The impact of a patient advisory board on a clinical comparative effectiveness trial: a comparison of patient and researcher perspectives
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To examine contributions of a patient advisory board (PAB) to the design and conduct of The Pulmonary Embolism Prevention after Hip and Knee Replacement (PEPPER) Trial (NCT02810704) and compare perceptions of PAB members and researchers on the Trial. Materials & methods This evaluation of the PAB was conducted by Clinical Coordinating Center (CCC) members who first discussed PAB contributions, leading to the design of a semi-structured WebEx interview individually querying PAB members on their experience. Two study team members analyzed transcriptions of the interviews for common themes, which were discussed and affirmed at an in-person meeting with PAB members. Results: The contribution most frequently cited as meaningful by PAB members was the creation of a recruitment video. In contrast, the research team considered the most impactful PAB recommendation to be omission of pneumatic compression boots as a study variable. PAB members spoke highly of their involvement in the trial and emphasized shared decision-making in the patient–physician relationship. Conclusion: Researchers and PAB members had different opinions about which PAB contributions were most impactful to the study. This likely derives from differences in perspective; PAB members focused on patient experience and the patient–surgeon relationship while researchers focused primarily on trial outcomes. PAB contributions led to two major protocol changes that had a substantial positive effect on trial design, recruitment and enrollment. This evaluation adds to the engagement literature, which contains little on what patients think of their involvement in the design and conduct of clinical research studies and will aid in encouraging treatment preference discussions between patient and surgeon, thereby supporting the goal of improved patient outcomes.
Plain language summary
What is this article about?
This article details the contributions of a patient advisory board (PAB) to a clinical trial. Perspectives of both PAB members and the research team were sought in order to compare and contrast opinions on the value of contributions.
What were the results?
The perceived value of patient advisory board and researcher contributions to clinical trial design and operations differed; the patient advisory board emphasized patient-centered trial design and shared decision-making while researchers valued benefits to data quality and study outcomes.
What do the results mean?
Patient advisory boards bring value and a diversity of perspective to clinical trials design and operations, ultimately improving trial design, patient enrollment, protocol adherence, data quality and enhancing patient-centered outcomes.
Introduction & background
Patient engagement in the design and conduct of clinical effectiveness trials is increasingly common [1], and arguably essential when comparing elective and discretionary surgical procedures. Patient advisory boards (PAB) help to ensure that study outcomes are of importance to patients, refine research questions, recruitment and retention materials and influence study design [2–4] often resulting in outcomes more meaningful to patients [2,5,6].
The Patient Centered Outcomes Research Institute (PCORI) publishes the Engagement Rubric, which requires grantees to engage patient stakeholders, regularly report engagement strategies and tactics [7,8] and value patient contributions to research, as evidenced by a requirement to provide patient compensation on par with research professionals on the same boards [1]. A PAB, working alongside researchers as co-investigators, can provide important insights as the voice of the patient. However, evaluation of patient engagement in clinical trials to date [9–11] has focused primarily on researchers' viewpoint and reveals little about the value and impact of patient engagement on a clinical trial from the patient perspective [3,12–14].
The Pulmonary Embolism Prevention after Hip and Knee Replacement (PEPPER) Trial: Balancing Safety and Effectiveness (NCT02810704) is a large randomized pragmatic comparative effectiveness trial funded by PCORI which includes a PAB. It seeks to clarify which of three commonly prescribed anticoagulants provides the best balance of preventing venous thromboembolism (VTE) and minimizing risk of untoward bleeding following total hip or knee arthroplasty (TJA), with concurrent analysis of patient reported outcomes (PROs) of overall well-being and joint specific function [15]. It also seeks to evaluate how patients individually value this tradeoff of benefits and risks via a preferences survey given to a subset of patients at one clinical site. In the event that no drug is shown to be superior, the use of shared decision making (SDM) to inform this choice takes on even greater importance.
The PAB has been integral to the PEPPER trial since its inception in 2016. We herein describe the PAB's contribution to the conception, design and operationalization of the trial, and explore the impact of the diverse perspectives of patients and clinical researchers on outcomes of a clinical trial that must reconcile differences in patient risk tolerances with surgeon treatment preferences.
Materials & methods
Formation of the PAB
Potential members were initially identified from a pool of over 6000 patients from the clinical practice of the PI who underwent prior THA or TKA between 1995 and 2015 at either Penn State Hershey Medical Center, the University of Maryland, or the Medical University of South Carolina. Priority consideration was given to patients who had expressed interest in perioperative anticoagulation choices after their joint replacement surgery and had declared a willingness to make the necessary time commitment to attend meetings and be meaningfully engaged in the project. Invitations were ultimately extended to 14 patients to confirm 10 interested participants; each individual was consulted to ascertain interest and willingness to participate, attend meetings and contribute to the design, conduct and analysis of the PEPPER trial. Patients were ultimately selected to create a geographically and socioeconomically diverse group that was representative of the general population undergoing total hip or knee replacement as well as the relative frequent of each procedure performed. Consigned members were schooled in the clinical problem of VTE after joint replacement and the existing controversy surrounding prophylaxis. They are expected to attend two meetings/year (with paid travel and lodging) and receive an honorarium for their time and service equal to that of PEPPER physician stakeholders. Due to the COVID-19 pandemic, virtual meetings were instituted in 2020. In person meetings resumed fall of 2022.
The PAB includes six women and four men representative of the age, sex and race distribution of the patient population receiving hip and knee replacement surgery; 6 patients (3 women, 3 men) had undergone TKA and 4 (3 women, 1 man) had undergone THA (Table 1) [16]. While many are retired, pre-retirement careers are occupationally diverse and include an engineer, compliance officer, cardiac nurse, non-profit administrator, bank branch manager, community hospital patient ambassador, two physicians (including one orthopaedic surgeon), a medical ethics professor and a sales manager in the automotive industry. Of these ten individuals, four had terminal degrees (MD or PhD), three had college degrees (Bachelors or Masters) and three completed a high school education. One male PAB member died and another male patient was recruited in 2019. All PAB members received at least one hip or knee replacement surgery and several experienced adverse events including PE and/or bleeding complications.
| Patient characteristic | PEPPER PAB (n = 10) | AJRR† (n = 860,080) |
|---|---|---|
| Age (median) | 69.5 | 67 |
| Sex‡ (%) | ||
| Male | 4 (40) | 352,633 (41) |
| Female | 6 (60) | 507,447 (59) |
| Race‡ (%) | ||
| White | 9 (90) | 557,322 (92) |
| African–American | 1 (10) | 36,694 (6) |
| Other | 0 | 12,055 (2) |
†
Patients receiving primary total hip or knee arthroplasty, revision and resurfacing.
‡
AJRR percentages have been recalculated to omit those that did not report sex/race.
AJRR: American Joint Replacement Registry; PAB: Patient advisory board; PEPPER: The Pulmonary Embolism Prevention after Hip and Knee Replacement Trial.
Cost of the PAB
As a part of our overall evaluation of the value of the PAB a simple cost analysis was performed. Because costs varied due to the effect of COVID (online rather than in-person meetings) we explored the average cost/year of the PAB in comparison to the overall cost of the trial.
Research team impressions of PAB impact
Semi-annual PAB meeting notes since July 2016 and PCORI engagement reports detailing methods and topics of engagement were reviewed to itemize and chronicle PAB contributions to the PEPPER trial. Research team perspectives pursuant to the PAB contributions were solicited during a series of Clinical Coordinating team meetings during September 2022 and informed the interview script used in key interviews with PAB members. (Figure 1) Having worked with the PAB since its formation, the Clinical Coordinating team, consisting of the Principal Investigator (PI, VDP), Project Director (CAL), IRB Specialist (MBP), Clinical Site Liaison (LMK), Program Assistant and a Clinical Research Coordinator, identified PAB suggestions felt to be impactful and discussed PAB successes, challenges and possible solutions.
Figure 1. Timeline of patient advisory board evaluation activities.
PAB: Patient advisory board; PCORI: The Patient Centered Outcomes Research Institute.
PAB member interviews
In October 2022, the newest research team member (LMK), who had minimal prior contact with the PAB and several years of qualitative interview experience, conducted key informant interviews. Interviews solicited perspectives regarding PAB impact on trial operationalization, value of participation and patient engagement. All PAB members interviewed received an email describing the intent of the interview and verbally consented to have the content of their interview used for this evaluation. A semi-structured interview guide was followed to ensure content consistency. (Figure 2) The 30 to 45-min interviews were recorded and transcribed by WebEx [17] with 8 PAB members. Due to health reasons, one member participated in an abbreviated ten-min interview and another was unavailable. The abbreviated interview focused primarily on PAB impact on the study, the process of contributing and the personal impact of participation.
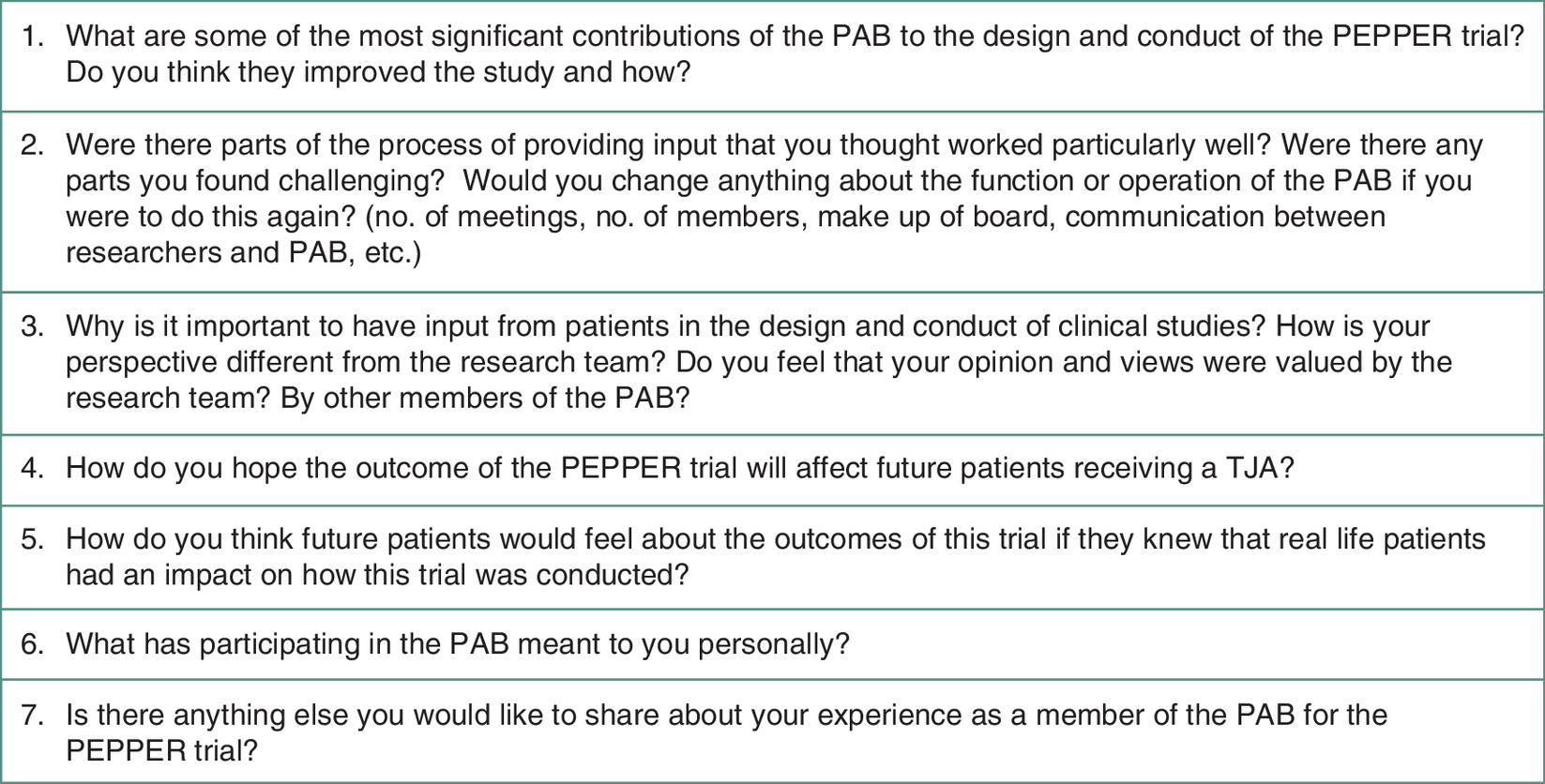
Figure 2. Patient advisory board interview guide.
PAB: Patient advisory board; PEPPER: The Pulmonary Embolism Prevention after Hip and Knee Replacement Trial.
Two team members (LMK, MBP) analyzed each interview transcript using a rapid framework analysis method [18–20], checked against source audio when unclear, and summarized findings in a Microsoft Word document. Summary results were organized into a matrix using Microsoft Excel and checked for accuracy. Common interview themes were identified, extracted and presented to PAB members for validation and discussion during a November 2022 in-person meeting.
Results
Most PAB contributions gleaned from meeting notes and PCORI reports fell into three categories: participant recruitment, participant retention and adherence to study protocol. Other contributions addressed study design, patient comprehension and patient preference data collection, data quality and the impact of COVID-19 on VTE risk. (Table 2).
| Contribution | Description | Times mentioned in PAB interviews (n) | Theorized impact | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study design | Increase protocol adherence | Increase patient recruitment | Increase patient retention | Increase patient comprehension | Data quality | Impact of COVID-19 on VTE risk | |||
| Recruitment video | Patient facing video explaining the purpose, process and goals of PEPPER | 4 | ✓ | ✓ | |||||
| “Delaying” preferences sub-study consenting | Delay recruitment into the preferences sub-study until after surgery | 3 | ✓ | ✓ | |||||
| No inclusion of pneumatic compression boots | Remove compression boots from the protocol, reducing arms in the study | 2 | ✓ | ✓ | ✓ | ||||
| Addition of COVID-19 vaccine questions to data collection | Addition of 3 questions to the patient survey regarding vaccination status | 2 | ✓ | ||||||
| Communication preferences for follow-up surveys | Asking patients how they would like to be contacted for surveys (mail, phone, email) in order to reduce the number of contacts | 2 | ✓ | ||||||
| Participation business card | Business card for patients to provide to PCP/specialist with study website and patient medication. Designed to reduce occurrence of physicians changing patient medication | 2 | ✓ | ||||||
| PCP/specialist explanatory letter | Letter for patients to provide to PCP/specialist describing PEPPER. Designed to reduce the occurrence of physicians changing patient medication | 2 | ✓ | ||||||
| Refrigerator magnet | Magnet with relevant study information to remind patients of their participation and goals of the study | 1 | ✓ | ||||||
| Development of preferences trade off instrument for patient preferences survey | Provide guidance in development of a tool which would demonstrate to patients the trade off in risks between blood clots and bleeding | 0 | ✓ | ✓ | |||||
PAB: Patient advisory board; PEPPER: The Pulmonary Embolism Prevention after Hip and Knee Replacement Trial.
Cost of the PAB
The average annual cost to run the PAB inclusive of all expenses (honoraria, travel and meeting expenses) was approximately $37,000 for a total of nearly $400,000 over the span of the 10-year trial. This represents 2.4% of the $17 million budget of the PEPPER Trial.
PAB impressions
Value of the patient perspective
PAB members uniformly emphasized how their perspectives differed from surgeons and researchers. One expressed that surgeons have ‘tunnel vision’, and that the process of including patient experience brought more empathy to planning a large study. They conveyed that meaningful conversation explaining the study fostered shared decision-making and effective patient–surgeon communication.
“The clinical view is a little bit different than the personal experience view. And I think that having that personal experience from patients who have actually gone through it perhaps brings a little more empathy and I think that that's the way that we can contribute.” – PAB Member #1
One member suggested more intentional introductions to PAB member expectations, noting it was initially unclear whether they were asked to participate because of their professional background or because they were patients. Although they expressed understanding of their role during interviews, they felt it beneficial to remind PAB members that they provide special expertise as patients.
Significant contributions
PAB members felt several contributions were particularly impactful. Most frequently mentioned was a 3½-min animated recruitment video made in 2018 to explain PEPPER to prospective patient participants (available at www.pepperstudy.org). Of nearly equal importance was the suggestion to delay recruitment and consenting of patient preferences survey participants post-main PEPPER trial enrollment and post-operatively. Other notable contributions included omitting compression boots from the study protocol due to patient inconvenience; optimizing follow-up survey communication; adopting a PEPPER business card, Primary Care Provider letter and refrigerator magnet reminder; and adding COVID-19 vaccine questions to participant surveys. It is important to emphasize that every PAB member idea was not adopted exactly as initially offered, but every serious suggestion did stimulate an engaged discussion with the research team and each did result in implementation of modifications to the study protocol. The most challenging discussion centered around the PAB suggestion to delay recruitment into the anticoagulation preferences study until after enrollment into the main comparative effectiveness trial. The PAB expressed concern that the detailed information conveyed for the anticoagulant preferences trial would likely deter some patients from enrolling in the main trial. The investigators were motivated to start preferences recruitment concurrent with that into the main trial in an effort to increase overall enrollment. After a protracted dialogue that extended across three PAB meetings and more than 12 months, the decision was made to heed the concerns of the PAB and the preferences enrollment discussion was delayed until the patient had completed the four week period of postoperative anticoagulation.
Process of contributing
Members spoke highly about the semi-annual meeting organization and conduct, appreciating that meetings were efficient, concise (4 h, twice/year), productive and inclusive. Many appreciated how the PI actively solicited input, offering everyone a speaking opportunity.
“I also know professionally that some of the best ideas of my staff came from the quiet ones who sat there and really listened and [the PI] is very good about getting everybody's involvement.” – PAB Member #3
Everyone expressed that the research team and PAB members were respectful of each other. Many spoke highly of the team's diverse backgrounds and stated that it was critical that some board members had experienced complications after surgery given the study's nature and outcomes. They agreed that group discussions of shared experiences were effective, with one member also appreciating the opportunity to connect individually during lunch or breaks.
“I certainly felt respected by the team, and I also at the same time never felt like I'd overstepped by making those comments.” – PAB Member #2
Members also spoke about challenges. Many expressed difficulties recalling study aspects between meetings and suggested interim updates. While most appreciated detailed slides and updates at meetings, one suggested these be simplified to the most relevant material. Another suggested sharing an “executive summary” in addition to agenda and slides prior to meetings. Several individuals expressed that maintaining a fluid, dynamic conversation was challenging during virtual meetings. One member identified that some individuals were more vocal than others and wondered, given the complexity of the study, whether everyone felt comfortable contributing.
Effect on future patients & members of the PAB
When speaking about the impact of the study on future patients, PAB members hoped that study findings would lead to improved and individualized treatment plans for VTE prevention supporting better patient recovery. They hoped to prompt surgeons to consider risk from a patient's perspective and foster shared decision-making discussions. Many believed that knowledge of the PAB's involvement would reassure future patients that someone was working directly for their benefit.
All members of the PAB expressed positive sentiments about their own involvement, using words like ‘privilege’, ‘pleasure’, ‘proud’ and ‘honor.’
“I thought the meetings of the advisory board were significant. I would like to think that we contributed a great deal. There was no hardship. It was an honor being a part of it.” – PAB Member #4
Research team impressions of the PAB
From the research team's perspective, the most impactful PAB contribution was their recommendation to not include compression boots as a variable in the study. Pneumatic compression devices enhance lower limb venous circulation, reduce stasis and mitigate thrombosis risk without a related increase in bleeding, making them popular among surgeons. Despite reluctant acceptance by surgeon investigators, the PAB identified inconvenience of device use as a deterrent to study participation and a threat to patient adherence to protocol. Ultimately, the team decided to stratify patients based on local preference for use of compression devices but not require or randomize their use; thus, the PAB's passionate stance simplified the study to comparison of three medicinal anticoagulants.
One research team concern was whether all PAB members felt comfortable contributing, noting that some individuals, particularly those with medical and doctorate-level training, seemed more comfortable in voicing their opinion. Suggestions to address these concerns included using other methods to collect PAB feedback, such as short surveys or smaller discussion groups.
Consensus conversation
Seven PAB members were present for an in-person meeting held during November 2022 and one attended virtually. The research team presented results of the informant interviews and research team perspectives to the PAB for their review and comment. Discussion focused on PAB impact on the study, PAB challenges and suggestions, and the impact of the study on future patients.
Greatest impact to study
The study Principal Investigator, as well as a majority of the researchers, felt that not including pneumatic compression boots was most impactful, while only two PAB members, both in the medical field, identified this as one of the greatest PAB contributions. The specific exclusion of sequential compression devices (SCDs) as a controlled variable in the study was a pivotal early decision that was initially met with skepticism by the PI and other investigators since SCDs were a popular and important VTE prophylaxis option that had little downside risk. Several discussions on the matter were held with the PAB, whose members unanimously agreed that a need to wear the devices after discharge would be a substantial dissatisfier for patients that would undoubtedly discourage patient enrollment in the overall trial. This patient-perceived deterrent to enrollment ultimately carried the day with the PI who joined the PAB opinion in persuading the remainder of the study team surgeons to relegate SCDs to a local preference item and retrospectively stratify for their use in the analysis. There is no doubt that this early critical decision that swung in favor of the PAB clearly established its place as an important partner in the trial. PAB members and researchers agreed that delaying enrollment in the patient preferences survey had substantial impact on the design and success of the study. The team postulated that asking patients to think deeply about surgery risk immediately before having an operation, especially the probability of a fatal VTE, would discourage involvement in either portion of the study. PAB members worried that concurrently recruiting patients to the main trial and the preferences study would confuse patients, leading them to decline involvement and possibly decline an ultimately beneficial surgery. Although this matter elicited conflicting views between researchers and PAB members, the strongly held convictions of the PAB again ultimately prevailed and resulted in the delay of patient enrollment in the preferences study post-operatively.
Challenges & suggestions
PAB members suggested brief interval updates including enrollment, operational issues and participant interactions to ease the transition between study meetings. Additionally, members suggested including an “executive summary” in slides shared before meetings to allow them to prepare thoughts. PAB member comfort in sharing their thoughts at meetings was of considerable concern to researchers and was explored in the combined meeting. PAB members reiterated that even when quiet, they never felt intimidated to speak. One member mentioned if someone had already voiced their thoughts, they didn't feel it necessary to speak, implying that variable contribution was a product of temperamental differences rather than reluctance to express differing opinions.
Impact of the study on future patients
Of the possible impacts that the study might have on future patients, the one most frequently emphasized by PAB members was strengthening of the patient–surgeon relationship. They were resolute in their hope that study results would engage surgeons and patients in deeper discussions about medication risks and benefits and the risk of life-threatening VTE and bleeding after surgery, facilitating trust in the surgeon and promoting shared decision-making.
Discussion
This evaluation of a patient advisory board (PAB) serving as collaborators with the primary research team on a large pragmatic comparative effectiveness trial vividly demonstrates how patients can optimize study design and conduct, and provide insights that may improve study outcomes. Considering its modest cost relative to the entire PEPPER budget and positive impact to the trial, the cost/benefit of the PAB cannot be overstated. Moreover, PAB members enjoyed their experience, were proud of their contributions, and felt good about giving their time and effort to improving the trial. This effective collaboration between patients and researchers may increase the number of patients interested in participating in clinical trials and the likelihood of researchers inviting patients to serve as co-investigators.
While differences of opinion arose between researchers and PAB members regarding which contributions were most impactful, two protocol changes were likely very influential on study outcome. The original design of PEPPER proposed medication treatment arms that were augmented by the use of pneumatic compression devices. Due to PAB insistence, the study was simplified to three treatment arms without compression boots, reducing operational challenges related to standardization of devices across multiple sites and avoiding potential adverse effects on trial enrollment, protocol adherence and data quality. Additionally, the PAB recommendation to delay patient enrollment into the preferences sub-study likely optimized enrollment for both the PEPPER trial and preferences sub-study. Common to both of these controversial PAB-driven decisions that met with initial resistance from the primary research team was a respectful and very candid discussion that was moderated by the study PI. It was essential that everyone's views were heard and considered prior to arriving at a final decision, which was determined in all instances by consensus.
Notably, this evaluation method uniquely involved PAB self-perceptions about their influence. The engagement literature contains little information on what patients think of their involvement in the design and operationalization of clinical research studies [3]. While most evaluations are performed from the researcher's viewpoint, we sought to explore how patients perceived their own involvement and its value to them.
Differences in patient and researcher perspectives were evident at the consensus meeting. PAB members uniformly emphasized that strengthening the patient–surgeon relationship was the most important byproduct of discussions catalyzed by the study. While researchers were primarily interested in answering the clinical question of optimal VTE anticoagulation, PAB members were focused on patient comfort around surgery and trust in their surgeon. They suggest that whatever the outcome of the trial, it will encourage treatment preference discussions between patient and surgeon that will increase patient confidence in their surgeon. While seemingly subordinate to the primary clinical therapeutic outcome, a positive doctor–patient relationship has been shown to have beneficial impact to patient outcomes [21,22]. Already essential in elective and discretionary procedures such as TJA, the conversation between patient and surgeon becomes increasingly important if trial results reveal no clear advantage with the study medications, in which case shared decision-making is essential to align anticoagulation choice with patient risk preferences. Such a process is not only ethical but increasingly preferred by patients [23,24]. Indeed, encouragement of such patient–surgeon discussions is an important component of patient engagement in comparative effectiveness trials as established by the Institute of Medicine [25,26] and endorsed by PCORI.
There were some limitations to this analysis that should be acknowledged. Evaluation of the PAB may have been biased toward the researcher perspective as it was performed by the PEPPER trial team. While an external evaluator may have further reduced risk of bias, the newest research team member's relative unfamiliarity with the PAB, prior experience with qualitative healthcare and program evaluations [27,28], and baseline knowledge of the trial was deemed preferable. Accordingly, all interviews were conducted one-on-one to encourage candor; PAB members understood only one other team member would access the interview for analysis, results would be aggregated, and quotes anonymized. All PAB members were the PI's patients and expressed strong positive feelings about the value of the patient–surgeon relationship. This augmented their dedication to the PAB yet may have also limited their willingness to be critical of the study or the PAB. Accordingly, it is important that the PI invite candor during PAB meetings and be excluded from PAB assessment interviews. Additionally, the PAB was formed with a broad emphasis on diversity, including socioeconomic background, vocation and life experience, to reflect the patient population receiving TJA. Racial diversity of the PAB reflected the national joint replacement registry [16] and was critical because underrepresented groups have more difficulty with post-operative TJA rehabilitation and access to care [29,30]. Inclusion of patients who have experienced surgical complications is essential for a balanced view of the risks and benefits of TJA.
Opportunities for optimization of patients engaged as co-investigators in clinical trials are noteworthy. The essential role of PAB members conveying the patient perspective should be prioritized, regardless of their professional background. Provision of a brief update about study progress a week prior to semi-annual PAB meetings may facilitate members' readiness to re-engage with the study at scheduled meetings. Finally, the PAB valued in-person meetings, so these were prioritized following COVID. Positive reinforcement on PAB meeting conduct included active solicitation of input from all members [31], which promoted feelings of value and mutual respect among PAB members. While the research team was concerned about whether PAB members felt comfortable in expressing opinions, they uniformly stressed their confidence sharing opinions with the board and wider research team. In summary, our experience with a patient advisory board in a large multi-site clinical comparative effectiveness trial produced benefits to both the scientific rigor and relevance of important trial outcomes to patients while engendering patient good will, supporting engagement in clinical research, and fostering meaningful conversations that nurtured the physician-patient relationship.
Summary points
•
Patient engagement in the design and conduct of clinical effectiveness trials is increasingly common, and helps to emphasize outcomes that are important to patients.
•
A patient advisory board (PAB), which may be involved in all research stages, is one method of formalizing patient engagement.
•
The Patient Centered Outcomes Research Institute (PCORI) has stimulated patient engagement in clinical trials by requiring grantees to detail how their research engages stakeholders, especially patients, and to regularly report engagement strategies and tactics.
•
The Pulmonary Embolism Prevention after Hip and Knee Replacement (PEPPER) Trial: Balancing Safety and Effectiveness, is an ongoing comparative effectiveness trial that was initiated in 2016 and has operated with a PAB since its inception.
•
Little has been published from the perspective of patient researchers on how they value their involvement as co-investigators in clinical trials.
•
The PEPPER Clinical Coordinating Team conducted an evaluation of the impact of the PAB on the design and conduct of the Trial and sought to compare and contrast patient and researcher perspectives on their most important contributions to the trial.
•
PAB members believed their most impactful contribution was a recruitment video while researchers believed it was the decision to not include compression boots as a study variable.
•
PAB members hoped that the results of the trial would lead to better patient–surgeon relationships and shared decision-making while researchers were more focused on trial outcomes, highlighting differences in perspectives that bring value to the design and conduct of the trial.
•
The contributions of the PAB led to two protocol changes that were very influential on study conduct and eventual outcomes, and will likely aid in encouraging treatment preference discussions between patient and surgeon, thereby supporting the ultimate goal of improved patient outcomes.
•
Central to having a functional and engaged patient advisory board was the serious consideration of every substantive PAB suggestion in an open minded moderated discussion that produced an outcome that was arrived at by consensus.
Author contributions
All authors contributed to the conception and design of this work and related manuscript. Interview script was prepared by LM Kernan and reviewed by VD Pellegrini and CA Lambourne. Data collection was performed by LM Kernan. Data analysis was performed by LM Kernan, MB Pearl, C Lambourne and V Pellegrini. The first draft of the manuscript was written by LM Kernan and all authors participated in review and revision of subsequent versions of the manuscript. All authors read and approved the final manuscript.
Acknowledgments
The research team would like to express our deep appreciation to all members of the PEPPER patient advisory board for their considerable contributions to the PEPPER trial: R Bulger (co-chair), R Bulger, MB Crummer, C McCollister Evarts (co-chair), D Hamilton, N Mullen, C Persels, R Schlegel, S Seely, D Smith and M Thompson (posthumously).
Financial disclosure
The PEPPER Trial and the work of the patient advisory board was funded by the Patient Centered Outcomes Research Institute (PCORI) PCS-1402-09328-IC. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interests disclosure
The authors have no financial and/or nonfinancial competing interests or relevant affiliations with any organization/entity to declare that are relevant to the subject matter or materials discussed in this manuscript. This includes employment, grants or research funding, consultancies, membership on scientific or other advisory boards, honoraria, stock ownership or options, paid expert testimony, patents received or pending, or royalties.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Investigational Review Board for Human Research (Pro00053742) of The Medical University of South Carolina which served as a single central IRB for the PEPPER Trial. Verbal informed consent was obtained prior to each participant interview.
Data sharing statement
The data underlying this article cannot be shared publicly to protect the privacy of the individuals that participated.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
PCORI. About PCORI. (2021). Available at: https://www.pcori.org/about/about-pcori
2.
Smith MY, Janssens R, Jimenez-Moreno AC et al. Patients as research partners in preference studies: learnings from IMI-PREFER. Res. Involv. Engagem. 9(1), 21 (2023).
• Describes patient engagement in patient preference research studies. It discusses which activities patients were involved in and their impact on the research.
3.
Forsythe LP, Carman KL, Szydlowski V et al. Patient engagement in research: early findings from the Patient-Centered Outcomes Research Institute. Health Aff. (Millwood) 38(3), 359–367 (2019).
• This review article examines descriptions of patient engagement in The Patient Centered Outcomes Research Institute (PCORI)-funded studies and examines evidence of its benefits to comparative effectiveness research.
4.
Crocker JC, Ricci-Cabello I, Parker A et al. Impact of patient and public involvement on enrolment and retention in clinical trials: systematic review and meta-analysis. BMJ 363, k4738 (2018).
5.
Carman KL, Workman TA. Engaging patients and consumers in research evidence: applying the conceptual model of patient and family engagement. Patient Educ. Couns. 100(1), 25–29 (2017).
6.
Domecq JP, Prutsky G, Elraiyah T et al. Patient engagement in research: a systematic review. BMC Health Serv. Res. 14, 89 (2014).
7.
PCORI (Patient Centered Outcomes Research Institute) Website. PCORI Engagement Rubric. (2014).
8.
Sheridan S, Schrandt S, Forsythe L, Hilliard TS, Paez KA. Advisory Panel on Patient Engagement (2013 inaugural panel). The PCORI engagement rubric: promising practices for partnering in research. Ann. Fam. Med. 15(2), 165–170 (2017).
• Describes the development of the PCORI Engagement Rubric, which provides researchers with guidelines on engaging patients in patient centered outcomes research.
9.
Vanderloo LM, Vanderhout SM, Tavares E, Maguire J, Straus S, Birken CS. Parent engagement in co-design of clinical trials: the PARENT trial. Trials 22(1), 347 (2021).
10.
Natafgi N, Tafari AT, Chauhan C, Bekelman JE, Mullins CD. Patients' early engagement in research proposal development (PEER-PD): patients guiding the proposal writing. J. Comp. Eff. Res. 8(6), 441–453 (2019).
11.
Poleshuck E, Wittink M, Crean H et al. Using patient engagement in the design and rationale of a trial for women with depression in obstetrics and gynecology practices. Contemp. Clin. Trials 43, 83–92 (2015).
12.
Gorbenko O, Cavillon P, Giles RH et al. Co-creating with patients an impact framework across the medicine's life cycle: a qualitative study exploring patients' experiences of involvement in and perceptions of impact measures. Res. Involv. Engagem. 8(1), 1 (2022).
13.
Marquis-Gravel G, Faulkner M, Merritt G et al. Importance of patient engagement in the conduct of pragmatic multicenter randomized controlled trials: The ADAPTABLE experience. Clin. Trials Lond. Engl. 20(1), 31–35 (2023).
14.
PCORI. Engagement in Health Research Literature Explorer. Available at: https://www.pcori.org/engagement/engagement-literature
15.
Pellegrini VD, Eikelboom JW, Evarts CM et al. Randomised comparative effectiveness trial of Pulmonary Embolism Prevention after hiP and kneE Replacement (PEPPER): the PEPPER trial protocol. BMJ Open 12(3), e060000 (2022).
16.
American Joint Replacement Registry. American Joint Replacement Registry 2017 Annual Report Figures. (2017).
17.
Webex. The leader in collaboration & customer experience. Available at: https://www.webex.com/
18.
Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 13(1), 117 (2013).
19.
Gale RC, Wu J, Erhardt T et al. Comparison of rapid vs in-depth qualitative analytic methods from a process evaluation of academic detailing in the Veterans Health Administration. Implement. Sci. IS 14, 11 (2019).
20.
Hamilton AB, Finley EP. Qualitative methods in implementation research: an introduction. Psychiatry Res. 280, 112516 (2019).
21.
Olaisen RH, Schluchter MD, Flocke SA, Smyth KA, Koroukian SM, Stange KC. Assessing the longitudinal impact of physician-patient relationship on functional health. Ann. Fam. Med. 18(5), 422–429 (2020).
22.
Kelley JM, Kraft-Todd G, Schapira L, Kossowsky J, Riess H. The Influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. PLOS ONE 9(4), e94207 (2014).
• This literature review and meta-analysis examines how the emotional and cognitive care of a physician may enhance the health outcomes of a patient.
23.
Stiggelbout AM, Pieterse AH, De Haes JCJM. Shared decision making: concepts, evidence, and practice. Patient Educ. Couns. 98(10), 1172–1179 (2015).
• Describes the history of shared decision making, its utility and current evidence of its practice. It also discusses ways to improve implementation of shared decision making.
24.
Chewning B, Bylund CL, Shah B, Arora NK, Gueguen JA, Makoul G. Patient preferences for shared decisions: a systematic review. Patient Educ. Couns. 86(1), 9–18 (2012).
25.
Sox HC, Greenfield S. Comparative effectiveness research: a report from the institute of medicine. Ann. Intern. Med. 151(3), 203–205 (2009).
26.
PCORI. Our Vision & Mission. Available at: https://www.pcori.org/about/about-pcori/our-vision-mission
27.
Kernan LM, Dryden EM, Nearing K et al. Integrating CFIR-ERIC and e-Delphi Methods to Increase Telegeriatrics Uptake. The Gerontologist 63(3), 545–557 (2023).
28.
Pimentel CB, Dryden EM, Nearing KA et al. The role of Department of Veterans Affairs community-based outpatient clinics in enhancing rural access to geriatrics telemedicine specialty care. J. Am. Geriatr. Soc. 72(2), 520–528 (2024).
29.
MacMahon AS, Mekkawy KL, Barry K, Khanuja HS. Racial and ethnic disparities in short-stay total knee arthroplasty. J. Arthroplasty 38(7), 1217–1223 (2023).
30.
Chun DS, Leonard AK, Enchill Z, Suleiman LI. Racial disparities in total joint arthroplasty. Curr. Rev. Musculoskelet. Med. 14(6), 434–440 (2021).
31.
Hamilton CB, Hoens AM, Backman CL et al. An empirically based conceptual framework for fostering meaningful patient engagement in research. Health Expect. Int. J. Public Particip. Health Care Health Policy 21(1), 396–406 (2018).
• Describes the evidence-based development and testing of a framework, endorsed by patients, for engaging patients in research.
Information & Authors
Information
Published In
Copyright
© 2025 The authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 28 March 2024
Accepted: 20 December 2024
Published online: 30 January 2025
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The impact of a patient advisory board on a clinical comparative effectiveness trial: a comparison of patient and researcher perspectives. (2025) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0050
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Seth S. Leopold, Editor’s Spotlight/Take 5: What Would Be the Effect of Lowering the Threshold of Statistical Significance From 0.05 to 0.005 in Foot and Ankle Randomized Controlled Trials?, Clinical Orthopaedics & Related Research, 10.1097/CORR.0000000000003779, 484, 1, (3-8), (2025).
- Hannah Leyva, John Fanikos, Zhou Lan, Giovanni Scimeca, Behnood Bikdeli, Gregory Piazza, Samuel Z. Goldhaber, Aspirin for Venous Thromboembolism Prophylaxis in Hip Fracture, Total Knee, and Hip Arthroplasty, The American Journal of Medicine, 10.1016/j.amjmed.2025.03.020, 138, 9, (1185-1196), (2025).