Characteristics of patients with chronic kidney disease and Type 2 diabetes initiating finerenone in the USA: a multi-database, cross-sectional study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Finerenone is safe and efficacious for treating patients with chronic kidney disease (CKD) and Type 2 diabetes (T2D). Evidence on the use of finerenone in clinical practice is lacking. Objective: To describe demographic and clinical characteristics of early adopters of finerenone in the United States, according to sodium-glucose cotransporter 2 inhibitor (SGLT2i) use and urine albumin–creatinine ratio (UACR) levels. Methods: Multi-database, observational, cross-sectional study, using data from two US databases (Optum Claims and Optum EHR). Three cohorts were included: finerenone initiators with prior CKD-T2D, finerenone initiators with prior CKD-T2D and concomitant SGLT2i use, finerenone initiators with prior CKD-T2D stratified according to UACR. Results: In total, 1015 patients were included, 353 from Optum Claims and 662 from Optum EHR. Mean age was 72.0 and 68.4 years in Optum claims and EHR, respectively. Median eGFR was 44 and 44 ml/min/1.73 m2; and median UACR was 132 (28–698)/365 (74–1185.4) mg/g, in Optum Claims and EHR, respectively. 70.5/70.4% were taking renin-angiotensin system inhibitors, 42.5/53.3% SGLT2i. Overall, 9.0/6.3% of patients had baseline UACR <30 mg/g, 15.0/20.2% had UACR 30–300 mg/g, and 14.4/27.6% had UACR >300 mg/g. Conclusion: Current management of patients with CKD-T2D reflects use of finerenone independently from background therapies and clinical characteristics, suggesting implementation of therapeutic strategies based on different modes of action.
Chronic kidney disease (CKD) is associated with a higher risk of end-stage kidney disease (ESKD) as well as cardiovascular (CV) complications and premature death [1]. This is especially relevant among patients with Type 2 diabetes (T2D). The prevalence of CKD among patients with T2D ranges from 17% to 46% across different countries [2–4].
Traditionally, renin-angiotensin system (RAS) inhibitor drugs (e.g., angiotensin-converting enzyme inhibitors [ACEi], angiotensin receptor blockers [ARB]) have been recommended for the treatment of patients with CKD and T2D [5]. More recently, sodium-glucose cotransporter 2 inhibitors (SGLT2i) have also been shown to reduce CKD progression and CV events in this population. However, despite these treatments, patients with CKD and T2D still have an important residual risk for such events [6].
Overactivation of the mineralocorticoid receptor (MR) plays a key role in the development of cardiac, vascular, and renal diseases, through the promotion of profibrotic and proinflammatory factors [7]. The FIDELIO and FIGARO trials [8,9] and the prespecified pooled analysis, FIDELITY [10], demonstrated that finerenone, in addition to RAS inhibition at the maximum tolerated dose, reduced the risk of CKD progression and CV complications across a broad range of patients with CKD and T2D. Finerenone was approved in the European Union for the treatment of CKD (with albuminuria) with T2D by the European Medicines Agency on 16 February 2022 [11] whereas, in United States (US), finerenone received approval from the Food and Drug Administration on 9 July 2021 to reduce the risk of sustained renal function decline, ESKD, CV death, non-fatal myocardial infarction, and hospitalization for heart failure in adult patients with CKD associated with T2D [12].
In summary, the clinical landscape for the treatment of patients with CKD and T2D is evolving rapidly with the introduction of new treatments, and it is of interest to study how they are used in routine patient management. Recent recommendations released by various international bodies have recommended finerenone as add-on therapy to optimized standard of care (SoC) defined as ACEi or ARB and SGLT2i [13]. In the UK, NICE guidelines recommend adding finerenone to the highest tolerated dose of SoC for all patients unless unsuitable [14]. However, since finerenone received marketing authorization recently, there is still a lack of evidence on its use in real-world settings including the demographic and clinical characteristics of patients using finerenone in the real-world according to concurrent use of SGLT2i and UACR category.
The aim of this study was to characterize a population of initiators of finerenone in the US focusing on demographic and clinical features, stratifying by concomitant SGLT2i use and by albuminuria levels at baseline.
Materials & methods
Study design
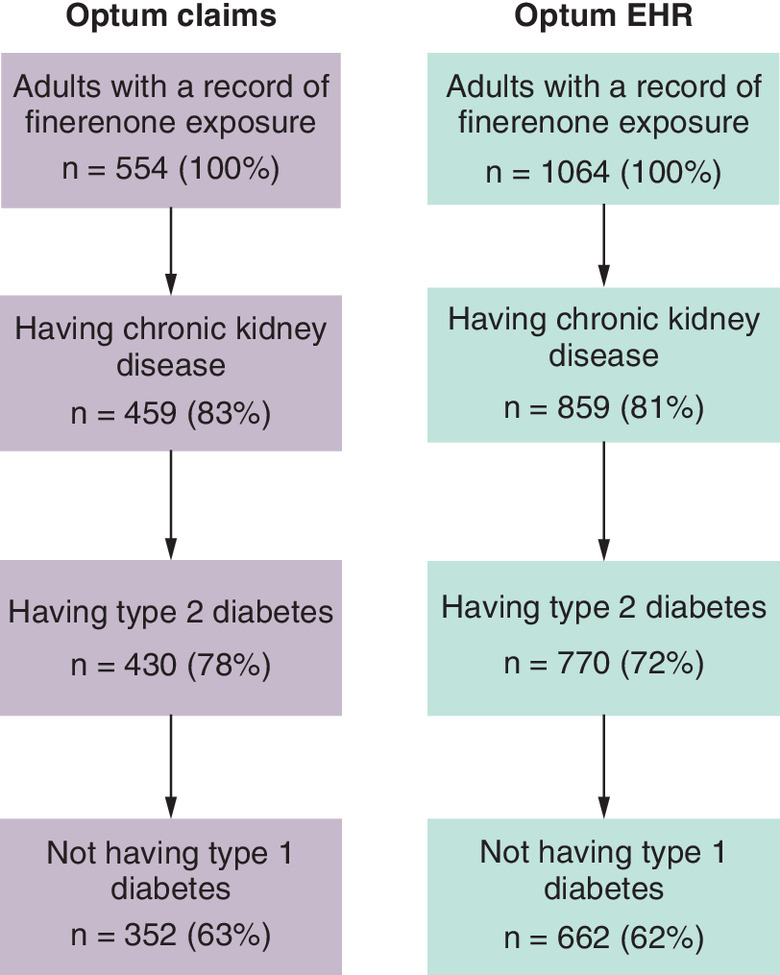
We conducted a multi-database, observational, cross-sectional study of early adopters of finerenone, using data from two US commercially available databases converted into the Observational Medical Outcomes Partnership (OMOP) common data model (CDM): Optum's de-identified Clinformatics® Data Mart Database (Optum CDM; hereafter referred to as Optum Claims; OptumInsight, MN), and Optum EHR (electronic health records). The observation period ran from August 2021 to September 2022, for Optum EHR and from August 2021 to March 2022, for Optum claims. Three non-mutually exclusive cohorts of finerenone initiators were included: those with prior CKD and T2D, those with prior CKD and T2D and concomitant SGLT2i use and those with prior CKD and T2D stratified according to urine albumin–creatinine ratio (UACR) recorded in the last 365 days before finerenone initiation (UACR below 30 mg/g, UACR between 30 and 300 mg/g, and UACR above 300 mg/g). This resulted in a total of five cohorts generated and described using the ATLAS tool developed by Observational Health Data Sciences and Informatics (OHDSI) [15]. Patients with Type 1 diabetes, estimated glomerular filtration rate (eGFR) <15 ml/min/1.73 m2, CKD stage 5 or on dialysis, or kidney transplant, on or before the index date were excluded from the study. Attrition of cohorts is shown in Figure 1.
The index event was defined as the first record indicating a finerenone prescription (Optum EHR) or a finerenone dispensation (Optum Claims). For cohort number 2, concomitant SGLT2i was defined as having a drug exposure to SGLT2i between 90 days before and 30 days after the index date. We used the 30 days after rule to account for co-initiation with finerenone with a potential date misspecification. CKD was defined as having either a diagnostic code for CKD, two eGFR measurements between 15 and 60 ml/min/1.73 m2 recorded between 90 and 548 days apart, or two UACR measurements ≥30 mg/g recorded between 90 and 548 days apart, the second of these measurements was considered the qualifying event for CKD onset. T2D was defined as having at least one diagnostic code for T2D. For the classification of patients into any of the three UACR categories, we used an algorithm based on UACR measurement records available during the 365 days before initiating finerenone. We considered a patient in the UACR<30 mg/g when there was at least one UACR measurement higher than 0 and below 30 mg/g, and no measurement of 30 mg/g or more. We considered a patient in the UACR 30–300 mg/g when there was at least one UACR measurement of 30 mg/g or higher and below 300 mg/g, and no measurement of 300 mg/g or more. Finally, we considered a patient in the UACR≥300 mg/g when there was at least one UACR measurement of 300 mg/g or higher.
Data sources
Optum Claims is a database, is a de-identified database is derived from a large adjudicated claims data warehouse. The Optum Claims database contains pharmacy claims that allow longitudinal tracking of medication refill patterns and changes in medications. Medical claims or encounter data are collected from all available healthcare sites. Additionally, Optum Claims includes results for outpatient laboratory tests processed by large national vendors.
The Optum EHR database contains electronic health records information from multispecialty practices, small group practices, physician providers, and integrated delivery networks throughout the US. The data contain demographic characteristics, medical history, and diagnoses for all types of encounters within the network, in-hospital procedures, physician prescriptions, and laboratory data for patients receiving care in contributing health systems.
Both databases were converted to the Observational Medical Outcomes Partnership (OMOP) common data model (CDM) prior to executing the analyses described in the following sections. Data quality assurance was applied before, during and after the ‘extraction, transformation and load’ process.
Variables
The following variables were used to describe patients: sociodemographic characteristics (age, sex, race), blood pressure, Charlson index [16], eGFR, UACR (1), CV risk factors (hypertension and hyperlipidemia), CV comorbidities (peripheral vascular disease, congestive heart failure coronary heart disease, acute coronary syndrome, and stroke), and complications of diabetes (retinopathy and neuropathy). The severity of diabetes was defined by the Diabetes Severity Complications Index [17]. Use of common treatments such as antihypertensives and anti-hyperglycemics was also described. For CV comorbidities, and complications of diabetes, we defined the occurrence of each condition as the presence of one diagnostic code ever in the available patient clinical history. For the rest of variables, we established a baseline period of 365 days prior to the finerenone initiation date. Missing data for lab measurements and sociodemographic variables were not imputed.
Statistical analysis
All continuous variables were summarized using mean or median and standard deviation (SD) or interquartile range (IQR), as appropriate, and all categorical variables were described as absolute (n) and relative (%) frequencies. Each database and cohort were analyzed and reported separately. No sample size was calculated, as all patients meeting the study eligibility criteria were included in the study cohorts. This analysis was planned as part of a larger study evaluating the real-world effectiveness of finerenone (NCT05703880; https://clinicaltrials.gov/ct2/show/NCT05703880). All analyses were conducted using ATLAS version 2.13.0.
Results
Optum claims
A total of 353 patients with CKD and T2D who started treatment with finerenone were identified (Table 1). Overall, mean (SD) age was 72.0 (8.3) years, 46.7% of patients were female, mean (SD) Charlson index was 7.3 (2.4), median (IQR) eGFR was 44 (35–54) ml/min/1.73 m2, and median (IQR) UACR 132 (28–698.0) mg/g. The most common comorbidities were hypertension (98.0%), peripheral vascular disease (66.6%), congestive heart failure (34.3%), and coronary heart disease (14.2%).
| Finerenone initiators (n = 353; 100%) | Finerenone initiators with SGLT2i co-prescription (n = 137; 38.9%) | Finerenone initiators with UACR <30 mg/g (n = 32; 9.0%) | Finerenone initiators with UACR 30–300 mg/g (n = 53; 15.0%) | Finerenone initiators with UACR >300 mg/g (n = 51; 14.4%) | |
|---|---|---|---|---|---|
| Sociodemographic characteristics | |||||
| Age, years, mean (SD) | 72.0 (8.3) | 69.7 (8.0) | 72 (9.6) | 73.6 (6.9) | 71.5 (8.5) |
| Age, 5-years categories, n (%) | |||||
| 45–49 | 6 (1.7) | 3 (2.2) | 1 (3.1) | 2 (3.9) | |
| 50–54 | 5 (1.4) | 3 (2.2) | |||
| 55–59 | 18 (5.1) | 10 (7.3) | 3 (9.4) | 2 (3.8) | 2 (3.9) |
| 60–64 | 18 (5.1) | 9 (6.6) | 1 (3.1) | 2 (3.9) | |
| 65–69 | 79 (22.4) | 40 (29.2) | 8 (25) | 12 (22.6) | 14 (27.5) |
| 70–74 | 91 (25.8) | 40 (29.2) | 6 (18.8) | 20 (37.7) | 9 (17.6) |
| 75–79 | 79 (22.4) | 20 (14.6) | 6 (18.8) | 9 (17) | 14 (27.5) |
| 80–84 | 35 (9.9) | 6 (4.4) | 5 (15.6) | 6 (11.3) | 7 (13.7) |
| 85–89 | 16 (4.5) | 6 (4.4) | 1 (3.1) | 1 (1.9) | |
| 90–94 | 6 (1.7) | 1 (3.1) | 3 (5.7) | 1 (2) | |
| Sex, n (%) | |||||
| Male | 188 (53.3) | 76 (55.5) | 17 (53.1) | 26 (49.1) | 24 (47.1) |
| Female | 165 (46.7) | 61 (44.5) | 15 (46.9) | 27 (50.9) | 27 (52.9) |
| Race, n (%) | |||||
| White | 158 (44.8) | 47 (34.3) | 13 (40.6) | 22 (41.5) | 22 (43.1) |
| Black or African–American | 65 (18.4) | 26 (19.0) | 7 (21.9) | 6 (11.3) | 4 (7.8) |
| Asian | 26 (7.4) | 17 (12.4) | 1 (3.1) | 6 (11.3) | 6 (11.8) |
| Charlson index - Romano adaptation, mean (SD) | 7.3 (2.4) | 7.2 (2.4) | 6.9 (2.6) | 7.3 (2.5) | 7.8 (2.1) |
| Physical examination | |||||
| Systolic BP, mm Hg, mean (SD) | 138.3 (20.8) | 139.2 (20.8) | 134.7 (16.7) | 132.3 (21.8) | 149.4 (23.2) |
| Diastolic BP, mm Hg, mean (SD) | 74 (14.8) | 74 (20.2) | 75.1 (10.5) | 73.8 (9.4) | 80.2 (11.1) |
| Laboratory data | |||||
| eGFR (as reported), ml/min/1.73 m2, median (IQR) | 44 (35–54) | 43 (34–55) | 50 (38–58) | 44 (36–54) | 46 (34–57) |
| UACR, mg/g, median (IQR) | 132 (28–698) | 93 (23–327) | 7 (3–12) | 72 (38–147) | 855 (463–1606) |
| Diabetes data | |||||
| Diabetes comorbidity severity index, mean (SD) | 5.9 (2.3) | 5.7 (2.0) | 5.8 (2.3) | 5.8 (2.2) | 6.4 (2.6) |
| Microvascular complications | |||||
| Neuropathy, n (%) | 189 (53.5) | 71 (51.8) | 20 (62.5) | 25 (47.2) | 29 (56.9) |
| Retinopathy, n (%) | 125 (35.4) | 46 (33.6) | 9 (28.1) | 17 (32.1) | 25 (49) |
| Cardiovascular risk factors‡ | |||||
| Hypertension, n (%) | 346 (98) | 135 (98.5) | 30 (93.8) | 53 (100) | 51 (100) |
| Hyperlipidemia, n (%) | 309 (87.5) | 123 (89.8) | 28 (87.5) | 49 (92.5) | 48 (94.1) |
| History of cardiovascular disease‡ | |||||
| Peripheral vascular disease, n (%) | 235 (66.6) | 90 (65.7) | 22 (68.8) | 43 (81.1) | 35 (68.6) |
| Congestive heart failure, n (%) | 121 (34.3) | 55 (40.1) | 9 (28.1) | 20 (37.7) | 19 (37.3) |
| Coronary heart disease, n (%) | 50 (14.2) | 20 (14.6) | 5 (15.6) | 9 (17) | 7 (13.7) |
| Acute coronary syndrome, n (%) | 35 (9.9) | 12 (8.8) | 5 (15.6) | 4 (7.5) | 4 (7.8) |
| Stroke, n (%) | 23 (6.5) | 6 (4.4) | 3 (9.4) | 1 (1.9) | 6 (11.8) |
| Drugs use at baseline† | |||||
| Cardiovascular drugs | |||||
| ACEI, n (%)/ARB, n (%) (Total) | 249 (70.5) | 104 (75.9) | 21 (65.6) | 44 (83.0) | 41 (80.4) |
| ACEI, n (%) | 150 (42.5) | 63 (46) | 12 (37.5) | 30 (56.6) | 27 (52.9) |
| ARB, n (%) | 187 (53.0) | 78 (56.9) | 17 (53.1) | 30 (56.6) | 31 (60.8) |
| Beta-blockers, n (%) | 212 (60.1) | 83 (60.6) | 20 (62.5) | 32 (60.4) | 42 (82.4) |
| CCB, n (%) | 178 (50.4) | 69 (50.4) | 15 (46.9) | 34 (64.2) | 35 (68.6) |
| Loop diuretics, n (%) | 142 (40.2) | 54 (39.4) | 14 (43.8) | 24 (45.3) | 20 (39.2) |
| Glucose-lowering therapies | |||||
| Total, n (%) | 321 (90.9) | 136 (99.3) | 30 (93.8) | 50 (94.3) | 49 (96.1) |
| Insulins and analogues, n (%) | 164 (46.5) | 68 (49.6) | 12 (37.5) | 26 (49.1) | 27 (52.9) |
| Metformin, n (%) | 152 (43.1) | 69 (50.4) | 17 (53.1) | 26 (49.1) | 26 (51.0) |
| SGLT2 inhibitors, n (%) | 150 (42.5) | 132 (96.4) | 17 (53.1) | 24 (45.3) | 22 (43.1) |
| GLP-1 agonists, n (%) | 124 (35.1) | 69 (50.4) | 14 (43.8) | 21 (39.6) | 22 (43.1) |
| Sulfonylurea, n (%) | 82 (23.2) | 36 (26.3) | 8 (25.0) | 15 (28.3) | 9 (17.6) |
| DPP-4 inhibitors, n (%) | 66 (18.7) | 34 (24.8) | 6 (18.8) | 14 (26.4) | 9 (17.6) |
†
365 days prior up to and including the index day.
‡
Any time prior to index.
ACEI: Angiotensin-converting enzyme inhibitor; ARB: Angiotensin, receptor blocker; BP: Blood pressure; CCB: Calcium channel blockers; CKD: Chronic kidney disease; DPP-4: Dipeptidyl peptidase-4; eGFR: Estimated glomerular filtration rate; GLP-1: Glucagon-like peptide 1; SGLT2: Sodium-glucose cotransporter-2; T2D: Type 2 diabetes; UACR: Urine albumin-to-creatinine ratio.
With regard to treatments, 249 patients (70.5%) received ACEi or ARB at baseline and almost all patients (90.9%) had records for glucose-lowering medications. Almost half of the patients (46.5%) were using insulin and analogs, followed by metformin (43.1%), SGLT2i (42.5%), and glucagon-like peptide-1 receptor agonists (GLP-1RA) (35.1%).
Overall, 137 (38.9%) finerenone initiators received SGLT2i concomitantly (Table 1). Compared with the overall population, patients were slightly younger (mean 69.7 years) and more frequently male (55.5%). Median (IQR) eGFR was 43, IQR: 34–55) ml/min/1.73 m2), and median (IQR) UACR 93 (23–327 mg/g). In addition, more patients had heart failure (40.1%), and received ACEi or ARB (75.9%) and glucose-lowering therapies (99.3%), more frequently at baseline.
Among finerenone initiators, 32 patients (9.0%) had a UACR <30 mg/g, 53 (15.0%) a UACR between 30 and 300 mg/g, and 51 (14.4%) a UACR >300 mg/g. Compared with the overall cohort, retinopathy was more frequent in the UACR >300 mg/g subgroup, and treatment prescription/dispensation with ACEi or ARB was more common in the UACR 30–300 mg/g and in the UACR >300 mg/g subgroups. Likewise, the proportion of patients with records for glucose-lowering therapies at baseline was higher in the UACR 30–300 mg/g (94.3%) and the UACR >300 mg/g (96.1%) subgroups compared to the overall cohort of finerenone initiators, with insulin and GLP-1RA being the most common anti-hyperglycemics used at baseline in these categories (Table 1).
Optum EHR
A total of 662 patients with CKD and T2D who started treatment with finerenone were identified (Table 2). Overall, mean (SD) age was 68.4 (10.5) years, 46.1% of patients were female, mean (SD) Charlson index was 6.5 (2.4), median (IQR) eGFR was 44 (33–60) ml/min/1.73 m2, and median (IQR) UACR 365 (74–1185.4) mg/g. Similarly to Optum Claims, the most frequent comorbidities recorded were hypertension (97.1%), peripheral vascular disease (57.6%), congestive heart failure (26.7%), and coronary heart disease (9.4%).
| Finerenone initiators (n = 662; 100%) | Finerenone initiators with SGLT2i co-prescription (n = 316; 47.7%) | Finerenone initiators with UACR <30 mg/g (n = 42; 6.3%) | Finerenone initiators with UACR 30–300 mg/g (n = 134; 20.2%) | Finerenone initiators with UACR >300 mg/g (n = 183; 27.6%) | |
|---|---|---|---|---|---|
| Sociodemographic characteristics | |||||
| Age, years, mean (SD) | 68.4 (10.5) | 67.2 (10.6) | 73.4 (7.4) | 68 (11.8) | 65.9 (11.2) |
| Age, 5-years categories, n (%) | |||||
| 30–34 | 2 (0.3) | 1 (0.3) | 2 (1.5) | ||
| 35–39 | 3 (0.5) | 3 (0.9) | 1 (0.7) | 2 (1.1) | |
| 40–44 | 7 (1.1) | 4 (1.3) | 1 (0.7) | 3 (1.6) | |
| 45–49 | 16 (2.4) | 10 (3.2) | 4 (3) | 8 (4.4) | |
| 50–54 | 37 (5.6) | 20 (6.3) | 8 (6) | 13 (7.1) | |
| 55–59 | 63 (9.5) | 37 (11.7) | 15 (11.2) | 24 (13.1) | |
| 60–64 | 90 (13.6) | 49 (15.5) | 4 (9.5) | 17 (12.7) | 29 (15.8) |
| 65–69 | 115 (17.4) | 52 (16.5) | 10 (23.8) | 21 (15.7) | 31 (16.9) |
| 70–74 | 121 (18.3) | 50 (15.8) | 11 (26.2) | 23 (17.2) | 28 (15.3) |
| 75–79 | 117 (17.7) | 54 (17.1) | 10 (23.8) | 23 (17.2) | 25 (13.7) |
| 80–84 | 55 (8.3) | 25 (7.9) | 2 (4.8) | 8 (6) | 12 (6.6) |
| 85–89 | 35 (5.3) | 11 (3.5) | 5 (11.9) | 11 (8.2) | 7 (3.8) |
| 90–94 | |||||
| Sex, n (%) | |||||
| Male | 357 (53.9) | 189 (59.8) | 21 (50) | 57 (42.5) | 114 (62.3) |
| Female | 305 (46.1) | 127 (40.2) | 21 (50) | 77 (57.5) | 69 (37.7) |
| Race, n (%) | |||||
| White | 420 (63.4) | 190 (60.1) | 29 (69) | 81 (60.4) | 104 (56.8) |
| Black or African–American | 134 (20.2) | 64 (20.3) | 11 (26.2) | 25 (18.7) | 46 (25.1) |
| Asian | 23 (3.5) | 12 (3.8) | 3 (2.2) | 10 (5.5) | |
| Charlson index – Romano adaptation, mean (SD) | 6.5 (2.4) | 6.4 (2.4) | 7 (3) | 6.2 (2.3) | 6.3 (2.1) |
| Physical examination | |||||
| Systolic BP, mm Hg, mean (SD) | 134.8 (23.8) | 133 (23.2) | 135.6 (23.7) | 128.8 (18.8) | 142.3 (22.2) |
| Diastolic BP, mm Hg, mean (SD) | 72.4 (12.8) | 73.5 (12.1) | 69.3 (14.3) | 72.7 (11.5) | 77.8 (11.3) |
| Laboratory data | |||||
| eGFR (as reported), ml/min/1.73 m2, median (IQR) | 44 (33–60) | 45 (35–60) | 44 (33–55) | 46 (33–63) | 48 (35–64) |
| UACR, mg/g, median (IQR) | 365 (74–1185.4) | 300 (80–861) | 10.3 (6.2–21) | 78.7 (43–136) | 910.2 (465.9–1882.8) |
| Diabetes data | |||||
| Diabetes comorbidity severity index, mean (SD) | 5.7 (2.5) | 5.7 (2.5) | 5.8 (2.5) | 5.2 (2.3) | 5.9 (2.5) |
| Microvascular complications | |||||
| Neuropathy, n (%) | 274 (41.4) | 124 (39.2) | 18 (42.9) | 56 (41.8) | 84 (45.9) |
| Retinopathy, n (%) | 141 (21.3) | 70 (22.2) | 7 (16.7) | 24 (17.9) | 55 (30.1) |
| Cardiovascular risk factors‡ | |||||
| Hypertension, n (%) | 643 (97.1) | 309 (97.8) | 41 (97.6) | 127 (94.8) | 181 (98.9) |
| Hyperlipidemia, n (%) | 518 (78.2) | 253 (80.1) | 32 (76.2) | 111 (82.8) | 152 (83.1) |
| History of cardiovascular disease‡ | |||||
| Peripheral vascular disease, n (%) | 381 (57.6) | 187 (59.2) | 28 (66.7) | 66 (49.3) | 108 (59) |
| Congestive heart failure, n (%) | 177 (26.7) | 78 (24.7) | 11 (26.2) | 30 (22.4) | 39 (21.3) |
| Coronary heart disease, n (%) | 62 (9.4) | 29 (9.2) | 7 (16.7) | 13 (9.7) | 17 (9.3) |
| Acute coronary syndrome, n (%) | 88 (13.3) | 46 (14.6) | 8 (19) | 17 (12.7) | 23 (12.6) |
| Stroke, n (%) | 62 (9.4) | 31 (9.8) | 6 (14.3) | 7 (5.2) | 20 (10.9) |
| Drugs use at baseline† | |||||
| Cardiovascular drugs | |||||
| ACEI, n (%)/ARB, n (%) (Total) | 466 (70.4) | 228 (72.2) | 27 (64.3) | 85 (63.4) | 146 (79.8) |
| ACEI, n (%) | 308 (46.5) | 152 (48.1) | 20 (47.6) | 48 (35.8) | 106 (57.9) |
| ARB, n (%) | 332 (50.2) | 155 (49.1) | 20 (47.6) | 63 (47) | 106 (57.9) |
| Beta-blockers, n (%) | 415 (62.7) | 201 (63.6) | 25 (59.5) | 73 (54.5) | 111 (60.7) |
| CCB, n (%) | 359 (54.2) | 182 (57.6) | 22 (52.4) | 52 (38.8) | 122 (66.7) |
| Loop diuretics, n (%) | 303 (45.8) | 136 (43) | 11 (26.2) | 47 (35.1) | 80 (43.7) |
| Glucose-lowering therapies | |||||
| Total, n (%) | 627 (94.7) | 315 (99.7) | 37 (88.1) | 128 (95.5) | 177 (96.7) |
| Insulins and analogues, n (%) | 389 (58.8) | 195 (61.7) | 14 (33.3) | 65 (48.5) | 122 (66.7) |
| SGLT2 inhibitors, n (%) | 353 (53.3) | 308 (97.5) | 20 (47.6) | 87 (64.9) | 104 (56.8) |
| Metformin, n (%) | 348 (52.6) | 188 (59.5) | 25 (59.5) | 85 (63.4) | 102 (55.7) |
| GLP-1 agonists, n (%) | 279 (42.1) | 170 (53.8) | 16 (38.1) | 70 (52.2) | 74 (40.4) |
| Sulfonylureas, n (%) | 165 (24.9) | 78 (24.7) | 15 (35.7) | 32 (23.9) | 39 (21.3) |
| DPP-4 inhibitors, n (%) | 117 (17.7) | 58 (18.4) | 8 (19) | 26 (19.4) | 35 (19.1) |
†
365 days prior up to and including the index day.
‡
Any time prior to index.
ACEI: Angiotensin-converting enzyme inhibitor; ARB: Angiotensin, receptor blocker; BP: blood pressure; CCB: Calcium channel blocker; CKD: Chronic kidney disease; DPP-4: Dipeptidyl peptidase-4; eGFR: Estimated glomerular filtration rate; GLP-1: Glucagon-like peptide 1; SGLT2: Sodium-glucose cotransporter-2; T2D: Type 2 diabetes; UACR: Urine albumin-to-creatinine ratio.
Regarding treatments, 466 patients (70.4%) had records for ACEi or ARB at baseline and almost all patients (94.7%) were receiving glucose-lowering medications. 58.8% of patients were using insulin and analogs, followed by SGLT2i (53.3%), metformin (52.6%), and GLP-1RA (42.1%).
There was evidence of concomitant use of finerenone and SGLT2i in 316 finerenone initiators (47.7%) (Table 2). Among these, and compared with the overall population, age was quite similar (mean 67.2 years), but patients were more commonly male (59.8%). Median (IQR) eGFR was 45 (35–60) ml/min/1.73 m2), and median (IQR) UACR 300 (80–861) mg/g. Of note, the proportion of patients with heart failure (24.7%), as well as those taking ACEi or ARB (72.2%), was similar to that in the overall population. There was ubiquitous concomitant use of glucose-lowering therapies (99.7%), particularly metformin (59.5%) and GLP-1RA (53.8%).
Among finerenone initiators, 42 patients (6.3%) had a UACR <30 mg/g, 134 (20.2%) a UACR between 30 and 300 mg/g, and 183 (27.6%) had a UACR >300 mg/g. At baseline, eGFR was higher, on average, among patients in the 30–300 mg/g and in the UACR >300 mg/g subgroups compared with the overall cohort. Retinopathy was more common in the UACR >300 mg/g subgroup, whereas neuropathy appeared to be similar across all UACR levels at baseline. With regard to baseline treatments, concomitant use ACEi or ARB and total glucose-lowering therapies appeared slightly higher in the UACR >300 mg/g subgroup (79.8 and 96.7%, respectively) compared with the overall cohort (70.4 and 94.7%, respectively). In addition, the proportion of patients taking insulin was highest among patients within the UACR >300 mg/g subgroup. The highest proportion of patients taking metformin, SGLT2i, and GLP-1RA was observed in the subgroup of patients with a UACR between 30 and 300 mg/g (Table 2).
Discussion
Our study, analyzing real-world data from the USA, shows that finerenone has been used across a broad range of clinical and demographic characteristics during the initial months of availability after its marketing-authorization approval. The results point toward the use of finerenone as a complementary mode of action to other renal and CV protective drugs recommended for patients with CKD and T2D such as ACEi, ARB and SGLT2i.
Of note, our study aimed to describe patients who started finerenone, stratifying by relevant characteristics such as concurrent SGLT2i use and UACR categories, where available. To incorporate elements of the US FDA label [12], we restricted the Entry Cohort Event (initiation of finerenone) using the inclusion criteria specified in the methods (1. aged 18 years or older, 2. having CKD, 3. having T2D, and 4. not having T1D). The more elements we included to restrict our cohort definition, such as eGFR between 25 and 90 ml/min/1.73 m2, the closer we would get to the definition used in the clinical trials and to the approved indication but at the expense of the sensitivity of a cohort that contained the patients using finerenone in real-world practice in the US. In a comparative setting, one would aim to narrow the definition to the specific label indication for larger internal validity, but the descriptive nature of our study warranted a focus on external validity to enhance generalizability.
Clinical practice shortly after finerenone availability seems to be in line with KDIGO recommendations, which position finerenone on top of RAS inhibition, with and without SGLT2i, as a drug to reduce CV and kidney risk in patients with T2D and CKD with albuminuria (UACR ≥30 mg/g) [1]. Furthermore, our study showed that around 40–50% of patients initiating finerenone received an SGLT2i during the 90 days before or the 30 days after initiating finerenone. In fact, a sensitivity analysis indicated that 10% of patients received an SGLT2i during the 30 days after finerenone initiation, suggesting a potential co-initiation of therapies.
Early intervention and intensive treatment is essential to reduce both CV and renal complications in patients with CKD and T2D [18]. Different clinical trials have shown the benefits of ACEi, ARB and SGLT2i to decrease CV outcomes and CKD progression among patients with CKD and T2D [5,19,20]. However, inflammation and fibrosis promoted by MR overactivation are generally not targeted by these therapies, leading to a persistent residual risk [21,22]. Consequently, it is necessary to perform a comprehensive approach that acts on the broader pathogenesis of CV and kidney disease. For example, SGLT2i act primarily on the hemodynamic and metabolic drivers of CKD progression, whereas finerenone appears to have a wider role on inflammation and fibrosis [23–25]. Despite the CONFIDENCE trial providing definite information about the effects of combining SGLT2i and finerenone in this population [26], it is important to ascertain how finerenone is being used in clinical practice, particularly with the concomitant use of both drugs.
Information about the use of finerenone in routine clinical practice is warranted. Consequently, our results are of great interest. In our study, mean age was 68–72, years, median eGFR 44 ml/min/1.73 m2, and median UACR 110–339 mg/g. Previous studies performed in European populations of patients with CKD and T2D have shown a similar clinical profile to that observed in our study [27,28]. In the FIDELITY pooled analysis, which combined data from the FIGARO and FIDELIO trials, mean age was 64.8 years, 30.2% of patients were female, baseline eGFR was 57.6 ml/min/1.73 m2, and baseline UACR 515 mg/g [10]. Therefore, compared with FIDELITY, our study's cohort of finerenone users seemed older, with worse renal function, but lower UACR on average.
Regarding baseline treatments, around 70.5% of patients were taking ACEi or ARB, 42–54% SGLT2i and 35–42% GLP-1RA. Compared with the overall population, patients taking concomitant SGLT2i had lower eGFR and UACR. This proportion of ACEi and ARB use is similar to that observed in prior observational studies of patients with CKD and T2D [28–30]. In FIDELITY, almost all patients were receiving RAS inhibitors, 7% SGLT2i and GLP-1RA, and the CV and renal benefits of finerenone were independent of treatment with SGLT2i and GLP-1RA [10,31]. Our data indicate that the combined use of finerenone and SGLT2i was significant in clinical practice independent of background therapies and clinical characteristics, potentially suggesting a healthcare practice acceptance of the complementary modes of action of finerenone and SGLT2i. Of note, the CONFIDENCE trial is a phase 2 study that is currently investigating the safety, tolerability and efficacy of the combination of empagliflozin with finerenone in 807 adults with T2D, stage 2–3 CKD, and UACR ≥300–<5000 mg/g [26].
Our study has some limitations which need to be considered when interpreting the results. This was a cross-sectional study using secondary databases, thus only anonymized data that had been recorded in the database could be collected. These data may not include all relevant information about a patient's health status or medical history, particularly if the patient has received care from multiple healthcare providers or institutions. Optum Claims contains records for drug dispensations which supposedly accurately reflect actual drug exposures, but we could not determine if patients were actually taking the drugs as indicated. Of note, the only element in our study design that contained data post-index was when we defined concomitant use of SGLT2i as an inclusion criterion for cohort number 2. We did so because concomitant use in the context of this cohort definition means evidence of use of SGLT2i around the initiation of finerenone; not necessarily only before but also shortly after. In addition, there could be a misspecification of the date in the database of origin thus a patient may have been indicated to start SGLT2i treatment on a given date but may not be recorded in the database until days or weeks later. Consequently, we included a 30-day post-index allowance to identify a record for SGLT2i exposure closely related to finerenone initiation. On the other hand, Optum EHR contains information on drug prescriptions which may or may not reflect actual dispensation and exposure to the drug. Moreover, drug prescriptions for chronic treatments in the US may be revised with a low frequency, since prescribers often rely on the patient getting refills periodically, thus a prescription may be a proxy for actual drug exposure even months later. When it comes to condition diagnoses, claims databases reflect the administrative management of the reimbursement schema of the patient, whereas EHR database reflect actual diagnoses made in a healthcare setting where patients are managed. In addition, Optum Claims has limited data availability when it comes to laboratory measurements, thus variables using eGFR or UACR constructs may not be complete. On the other hand, Optum EHR contains a more systematic collection of laboratory values. This notably affected our stratification by UACR, which is already impacted by low adherence to UACR monitoring recommendations in the US [32]; from the large proportion of patients without an identifiable record for UACR at baseline, we could not disentangle whether it is because of it not being monitored or because of it not being recorded in the database. This, along with the high intrapersonal variability of UACR, may cause a certain degree of misclassification of patients according to baseline UACR levels. Our study uses data from July 2021, when finerenone was approved in the US, until the most recent data available (September 2022 for Optum EHR and March 2022 for Optum Claims). This has two immediate consequences on our study. First, there is limited uptake appearing in the databases, therefore limiting the sample size of our study. Second, our study reflects a population of early adopters of finerenone. Regarding the former, despite the limited sample size compared with other studies using secondary real-world data, our results show consistency between databases, and we provided a comprehensive overview of the precision of continuous variables. In fact, we did not attempt to test comparative hypotheses, thus not affecting type II error probability due to low sample size. For the latter, we anticipate that the patient profile may change as more evidence and experience of real-world finerenone use becomes available. This is partially compensated by using the OMOP CDM and the OHDSI tools, as we were able to replicate the results of our analysis in two complementary databases, one administrative claims and one EHR, without affecting study design and assumptions, and, therefore, obtained a more comprehensive picture of the characteristics of patients. Furthermore, the analysis can easily be reproduced in other suitable data sources converted into OMOP CDM. To further enhance the transparency of our research conduct, our cohort definitions, concept sets, and Json scripts are available as Supplementary Materials to this publication. Retrospective claims database studies are observational in nature, so they cannot establish causality between exposure and outcome. Lack of generalizability may influence the results, and alternative explanations for the findings cannot be ruled out. Our cohorts were generated using the most recently available data and it provides understanding on the characteristics of patients as finerenone becomes available in other countries. Although this information may be especially relevant to a specific patient population and not fully generalizable outside the US, it provides contemporary insights on the attitude of prescribers toward the use of finerenone in patients for whom this therapy could be beneficial.
Conclusion
This contemporary study showed that the use of finerenone in clinical practice in the US is mostly aligned with international clinical guidance in terms of patient profile. Current management of CKD and T2D patients potentially reflects the use of finerenone independently from background therapies and clinical characteristics, suggesting implementation of therapeutic strategies based on different modes of action to address underlying pathologies.
Summary points
•
Patients with chronic kidney disease (CKD) and Type 2 diabetes (T2D) have a high risk of CKD progression and the development of cardiovascular (CV) outcomes.
•
Despite treatment with renin-angiotensin system (RAS) inhibitors and SGLT2i, residual risk remains high.
•
Overactivation of the mineralocorticoid receptor plays a key role in the development of cardiac, vascular and renal complications in this population.
•
Clinical trials have demonstrated that finerenone significantly reduces the risk of developing CV and renal complications. However, data about the use of finerenone in clinical practice are lacking.
•
This study aimed to characterize a population of early adopters of finerenone in the US, focusing on demographic and clinical features, according to SGLT2i use status.
•
This was a multi-database, observational, cross-sectional study, using data from two US databases (Optum Clinformatics [Optum Claims] and Optum EHR).
•
Overall, 1014 patients were included, 352 from Optum Claims and 662 from Optum EHR: mean (SD) age 72.1(8.3)/68.4(10.5) years, median (IQR) eGFR 44 (35–75)/44 (32–57) ml/min/1.73 m2; median (IQR) UACR 110.0 (20.0–698.0)/339 (61–1143) mg/g), respectively.
•
70.5/70.4% were receiving RAS inhibitors, 42.3/53.5% SGLT2i.
•
Among finerenone initiators, 8.2/9.7% of patients had a baseline UACR <30 mg/g, 13.4/23.7% had UACR 30–300 mg/g, and 8.8/27.6% had UACR >300 mg/g.
•
The use of finerenone in clinical practice in the US is mostly aligned with international guidance in terms of patient profile and place in therapy.
Author contributions
D Vizcaya, C Kovesdy, A Reyes, E Pessina, P Pujol, G James, NG Oberprieler, contributed extensively to the work presented in this paper. All authors have contributed significantly to the conception, design, or acquisition of data, or analysis and interpretation of data. All authors have participated in drafting, reviewing, and/or revising the manuscript and have approved its submission.
Acknowledgments
The authors thank O Piqué-Duró, from University Pompeu Fabra, for assistance in reviewing the initial draft and quality control.
Financial & competing interests disclosure
The study is funded by Bayer AG. D Vizcaya, E Pessina, P Pujol, G James, A Reyes and NG Oberprieler are full-time employees of Bayer and may own stock. OP-D was master's intern student at Bayer Pharmaceuticals, Sant Joan Despí, the time of this study. CP Kovesdy has received consulting fees from Abbott, Akebia, Astra Zeneca, Bayer, Boehringer Ingelheim, Cara Therapeutics, CSL Vifor, GSK and ProKidney. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance was provided by Content Ed (Madrid, Spain) with funding from Bayer.
Ethical conduct of research
This study was conducted in accordance with Good Pharmacoepidemiology Practices. This analysis was planned as part of a larger study evaluating the real-world effectiveness of finerenone (NCT05703880; https://clinicaltrials.gov/ct2/show/NCT05703880).
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease Introduction. Kidney Int. 98(4S), S1–S115 (2020).
2.
Thomas MC, Cooper ME, Zimmet P. Changing epidemiology of type 2 diabetes mellitus and associated chronic kidney disease. Nat. Rev. Nephrol. 12(2), 73–81 (2016).
3.
Rodriguez-Poncelas A, Garre-Olmo J, Franch-Nadal J et al. Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrol. 14(1), 46 (2013).
4.
Wu B, Bell K, Stanford A et al. Understanding CKD among patients with T2DM: prevalence, temporal trends, and treatment patterns—NHANES 2007–2012. BMJ Open Diab. Res. Care. 4(1), e000154 (2016).
• In the US, the prevalence of chronic kidney disease (CKD) in patients with Type 2 diabetes (T2D) was 38.3%.
5.
Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N. Engl. J. Med. 329(20), 1456–1462 (1993).
6.
Wheeler DC, James J, Patel D et al. SGLT2 inhibitors: slowing of chronic kidney disease progression in Type 2 diabetes. Diabetes Ther. 11(12), 2757–2774 (2020).
7.
Baran W, Krzemińska J, Szlagor M et al. Mineralocorticoid receptor antagonists – use in chronic kidney disease. Int. J. Mol. Sci. 22(18), 9995 (2021).
8.
Bakris GL, Agarwal R, Anker SD et al. Effect of finerenone on chronic kidney disease outcomes in Type 2 diabetes. N. Engl. J. Med. 383(23), 2219–2229 (2020).
9.
Pitt B, Filippatos G, Agarwal R et al. Cardiovascular events with finerenone in kidney disease and Type 2 diabetes. N. Engl. J. Med. 385(24), 2252–2263 (2021).
10.
Agarwal R, Filippatos G, Pitt B et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur. Heart J. 43(6), 474–484 (2022).
•• Finerenone reduced the risk of CV and kidney outcomes in patients with T2D and CKD.
11.
EMA. Kerendia [product information website] (2022). www.ema.europa.eu/en/documents/product-information/kerendia-epar-product-information_en.pdf
12.
US FDA. Kerendia PI. Kerendia (finerenone) tablets. [Internet] (2021). www.accessdata.fda.gov/drugsatfda_docs/label/2021/215341s000lbl.pdf
13.
Canada's Drug and Health Technology Agency. Finerenone [Internet] (2023). www.cadth.ca/finerenone
14.
NICE. Finerenone for treating chronic kidney disease in people with type 2 diabetes. NICE Technology Appraisal Guidance [TA877] (2023). www.nice.org.uk/guidance/ta877
15.
OHDSI. The Book of OHDSI: Observational Health Data Sciences and Informatics. OHDSI (2019). https://ohdsi.github.io/TheBookOfOhdsi/OhdsiAnalyticsTools.html#atlas
16.
Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 91(1), 8–35 (2022).
17.
Glasheen WP, Renda A, Dong Y. Diabetes Complications Severity Index (DCSI) – update and ICD-10 translation. J. Diabetes Complications 31(6), 1007–1013 (2017).
18.
Handelsman Y, Butler J, Bakris GL et al. Early intervention and intensive management of patients with diabetes, cardiorenal, and metabolic diseases. J. Diabetes Complications 37(2), 108389 (2023).
19.
Heerspink HJ, Stefánsson BV, Correa-Rotter R et al. Dapagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 383(15), 1436–1446 (2020).
•• Among patients with CKD, dapagliflozin reduced the risk of CKD progression, regardless of the presence of T2D.
20.
Perkovic V, Jardine MJ, Neal B et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N. Engl. J. Med. 380(24), 2295–2306 (2019).
21.
Chaudhuri A, Ghanim H, Arora P. Improving the residual risk of renal and cardiovascular outcomes in diabetic kidney disease: a review of pathophysiology, mechanisms, and evidence from recent trials. Diabetes Obes. Metab. 24(3), 365–376 (2022).
22.
Terpening CM. Prevention of cardiovascular events in patients with chronic kidney disease. Ann. Pharmacother. 10600280231165774 (2023).
23.
Kolkhof P, Delbeck M, Kretschmer A et al. Finerenone, a novel selective nonsteroidal mineralocorticoid receptor antagonist protects from rat cardiorenal injury. J. Cardiovasc. Pharmacol. 64(1), 69–78 (2014).
24.
Zelniker TA, Braunwald E. Mechanisms of cardiorenal effects of sodium-glucose cotransporter 2 inhibitors. J. Am. Coll. Cardiol. 75(4), 422–434 (2020).
25.
Grune J, Beyhoff N, Smeir E et al. Selective mineralocorticoid receptor cofactor modulation as molecular basis for finerenone's antifibrotic activity. Hypertension 71(4), 599–608 (2018).
26.
Green JB, Mottl AK, Bakris G et al. Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using a UACR Endpoint study (CONFIDENCE). Nephrol. Dial. Transplant. 38(4), 894–903 (2023).
27.
González-Pérez A, Saéz ME, Vizcaya D, Lind M, García Rodríguez LA. Impact of chronic kidney disease definition on assessment of its incidence and risk factors in patients with newly diagnosed type 1 and type 2 diabetes in the UK: a cohort study using primary care data from the United Kingdom. Prim. Care Diabetes. 14(4), 381–387 (2020).
28.
Cunillera-Puértolas O, Vizcaya D, Cerain-Herrero MJ, Gil-Terrón N, Cobo-Guerrero S, Salvador-González B. Cardiovascular events and mortality in chronic kidney disease in primary care patients with previous type 2 diabetes and/or hypertension. A population-based epidemiological study (KIDNEES). BMC Nephrol. 23(1), 376 (2022).
29.
Kovesdy CP, Isaman D, Petruski-Ivleva N et al. Chronic kidney disease progression among patients with type 2 diabetes identified in US administrative claims: a population cohort study. Clin. Kidney J. 14(6), 1657–1664 (2021).
30.
Stengel B, Muenz D, Tu C et al. Adherence to the kidney disease: improving global outcomes ckd guideline in nephrology practice across countries. Kidney Int. Rep. 6(2), 437–448 (2021).
31.
Rossing P, Anker SD, Filippatos G et al. Finerenone in Patients With Chronic Kidney Disease and Type 2 Diabetes by Sodium–Glucose Cotransporter 2 Inhibitor Treatment: The FIDELITY Analysis. Diabetes Care 45(12), 2991–2998 (2022).
• In FIDELITY, the CV and renal benefits of finerenone were independent of treatment with SGLT2i.
32.
Folkerts K, Petruski-Ivleva N, Comerford E et al. Adherence to chronic kidney disease screening guidelines among patients withType 2 diabetes in a US Administrative Claims Database. Mayo Clin. Proc. 96(4), 975–986 (2021).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 12 May 2023
Accepted: 17 June 2023
Published online: 30 June 2023
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Characteristics of patients with chronic kidney disease and Type 2 diabetes initiating finerenone in the USA: a multi-database, cross-sectional study. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0076
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Csaba P. Kovesdy, Craig I. Coleman, Catherine B. Johannes, Anam M. Khan, Ryan Ziemiecki, J. Bradley Layton, David Vizcaya, Fangfang Liu, Nikolaus G. Oberprieler, Utilization and clinical characteristics of patients with type 2 diabetes and chronic kidney disease prescribed finerenone in the United States, Journal of Clinical & Translational Endocrinology, 10.1016/j.jcte.2026.100435, 44, (100435), (2026).
- Xiaoqing Deng, Yanyan Chen, Zhe Xu, Huan Wei, Yuqin Liao, Fangfang Liu, Alfredo E Farjat, Nikolaus G Oberprieler, Liming Chen, Clinical characteristics and outcomes of patients with type 2 diabetes mellitus and chronic kidney disease from two new-user medication cohorts: a retrospective cohort study using regional electronic health records database in China, BMJ Open, 10.1136/bmjopen-2025-106126, 15, 12, (e106126), (2025).
- Yu Sun, Mingzhu Wang, Role and application prospective of non-steroidal MRA in the treatment of diabetic kidney disease, International Urology and Nephrology, 10.1007/s11255-025-04456-8, 57, 8, (2567-2577), (2025).
- Csaba P. Kovesdy, Natalie Ebert, David Vizcaya, Michael Walsh, Mikhail N. Kosiborod, J. Bradley Layton, Ryan Ziemiecki, Catherine B. Johannes, Manel Pladevall-Vila, Patrick O. Gee, Nichole Jefferson, Annie Chicoye, Maria Lopes, Bishnu Bahadur Thapa, Gary Curhan, Luis Rangel, Mudit Bhartia, Fangfang Liu, Alfredo E. Farjat, Nikolaus G. Oberprieler, Change in Urine Albumin-Creatinine Ratio and Occurrence of Hyperkalemia in Patients Initiating Finerenone in the USA: A Cohort Study from the FOUNTAIN Platform, Nephron, 10.1159/000543923, 149, 7, (371-383), (2025).
- Nikolaus G. Oberprieler, Manel Pladevall-Vila, Catherine Johannes, J. Bradley Layton, Asieh Golozar, Martin Lavallee, Fangfang Liu, Maria Kubin, David Vizcaya, FOUNTAIN: a modular research platform for integrated real-world evidence generation, BMC Medical Research Methodology, 10.1186/s12874-024-02344-w, 24, 1, (2024).
- Susanne B. Nicholas, Ricardo Correa-Rotter, Nihar R. Desai, Lixin Guo, Sankar D. Navaneethan, Kevin M. Pantalone, Christoph Wanner, Stefanie Hamacher, Samuel T. Fatoba, Andrea Horvat-Broecker, Antonio Garreta-Rufas, Alain Gay, Martin Merz, David C. Wheeler, First interim results from FINE-REAL: a prospective, non-interventional, phase 4 study providing insights into the use and safety of finerenone in a routine clinical setting, Journal of Nephrology, 10.1007/s40620-024-02070-y, 37, 8, (2223-2232), (2024).
- Atsuhisa Sato, Daloha Rodriguez-Molina, Kanae Yoshikawa-Ryan, Satoshi Yamashita, Suguru Okami, Fangfang Liu, Alfredo Farjat, Nikolaus G. Oberprieler, Csaba P. Kovesdy, Keizo Kanasaki, David Vizcaya, Early Clinical Experience of Finerenone in People with Chronic Kidney Disease and Type 2 Diabetes in Japan—A Multi-Cohort Study from the FOUNTAIN (FinerenOne mUltidatabase NeTwork for Evidence generAtIoN) Platform, Journal of Clinical Medicine, 10.3390/jcm13175107, 13, 17, (5107), (2024).
- Yu. Sh. Khalimov, G. V. Semikova, Yu. A. Shutova, Novel cardioprotective and nephroprotective combination in patients with type 2 diabetes and chronic kidney disease: perspectives of use, Diabetes mellitus, 10.14341/DM13113, 27, 1, (93-103), (2024).
- Wenmin Chen, Lingqian Zheng, Jiali Wang, Yongda Lin, Tianbiao Zhou, Overview of the safety, efficiency, and potential mechanisms of finerenone for diabetic kidney diseases, Frontiers in Endocrinology, 10.3389/fendo.2023.1320603, 14, (2023).