Assessment of second primary malignancies among treated and untreated patients with chronic lymphocytic leukemia using real-world data from the USA
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Improved management of chronic lymphocytic leukemia (CLL) has resulted in a growing population of CLL survivors; these patients have a higher risk of developing second primary malignancies (SPMs) versus the general population. This retrospective cohort study aims to assess the timing, frequency, incidence and types of SPMs in treated and untreated patients with CLL in the USA, using the Surveillance, Epidemiology, and End Results (SEER) Medicare database, which links a nationally representative cancer registry with Medicare claims data. Patients & methods: Patients aged ≥66 years with newly diagnosed CLL between 1 January 2010 and 31 December 2016, who were enrolled in Parts A and B of Medicare for ≥12 months pre-diagnosis of CLL were selected from the database. Patients were assessed for ≥36 months until the end of continuous enrollment in Medicare Parts A, B and D, a switch to a health maintenance organization, death, or end of the study period (December 2019). Results: Of 3053 patients included in the analyses, 620 (20.3%) were treated and 2433 (79.7%) were untreated within 36 months of diagnosis. Overall, 638 (20.9%) patients developed a SPM, 26.8% of patients in the treated cohort and 19.4% of patients in the untreated cohort. The most common SPMs for both cohorts were squamous cell carcinoma and acute myeloid leukemia. Among the 166 treated patients who developed a SPM, a greater proportion developed their first SPM after treatment initiation versus those who developed their first SPM prior to treatment initiation (p < 0.001). A significantly lower percentage of patients who received targeted therapy developed a SPM (p < 0.05) versus patients treated with anti-CD20 + chemotherapy. Conclusion: Findings indicate that treatment type and timing can affect SPM development in patients with CLL. Combined with previous findings, this can help inform best practices in monitoring for SPM in patients with CLL.
Plain language summary
Second primary cancers in both treated & untreated patients with chronic lymphocytic leukemia in the USA
What is this article about?
This study looks at how many patients aged 66 years or over and diagnosed with chronic lymphocytic leukemia (CLL; a type of blood cancer) between 1 January 2010 and 31 December 2016 also had second primary cancers (a new type of cancer that occurs in someone who has had cancer before). Patient information was taken from the Surveillance, Epidemiology, and End Results (SEER)-Medicare database and looked at patients within the USA.
What do the results mean?
More patients with CLL had a second primary cancer if they received treatment compared with those who did not receive treatment. More patients had their first second primary cancer after receiving treatment versus before receiving treatment. This shows that second primary cancers can be linked to treatment. The speed at which second primary cancers developed and the number of second primary cancers was different depending on what type of treatment was received.
This study gives an overview of second primary cancers in patients with CLL and the link between them and treatments for CLL. In addition, the study can be used along with other previously published data to help healthcare providers monitor for second primary cancers when treating their patients with CLL.
Improvements in the management of chronic lymphocytic leukemia (CLL), the most frequently diagnosed leukemia among adults in the western world, have resulted in a growing population of CLL survivors [1,2]. The emergence of targeted therapies for treatment of CLL (including acalabrutinib, ibrutinib, zanubrutinib and idelalisib [all administered as continuous treatment until disease progression or unacceptable toxicity], and venetoclax [a fixed-duration treatment regimen]) has improved clinical outcomes compared with standard chemotherapy and chemoimmunotherapy treatments and has changed clinical practice [3–5]. Retrospective studies have indicated that patients with CLL have a higher risk of developing second primary malignancies (SPMs), both hematologic and solid organ, compared with the general population [6–8]. It is possible that this is influenced by immunodeficiency related to CLL and/or standard treatments for CLL [9,10].
Although clinical trials often exclude patients with SPMs, some have assessed the frequency of and contributing factors for SPMs among patients treated with chemoimmunotherapy. For instance, analyses from four phase II/III trials found that age (>65 years), male sex, comorbidities, and ≥1 subsequent treatments were all associated with an adverse effect on SPM-free survival [11]. Similarly, a retrospective study of bruton tyrosine kinase inhibitors (BTK), ibrutinib and acalabrutinib, indicated that smoking was associated with a higher SPM risk, while a high CD8 count at baseline was associated with a lower SPM risk. However, no association was found between prior lines of treatment and overall SPM incidence, and no difference in SPM incidence was observed between patients treated with ibrutinib and those treated with acalabrutinib [12]. Most retrospective studies, however, have not assessed whether the risk of developing SPMs is affected by type of therapy and especially if novel targeted agents have changed that risk, highlighting an area which requires further research.
Although a retrospective cohort study of patients with CLL (n = 265), managed at a large tertiary care center between 1994 and 2018, did not observe any differences in the cumulative incidence of SPMs in patients receiving chemotherapy versus chemoimmunotherapy versus targeted therapy [13], a more up to date population-based assessment would be beneficial considering the growing use of targeted therapies in recent years, especially at a community level. Thus, this study aims to assess the incidence, timing, frequency, and types of SPMs in treated and untreated patients with CLL, using population-based data from the USA.
Patients & methods
This retrospective cohort study evaluated data from the Surveillance, Epidemiology, and End Results (SEER)/SEER-Medicare database, which links a cancer registry with claims data from Medicare (a health insurance program, that in 2010 insured ~94% of the US population aged ≥65 years [14]), thus providing additional data on cancer-directed therapies, and treatments patients have received. There are four parts of Medicare: Part A provides inpatient/hospital coverage (including inpatient hospital stays, skilled nursing facility stays and hospice care); Part B provides outpatient/medical coverage (including physician visits, outpatient services and preventative services); Part C offers an alternate way to receive Medicare benefits by joining a privately managed care plan (such as a health maintenance organization or preferred provider organization); and Part D provides prescription drug coverage. Patients aged ≥66 years with newly diagnosed CLL (ICD-9: 204.1, ICD-10: C83.0, C91.10 and ICD-O-3: 9823/3) between 1 January 2010 and 31 December 2016 who were enrolled in Parts A and B of Medicare (and were not in a Health Maintenance Organization health plan) for ≥12 months pre-diagnosis of CLL were selected. Patients were assessed for ≥36 months post-diagnosis through to the end of continuous enrollment in Medicare Parts A, B and D, a switch to a Health Maintenance Organization, death, or end of the study period (December 2019; Supplementary Figure 1). This study was reviewed by Western Institutional Review Board-Copernicus Group (WCG® IRB) and received an institutional review board exemption and waiver of Health Insurance Portability and Accountability Act of 1996 (HIPAA) authorization.
Patients were excluded if CLL was not the primary (initially diagnosed) malignancy, if the SPM was diagnosed within 2 months post-CLL diagnosis, in alignment with the Kumar 2019 study [9] to avoid or mitigate ascertainment bias, and if the primary payer was TRICARE, Military or Veterans Affairs at diagnosis. Further exclusion criteria included enrollment in a clinical trial during the study period, cancer cases occurring in Hawaii (due to masking of Hawaii vital statistics for our data delivery of the SEER-Medicare database), diagnosis at death or autopsy from SEER data, and disagreement between SEER and Medicare for the date of death or birth.
Patients were defined as untreated or treated based on procedures and/or drug codes for CLL treatments (Supplementary Table 1) up to 36 months post diagnosis. Demographic and clinical characteristics were assessed either at CLL diagnosis or in the 12 months prior to CLL diagnosis (this long time-window allows us to assess characteristics which may not be available in Medicare claims data at the exact day of diagnosis) and analyzed by descriptive statistics. Notably, numbers less than 11 (and percentages or other mathematical formulas that could allow the derivation of patient, facility or provider counts less than 11) are suppressed to prevent patients or providers from being identified, as per the compliance agreement with SEER-Medicare database providers. SPMs were defined as having an inpatient diagnosis code for a hematologic (excluding CLL) or solid tumor malignancy, or two outpatient codes at least 30 days apart (Supplementary Table 2); the SPM development date would be defined as the first of the two dates. Non-Hodgkin lymphoma (NHL) was excluded as a SPM for the main analysis, due to the potential diagnostic overlap between CLL and NHL (guided by the analysis for hematologic SPMs excluding NHL in a prior SEER database study [9]); results including NHL as a SPM were assessed in a sensitivity analysis.
Timing of SPM development, types of SPMs and SPM incidence rates were evaluated for the overall cohort, by treatment status, by treatment groups, and relative to diagnosis or treatment initiation. Time from diagnosis to SPM was analyzed using Kaplan–Meier curves. While all patients had a diagnosis date, only treated patients had a treatment initiation date. It could be possible that treated patients developed SPMs prior to their treatment initiation, but by grouping patients by treatment status, these SPMs would be attributable to treatment. To better compare SPM rates between treated and untreated cohorts and by treatment groups relative to treatment initiation, a 1:1 propensity score match using nearest-neighbor matching based on demographic and clinical characteristics (age, sex, race, year of diagnosis, advanced state and non-cancer Charlson Comorbidity Index [CCI; non-cancer CCI is a modified version that excludes the cancer diagnosis from the algorithm to obtain a measure of each patient's overall baseline comorbidity burden at the time of diagnosis]) was performed (an approach used in previous publications to address immortal time bias [15–19]). After matching, the covariate balance between the treated and untreated within 36 months subgroups is improved (Supplementary Figure 2). Once an untreated patient was matched to a treated patient, the duration from diagnosis to treatment for the matched treated patient was added to the date of diagnosis for the untreated patient. This resulted in a “pseudo”-treatment initiation date (Supplementary Figure 1).
Results
Overall, 32,197 patients with a newly diagnosed primary CLL malignancy between 1 January 2010 and 31 December 2016 were identified from the SEER-Medicare database. A total of 3053 patients met the inclusion criteria for this study and were included in the analyses (Figure 1); 620 (20.3%) patients were treated, and 2433 (79.7%) patients were untreated within 36 months of diagnosis (Table 1). The median age of patients was 75.0 years for both the treated and untreated cohort, most patients were white (92.6% for the treated and 92.4% for the untreated cohort), and both cohorts had generally similar non-cancer CCI and CCI. Mean follow-up for the 3053 patients in the study was 67.6 months (standard deviation: 22.4).
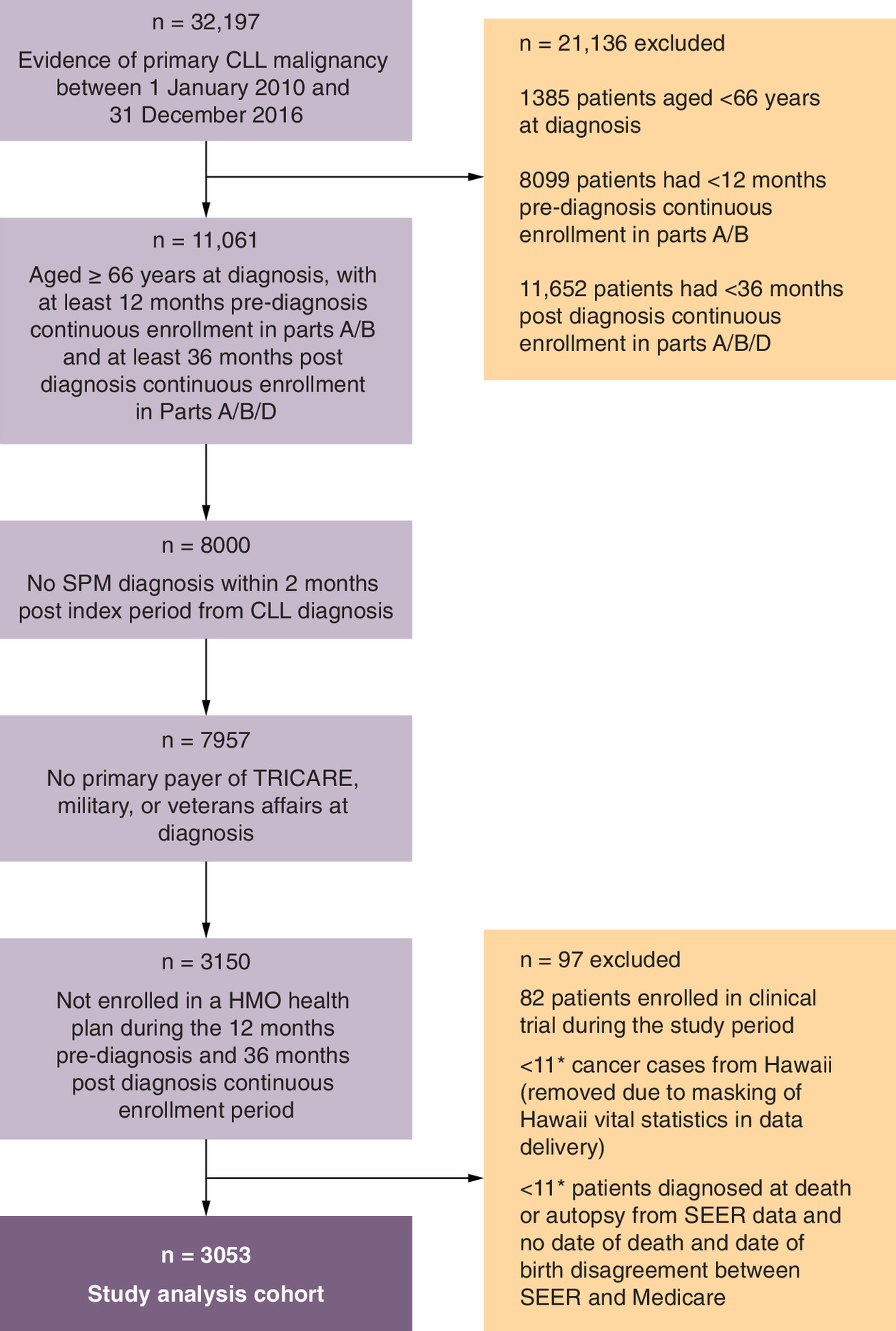
Figure 1. Patient attrition.
*Per the SEER-Medicare data use agreement and the Research Data Assistance Center CMS cell size suppression policy, any instances where there are fewer than 11 patients for a particular characteristic or variable have been described as such to eliminate potential patient re-identification.
CLL: Chronic lymphocytic leukemia; HMO: Health Maintenance Organization; ICD: International Classification of Diseases; SEER: Surveillance, Epidemiology, and End Results; SPM: Second primary malignancy.
| Characteristic | Treated within 36 months post diagnosis (n = 620) | Untreated within 36 months post diagnosis (n = 2433) |
|---|---|---|
| Age at CLL diagnosis, years Mean (SD) Median (Q1, Q3) | 75.8 (6.7) 75.0 (70.0, 80.0) | 76.5 (7.1) 75.0 (71.0, 82.0) |
| Race, n (%) White Black Asian or Pacific Islander Other | 574 (92.6) 29 (4.7) <11 (<1.8)† <11 (<1.8)† | 2249 (92.4) 48 (2.0) 32 (1.3) 104 (4.3) |
| Sex, n (%) Male Female | 346 (55.8) 274 (44.2) | 1182 (48.6) 1251 (51.4) |
| Year of CLL diagnosis, n (%) 2010 2011 2012 2013 2014 2015 2016 | 56 (9.0) 70 (11.3) 64 (10.3) 83 (13.4) 107 (17.3) 103 (16.6) 137 (22.1) | 255 (10.5) 258 (10.6) 309 (12.7) 357 (14.7) 392 (16.1) 400 (16.4) 462 (19.0) |
| Time to first treatment, months Mean (SD) Median (Q1, Q3) Untreated during full study period, n (%) | 15.0 (11.5) 13.9 (3.6, 25.0) 0 (0) | 55.0 (15.9) 51.0 (42.4, 63.0) 2128 (87.5) |
| Advanced stage‡, n (%) | 228 (36.8) | 709 (29.1) |
| Non-cancer CCI Mean (SD) Median (Q1, Q3) | 1.6 (1.8) 1.0 (0.0, 2.0) | 1.6 (1.8) 1.0 (0.0, 3.0) |
| CCI category, n (%) ≥2 categories Myocardial infarction Congestive heart failure Peripheral vascular disease Cerebrovascular disease Dementia Chronic pulmonary disease Rheumatic disease Peptic ulcer disease Mild liver disease Diabetes without chronic complications Diabetes with chronic complications Hemiplegia Renal disease Moderate or severe liver disease Metastatic solid tumor HIV/AIDS | 241 (38.9) 24 (3.9) 60 (9.7) 97 (15.6) 89 (14.4) 14 (2.3) 145 (23.4) 44 (7.1) <11 (<1.8)† 37 (6.0) 14 (2.3) 126 (20.3) <11 (<1.8)† 63 (10.2) 0 (0) <11 (<1.8)† <11 (<1.8)† | 1027 (42.2) 116 (4.8) 239 (9.8) 439 (18.0) 334 (13.7) 75 (3.1) 528 (21.7) 127 (5.2) 31 (1.3) 158 (6.5) 47 (1.9) 535 (22.0) 30 (1.2) 235 (9.7) <11 (<0.5)† 19 (0.8) <11 (<0.5)† |
†
Per the SEER-Medicare data use agreement and the Research Data Assistance Center CMS cell size suppression policy, any instances where there are fewer than eleven patients for a particular characteristic or variable have been described as such to eliminate potential patient re-identification.
‡
Advanced disease was defined as a diagnosis of thrombocytopenia or anemia at baseline.
CCI: Charlson Comorbidity Index; CCL: Chronic lymphocytic leukemia; HIV/AIDS: Human immunodeficiency virus infection/acquired immunodeficiency syndrome; Q: Quartile; SD: Standard deviation.
Median time to first treatment was 13.9 months in the treated cohort; in the untreated cohort, 12.5% of patients received treatment at a median of 51.0 months following CLL diagnosis. Among those treated within 36 months post diagnosis (where patients may have received multiple treatments), the first treatment after diagnosis was anti-CD20 monotherapy (rituximab, obinutuzumab, or ofatumumab) for 22.1% of patients, anti-CD20 + chemotherapy for 44.8% of patients, targeted oral agents (ibrutinib [a BTK inhibitor] and venetoclax [a B-cell lymphoma 2 (BCL-2) inhibitor]) as either monotherapy or combination therapy (venetoclax + rituximab, ibrutinib + rituximab or ibrutinib + obinutuzumab) for 19.7% of patients (<11 patients had combination therapy; <11 patients received venetoclax) and other treatments (bendamustine, chlorambucil, cyclophosphamide, fludarabine, lenalidomide or stem cell transplant) for 13.7% of patients.
Overall, 20.9% (638/3053) of patients developed at least one SPM; 26.8% (166/620) of patients in the treated cohort and 19.4% (472/2433) of patients in the untreated cohort (Table 2). In the treated cohort, 22.3% (37/166) of patients developed ≥2 SPMs, while 14.2% (67/472) of patients developed ≥2 SPMs in the untreated cohort (Table 2). Similarly, the sensitivity analysis, that included NHL as a SPM, observed SPMs in 39.2% (243/620) of patients in the treated cohort and 23.3% (568/2433) of patients in the untreated cohort. The most common SPMs for both the treated and untreated cohorts were squamous cell carcinoma (related to skin), acute myeloid leukemia (AML), acute lymphocytic leukemia (ALL), prostate cancer, lung adenocarcinoma and chronic myeloid leukemia (CML; Table 3).
| Treated within 36 months post diagnosis (n = 620) | Untreated within 36 months post diagnosis (n = 2433) | |
|---|---|---|
| Patients with CLL developing a SPM, n (%) | 166 (26.8) | 472 (19.4) |
| 1 SPM | 129/166 (77.7) | 405/472 (85.8) |
| ≥2 SPMs | 37/166 (22.3) | 67/472 (14.2) |
| Total SPMs developed, n | 218 | 544 |
CLL: Chronic lymphocytic leukemia; SPM: Secondary primary malignancy.
| SPMs, n (%)† | Treated within 36 months post diagnosis (n = 218) | Untreated within 36 months post diagnosis (n = 544) |
|---|---|---|
| Squamous cell carcinoma | 52 (23.9) | 94 (17.3) |
| Acute myeloid leukemia | 39 (17.9) | 147 (27.0) |
| Acute lymphocytic leukemia | 21 (9.6) | 37 (6.8) |
| Prostate cancer | 18 (8.3) | 39 (7.2) |
| Lung adenocarcinoma | 13 (6.0) | 48 (8.8) |
| Chronic myeloid leukemia | 11 (5.0) | 28 (5.1) |
| Other SPMs | 64 (29.4) | 151 (27.8) |
†
Patients may have developed multiple SPMs and may be represented in multiple rows.
CLL: Chronic lymphocytic leukemia; SPM: Secondary primary malignancy.
Of the 638 patients who developed a SPM, 29.3% had developed a SPM by 12 months post diagnosis, 49.5% had developed a SPM by 24 months post diagnosis and 64.9% had developed a SPM by 36 months post diagnosis. Median time from diagnosis to first SPM was not reached for either the treated or untreated cohort using Kaplan–Meier analysis; the first quartile was 55.7 months for the treated cohort and 94.6 months for the untreated cohort (Figure 2). Among the 166 treated patients who developed a SPM, a greater proportion developed their first SPM after treatment initiation (69.3% [115/166]) compared with those who developed their first SPM prior to treatment initiation (30.7% [51/166]; p < 0.001).
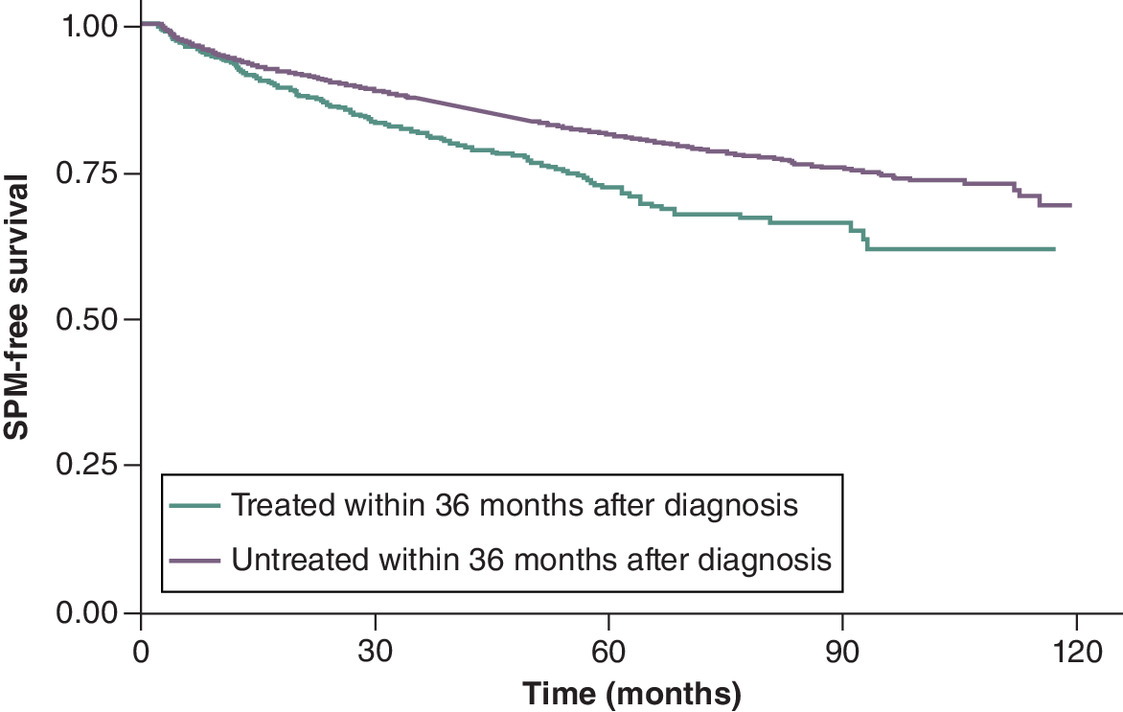
Figure 2. Time from diagnosis to SPM accounting for censoring (in months).
SPM: Secondary primary malignancy.
SPM development occurred in 30.6% (85/278) of patients who received anti-CD20 + chemotherapy, 21.9% (30/137) who received anti-CD20 monotherapy, and 20.5% (25/122) who received targeted oral monotherapy or combination therapy (pairwise tests were not significant at 0.05). For all treatment groups, development of the first SPM occurred more frequently after treatment initiation compared with before treatment initiation.
To understand SPM development attributed to treatment, SPMs were assessed after treatment initiation. SPM development rates were significantly lower among those receiving targeted therapy (15.6%) compared with anti-CD20 + chemotherapy (28.8%; Table 4). Similarly, SPM incidence rates were numerically lower among those receiving targeted therapies compared with anti-CD20 + chemotherapy (Table 5). There were no significant differences in SPM development or incidence between targeted therapies and anti-CD20 monotherapy. In addition, compared with the untreated group using a “pseudo” treatment initiation date, patients receiving treatment had a statistically significantly greater incidence of SPM development (Table 5).
| Anti-CD20 (n = 137) | Anti-CD20 + chemotherapy (n = 278) | Targeted oral agent (monotherapy or with anti-CD20) (n = 122) | |
|---|---|---|---|
| Patients with CLL developing a SPM, n (%) | 29 (21.2) | 80 (28.8) | 19 (15.6) |
†
Treatment regimen categories are mutually exclusive groups that make up the ‘treated’ patient cohort but are not comprehensive – patients may be treated with other regimens not listed here.
p-values: across different treatment regimens <0.05; anti-CD20 vs anti-CD20 + chemotherapy was not significant; anti-CD20 vs targeted oral agent was not significant; anti-CD20 + chemo vs targeted oral agent <0.05.
SPM: Secondary primary malignancy.
| Total SPM cases | Total person-years | Incidence rate per 1000 person-years at risk (95% CI) | |
|---|---|---|---|
| Treated within 36 months post diagnosis (n = 620) | 195 | 2487.5 | 78.4 (67.8–89.8) |
| Anti-CD20 (n = 137) | 33 | 568.8 | 58.0 (40.0–79.4) |
| Anti-CD20 + chemotherapy (n = 278) | 109 | 1226.1 | 88.9 (73.0–106.3) |
| Targeted oral agent (monotherapy or with anti-CD20) (n = 122) | 20 | 333.6 | 60.0 (36.6–88.9) |
| Untreated within 36 months post diagnosis and matched with treated patients (n = 620) | 134 | 2607.7 | 51.4 (43.1–60.4) |
†
For the untreated cohort a “pseudo” treatment initiation date was assigned, as described in the methods.
‡
Treatment regimen categories are mutually exclusive groups that make up the ‘treated’ patient cohort but are not comprehensive – patients may be treated with other regimens not listed here.
p-values: treated vs untreated <0.0001; anti-CD20 vs anti-CD20 + chemotherapy <0.05; anti-CD20 vs targeted oral agent was not significant; anti-CD20 + chemotherapy vs targeted oral agent was not significant.
CI: Confidence interval; SPM: Secondary primary malignancy.
Discussion
In this recent retrospective study, 20.9% of patients diagnosed with CLL experienced a SPM over a mean follow-up time of 67.6 months, with a greater proportion observed within 36 months of diagnosis in the treated versus untreated cohort. The most common SPMs to develop were squamous cell carcinoma (related to skin) and AML. Among the treated cohort, a greater proportion developed their first SPM after treatment initiation compared with those who developed their first SPM prior to treatment initiation. A possible explanation for this is that patients who require CLL therapy initiation closer to their diagnosis may have a more aggressive form of the disease; this may have a consequential impact on the incidence of SPMs due to immunodeficiencies associated with CLL predisposing the patient to an increased risk of other malignancies [10].
Following treatment initiation, SPM development and SPM incidence were significantly lower among patients receiving targeted oral agents compared with those receiving anti-CD20 + chemotherapy regimens. Notably, in this study most patients received ibrutinib as the targeted oral agent (with <11 patients receiving venetoclax as monotherapy or combination treatment), thus the outcomes are largely indicative of patients receiving BTK inhibitors. Findings indicate that the type of CLL treatment may affect SPM development. This is supported by the findings from the phase III CLL12 trial (NCT02863718), where second cancers were reported in 10.8% of patients treated with ibrutinib versus 15.5% of patients treated with placebo [20]. As novel oral agents are associated with fewer reported cases of neutropenia and have a reduced impact on immunoglobulin levels compared with chemoimmunotherapy regimens, this may lead to reduced development of SPMs, as well as better control of CLL disease and restoration of the immune system [21–23].
The SEER database has been used previously to assess the risk of SPM among survivors of CLL [9]. An earlier SEER database study observed a significant increase in SPMs in years 2003–2015 compared with years 1973–1982 and a higher risk of SPMs in patients who received prior chemotherapy compared with untreated patients or those whose treatment status was unknown [9]. Our study expands on these previous findings by using the linkage to Medicare data, allowing identification of specific and recent treatments like targeted therapies, which enables assessment of SPM risk associated with targeted oral agents versus chemotherapy.
A Dutch study which included 24,815 patients with CLL diagnosed between 1989 and 2019 in The Netherlands, indicated that an elevated risk was observed for both solid and hematological SPMs [24]. It was also noted that the risk of SPMs was higher in patients who received anti-neoplastic therapy (subdivided into chemotherapy alone and chemoimmunotherapy) compared with those who did not receive anti-neoplastic therapy [24]. Conclusions from the Dutch study suggest that surveillance and patient management to control SPMs are essential for improving long-term survival outcomes of patients with CLL.
Analyses from other countries, such as Australia, have indicated that the high incidence of SPMs has a substantial impact and health burden on patients with CLL and their management and survival [25]. Further, a review which pooled SPM data from publications of clinical trials concluded that SPM should be considered an important adverse outcome for chemoimmunotherapy regimens, indicating that only a proportion of clinical studies have this information available [26]. Therefore, findings from the current study are imperative, to show the outcomes for clinical practice in the USA.
Notably, the most common SPMs to develop in the current study were the same as those in the Dutch study (squamous cell carcinoma) [24] and are a subgroup of non-melanomatous skin cancer, the most common SPMs to develop in the Australian study [25]. However, development of AML as a SPM was low in both studies, (56 [1.3%] patients in the Dutch study and 7 [1.4%] patients in the Australian study) compared with the current study (186 [24.4%] patients). The Dutch and Australian studies include data spanning several decades (1989 to 2019 and 1981 to 2020, respectively), therefore changes in clinical practice (including improved treatment and management) resulting in prolonged survival for patients with CLL, and advances in the diagnosis of AML (following the European LeukemiaNet recommendations in 2010 [27]) will have occurred only in the latter part of these studies, which likely contributes to the lower rates of AML reported. This is corroborated by the Dutch study highlighting that the risk of AML increased from the early 2000s (which they attributed to changes in therapy).
It is worth highlighting that the outcomes of this study are only reflective of a portion of patients in the USA. While SEER data registries collect cancer cases reported from 22 US geographic areas, which are representative of the demographics of the wider US population [28] and covers approximately 48% of the US population [29], the linkage to Medicare data may limit the generalizability of these results to a Medicare population of older adults (aged ≥65 years). In addition, patients with multiple insurance providers are excluded from the SEER Medicare database, further reducing the generalizability of the study. However, it is important to note that the linkage to Medicare data allows treatment-related details to be extracted, which would not be possible using data from SEER registries alone. Limitations associated with the use of the SEER Medicare database are those inherent to using real-world databases including the potential for inaccurate coding, incomplete data entry and missing data [30,31].
Further limitations of the present study include possible confounding factors which may have affected the immune system and propensity to SPMs, such as the evaluation of CLL disease state at diagnosis, cytogenetic characteristics, as well as overlap with other risk factors including autoimmune diseases and chronic use of corticosteroids. In addition, as 12.5% of the ‘untreated’ group eventually did receive initial CLL treatment, at a median of 51 months following CLL diagnosis, SPMs attributed to treatment may have been missed in these patients. Finally, in the present study, patients with previous malignancies were excluded from the analyses and so this may have an impact on how likely the study reflects the development of SPMs in the real world.
Conclusion
Findings indicate that SPMs could be linked to CLL treatment, with the type of treatment possibly having an influence on SPM development. The current study, alongside previously reported data from trials and real-world studies, suggests that targeted agents may help decrease the rate of development of SPMs in patients with CLL. Further, adequately monitoring the detection of SPMs and the use of novel therapies could provide better control of the disease and potentially reduce the burden of a SPM diagnosis for patients.
Summary points
•
Improvements in the management of chronic lymphocytic leukemia (CLL) have resulted in a growing population of CLL survivors, but patients with CLL have a higher risk of developing second primary malignancies (SPMs).
•
This retrospective cohort study used data from the Surveillance, Epidemiology, and End Results (SEER)-Medicare database.
•
Overall, 32,197 patients aged ≥66 years with newly diagnosed CLL between 1 January 2010 and 31 December 2016 were identified from the SEER-Medicare database. After applying additional study criteria, the final analyses included 3053 patients.
•
Of the 3053 patients, 620 (20.3%) were treated and 2433 (79.7%) patients were untreated within 36 months of diagnosis.
•
Overall, 20.9% (638/3053) of patients developed a SPM, with a greater proportion observed in the treated versus untreated cohort.
•
Among the 166 treated patients who developed a SPM, a greater proportion developed their first SPM after treatment initiation (69.3%) compared with those who developed their first SPM prior to treatment initiation (30.7%).
•
SPM development rates were significantly lower and SPM incidence rates were numerically lower among patients who received targeted therapy compared with patients who were treated with anti-CD20 + chemotherapy.
•
Findings from this study, alongside previously reported data from trials and real-world studies, suggest that targeted agents could help decrease the rate of development of SPMs in patients with CLL.
•
Further, adequately monitoring the detection of SPMs and use of novel therapies could provide better control of the disease and potentially reduce the burden of a SPM diagnosis for patients.
Author contributions
S Ailawadhi, A Ravelo, CD Ng, R Wang, K Eakle and J ML Biondo were responsible for study conception and design; CD Ng, B Shah, N Lamarre and R Wang were responsible for acquisition of data and data analysis; all authors were involved in drafting and revising the manuscript.
Acknowledgments
This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the National Cancer Institute; the Office of Research, Development and Information, CMS; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database.
Financial disclosure
This analysis was sponsored by Genentech. Third-party medical writing assistance, under the direction of the authors, was provided by R Dobb of Ashfield MedComms, an Inizio company, funded by Genentech/F. Hoffmann-La Roche Ltd. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interest disclosure
S Ailawadhi: GSK, Sanofi, BMS, Takeda, Beigene, Pharmacyclics, Amgen, Janssen, AstraZeneca, Regeneron – consultancy; GSK, BMS, Pharmacyclics, Amgen, Janssen, Cellectar, Xencar, AbbVie – research funding. A Ravelo, K Eakle: Genentech – current employment; F. Hoffmann-La Roche Ltd – current holder of individual stocks in a privately-held company and current holder of stock options in a privately-held company. CD Ng: Genentech – current employment; F. Hoffmann-La Roche Ltd – current equity holder in publicly traded company. B Shah: nothing to disclose. N Lamarre: Genesis Research – current employment. R Wang: Genentech – current employment; F. Hoffmann-La Roche Ltd – current holder of individual stocks in a privately-held company. JML Biondo: Genentech – current employment; F. Hoffmann La Roche Ltd – current holder of individual stocks in a privately held company and current holder of stock options in a privately held company. The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention's (CDC) National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the National Cancer Institute's Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This is a retrospective study registry and claims data study which was reviewed by the Western Institutional Review Board-Copernicus Group (WCG® IRB) and received an institutional review board exemption and waiver of Health Insurance Portability and Accountability Act of 1996 (HIPAA) authorization.
Data sharing statement
The authors certify that this manuscript reports data derived from the SEER-Medicare database. The data (individual, de-identified patient data that underlie the results reported in this article) will not be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 208.58 KB
References
1.
van der Straten L, Levin MD, Visser O et al. Survival continues to increase in chronic lymphocytic leukaemia: a population-based analysis among 20,468 patients diagnosed in The Netherlands between 1989 and 2016. Br. J. Haematol. 189(3), 574–577 (2020).
2.
Sigurdur YK, Paul WD, Wyndham HW, Neil C, Magnus B, Ola L. Improved survival in chronic lymphocytic leukemia in the past decade: a population-based study including 11,179 patients diagnosed between 1973–2003 in Sweden. Haematologica 94(9), 1259–1265 (2009).
3.
Kipps TJ, Choi MY. Targeted therapy in chronic lymphocytic leukemia. Cancer J. 25(6), 378–385 (2019).
4.
Patel K, Pagel JM. Current and future treatment strategies in chronic lymphocytic leukemia. J. Hematol. Oncol. 14, 69 (2021).
5.
Sharma S, Rai KR. Chronic lymphocytic leukemia (CLL) treatment: so many choices, such great options. Cancer 125(9), 1432–1440 (2019).
6.
Kommalapati A, Tella SH, Goyal G. Risk of second primary malignancies in chronic lymphocytic leukemia. Blood 132, 3581 (2018).
7.
Royle JA, Baade PD, Joske D, Girschik J, Fritschi L. Second cancer incidence and cancer mortality among chronic lymphocytic leukaemia patients: a population-based study. Br. J. Cancer 105(7), 1076–1081 (2011).
8.
da Cunha-Bang C, Rostgaard K, Andersen MA et al. Risk of new malignancies among patients with CLL treated with chemotherapy: results of a Danish population-based study. Br. J. Haematol. 193(2), 339–345 (2021).
9.
Kumar V, Ailawadhi S, Bojanini L et al. Trends in the risk of second primary malignancies among survivors of chronic lymphocytic leukemia. Blood Cancer J. 30(10), 75 (2019).
10.
Benjamini O, Jain P, Trinh L et al. Second cancers in patients with chronic lymphocytic leukemia who received frontline fludarabine, cyclophosphamide and rituximab therapy: distribution and clinical outcomes. Leuk. Lymphoma 56(6), 1643–1650 (2015).
11.
Maurer C, Langerbeins P, Bahlo J et al. Effect of first-line treatment on second primary malignancies and Richter's transformation in patients with CLL. Leukemia 30(10), 2019–2025 (2016).
12.
Bond DA, Huang Y, Fisher JL et al. Second cancer incidence in CLL patients receiving BTK inhibitors. Leukemia 34(12), 3197–3205 (2020).
13.
Eversman A, Cao S, Boughan KM et al. Risk of secondary malignancy in CLL patients treated with novel targeted agents. Blood 136, 46–47 (2020).
14.
West LA, Samantha C, Goodkins D, He W. 65+ in the United States: 2010 Special Studies: Current Population Reports. Table 2–10. https://www.census.gov/content/dam/Census/library/publications/2014/demo/p23-212.pdf (2023).
15.
Zhou Z, Rahme E, Abrahamowicz M, Pilote L. Survival bias associated with time-to-treatment initiation in drug effectiveness evaluation: a comparison of methods. Am. J. Epidemiol. 162(10), 1016–1023 (2005).
16.
Walkey AJ, Wiener RS. Utilization patterns and patient outcomes associated with use of rescue therapies in acute lung injury. Crit. Care Med. 39(6), 1322–1328 (2011).
17.
Li G, Holbrook A, Delate T, Witt DM, Levine MA, Thabane L. Prediction of individual combined benefit and harm for patients with atrial fibrillation considering warfarin therapy: a study protocol. BMJ Open 5(6), e009518 (2015).
18.
Sussell JA, Sheinson D, Wu N, Shah-Manek B, Seetasith A. HER2-positive metastatic breast cancer: a retrospective cohort study of healthcare costs in the targeted-therapy age. Adv. Ther. 37(4), 1632–1645 (2020).
19.
Lee JM, Wang R, Johnson A, Ogale S, Kent M, Lee JS. Economic burden of recurrence among resected medicare patients with early stage NSCLC. JTO Clin. Res. Rep. 4(4), 100487 (2023).
20.
Langerbeins P, Zhang C, Robrecht S et al. The CLL12 trial: ibrutinib vs placebo in treatment-naïve, early-stage chronic lymphocytic leukemia. Blood 139(2), 177–187 (2022).
21.
Robak T, Burger JA, Tedeschi A et al. Single-agent ibrutinib versus chemoimmunotherapy regimens for treatment-naïve patients with chronic lymphocytic leukemia: a cross-trial comparison of phase 3 studies. Am. J. Hematol. 93(11), 1402–1410 (2018).
22.
Sharman JP, Egyed M, Jurczak W et al. Efficacy and safety in a 4-year follow-up of the ELEVATE-TN study comparing acalabrutinib with or without obinutuzumab versus obinutuzumab plus chlorambucil in treatment-naïve chronic lymphocytic leukemia. Leukemia 36(4), 1171–1175 (2022).
23.
Moreno C, Muñoz C, Terol MJ, Hernández-Rivas JÁ, Villanueva M. Restoration of the immune function as a complementary strategy to treat chronic lymphocytic leukemia effectively. J. Exp. Clin. Cancer. Res. 40(1), 321 (2021).
24.
van der Straten L, Levin MD, Dinnessen MAW et al. Risk of second primary malignancies in patients with chronic lymphocytic leukemia: a population-based study in The Netherlands 1989–2019. Blood Cancer J. 13, 15 (2023).
25.
Shen Y, Coyle L, Kerridge I et al. Second primary malignancies in chronic lymphocytic leukaemia: skin, solid organ, haematological and Richter's syndrome. eJHaem. 3, 129–138 (2022).
26.
Csanádi M, Ágh T, Tordai A, Tapprich C, Vokó Z, Stamatopoulos K. Secondary primary malignancies after treatment with chemo-immunotherapy in treatment-naïve patients with CLL: a systematic literature review. Expert. Rev. Hematol. 15(3), 273–284 (2022).
27.
Döhner H, Estey EH, Amadori S et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood 115(3), 453–474 (2010).
28.
National Cancer Institute. Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/about/using-website.html (2023).
29.
National Cancer Institute. Surveillance, Epidemiology, and End Results Program Overview. https://seer.cancer.gov/about/factsheets/SEER_Overview.pdf (2023).
30.
Ho YF, Hu FC, Lee PI. The advantages and challenges of using real-world data for patient care. Clin. Transl. Sci. 13(1), 4–7 (2020).
31.
Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and impact of real-world clinical data for the practicing clinician. Adv. Ther. 35(11), 1763–1774 (2018).
Information & Authors
Information
Published In
Copyright
© 2024 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 18 July 2023
Accepted: 5 December 2023
Published online: 31 January 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Assessment of second primary malignancies among treated and untreated patients with chronic lymphocytic leukemia using real-world data from the USA. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0119
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Julian J. Guetta-Weiss, Danielle M. Brander, Second Primary Malignancies in Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: A Comprehensive Review, Clinical Lymphoma Myeloma and Leukemia, 10.1016/j.clml.2026.05.012, (2026).