First in class, best in class or a wild card: who will dominate the anti-obesity medication market?
Publication: Journal of Comparative Effectiveness Research
The anti-obesity medication (AOM) market presents a significant opportunity for pharmaceutical companies, with the global prevalence of obesity estimated to reach 1.9 billion by 2035. This review examines the unique characteristics of the AOM market and evaluates whether the principles of ‘first-in-class’ or ‘best-in-class’ are likely to determine market success. We argue that the multifactorial nature of obesity and the rapidly evolving AOM market necessitate a more nuanced approach. Factors such as weight loss efficacy, impact on obesity-related complications, mode of administration, patient access through reimbursement and strategic positioning will play crucial roles in determining the success of AOMs. While Novo Nordisk and Eli Lilly currently lead the race with their GLP-1 agonists, the competitive landscape is expanding with numerous drug candidates in the pipeline. We conclude that pharmaceutical companies must carefully consider their strategies, balancing clinical efficacy, patient preferences and market access to unlock the full potential of the AOM market. Ultimately, the winner will likely be determined by a combination of factors rather than a single ‘first-in-class’ or ‘best-in-class’ approach.
Obesity & the need for interventions
Obesity, and the multimorbidity commonly associated with it, is one of the most pressing challenges facing healthcare systems and wider society today. This makes the AOM market a significant commercial opportunity for pharmaceutical companies. The global prevalence of obesity, defined as BMI ≥30, was estimated to be 14% [1] (nearly 1 billion people) in 2020 with predictions that obesity prevalence could reach 24% (1.9 billion) by 2035 [1]. The resulting global economic impact is equally striking at US$1.96 trillion in 2020, rising to over US$4 trillion in 2035 [1] (considering the cost of treating obesity and its consequences, impact on economic productivity and premature retirement or death) and demonstrates the undeniable importance of obesity from a public health perspective.
The underlying etiology of obesity is multifactorial with contribution from poor diet, physical inactivity and other environmental factors. Not only does obesity have direct medical implications, it is also associated with an increased risk of a variety of other conditions termed obesity related complications (ORCs), such as Type II diabetes mellitus (T2DM), cardiovascular disease (CVD), osteoarthritis, sleep apnoea and certain types of cancers [2]. The risks of developing and the prevalence of a selection of ORCs are shown in Figure 1 [3,4]. There is therefore a clear need for interventions to reduce rates of obesity, for the benefit of patient outcomes, health system sustainability and society at large. However, there is a significant challenge with respect to contention around the recognition of obesity as a disease or not, and the implications of this on both clinical guidelines and funding for the treatment of obesity. For example, under the German Social Code, obesity is not recognised as a disease and hence pharmacological treatments are not reimbursed [5].
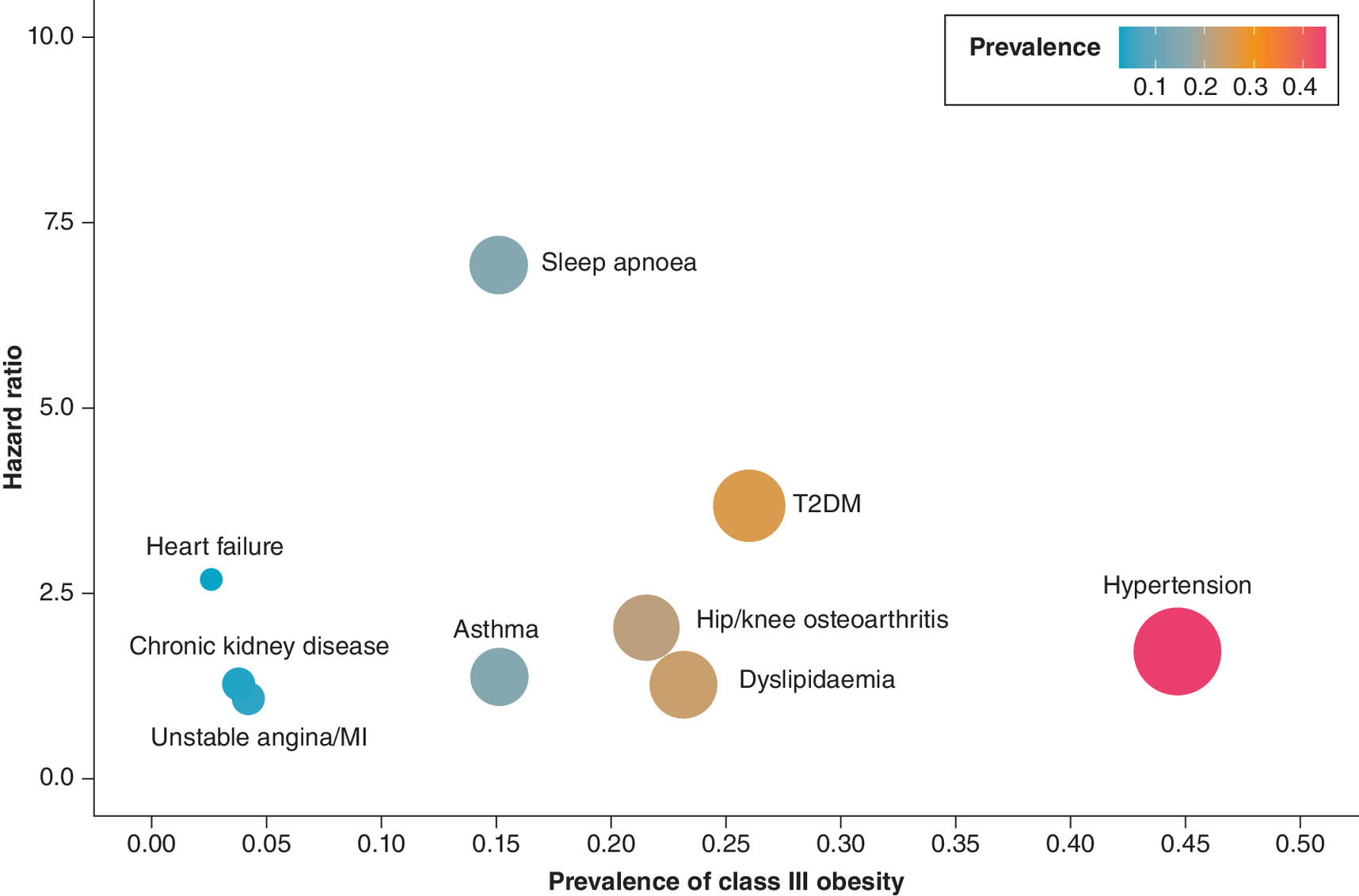
Figure 1. Hazard ratios for individuals with BMI of 45 kg/m2 relative to a stable BMI of 30 kg/m2 and prevalence of obesity related complications for individuals between BMI 40 kg/m2 and 70 kg/m2 (class III).
Current treatments for obesity include lifestyle interventions (such as improved diet and increased physical activity), pharmacotherapy and bariatric surgery, with tailoring required for each patient. Despite the apparent need for intervention, historically there have been few pharmacological treatment options available. However, it is a therapeutic area that is now experiencing strong innovation with the field recently being opened up by the glucagon-like peptide-1 (GLP-1) agonist class, and the rewards for the winner are staggering – analysis by Goldman Sachs estimates that the AOM market will grow to around $100 billion in 2030 [6]. As there are now a number of pharmaceutical companies vying to become the market leader in the AOM space, it begs the question of who will come out on top and how will they get there?
Best in class versus first in class
The common debate of whether ‘first-in-class’ or ‘best-in-class’ medications will gain the lion's share of a market is challenging to answer in the context of AOMs, given the market's unique characteristics: the scale of the eligible population, access challenges due to differing payer perception of obesity, and rapid innovation with newer treatment classes already entering the market. It is however an important debate to consider, given the impact it will have on the future drug development ecosystem, as well as clinical practice and patient outcomes. Drawing on our experience of obesity, market access and pharmaceutical commercial strategy, this review considers whether either of the first-in-class or best-in-class principles might apply to the AOM market, or if other factors are more likely to drive success.
A previous analysis has shown that first to-launch products are more and more likely to become the market leaders. For example, the RET kinase inhibitor selpercatinib (Retevmo; Eli Lilly), launched just 3 months before pralsetinib (Gavreto; Blueprint Medicines), has managed to obtain more than 70% market share in USA, and now has the entire ex-US market to itself given the withdrawal of pralsetinib from these markets [7,8]. Despite examples like these, market share can be won by having a best-in-class profile, differentiating on efficacy, safety or convenience. A well cited example of best-in-class being successful, when viewing ‘best’ from the perspective of the drug being the most clinically efficacious, is the treatment of raised LDL cholesterol with atorvastatin (Lipitor; Pfizer). It was the fifth statin that came to market but became the market leader (and highest grossing drug of all time) due to its therapeutic advantage over statins launched before it. However, despite this being a widely cited example of best-in-class winning out, Pfizer also had other strategies to support the success of Lipitor including pricing lower than competitors and aggressive marketing (including direct to consumer marketing in USA) [9]. Similarly, other strategies besides increased efficacy have proved effective in the oncology therapeutic area, with clinical trial strategy determining success for pembrolizumab (Keytruda; Merck). Both pembrolizumab and nivolumab (Opdivo; Bristol Myers Squibb) are programmed death receptor-1 (PD-1) inhibitors that are used to treat many different types of cancers with similar levels of efficacy. Opdivo was the first PD-1 inhibitor in the world to receive regulatory approval, however Keytruda now outsells Opdivo by more than two to one. This was as a result of Bristol Myers Squibb taking a big risk by performing a randomized controlled trial in all patients for first-line treatment of the one of the largest cancer indications (non-small-cell lung cancer [NSCLC]), whereas Merck pursued a more cautious approach by focusing on a narrower segment of biomarker positive NSCLC patients [10]. The Bristol Myers Squibb clinical trial failed, whereas the Merck trial was successful, meaning Merck's strategic decision enabled to them to take the lead in NSCLC and ultimately Bristol Myers Squibb was never able to catch up.
The anti-obesity medication market
Taking a view of the AOM market, we believe that the concept of first-in-class winning does not necessarily hold, and believe the alternative avenues that pharmaceutical companies might take will become increasingly important. GLP-1 agonists are the only example currently where there are multiple AOMs within the same class approved for treating obesity. The first GLP-1 agonist on the market was liraglutide (Saxenda; Novo Nordisk), which had some success due to proven efficacy, however semaglutide (Wegovy; Novo Nordisk) then took the market by storm when it followed with even superior efficacy. Semaglutide was shown to facilitate a six-percentage point greater weight loss effect than liraglutide (13.8 vs 7.8%) [11]. More recently in November 2023, the US FDA approved tirzepatide (Zepbound; Eli Lilly) for chronic weight management (including weight reduction and maintenance) [12]. While tirzepatide is a GLP-1 agonist, it is also a glucose-dependent insulinotropic polypeptide (GIP) agonist, hence does not fit wholly into the same narrow definition of drug class as semaglutide/liraglutide but highlights the rapid innovation in the field. Further drugs in the pipeline utilizing novel treatment class combinations include: a combination of semaglutide and a long-acting amylin analog cagrilintide, called CagriSema (Novo Nordisk); and a triple agonist of GLP-1, GIP and glucagon receptors, called Retatrutide (Eli Lilly). We therefore consider AOMs broadly as treatments for obesity rather than focusing on a specific class. A summary of key current AOMs and upcoming AOMs are shown in Figure 2 [13–34].
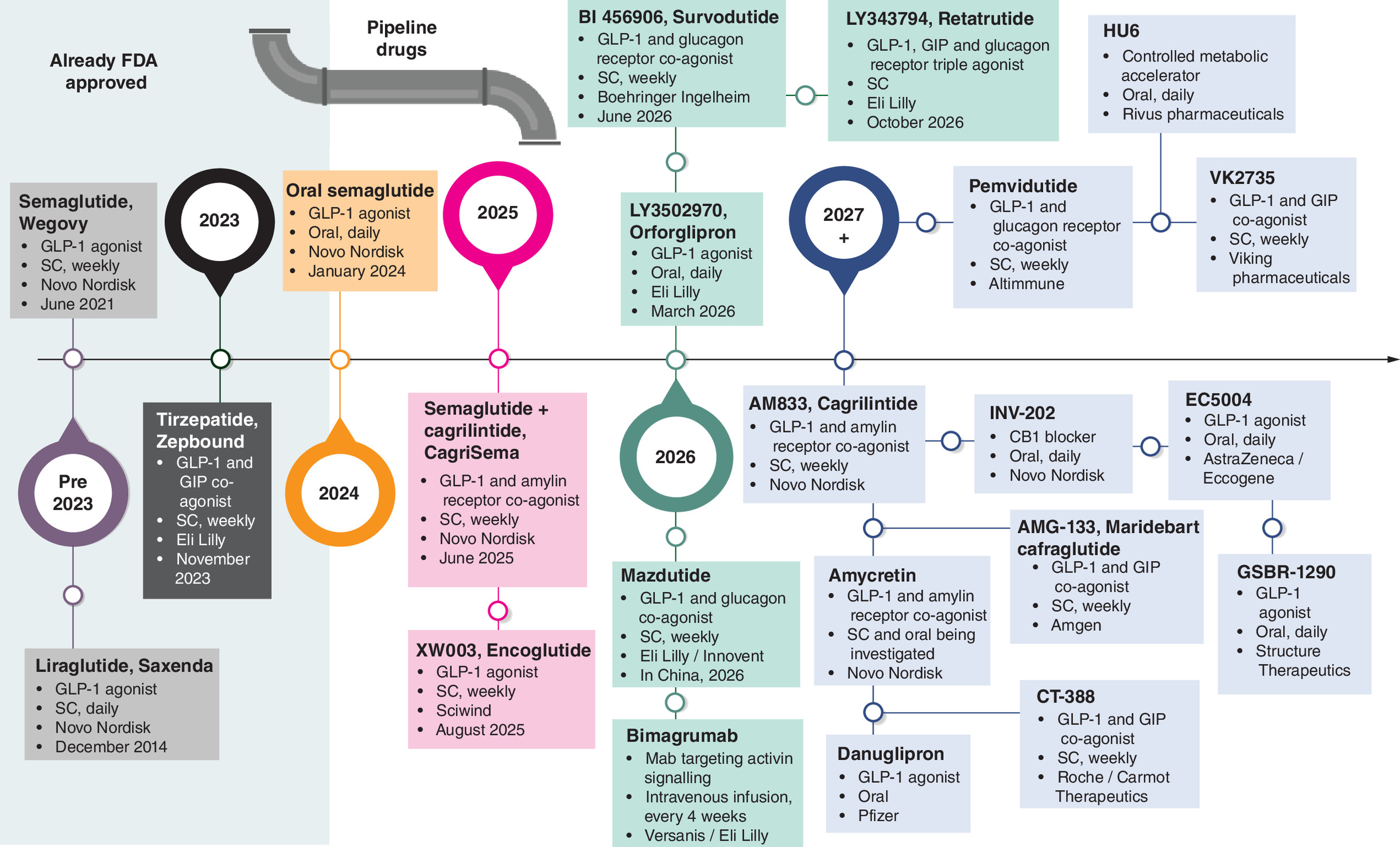
Figure 2. Current GLP-1 agonist anti-obesity medications and expected upcoming anti-obesity medications.
Information from https://clinicaltrials.gov/ and/or company websites [13–34].
SC: Subcutaneaous.
What does best in class mean in the AOM market?
Given the multifactorial nature of obesity and the highly competitive, rapidly evolving AOM market, the factors that will determine which AOM is considered best-in-class are also likely to be complex. In the example above, it is already apparent that semaglutide won out over the first-in-class medicine, liraglutide, most likely due to its superior clinical efficacy in terms of weight loss, but there was also another advantage in terms of its once weekly administration as opposed to liraglutide's daily requirement [35]. In the AOM market, the best-in-class medication is likely to be determined by not only clinical efficacy in terms of weight reduction, but also in terms of weight maintenance, impact on ORCs and mode of administration.
Weight loss & maintenance
While there are likely to be multiple factors that determine what constitutes the best-in-class drug for AOMs, the focus for current AOMs is weight reduction. Current market leader Novo Nordisk's semaglutide showed a 14.9% weight reduction in the STEP-1 clinical trial in comparison to 2.4% reduction with the placebo at 68 weeks [36]. Meanwhile, ahead of its recent approval by the FDA, Eli Lilly's tirzepatide showed a 20.9% weight reduction at 72 weeks compared with 3.1% reduction with the placebo in the SURMOUNT-1 trial [37]. The phase IIIb clinical trial directly comparing both medications (SURMOUNT-5) is ongoing [38]. AOMs due to come to market in the future are likely to show incrementally improvements in weight reduction including Novo Nordisk's CagriSema and Eli Lilly's triple agonist retatrutide. However, it remains to be seen whether there will be a limit in how much weight reduction is clinically relevant or beneficial to patients. For a patient with BMI of 35, a weight reduction of approximately 29% will result in them achieving a BMI of less than 25, considered a healthy BMI. Furthermore, as there are fewer patients in the highest BMI categories, the market for AOMs with greater weight reduction becomes smaller; meanwhile high amounts of weight reduction may not be clinically appropriate for patients with only moderately raised BMIs. Hence weight maintenance is likely to become an increasingly crucial factor in determining best in class AOM. When considering weight maintenance, recent AOMs such as semaglutide and tirzepatide have shown substantial weight regain after treatment cessation [39,40]. Additional longer-term data is crucial to assess these therapies after multiple years of continuous therapy and the effect of this on weight maintenance and complications relating to obesity. Having different dosing options (or different assets with varying degrees of efficacy) may give manufacturers an edge to potentially allow for dosing flexibility for weight maintenance.
It is not just about weight
In addition to weight loss and maintenance, the impact of novel AOMs on ORCs could be key to unlocking access to the obesity market. From a clinical perspective, it is important that AOMs not only lead to weight reduction, but that this in turn leads to improved patient clinical outcomes by reducing morbidity and mortality, while avoiding significant adverse effects. For example, while the risk of obstructive sleep apnea (OSA) is known to be higher in individuals with obesity (shown in Figure 1), it will be important to show that a reduction in weight with AOMs also leads to a reduction in OSA and its complications, such as hypertension and heart failure. Proving that AOMs improve ORC outcomes that are ‘hard’ and that have a significant cost to patients and healthcare systems (e.g., cardiovascular disease) will be critical for payers who are open to consider the benefits of therapeutics but need to be convinced of their value (especially if they apply a cost per quality-adjusted life year valuation framework) [41]. Alongside a weight loss benefit, demonstrating the extent of improvements in ORC outcomes could, in relevant markets, increase the likelihood of reimbursement or lead to better pricing for manufacturers.
Recently, the first clinical trial to show the benefit of AOMs in ORC outcomes was published; the SELECT trial looked at the impact of semaglutide on cardiovascular risk in patients with overweight and obesity. Results showed a 20% reduction in the risk of major adverse cardiovascular events including cardiovascular mortality [42]. Furthermore, semaglutide and tirzepatide are both in phase III trials investigating their benefits for several ORCs, including non-alcoholic steatohepatitis (NASH), OSA and osteoarthritis. Targeting ORCs with high unmet need, such as NASH will potentially be appealing to payers, clinicians and patients. However, trial design for these ORCs will be important for success. As potentially observed for semaglutide, treating NASH ‘too late’ may lead to a trial failure [43]. Companies will have to carefully plan elements of trial design, including who to treat, when to treat and end points to use to increase the likelihood of positive findings. However, excessive planning will also need to be balanced with speed to produce results before competitors. Trade-offs will need to be made based on stakeholder needs – does a company conduct a large trial for many years to achieve a payer gold standard of hard outcomes, or do they use surrogate end points? As noted for Keytruda, trial design can make or break a product.
The occurrence of adverse effects could also be a strong differentiator when it comes to patient preferences between similar efficacy drugs. While there is a list of possible side effects that can be experienced with the current AOMs on the market, in general they are well tolerated. However, fewer and more minor side effects can only support an AOM and will likely be another contributing factor to success as patients potentially need to take these medicines for a number of years.
Mode of administration
Another key differentiator that pharmaceutical companies could consider is the mode of administration. Patient preferences for the type of delivery (oral vs injectable), regularity of dosage (daily vs weekly) and additional limitations (e.g., taking on an empty stomach and drug interactions) are important to understand in order to design a drug that appeals to the majority of patients and trumps competitor drugs. A study considering administration of T2DM medications showed that patients generally prefer a daily oral T2DM medication over a weekly injectable medication by a ratio of approximately 3:1 (when provided with no additional information and assuming both products are similar in terms of overall effectiveness, side effects and cost) [44]. In the AOM space, patient preference regarding the frequency of dosing may be a contributor to the success of the once weekly dosing regime of semaglutide compared with the once daily dosing of liraglitide [35]. However, the question of whether the oral or injectable route impacts patients is up for debate. It will be interesting to see how patients and the market reacts if Rybelsus, the once-daily oral version of semaglutide, which is currently in clinical trials, gains approval for the treatment of obesity. While Rybelsus is an oral form which could appeal to patients more, there is a requirement for it to be taken on an empty stomach and at a daily frequency, which as noted in the T2DM medication study, could have a negative impact on daily life that ultimately makes it undesirable. This is therefore another key aspect that pharmaceutical companies will need to think about when developing new drugs for the AOM market.
Patient access: perhaps the biggest consideration for success
It is clear that improving solely weight loss efficacy is not the only way for a drug to become considered best-in-class in the AOM market, with weight maintenance, impact on ORCs and mode of administration all having the potential to play a key role in the success of new AOMs. On top of this, there are hurdles that need to be overcome in terms of access and reimbursement of AOMs, and there are also strategic positioning considerations to facilitate a new drug becoming the first choice for patients and physicians.
Unlocking reimbursement
Perhaps the greatest challenge for AOM contenders is to unlock access and reimbursement. This could be considered an area where the AOM market is most unique, in that obesity is perceived by countries such as Germany as a lifestyle choice rather than a clinical disease [5] and therefore AOMs are not publicly reimbursed. In the UK and USA, while obesity is recognized as a medical condition, there are several restrictions that limit reimbursement. England's NICE clinical guidelines recommend semaglutide for use within a specialist weight management service, many of which currently have long waiting list times, and for a maximum of 2 years of treatment. Semaglutide is also limited to patients with at least one weight-related comorbidity, either with BMI >35 kg/m2 or BMI between 30 and 34.9 kg/m2 and meet certain criteria for weight management service referral. In USA, Medicare currently does not cover AOMs broadly due to a provision excluding agents used for weight loss or weight gain. Medicaid covers Wegovy in some capacity for chronic weight management in 14 states and a minority of employer insurance plans cover AOMs: perhaps only about 22% of US employers. Whoever can unlock public reimbursement/insurance coverage of AOMs globally potentially stands to benefit greatly. Tactics may include outcome-based agreements, pricing strategies tailored to address budget impact concerns of payers, and/or the demonstration of the long term, wider benefits of AOMs (e.g. on payer-relevant ORCs and/or the demonstration of the need for continued treatment rather to remove payer enforced stopping rules). Indeed the SELECT data for semaglutide seems to have opened up wider reimbursement through Medicare and Medicaid in USA [45].
The out-of-pocket market versus public reimbursement/insurance
Alternatively, not all obesity treatments are currently paid via insurance or through public reimbursement. In many countries there is a large out-of-pocket market. Here, there is a greater role for effective marketing strategies, the success of which is noted above for Lipitor. Again, as patients themselves are paying, pricing needs to be considered in relation to competitors – will undercutting on price lead to success? Ultimately for patient access there are some strategic considerations to be made – will the focus be on public reimbursement/insurance or on patients paying themselves? Focusing on each segment has its advantages and disadvantages: with patients paying themselves, pricing could potentially be higher for this smaller market, but patients are less likely to adhere to treatment and solely focusing on this route of access will lead to inequity, further exacerbating the inequalities already existing in this therapeutic area. With public reimbursement/insurance coverage, pricing to unlock broad access will be an issue, but once achieved it is likely that more patients will adhere longer to treatment. The optimal solution to the price × volume × length of the treatment equation will need to be found. In terms of ORCs, it is plausible that some may be relevant to an out-of-pocket market even if not deemed payer relevant; further with patients paying themselves, convenience for this population is likely to be a significant value driver.
Positioning
With many different treatment options soon to be available (including many from the same manufacturer), being strategic in positioning of these medicines can help payers, prescribers and patients know when to best use them. For example, depending on their weight loss efficacy, medicines could be positioned based on starting BMI, with those with lower BMI needing a less efficacious product. More efficacious medicines could be used for those with a high BMI, or those already having or at a high risk of specific ORCs and/or those who have been unable to achieve a target weight loss on a less efficacious product (e.g., an escalation strategy).
Eli Lilly has taken a new step to position their obesity drugs at the forefront, launching LillyDirect which connects patients with independent providers who can prescribe AOMs such as Lilly's new drug Zepbound. This marketing approach offers a novel route for individuals to access AOMs, which will ultimately facilitate higher sales of AOMs like Zepbound. By having clear positioning, manufacturers can differentiate their product and potentially achieve a pricing premium.
Conclusion
It remains to be seen as to whether first-in-class, best-in-class or an entirely different strategy will underpin success in the AOM market. Given the highly competitive arena, alongside the substantial unmet need and associated healthcare and economic burden, pharmaceutical companies taking part in the AOM competition will need to spend time considering their strategy. Will they seek to differentiate on efficacy and/or price? If efficacy, will it be on weight loss or on ORCs? If ORCs, what should they demonstrate improvements in and what is the best trial design to prove benefits to stakeholders, but also have results read out before competitors? Importantly, whoever unlocks reimbursement opportunities and shapes the global perception of obesity from a lifestyle choice to a treatable disease will have a significant advantage. All of these factors will trade off against each other to determine the winner – apixaban (Eliquis; Bristol Myers Squibb/Pfizer), despite being the third to market, less convenient than the initial leading competitor (taken twice a day as compared with once a day for rivaroxaban (Xarelto; Janssen)), became the market leader in direct oral anti-coagulants because of its best-in-class clinical efficacy and a strong commercial strategy of demonstrating this profile through real-world data [46]. While it appears that Novo Nordisk and Eli Lilly are currently the front runners in the AOM race, there are numerous other drug candidates in the pipeline across the pharmaceutical industry: it seems that the race is just beginning, and only time will tell who will win it and how.
Financial disclosure
The authors are employees of Lane Clark and Peacock LLP, which advises life sciences organizations developing treatments for obesity. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
1.
World Obesity Day Atlases. Obesity Atlas 2023. World Obesity Federation Global Obesity Observatory. Available from: https://data.worldobesity.org/publications/?cat=19
2.
Mohajan D, Mohajan HK. Obesity and its related diseases: a new escalating alarming in global health. J. Innov. Med. Res. 2, 12–23 (2023).
3.
Haase CL, Lopes S, Olsen AH, Satylganova A, Schnecke V, McEwan P. Weight loss and risk reduction of obesity-related outcomes in 0.5 million people: evidence from a UK primary care database. Int. J. Obes. 45, 1249–1258 (2021).
4.
Evans M, de Courcy J, de Laguiche E et al. Obesity-related complications, healthcare resource use and weight loss strategies in six European countries: the RESOURCE survey. Int. J. Obes. 47, 750–757 (2023).
5.
WHO MiNDbank - Sozialgesetzbuch (SGB) Fünftes Buch (V) Gesetzliche Krankenversicherung (Social Code (SGB) Book Five (V) Statutory Health Insurance). Available from: https://extranet.who.int/mindbank/item/2266
6.
Obesity drugs are a potential US$100 billion opportunity by 2030, say Goldman Sachs analysts, Companies & Markets - THE BUSINESS TIMES. Available from: https://www.businesstimes.com.sg/companies-markets/obesity-drugs-are-potential-us100-billion-opportunity-2030-say-goldman-sachs
7.
Lilly Reports Second-Quarter 2023 Financial Results, Highlights Accelerating Revenue Growth and Key Pipeline Advancements | Eli Lilly and Company. Available from: https://investor.lilly.com/news-releases/news-release-details/lilly-reports-second-quarter-2023-financial-results-highlights
8.
Liu A. After splashing $1B, Roche returns Gavreto to Blueprint. Available from: https://www.fiercepharma.com/pharma/after-splashing-1b-roche-returns-lagging-cancer-drug-gavreto-blueprint (2023).
9.
The fall of the world's best-selling drug. Available from: https://www.ft.com/content/d0f7af5c-d7e6-11de-b578-00144feabdc0
10.
Keytruda vs. Opdivo: No Contest. Available from: https://www.science.org/content/blog-post/keytruda-vs-opdivo-no-contest
11.
Irfan H. Obesity, cardiovascular disease, and the promising role of semaglutide: insights from the SELECT Trial. Curr. Probl. Cardiol. 49, 102060 (2024).
12.
FDA. FDA Approves New Medication for Chronic Weight Management. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management (2023).
13.
Drugs@FDA. FDA-Approved Drugs. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm
14.
Drugs@FDA. FDA-Approved Drugs. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=206321
15.
Drugs@FDA. FDA-Approved Drugs. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=BasicSearch.process
16.
Drugs@FDA. FDA-Approved Drugs. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=217806
17.
Kalapala R. Efficacy of Oral Semaglutide in Overweight or Obesity: Randomized Controlled Trial (OSO Study - Oral Semaglutide for Obesity). (2022). Available from: https://clinicaltrials.gov/study/NCT05442450
18.
Novo Nordisk A/S. Efficacy and Safety of Cagrilintide s.c. 2.4 Mg in Combination With Semaglutide s.c. 2.4 Mg (CagriSema s.c. 2.4 Mg/2.4 Mg) Once-Weekly in Participants With Overweight or Obesity and Type 2 Diabetes. (2024).Available from: https://clinicaltrials.gov/study/NCT05394519
19.
Hangzhou Sciwind Biosciences Co., Ltd. A Phase III, Multi-Center, Randomized, Double-Blind and Placebo-Controlled Study to Evaluate the Efficacy and Safety of XW003 in Adults With Overweight or Obesity (SLIMMER). (2023).Available from: https://clinicaltrials.gov/study/NCT05813795
20.
Eli Lilly and Company. A Phase III, Randomized, Double-Blind Study to Investigate the Efficacy and Safety of Once-Daily Oral LY3502970 Compared With Placebo in Adult Participants With Obesity or Overweight With Weight-Related Comorbidities (ATTAIN-1). (2023).Available from: https://clinicaltrials.gov/study/NCT05869903
21.
Boehringer Ingelheim. A Phase III, Randomised, Double-Blind, Parallel-Group, 76-Week, Efficacy and Safety Study of BI 456906 Administered Subcutaneously Compared With Placebo in Participants With Overweight or Obesity and Type 2 Diabetes Mellitus. (2024).Available from: https://clinicaltrials.gov/study/NCT06066528
22.
Eli Lilly and Company. A Master Protocol to Investigate the Efficacy and Safety of LY3437943 Once Weekly in Participants Without Type 2 Diabetes Who Have Obesity or Overweight: A Randomized, Double-Blind, Placebo-Controlled Trial (TRIUMPH-1). (2023).Available from: https://clinicaltrials.gov/study/NCT05929066
23.
Priyan V. Innovent doses first subject in phase III trial of obesity drug. Clinical Trials Arena (2024).Available from: https://www.clinicaltrialsarena.com/news/innovent-obesity-drug-trial/
24.
Eli Lilly and Company. A Randomized, Double-Blind, Placebo-Controlled Multi-Center Study of Intravenous Bimagrumab, Alone or in Addition to Open Label Subcutaneous Semaglutide, to Investigate the Efficacy and Safety in Overweight or Obese Men and Women. (2023).Available from: https://clinicaltrials.gov/study/NCT05616013
25.
Inc, A. Altimmune Announces Positive Topline Results from MOMENTUM 48-Week Phase 2 Obesity Trial of Pemvidutide. GlobeNewswire News Room (2023).Available from: https://www.globenewswire.com/news-release/2023/11/30/2788970/0/en/Altimmune-Announces-Positive-Topline-Results-from-MOMENTUM-48-Week-Phase-2-Obesity-Trial-of-Pemvidutide.html
26.
VK2735. Viking Therapeutics Available from: https://vikingtherapeutics.com/pipeline/metabolic-disease-program/vk2735/
27.
Amgen. A Phase 2 Randomized, Placebo-Controlled, Double-Blind, Dose-Ranging Study to Evaluate the Efficacy, Safety, and Tolerability of AMG 133 in Adult Subjects With Overweight or Obesity, With or Without Type 2 Diabetes Mellitus. (2024).Available from: https://clinicaltrials.gov/study/NCT05669599
28.
Structure Therapeutics Announces Positive Results from Phase 1b Clinical Study of Oral GLP-1 Receptor Agonist GSBR-1290 and Provides Program Update | Structure Therapeutics. Available from: https://ir.structuretx.com/news-releases/news-release-details/structure-therapeutics-announces-positive-results-phase-1b/
29.
Rivus Pharmaceuticals. Rivus Available from: https://www.rivuspharma.com/
30.
Carmot Therapeutics, Inc. A Phase 1 Randomized, Double Blind, Placebo Controlled, Study to Evaluate the Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of CT-388 in Otherwise Healthy Overweight and Obese Adult Participants and in Obese Patients With Type 2 Diabetes Mellitus. (2022).Available from: https://clinicaltrials.gov/study/NCT04838405
31.
Our Pipeline. Carmot Therapeutics. Drug Discovery and Development. Carmot Therapeutics Available from: https://carmot.us/pipeline/
32.
New Drug Development Pipeline: Pfizer's Medicine, Vaccine Discovery | Pfizer. Available from: https://www.pfizer.com/science/drug-product-pipeline
33.
AstraZeneca licenses novel agent for the treatment of cardiometabolic conditions and obesity. Available from: https://www.astrazeneca.com/media-centre/press-releases/2023/agreement-with-eccogene-for-clinical-stage-glp-1ra.html (2023).
34.
R&D pipeline. Novo Nordisk. Available from: https://www.novonordisk.com/content/nncorp/global/en/science-and-technology/r-d-pipeline.html
35.
Boye KS, Matza LS, Walter KN, Van Brunt K, Palsgrove AC, Tynan A. Utilities and disutilities for attributes of injectable treatments for type 2 diabetes. Eur. J. Health Econ. 12, 219–230 (2011).
36.
Wilding JPH, Batterham RL, Calanna S et al. STEP 1 Study Group. Once-weekly semaglutide in adults with overweight or obesity. N. Engl. J. Med. 384(11), 989–1002 (2021).
37.
Jastreboff AM, Aronne LJ, Ahmad NN et al. SURMOUNT-1 Investigators. Tirzepatide once weekly for the treatment of obesity. N. Engl. J. Med. 387(3), 205–216 (2022).
38.
A Study of Tirzepatide (LY3298176) in Participants With Obesity or Overweight With Weight Related Comorbidities (SURMOUNT-5). Available from: https://trials.lilly.com/en-US/trial/399775
39.
Wilding JPH, Batterham RL, Davies M et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes. Metab. 24, 1553–1564 (2022).
40.
Aronne LJ, Sattar N, Horn DB et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 Randomized Clinical Trial. JAMA 331, 38–48 (2024).
41.
Lipska KJ, Krumholz HM. Is hemoglobin A1c the right outcome for studies of diabetes? JAMA 317, 1017–1018 (2017).
42.
Lincoff AM, Brown-Frandsen K, Colhoun HM et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N. Engl. J. Med. 389, 2221–2232 (2023).
43.
Bril F. Semaglutide in NASH-related cirrhosis: too late to the party? Lancet Gastroenterol. Hepatol. 8, 494–495 (2023).
44.
Boye K, Ross M, Mody R, Konig M, Gelhorn H. Patients' preferences for once-daily oral versus once-weekly injectable diabetes medications: The REVISE study. Diabetes Obes. Metab. 23, 508–519 (2021).
45.
Choi J. Medicare to cover obesity drugs, but not for weight loss, The Hill (2024) Available from: https://thehill.com/policy/healthcare/4548098-medicare-obesity-drugs-weight-loss/
46.
Blankenship K. ESC: New Pfizer, BMS real-world data could boost Eliquis in Europe | Fierce Pharma Available from: https://www.fiercepharma.com/pharma/esc-pfizer-bms-eliquis-adds-to-lead-competitor-topping-french-real-world-data (2019).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 22 March 2024
Accepted: 3 May 2024
Published online: 29 May 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
First in class, best in class or a wild card: who will dominate the anti-obesity medication market?. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2024-0044
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Brian E. Roe, De gustibus est disputandum : The role of agricultural and applied economists in an era of behavior change initiatives and endogenous preferences , American Journal of Agricultural Economics, 10.1002/ajae.70049, 108, 2, (429-442), (2026).
- Livio Garattini, Antonino Mazzone, Obesity in Europe: Less impact on chronic diseases thanks to internists?, European Journal of Internal Medicine, 10.1016/j.ejim.2025.01.011, 136, (138-139), (2025).
- Livio Garattini, Giovanni Fattore, Obesity epidemic in European countries: from an unaddressed risk factor to a medicalized disease?, The European Journal of Health Economics, 10.1007/s10198-024-01752-5, 26, 1, (1-5), (2024).
- Paul Arora, Sreeram V Ramagopalan, R WE ready for reimbursement? A round up of developments in real-world evidence relating to health technology assessment: part 17, Journal of Comparative Effectiveness Research, 10.57264/cer-2024-0212, 14, 1, (2024).