Efficacy of CARVYKTI in CARTITUDE-4 versus other conventional treatment regimens for lenalidomide-refractory multiple myeloma using inverse probability of treatment weighting
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The phase III randomized controlled trial (RCT) CARTITUDE-4 (NCT04181827) demonstrated superiority of CARVYKTI (ciltacabtagene autoleucel; cilta-cel) over daratumumab, pomalidomide and dexamethasone (DPd) and pomalidomide, bortezomib and dexamethasone (PVd) for relapsed/refractory multiple myeloma (RRMM) patients who have received one to three prior line(s) of therapy (LOT[s]) including an immunomodulatory agent and a proteasome inhibitor, and are refractory to lenalidomide. These analyses estimate the relative efficacy between cilta-cel and other common treatment regimens, for which no direct comparative evidence is available. Materials & methods: Patient data were available from the CARTITUDE-4, CASTOR, CANDOR and APOLLO RCTs. Imbalances between cohorts on key patient characteristics were adjusted for using inverse probability of treatment weighting (IPTW). Relative efficacies were estimated with response rate ratios (RRs) and 95% confidence intervals (CIs) for overall response rate (ORR), very good partial response or better rate (≥VGPR) and complete response or better rate (≥CR), and with hazard ratios (HRs) and 95% CIs for progression-free survival (PFS). Sensitivity analyses using different analytical methods and additional covariates were explored. Results: Key characteristics were well balanced across cohorts after IPTW. Cilta-cel showed statistically significant benefit in PFS (HRs: 0.11–0.51), ≥VGPR (RRs: 1.51–5.13) and ≥CR (RRs: 2.90–35.24) versus all comparators, and statistically significant improvements in ORR over most comparator regimens (RRs: 1.22–1.90). Results were consistent across sensitivity analyses. Conclusion: Cilta-cel demonstrated benefit over other common treatment regimens, highlighting its potential to become a new standard of care option for lenalidomide-refractory RRMM patients with one to three prior LOT(s). These comparisons help to demonstrate the improved efficacy of cilta-cel in countries where the standard of care may differ from DPd/PVd.
Background
Multiple myeloma (MM) is a malignant disorder of plasma cells, with the potential to cause significant immunodeficiency, skeletal destruction, anemia, renal failure, hyperviscosity and secondary amyloidosis [1,2]. The disease is defined as relapsed or refractory multiple myeloma (RRMM) when it becomes nonresponsive or progressive on therapy within 60 days of the last treatment in patients who had previously achieved a minimal response or better on therapy [3]. Treatment regimens for patients with RRMM often include immunomodulatory agents (IMiDs) and proteasome inhibitors (PIs). Lenalidomide is an IMiD that has been increasingly preferred as part of first-line treatment for MM patients; as a result, many patients become refractory to lenalidomide as early as first relapse [4,5]. There is an unmet need in the lenalidomide-refractory patient population as these patients have limited treatment options, poor prognosis and there is no clear standard of care [6].
CARVYKTI (ciltacabtagene autoleucel; cilta-cel) is a chimeric antigen receptor T-cell (CAR-T) therapy that potentially addresses this unmet medical need, treating RRMM by targeting the B-cell maturation antigen (BCMA), which is a surface-antigen of myeloma cells. Results from the CARTITUDE-4 randomized trial demonstrated the superiority of cilta-cel over the treatment regimens of pomalidomide, bortezomib and dexamethasone (PVd) and daratumumab, pomalidomide and dexamethasone (DPd) on multiple clinical end points in patients with RRMM who have received one to three prior line(s) of therapy (LOT[s]) that included an IMiD and a PI, and who are refractory to lenalidomide [7]. However, standard of care options for lenalidomide-refractory patients with RRMM can vary in different regions of the world where DPd and PVd may not be among the currently accepted treatments. Moreover, the PI carfilzomib has activity in RRMM and is the backbone of various treatment regimens in this setting. Thus, a comparison of cilta-cel against other treatment options including carfilzomib-based regimens would be necessary to determine its potential as a new standard of care.
Other treatment options for RRMM patients who are refractory to lenalidomide include: daratumumab in combination with bortezomib and dexamethasone (DVd) [8], bortezomib in combination with dexamethasone (Vd) [8], daratumumab in combination with carfilzomib and dexamethasone (DKd) or carfilzomib in combination with dexamethasone (Kd) [9], and pomalidomide in combination with dexamethasone (Pd) [10]; all of which were treatment regimens assessed in the CASTOR, CANDOR and APOLLO randomized controlled trials (RCTs) [8–10]. In the absence of head-to-head trial data comparing cilta-cel versus these other therapies, adjusted comparisons between cilta-cel and these treatment regimens can be used to assess the relative efficacy while accounting for differences in patient populations across trials. The availability of individual patient data (IPD) for DVd, Vd, DKd, Kd and Pd allowed for identification of a sub-cohort from the trial populations in line with the CARTITUDE-4 inclusion criteria for use in inverse probability of treatment weighting (IPTW) and multivariable regression analyses. The objective of this analysis was to estimate the relative efficacy in patients randomized to the cilta-cel cohort (i.e., patients who underwent apheresis) in CARTITUDE-4 versus each of these treatment regimens in the same target population using IPTW by leveraging IPD. These comparisons can provide valuable information to demonstrate the improved efficacy of cilta-cel in settings where the standard of care may be different from DPd/PVd.
Methods
Data sources
CARTITUDE-4
CARTITUDE-4 is a global phase III, open-label RCT (NCT04181827) evaluating cilta-cel versus PVd or DPd in patients with RRMM who have received one to three prior LOT(s) that included an IMiD and a PI, and who are refractory to lenalidomide. Details for CARTITUDE-4 have been previously published [7]. At the data cut off for this interim analysis (1 November 2022), the median duration of follow-up was 15.9 months.
Daratumumab clinical trials
CASTOR [8], CANDOR [9] and APOLLO [10] are multicenter, open-label, randomized, phase III trials in RRMM patients evaluating the efficacy and safety of DVd versus Vd (CASTOR), DKd versus Kd (CANDOR), and DPd versus Pd (APOLLO). Full study details have been published [8–10]. As direct comparisons between cilta-cel and DPd were conducted in the CARTITUDE-4 trial, DPd was not included as a comparator in the present analysis. Based on the availability of the IPD for each trial, the median follow-up for patients included in the present analysis was 74.3 months (data cut-off: 23 June 2021) for CASTOR, 16.9 months (data cut-off: 14 July 2019) for CANDOR and 39.9 months (data cut-off: 31 May 2022) for APOLLO. A summary of the study characteristics of the comparator trials is included in Supplementary Table 1. These treatment regimens were selected due to the availability of IPD for which a wider and stronger range of adjusted comparisons could be conducted. Additional analyses utilizing matching-adjusted indirect comparisons are being reported separately.
Study population & design
IPD were available from all data sources. The CARTITUDE-4 cohort consisted of patients who were randomized to the cilta-cel cohort (all patients underwent apheresis). Comparison of the cilta cel cohort was done versus each of the comparator cohorts, which consisted of all eligible patients who had received one of the following comparator treatments: DVd, Vd, DKd, Kd, or Pd. Patients from the daratumumab clinical trials were included in the comparator cohorts if they met at baseline the following key inclusion criteria from the CARTITUDE-4 trial: have received one to three prior LOTs including a PI and an IMiD, were refractory to lenalidomide and Eastern Cooperative Oncology Group (ECOG) status 0–1. As none of the patients in the daratumumab clinical trials had prior treatment with anti-CD38, patients with prior exposure to anti-CD38 therapies in the cilta-cel cohort were excluded. The index date was defined as the date of randomization within each trial.
Baseline characteristics for population alignment
Comparisons of outcomes between studies may be prone to bias due to confounding if not properly adjusted [11]. IPTW using average treatment effect in the treated (ATT) weights derived from propensity scores, was used to emulate hypothetical comparative trials in which patients were randomized to cilta-cel or one of the comparator regimens. Prognostic baseline characteristics for adjustment were identified and ranked in order of importance prior to the present analysis, based on input from independent clinical experts [12,13]. The following five factors were identified as most prognostic and clinically relevant: refractory status, cytogenetic risk [14], International Staging System (ISS), presence of plasmacytomas/extramedullary disease and time to progression in prior line. However, due to the high proportion of patients with unknown cytogenetics in the daratumumab clinical trials (ranging from 25% to 60%), cytogenetic risk could not be included. The remaining four factors constitute the base case adjustment set. A full list of the prognostic factors and their availability is shown in Supplementary Table 2.
Outcomes
Outcomes of interest included overall response rate (ORR), rate of very good partial response or better (≥VGPR), rate of complete response or better (≥CR) and progression-free survival (PFS). ORR was defined as the proportion of patients who achieved partial response (PR) or better (stringent CR [sCR], CR, VGPR, or PR). ≥VGPR was defined as the proportion of patients who achieved a VGPR, CR, or sCR based on International Myeloma Working Group (IMWG) consensus criteria. ≥CR was defined as the proportion of patients who achieved a CR or sCR based on IMWG consensus criteria. PFS was defined as the time from index date to the date of progression or death, whichever occurred first.
Statistical analysis
IPTW with the base case covariates was used to generate adjusted comparisons between the cilta-cel cohort versus DVd, Vd, DKd, Kd and Pd [15]. Propensity scores were estimated using a logistic regression model that predicted assignment in the cilta-cel cohort as a function of key prognostic factors. The estimated propensity scores, p, were used to derive ATT weights, where patients in the comparator arms were assigned a weight of p/(1-p), while patients from the cilta-cel cohort were kept as observed (assigned a weight of one) [15]. Consequently, patients in the comparator arms with more similar baseline characteristics to the cilta-cel cohort received larger weights while less similar patients were down weighted to balance the two groups. To reflect the original sample size, a rescaled version of these weights was used (see details in Appendix B).
Relative efficacy was assessed for both the unadjusted (i.e., cilta-cel versus comparative treatment prior to IPTW) and for the adjusted (i.e., with IPTW) comparisons for all outcomes. For response outcomes (i.e., binary outcomes) (ORR, ≥VGPR and ≥CR), logistic regression and Poisson regression models [16] (with weights applied for the adjusted comparison) were used to estimate odds ratios (ORs) and rate ratios (RRs), respectively. For PFS (i.e., time-to-event outcome), a Cox proportional hazards model (with weights applied for the adjusted comparison) was used to derive hazard ratios (HRs). Corresponding 95% confidence intervals (CIs) were calculated, where the variance was estimated using the robust sandwich variance estimator [17,18]. Appropriateness of the proportional hazards assumption for PFS was assessed based on visual inspection of the log-cumulative hazard plot, visual inspection of the Schoenfeld residuals plot and performance of the Grambsch–Therneau test [19] (with a p-value less than 0.05 considered to indicate a violation of the assumption). In case of violations of the proportional hazards assumption, time-dependent HRs were estimated. Furthermore, the restricted mean survival time (RMST) difference [20], restricted at the minimum of the largest observed event time in each of the two arms, was additionally reported.
Variables with a proportion of missing values less than 25% were imputed using multiple imputation with chained equation. Statistical analyses and graphical visualization were conducted using SAS 9.4 (SAS Institute, NC, USA) and R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).
Sensitivity analyses
Several sensitivity analyses were conducted to assess the robustness of results. The first sensitivity analysis was an IPTW using average treatment effect in the control (ATC) weights, where patients in the cilta-cel cohort were reweighted to reflect each of the comparator cohorts, whereas the comparator cohorts were kept as observed. While the primary ATT-based analyses estimate comparative efficacy in the cilta-cel population, ATC weighting provides comparative estimates in the patient cohort for the comparator. When the sample size of the external cohort is small, ATT weights may become unstable if adding several covariates in the PS model; therefore, ATC weights are a valid alternative [21]. As sample size for some of the comparator cohorts in the current analyses was limited, IPTW-ATC allowed for the adjustment of number of prior lines, years since diagnosis, age and hemoglobin levels, in addition to the covariates included in the base case. Finally, multivariable regression models were used as an alternative option to IPTW to explore the impact of further adding prior transplant, ECOG status, MM type, creatinine clearance, gender and race as covariates.
Results
Adjustments for imbalances between cohorts
The comparative analysis consisted of 155 patients in the cilta-cel cohort of CARTITUDE-4 that had no prior exposure to anti-CD38 therapies, 44 patients treated with DVd, 46 patients treated with Vd, 98 patients treated with DKd, 46 patients treated with Kd, and 92 patients treated with Pd that fulfilled the CARTITUDE-4 eligibility criteria across the CANDOR, CASTOR and APOLLO studies (Figure 1).

Figure 1. Flow chart of patient selection.
DKd: Daratumumab with carfilzomib and dexamethasone; DVd: Daratumumab in combination with bortezomib and dexamethasone; ECOG: Eastern Cooperative Oncology Group; IMiD: Immunomodulatory agent; Kd: Carfilzomib and dexamethasone; LOTs: Lines of therapy; Pd: Pomalidomide plus dexamethasone; PI: Proteasome inhibitor; Vd: Bortezomib and dexamethasone.
Multiple imputation was required for the following missing variables in CANDOR: time to progression on prior line (missing 4.1% for DKd and 4.4% for Kd), years since MM diagnosis (missing 5.1% for DKd and 2.2% for Kd) and hemoglobin (missing 1% for DKd) (Supplementary Table 3). Imputation was not necessary for CARTITUDE-4, CASTOR and APOLLO, as there were no other missing values.
The cilta-cel cohort had a higher proportion of patients with ISS stage I, longer time to progression in prior line and a higher presence of plasmacytomas / extramedullary disease (Table 1). After IPTW, key baseline covariates were well balanced across the cohorts (Supplementary Tables 4–8).
| Variable | Categories | Cilta-cel CARTITUDE-4 | DVd CASTOR | Vd CASTOR | DKd CANDOR | Kd CANDOR | Pd APOLLO |
|---|---|---|---|---|---|---|---|
| n = 155 n (%) | n = 44 n (%) | n = 46 n (%) | n = 98 n (%) | n = 46 n (%) | n = 92 n (%) | ||
| Refractory status | < Double refractory† ≥ Double refractory | 82 (52.9%) 73 (47.1%) | 18 (40.9%) 26 (59.1%) | 22 (47.8%) 24 (52.5%) | 54 (55.1%) 44 (44.9%) | 26 (56.5%) 20 (43.5%) | 45 (48.9%) 47 (51.1%) |
| ISS stage | I II III | 103 (66.5%) 44 (28.4%) 8 (5.2%) | 19 (43.2%) 15 (34.1%) 10 (22.7%) | 19 (41.3%) 19 (41.3%) 8 (17.4%) | 51 (52.0%) 28 (28.6%) 19 (19.4%) | 23 (50.0%) 15 (32.6%) 8 (17.4%) | 41 (44.6%) 33 (35.9%) 18 (19.6%) |
| Time to progression on prior line (months) | <6 ≥6 | 22 (14.2%) 133 (85.8%) | 7 (15.9%) 37 (84.1%) | 11 (23.9%) 35 (76.1%) | 20 (20.4%) 78 (79.6%) | 14 (30.4%) 32 (69.6%) | 19 (20.7%) 73 (79.3%) |
| Presence of plasmacytomas/ extramedullary disease | Yes No | 29 (18.7%) 126 (81.3%) | 1 (2.3%) 43 (97.7%) | 2 (4.3%) 44 (95.7%) | 6 (6.1%) 92 (93.9%) | 3 (6.5%) 43 (93.5%) | 3 (3.3%) 89 (96.7%) |
| Prior LOTs (n) | 1–2 3 | 120 (77.4%) 35 (22.6%) | 24 (54.5%) 20 (45.5%) | 30 (65.2%) 16 (34.8%) | 54 (55.1%) 44 (44.9%) | 26 (56.5%) 20 (43.5%) | 65 (70.7%) 27 (29.3%) |
| Years since MM diagnosis | <4 ≥4 | 101 (65.2%) 54 (34.8%) | 17 (38.6%) 27 (61.4%) | 27 (58.7%) 19 (41.3%) | 55 (56.1%) 43 (43.9%) | 28 (60.9%) 18 (39.1%) | 49 (53.3%) 43 (46.7%) |
| Hemoglobin (g/dl) | <10 10–12 >12 | 40 (25.8%) 55 (35.5%) 60 (38.7%) | 18 (40.9%) 11 (25.0%) 15 (34.1%) | 11 (23.9%) 20 (43.5%) 15 (32.6%) | 25 (25.5%) 40 (40.8%) 33 (33.7%) | 9 (19.6%) 20 (43.5%) 17 (37.0%) | 25 (27.2%) 39 (42.4%) 28 (30.4%) |
| Prior autologous stem cell transplant | Yes No | 129 (83.2%) 26 (16.8%) | 36 (81.8%) 8 (18.2%) | 30 (65.2%) 16 (34.8%) | 60 (61.2%) 38 (38.8%) | 21 (45.7%) 25 (54.3%) | 42 (45.7%) 50 (54.3%) |
| ECOG status | 0 1 | 85 (54.8%) 70 (45.2%) | 21 (47.7%) 23 (52.3%) | 25 (54.3%) 21 (45.7%) | 46 (46.9%) 52 (53.1%) | 23 (50.0%) 23 (50.0%) | 58 (63.0%) 34 (37.0%) |
| Type of MM | IgA IgG Other | 26 (16.8%) 86 (55.5%) 43 (27.7%) | 6 (13.6%) 26 (59.1%) 12 (27.3%) | 12 (26.1%) 25 (54.3%) 9 (19.6%) | 25 (25.5%) 53 (54.1%) 20 (20.4%) | 10 (21.7%) 27 (58.7%) 9 (19.6%) | 20 (21.7%) 52 (56.5%) 20 (21.7%) |
| Creatinine clearance (ml/min) | <60 ≥60 | 20 (12.9%) 135 (87.1%) | 13 (29.5%) 31 (70.5%) | 16 (34.8%) 30 (65.2%) | 16 (16.3%) 82 (83.7%) | 12 (26.1%) 34 (73.9%) | 31 (33.7%) 61 (66.3%) |
| Sex | Male Female | 86 (55.5%) 69 (44.5%) | 21 (47.7%) 23 (52.3%) | 29 (63.0%) 17 (37.0%) | 54 (55.1%) 44 (44.9%) | 29 (63.0%) 17 (37.0%) | 47 (51.1%) 45 (48.9%) |
| Age (years) | <65 ≥65 | 96 (61.9%) 59 (38.1%) | 22 (50.0%) 22 (50.0%) | 25 (54.3%) 21 (45.7%) | 50 (51.0%) 48 (49.0%) | 28 (60.9%) 18 (39.1%) | 37 (40.2%) 55 (59.8%) |
| Race | White Not reported/Other | 115 (74.2%) 40 (25.8%) | 38 (86.4%) 6 (13.6%) | 41 (89.1%) 5 (10.9%) | 75 (76.5%) 23 (23.5%) | 38 (82.6%) 8 (17.4%) | 83 (90.2%) 9 (9.8%) |
†
‘< Double refractory’ category consisted of lenalidomide-refractory only patients.
DKd: Daratumumab with carfilzomib and dexamethasone; DVd: Daratumumab in combination with bortezomib and dexamethasone; ECOG: Eastern Cooperative Oncology Group; IPTW: Inverse probability of treatment weighting; ISS: International Staging System; Kd: Carfilzomib and dexamethasone; LOT: Line of therapy; MM: Multiple myeloma; Pd: Pomalidomide plus dexamethasone; Vd: Bortezomib and dexamethasone.
Comparative efficacy results
The observed ORR was 89.7% in the cilta-cel cohort and ranged from 42.4% to 79.6% among patients treated with comparator regimens (Figure 2). After adjustment, patients in the cilta-cel cohort were 1.2 (vs DKd) to 2.0 (vs Pd) times more likely than patients treated with comparator regimens to achieve ORR (Figure 3). The observed ≥VGPR rates were 85.2% in the cilta-cel cohort and ranged from 14.1% to 64.3% in patients treated with comparator regimens (Figure 2). After adjustment, patients in the cilta-cel cohort were 1.5 (vs DKd) to 5.1 (vs Vd) times more likely to achieve ≥VGPR than patients treated with comparator regimens, and all comparisons were statistically significant (Figure 3). The observed ≥CR rates were 78.1% in the cilta-cel cohort and ranged from 2.2% to 26.5% in patients treated with comparator regimens (Figure 2). After adjustment, patients in the cilta-cel cohort were 2.9 (vs DKd) to 38.8 (vs Pd) times more likely to achieve ≥CR than patients treated with comparator regimens, all results were statistically significant (all p < 0.01) (Figure 3). Cilta-cel also significantly reduced the risk of disease progression or death by 49% (DKd: HR: 0.51 [95% CI: 0.30, 0.88; p = 0.015]) to 89% (Vd: HR: 0.11 [95% CI: 0.07, 0.17; p < 0.0001]). The median PFS for the cilta-cel and DKd arms was not reached whereas the median PFS post-adjustment was 9.79 months for DVd, 6.21 months for Vd, 11.09 months for Kd and 8.34 months for Pd (Figure 4). The assessment of proportional hazards indicated the proportional hazards held for comparisons versus all regimens, except Vd. Nevertheless, the overall HR represents the average HR across the entire treatment period, and remains a meaningful measure of average benefit [22]. Time-dependent hazard ratios showed an increasing benefit over time, with HR beyond 3 months ranging from 0.05 to 0.43 (Supplementary Table 9). Finally, the RMST difference after approximately 18 months ranged from 2.9 months (DKd) to 8.1 months (Vd), indicating that cilta-cel also significantly increased the average PFS time over all comparator treatments (Supplementary Figure 1).

Figure 2. Observed response rates for cilta-cel versus comparative treatment.
≥CR: Complete response or better; DKd: Carfilzomib in combination with daratumumab and dexamethasone; DVd: Daratumumab in combination with bortezomib and dexamethasone; Kd: Carfilzomib and dexamethasone; ORR: Overall response rate; Pd: Pomalidomide in combination with dexamethasone; PR: Partial response; Vd: Bortezomib with dexamethasone; ≥VGPR: Very good partial response.
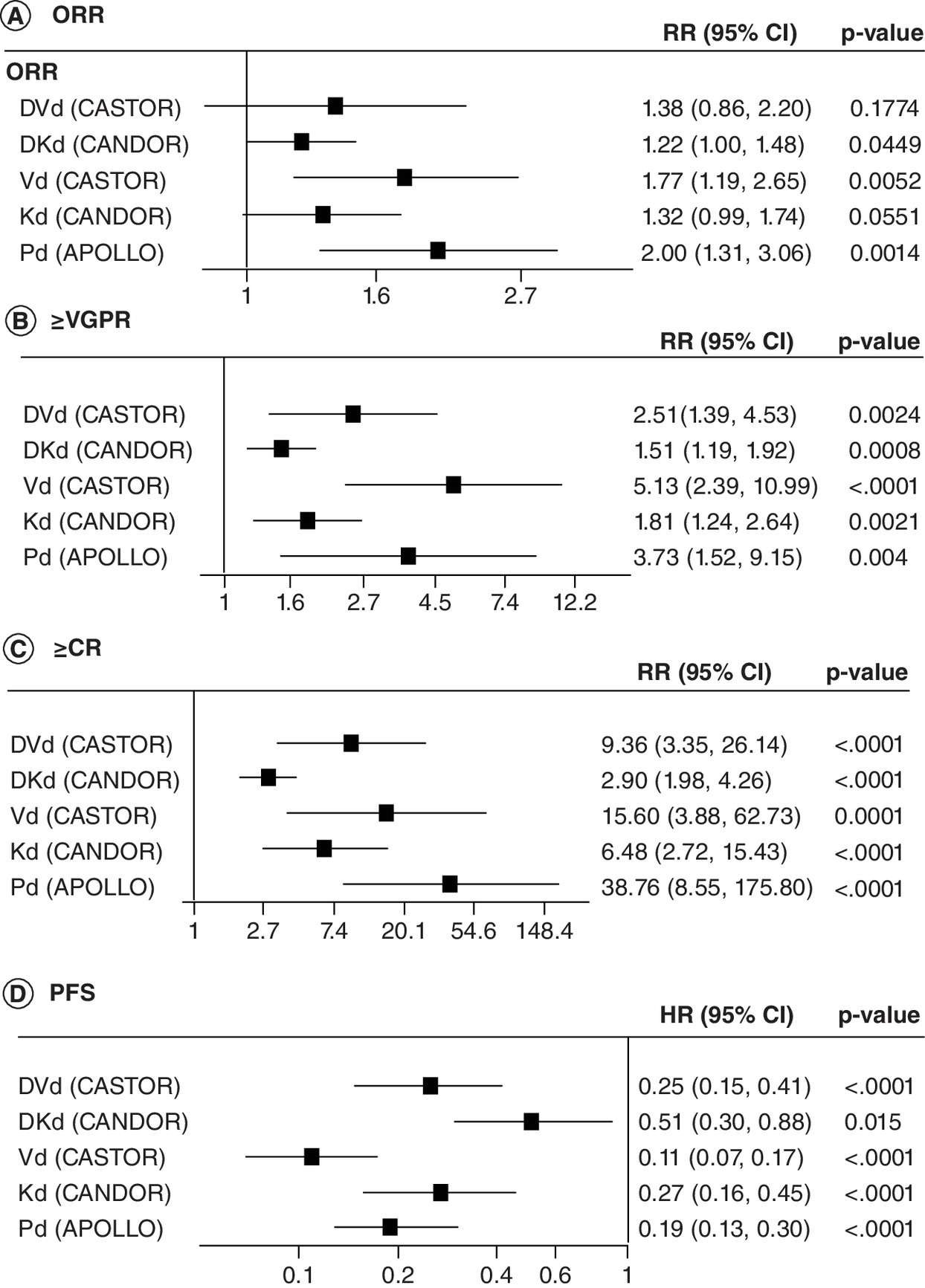
Figure 3. Average treatment effect in the treated-adjusted comparative efficacy of cilta-cel versus comparator treatments on overall response rate, very good partial response or better, complete response or better, and progression-free survival.
Adjusted for refractory status, International Staging System stage, presence of plasmacytomas/extramedullary disease and time to progression on prior lines of therapy. HR less than 1 and RR greater than 1 indicates favorable treatment effect for cilta-cel.
CI: Confidence interval; ≥CR: Complete response or better; DKd: Carfilzomib in combination with daratumumab and dexamethasone; DVd: Daratumumab in combination with bortezomib and dexamethasone; HR: Hazard ratio; Kd: Carfilzomib and dexamethasone, ORR: Overall response rate; Pd: Pomalidomide in combination with dexamethasone; PFS: Progression-free survival; RR: Rate ratio; Vd: Bortezomib with dexamethasone; ≥VGPR: Very good partial response or better.
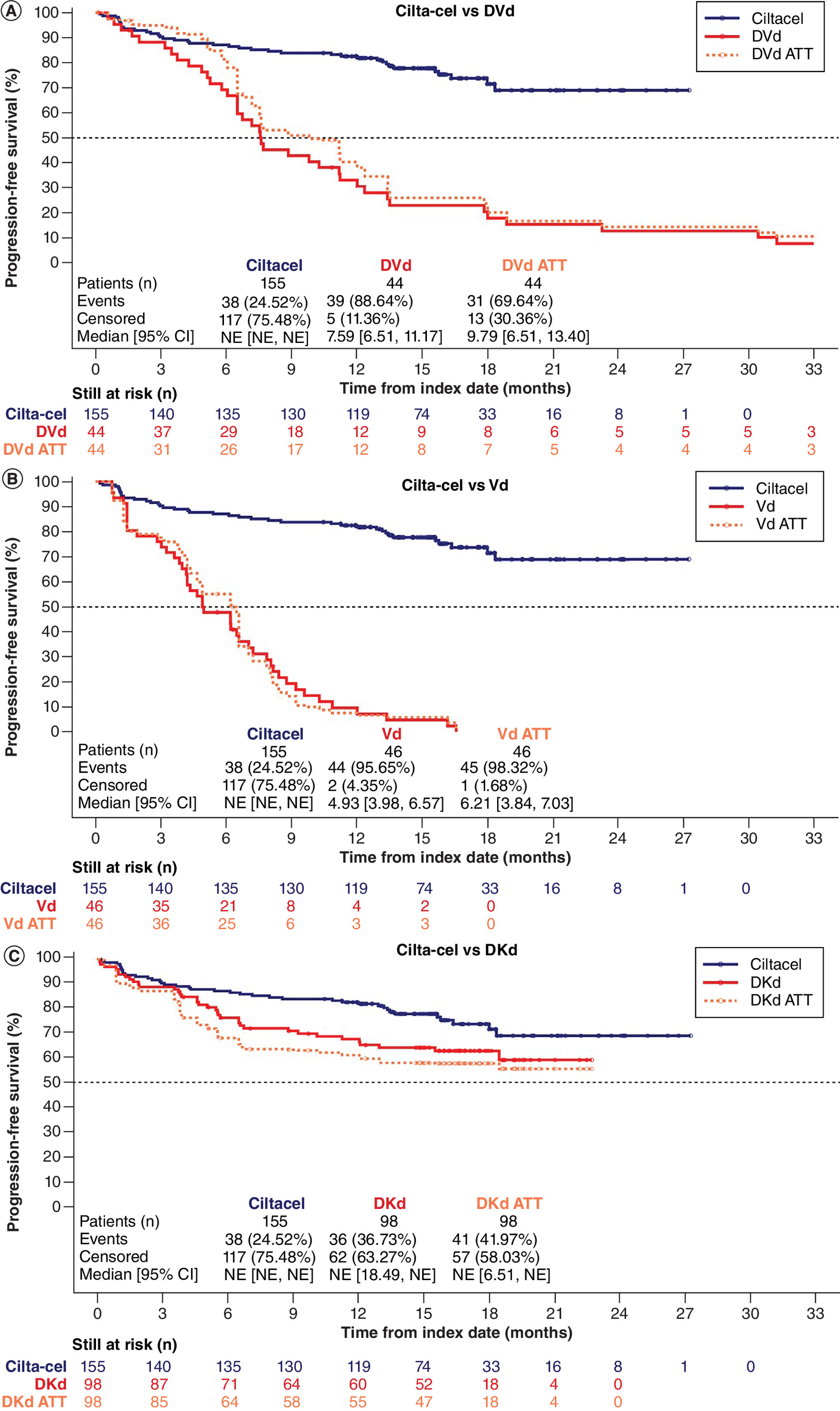
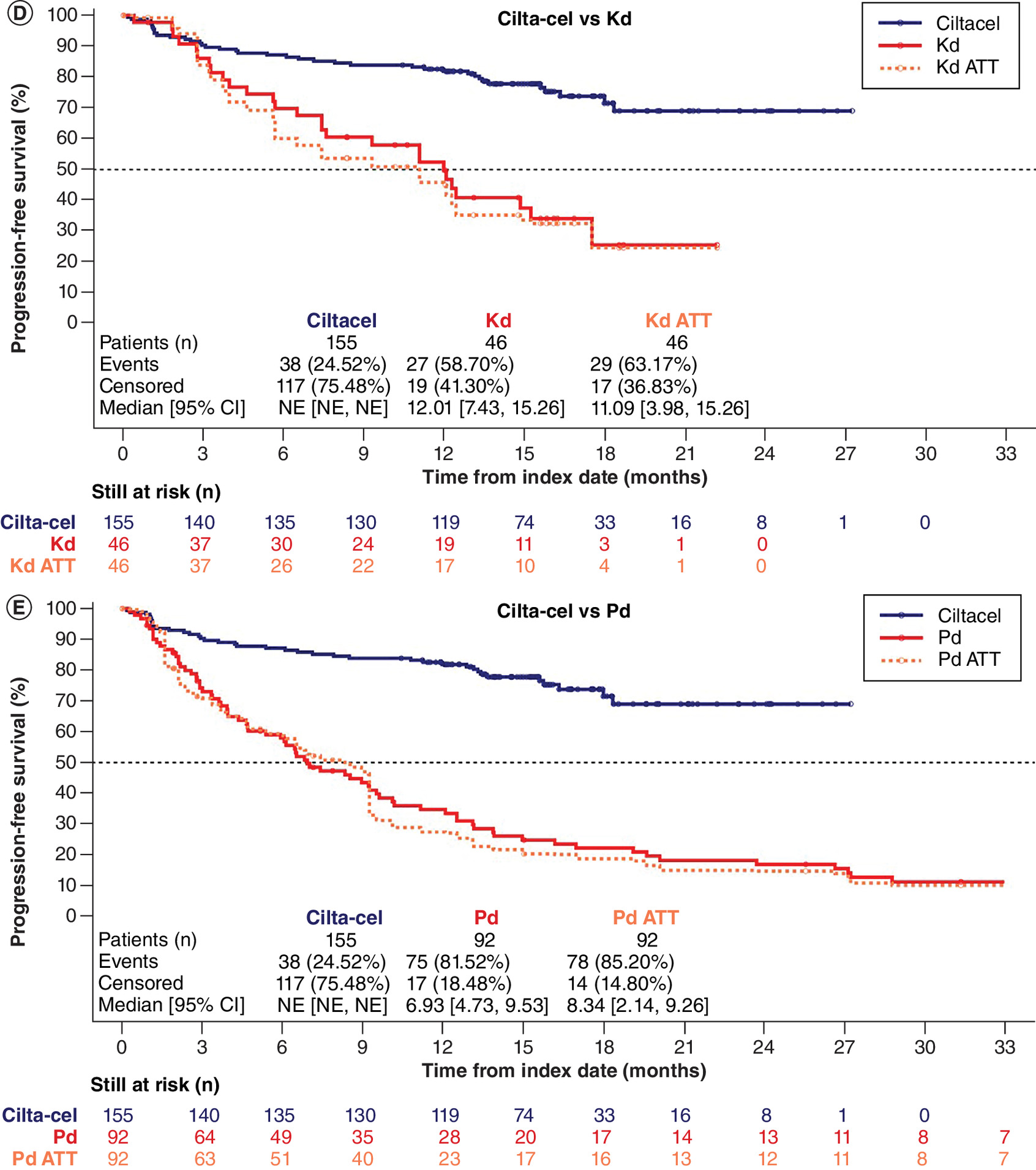
Figure 4. Observed and average treatment effect in the treated-adjusted Kaplan–Meier curves for p rogression-free survival for cilta-cel versus comparator treatments.
Adjusted for refractory status, International Staging System stage, presence of plasmacytomas/extramedullary disease, and time to progression on prior lines of therapy.
ATT: Average treatment effect in the treated; CI: Confidence interval; DKd: Carfilzomib in combination with daratumumab and dexamethasone; DVd: Daratumumab in combination with bortezomib and dexamethasone; Kd: Carfilzomib and dexamethasone; Pd: Pomalidomide in combination with dexamethasone; PFS: Progression-free survival; Vd: Bortezomib with dexamethasone.
Sensitivity analyses
Results from the IPTW-ATC analyses, including base case covariates and an additional four variables, were consistent with the main analysis (IPTW-ATT) with smaller standardized mean differences (Supplementary Tables 4–8), with cilta-cel demonstrating statistically significant improvement over comparator treatments for all outcomes. The multivariable regression models including all 14 available baseline covariates also showed consistency with the main analysis, with cilta-cel demonstrating improvement over comparator treatments for all outcomes (Supplementary Figures 2–5).
Discussion
Despite the availability of a multitude of treatment regimens for RRMM, patients refractory to lenalidomide still frequently progress, require continuous anti-myeloma therapies and the overall prognosis remains poor. Therefore, additional treatment options are needed to promote deep and durable responses, delay progression and maintain or even improve quality of life. Based on our analyses, cilta-cel provides the most effective treatment option compared with other available treatment regimens.
The superiority of cilta-cel over the DPd and PVd treatment regimens was demonstrated in the phase III RCT CARTITUDE-4 among RRMM patients who have received one to three prior LOT(s) that included an IMiD and a PI, and who are refractory to lenalidomide. However, as standard of care options for lenalidomide-refractory RRMM patients can vary across countries and regions of the world and many different drug combinations can be used in RRMM, a comparison of cilta-cel against other conventional treatment options is necessary to determine its potential as a new standard of care. Using IPD from CARTITUDE-4 and three daratumumab clinical trials, the present analyses report adjusted comparisons between cilta-cel and other commonly utilized regimens used in RRMM patients who have received one to three prior LOT(s) that included an IMiD and a PI, and who are refractory to lenalidomide. The availability of patient level data from RCTs for these regimens allowed to include only patients refractory to lenalidomide, who generally have significantly worse outcomes than non-lenalidomide-refractory patients. Additionally, the available data allowed to further adjust for differences on other important risk factors between patient populations across studies, using a range of statistical approaches including IPTW and multivariable regression to estimate relative efficacy in the most robust way, in the absence of direct head-to-head data. Results show the benefits of cilta-cel treatment in response outcomes (ORR, ≥VGPR and ≥CR) and PFS versus all comparators. While treatment with DKd consistently yielded the best outcomes across all comparator regimens, comparative estimates for cilta-cel versus DKd were also statistically significant in favor of cilta-cel across all end points.
As in any comparative analysis of non-randomized cohorts, it is important to acknowledge that the potential for residual confounding cannot be excluded. To address this, clinically important covariates were selected for balancing between groups through an evidence-based process involving a literature review, expert clinical opinion, and previously conducted adjusted comparisons in RRMM patients [12,13]. The IPTW approach using ATT weights was a priori selected as the primary analysis, as it allows for the estimation of the relative treatment effect versus all comparators in the same (cilta-cel) population. However, the small sample size for some of the comparator cohorts limited the adjustment to the four clinically most relevant prognostic variables adjusted for. The IPTW-ATC models were able to account for this by including a wider list of prognostic factors while also achieving a good balance. Furthermore, multivariable regression models were able to account for additional prognostic factors. The consistency of the comparative estimates across all three approaches illustrates the robustness of the results.
While follow-up time in the CARTITUDE-4 trial is shorter compared with other trials (15.9 months for CARTITUDE-4 versus 74.3 months for CASTOR, 16.9 months for CANDOR and 39.9 months for APOLLO), HR estimates are not biased by differences in follow-up lengths as PFS was analyzed using survival analysis and patients still at risk at time of data cut were censored. This form of administrative censoring is non-informative and does not impact the HR estimates. Comparative estimates may rather be conservative for the response outcomes, given that patients may continue to deepen the level of response over time.
It is also worth noting that while excluding CD38-exposed patients from the cilta-cel cohort might allow better comparability across populations, the results could be perceived as less generalizable. On the other hand, the interaction between treatment effect and anti-CD38 exposure within the CARTITUDE-4 trial was not found to be statistically significant, meaning that the relative effect of cilta-cel would be comparable among the anti-CD38-exposed and the anti-CD38-naive patients [7]. As most of the triple-class exposed patients in the CARTITUDE-4 population were in the third- and fourth-LOT, this is comparable to estimates with the patient population from CARTITUDE-1 [23]. Comparative estimates between triple class exposed patients from CARTITUDE-1 versus the LocoMMotion study of real-world clinical practice showed similar treatment benefit, including for OS [23].
Further investigation and comparisons with longer follow-up are needed to assess safety, efficacy, quality of life benefits and comparisons on OS of cilta-cel over additional accepted treatment regimens.
Conclusion
The adjusted comparative efficacy analysis of cilta-cel using patient level data available from daratumumab trials demonstrates significant benefit for cilta-cel on ORR, ≥VGPR, ≥CR and PFS versus DKd, DVd, Pd, Vd and Kd in RRMM patients who have received one to three prior LOT(s) that included an IMiD and a PI, and who are refractory to lenalidomide. These results further complement the comparative evidence versus DPd and PVd from CARTITUDE-4 on the added benefit that cilta-cel can provide in this difficult to treat patient population.
Summary points
•
Despite the introduction of new treatments, multiple myeloma remains incurable and the majority of patients progress to relapsed or refractory multiple myeloma (RRMM).
•
CARVYKTI (ciltacabtagene autoleucel; cilta-cel) is a chimeric antigen receptor T-cell (CAR-T) therapy that has demonstrated superiority over two other commonly accepted non-CAR-T treatment regimens in the CARTITUDE-4 randomized trial, across multiple clinical end points in patients with RRMM, who have received one to three prior line(s) of therapy (LOT(s)) and are refractory to lenalidomide.
•
However, standard of care options for these patients can vary in different regions of the world where the comparators used in the CARTITUDE-4 trial may not be among the currently accepted treatments.
•
In the absence of head-to-head trials between cilta-cel and other standard of care therapies in this population, indirect comparisons can be utilized to estimate the relative effects between these treatment options.
•
Individual patient data for cilta-cel from CARTITUDE-4 and other treatment regimens were available from the CASTOR (daratumumab with bortezomib and dexamethasone [DVd] and bortezomib with dexamethasone [Vd]), CANDOR (daratumumab with carfilzomib and dexamethasone [DKd] and carfilzomib with dexamethasone [Kd]), and APOLLO (pomalidomide in combination with dexamethasone [Pd]) randomized trials.
•
Patients who met the CARTITUDE-4 eligibility criteria were identified from these comparator treatment regimens and imbalances between cohorts on clinically important prognostic factors at baseline were adjusted using inverse probability of treatment weighting (IPTW).
•
Key prognostic factors were well balanced across the cohorts after IPTW adjustment.
•
Patients randomized to the cilta-cel cohort showed statistically significant improvements over most comparator regimens with respect to overall response rate, and over all comparator regimens in rate of very good partial response or better, rate of complete response or better and progression-free survival.
•
Cilta-cel demonstrated benefit over other treatment regimens commonly used in clinical practice, highlighting its potential as a new standard of care option for patients with RRMM refractory to lenalidomide, who have received one to three prior LOT(s).
Author contributions
All authors were responsible for the study conception and design. J Diels and F Ghilotti were responsible for acquisition and analysis. All authors were responsible for interpretation of the data and revising it critically.
Acknowledgments
The authors thank IA Samjoo, A Haltner, K Tantakoun and J Esguerra for revising the manuscript critically. All were employed by EVERSANA, Canada and USA.
Financial disclosure
This work was supported by Janssen Pharmaceuticals and Legend Biotech. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
The authors have no financial and/or nonfinancial competing interests or relevant affiliations with any organization/entity to declare that are relevant to the subject matter or materials discussed in this manuscript. This includes employment, grants or research funding, consultancies, membership on scientific or other advisory boards, honoraria, stock ownership or options, paid expert testimony, patents received or pending, or royalties.
Writing disclosure
Medical writing and editorial support were provided by EVERSANA and Eloquent Scientific Solutions, and were funded by Janssen.
Ethical conduct of research
The CARTITUDE-4 trial protocol was reviewed and approved by an independent ethics committee/institutional review board at all participating sites. All patients participating in the trial provided written informed consent. Similarly, the protocols of the clinical trials of daratumumab were approved by local or independent institutional review board or ethics committees at participating sites and all patients provided written informed consent. The current analyses were conducted in accordance with a protocol and statistical analysis plan developed prior to the start of data analysis.
Data sharing statement
Requests for access to the CARTITUDE-4 trial study data may be submitted through the Yale Open Data Access (YODA) Project site at http://yoda.yale.edu. The data sharing policy of Janssen Pharmaceutical Companies is available at https://www.janssen.com/clinical-trials/transparency.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 5.74 MB
References
1.
Chung C. Role of immunotherapy in targeting the bone marrow microenvironment in multiple myeloma: an evolving therapeutic strategy. Pharmacotherapy 37(1), 129–143 (2017).
2.
Orlowski RZ. Why proteasome inhibitors cannot ERADicate multiple myeloma. Cancer Cell 24(3), 275–277 (2013).
3.
Anderson KC, Kyle RA, Rajkumar SV, Stewart AK, Weber D, Richardson P. Clinically relevant end points and new drug approvals for myeloma. Leukemia 22(2), 231–239 (2008).
4.
Yang Y, Li Y, Gu H, Dong M, Cai Z. Emerging agents and regimens for multiple myeloma. J. Hematol. Oncol. 13(1), 150 (2020).
5.
Botta C, Martino EA, Conticello C et al. Treatment of lenalidomide exposed or refractory multiple myeloma: network meta-analysis of lenalidomide-sparing regimens. Front. Oncol. 11, 643490 (2021).
6.
Lecat CSY, Taube JB, Wilson W et al. Defining unmet need following lenalidomide refractoriness: real-world evidence of outcomes in patients with multiple myeloma. Front. Oncol. 11, 703233 (2021).
7.
San-Miguel J, Dhakal B, Yong K et al. Cilta-cel or standard care in lenalidomide-refractory multiple myeloma. N. Engl. J. Med. 389(4), 335–347 (2023).
8.
Palumbo A, Chanan-Khan A, Weisel K et al. Daratumumab, bortezomib, and dexamethasone for multiple myeloma. N. Engl. J. Med. 375(8), 754–766 (2016).
9.
Usmani SZ, Quach H, Mateos M-V et al. Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): updated outcomes from a randomised, multicentre, open-label, phase III study. Lancet Oncol. 23(1), 65–76 (2022).
10.
Dimopoulos MA, Terpos E, Boccadoro M et al. Daratumumab plus pomalidomide and dexamethasone versus pomalidomide and dexamethasone alone in previously treated multiple myeloma (APOLLO): an open-label, randomised, phase III trial. Lancet Oncol. 22(6), 801–812 (2021).
11.
Dahlberg S, Liu PY. Prognostic factors in clinical trials. Breast Cancer Res. Treat. 22(3), 193–196 (1992).
12.
Martin T, Krishnan A, Yong K et al. Comparative effectiveness of ciltacabtagene autoleucel in CARTITUDE-1 versus physician's choice of therapy in the Flatiron Health multiple myeloma cohort registry for the treatment of patients with relapsed or refractory multiple myeloma. EJHaem. 3(1), 97–108 (2022).
13.
Weisel K, Martin T, Krishnan A et al. Comparative efficacy of ciltacabtagene autoleucel in CARTITUDE-1 vs physician's choice of therapy in the long-term follow-up of POLLUX, CASTOR, and EQUULEUS Clinical trials for the treatment of patients with relapsed or refractory multiple myeloma. Clin. Drug Investig. 42(1), 29–41 (2022).
14.
Sonneveld P, Avet-Loiseau H, Lonial S et al. Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group. Blood 127(24), 2955–2962 (2016).
15.
Li F, Morgan KL, Zaslavsky AM. Balancing covariates via propensity score weighting. J. Am. Stat. Assoc. 113(521), 390–400 (2018).
16.
Zou G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 159(7), 702–706 (2004).
17.
Chesnaye NC, Stel VS, Tripepi G et al. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 15(1), 14–20 (2022).
18.
Hernán MA, Robins JM. Using big data to emulate a target trial when a randomized trial is not available. Am. J. Epidemiol. 183(8), 758–764 (2016).
19.
Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 81(3), 515–526 (1994).
20.
Royston P, Parmar MK. Restricted mean survival time: an alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med. Res. Methodol. 13, 152 (2013).
21.
Dong N, Kelcey B, Spybrook J. Identifying and estimating causal moderation for treated and targeted subgroups. Multivariate Behav. Res. 58(2), 221–240 (2023).
22.
Mukhopadhyay P, Huang W, Metcalfe P, Ohrn F, Jenner M, Stone A. Statistical and practical considerations in designing of immuno-oncology trials. J. Biopharm. Stat. 30(6), 1130–1146 (2020).
23.
Mateos MV, Weisel K, Martin T et al. Adjusted comparison of outcomes between patients from CARTITUDE-1 versus multiple myeloma patients with prior exposure to proteasome inhibitors, immunomodulatory drugs and anti-CD38 antibody from the prospective, multinational LocoMMotion study of real-world clinical practice. Haematologica 108(8), 2192–2204 (2023).
Information & Authors
Information
Published In
Copyright
© 2024 Janssen Pharmaceuticals. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 9 May 2024
Accepted: 16 July 2024
Published online: 20 August 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Efficacy of CARVYKTI in CARTITUDE-4 versus other conventional treatment regimens for lenalidomide-refractory multiple myeloma using inverse probability of treatment weighting. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0080
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ainsley Ryan Yan Bin Lee, Hon Jen Wong, Chi Ching Lim, Sanjay De Mel, Melissa Ooi, Wee Joo Chng, Yu Yang Soon, Cinnie Yentia Soekojo, Monospecific and Bispecific Chimeric Antigen Receptor (CAR) T-cell Therapy in Multiple Myeloma: A Systematic Review, Meta-analysis and Meta-regression, Transplantation and Cellular Therapy, 10.1016/j.jtct.2026.06.001, (2026).
- Lotte Delemarre, Isabelle Huys, Walter Van Dyck, Steven Simoens, Addressing clinical uncertainties in ATMP reimbursement: a review of methodological guidelines and European practice, Frontiers in Pharmacology, 10.3389/fphar.2026.1749386, 17, (2026).
- Doris K. Hansen, Xiaoxiao Lu, Omar Castaneda Puglianini, Eileen Zhang, Saad Z. Usmani, Rameet Sachdev, Matthew Perciavalle, Denise De Wiest, Stephen Huo, Seina Lee, Zaina P. Qureshi, Sundar Jagannath, Comparative cost per responder analysis of ciltacabtagene autoleucel and real-world standard of care therapy in patients with lenalidomide-refractory multiple myeloma, Expert Review of Pharmacoeconomics & Outcomes Research, 10.1080/14737167.2026.2634771, 26, 3, (369-378), (2026).
- David Kegyes, Bogdan Borlea, Marc Damian, Adrian Bogdan Tigu, Madalina Nistor, Diana Cenariu, Raluca Munteanu, Diana Gulei, Angela Dascalescu, Ion Antohe, Alina Tanase, Evangelos Terpos, Hermann Einsele, Ciprian Tomuleasa, Adoptive cellular therapies in multiple myeloma, Best Practice & Research Clinical Haematology, 10.1016/j.beha.2025.101638, 38, 3, (101638), (2025).
- Rafael Fonseca, Joris Diels, Francesca Ghilotti, João Mendes, Sandra Van Hoorenbeeck, Seina Lee, Jordan M. Schecter, Nikoletta Lendvai, Nitin Patel, Ana Triguero, Winfried Alsdorf, Niels W. C. J. van de Donk, Margherita Ursi, Survival Outcomes with Cilta-cel Versus Conventional Treatment Regimens for Patients with Lenalidomide-Refractory Multiple Myeloma Using Inverse Probability of Treatment Weighting, Advances in Therapy, 10.1007/s12325-025-03278-5, 42, 9, (4418-4431), (2025).
- Noemi Puig, Joris Diels, Suzy van Sanden, João Mendes, Heather Burnett, Allie Cichewicz, Seina Lee, Teresa Hernando, Jordan M. Schecter, Nikoletta Lendvai, Nitin Patel, José María Sanchez-Pina, Serena Rocchi, Roberto Mina, Paolo Corradini, Michele Cavo, Jesús San Miguel, Leyla Shune, Abdullah M. Khan, Surbhi Sidana, Xavier Leleu, Salomon Manier, Brea Lipe, Katja Weisel, Joaquin Martinez-Lopez, Comparative Efficacy of Ciltacabtagene Autoleucel Versus Standard-of-Care Treatments for Patients with Previously Treated Relapsed or Refractory Multiple Myeloma: A Matching-Adjusted Indirect Comparison, Advances in Therapy, 10.1007/s12325-025-03205-8, 42, 7, (3223-3239), (2025).
- Marya Radhi, Dalal A Yusuf, Ghufran M AlSaffar, Zainab A Toorani, Role of Chimeric Antigen Receptor T-Cells in the Evolving Therapeutic Landscape of Multiple Myeloma: A Literature Review, Cureus, 10.7759/cureus.80068, (2025).
- Sandeep Singh, Vivek Uttam, Shafiul Haque, Hardeep Singh Tuli, Pallavi Mishra, Aklank Jain, Comprehensive review on outcomes from Phase 3 clinical trials of drugs in multiple myeloma, Cancer Treatment and Research Communications, 10.1016/j.ctarc.2025.101041, 45, (101041), (2025).