Real-world evidence on the effectiveness and safety of gliclazide MR 60 mg in Bangladeshi patients with Type II diabetes during fasting: a sub-analysis from the global DIA-RAMADAN study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Many Muslims with Type II diabetes (T2DM) fast during Ramadan, which can put them at increased risk of hypoglycemia. This sub-analysis of the global DIA-RAMADAN study assessed the effectiveness and safety of gliclazide modified release (MR) 60 mg in the Bangladeshi cohort. Materials & methods: DIA-RAMADAN was an international, prospective, observational study conducted in adult T2DM patients intending to fast and receiving gliclazide MR 60 mg once daily for ≥90 days before Ramadan. Dosing was switched from morning to evening at the start of Ramadan. The primary outcome was the proportion of patients with ≥1 symptomatic hypoglycemic event. Secondary outcomes included changes between inclusion (V0) and end of study visit (V1) in glycated hemoglobin (HbA1c), body weight and fasting plasma glucose (FPG). Results: Among the 98 Bangladeshi patients, 80 (81.6%) were at moderate/low-risk (category 3) for fasting and 18 (18.4%) were high-risk (category 2), as per International Diabetes Federation and Diabetes and Ramadan International Alliance (IDF-DAR) guidelines. Gliclazide MR was being prescribed as monotherapy to 59 (60.2%) patients and in combination with metformin to 39 (39.8%). There was no incidence of severe hypoglycemic events. Mean (±SD) HbA1c change from V0 was -0.1 ± 0.8% (p = 0.159). Mean (±SD) changes in FPG and body weight were -0.8 ± 39.7 mg/dl (p = 0.876) and -0.0 ± 1.5 kg (p = 0.810), respectively. Conclusion: In a real-world setting, this sub-analysis in Bangladeshi patients shows that patients with T2DM treated with gliclazide MR 60 mg can fast safely during Ramadan with a very low risk of hypoglycemia, while maintaining glycemic control and body weight.
Tweetable abstract
A recent subanalysis of an international study shows that the sulphonylurea, gliclazide MR 60 mg, is a safe option for patients with Type II diabetes in Bangladesh who plan to fast during Ramadan.
Plain language summary
What is this article about?
Many Muslims with Type II diabetes choose to observe the religious fast during Ramadan. However, even among those with stable levels of blood glucose, the management of Type II diabetes can be challenging. With only two meals per day and no food during daylight, large swings in blood glucose levels may occur because of the long gap between meals, larger amounts of food consumed and no intake of oral antidiabetes drugs during daylight. This sub-analysis of the international DIA-RAMADAN study examined the real-world safety and effectiveness of gliclazide modified release (MR) 60 mg among fasting patients with Type II diabetes in Bangladesh.
What were the results?
The results showed that Type II diabetes in Bangladeshi patients can be safely managed during Ramadan fasting when intake of the patient's gliclazide MR dose is switched from morning to evening dosing. No severe hypoglycemic events were reported and patients maintained glycemic control with no weight changes.
What do the results of the study mean?
The gliclazide MR formulation results in gradual drug release with a low risk of hypoglycemia and is a safe option for patients who plan to fast during Ramadan.
Ramadan is the month-long (29–30 day) fast that is obligatory for all healthy Muslims who have attained puberty. The majority of Bangladeshis are Muslim and observe Ramadan fasting. In 2019, the International Diabetes Federation (IDF) estimated that 8.4 million adults were living with diabetes in Bangladesh; this number is projected to increase to 11.4 million by 2030 [1].
Ramadan is based on the lunar calendar, which is shorter than the Gregorian calendar, and occurs 10–11 days earlier every year. As a result, the length of daylight fasting varies according to the season. For example, at the height of summer, daylight can last up to 20 h in some parts of the world. In Bangladesh, climate conditions vary depending on the date of Ramadan, with people fasting in hot weather in some years and cold temperatures in others, which may influence the risk of hypoglycemia among people with Type II diabetes (T2DM).
The Ramadan fast necessitates a significant shift in everyday eating habits to an exclusively nocturnal pattern. This can be associated with physiological changes, including shifts in sleep-wake cycles, circadian rhythm, fluid and energy expenditure and glucose metabolism [2]. These alterations can stimulate or modify pathophysiological states, depending on pre-existing comorbidities and the individual's adherence to lifestyle, diet and treatment regimens [3]. Due consideration should therefore be given to type of anti-diabetes medication during this period.
Sulphonylureas are a class of oral T2DM medications that act on pancreatic beta cells to increase insulin secretion [4]. They are widely-available, safe and efficacious, and are used by many patients to control their blood sugar levels. They are associated with an increased risk of hypoglycemia compared with other oral anti-diabetes agents, which is heightened further by fasting during Ramadan, but this risk varies within the class. More recent sulphonylureas are associated with a lower risk of hypoglycemia and deemed safe for use during fasting [5–7].
Gliclazide is a newer-generation sulphonylurea available in immediate-release (IR) and modified-release (MR) formulations. Compared with other drugs in this class, the gliclazide MR formulation results in progressive drug release based on a once-daily dosing regimen, with evidence of a lower risk of hypoglycemia [8,9].
Given the altered eating habits, varying climatic conditions and modulation of human physiology during Ramadan, treatments should be selected from those with the lowest risk of hypoglycemia. Guidelines for safe fasting during Ramadan state that many patients with T2DM may continue to use newer generation sulphonylureas to manage their diabetes. The DIA-RAMADAN study was conducted to explore the real-world safety and effectiveness of gliclazide MR among fasting patients with T2DM of different ethnicity, culture, geo-environmental conditions and different lengths of daylight fasting [10]. Taking into account the important Muslim population in Bangladesh, the aim of the current subanalysis was to assess the safety and efficacy of gliclazide MR use during Ramadan in the Bangladeshi cohort of DIA-RAMADAN.
Materials & methods
Study design
The current study is a sub-analysis of DIA-RAMADAN, an international, real-world, prospective, observational study of 1244 patients with T2DM conducted at clinical centers in nine Asian, Middle-Eastern and Gulf countries (Bangladesh, India, Pakistan, Malaysia, Indonesia, Kuwait, Saudi Arabia, Egypt and the United Arab Emirates) between March 2019 and August 2019 [10]. The study was carried out following the principles of the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice guidelines. Before commencement of the study, ethical approval was obtained from the Bangladesh Medical and Research Council ([BMRC/NREC/2016-2019/933] [1–3]) and informed written consent was obtained from all the study participants. The trial was registered on ClinicalTrials.gov (NCT04132934).
In this descriptive sub-analysis data are presented for the Bangladeshi cohort who were recruited from nine different sites. As per the global DIA-RAMADAN inclusion criteria, participants were required to be adults (aged ≥18 years) with T2DM willing to fast during Ramadan, receiving a gliclazide-based regimen once daily for at least 90 days before Ramadan, with a glycated hemoglobin (HbA1c) level ≥6.5% and a BMI ≥25–≤45 kg/m2. Exclusion criteria included: requirement for insulin therapy; severe liver or renal failure; HbA1c ≥9%; previous experience of severe or repeated hypoglycemic events without a trigger factor in the year before the start of the study; and pregnancy or breastfeeding.
Study procedure
There were two visits in this real-world study. The first visit (V0) was planned 6–8 weeks before Ramadan, at which time patient eligibility criteria were assessed and baseline information collected. Patients were stratified into low/moderate, high, or very high risk of fasting during Ramadan according to International Diabetes Federation and Diabetes and Ramadan International Alliance (IDF-DAR) guidelines current at the time of the study [11]. The second visit (V1) was scheduled 4–6 weeks after Ramadan completed (Figure 1). Ramadan-focused education was provided to patients per IDF-DAR guidelines at V0 [11]. Patients were advised about changing the timing of their gliclazide MR dose during Ramadan from breakfast administration to iftar (i.e., the post-sunset meal). They were also provided with a diary to record any changes in the treatment regimen and details of any symptoms indicating hypoglycemia or other adverse events throughout the study. Treatment adherence was calculated as follows: (sum of number of intakes during Ramadan/sum of number of intakes to be taken during Ramadan) × 100 [10].
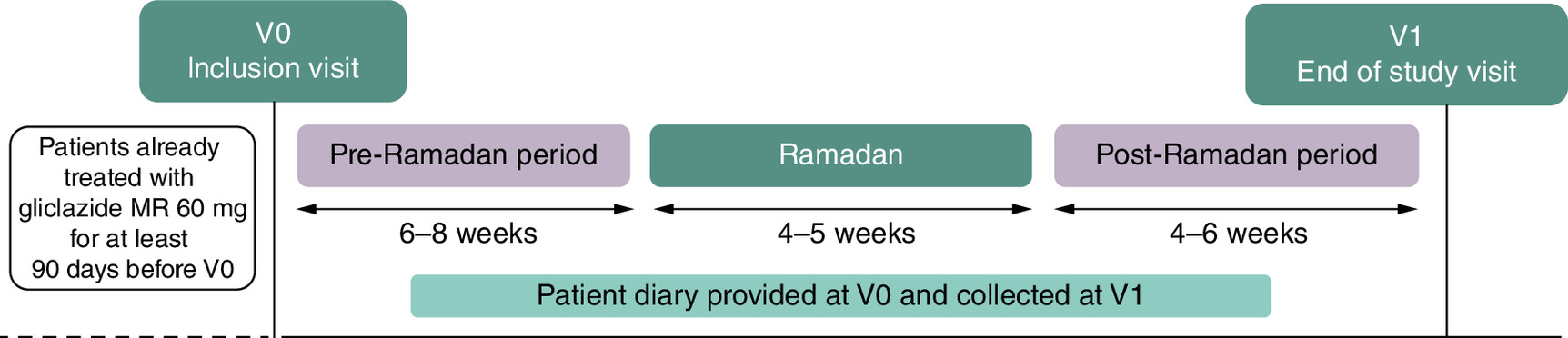
Figure 1. Study design and duration.
MR: Modified release.
Data collection & end points
Data concerning patients' anthropometric measurements, biochemical parameters, IDF-DAR risk classification [11], T2DM-related diseases and relevant medical/surgical history were recorded. The primary end point was the proportion of patients with at least one symptomatic hypoglycemic event (either suggestive or confirmed by a measured glucose concentration of ≤4 mmol/l or ≤72 mg/dl). Changes in glycated hemoglobin (HbA1c), fasting plasma glucose (FPG) levels and body weight were secondary end points. For all adverse events reported during the study, the treating physician assessed the potential relationship with the study drug, the seriousness of the reported adverse event and the clinical outcome. The definition and symptoms of hypoglycemia are summarized in Table 1.
| Type of HE | Definition | Typical hypoglycemia symptoms |
|---|---|---|
| Asymptomatic HE | Absence of typical hypoglycemia symptoms with measured glucose concentration <70 mg/dl (<3.9 mmol/l) | Sweating, pallor, tremor, intense hunger, pounding heart, visual disturbance, drowsiness, weakness, dizziness, difficulty in concentrating, difficulty in speaking or writing, incoordination, unexplained behavior or mood change, confusion, nausea, or headache |
| Suggestive HE | Presence of typical hypoglycemic symptoms without a measured glucose concentration or with measured glucose concentration >72 mg/dl (>4 mmol/l) | |
| Confirmed symptomatic HE | Presence of typical symptoms of hypoglycemia with glucose concentration ≤72 mg/dl (≤4 mmol/l) | |
| Severe hypoglycemia | Symptoms of severe cognitive impairment and requiring third-party assistance for recovery with a measured glucose concentration <70 mg/dl (<3.9 mmol/l) |
HE: Hypoglycemic event.
Data taken from [10].
Statistical analysis
Most of the statistical analysis was based on descriptive statistics. Continuous variables were expressed as mean ± standard deviation (SD). Categorical variables were expressed as frequencies and percentages. The paired Student's t-test was used to analyze differences in mean HbA1c and FPG between V0 and V1. A sign-ranked test was used to analyze the change in weight between V0 and V1. SAS software, version 9.4 or higher, was used for all analyses (SAS Institute, NC, USA). A p-value ≤0.05 was considered significant.
Results
The Bangladeshi cohort of DIA-RAMADAN comprised 98 patients. Patient demographic characteristics and medical history pre-Ramadan are summarized in Table 2. Gender distribution was approximately equal with 50 (51%) women to 48 (49%) men. Mean age of the patients was 50.7 ± 11.9 years and mean BMI 27.5 ± 2.6 kg/m2. Duration of T2DM was 5.3 ± 4.9 years, and baseline HbA1c and FPG levels were 7.4 ± 0.8% and 145.6 ± 29.6 mg/dl, respectively. Risk categorization of patients as per 2017 IDF-DAR guidelines showed that most (81.6%) patients had moderate/low risk (category 3) for hypoglycemia during Ramadan and 18.4% were at high risk (category 2). No patients belonged to the very high-risk group (category 1). The guidelines have subsequently been updated, but the majority of patients would still fall into the low or moderate risk categories with a risk score ≤6. The proportion of patients on gliclazide MR 60 mg monotherapy at V0 was 60.2%; the remainder were receiving gliclazide MR in combination with metformin. No dose modification was performed during the study. All patients who attended the inclusion visit (V0) also attended the end of the study visit (V1). Adherence to study medication during Ramadan was high: 99.8 ± 1.7%. Mean number of days fasted during Ramadan was 28.5 ± 1.3 days and mean number of h of daily fasting was 15.0 ± 0.1.
| Parameters | n = 98 |
|---|---|
| Age (years) mean (±SD) | 50.7 (11.9) |
| Age category, n (%) | |
| <50 years | 49 (50.0%) |
| ≥50 to <65 years | 37 (37.8%) |
| ≥65 years | 12 (12.2%) |
| Sex, n (%) | |
| Male | 48 (49.0%) |
| Female | 50 (51.0%) |
| Duration of T2DM (years), mean (±SD) | 5.3 (4.9%) |
| Bodyweight (kg), mean (±SD) | 68.8 (10.2) |
| BMI (kg/m2), mean (±SD) | 27.5 (2.6) |
| HbA1c (%), mean (±SD) | 7.4 (0.8) |
| FPG (mg/dl), mean (±SD) | 145.6 (29.6) |
| Arterial hypertension, n (%) | 55 (56.1%) |
| Dyslipidemia, n (%) | 38 (38.8%) |
| Type of anti-diabetic treatment | |
| Gliclazide MR alone, n (%) | 59 (60.2%) |
| Gliclazide MR+ Metformin, n (%) | 39 (39.8%) |
| Dose of gliclazide MR (mg), mean (±SD) | 60.0 (0.0) |
| Dose of metformin (mg), mean (±SD) | 952.1 (437.3) |
| IDF-DAR risk category, n (%) | |
| Category 1 (very high risk) | 0 (0.0%) |
| Category 2 (high risk) | 18 (18.4%) |
| Category 3 (low risk/moderate risk) | 80 (81.6%) |
FPG: Fasting plasma glucose; HbA1c: Glycosylated hemoglobin; MR: Modified release; SD: Standard deviation.
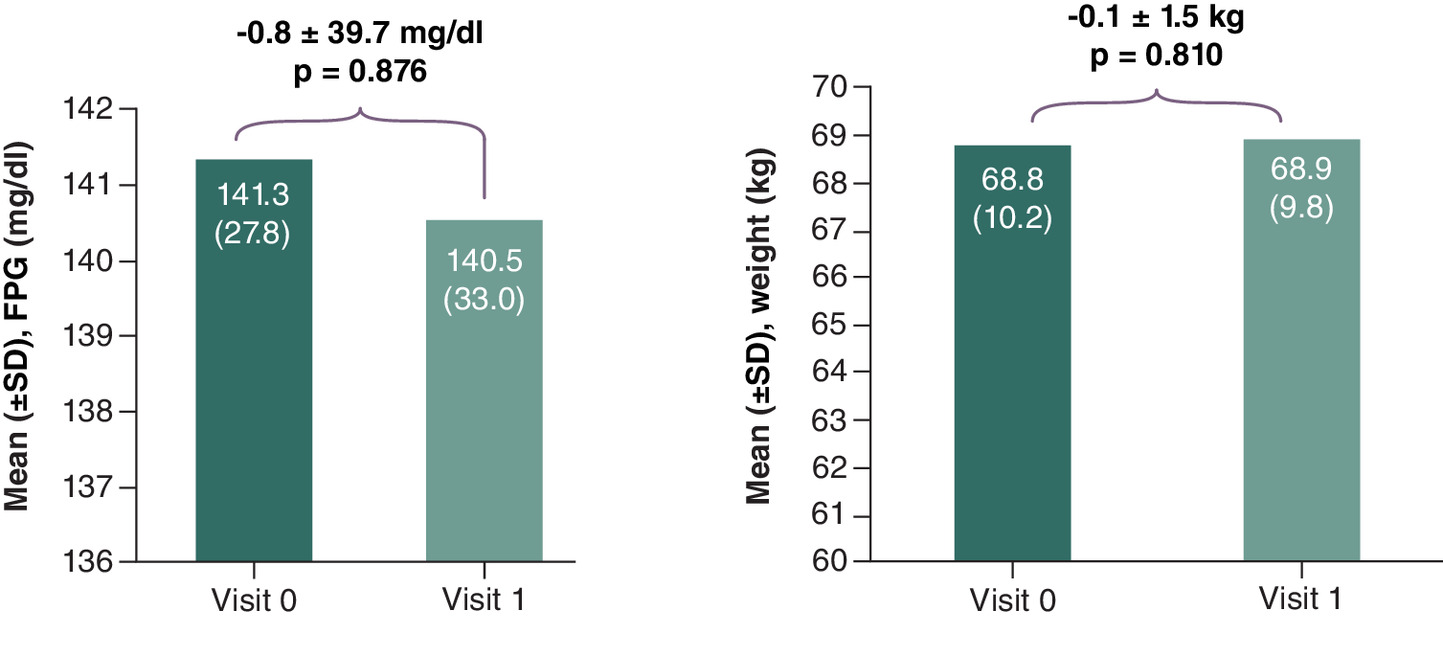
The mean (±SD) HbA1c change from V0 to V1 was -0.1 ± 0.8% (p = 0.159). When analyzed by age group, a decrease of -0.3 ± 0.8% (p = 0.043) was observed in the ≥50 to <65 year age group (n = 37), but changes did not achieve statistical significance in the other age groups (Table 3). Mean (±SD) FPG change was -0.8 ± 39.7 mg/dl (p = 0.876) and no impact on mean weight change was reported (0.1 ± 1.5 kg (p = 0.810) (Figure 2).
| Age group (years) | Pre-Ramadan HbA1c | Post-Ramadan HbA1c | Change | p-value |
|---|---|---|---|---|
| <50 (n = 49) | 7.4 (0.7) | 7.3 (0.9) | -0.1 (0.8) | 0.641 |
| ≥50 to <65 (n = 37) | 7.5 (0.9) | 7.2 (0.8) | -0.3 (0.8) | 0.043 |
| ≥65 (n = 12) | 7.2 (0.3) | 7.3 (1.5) | 0.0 (1.3) | 0.990 |
The p-value in bold is statistically significant.
There were no incidences of severe hypoglycemia. Only two patients developed symptomatic hypoglycemia, which developed near the end of the day. The patients continued fasting until iftar as usual. Both patients were less than 50 years of age, at low/moderate risk for fasting during Ramadan, and were receiving gliclazide MR in combination with metformin. HbA1c at baseline was less than 7.5% in one patient, and between 7.5–≤8% in the other. Both were also suffering from acute gastroenteritis.
Discussion
This sub-analysis of Bangladeshi patients with T2DM participating in the DIA-RAMADAN study indicates that gliclazide MR, either as monotherapy or in combination with metformin, is a suitable sulphonylurea for use during Ramadan in routine clinical practice. Despite a prolonged period of fasting (mean of 28.5 days and 15.0 h/day) there were no cases of severe hypoglycemia and only two (2%) patients reported symptomatic hypoglycemia. As the latter also developed acute gastroenteritis, the hypoglycemic events may not have been attributable to gliclazide MR alone. These results are in line with those of the global DIA-RAMADAN study which also reported that 2.2% of patients experienced symptomatic hypoglycemia during Ramadan (27 out of 1214 patients with at least one confirmed or suggestive hypoglycemic event) [10].
The sulphonylureas have undergone several stages of development since the first agent became available more than 60 years ago. While they all share the same general mechanism of action, their pharmacokinetic properties are influenced by factors such as tissue specificity and binding affinity for the pancreatic β-cell receptor, rate of absorption, duration of action and route of elimination [12]. The resulting differences in pharmacokinetic profiles instil the sulphonylureas with varying levels of hypoglycemic risk [13]. The risk of hypoglycemia is lower with agents such as gliclazide MR because of its reversible and specific binding affinity to sulphonylurea receptors (SUR1) on pancreatic beta cells and neutral effect on exchange protein directly activated by cAMP 2 (Epac2), activation of which contributes to the potentiation of glucose-stimulated insulin secretion [13,14]. Gliclazide is also broken down to inactive metabolites and the modified release formulation allows a gradual increase in drug plasma concentrations.
Several studies in T2DM patients have reported that among the sulphonylureas, gliclazide has one of the lowest risks of hypoglycemia [15–17]. Gliclazide MR is also associated with low rates of hypoglycemia in Muslim T2DM patients fasting during Ramadan [5,7,18–22].
In an observational study among patients with T2DM (age ≥18 years) from five countries (n = 1378) which assessed the incidence of symptomatic hypoglycemia during Ramadan, gliclazide MR was associated with the lowest incidence, reported in 14% of patients, compared with 17% for glimepiride, 26% for glibenclamide and 28% for glipizide [23].
An observational study assessing the effect of switching from a morning to evening administration of gliclazide MR 60 mg during Ramadan, conducted among male T2DM patients (n = 136) recruited from Bangladesh, India and Pakistan, showed that there was no increase in hypoglycemia risk, and that the patients could safely maintain their glycemic control with administration of gliclazide MR 60 mg at iftar during the Ramadan fast [24].
A 2015 meta-analysis by Mbanya et al. found no difference in hypoglycemic risk potential between gliclazide- and DPP-4-inhibitor-treated patients who were observing Ramadan fasting (7.2% vs 5.6%, risk ratio 1.12, 95% CI 0.73-1.73, p = 0.61) [25].
During the pre-Ramadan visit, 18% of Bangladeshi patients were categorized as high risk (risk score >6) by the IDF-DAR risk assessment [11]. Despite this, none of these high-risk patients developed hypoglycemia, which may reflect the level of pre-Ramadan education and counselling provided. A previous study evaluating the efficacy of a pre-Ramadan structured educational program for patients with diabetes noted a significant reduction in the risk of hypoglycemia (by up to 50%), leading the authors to conclude that adequate education and counselling are critical factors for reducing hypoglycemic episodes [26]. A systematic review and meta-analysis to assess the effect of Ramadan-focused diabetes education on hypoglycemia risk also found a substantial reduction in risk of hypoglycemia (81% reduction) among fasting patients receiving education compared with those on conventional care alone [27].
In the current study, changes in HbA1c and FPG levels and body weight were non-significant, consistent with findings from other studies with sulphonylureas during Ramadan. A multicenter observational study in Indian Muslims with T2DM found that patients treated with sulphonylureas had a non-significant increase in HbA1c (0.01%, p = 0.958) and a decrease in mean FPG (20 mg/dl) after Ramadan [28]. The STEADFAST study (n = 557), which was conducted during Ramadan in 16 countries, including Asia, Europe and the Middle East, observed similar changes in HbA1c with vildagliptin and gliclazide (0.05 ± 0.04% vs 0.03 ± 0.04%, p = 0.165), as well as a mean weight reduction of -1.1 ± 0.2 kg (p = 0.987) in both treatment groups [18].
The adherence of the Bangladeshi patients to treatment was high with all reporting that they took their medication regularly throughout Ramadan as prescribed by their physician with no self-modifications to dose. All were taking gliclazide MR at the 60 mg dose and did not require any dose adjustments during or after Ramadan, suggesting that they were adhering to their treatment regimen. Together, these findings indicate that patients on gliclazide MR can control blood sugar levels and maintain body weight with a low risk of hypoglycemia without modifying their gliclazide dose during Ramadan fasting.
Limitations of this sub-analysis were those associated with its observational and uncontrolled design and small sample size. This study provides real-world evidence from physicians treating fasting T2DM patients according to standard clinical practice in Bangladesh, for which data are lacking in the published literature. One of the strengths of the study was that hypoglycemia was recorded using self-reported patient diaries, allowing all hypoglycemic or other adverse events to be captured and reported to treating physicians during the study.
Conclusion
This sub-analysis of Bangladeshi patients with T2DM from the DIA-RAMADAN study provides real-world data for the effectiveness and safety of gliclazide MR 60 mg to control blood glucose during fasting. The majority of patients had low-to-moderate risk for hypoglycemia during Ramadan. Consistent with the global DIA-RAMADAN findings, switching the morning gliclazide MR dose to iftar during Ramadan fasting was associated with a very low risk of hypoglycemia, while maintaining glycemic control and with a neutral effect on body weight. Gliclazide MR 60 mg is a safe option for patients who plan to fast during Ramadan.
Summary points
•
Management of Type II diabetes among people observing the Ramadan fast is challenging due to disrupted eating patterns, particularly in hot climates.
•
This sub-analysis of the international DIA-RAMADAN study confirms that Type II diabetes in Bangladeshi patients can be safely managed during Ramadan fasting when gliclazide 26% for modified release glibenclamide administration is switched from morning to evening dosing. No severe hypoglycemic events were reported and patients maintained glycemic control with no weight changes.
Author contributions
M Ahamed Khan wrote the manuscript and acted as a co-investigator. M Farid Uddin worked as principal investigator, reviewing and editing the manuscript. All other authors served as co-investigators and approved the final manuscript for publication.
Acknowledgments
The authors gratefully acknowledge the International Centre for Diarrheal Disease Research, Bangladesh (ICDDR, B) for its contribution as contract research organization. The authors also express gratitude to the patients, their families and the staff at the study sites.
Financial disclosure
This study was sponsored by Servier (Servier Affaires Medicals). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Writing disclosure
Medical writing support was provided by Servier Affaires Medicals.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. Deidentified, individual data that underlie the results reported in this article are available from the corresponding author upon reasonable request. The study protocol is available on ClincalTrials.gov (NCT04132934).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Saeedi P, Petersohn I, Salpea P et al. IDF Diabetes Atlas Committee. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 157, 107843 (2019).
2.
Bahammam A, Alrajeh M, Albabtain M, Bahammam S, Sharif M. Circadian pattern of sleep, energy expenditure, and body temperature of young healthy men during the intermittent fasting of Ramadan. Appetite 54(2), 426–429 (2010).
3.
Gibney ER. Energy expenditure in disease: time to revisit? Proc. Nutr. Soc. 59(2), 199–207 (2000).
4.
Sola D, Rossi L, Schianca GP et al. Sulfonylureas and their use in clinical practice. Arch. Med. Sci. 11(4), 840–848 (2015).
5.
Al Sifri S, Basiounny A, Echtay A et al. 2010 Ramadan Study Group. The incidence of hypoglycaemia in Muslim patients with Type II diabetes treated with sitagliptin or a sulphonylurea during Ramadan: a randomised trial. Int. J. Clin. Pract. 65(11), 1132–1140 (2011).
6.
Al-Arouj M, Hassoun AA, Medlej R et al. The effect of vildagliptin relative to sulphonylureas in Muslim patients with Type II diabetes fasting during Ramadan: the VIRTUE study. Int. J. Clin. Pract. 67(10), 957–963 (2013).
7.
Aravind SR, Ismail SB, Balamurugan R et al. Hypoglycemia in patients with Type II diabetes from India and Malaysia treated with sitagliptin or a sulfonylurea during Ramadan: a randomized, pragmatic study. Curr. Med. Res. Opin. 28(8), 1289–1296 (2012).
8.
Avogaro A. Treating diabetes today with gliclazide MR: a matter of numbers. Diabetes Obes. Metab. 14(Suppl. 1), 14–19 (2012).
9.
Schernthaner G, Grimaldi A, Di Mario U et al. GUIDE study: double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients. Eur. J. Clin. Invest. 4(8), 535–542 (2004).
• A head-to-head comparison of gliclazide MR and glimepiride confirmed similar decreases in HbA1c, but 50% fewer hypoglycemic episodes with gliclazide MR.
10.
Hassanein M, Al Sifri S, Shaikh S et al. DIA-RAMADAN study investigators. A real-world study in patients with Type II diabetes mellitus treated with gliclazide modified-release during fasting: DIA-RAMADAN. Diabetes Res. Clin. Pract. 163, 108154 (2020).
•• The main DIA-RAMADAN study was an international observational study and one of the first to demonstrate the safety and effectiveness of gliclazide MR treatment during a period of religious Muslim fasting in a real-world setting.
11.
Hassanein M, Al-Arouj M, Hamdy O et al. International Diabetes Federation (IDF), in collaboration with the Diabetes and Ramadan (DAR) International Alliance. Diabetes and Ramadan: practical guidelines. Diabetes Res. Clin. Pract. 126, 303–316 (2017).
• Evidence-based practice guidelines developed to assist healthcare providers deliver the best possible care and support to patients with diabetes choosing to fast during Ramadan.
12.
Harrower AD. Comparison of diabetic control in type 2 (non-insulin dependent) diabetic patients treated with different sulphonylureas. Curr. Med. Res. Opin. 9(10), 676–680 (1985).
13.
Colagiuri S, Matthews D, Leiter LA, Chan SP, Sesti G, Marre M. The place of gliclazide MR in the evolving Type II diabetes landscape: a comparison with other sulfonylureas and newer oral antihyperglycemic agents. Diabetes Res. Clin. Pract. 143, 1–14 (2018).
• A review of currently available sulphonylureas examining differences in efficacy and durability, weight changes, hypoglycemia, renal effects and cost.
14.
Seino S, Takahashi H, Takahashi T, Shibasaki T. Treating diabetes today: a matter of selectivity of sulphonylureas. Diabetes Obes. Metab. 14(Suppl. 1), 9–13 (2012).
15.
Chan SP, Colagiuri S. Systematic review and meta-analysis of the efficacy and hypoglycemic safety of gliclazide versus other insulinotropic agents. Diabetes Res. Clin. Pract. 110(1), 75–81 (2015).
16.
Harrower AD. Comparison of efficacy, secondary failure rate, and complications of sulfonylureas. J. Diabetes Complications 8(4), 201–203 (1994).
17.
Harrower AD, Wong C. Comparison of secondary failure rate between three second-generation sulphonylureas. Diabetes Res. 13(1), 19–21 (1990).
18.
Hassanein M, Abdallah K, Schweizer A. A double-blind, randomized trial, including frequent patient-physician contacts and Ramadan-focused advice, assessing vildagliptin and gliclazide in patients with Type II diabetes fasting during Ramadan: the STEADFAST study. Vasc. Health Risk. Manag. 10, 319–326 (2014).
•• A double-blind randomized study of vildagliptin versus gliclazide in patients with Type II diabetes fasting during Ramadan. The results showed a similar low rate of hypoglycemic events in both treatment groups.
19.
Brady EM, Davies MJ, Gray LJ et al. A randomized controlled trial comparing the GLP-1 receptor agonist liraglutide to a sulphonylurea as add on to metformin in patients with established Type II diabetes during Ramadan: The Treat 4 Ramadan Trial. Diabetes Obes. Metab. 16(6), 527–536 (2014).
20.
Sadikot S, Jothydev K, Zargar AH, Ahmad J, Arvind SR, Saboo B. Clinical practice points for diabetes management during RAMADAN fast. Diabetes Metab. Syndr. 11(Suppl. 2), S811–S819 (2017).
21.
Rashid F, Abdelgadir E. A systematic review on efficacy and safety of the current hypoglycemic agents in patients with diabetes during Ramadan fasting. Diabetes Metab. Syndr. 13(2), 1413–1429 (2019).
22.
Shiju R, Akhil A, Thankachan S, Tuomilehto J, Al Arouj M, Bennakhi A. Safety assessment of glucose-lowering drugs and importance of structured education during Ramadan: a systematic review and meta-analysis. J. Diabetes Res. 2022, 3846253 (2022).
23.
Aravind SR, Al Tayeb K, Ismail SB et al. 2009 Ramadan Study Group. Hypoglycaemia in sulphonylurea-treated subjects with Type II diabetes undergoing Ramadan fasting: a five-country observational study. Curr. Med. Res. Opin. 27(6), 1237–1242 (2011).
24.
Zargar AH, Siraj M, Jawa AA, Hasan M, Mahtab H. Maintenance of glycaemic control with the evening administration of a long acting sulphonylurea in male type 2 diabetic patients undertaking the Ramadan fast. Int. J. Clin. Pract. 64(8), 1090–1094 (2010).
25.
Mbanya JC, Al-Sifri S, Abdel-Rahim A, Satman I. Incidence of hypoglycemia in patients with Type II diabetes treated with gliclazide versus DPP-4 inhibitors during Ramadan: a meta-analytical approach. Diabetes Res. Clin. Pract. 109(2), 226–232 (2015).
• A pooled analysis of three trials showing no significant difference in the incidence of symptomatic hypoglycemic events in patients fasting during Ramadan treated with either a DPP-4 inhibitor or gliclazide.
26.
Mohamed OM, Hassanein M, Syeed A et al. Impact of pre-Ramadan intervention program on diabetic patients (PRINTED 1): a randomised controlled trial in a family medicine clinic-Abu Dhabi. Middle East J. Fam. Med. 10, 10 (2019).
27.
Tourkmani AM, Abdelhay O, Alharbi TJ et al. Impact of Ramadan-focused diabetes education on hypoglycemia risk and metabolic control for patients with Type II diabetes mellitus: a systematic review. Int. J. Clin. Pract. 75(3), e13817 (2021).
28.
Shete A, Shaikh A, Nayeem KJ et al. Vildagliptin vs sulfonylurea in Indian Muslim diabetes patients fasting during Ramadan. World J. Diabetes 4(6), 358–364 (2013).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 August 2023
Accepted: 23 November 2023
Published online: 31 January 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world evidence on the effectiveness and safety of gliclazide MR 60 mg in Bangladeshi patients with Type II diabetes during fasting: a sub-analysis from the global DIA-RAMADAN study. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0132
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Toka Elemary, Mohamed E. A. Abdelrahim, Mina Nicola, Dalia Zaafar, Therapeutic impact of vildagliptin vs. gliclazide on insulin resistance and advanced glycated end product levels in newly diagnosed Egyptian diabetics: a randomized controlled trial, European Journal of Clinical Pharmacology, 10.1007/s00228-025-03894-8, 81, 11, (1593-1608), (2025).
- Salem A. Beshyah, Khadija Hafidh, Hussam Abusahmin, Diabetes and Ramadan Fasting (2024): A Thematic Overview, Journal of Diabetes and Endocrine Practice, 10.1055/s-0045-1809319, 08, 03, (157-165), (2025).