A review of 25 years of National Institute of Health and Care Excellence decision making
Publication: Journal of Comparative Effectiveness Research
Many high-income countries use health technology assessment (HTA) to perform a value assessment of new medicines [1]. Patients may have limited or no access to therapies that receive unfavorable assessments from HTA bodies [2]. As there are currently considerations in the USA [3] and other countries around implementing a HTA process, it is relevant to consider the impact that HTA agency decisions have made on patient access to medicines. As such, we investigated the decisions made by the English HTA agency, the National Institute for Health and Care Excellence (NICE) since its founding in 1999 [4].
All medicines appraised by NICE from its inception to 12 February 2024 were reviewed. Replaced or withdrawn appraisals were excluded. NICE's decisions were classified into six groups: recommended, optimized recommendation (meaning a restriction in patients who can access the treatment as compared with the regulatory label), entry into cancer drugs fund (CDF; recommended or optimized), entry into innovative medicines fund (IMF; recommended or optimized), not recommended (including only in research recommendations) and unable to make a recommendation due to non-submission. Percentages for each group over 4-year intervals were calculated. Medicines not recommended by NICE were checked to see if they went through a HTA process in Canada and Germany. Germany's HTA system was implemented through the Pharmaceutical Market Restructuring Act (AMNOG) in 2011. For decisions made after 2011, any major, considerable, minor or non-quantifiable added benefit rating was classified as a positive recommendation. NICE appraised 885 pharmaceuticals over the study period (Figure 1). The most common disease areas appraised were oncology (32%), blood and immune system conditions (20%) and musculoskeletal conditions (10%). Out of all appraisals, 42% were recommended, 31% received an optimized recommendation, 3% were entered into the CDF, 0.2% were entered into the IMF, 11% were not recommended and 12% were not submitted for appraisal by the manufacturer. The proportion of positive recommendations decreased over time from 95% to 28% from the initial 4-year period (from 2000/01 to 2003/04) compared with the most recent 4-year period (from 2020/21 to 2023/24). The percentages for optimized recommendations and non-submitted appraisals conversely increased from 5 to 39% and from 0 to 20%, respectively, for the same time periods. Of the 107 non-submitted appraisals, 18% were for combination therapies and 33% for monoclonal antibody monotherapies. Of all the drugs not recommended by NICE (94), 31% received favorable recommendations by Canada's HTA body. Forty-three not-recommended medications were authorized by the European Medicines Agency after 2011, of these, 56% were assessed to have additional benefit in Germany.
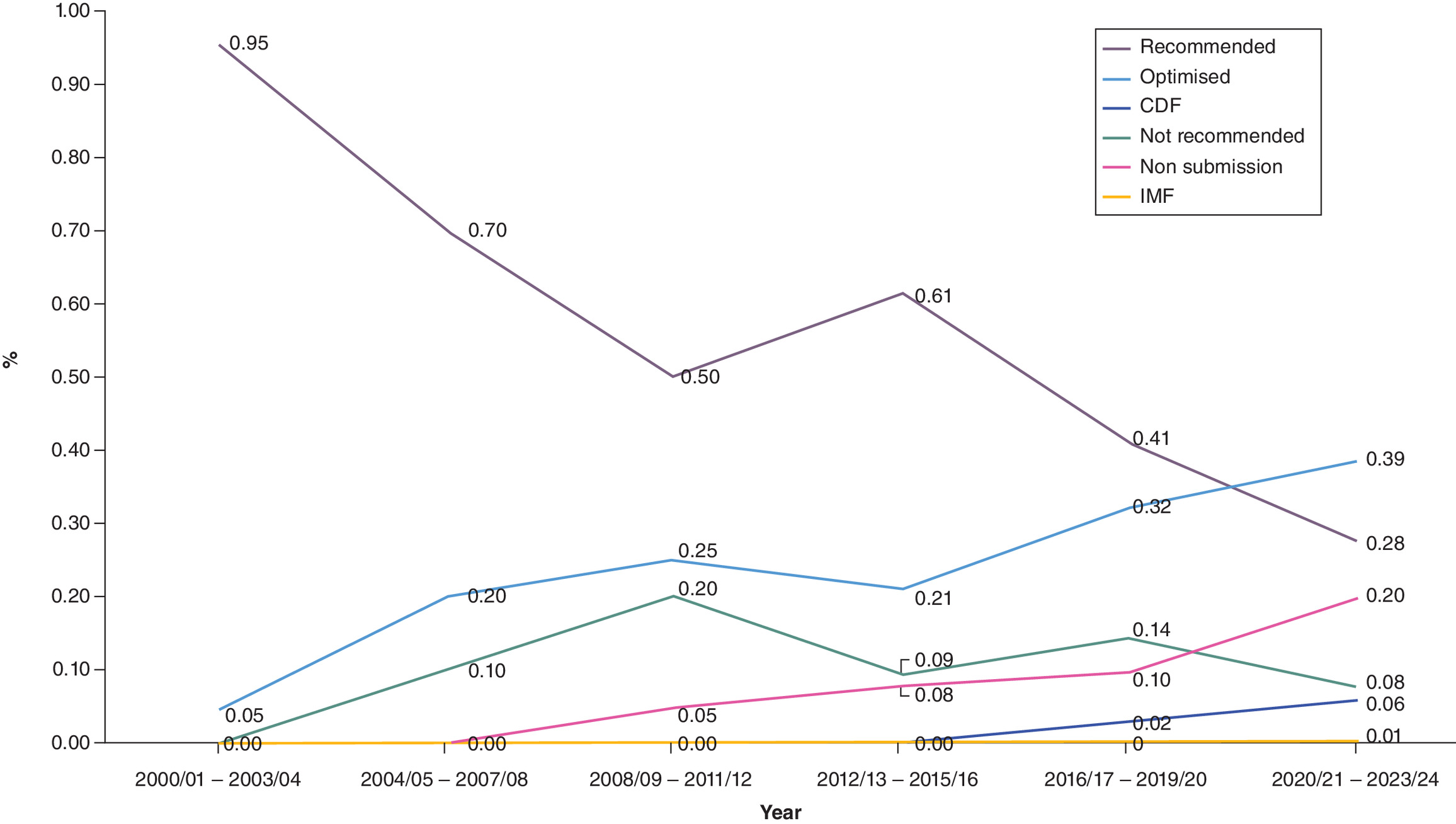
Figure 1. NICE decisions made on medicines over time.
CDF: Cancer drugs fund; IMF: Innovative medicines fund.
Since its inception, the majority of appraisals by NICE have led to a limitation in patient access, either through an optimized recommendation, a rejection or the manufacturer has chosen not to submit for appraisal. For medicines not recommended by NICE, nearly one third were positively appraised in Canada and a higher proportion in Germany where comparable data were available, highlighting disparities in global HTA decision making and patient medicine access. Despite potentially not being valued in one country, a medicine maybe valued in another. In recent years, the proportion of optimized recommendations and manufacturers not submitting for appraisal have increased. A recent study has shown that an optimized recommendation by NICE may allow less than half of patients eligible for the medicine according to the regulatory label obtain access [2]. The increase in non-submissions may be related to the difficulties in demonstrating value of combination therapies using current methods of assessment [5], as well as the fact that the ability to offer indication-based pricing is limited [6] and therefore manufacturers believe that their efforts in developing new treatments will not be adequately rewarded. Limitations of the work include not directly assessing the access impact of optimized recommendations and inability to identify true reasons for manufacturer non-submissions. While HTA can help to control healthcare spending, as well as provide guidance on appropriate use of healthcare technologies, our results nevertheless highlight the substantial impact on patient access to medicines by implementing HTA.
Financial disclosure
The authors have no financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
Jenei K, Raymakers AJN, Bayle A et al. Health technology assessment for cancer medicines across the G7 countries and Oceania: an international, cross-sectional study. Lancet Oncol. 24(6), 624–635 (2023).
2.
OHE. NICE ‘optimized’ Decisions: What is the Recommended Level of Patient Access? (2020). https://www.ohe.org/publications/nice-optimized-decisions-what-recommended-level-patient-access/
3.
Neumann PJ, Tunis SR. Turning CMS into a health technology assessment organization. N. Engl. J. Med. 389(8), 682–684 (2023).
4.
NICE. The National Institute for Health and Care Excellence. https://www.nice.org.uk/ (2024).
5.
Latimer NR, Pollard D, Towse A et al. Challenges in valuing and paying for combination regimens in oncology: reporting the perspectives of a multi-stakeholder, international workshop. BMC Health Serv. Res. 21(1), 412 (2021).
6.
Preckler V, Espín J. The role of indication-based pricing in future pricing and reimbursement policies: a systematic review. Value Health 25(4), 666–675 (2022).
Information & Authors
Information
Published In
Copyright
© 2024 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 April 2024
Accepted: 28 June 2024
Published online: 16 July 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
A review of 25 years of National Institute of Health and Care Excellence decision making. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0063
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sreeram V Ramagopalan, Annie Jullien Pannelay, Access in all areas? A round-up of developments in market access and health technology assessment: part 13, Journal of Comparative Effectiveness Research, 10.57264/cer-2026-0041, 15, 4, (2026).