Cost–effectiveness of weekly gastro-resistant risedronate 35 mg, compared with weekly alendronate 70 mg tablets, in the treatment of postmenopausal osteoporosis in Spain
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To estimate the cost–effectiveness of treating postmenopausal osteoporosis (PMO) with weekly gastro-resistant risedronate 35 mg gastro-resistant tablets (RIS-GR), compared with weekly alendronate 70 mg tablets (ALN) in Spain. Methods: A probabilistic analysis (second-order Monte Carlo simulation) was performed with a time horizon of 5 years, from the perspective of the Spanish National Health System. The bone fracture probabilities were obtained from a cohort study of 3614 women from USA with PMO treated with RIS-GR (1807) or ALN (1807) (Thomasius, 2022). The pharmacological cost and the cost of fractures were obtained from Spanish sources (€ 2022). The utilities of patients with and without fracture (quality-adjusted life years [QALYs]) were obtained from the medical literature. Results: Compared with ALN, treatment with RIS-GR can avoid 79 fractures (between 75 and 82) every 1000 patients treated, and 0.0119 QALYs would be gained (between 0.0098 and 0.0140) per patient. Additionally, GR-RIS would generate a cost saving per patient of €1994 (€1437–2904) with a probability of 99.7%. The scenario analyses confirmed the stability of the base case results. Conclusion: According to this study, RIS-GR would be the dominant treatment (lower costs with QALY gain) compared with ALN.
Plain language summary
What is this article about?
In a context of scarcity of resources, it is important to analyze the economic impact of the differences in persistence and probability of fractures of postmenopausal osteoporosis treatments. An economic model of the probabilistic type was carried out, with the aim of estimating the cost–effectiveness of treating postmenopausal osteoporosis (PMO) with weekly gastro-resistant risedronate 35 mg gastro-resistant tablets (RIS-GR), compared with weekly alendronate 70 mg tablets (ALN) in Spain.
What were the results?
In a period of 5 years, due to the lower probability of bone fractures observed with RIS-GR versus ALN, for every 1000 patients, 79 fractures would be avoided. In addition, 0.0119 QALYs would be gained and €1994 saved per patient treated with RIS-GR.
What do the results of the study mean?
Weekly RIS-GR 35 mg is a dominant treatment (lower costs with QALY gain) for PMO compared with weekly ALN 70 mg in Spain.
Osteoporosis, defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture [1,2], has become a major and growing healthcare burden in Europe, resulting today in more than 4.3 million fragility fractures and huge associated healthcare costs in excess of €56 billion annually [3].
According to SCOPE 2021 report, 25.5 million women and 6.5 million men in the 27countries of the European Union plus the UK and Switzerland (EU27+2), in 2019, were estimated to suffer osteoporosis. Furthermore, the number of fragility fractures is increasing with the ageing of Europe's population, which will lead to an increase in related costs, disability and premature deaths [4,5].
Over the past fifty years, several pharmacological agents have been approved for the treatment and prevention of the risk of fractures in osteoporotic patients. At present, despite the development of other potent and effective treatments for osteoporosis, oral bisphosphonates represent the most commonly used anti-osteoporotic therapy worldwide [6] and European guideline recommend them as initial treatment in the majority of cases [7].
However, oral bisphosphonates are poorly absorbed, and their strict dosing instructions, requiring a necessary fasting time before the drug intake, limit the patient's treatment compliance and persistence [8,9] and, hence, the drug anti-fracture effectiveness [10].
Gastro-resistant risedronate (RIS-GR) was developed with the objective of overcoming the inconvenient dosing instructions, increasing absorption independently of food intake, and reducing the risk of gastrointestinal side effects, by eliminating the need for fasting [11,12]. Thus, treatment effectiveness would be preserved, and even enhanced, by increasing the drug absorption and bioavailability [12,13].
Unfortunately, no randomized clinical trials have compared directly the antifracture efficacy of RIS-GR with other oral inmediate-release bisphosphonates. However, recently, in a USA retrospective observational study based on claims data, patients prescribed RIS-GR were associated with a lower incidence of fractures compared with those prescribed other oral bisphosphonates, leading to lower utilization of inpatient services which translated into lower inpatient costs [13].
A validated Markov microsimulation model was used to estimate the cost–effectiveness of RIS-GR compared with weekly alendronate and generic risedronate for the treatment of postmenopausal women with osteoporosis in France, using pooled efficacy data for bisphosphonates derived from a previous meta-analysis, and persistence data (up to 3 years) obtained from a large Australian longitudinal database. The conclusion of the authors was that RIS-GR compared with alendronate and generic risedronate was cost effective for the French postmenopausal women with osteoporosis [14].
In a context of scarcity of resources, it is important to analyze the economic impact of the differences in persistence and probability of fractures of postmenopausal osteoporosis treatments. Nevertheless, to date no cost–effectiveness analyses using direct comparative fracture data between RIS-GR and other oral immediate-release bisphosphonates (either through a controlled clinical trial or a retrospective observational study based on claims data) have been performed.
The objective of the present study was to estimate the anti-fracture cost–effectiveness of treating postmenopausal osteoporosis with weekly RIS-GR 35 mg, compared with weekly alendronate 70 mg in Spain.
Design & methods
Economic model
A probabilistic analysis was made using a second order Monte Carlo simulation to analyse the uncertainty of the model variables (probabilities, costs and utilities) [15,16].
This type of model, whose basic methodology has been described in other previously published studies [17,18], made it possible to: (i) take into account the variability of the patient characteristics and the uncertainty of the model variables in a hypothetical cohort of 1000 patients with the characteristics described in ‘Population’ section; and (ii) calculate the probability of savings with the lowest cost option. The probabilistic analysis was made considering that probabilities fit beta distributions and that costs and utilities would fit gamma distributions [15,17]. The model was developed using Microsoft Excel 2021.
| No. | Base case main model assumptions | Study, year | Ref. |
|---|---|---|---|
| 1 | The probability of hip/pelvic, vertebral, and wrist/arm fractures with RIS-GR and ALN were obtained from the cohort study by Thomasius et al. | Thomasius, 2022 | [13] |
| 2 | Treatment persistence over 5 years was obtained from the observational study by Thomasius et al. | Thomasius, 2022 | [13] |
| 3 | The effect of treatment was assumed to be maintained for two years (years 4 and 5) after its discontinuation. | Darbá, 2015 | [21] |
| 4 | The mortality of the patient without fracture was obtained from the National Institute of Statistics. | INE, 2022 | [22] |
| 5 | The mortality of the patient with fracture was obtained from a previously published Spanish study. | Darbá, 2015 | [21] |
| 6 | The cost of fractures in Spain was calculated as the average of public prices in the regions that have specific prices for the three fractures considered or their DRGs. The average cost of the fractures was calculated according to the percentages observed in Thomasius et al. | Public prices Bartra, 2019; Thomasius, 2022 | [13,19] |
| 7 | Pharmacological cost was obtained from retail prices (PVP) plus VAT, available in the BotPlus web database. | BotPlus, 2022 | [20] |
| 8 | The utilities were obtained from the study by Hiligsmann et al. and Darbá et al. | Darbá, 2015; Hiligsmann, 2019 | [14,21] |
ALN: Weekly alendronate 70 mg tablets; PVP: Drug retail price; RIS-GR: Weekly gastro-resistant risedronate 35 mg gastro-resistant tablets; VAT: Value added tax.
Population
The modelled population was that of the observational study by Thomasius et al. [13]. In the total cohorts of the study (2726 patients per treatment group), postmenopausal women treated with RIS-GR and other bisphosphonates (alendronate sodium, ibandronate sodium and risedronate sodium) had a mean age of 62.0 ± 10.2 and 62.1 ± 10.3 years, respectively, a mean Charlson comorbidity index of 0.1 ± 0.8 and 0.0 ± 0.8, respectively, and a fracture rate history during the 6-month prior to bisphosphonate initiation of 1.7% and 1.7%, respectively. To be eligible, they were required to have at least one bisphosphonate prescription, with no treatment changes (i.e., from RIS-GR to other oral bisphosphonates or from other oral bisphosphonates to RIS-GR) during at least the previous two years. To balance the prognostic factors of the patients in the compared cohorts, each woman in the RIS-GR cohort was paired with one woman in the other bisphosphonates cohort, with similar baseline demographic and clinical characteristics, including age, Charlson comorbidity index, incidence of 13 selected comorbidities and previous fractures (hip, pelvis, spine, wrist/arm), and the use of drugs affecting bone mineral density (abaloparatide, aromatase inhibitors, estrogens, denosumab, gonadotropin-releasing hormone agonists, bisphosphonates for injection, romosozumab, systemic corticosteroids and teriparatide) [13]. The results of the present model would only be applicable to a patient population with the baseline characteristics of the patients in the observational study from which the efficacy data were derived. It should be noted that it would be of interest to have a pragmatic clinical trial directly comparing the efficacy of RIS-GR and ALN, since such a design could reduce the likelihood of bias typical of observational studies.
The cost of fractures, increased mortality and reduced utility were accounted for when the event occurred.
Perspective & time horizon
The analysis was carried out from the perspective of the Spanish National Health System (SNS), thus considering only the direct healthcare costs. The primary objective of the National Health System of Spain is to ensure and enable public financing, universality, as well as the quality and safety of its benefits in terms of health. The time horizon of the analysis was 5 years, according to available data from the study by Thomasius et al. [13]. Separate analyses were done for years 1, 2, 3, 4 and 5.
Probabilities of fracture & mortality
The probabilities of bone fracture used in the model are shown in Table 2. These are those obtained in the clinical practice study (retrospective observational cohort study) of Thomasius et al. [13]. Fracture probabilities were taken from the full cohort of patients. Table 2 also shows the annual mortality risk without bone fracture [22] and the increase in mortality risk resulting from fractures [21].
| Bone fracture probabilities | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Year | Treatment | Mean bone fracture probability | 95% CI | SD | Distribution | Alpha | Beta | |||
| 1 | Risedronate GR | 0.0257 | 0.0204–0.0323 | 0.0030 | Beta | 69.8 | 2646.2 | |||
| Alendronate | 0.0326 | 0.0266–0.0400 | 0.0034 | Beta | 87.9 | 2609.9 | ||||
| 2 | Risedronate GR | 0.0510 | 0.0434–0.0599 | 0.0042 | Beta | 139.2 | 2591.4 | |||
| Alendronate | 0.0591 | 0.0508–0.0686 | 0.0045 | Beta | 159.3 | 2536.5 | ||||
| 3 | Risedronate GR | 0.0708 | 0.0615–0.0814 | 0.0050 | Beta | 180.6 | 2371.0 | |||
| Alendronate | 0.0867 | 0.0765–0.0981 | 0.0055 | Beta | 226.0 | 2380.9 | ||||
| 4 | Risedronate GR | 0.0952 | 0.0836–0.1083 | 0.0063 | Beta | 206.4 | 1962.0 | |||
| Alendronate | 0.1046 | 0.1046–0.1308 | 0.0066 | Beta | 270.4 | 2041.2 | ||||
| 5 | Risedronate GR | 0.1185 | 0.1044–0.1343 | 0.0076 | Beta | 212.6 | 1581.7 | |||
| Alendronate | 0.1444 | 0.1297–0.1607 | 0.0079 | Beta | 285.1 | 1689.4 | ||||
| Mortality risk without bone fracture and mortality risk increase with bone fracture vs normal population | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 60 years | 61 years | 62 years | 63 years | 64 years | |||||
| Year 1 | Year 2+ | Year 1 | Year 2+ | Year 1 | Year 2+ | Year 1 | Year 2+ | Year 1 | Year 2+ | |
| Mortality risk without bone fractures | 0.0061 | 0.0061 | 0.0067 | 0.0067 | 0.0073 | 0.0073 | 0.0081 | 0.0081 | 0.0088 | 0.0088 |
| Mortality risk increase with bone fractures | 5.42 | 3.07 | 5.42 | 3.07 | 5.42 | 3.07 | 5.42 | 3.07 | 5.42 | 3.07 |
CI: Confidence interval; GR: Gastro-resistant; SD: Standard deviation.
Persistence of treatment
The data on treatment persistence (RIS-GR and ALN), likewise obtained in the aforementioned observational study [13] are shown in Table 3.
| Year | RIS-GR Mean (95% CI) | ALN Mean (95% CI) |
|---|---|---|
| 1 | 31.0% (29.3–32.8%) | 37.2% (35.4–39.0%) |
| 2 | 19.5% (18.1–21.0%) | 25.6% (24.0–27.3%) |
| 3 | 11.6% (10.3–12.8%) | 18.2% (16.8–19.8%) |
| 4 | 6.6% (5.5–7.7%) | 12.6% (11.3–14.1%) |
| 5 | 3.8% (2.9–4.9%) | 9.1% (7.7–10.5%) |
ALN: Weekly alendronate 70 mg tablets; CI: Confidence interval; RIS-GR: Weekly risedronate 35 mg gastro-resistant tablets.
Costs
Two types of cost have been considered: pharmacological and referred to bone fractures. The cost of fractures in Spain was calculated as the average of the public prices in the 8 regions that have specific prices for the three types of fractures considered or their diagnosis-related groups (DRGs) (Table 4) [19,24–31]. The average cost of a fracture was calculated from the unit costs of hip/pelvis, vertebral, and wrist/arm fractures, considering the incidence of each type of fracture observed in the observational study. The pharmacological cost was obtained from the public retail prices (PRP) plus VAT, available in the BotPlus web database (Table 4) [20].
| Unit costs | ||||||
|---|---|---|---|---|---|---|
| Resource | Mean | SD | Distribution | Alpha | Beta | References |
| Bone fracture (all) | 7128.85 € | 3929.93 € | Gamma | 3.29 | 2166.46 | Calculated |
| Hip/pelvic fracture | 10,051.16 € | 5644.77 € | Gamma | 3.17 € | 3170.13 € | Public prices |
| Vertebral fracture | 6905.32 € | 3750.50 € | Gamma | 3.39 € | 2037.02 € | Public prices |
| Wrist/arm fracture | 5209.73 € | 2917.27 € | Gamma | 3.19 € | 1633.57 € | Public prices |
| Drugs | PVP+VAT | Units | Dose/unit | Units/year | Cost/year | Reference |
|---|---|---|---|---|---|---|
| Weekly RIS-GR | 19.84 € | 4 | 35 mg | 52.1 | 258.42 € | (20) |
| Weekly ALN | 9.99 € | 4 | 70 mg | 52.1 | 130.25 € | (20) |
| Utilities | ||||||
|---|---|---|---|---|---|---|
| Item | Mean | SD | Distribution | Alpha | Beta | References |
| Without fractures | 0.77 | 0.04 | Gamma | 355.89 | 0.00216 | (14) |
| All fractures | 0.62 | 0.03 | Gamma | 410.20 | 0.00151 | Calculated |
| Hip/pelvic fractures | 0.55 | 0.01 | Gamma | 2905.21 | 0.00019 | (14) |
| Vertebral fractures | 0.59 | 0.03 | Gamma | 384.16 | 0.00154 | (21) |
| Wrist/arm fracture | 0.62 | 0.03 | Gamma | 410.20 | 0.00151 | (14) |
ALN: Weekly alendronate 70 mg tablets; PVP: Drug retail price; RIS-GR: Weekly risedronate 35 mg gastro-resistant tablets; SD: Standard deviation; VAT: Value added tax.
Utilities
Scenario analyses
Scenario analyses were performed for the following assumptions: (i) a gradual loss of treatment effect at years 4 and 5, after 3 years of treatment; (ii) a ± 20% variability in fracture incidence observed with RIS-GR and ALN; (iii) a ± 20% variability in the unit cost of bone fractures; (iv) a ± 20% variability in fracture-associated utilities; (v) patients under 65 years of age; and (vi) patients aged 65 years or older.
In our study, probabilistic analyses were performed for each year, separately, up to a time horizon of 5 years. In each analysis, the annual values of all the variables were considered, including the probability of fracture, mortality, and persistence of treatment. For this reason, in the base case of the analysis, a discount equal to zero percent (for 1 year) was assumed. However, an additional analysis has been carried out, assuming that the annual data in the 5-year period were indicative of the evolution of the patients in that period, for which an annual discount rate of 3% was applied both for the costs and for the utilities.
Results
Healthcare impact
In comparison with ALN, treatment with RIS-GR would avoid 79 fractures (between 75 and 82) per 1000 treated patients over a 5-year period (Table 5). It is estimated that 168,701 osteoporotic fractures would be avoided in that same period if all patients with osteoporosis were treated with RIS-GR. In addition, treatment with RIS-GR would result in a gain of 0.0119 QALYs (between 0.0098 and 0.0140) per patient over a 5-year period (Table 5).
| Fractures avoided with weekly risedronate GR vs weekly alendronate (per 1000 patients) | |||||||
|---|---|---|---|---|---|---|---|
| Treatment duration | 1 year | 2 years | 3 years | 4 years | 5 years | Total | |
| Risedronate GR fractures | Mean | 26 | 51 | 71 | 96 | 119 | 363 |
| Minimum | 20 | 43 | 61 | 83 | 104 | 312 | |
| Maximum | 32 | 60 | 82 | 109 | 135 | 418 | |
| Alendronate fractures | Mean | 33 | 59 | 87 | 118 | 145 | 442 |
| Minimum | 26 | 51 | 76 | 104 | 129 | 387 | |
| Maximum | 40 | 69 | 99 | 131 | 161 | 500 | |
| Bone fractures avoided | Mean | -7 | -8 | -16 | -22 | -26 | -79 |
| Minimum | -6 | -7 | -15 | -21 | -25 | -75 | |
| Maximum | -8 | -9 | -17 | -23 | -26 | -82 | |
| QALYs gained per patient with weekly risedronate GR vs weekly alendronate | |||||||
|---|---|---|---|---|---|---|---|
| Treatment duration | 1 year | 2 years | 3 years | 4 years | 5 years | Total | |
| QALYs with weekly RIS-GR | Mean | 0.7679 | 0.7587 | 0.7546 | 0.7496 | 0.7445 | 3.7753 |
| Minimum | 0.6910 | 0.6833 | 0.6800 | 0.6760 | 0.6719 | 3.4022 | |
| Maximum | 0.8483 | 0.8374 | 0.8325 | 0.8263 | 0.8200 | 4.1645 | |
| QALYs with weekly ALN | Mean | 0.7669 | 0.7574 | 0.7522 | 0.7463 | 0.7406 | 3.7634 |
| Minimum | 0.6902 | 0.6823 | 0.6780 | 0.6732 | 0.6686 | 3.3924 | |
| Maximum | 0.8470 | 0.8359 | 0.8296 | 0.8225 | 0.8155 | 4.1504 | |
| QALYs gained with RIS-GR | Mean | 0.0010 | 0.0012 | 0.0024 | 0.0033 | 0.0039 | 0.0119 |
| Minimum | 0.0008 | 0.0010 | 0.0020 | 0.0028 | 0.0033 | 0.0098 | |
| Maximum | 0.0013 | 0.0015 | 0.0029 | 0.0039 | 0.0045 | 0.0140 | |
| Total cost per patient with weekly risedronate GR vs weekly alendronate | |||||||
|---|---|---|---|---|---|---|---|
| Treatment duration | 1 year | 2 years | 3 years | 4 years | 5 years | Total | |
| Risedronate GR | Mean | 281.32 € | 441.21 € | 569.19 € | 740.06 € | 909.01 € | 2940.80 € |
| Minimum | 109.76 € | 119.03 € | 129.62 € | 154.33 € | 182.47 € | 695.20 € | |
| Maximum | 627.99 € | 1064.56 € | 1407.87 € | 1849.51 € | 2282.05 € | 7231.97 € | |
| Alendronate | Mean | 834.39 € | 850.07 € | 940.77 € | 1080.22 € | 1229.98 € | 4935.43 € |
| Minimum | 597.37 € | 458.45 € | 388.72 € | 350.36 € | 337.35 € | 2132.26 € | |
| Maximum | 1282.44 € | 1582.63 € | 1964.78 € | 2428.76 € | 2878.02 € | 10,136.63 € | |
| Savings with RIS-GR | Mean | -553.07 € | -408.86 € | -371.57 € | -340.16 € | -320.97 € | -1994.63 € |
| Minimum | -487.61 € | -339.43 € | -259.10 € | -196.04 € | -154.89 € | -1437.06 € | |
| Maximum | -654.45 € | -518.07 € | -556.91 € | -579.26 € | -595.97 € | -2904.66 € | |
Bold numbers represent the final results.
ALN: Weekly Alendronate 70 mg tablets; QALYs: Quality-adjusted life-years; RIS-GR: Weekly risedronate 35 mg gastro-resistant tablets.
Economic impact
Compared with ALN, RIS-GR would generate savings per treated patient of €1994 (€1437–2904), with the probability of savings with RIS-GR being 99.7% (Tables 5 & 6). It is estimated that savings of €1200 million could be generated as a result of the reduction in bone fracture rates (Table 6).
| Treatment | Cost per patient | Cost differences† | QALYs per patient | QALY difference | Fractures | Fractures avoided | Cost per QALY gained | Cost per Fracture avoided |
|---|---|---|---|---|---|---|---|---|
| RIS-GR ALN | 2940.80 € 4935.43 € | -1994.63 € | 3.7753 3.7634 | 0.0119 | 363 442 | -79 | Risedronate GR is the dominant treatment‡ | Risedronate GR is the dominant treatment‡ |
†
Probability of savings with weekly Risedronate GR vs weekly alendronate: 99.7%; estimated savings due to fractures avoided with weekly risedronate GR vs weekly alendronate: 1,202 million euros (1,202,682,218 €).
‡
With weekly risedronate GR, fractures are avoided or QALYs are gained, with lower costs per patient, than with weekly alendronate.
GR: Gastro-resistant; QALYs: Quality-adjusted life-years.
Cost–effectiveness
RIS-GR would be the dominant treatment versus ALN, as it would prevent a considerable number of bone fractures and generate gains in QALY for the patient, as well as savings for the SNS (Table 6). These results were confirmed in all the scenario analyses, with RIS-GR versus ALN being the dominant treatment in all cases (Table 7 & Figure 1).
| Scenario | Treatment | Cost per patient | QALYs per patient | Fractures | Cost per QALY gained | Cost per Fracture avoided |
|---|---|---|---|---|---|---|
| Gradual loss of treatment effect at years 4 and 5, after treatment for 3 years | RIS-GR ALN | 2829 € 4799 € | 3.7631 3.7513 | 361 439 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Incidence of fractures with RIS-GR and ALN (-20%) | RIS-GR ALN | 2379 € 4254 € | 3.7885 3.7790 | 290 353 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Incidence of fractures with RIS-GR and ALN (+20%) | RIS-GR ALN | 3235 € 5291 € | 3.7398 3.7257 | 431 526 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Unit cost of bone fractures (-20%) | RIS-GR ALN | 2301 € 4158 € | 3.7611 3.7493 | 360 439 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Unit cost of bone fractures (+20%) | RIS-GR ALN | 2376 € 4250 € | 3.7724 3.7606 | 362 441 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Utilities with bone fractures (-20%) | RIS-GR ALN | 3296 € 5366 € | 3.7601 3.7483 | 360 439 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Utilities with bone fractures (+20%) | RIS-GR ALN | 2864 € 4843 € | 3.8143 3.8123 | 362 440 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Patients <65 years of age | RIS-GR ALN | 1270 € 2715 € | 3.8011 3.8005 | 139 143 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Patients ≥65 years of age | RIS-GR ALN | 2805 € 5167 € | 3.7710 3.7514 | 345 475 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
| Annual discount cost and benefits: 3% | RIS-GR ALN | 2530 € 4345 € | 3.4456 3.4351 | 324 394 | Risedronate GR is the dominant treatment† | Risedronate GR is the dominant treatment† |
†
With weekly risedronate GR, fractures are avoided or QALYs are gained, with lower costs per patient, than with weekly Alendronate.
ALN: Weekly Alendronate 70 mg tablets; RIS-GR: Weekly risedronate 35 mg gastro-resistant tablets.
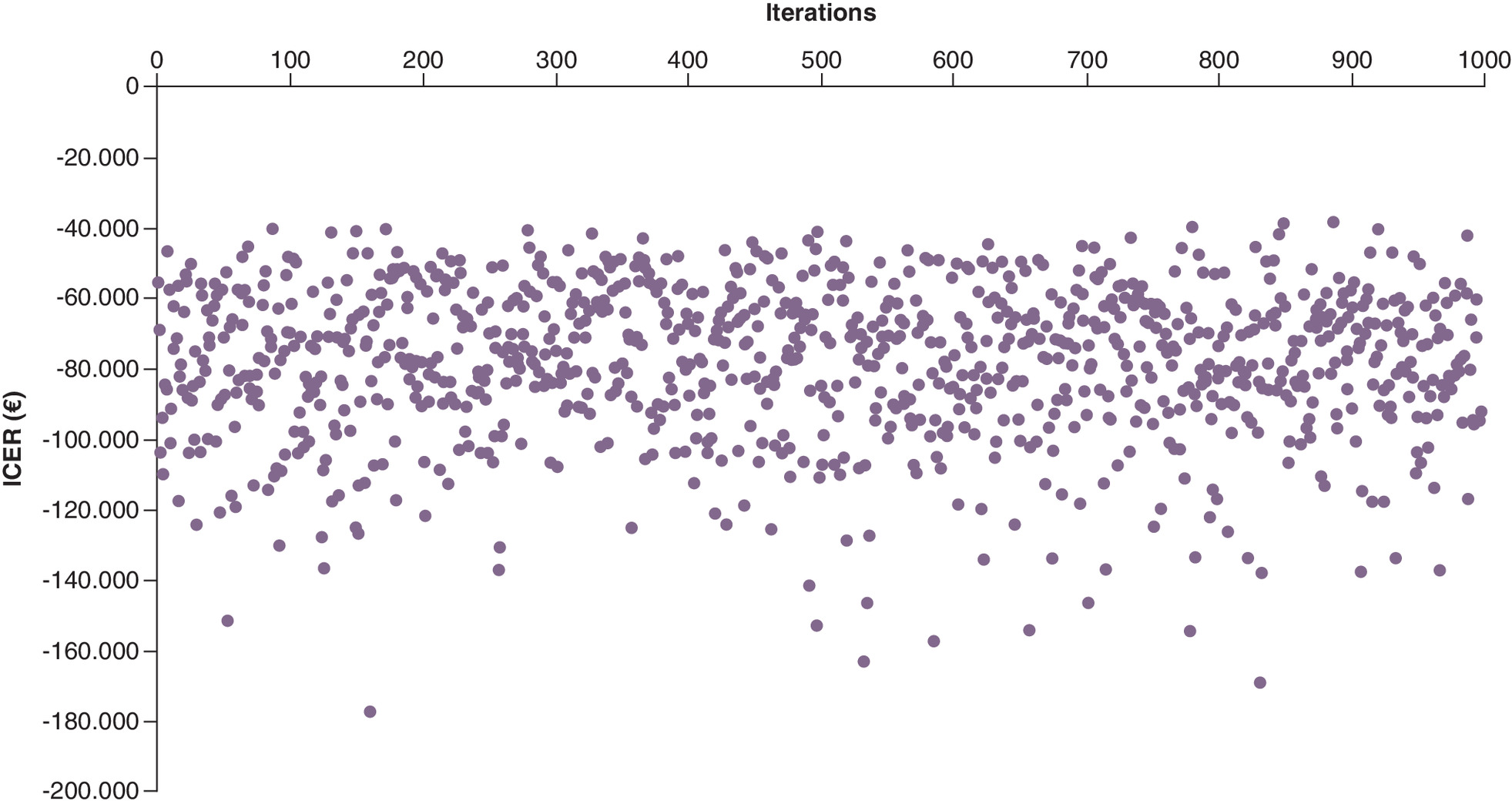
Figure 1. cost–effectiveness results (cost per quality-adjusted life year gained with weekly gastro-resistant risedronate 35 mg gastro-resistant tablets vs weekly alendronate 70 mg tablets).
ICER: Incremental cost–effectiveness ratio (cost per quality-adjusted life year gained with weekly gastro-resistant risedronate 35 mg gastro-resistant tablets vs weekly alendronate 70 mg tablets).
Discussion
Based on the results of the study, the treatment of postmenopausal osteoporosis with RIS-GR would avoid a considerable number of fractures, being cost-effective (dominant) compared with ALN in Spain. In assessing these results, we must consider both the strengths and possible weaknesses of the study. The fact that it is the first study to analyse the cost–effectiveness of RIS-GR compared with ALN in Spain can be considered a strength, and, for this purpose, the results from more than 2700 patients in each branch of the observational study were analysed.
The characteristics of the clinical study from which the model data were obtained imply a number of weaknesses. First of all, the Thomasius et al. study only provides average rates for all bone fractures as a whole, not annual rates for each type of fracture [13]. This is a weakness of the study, determined by the available clinical data. In second place, the average mortality rate from bone fractures was calculated from the mortality risk of joint hip/pelvic fractures, vertebral fractures, and joint wrist/arm fractures from a previously published Spanish study [21], for ages 60–65 years and for the frequency of each type of fracture in the Thomasius et al. study [13]. This simplification was necessary due to the aforementioned limitation. Finally, although the ability of claims to capture vertebral fractures may be poor, in the study by Thomasius et al., 29.4% of the total fractures observed were vertebral [13].
A second weakness to be considered is the fact that the probabilities of bone fracture used in the model come from a retrospective observational cohort study in clinical practice, in cohorts of patients from the USA [13]. However, the results from clinical efficacy trials conducted in other countries should be considered acceptable in Europe, in accordance with the recommendations of the European Medicines Agency [32,33]. During the period from January 2019 to June 2021, in 116 approvals of the US FDA, evaluation was made of the results of clinical practice effectiveness studies [34]. The data from the USA can be regarded as effectiveness outcomes that can be extrapolated to European countries with a similar sociosanitary level [33]. Variability in clinical practice is not limited to comparisons between countries but is also found within Spain's own National Health System [35]. On the other hand, life expectancy at birth may be an indirect indicator of the efficiency of the health system [36], and thus can be used to analyse the comparability of health systems in different countries. Life expectancy in Spain in men and women is 79.6 and 85.1 years, respectively, according to 2020 data from the National Statistics Institute (INE) [37], while in the US it is 74.5 and 80.2 years, respectively, likewise in 2020 [38]. The potential uncertainty regarding extrapolation of the effectiveness outcomes from the USA to Spain has nevertheless been analysed through second order Monte Carlo simulations [15,16]. The Monte Carlo simulation is a probabilistic analysis that performs repeated random calculations in -lato sensu- each patient of a hypothetical cohort (or in each iteration). In each calculation, the patient (or iteration) follows a different course and acquires different cost, survival and transition probability values that are adjusted to certain statistical distributions [39]. The stability of the base case results in all the scenario analyses may also be considered a strength of the study. With regard to other weaknesses of the study, it should be noted that this is a theoretical model, which by definition constitutes a simplified simulation of reality. In addition, there were discrepancies in the results referred to the persistence of RIS-GR treatment in the observational study of Thomasius et al. [13] and in an economic model published in 2019 [14]. In the Thomasius study, a lower treatment persistence observed in the RIS-GR cohort might be due to the detrimental impact of the comparatively higher out-of-pocket cost of RIS-GR [13]. In the latter, higher three-year persistence data were used with RIS-GR versus ALN. In this regard, it was considered more appropriate to model the persistence data obtained in the observational study, from which the bone fracture rates were likewise taken, with the availability of data at 5 years, the time horizon of our model. According to the study by Hiligsmann et al. [14], in women with a bone mineral density T-score ≤ – 2.5 and prevalent vertebral fractures, the cost per quality-adjusted life year (QALY) gained with RIS-GR versus ALN, generic RIS and no treatment would be under €20,000. The results of the present model would only be applicable to a patient population with the baseline characteristics of the patients in the observational study from which the efficacy data were derived.
In Spain, other economic analyses have been published comparing RIS and ALN, but none with RIS-GR. In 2002, a Markov model was published [40], according to which the cost per avoided hip fracture (in treated women from the age of 70 years, with or without previous vertebral fracture, and after 10 years of treatment) ranged with daily administered RIS between €54,134 and €84,287. The costs were higher with alendronate: €67,853 and €173,748. The cost per quality-adjusted life year (QALY) gained was also lower with risedronate (€43,601–61,064) than with alendronate (€49,483–88,634) in patients with or without previous vertebral fracture. Therefore, daily administered RIS was more cost-effective than weekly administered alendronate.
According to a cost-utility analysis published in 2009 and comparing weekly RIS and weekly ALN, the cost per hip fracture avoided with RIS and the cost per QALY gained with RIS was €5318 and €10,636, respectively, with weekly RIS being cost-effective versus weekly ALN [41].
Although the persistence rate would be lower with RIS-GR than with ALN, fracture rates were favorable to RIS-GR throughout the 5 years of the study by Thomasius et al. [13]. These results would be consistent with the hypothesis that the independent administration of food intake could increase the bioavailability of the drug and reduce the probability of fractures compared with ALN [14,42,43].
Conclusion
According to the economic model, the treatment of postmenopausal osteoporosis with RIS-GR would avoid a considerable number of fractures, being cost-effective compared with ALN in Spain.
Summary points
•
A probabilistic modeling analysis was performed, using second-order Monte Carlo simulations, with 1000 simulations, in postmenopausal osteoporosis patients treated with weekly gastro-resistant risedronate 35 mg gastro-resistant tablets (RIS-GR), compared with weekly alendronate 70 mg (ALN) from the perspective of the Spanish National Health System.
•
In a period of 5 years, due to the lower probability of bone fractures observed with RIS-GR versus ALN, for every 1000 patients, 79 fractures would be avoided. In addition, 0.0119 QALYs would be gained and €1994 saved per patient treated with RIS-GR.
•
Consequently, weekly RIS-GR 35 mg is a dominant treatment (lower costs with QALY gain) for PMO compared with weekly ALN 70 mg in Spain.
Financial disclosure
Study conducted with an aid to research, without restrictions, from Theramex Spain. The authors have received no other financial and/or material support for this research or the creation of this work apart from that disclosed.
Competing interest disclosure
E Casado has received consulting fees or speaker remuneration from Amgen, UCB, Theramex, Gedeon-Richter, STADA and Rubió. C Rubio-Terrés and D Rubio-Rodríguez received fees from Theramex Spain, regarding the present manuscript. I Arístegui is an employee of Theramex Spain. The authors have no other competing interests or relevant affiliations with any organization/entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 285, 785–795 (2001).
2.
Lorentzon M, Cummings SR. Osteoporosis: the evolution of a diagnosis. J. Intern. Med. 277, 650–661 (2015).
3.
Osteoporosis: new online map shows burden across Europe (2023). https://healthcare-in-europe.com/en/news/osteoporosis-map-burden-europe
4.
SCOPE 2021 Report (2023). https://www.osteoporosis.foundation/scope-2021
5.
Kanis JA, Norton N, Harvey NC et al. SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch. Osteoporos. 16, 82 (2021).
6.
Adami G, Fassio A, Gatti D et al. Osteoporosis in 10 years' time: a glimpse into the future of osteoporosis. Ther. Adv. Musculoskelet. Dis. 14, 1759720X221083541 (2022).
7.
Kanis JA, Cooper C, Rizzoli R, Reginster JY. Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) and the Committees of Scientific Advisors and National Societies of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 30, 3–44 (2019).
8.
Ettinger B, Pressman A, Schein J, Chan J, Silver P, Connolly N. Alendronate use among 812 women: prevalence of gastrointestinal complaints, noncompliance with patient instructions, and discontinuation. J. Manag. Care Pharm. 4, 488–492 (1998).
9.
Vytrisalova M, Touskova T, Ladova K et al. Adherence to oral bisphosphonates: 30 more minutes in dosing instructions matter. Climacteric 18, 608–616 (2015).
10.
Chodick G, Moser SS, Goldshtein I. Non-adherence with bisphosphonates among patients with osteoporosis: impact on fracture risk and healthcare cost. Expert Rev. Pharmacoecon. Outcomes Res. 16, 359–370 (2016).
11.
Pazianas M, Abrahamsen B, Ferrari S, Russell RG. Eliminating the need for fasting with oral administration of bisphosphonates. Ther. Clin. Risk Manag. 9, 395–402 (2013).
12.
McClung MR, Balske A, Burgio DE, Wenderoth D, Recker RR. Treatment of postmenopausal osteoporosis with delayed-release risedronate 35 mg weekly for 2 years. Osteoporos. Int. 24, 301–310 (2013).
13.
Thomasius F, Palacios S, Alam A, Boolell M, Vekeman F, Gauthier G. Fracture rates and economic outcomes in patients with osteoporosis prescribed risedronate gastro-resistant versus other oral bisphosphonates: a claims data analysis. Osteoporos. Int. 33, 217–228 (2022).
•• of considerable interest
14.
Hiligsmann M, Reginster JY. Cost effectiveness of gastro resistant risedronate tablets for the treatment of postmenopausal women with osteoporosis in France. Osteoporos. Int. 30, 649–658 (2019).
•• of considerable interest
15.
Briggs A, Claxton K, Sculpher M. Decision Modelling for Health Economic Evaluation. Oxford University Press, UK (2006).
16.
Rubio-Terrés C, Rubio-Rodríguez D. Probabilistic analysis: sensitivity analysis or main result? [editorial]. Pharmacoecon. Open 1, 1000e102 (2016).
17.
Kim HK, Peral C, Rubio-Rodríguez D, Rubio-Terrés C. Cost of patients with hemophilia A treated with standard half-life or extended half-life FVIII in Spain. Expert Rev. Pharmacoecon. Outcomes Res. 21(2), 315–320 (2021).
18.
Formiga F, García-Pavía P, Martín Sánchez FJ et al. Health and economic impact of the correct diagnosis of transthyretin cardiac amyloidosis in Spain. Expert Rev. Pharmacoecon. Outcomes Res. 21, 1127–1133 (2021).
19.
Bartra A, Caeiro JR, Mesa-Ramos M et al. en representación de los investigadores del estudio PROA. Cost of osteoporotic hip fracture in Spain per Autonomous Region. Rev. Esp. Cir. Ortop. Traumatol. (Engl. Ed.) 63, 56–68 (2019).
20.
BotPlus (2022). https://botplusweb.portalfarma.com
21.
Darbá J, Kaskens L, Sorio Vilela F, Lothgren M. Cost-utility of denosumab for the treatment of postmenopausal osteoporosis in Spain. Clinicoecon. Outcomes Res. 7, 105–117 (2015).
• of interest
22.
INE. Tablas de mortalidad por año, sexo, edad y funciones. Resultados nacionales, por comunidades autónomas y provincias. Instituto Nacional de Estadística (2022). https://ine.es
23.
Ley 20/2017, de 28 de diciembre, de tasas. BOE N° 38, 12 de febrero de 2018: 16727 (2023). https://www.boe.es/eli/es-vc/l/2017/12/28/20/dof/spa/pdf
24.
Orden 727/2017, de 7 de agosto, del consejero de Sanidad, por la que se fijan los precios públicos por la prestación de los servicios y actividades de naturaleza sanitaria de la red de centros de la Comunidad de Madrid. BOCM N° 198, 21 de agosto de 2017 (2023). http://www.madrid.org/wleg_pub/#
25.
Orden SAN/35/2017, de 15 de diciembre, por la que se fijan las cuantías de los Precios Públicos de los Servicios Sanitarios prestados por el Servicio Cántabro de Salud. BOC N° 248, 29 de diciembre de 2017 (2023). https://boc.cantabria.es/boces/verAnuncioAction.do?idAnuBlob=320839
26.
Orden SLT/71/2020, de 2 de junio, por la que se regulan los supuestos y conceptos facturables y se aprueban los precios públicos correspondientes a los servicios que presta el Instituto Catalán de la Salud. DOGC N° 8153, 12 de junio de 2020 (2023). https://vlex.es/vid/orden-slt-71-2020-845025418
27.
Precios públicos de servicios sanitarios prestados en el SSPA. 28/10/2021 (2022). https://datos.gob.es/es/catalogo/a01002820-precios-publicos-de-servicios-sanitarios-prestados-en-el-sspa
28.
Resolución del director general del Servicio de Salud de las Islas Baleares por la que se modifica la Orden de la consejera de Salud y Consumo de 22 de diciembre de 2006 por la que se establecen los precios públicos a aplicar por los centros sanitarios de la Red Pública de las Islas Baleares por la prestación de servicios sanitarios, cuando existan terceros obligados al pago o usuarios sin derecho a asistencia sanitaria de la Seguridad Social. BOIB N° 2, 4 de enero de 2018: 111 (2023). http://www.caib.es/eboibfront/pdf/es/2018/2/998038
29.
Resolución 1564/2018, de 20 de diciembre, del Director Gerente del Servicio Navarro de Salud, por la que se fijan las tarifas por los servicios prestados por el Servicio Navarro de Salud. BON N° 14, 22 de enero de 2019 (2023). https://bon.navarra.es/es/anuncio/-/texto/2019/14/5
30.
Resolución SLT/474/2022, de 25 de febrero, sobre la revisión de precios públicos correspondientes a los servicios sanitarios que presta el Instituto Catalán de la Salud. DOGC N° 8617, 2 de marzo de 2022 (2023). https://noticias.juridicas.com/base_datos/CCAA/720757-r-slt-474-2022-de-25-feb-ca-cataluna-revision-de-precios-publicos-correspondientes.html
31.
Tarifas para facturación de servicios sanitarios y docentes del Servicio vasco de salud para el año 2021. Vitoria: departamento vasco de salud, diciembre de 2020 (2023). https://www.osakidetza.euskadi.eus/contenidos/informacion/osk_servic_para_empresas/es_def/adjuntos/Libro_de_Tarifas_2022_CAS.pdf
32.
Reflection paper on the extrapolation of results from clinical studies conducted outside the USA to the EU-population. Committee for Medicinal Products for Human Use (CHMP): EMEA/CHMP/EWP/692702/2008. London (2023). https://www.ema.europa.eu/en/documents/scientific-guideline/reflection-paper-extrapolation-results-clinical-studies-conducted-outside-european-union-eu-eu_en.pdf
• of interest
33.
Note for guidance on ethnic factors in the acceptability of foreign clinical data (CPMP/ICH/289/95). CHMP/ICH/289/95. 1998 Sep (2023). https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-5-r1-ethnic-factors-acceptability-foreign-clinical-data-step-5_en.pdf
• of interest
34.
Purpura CA, Garry EM, Honig N, Case A, Rassen JA. The Role of Real-World Evidence in FDA-Approved New Drug and Biologics License Applications. Clin. Pharmacol. Ther. 111, 135–144 (2022).
35.
Atlas de Variaciones en la Práctica Médica (2022). https://www.atlasvpm.org/
36.
Zarulli V, Sopina E, Toffolutti V, Lenart A. Health care system efficiency and life expectancy: a 140-country study. PLOS ONE 16, e0253450 (2021).
37.
Esperanza de vida al nacer. 2020. Mujeres y hombres (2023). https://www.ine.es/jaxi/Tabla.htm?path=/t00/mujeres_hombres/tablas_2/&file=d2g4.px
38.
La esperanza de vida retrocede en Estados Unidos hasta los 77,28 años (2023). https://datosmacro.expansion.com/demografia/esperanza-vida/usa
39.
Rubio-Terrés C, Rubio-Rodríguez D. Glosario de Farmacoeconomía. 30 de septiembre de 2019 (2022). https://www.healthvalue.org/pdfs/ GLOSARIO%20DE%20FARMACOECONOM%-C3%8DA.pdf
40.
Hart WM, Rubio-Terrés C, Burrell A, Arístegui I, Escobar-Jiménez F. Análisis farmacoeconómico del tratamiento de la osteoporosis postmenopáusica con risedronato o alendronato. REEMO 11, 97–104 (2002).
41.
Betegón L, Gómez C, Marqués M. Análisis farmacoeconómico de risedronato semanal frente a alendronato semanal en España. REEMO 18, 9–14 (2009).
• of interest
42.
Adachi J, Lynch N, Middelhoven H et al. The association between compliance and persistence with bisphosphonate therapy and fracture risk: a review. BMC Musculoskelet. Disord. 8, 97 (2007).
43.
Siris ES, Fan CPS, Yang X et al. Association between gastrointestinal events and compliance with osteoporosis therapy. Bone Rep. 4, 5–10 (2016).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 July 2023
Accepted: 4 September 2023
Published online: 15 September 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness of weekly gastro-resistant risedronate 35 mg, compared with weekly alendronate 70 mg tablets, in the treatment of postmenopausal osteoporosis in Spain. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0115
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Zenghui Tian, Kaiying Cui, Yuxiao Tian, Yungang Chen, Guoyan Liu, Farong Zhang, Yanke Hao, Yingying Li, Exploring the mechanism of Heidihuang Pill in the treatment of osteoporosis based on network pharmacology, molecular docking, and experimental validation, Frontiers in Endocrinology, 10.3389/fendo.2025.1664254, 16, (2025).