; n = 9), 200 mg Q4W (n = 8), 600 mg Q4W (n = 7) or PBO (n = 8) [5]. Patients received treatment over a period of 12 weeks.
HELP was a double-blind, parallel arm, phase III randomized placebo controlled clinical trial conducted to characterize safety and efficacy of lanadelumab in patients with HAE [10]. A total of 125 patients were included in the ITT population and were randomized to receive lanadelumab SC at 150 mg Q4W (n = 29), 300 mg Q4W (n = 29), 300 mg Q2W (n = 27) or PBO (n = 41). The treatment period was 26 weeks.
IPD were available for the VANGUARD and the phase II garadacimab trials, and SLD were available for the HELP trial. The present analysis pools the IPD from VANGUARD and the phase II garadacimab trials in the analyses of all outcomes, except for change from baseline in total AE-QoL score, which was not reported in the phase II garadacimab trial.
Dosages of interest
Dosages of interest included garadacimab 200 mg QM, lanadelumab 300 mg once every 2 weeks (300 Q2W) and lanadelumab 300 mg once every 4 weeks (300 Q4W; Table 1). For the purposes of this analysis, the dosages of lanadelumab were compared with garadacimab 200 QM in separate MAICs.
Selection of treatment effect modifiers
Cross-trial differences in treatment effect modifiers (TEMs) of the study populations can bias comparisons if left unadjusted [15]. Before conducting the analyses, a list of potential TEMs consisting of baseline characteristics reported across the VANGUARD, phase II garadacimab, and HELP trials were identified. The TEMs were then ranked by internal clinical experts (IJ and IP) based on the likelihood that each covariate would be treatment effect modifying of the outcomes of interest. Once a consensus among all internal clinical experts was reached, a pooled rank-ordered list of TEMs was generated. To reduce the potential for bias, this list was shared with an external European clinical expert for objective validation. Once validated, the final ranked list of TEMs was applied to all outcomes of interest (Supplementary Appendix E). The base case analyses adjusted for all TEMs based on availability across trials.
Statistical analysis
Separate MAICs between garadacimab 200 mg QM and the two doses of lanadelumab (300 mg Q2W and Q4W) were conducted using methods outlined by the National Institute for Health and Care Excellence (NICE) Decision Support Unit (DSU) Technical Support Document (TSD) 18 [15,17]. Detailed MAIC methodology is provided in Supplementary Appendix F. All MAIC analyses were performed using R version 3.6.1 or higher (R Core Team, Vienna, Austria) based on the code provided in the NICE DSU TSD 18 [15].
Since VANGUARD, the phase II trial for garadacimab, and HELP can be connected via a common comparator (placebo), anchored MAICs were conducted to compare all continuous and rate outcomes. Unanchored MAICs (i.e., exclusion of placebo arms) were performed for the binary outcome (proportion of attack-free patients), given zero patients experienced an event in the placebo arms of VANGUARD and the phase II garadacimab trial for this outcome. To reduce between-study heterogeneity, the IPD from VANGUARD and the phase II garadacimab trials were ‘matched and adjusted’ to the HELP SLD based on the ranked TEMs. Patients in the garadacimab trials were reweighted using a propensity score model so that the distribution of the identified baseline characteristics (that are TEMs) matched those reported in HELP [17,24]. Between-study heterogeneity was assessed using standardized mean differences (SMDs) before and after adjustment (where an SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference) [25]. The effective sample size (ESS) was calculated to reflect the impact of weighting on the available information in the IPD [17].
The relative treatment effect estimate for garadacimab versus lanadelumab was then derived using the reweighted garadacimab trials population. The target estimate for the MAIC was perceived as the average treatment effect in the comparator; a mapping of the outcome for patients taking garadacimab to the HELP population. Continuous outcomes were modelled using a weighted generalized linear model (GLM) with a Gaussian likelihood and identity link function with the outcome and the binary treatment indicator. For rate outcomes, estimates were derived from a weighted GLM using a Poisson likelihood and log link function with the outcome, the binary treatment indicator, and normalized baseline attack rate in the model to align with reported data from HELP [10]. For the binary outcome, simulated IPD was generated for HELP with follow-up set to 182 days (26 weeks) for each simulated patient and included together with the pooled IPD for the garadacimab trials in a weighted GLM using a binomial likelihood and complementary log-log (cloglog) link function with the outcome and covariates for treatment. Differences in trial follow-up were adjusted for in the rate and binary outcomes. Relative treatment effects for garadacimab versus lanadelumab were expressed as mean differences (MD) for continuous outcomes, rate ratios (RRs) for rate outcomes, and hazard ratios (HRs) for binary outcomes. The corresponding variance was estimated using a robust sandwich estimator and 95% confidence intervals (CIs) were reported [15,26,27].
Scenario analyses
Scenario analyses were conducted to investigate the impact on the treatment effect estimates, and the ESS, when adjusting sequentially for TEMs in the analyses. For example, the first MAIC scenario adjusted for the top ranked TEM only, the second scenario adjusted for the top two ranked TEMs, the third scenario analysis adjusted for the top three ranked TEMs and the final scenario, i.e., base case, adjusted for all available ranked TEMs.
Results
Garadacimab 200 QM versus lanadelumab 300 Q2W
Balance of populations
The distribution of baseline characteristics before and after the adjustment process for the anchored analyses of the rate outcomes (e.g., time-normalized number of HAE attacks, time-normalized number of HAE attacks requiring on-demand treatment and time-normalized number of moderate and/or severe attacks) is presented in Table 2. The percentage of patients age <40 years was similar between trials (SMD = 0.005). The pooled garadacimab 200 QM + PBO population had a moderately lower mean HAE attack rate during run-in (SMD = 0.165), and substantially fewer patients with weight <75 kg (SMD = 0.357) and female patients (SMD = 0.347) compared with the lanadelumab 300 Q2W + PBO population. After adjustment, there was a 23% reduction in ESS and the pooled patient characteristics of garadacimab 200 QM + PBO matched those of lanadelumab 300 Q2W + PBO.
| Characteristics | HELP (lanadelumab 300 Q2W and PBO arms)† | Pooled VANGUARD and phase II (garadacimab 200 QM and PBO arms) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 characteristic | 2 characteristics | 3 characteristics | 4 characteristics | ||||||||
| n = 68 | n = 79‡ | ESS = 74 | ESS = 64 | ESS = 64 | ESS = 61 | ||||||
| Stat. | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | |
| HAE attack rate during run-in, mean (SD) | 3.8 (2.9)§ | 3.4 (2.28) | 0.165 | 3.8 (2.95) | 0 | 3.8 (2.96) | 0 | 3.8 (2.96) | 0 | 3.8 (2.96) | 0 |
| Weight <75 kg, % | 52.9%¶ | 35.4% | 0.357 | 33.8% | 0.392 | 52.9% | 0 | 52.9% | 0 | 52.9% | 0 |
| Age <40 years, % | 47.1%¶ | 46.8% | 0.005 | 46.3% | 0.017 | 46.2% | 0.017 | 47.1% | 0 | 47.1% | 0 |
| Female, % | 72.1%§ | 55.7% | 0.347 | 54.4% | 0.373 | 61.4% | 0.228 | 61.3% | 0.231 | 72.1% | 0 |
†
HELP SLD was pooled for the lanadelumab 300 Q2W and PBO arms following the methods reported in the Cochrane Handbook for Systematic Reviews of Interventions version 6.4.(22).
‡
One subject who received placebo in VANGUARD had missing outcome data and was removed from the analysis.
An SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference. ESS is rounded to whole numbers.
ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; PBO: Placebo; QM: Once monthly; Q2W: Every 2 weeks; SD: Standard deviation; SLD: Summary-level data; SMD: Standardized mean difference.
For the unanchored analysis performed for the proportion of attack-free patients outcome, the distribution of baseline characteristics before and after the adjustment process is presented in Table 3. The pooled garadacimab 200 QM population had slightly fewer patients with weight <75 kg (SMD = 0.017). The mean HAE attack rate during run-in (SMD = 0.006) and percentage of female patients were almost identical between populations (SMD = 0.006). There was a moderately lower percentage of patients age <40 years (SMD = 0.188) in the pooled garadacimab 200 QM population compared with the lanadelumab 300 Q2W population. After adjustment, there was a 4% reduction in ESS and the pooled patient characteristics of garadacimab 200 QM matched those of lanadelumab 300 Q2W.
| Characteristics | HELP (lanadelumab 300 Q2W) | Pooled VANGUARD and phase II (garadacimab 200 QM) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 characteristic | 2 characteristics | 3 characteristics | 4 characteristics | ||||||||
| n = 27 | n = 47 | ESS = 47 | ESS = 47 | ESS = 45 | ESS = 45 | ||||||
| Stat. | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | |
| HAE attack rate during run-in, mean (SD) | 3.5 (2.3)† | 3.5 (2.56) | 0.006 | 3.5 (2.33) | 0 | 3.5 (2.33) | 0 | 3.5 (2.33) | 0 | 3.5 (2.33) | 0 |
| Weight <75 kg, % | 37.0%‡ | 36.2% | 0.017 | 36.2% | 0.016 | 37.0% | 0 | 37.0% | 0 | 37.0% | 0 |
| Age <40 years, % | 51.9%‡ | 42.6% | 0.188 | 42.5% | 0.189 | 42.5% | 0.190 | 51.9% | 0 | 51.9% | 0 |
| Female, % | 55.6%† | 55.3% | 0.006 | 55.9% | 0.006 | 56.0% | 0.008 | 54.3% | 0.026 | 55.6% | 0 |
An SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference. ESS is rounded to whole numbers.
ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; PBO: Placebo; QM: Once monthly; Q2W: Every 2 weeks; SD: Standard deviation; SMD: Standardized mean difference.
For the anchored analysis performed for the AE-QoL change from baseline to day 182, the distribution of baseline characteristics before and after the adjustment process is presented in Table 4. The garadacimab 200 QM + PBO population from VANGUARD had a moderately lower percentage of patients age <40 years (SMD = 0.113) and substantially lower mean HAE attack rate during run-in (SMD = 0.304), percentage of patients with weight <75 kg (SMD = 0.348) and percentage of female patients (SMD = 0.250), compared with patient characteristics of lanadelumab 300 Q2W + PBO population. After adjustment, there was a 49% reduction in ESS and the patient characteristics of garadacimab 200 QM + PBO from VANGUARD matched those of lanadelumab 300 Q2W + PBO.
| Characteristics | HELP (lanadelumab 300 Q2W and PBO arms) | VANGUARD (garadacimab 200 QM and PBO arms) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 characteristic | 2 characteristics | 3 characteristics | 4 characteristics | ||||||||
| n = 68† | n = 53‡ | ESS = 31 | ESS = 27 | ESS = 27 | ESS = 27 | ||||||
| Stat. | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | |
| HAE attack rate during run-in, mean (SD) | 3.8 (2.9)§ | 3.1 (1.80) | 0.304 | 3.8 (2.97) | 0.000 | 3.8 (2.97) | 0.000 | 3.8 (2.97) | 0.000 | 3.8 (2.97) | 0.000 |
| Weight <75 kg, % | 52.9%¶ | 35.8% | 0.348 | 31.0% | 0.454 | 52.9% | 0.000 | 52.9% | 0.000 | 52.9% | 0.000 |
| Age <40 years, % | 47.1%¶ | 41.5% | 0.113 | 51.0% | 0.078 | 49.8% | 0.054 | 47.1% | 0.000 | 47.1% | 0.000 |
| Female, % | 72.1%§ | 60.4% | 0.250 | 63.0% | 0.195 | 69.7% | 0.052 | 70.7% | 0.032 | 72.1% | 0.000 |
†
HELP baseline characteristics presented are for all subjects included in ITT population, however the HELP AE-QoL outcome data is only based on 64 patients.
‡
11 subjects in VANGUARD had missing outcome data and were removed from the analysis.
An SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference. ESS is rounded to whole numbers.
ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; PBO: Placebo; QM: Once monthly; Q2W: Every 2 weeks; SD: Standard deviation; SMD: Standardized mean difference.
Time-normalized number of HAE attacks
The attack rate for patients receiving garadacimab 200 QM was lower than that of patients receiving lanadelumab 300 Q2W (RR: 0.55; 95% CI: 0.22, 1.37; p = 0.200), but this result was not statistically significant (Table 5). Scenario analyses showed consistent results (Figure 1).
| Outcome | Treatment effect | MAIC results | |||
|---|---|---|---|---|---|
| Garadacimab 200 QM vs lanadelumab 300 Q2W | Garadacimab 200 QM vs lanadelumab 300 Q4W | ||||
| Unadjusted | Fully adjusted | Unadjusted | Fully adjusted | ||
| Time-normalized number of HAE attacks | RR (95% CI) | 0.48 (0.20, 1.18) | 0.55 (0.22, 1.37) | 0.23 (0.11, 0.50) | 0.29 (0.13, 0.63) |
| Proportion of attack-free patients over the trial period† | HR (95% CI) | 1.98 (1.00, 3.93) | 1.93 (0.92, 4.03) | 3.13 (1.47, 6.67) | 3.25 (1.45, 7.29) |
| Time-normalized number of HAE attacks requiring on-demand treatment | RR (95% CI) | 0.44 (0.17, 1.13) | 0.52 (0.20, 1.35) | 0.22 (0.09, 0.51) | 0.29 (0.13, 0.66) |
| Time-normalized number of moderate and/or severe HAE attacks | 0.26 (0.08, 0.83) | 0.25 (0.07, 0.84) | 0.16 (0.06, 0.48) | 0.15 (0.05, 0.49) | |
| Change from baseline to day 182 in total AE-QoL score | MD (95% CI) | -7.69 (-23.41, 8.02) | -17.38 (-33.67, -1.08) | -11.60 (-27.24, 4.03) | -21.29 (-37.39, -5.18) |
Bold values indicate statistical significance and correspond to a two-tailed p-value < 0.05.
An RR <1 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W or lanadelumab 300 Q4W.
An HR >1 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W or lanadelumab 300 Q4W.
An MD <0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W or lanadelumab 300 Q4W.
†
Unanchored MAICs were considered the base case analysis for the proportion of attack-free patients. Anchored MAICs were not feasible.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; HR: Hazard ratio; MAIC: Matching-adjusted indirect comparison; MD: Mean difference; QM: Once monthly; Q2W: Every 2 weeks; Q4W: Every 4 weeks; RR: Rate ratio.
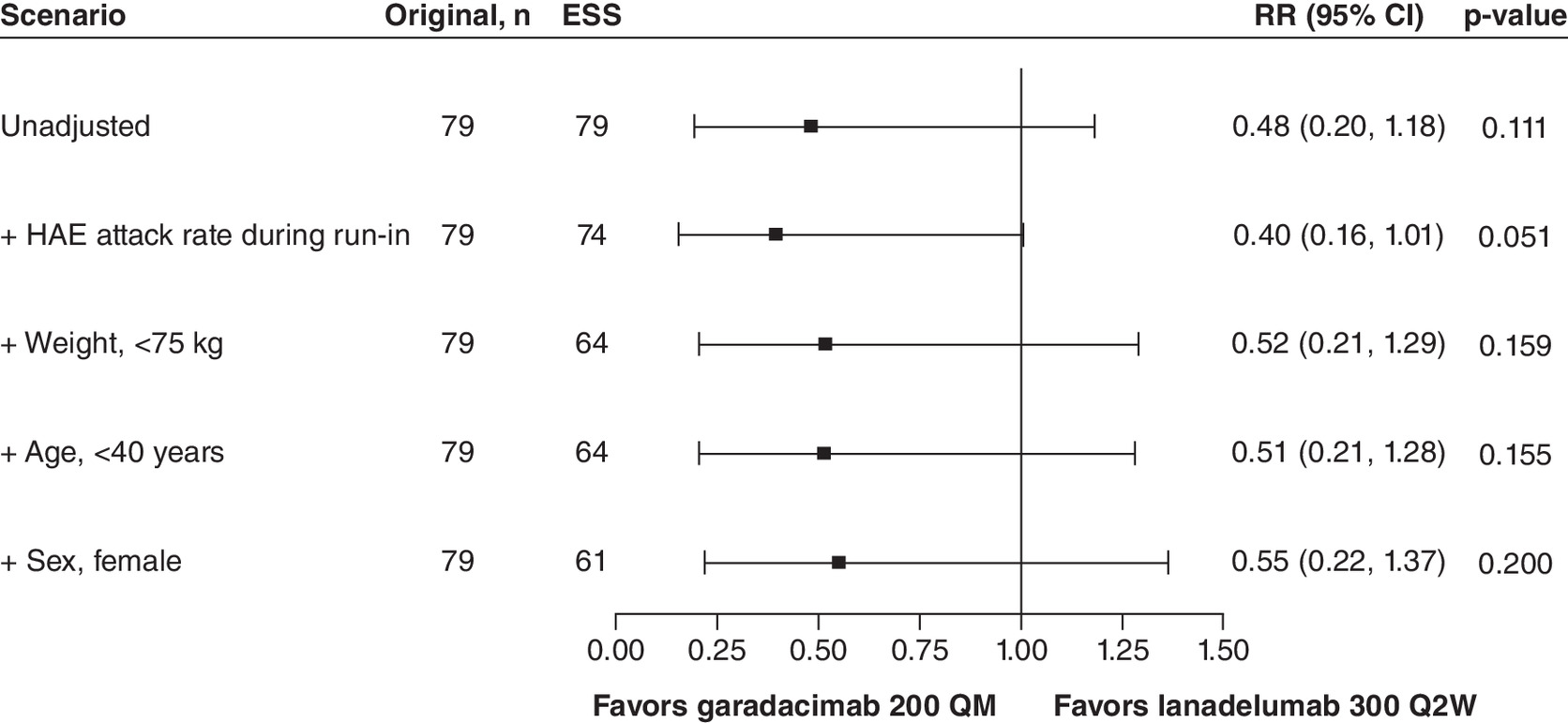
Figure 1. Summary of time-normalized number of hereditary angioedema attacks versus lanadelumab 300 Q2W.
An RR below 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W. To align with the statistical analysis methodology reported for HELP, normalized baseline HAE attack rate was included as a model covariate and the logarithm of time (days) for each patient that was observed during the treatment period was included as an offset in the model that estimates the relative treatment effect of garadacimab 200 QM versus placebo. This model-adjustment covariate and offset were included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; QM: Once monthly; Q2W: Every 2 weeks; RR: Rate ratio.
Proportion of attack-free patients (unanchored MAIC)
Patients receiving garadacimab 200 QM were more likely to be attack-free than patients receiving lanadelumab 300 Q2W (HR: 1.93; 95% CI: 0.92, 4.03; p = 0.080), but this result was not statistically significant (Table 5). Scenario analyses showed consistent results (Figure 2).
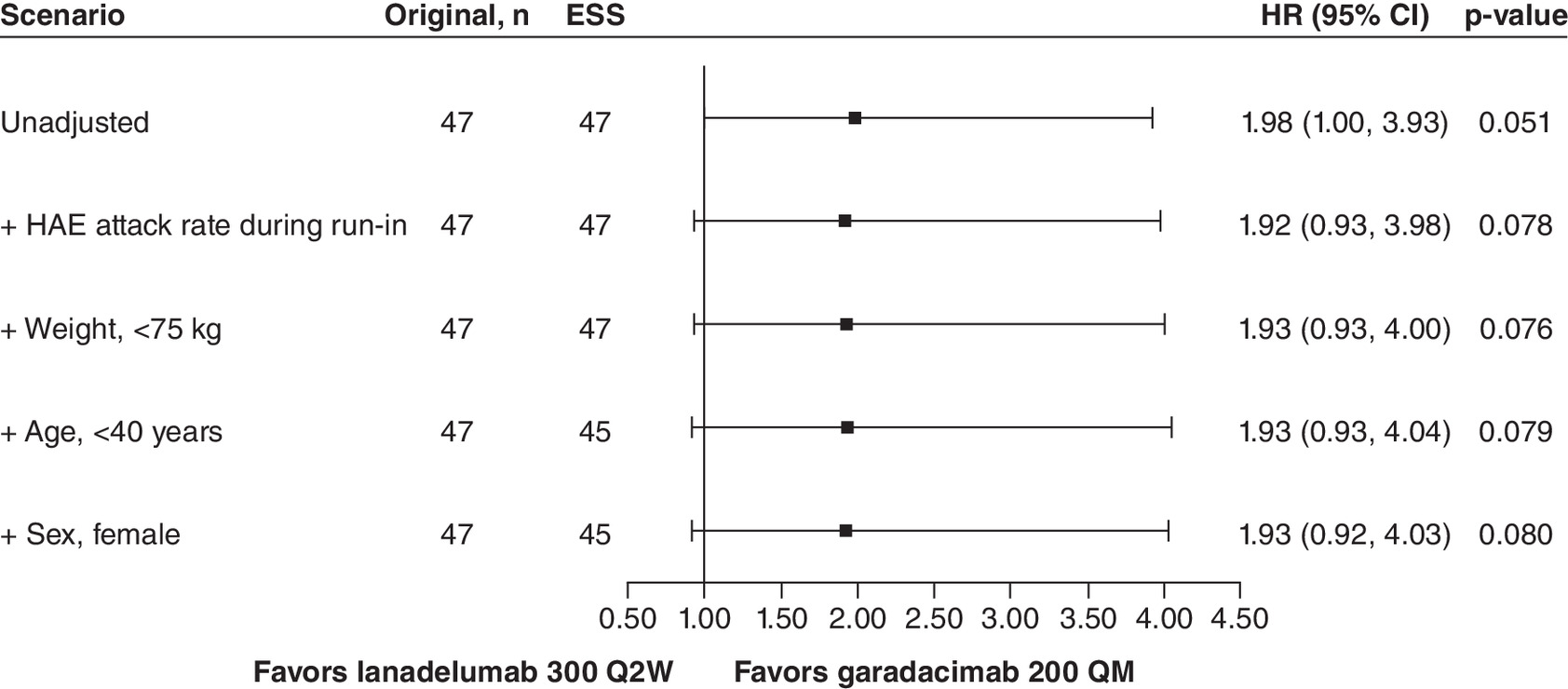
Figure 2. Summary of proportion of attack-free patients versus lanadelumab 300 Q2W.
An HR above 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W. To account for differences in trial duration, an offset of the logarithm of time (days) of the maximum follow-up for each patient was included in the model. This offset was included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; HR: Hazard ratio; QM: Once monthly; Q2W: Every 2 weeks.
Time-normalized number of HAE attacks requiring on-demand treatment
The rate of attacks requiring on-demand treatment for patients receiving garadacimab 200 QM was lower than that of patients receiving lanadelumab 300 Q2W (RR: 0.52; 95% CI: 0.20, 1.35; p = 0.180), but this result was not statistically significant (Table 5). The first scenario analysis showed a statistically significant result favoring garadacimab (Figure 3).
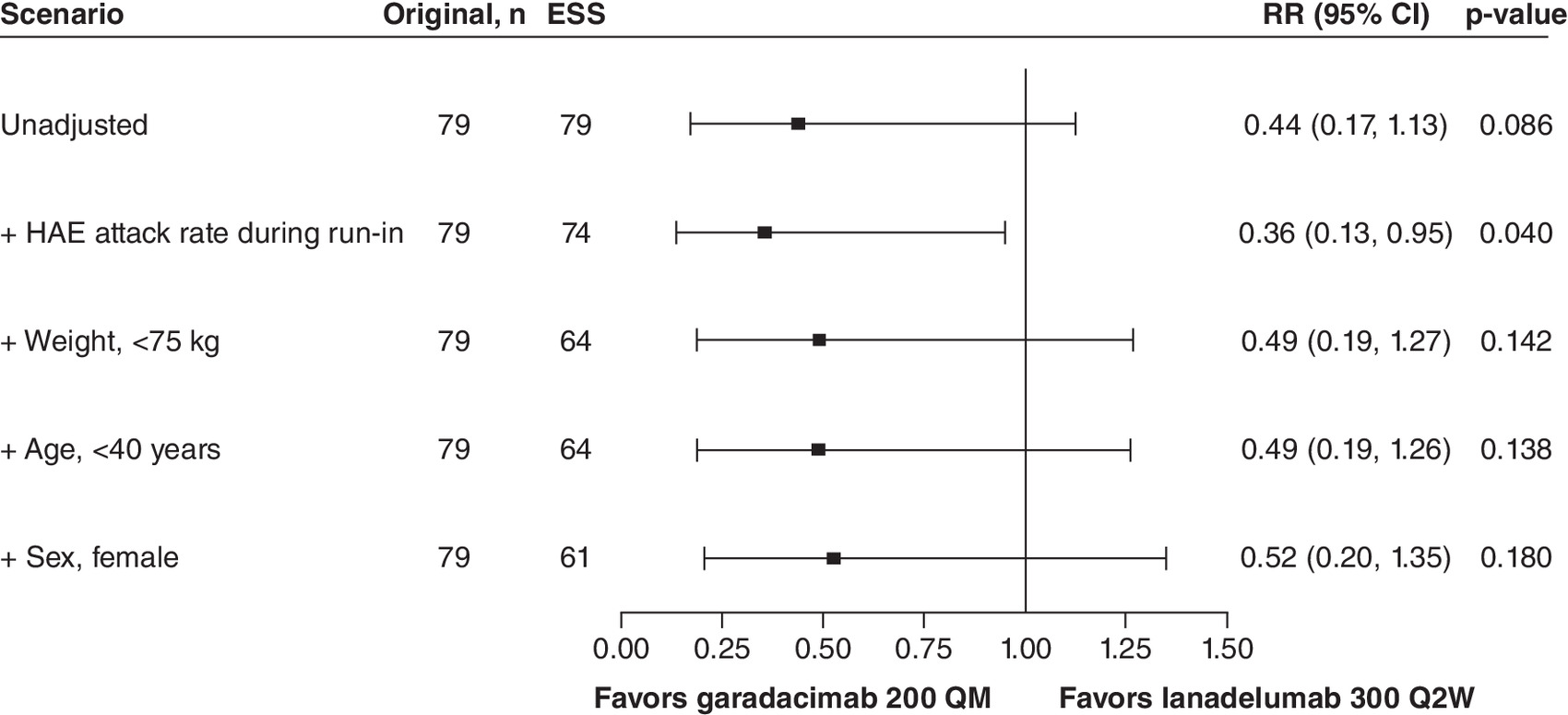
Figure 3. Summary of time-normalized number of hereditary angioedema attacks requiring on-demand treatment versus lanadelumab 300 Q2W.
An RR below 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W. To align with the statistical analysis methodology reported for HELP, normalized baseline HAE attack rate was included as a model covariate and the logarithm of time (days) for each patient that was observed during the treatment period was included as an offset in the model that estimates the relative treatment effect of garadacimab 200 QM versus placebo. This model-adjustment covariate and offset were included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; QM: Once monthly; Q2W: Every 2 weeks, RR: Rate ratio.
Time-normalized number of moderate &/or severe HAE attacks
The rate of moderate and/or severe attacks for patients receiving garadacimab 200 QM was a quarter that of patients receiving lanadelumab 300 Q2W (RR: 0.25; 95% CI: 0.07, 0.84; p = 0.026) and this was statistically significant (Table 5). Scenario analyses showed consistent results (Figure 4).
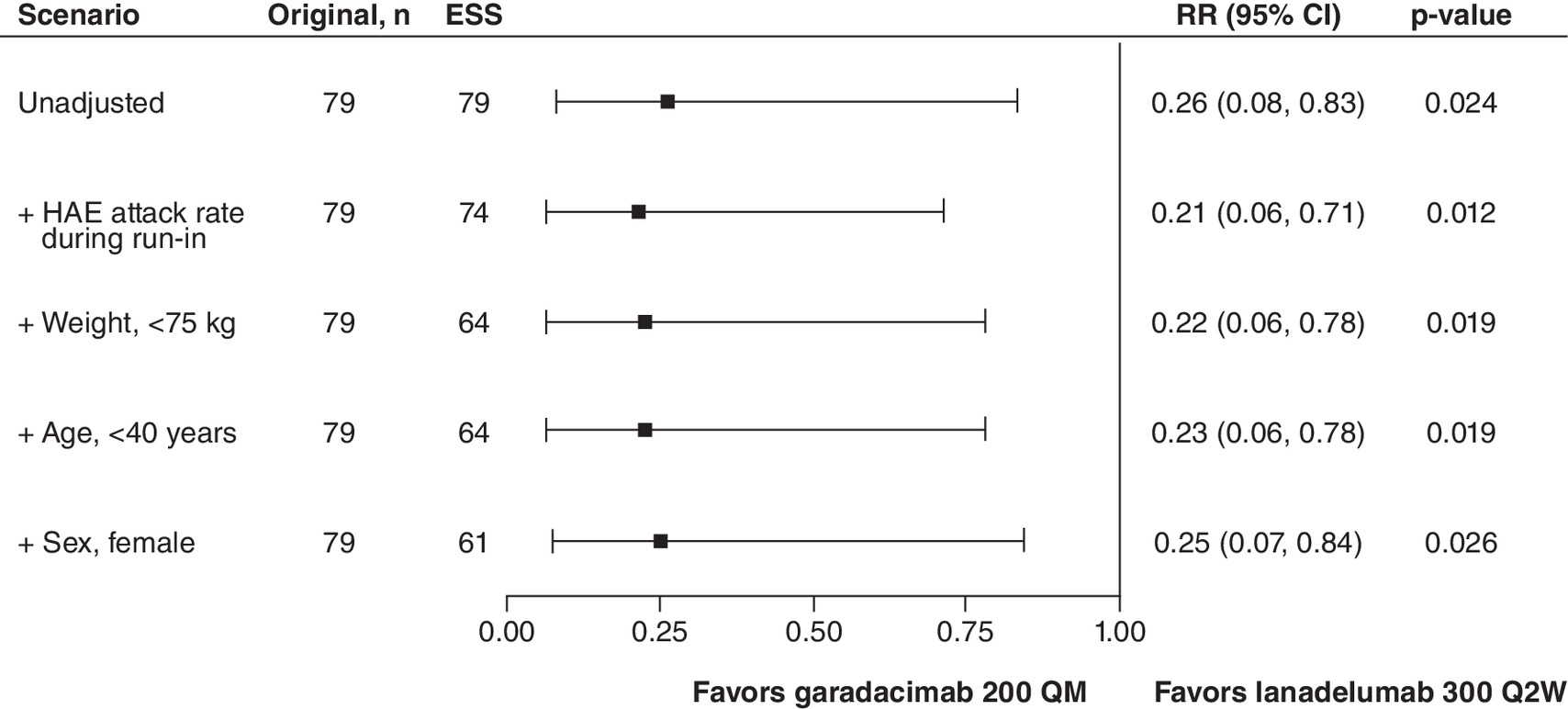
Figure 4. Summary of time-normalized number of moderate and/or severe hereditary angioedema attacks versus lanadelumab 300 Q2W.
An RR below 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W. To align with the statistical analysis methodology reported for HELP, normalized baseline HAE attack rate was included as a model covariate and the logarithm of time (days) for each patient that was observed during the treatment period was included as an offset in the model that estimates the relative treatment effect of garadacimab 200 QM versus placebo. This model-adjustment covariate and offset were included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; QM: Once monthly; Q2W: Every 2 weeks; RR: Rate ratio.
Change from baseline to day 182 in total AE-QoL score
AE-QoL scores for patients receiving garadacimab 200 QM from VANGUARD were estimated to improve by an average of 17.38 points compared with patients receiving lanadelumab 300 Q2W (MD: -17.38; 95% CI: -33.67, -1.08; p = 0.037), and this result was statistically significant (Table 5). The second and third scenario analyses showed statistically significant results favoring garadacimab (Figure 5).
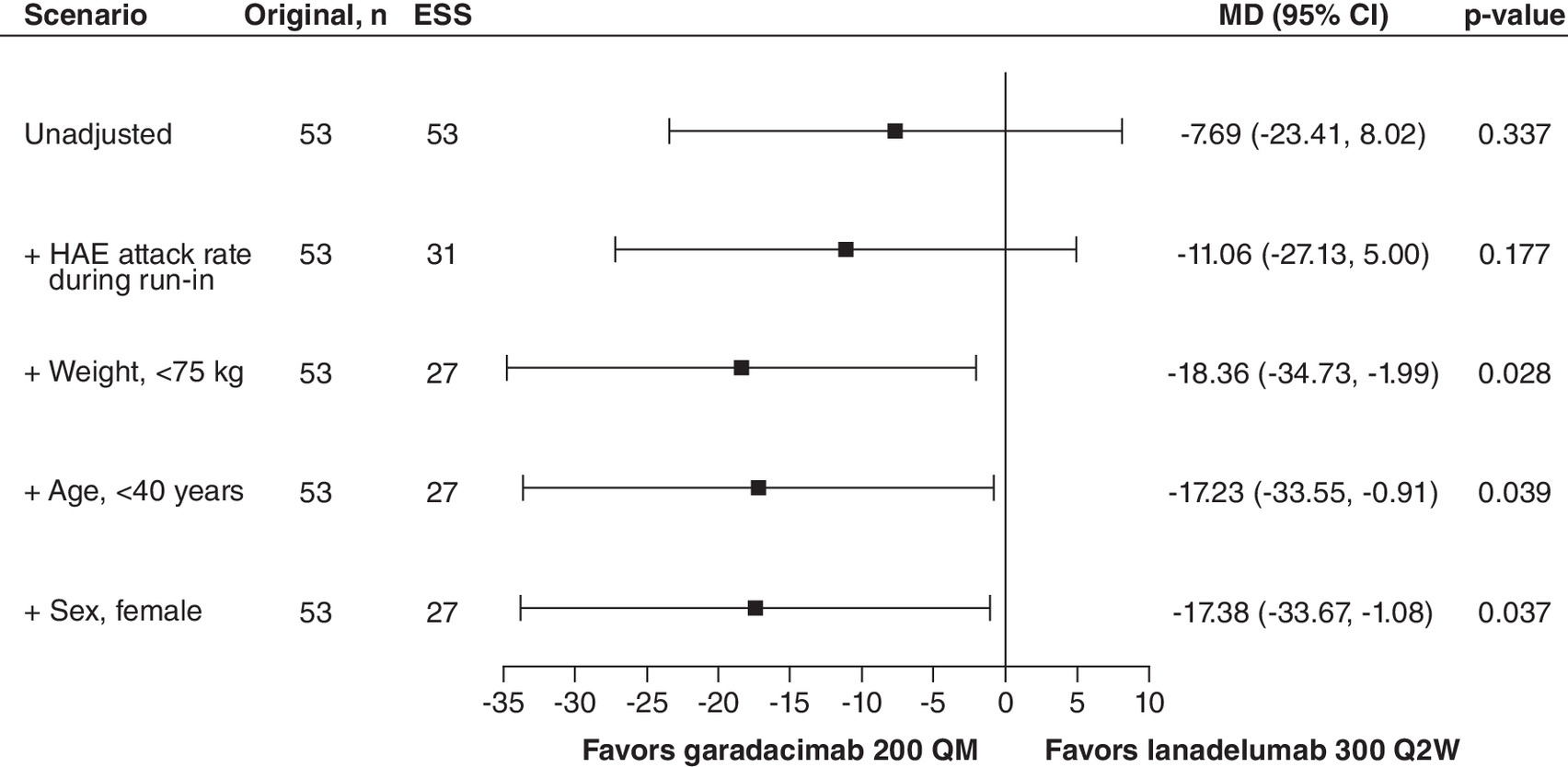
Figure 5. Change from baseline to day 182 in AE-QoL total score versus lanadelumab 300 Q2W.
An MD below 0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q2W.
AE-QoL: Angioedema Quality of Life Questionnaire; ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; MD: Mean difference; QM: Once monthly; Q2W: Every 2 weeks.
Garadacimab 200 QM versus Lanadelumab 300 Q4W
Balance of populations
The distribution of baseline characteristics before and after the adjustment process for the anchored analysis is presented in Table 6. The pooled garadacimab 200 QM + PBO population had a slightly higher percentage of patients age <40 years (SMD = 0.051) and a substantially lower mean HAE attack rate during run-in (SMD = 0.201) compared with the lanadelumab 300 Q4W + PBO population. There were also substantially fewer patients with weight <75 kg (SMD = 0.445) and female patients (SMD = 0.431) in the pooled garadacimab 200 QM population compared with the lanadelumab 300 Q4W + PBO population. After adjustment, there was a 30% reduction in ESS and the pooled patient characteristics of garadacimab 200 QM + PBO matched those of lanadelumab 300 Q4W + PBO.
| Characteristics | HELP (lanadelumab 300 Q4W and PBO arms)† | Pooled VANGUARD and phase II (garadacimab 200 QM and PBO arms) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 characteristic | 2 characteristics | 3 characteristics | 4 characteristics | ||||||||
| n = 70 | n = 79‡ | ESS = 73 | ESS = 58 | ESS = 58 | ESS = 55 | ||||||
| Stat. | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | |
| HAE attack rate during run-in, mean (SD) | 3.9 (3.0)§ | 3.4 (2.28) | 0.201 | 3.9 (3.00) | 0 | 3.9 (3.00) | 0 | 3.9 (3.00) | 0 | 3.9 (3.00) | 0 |
| Weight <75 kg, % | 57.1%¶ | 35.4% | 0.445 | 33.4% | 0.490 | 57.1% | 0 | 57.1% | 0 | 57.1% | 0 |
| Age <40 years, % | 44.3%¶ | 46.8% | 0.051 | 46.1% | 0.037 | 46.3% | 0.040 | 44.3% | 0 | 44.3% | 0 |
| Female, % | 75.7%§ | 55.7% | 0.431 | 54.4% | 0.459 | 63.2% | 0.275 | 63.4% | 0.269 | 75.7% | 0 |
†
HELP SLD was pooled for the lanadelumab 300 Q4W and PBO arms following the methods reported in the Cochrane Handbook for Systematic Reviews of Interventions version 6.4 [22].
‡
One subject who received placebo in VANGUARD had missing outcome data and was removed from the analysis.
An SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference. ESS is rounded to whole numbers.
ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; PBO: Placebo; QM: Once monthly; Q4W: Every 4 weeks; SD: Standard deviation; SMD: Standardized mean difference.
For the unanchored analysis performed for proportion of attack-free patients outcome, the distribution of baseline characteristics before and after the adjustment process is presented in Table 7. The pooled garadacimab 200 QM population had a slightly lower percentage of patients age <40 years (SMD = 0.045) and a slightly lower mean HAE attack rate during run-in (SMD = 0.073). There were substantially fewer patients with weight <75 kg (SMD = 0.247) and female patients (SMD = 0.209) in the pooled garadacimab 200 QM population compared with the lanadelumab 300 Q4W population. After adjustment, there was an 11% reduction in ESS and the pooled patient characteristics of garadacimab 200 QM matched those of lanadelumab 300 Q4W.
| Characteristics | HELP (lanadelumab 300 Q4W) | Pooled VANGUARD and phase II (garadacimab 200 QM) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 characteristic | 2 characteristics | 3 characteristics | 4 characteristics | ||||||||
| n = 29 | n = 47 | ESS = 47 | ESS = 43 | ESS = 43 | ESS = 42 | ||||||
| Stat. | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | |
| HAE attack rate during run-in, mean (SD) | 3.7 (2.5)† | 3.5 (2.56) | 0.073 | 3.7 (2.53) | 0 | 3.7 (2.53) | 0 | 3.7 (2.53) | 0 | 3.7 (2.53) | 0 |
| Weight <75 kg, % | 48.3%‡ | 36.2% | 0.247 | 35.1% | 0.269 | 48.3% | 0 | 48.3% | 0 | 48.3% | 0 |
| Age <40 years, % | 44.8%‡ | 42.6% | 0.045 | 42.7% | 0.042 | 42.5% | 0.047 | 44.8% | 0 | 44.8% | 0 |
| Female, % | 65.5%† | 55.3% | 0.209 | 55.5% | 0.205 | 57.4% | 0.167 | 57.0% | 0.176 | 65.5% | 0 |
An SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference. ESS is rounded to whole numbers.
ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; PBO: Placebo; QM: Once monthly; Q4W: Every 4 weeks; SD: Standard deviation; SMD: Standardized mean difference.
For the anchored analysis performed for the AE-QoL change from baseline to day 182, the distribution of baseline characteristics before and after the adjustment process is presented in Table 8. The garadacimab 200 QM + PBO population from VANGUARD had a slightly lower percentage of patients age <40 years (SMD = 0.056) and substantially lower mean HAE attack rate during run-in (SMD = 0.341), percentage of patients with weight <75 kg (SMD = 0.436), and percentage of female patients (SMD = 0.333), compared with patient characteristics of the lanadelumab 300 Q4W + PBO population. After adjustment, there was a 55% reduction in ESS and the patient characteristics of garadacimab 200 QM + PBO from VANGUARD matched those of lanadelumab 300 Q4W + PBO.
| Characteristics | HELP (lanadelumab 300 Q4W and PBO arms) | VANGUARD (garadacimab 200 QM and PBO arms) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | ||||||||||
| 1 characteristic | 2 characteristics | 3 characteristics | 4 characteristics | ||||||||
| n = 70† | n = 53‡ | ESS = 30 | ESS = 24 | ESS = 24 | ESS = 24 | ||||||
| Stat. | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | Stat. | SMD | |
| HAE attack rate during run-in, mean (SD) | 3.9 (3.0)§ | 3.1 (1.80) | 0.341 | 3.9 (3.01) | 0.000 | 3.9 (3.02) | 0.000 | 3.9 (3.02) | 0.000 | 3.9 (3.02) | 0.000 |
| Weight <75 kg, % | 57.1%¶ | 35.8% | 0.436 | 30.5% | 0.556 | 57.1% | 0.000 | 57.1% | 0.000 | 57.1% | 0.000 |
| Age <40 years, % | 44.3%¶ | 41.5% | 0.056 | 51.2% | 0.139 | 49.7% | 0.108 | 44.3% | 0.000 | 44.3% | 0.000 |
| Female, % | 75.7%§ | 60.4% | 0.333 | 63.2% | 0.274 | 71.6% | 0.093 | 73.5% | 0.051 | 75.7% | 0.000 |
†
HELP baseline characteristics presented are for all subjects included in ITT population, however the HELP AE-QoL outcome data is only based on 65 patients.
‡
11 subjects in VANGUARD had missing outcome data and were removed from the analysis.
An SMD between 0 and 0.1 is considered a small difference, an SMD >0.1 and ≤0.2 is a moderate difference, and an SMD >0.2 is a substantial difference. ESS is rounded to whole numbers.
ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; PBO: Placebo; QM: Once monthly; Q4W: Every 4 weeks; SD: Standard deviation; SMD: Standardized mean difference.
Time-normalized number of HAE attacks
The attack rate for patients receiving garadacimab 200 QM was less than a third of that for patients receiving lanadelumab 300 Q4W (RR: 0.29; 95% CI: 0.13, 0.63; p = 0.002) and this result was statistically significant (Table 5). Scenario analyses showed consistent results (Figure 6).
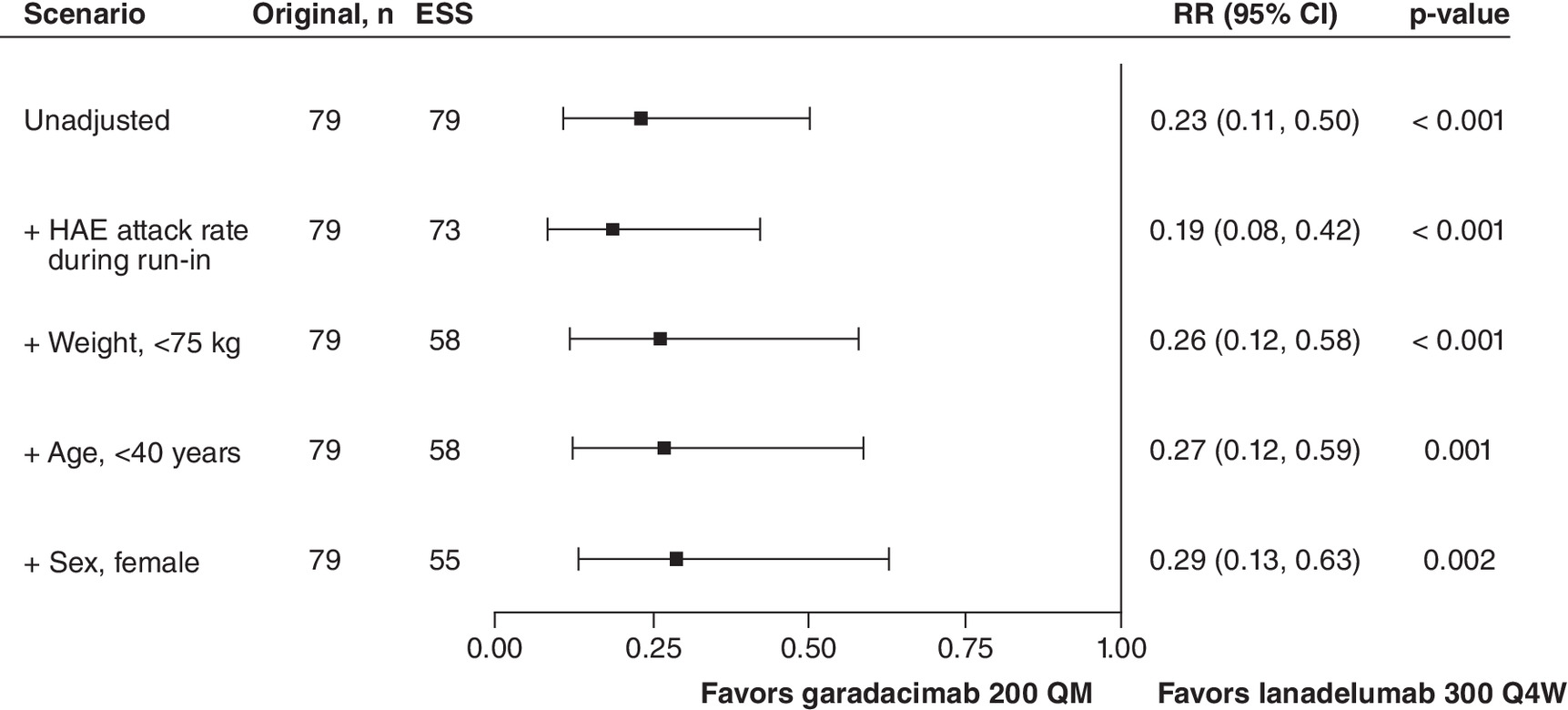
Figure 6. Summary of time-normalized number of hereditary angioedema attacks versus lanadelumab 300 Q4W.
An RR below 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q4W. To align with the statistical analysis methodology reported for HELP, normalized baseline HAE attack rate was included as a model covariate and the logarithm of time (days) for each patient that was observed during the treatment period was included as an offset in the model that estimates the relative treatment effect of garadacimab 200 QM versus placebo. This model-adjustment covariate and offset were included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; QM: Once monthly; Q4W: Every 4 weeks; RR: Rate ratio.
Proportion of attack-free patients (unanchored MAIC)
Patients receiving garadacimab 200 QM were at least three-times more likely to be attack-free than patients receiving lanadelumab 300 Q4W (HR: 3.25; 95% CI: 1.45, 7.29; p = 0.004) and this result was statistically significant (Table 5). Scenario analyses showed consistent results (Figure 7).
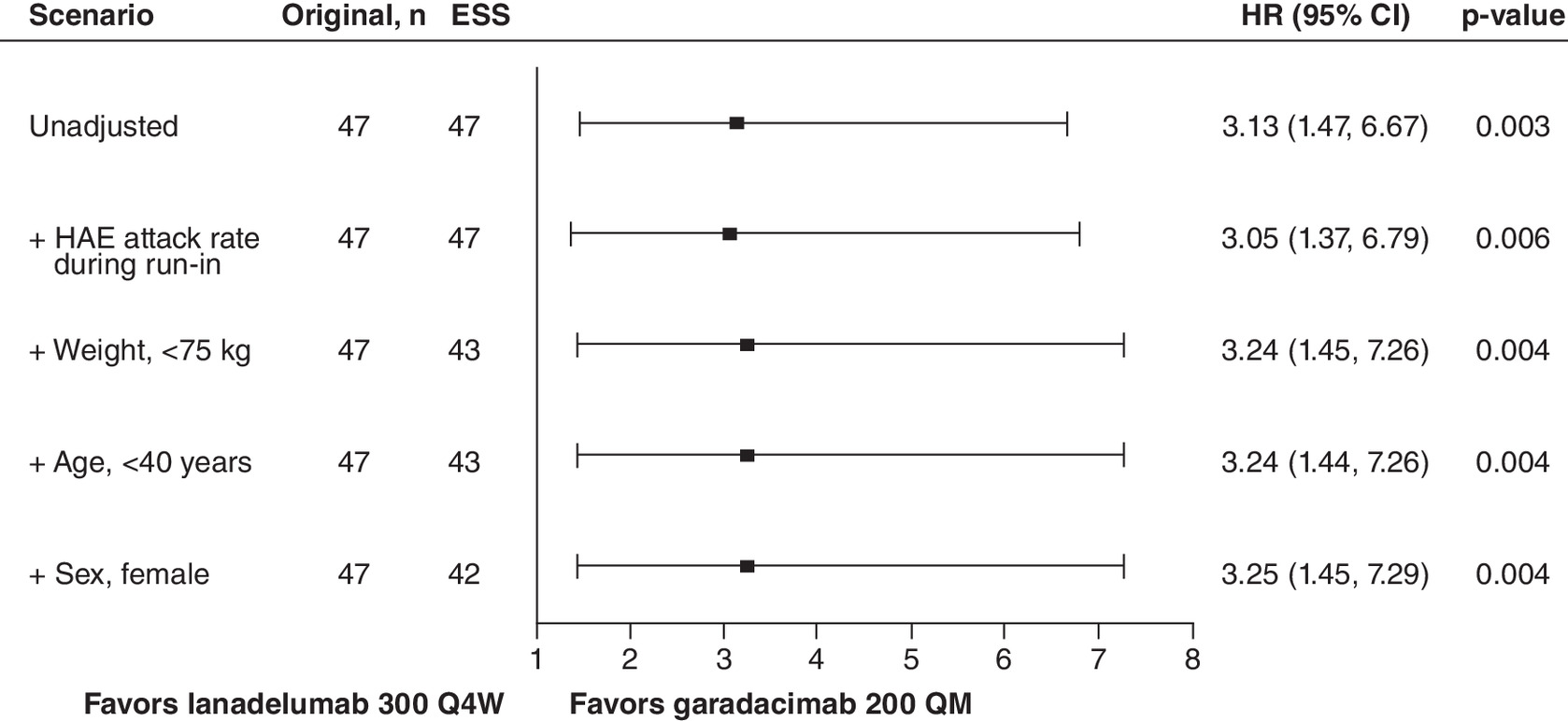
Figure 7. Summary of proportion of attack-free patients versus lanadelumab 300 Q4W.
An HR above 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q4W. To account for differences in trial duration, an offset of the logarithm of time (days) of the maximum follow-up for each patient was included in the model. This offset was included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; HR: Hazard ratio; QM: Once monthly; Q4W: Every 4 weeks.
Time-normalized number of HAE attacks requiring on-demand treatment
The attack rate for patients receiving garadacimab 200 QM was less than a third of that for patients receiving lanadelumab 300 Q4W (RR: 0.29; 95% CI: 0.13, 0.66; p = 0.003) and this result was statistically significant (Table 5). Scenario analyses showed consistent results (Figure 8).
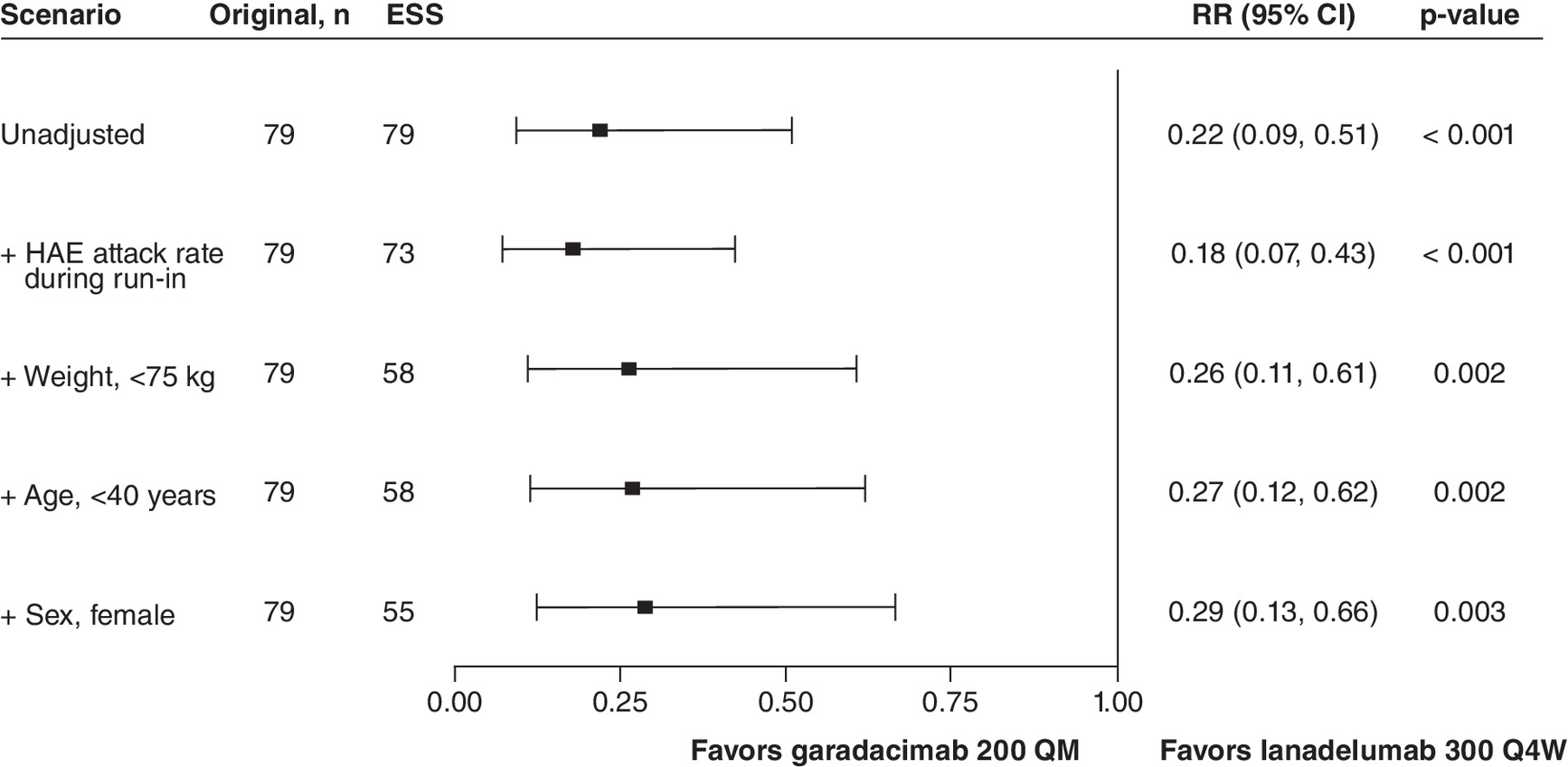
Figure 8. Summary of time-normalized number of HAE attacks requiring on-demand treatment versus lanadelumab 300 Q4W.
An RR below 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q4W. To align with the statistical analysis methodology reported for HELP, normalized baseline HAE attack rate was included as a model covariate and the logarithm of time (days) for each patient that was observed during the treatment period was included as an offset in the model that estimates the relative treatment effect of garadacimab 200 QM versus placebo. This model-adjustment covariate and offset were included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; QM: Once monthly; Q4W: Every 4 weeks; RR: Rate ratio.
Time-normalized number of moderate and/or severe HAE attacks
The attack rate for patients receiving garadacimab 200 QM was less than a fifth of that for patients receiving lanadelumab 300 Q4W (RR: 0.15; 95% CI: 0.05, 0.49; p = 0.001) and this result was statistically significant (Table 5). Scenario analyses showed consistent results (Figure 9).
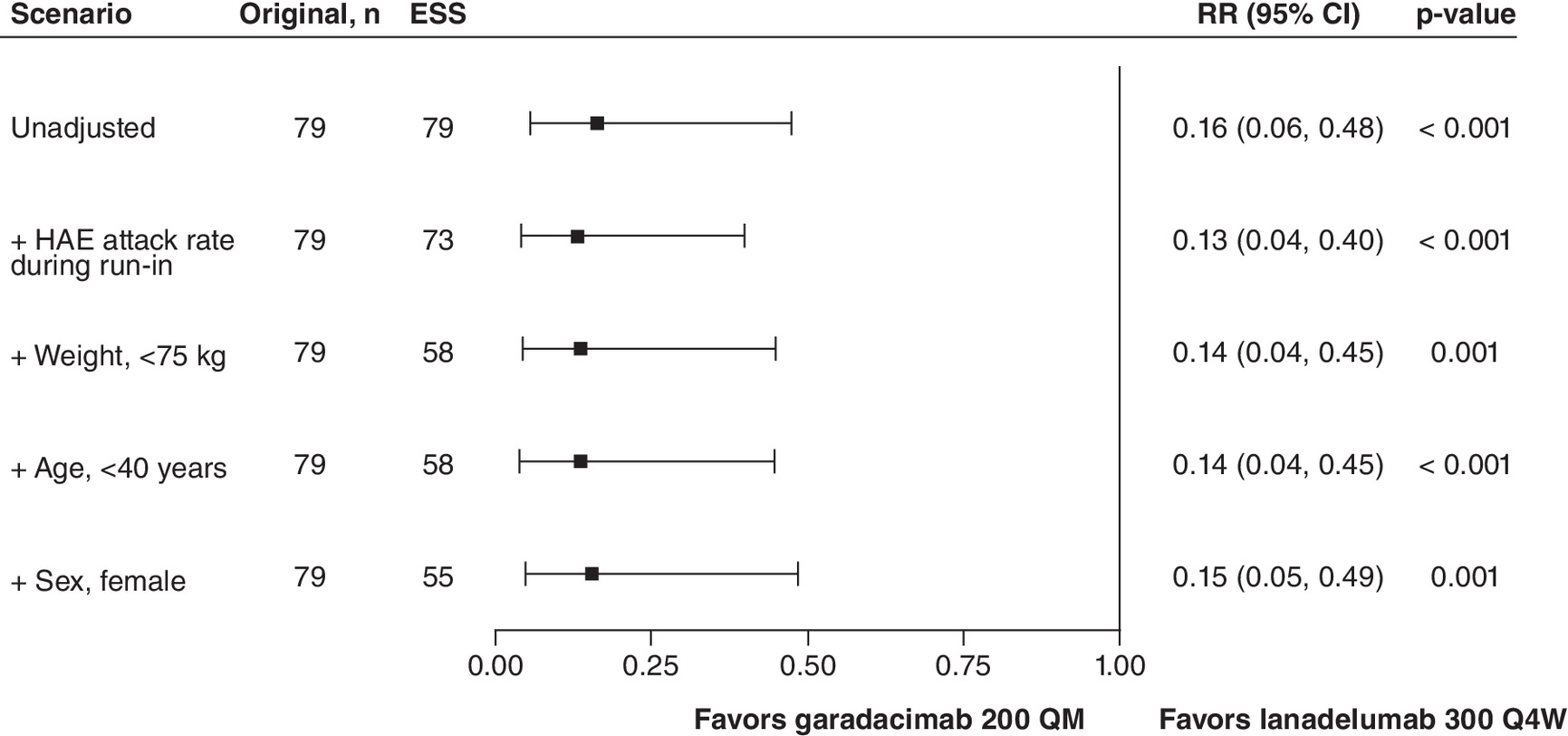
Figure 9. Summary of time-normalized number of moderate and/or severe hereditary angioedema attacks versus lanadelumab 300 Q4W.
An RR below 1.0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q4W. To align with the statistical analysis methodology reported for HELP, normalized baseline HAE attack rate was included as a model covariate and the logarithm of time (days) for each patient that was observed during the treatment period was included as an offset in the model that estimates the relative treatment effect of garadacimab 200 QM versus placebo. This model-adjustment covariate and offset were included in every MAIC scenario as well as the ‘unadjusted’ analysis.
CI: Confidence interval; ESS: Effective sample size; HAE: Hereditary angioedema; QM: Once monthly; Q4W: Every 4 weeks; RR: Rate ratio.
Change from baseline to day 182 in total AE-QoL score
AE-QoL scores for garadacimab 200 QM from VANGUARD were estimated to improve by an average of 21.29 points compared with lanadelumab 300 Q4W (MD: -21.29; 95% CI: -37.39, -5.18; p = 0.010) and this result was statistically significant (Table 5). The second and third scenario analyses showed statistically significant results favoring garadacimab (Figure 10).
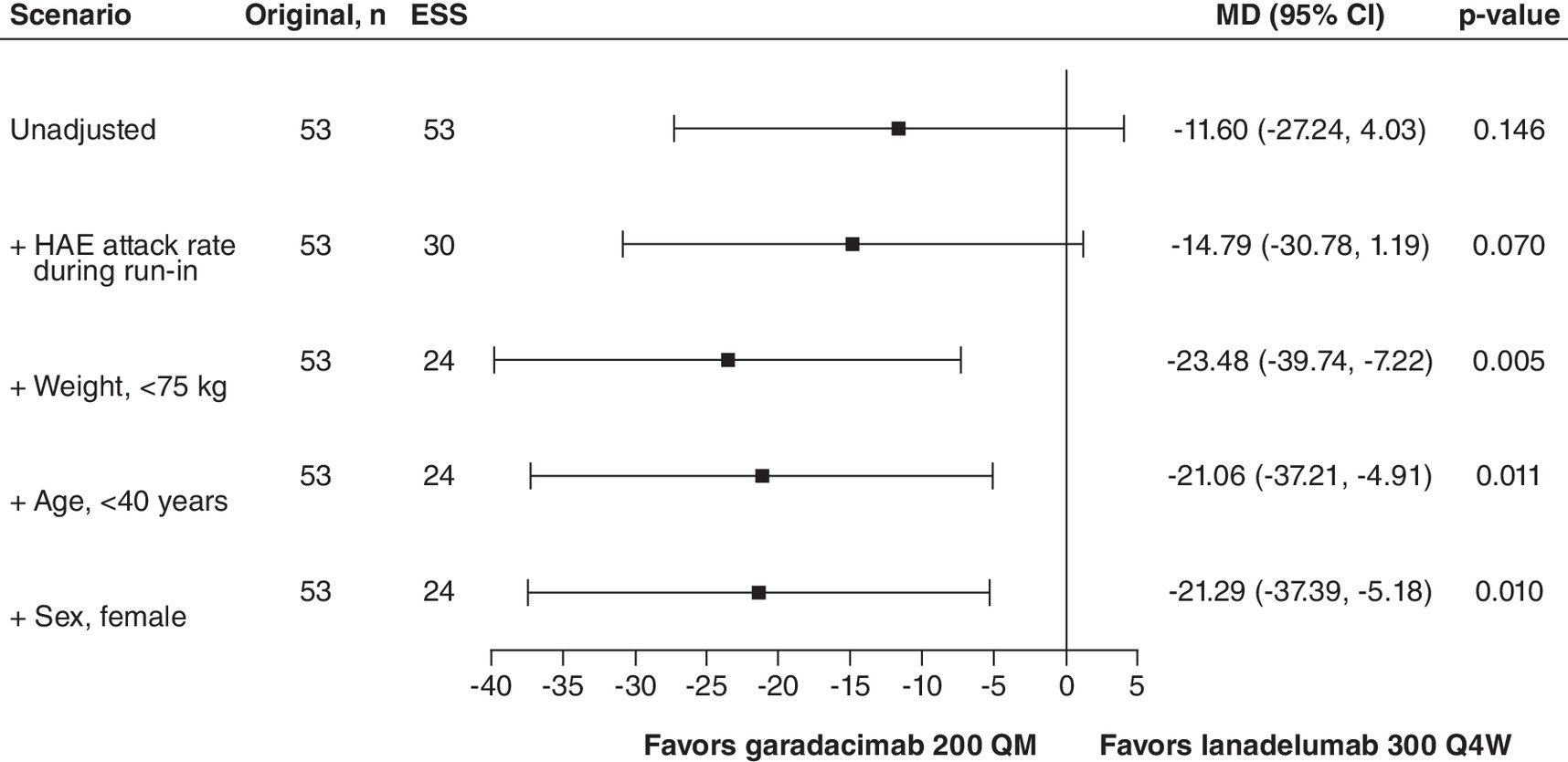
Figure 10. Change from baseline to day 182 in AE-QoL total score versus lanadelumab 300 Q4W.
An MD below 0 indicates an improved outcome for garadacimab 200 QM relative to lanadelumab 300 Q4W.
AE-QoL: Angioedema Quality of Life Questionnaire; ESS: Effective sample size; HAE: Hereditary angioedema; MAIC: Matching-adjusted indirect comparison; MD: Mean difference; QM: Once monthly; Q4W: Every 4 weeks.
Discussion
Garadacimab and lanadelumab, two monoclonal antibodies targeting respectively activated FXII [6] and kallikrein [10] in the pathophysiology of HAE, have demonstrated favorable outcomes as long-acting prophylactic treatments for HAE [6,10,23], but have not been compared in any head-to-head trials. To fill this knowledge gap, the present study conducted MAICs to estimate the comparative efficacy of garadacimab 200 QM (using IPD from VANGUARD and the phase II trial) and lanadelumab 300 Q2W/Q4W (using SLD from HELP).
In comparison to lanadelumab 300 Q2W, garadacimab 200 QM reduced the rate of time-normalized number of moderate and/or severe HAE attacks by 75% and improved AE-QoL scores from baseline to day 182 by an average of 17 points; both of these findings were statistically significant. Furthermore, in the comparison to lanadelumab 300 Q4W, garadacimab 200 QM reduced both the rate of time-normalized number of HAE attacks and HAE attacks requiring on-demand treatment by 71%, reduced the rate of time-normalized number of moderate and/or severe HAE attacks by 85%, and improved AE-QoL scores from baseline by an average of 21 points; all of these findings were statistically significant. Additionally, patients receiving garadacimab 200 QM were three-times more likely to be attack-free than patients receiving lanadelumab 300 Q4W, and this finding was statistically significant. Garadacimab also showed improvements of the remaining outcomes in comparison to lanadelumab 300 Q2W, but these results were not statistically significant.
Both garadacimab and lanadelumab inhibit bradykinin production, but they have different molecular targets in the signaling cascade. While garadacimab targets activated factor XIIa, lanadelumab inhibits a downstream target kallikrein, both of which reduce the bradykinin formation characteristic of HAE [7]. Given that the present indirect treatment comparisons showed garadacimab improved outcomes or provided at least similar benefit compared with two regimens of lanadelumab, it is possible that the inhibition of a mediator earlier in the pathway may more effectively improve outcomes for LTP in patients with HAE.
Another possible reason for the observed results is the difference in treatment schedules between trials. In the VANGUARD and phase II trials evaluating garadacimab, patients were given a loading dose (400 mg in VANGUARD, and 100 mg in phase II) once in the first month of treatment with subsequent doses of 200 mg every month for the remainder of the study duration. The HELP trial evaluating lanadelumab did not have a loading dose schedule. Although it is unclear what the impact of this loading dose has on these results, given the relatively short duration of the trials – both 26 weeks, we can speculate that the impact of the garadacimab loading dose may have influenced the beneficial outcomes observed in our analysis via increased bioavailability or through some other biological interaction of pharmacodynamic/pharmacokinetic properties leading patients to reach the therapeutic window sooner, which was then maintained by subsequent doses. While MAICs can adjust for population-level differences, inherent residual limitations to study designs may persist.
The impact of HAE on health-related QoL and patient burden should be considered when a patient is presented with LTP treatment options. Validated patient-reported outcome measures, such as the AE-QoL, are recommended to monitor disease activity, impact, and control for LTP in patients with HAE [29]. In both VANGUARD and HELP trials, AE-QoL was assessed prior to treatment administration. However, AE-QoL was assessed more frequently in VANGUARD (every month for 6 months) than in HELP (only at baseline, day 98, day 182 and follow-up). These differences in assessment frequency cannot be addressed by the present analysis, but monthly garadacimab showed statistically significant favorable change in AE-QoL score when compared with both Q2W and Q4W doses of lanadelumab. Therefore, these consistent findings suggest that the impact of assessment frequency is minimal on QoL in patients with HAE. Additionally, a minimal clinically important difference in AE-QoL score of at least 6 points for patients to notice a change has been established [30]. In this analysis, garadacimab was shown to improve AE-QoL by 17 points when compared with lanadelumab Q2W and by 21 points when compared with Q4W, suggesting that the QoL improvement with garadacimab is both statistically significant and clinically meaningful. In terms of treatment burden, patient compliance in LTP is paramount in achieving treatment success, and this can be affected by dosing schedules. While patient burden was not assessed in this analysis, in cases where the clinical efficacy between treatments is similar, a patient may prefer infrequent dosing to improve compliance and lessen the treatment burden. For this reason, once monthly dosing may be preferrable to biweekly dosing.
The comparative efficacy of lanadelumab has been previously assessed in HAE via two network meta-analyses (NMAs). One of which investigated lanadelumab versus berotralstat versus intravenous C1-esterase inhibitor [31], and another that investigated lanadelumab versus intravenous C1-esterase inhibitor [32]. Both NMAs found lanadelumab to be favored over the comparator in terms of efficacy (e.g., reduction in HAE attack rate, achieving ≥90% reduction in monthly HAE attacks, and extending attack-free intervals) [31,32]. Since garadacimab was not included in the aforementioned published NMAs, the present study is the first indirect treatment comparison analysis utilizing IPD in the form of MAICs to indirectly compare garadacimab and lanadelumab for the LTP treatment of HAE, and it is the first indirect treatment comparison to evaluate lanadelumab's comparative impact on QoL. Additionally, a prospective study was conducted in Hong Kong that investigated the efficacy, safety, and QoL of LTP in HAE using garadacimab or lanadelumab, but only aggregate outcomes were reported and the two treatments were not compared [33].
Several strengths of this study should be noted. First, analyses were performed according to best practice for conducting and reporting MAICs following the NICE DSU TSD 18 to ensure transparency and reproducibility [15]. Further, a rigorous feasibility assessment was performed to highlight any sources of inter-trial heterogeneity between the included studies (Supplementary Appendix B). One such source of heterogeneity was variation in trial duration/follow-up time across the included studies. While VANGUARD and HELP had a similar follow-up time of 26 weeks, the phase II trial for garadacimab had a notably shorter follow-up time of 12 weeks. Since patients are more likely to experience fewer events for the binary endpoint included (proportion of attack-free patients) simulated IPD was generated for HELP to account for this difference.
Additionally, since placebo was a common comparator in VANGUARD, the phase II trial for garadacimab, and HELP, anchored analyses were conducted for all outcomes, except proportion of attack-free patients due to zero events which necessitated unanchored analysis. As such, the MAICs only needed to adjust for differences in TEMs across trials. Scenario analyses were also conducted to explore how the results and ESS were impacted by incrementally adjusting for all TEMs in order of importance, as indicated by clinical experts. The base case MAIC analyses for each outcome adjusted for all feasible clinically important TEMs to ensure trial populations were aligned as closely as possible. The results across unadjusted and adjusted scenarios analyses showed similar relative efficacy of garadacimab 200 QM to lanadelumab 300 Q2W or lanadelumab 300 Q4W. This demonstrates the robustness of results and reinforces the findings from the base case analyses in this study.
This study was not without limitations. The language of the SLR was restricted to include English-only articles at the study selection stage, which may have led to the exclusion of relevant documents in other languages. The literature review results were validated by clinical experts in an attempt to mitigate the language bias. Given that most of the key studies identified were published in English journals, it is likely that this was a minor limitation. However, it should be noted that this restriction was not applied to the search strategy.
Regarding the analysis, one limitation was the inability to fully match patient populations according to eligibility criteria across trials. Despite efforts made to align populations, VANGUARD and, especially the phase II trial for garadacimab, were narrower for some eligibility criteria compared with HELP resulting in unresolved heterogeneity between trials. Key sources of heterogeneity included trial phase (the phase II trial for garadacimab differed from VANGUARD and HELP which were phase III trials), treatment period duration (the phase II trial had a shorter treatment period at 12 weeks than VANGUARD and HELP at 26 weeks), dosing schedules (every 4 weeks in the phase II trial for garadacimab, once monthly in VANGUARD, and every 2 or 4 weeks in HELP), and trial eligibility criteria (e.g., age and baseline HAE attack rate; the phase II trial for garadacimab enrolled patients ≥18 years old whereas VANGUARD and HELP enrolled patients aged ≥12 years old, and minimum baseline HAE attack rates were ≥2 attacks per month in the phase II trial for garadacimab and ≥1 attack per month in VANGUARD and HELP). Additionally, there is inherent heterogeneity in trial designs that was unable to be accommodated by the MAIC. These differences include trial phases (VANGUARD and HELP were phase III), study sponsors (VANGUARD and phase II garadacimab trials were sponsored by CSL Behring; HELP was sponsored by Shire), study locations (all trials enrolled patients from Canada, Germany and the US; VANGUARD enrolled patients from Hungary, Israel and the Netherlands; the phase II garadacimab trial enrolled patients from Israel; and HELP enrolled patients from Italy, Jordan, Puerto Rico and the UK), and the use of loading doses (present in the VANGUARD and phase II garadacimab trials; absent in the HELP trial). Although MAICs can adjust for differences in TEMs, the uncertainty in the analysis estimates must be considered in the context of these remaining differences.
Another limitation was related to data availability of all TEMs. Anchored MAIC methodology assumes that all TEMs are balanced across trials; however, these analyses could only account for characteristics reported in the comparator publications. Therefore, it is possible that covariates not considered in this analysis could have impacted the outcomes of interest. For example, history of anxiety and history of depression were respectively ranked as the third and fourth most important covariates to adjust for by clinical experts; however, these characteristics were not reported by HELP and could not be adjusted for in these analyses. Another limitation was related to low event numbers in the outcome of proportion of attack-free patients. Since zero subjects achieved attack-free status in the placebo arms of VANGUARD and the phase II trial for garadacimab, it was inappropriate to conduct an anchored MAIC for this outcome. Instead, an unanchored MAIC was performed. Unanchored MAICs rely on the assumption that both prognostic factors and TEMs are balanced across trials; however, only one subject achieved an attack-free status in the placebo arm of HELP which suggests that prognostic differences across trials may be minimal. Lastly, it should be acknowledged that some TEMs may not be accounted for in the MAICs of QoL due to reporting limitations. However, given the importance of improving QoL in aiding clinical decision-making in HAE, it was of interest for these analyses.
This study has practical implications in the treatment of patients with HAE using LTP. While indirect treatment comparisons are not replacements for direct head-to-head evidence of comparative efficacy, these analyses serve as a tool to support clinical, regulatory and reimbursement decision-making. Future directions in the LTP for HAE disease space should involve indirect analyses of safety outcomes to provide a holistic understanding of treatment benefit. Patients with HAE vary in demographics and disease-related factors, and thus population-adjusted analyses like MAICs provide valuable insight in the absence of direct evidence. This is particularly valuable in regions where modern diagnostics and therapies are limited; as international guidelines for HAE are regularly revised and updated, this analysis may be used to aid in developing a global standard for LTP in patients with HAE [29].
Conclusion
The results of these MAICs show improved efficacy and QoL with garadacimab compared with lanadelumab in the long-term prophylactic treatment of patients with HAE. Compared with lanadelumab Q2W, garadacimab statistically significantly reduced the rate of time-normalized number of moderate and/or severe HAE attacks by at least 75% and significantly improved QoL as assessed by a change from baseline in AE-QoL total score compared with lanadelumab Q2W. Compared with lanadelumab Q4W, treatment with garadacimab provided statistically significant improvements in all clinical outcomes assessed, which includes number of HAE attacks, proportion of attack-free patients, number of HAE attacks requiring on-demand treatment, number of moderate and/or severe HAE attacks and change from baseline in total AE-QoL score. Overall, these results suggest that garadacimab may provide improved therapeutic benefit compared with lanadelumab in the long-term prophylactic treatment of patients with HAE.
Summary points
•
Garadacimab and lanadelumab are two monoclonal antibodies targeting activated FXII and kallikrein, respectively in the pathophysiology of hereditary angioedema (HAE), that have demonstrated favorable outcomes as long-acting prophylactic treatments for HAE; however, the comparative efficacy of garadacimab and lanadelumab has not been assessed in any head-to-head clinical trials.
•
To fill this data gap, matching-adjusted indirect comparisons (MAICs) were conducted to assess the relative efficacy and impact on quality of life of garadacimab (200 mg QM) and two dosages of lanadelumab (300 mg Q2W and 300 mg Q4W) for the long-term prophylaxis treatment in patients with HAE.
•
The MAICs used individual patient data from two garadacimab trials (VANGUARD and a phase II trial) and summary-level data from one trial for lanadelumab (HELP). Prior to analysis, a rigorous feasibility assessment of inter-trial heterogeneity was conducted and trials were determined to be similar enough to compare.
•
A list of potential treatment effect modifiers was developed and then ranked in order of importance by clinical experts. The final list was applied to all outcomes and the base case analyses adjusted for all treatment effect modifiers based on availability.
•
The primary outcome was time-normalized number of HAE attacks. Secondary efficacy outcomes included time-normalized number of HAE attacks requiring on-demand treatment, time-normalized number of moderate and/or severe HAE attacks and proportion of attack-free patients. Quality of life was also assessed via change from baseline in AE-QoL total score.
•
Given the presence of a common comparator (placebo), anchored MAICs were considered feasible for all outcomes except proportion of attack-free patients. Unanchored MAICs were conducted for this outcome given zero patients experienced an event in the placebo arms of VANGUARD and the phase II garadacimab trials.
•
Compared with lanadelumab 300 Q2W, garadacimab 200 QM statistically significantly reduced number of moderate and/or severe HAE attacks and improved AE-QoL score.
•
Compared with lanadelumab 300 Q4W, garadacimab 200 QM showed statistically significant improvements in all outcomes assessed, which includes number of HAE attacks, proportion of attack-free patients, number of HAE attacks requiring on-demand treatment, number of moderate and/or severe HAE attacks and change from baseline in total AE-QoL score.
•
Our results suggest that garadacimab may provide improved efficacy and quality of life in long-term prophylactic treatment of patients with hereditary angioedema.
Author contributions
All authors participated in the conception and design of the study. S Walsh, A Haltner, M Bartlett and IA Samjoo contributed to the collection and analysis of the data. All authors contributed to the interpretation of the data and critically reviewed for importance of intellectual content for the work. All authors were responsible for drafting or reviewing the manuscript and for providing final approval. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work and have given their approval for this version to be published.
Acknowledgments
The authors acknowledge Joanna Bielecki who developed, conducted and documented the database searches; and Elizabeth Halloran, Kerise Clarke and Amrita Debnath for their assistance with the literature review. All are employed by EVERSANA, Canada.
Financial disclosure
This work was supported by CSL Behring. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
J Sears, Y Li, I Jacobs and N Ray are employees of CSL Behring, USA. M Kelly is an employee of CSL Behring Ltd. S Gavata-Steiger and C Nenci are employees of CSL Behring AG. I Pragst is an employee of CSL Innovation GmbH, Germany. S Walsh, A Haltner, M Bartlett and IA Samjoo are employees of EVERSANA, Canada and USA, which was a paid consultant to CSL Behring in connection with the development of this manuscript. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
Medical writing and editorial assistance were provided by S Walsh, A Haltner, M Bartlett and IA Samjoo from EVERSANA, Canada and USA. Medical writing and editorial assistance were funded by CSL Behring Ltd.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 215.09 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bernstein J. Severity of hereditary angioedema, prevalence, and diagnostic considerations. Am. J. Manag. Care 24(Suppl. 14), S292–S298 (2018).
2.
Banerji A, Davis KH, Brown TM et al. Patient-reported burden of hereditary angioedema: findings from a patient survey in the United States. Ann. Allergy Asthma Immunol. 124(6), 600–607 (2020).
3.
Mendivil J, Murphy R, de la Cruz M et al. Clinical characteristics and burden of illness in patients with hereditary angioedema: findings from a multinational patient survey. Orphanet J. Rare Dis. 16(1), 94 (2021).
4.
CSL312 (Garadacimab) in the prevention of hereditary angioedema attacks (NCT04656418). Updated 3 August 2022. Available from: https://ClinicalTrials.gov/show/NCT04656418
5.
CSL Behring. Study Report: a multicenter, randomized, placebo-controlled, parallel-arm study to investigate the efficacy, pharmacokinetics, and safety of CSL312 in subjects with hereditary angioedema. (2022).
6.
Craig TJ, Reshef A, Li HH et al. Efficacy and safety of garadacimab, a factor XIIa inhibitor for hereditary angioedema prevention (VANGUARD): a global, multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 401(10382), 1079–1090 (2023).
•• Presents baseline characteristics and primary and secondary outcome results (including efficacy and safety outcomes) from the pivotal Phase III VANGUARD trial investigating garadacimab.
7.
Cohn DM, Renné T. Targeting factor XIIa for therapeutic interference with hereditary angioedema. J. Intern. Med. 296(4), 311–326 (2024).
8.
CSL Behring. Long-term safety and efficacy of CSL 312 (garadacimab) in the prophylactic treatment of hereditary angioedema attacks. Updated 17 October 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT04739059?term=garadacimab&draw=2&rank=2
9.
EMA. Andembry garadacimab EMEA/H/C/006116 Authorisation Details. (2025).
• Details the market authorization status of garadacimab by the EMA.
10.
Banerji A, Riedl MA, Bernstein JA et al. Effect of lanadelumab compared with placebo on prevention of hereditary angioedema attacks: a randomized clinical trial. JAMA 320(20), 2108–2121 (2018).
•• Presents baseline characteristics and primary and secondary outcome results (including efficacy, safety and quality of life outcomes) from the Phase III HELP trial investigating lanadelumab.
11.
European Medicines Agency. Takhzyro (lanadelumab). Product information (2018). Available from: https://www.ema.europa.eu/en/documents/overview/takhzyro-epar-medicine-overview_en.pdf
12.
Food and Drug Administration. TAKHZYRO® (lanadelumab-flyo) injection, for subcutaneous use 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761090s010lbl.pdf
13.
Government of Canada. Summary Basis of Decision for Takhzyro. Updated 18 February 2019. Available from: https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?linkID=SBD00420#:∼:text=To%20ensure%20safe%20and%20effective,acute%20treatment%20of%20HAE%20attacks
14.
TGA. Australian Public Assessment Report for Lanadelumab. Updated March 2020. Available from: https://www.tga.gov.au/sites/default/files/auspar-lanadelumab-200304.pdf
15.
Phillippo D, Ades T, Dias S, Palmer S, Abrams KR, Welton N. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE. (2016).
•• Outlines recommendations for methods of conducting matching-adjusted indirect comparisons.
16.
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 50(6), 683–691 (1997).
17.
Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. Methods for population-adjusted indirect comparisons in health technology appraisal. Med. Decision Making 38(2), 200–211 (2018).
18.
Moher D, Shamseer L, Clarke M et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 4(1), 1 (2015).
19.
Shamseer L, Moher D, Clarke M et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 350, g7647 (2015).
20.
York Uo. Systematic Reviews CRD's guidance for undertaking reviews in health care. (2008).
21.
ClinicalTrials.gov. A study of JNJ-68284528, a chimeric antigen receptor T cell (CAR-T) therapy directed against B-cell maturation antigen (BCMA) in participants with relapsed or refractory multiple myeloma (CARTITUDE-1). Updated 10 March 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03548207?term=NCT03548207&draw=2&rank=1
22.
CSL Behring. 253590_CSL312_3001_Final_Tables_20220829. (2022).
23.
Craig T, Magerl M, Levy DS et al. Prophylactic use of an anti-activated factor XII monoclonal antibody, garadacimab, for patients with C1-esterase inhibitor-deficient hereditary angioedema: a randomised, double-blind, placebo-controlled, Phase II trial. Lancet 399(10328), 945–955 (2022).
24.
Signorovitch JE, Wu EQ, Yu AP et al. Comparative effectiveness without head-to-head trials. Pharmacoeconomics 28(10), 935–945 (2010).
25.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 28(25), 3083–3107 (2009).
26.
Zeileis A. Object-oriented computation of sandwich estimators. J. Stat. Software 16(9), 1–16 (2006).
27.
Zeileis A. Econometric computing with HC and HAC covariance matrix estimators. J. Stat. Software 11(10), 1–17 (2004).
28.
CADTH. CADTH common drug review clinical review report for lanadelumab (Takhzyro). (2020).
29.
Maurer M, Magerl M, Betschel S et al. The international WAO/EAACI guideline for the management of hereditary angioedema—the 2021 revision and update. Allergy 77(7), 1961–1990 (2022).
30.
Kulthanan K, Chularojanamontri L, Rujitharanawong C, Weerasubpong P, Maurer M, Weller K. Angioedema quality of life questionnaire (AE-QoL) – interpretability and sensitivity to change. Health Qual. Life Outcomes 17(1), 160 (2019).
31.
Watt M, Malmenäs M, Romanus D, Haeussler K. Network meta-analysis for indirect comparison of lanadelumab and berotralstat for the treatment of hereditary angioedema. J. Comp. Eff. Res. 12(6), e220188 (2023).
• Presents efficacy results of an network meta-analyses (NMA) investigating lanadelumab versus berotralstat versus intravenous C1-esterase inhibitor.
32.
Mendivil JA-O, Malmenäs M, Haeussler K, Hunger M, Jain G, Devercelli G. Indirect comparison of lanadelumab and intravenous C1-INH using data from the HELP and CHANGE studies: bayesian and frequentist analyses. Drugs R D 21(1), 113–121 (2021).
• Presents efficacy results of an NMA investigating lanadelumab versus intravenous C1-esterase inhibitor.
33.
Wong JCY, Chiang V, Lam DLY et al. Long-term prophylaxis for hereditary angioedema: initial experiences with garadacimab and lanadelumab. J. Allergy Clin. Immunol. Glob. 2(4), 100166 (2023).
Information & Authors
Information
Published In
Copyright
© 2025 CSL Behring. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 20 December 2024
Accepted: 5 June 2025
Published online: 10 July 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Matching-adjusted indirect comparison between garadacimab and lanadelumab for the long-term prophylactic treatment of patients with hereditary angioedema. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0237
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sabrina Meisgen, Franziska Fischer, Yinglei Li, The evolving treatment landscape for hereditary angioedema in Sweden, Frontiers in Immunology, 10.3389/fimmu.2026.1828443, 17, (2026).
- Katarzyna Poznańska-Kurowska, Małgorzata Skibińska, Dorota Lorenz, Waleed Aman Ur Rahman, Marcin Kurowski, Acquired Angioedema—A Challenge in Medical Practice: A Narrative Review, Journal of Clinical Medicine, 10.3390/jcm15103800, 15, 10, (3800), (2026).
- Emel Aygören‐Pürsün, Regina Treudler, Petra Staubach, Inmaculada Martinez Saguer, Thomas Linhoff, Markus Magerl, Garadacimab for the long‐term prophylaxis of hereditary angioedema, JDDG: Journal der Deutschen Dermatologischen Gesellschaft, 10.1111/ddg.70276, (2026).
- Henriette Farkas, Lili Voloncs-Mindszenthy, Hanga Réka Horváth, Monoclonal antibodies in the management of hereditary angioedema, Expert Opinion on Biological Therapy, 10.1080/14712598.2026.2664733, (1-15), (2026).
- A. Volf, D. Tabynbayeva, A. Nagornaya, S. Kerimbay, M. Nalobina, O. Dedova, B. Koshkarbayeva, A. Knaus, M. Izmailovich, Diagnostic Challenges in Hereditary Angioedema with Normal C1-Inhibitor Levels: A Clinical Case Report, Juvenis Scientia, 10.32415/jscientia_2025_11_5_27-34, 11, 5, (27-34), (2025).