PEG hydrogel sealant versus fibrin glue in posterior fossa surgery: an economic comparison across five European countries
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Posterior cranial fossa (PCF) surgery is associated with complications, including cerebrospinal fluid (CSF) leakage. Dural sealants such as polyethylene glycol (PEG)-based hydrogels and fibrin glue can prevent CSF leaks, with evidence suggesting PEG hydrogels may outperform fibrin glue. However, the budget impact of using PEG hydrogels in PCF surgeries in Europe is unclear. Materials & methods: A decision tree was developed based on a previous US model, to assess the budget impact of switching from fibrin glue to PEG hydrogel in PCF surgery across five European countries. Input costs were derived from published sources for the financial year 2022/2023. Health outcomes, including CSF leaks, were considered. Results: The model predicted that using PEG hydrogel instead of fibrin glue in PCF surgery can lead to cost savings in five European countries. Cost savings per patient ranged from EUR 419 to EUR 1279, depending on the country. Sensitivity analysis showed that the incidence of CSF leaks and pseudomeningoceles had a substantial impact on the model's results. Conclusion: PEG hydrogels may be a cost-effective alternative to fibrin glue in PCF surgery. The model predicted that cost savings would be mainly driven by a reduction in the incidence of postoperative CSF leaks, resulting in reduced reliance on lumbar drains, reparative surgery and shortened hospital stays.
Surgical interventions in the posterior cranial fossa (PCF) are the primary treatments for disorders like tumors, Chiari's malformations and brainstem decompression [1]. These procedures have varying success rates and bear inherent operative and postoperative risks of complications, with cerebrospinal fluid (CSF) leakage being a major concern and the most common non-neurological postoperative complication [2–6].
The incidence of CSF leaks varies in the literature between 4.4 and 13% in pediatric and adult patients, respectively [5,7–11]. However, the absence of established consensus on defining CSF leaks and diverse surgical approaches might partly explain the variance in reported incidences [7,12].
Postoperative CSF leaks, which can occur following deficient dural closure, can lead to serious complications such as increased risk of meningitis [13,14], wound infections [14,15], pseudomeningocele [16], resulting in extended hospital stays and increased healthcare costs.
A recent retrospective study in The Netherlands quantified the average additional economic burden of EUR 9700 per procedure in 2018. Prolonged inpatient stays by an average of 8.5 days, were the main contributor, with expenses rising to EUR 15,700 (2018) in cases requiring reoperation [16].
Preventing CSF leaks in PCF surgeries is critically dependent on attaining a watertight closure of the dura mater [17,18]. Optimal closure is often achieved using the long-established fibrin glue [19] or polyethylene glycol (PEG) derivatives with sealant characteristics [20]. PEG-based hydrogels have been demonstrated to outperform fibrin glue in reducing the incidence of postoperative CSF leaks by ∼80% and shortening hospital stays by ∼20% in PCF surgery patients [12,21].
Despite the clinical benefits, the economic implications of using PEG hydrogels instead of fibrin glue in PCF surgeries are not fully understood, especially in European healthcare contexts. A single previous study suggesting potential cost savings per procedure, mainly due to reduced hospitalization and management costs of CSF leaks, is limited to USA, a one-of-a-kind healthcare system that hardly compares to any European counterpart. Given this knowledge gap, this study aims to transpose and expand upon the health economics model by Carter [22] to the diverse healthcare systems of five European countries and provide an initial assessment of the potential cost impact of adopting a PEG hydrogel in place of fibrin glue in PCF surgeries.
Methods
We developed a decision tree based on a cost-benefit model from Carter [22] to estimate the budget impact of switching from fibrin glue to a PEG hydrogel. The model's adequacy for this evaluation and its adherence to current clinical practice in Europe were assessed GT and JAH, practicing neurosurgeons and co-authors of this manuscript. The model was subsequently reverse-engineered from the publication, using the descriptions and calculations laid out in the original publication [22]. This study abides by the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist and the International Society of Pharmacoeconomics and Outcomes Research (ISPOR) good practice guidelines [23,24].
Target population, setting & perspective
This model focused on patients who underwent PCF surgery. Health outcomes were considered for 19 months. After using the administration of a sealant, the costs associated with PCF surgeries and health outcomes in Belgium, France, Germany, Italy and UK were considered. The model took the perspective of the local hospital payer, with costs for the financial year 2022/2023 in EUR or GBP, as appropriate.
Setting & location
This study explored the hospital budget implications in Belgium, France, Germany, Italy and UK of switching from the standard of care (SOC) fibrin glue to the comparator in PCF surgeries from adjuvant administration throughout a 19-month observation period.
Study perspective
This study was designed to account for the hospital setting perspective in Belgium, France, Germany, Italy and UK.
Comparator
As presented by Than et al. [21], fibrin glue was regarded as the SOC in the investigated countries (Tisseel VH 4 ml; Baxter International, IL, USA). The chosen comparator was DuraSeal® Cranial Sealant System 5 ml (Integra LifeSciences, NJ, USA), a PEG hydrogel 4 ml approved for distribution in every target country.
Time horizon
The time horizon spanned 19 months, as in the original US model [22].
Discount rate
No discount rate was applied.
Choice of health outcomes
Health outcomes were chosen as provided by Than et al. [21] and represented the most significant safety outcomes associated with PCF surgery and sealant's effectiveness. The outcomes included CSF leaks at the incision site, pseudomeningoceles, wound infection, and aseptic meningitis. The postoperative complications correspond to those described by Than et al. [21]. Briefly, a CSF leak was defined as the clear exudation of fluid from a sealed wound. A pseudomeningoceles was a fluid accumulation distinguished exclusively by patient symptoms or clinical examination; radiographic diagnoses were not considered. Wound infections and meningitis were diagnosed by clinical examination and CSF culture. Each complication is assigned appropriate clinical management, schematized in Figure 1 & Table 1. A CSF is invariably treated through operative repair and five ensuing inpatient days. Only one in five pseudomeningoceles (20%) is treated by either operative repair (50%) or lumbar drain (50%) [4,25]; a five-day inpatient stay ensues. All wound infections undergo a seven-day antibiotic treatment and are assigned two outpatient visits. One in two aseptic meningitis receives lumbar drainage, CSF culture, seven-day antibiotics, two days in hospital, and one outpatient visit. The remaining 50% of aseptic meningitis are treated expectantly at two outpatient visits. All aseptic meningitis are prescribed steroids for either 14 (75%) or 112 (25%) days.
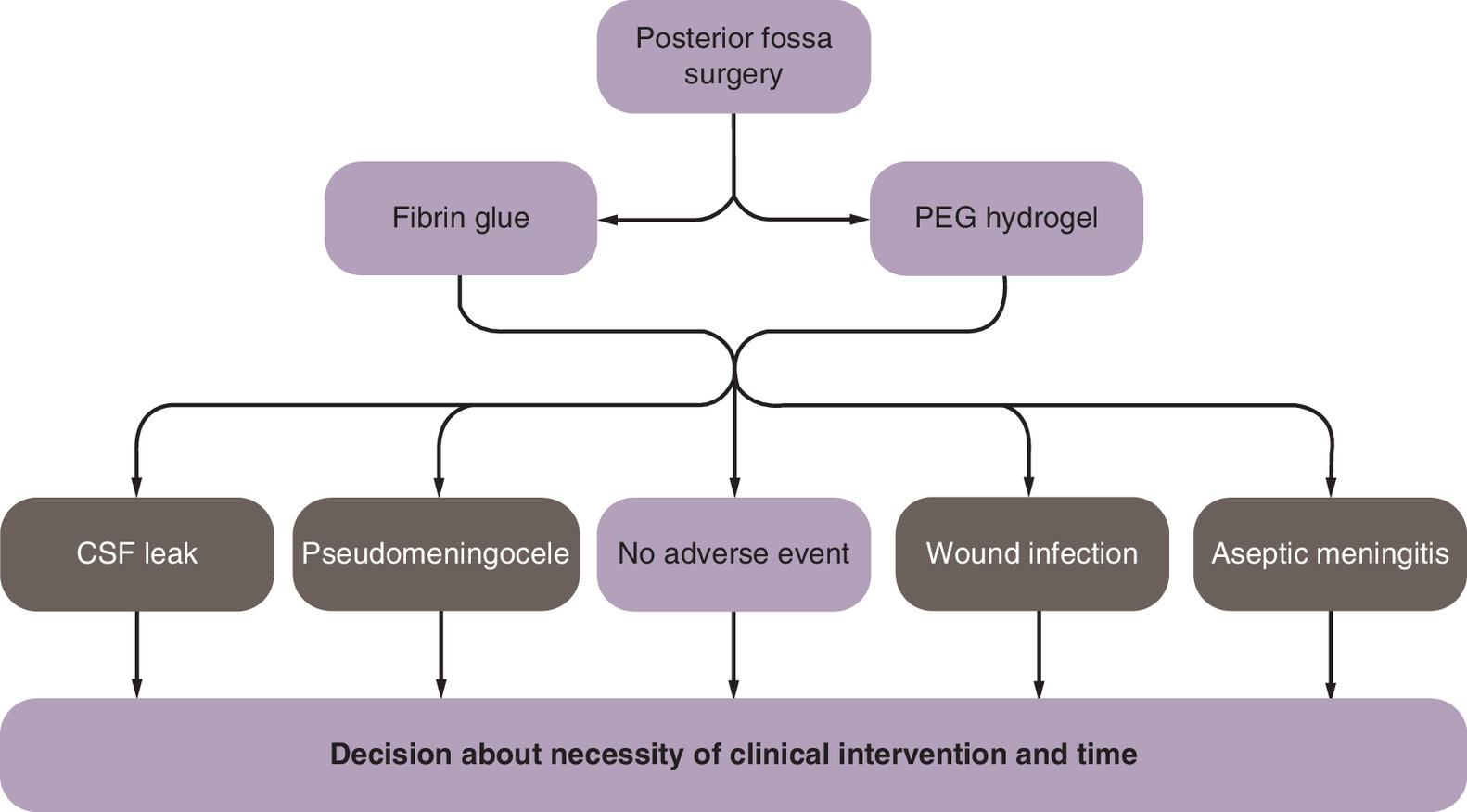
Figure 1. Decision tree diagram.
According to the complication rates in Table 1, a posterior cranial fossa patient receives either fibrin glue or PEG Hydrogel and proceeds through a complicated or uncomplicated postoperative course.
CSF: Cerebrospinal fluid; PEG: Polyethylene glycol.
| PEG hydrogel | Fibrin glue | Clinical intervention | Management | Care | ||
|---|---|---|---|---|---|---|
| CSF leaks | 2.4% | 10.0% | 100% | Operative repair | 5 hospital days | |
| Pseudomenigoceles | 9.6% | 5.0% | 20% | 50% operative repair | 5 hospital days | |
| 50% lumbar drain | ||||||
| Wound infection | 2.4% | 2.0% | 100% | 100% Antibiotics | 7 days | |
| 100% Outpatient | 2 visits | |||||
| Aseptic meningitis | 4.0% | 5.0% | 100% | 50% Lumbar drain and CSF culture | 2 hospital days | 25% 112 days steroids 75% 14 days steroids |
| 1 outpatient | ||||||
| 7 days antibiotics | ||||||
| 50% No lumbar drain | 2 outpatient visits |
Complication rates and clinical courses were derived from Carter [22].
CSF: Cerebrospinal fluid; PEG: Polyethylene glycol.
Measurements of effectiveness
The cost model was adapted from the model tailored to the US specifics by Carter [22]. Two European clinical experts deemed the model structure and outcomes adequate for the European setting. The follow-up length of the fibrin glue cohort from the leading paper by Than et al. [21] was adjusted to reflect renewed literature and better capture the incidence of adverse events. The comparative performance of both sealants was measured in monetary units in the respective local currency. Costs were accrued by the ratio of expected events and related management costs. Estimated costs were reported as per patient average undergoing posterior fossa surgery.
Measurement & valuation of preference-based outcomes
No preference-based outcomes were implemented.
Input costs
Resources and costs in Euro (EUR, €) or Great British Pound (GBP, £) were derived from published sources and, when necessary, supplemented with reimbursement and wholesale prices. Where required, costs were inflated to 2022, as inflation rates of 2023 were not available at the time of the analysis. rates, as appropriate (Table 2) [22,26–36]. Unavailable rates were extrapolated based on similarities between the examined countries. The resource utilization was deducted from the literature and validated by two practicing neurosurgeons [22]. The operating costs and duration between the two groups were assumed to be identical and not detailed in the model. The model assumes similar pre- and periprocedural costs between the cohorts. Therefore, only the different costs of the sealants and postoperative events were taken into consideration. Whenever applicable, hospitalization costs per complication were included.
| Parameter | Belgium (EUR) [26,27] | France (EUR) [28,29] | Germany (EUR) [30,35] | Italy (EUR) [32,33] | UK (GBP)† [34–36] |
|---|---|---|---|---|---|
| Hospital stay per day | 619 | 137 | 356 | 310 | 299 |
| Outpatient visit | 74 | 69 | 71 | 23 | 71 |
| Operative repair | 7306 | 5920 | 6052 | 3825 | 6211 |
| Lumbar drain | 887 | 1,924 | 2265 | 2642 | 3596 |
| CSF culture | 37 | 32 | 34 | 8 | 37 |
| Antibiotics | 7 | 2 | 30 | 3 | 0.4 |
| Steroids | 6 | 6 | 33 | 6 | 5 |
| Fibrin glue cost | 166 | 166 | 174 | 180 | 195 |
| PEG hydrogel cost | 298 | 308 | 418 | 480 | 428 |
†
Average 2022 GBP to EUR exchange rate at 1.1729 [37].
CSF: Cerebrospinal fluid; PEG: Polyethylene glycol.
Decision tree model
The decision tree model diagram is reported in Figure 1; Upon surgery completion, patients receive either dural sealant and proceed through uncomplicated or complicated recovery. A complicated recovery includes CSF leak, pseudomeningoceles, wound infection, or aseptic meningitis at rates defined in Table 1 for either sealant. Depending on the diagnosis, appropriate management is assigned. After treatment, it is assumed that no secondary event occurs.
Assumptions
The resource utilization was assumed identical across the investigated European systems. The unavailable rates were derived from country similarity. Periprocedural costs other than sealant procurement and complication events were assumed to be identical between cohorts. The safety and efficacy of sealants were assumed not to deviate across target countries. PCF surgery was assumed to yield the same result, irrespective of the sealant.
Analytical methods
The model was designed as a budget-impact analysis, evaluating the effect of a cohort of patients on the hospital budget.
Sensitivity analysis
The influence of key input parameters was tested by one-way sensitivity analysis (OWSA), particularly for changing incidences of CSF leaks and pseudomeningoceles, surgery cost, hospitalization and lumbar drain costs. Constraints for the sensitivity analysis were taken from Carter et al. [22] as those variations were seen as sensible variations that could be observed due to local differences in practice; given the high difference in reported CSF leak incidence, we also included similarity in both incidences into the analysis.
Results
Modelling the implementation of PEG sealant in place of the SOC reduced the cost impact for the five investigated European countries between EUR 419 (lowest) and EUR 1279 (highest) per patient in Italy and Belgium, respectively (detailed in Table 3). The reduction in CSF leak management and inpatient stay costs drove the overall savings in every healthcare examined. In detail, preventing incisional CSF leaks cut between EUR 408 and 790 in costs, offsetting the minor cost increase due to more frequent pseudomeningoceles (EUR 42 to 66) and the cost increase for sealant procurement. Savings between EUR 36 and 62 could also be expected from improved aseptic meningitis prophylaxis, while the differential in wound infection costs was negligible. The consequent shortened hospital stays cut an additional EUR 141 to 639. The relative volatility in absolute figures gives way to a more consistent portrayal of cost-cutting in percentage terms, on average at approximately 22%, apart from Italy at ∼15%.
| Belgium (EUR) | France (EUR) | Germany (EUR) | Italy (EUR) | UK (GBP)† | |
|---|---|---|---|---|---|
| Index hospital stay | -639 | -141 | -367 | -320 | -309 |
| Sealant procurement | 132 | 142 | 244 | 300 | 233 |
| CSF leak | -790 | -502 | -595 | -408 | -586 |
| Pseudomenigoceles | 66 | 42 | 55 | 44 | 59 |
| Aseptic meningitis | -49 | -42 | -47 | -36 | -53 |
| Wound infection | 0.62 | 0.56 | 0.69 | 0.20 | 0.57 |
| Total | -1279 (-24.6%) | -501 (-26.4%) | -711 (-21.1%) | -419 (-15.1%) | -655 (-21.3%) |
†
Average 2022 GBP to EUR exchange rate at 1.1729 [37]. Differences calculated from costs and reimbursement at 2022/2023 rates.
The cost difference is broken down for the individual contributors for the five target countries. A negative cost difference indicates a reduction in costs from adopting PEG hydrogel over fibrin glue.
CSF: Cerebrospinal fluid; PEG: Polyethylene glycol.
Figure 2 displays the expected deviation of the model's output as a function of changes in prominent input parameters. The CSF leak input incidence resulted in significant variations in both cohorts. The pseudomenigoceles incidence in the PEG hydrogel cohort also had a substantial impact.
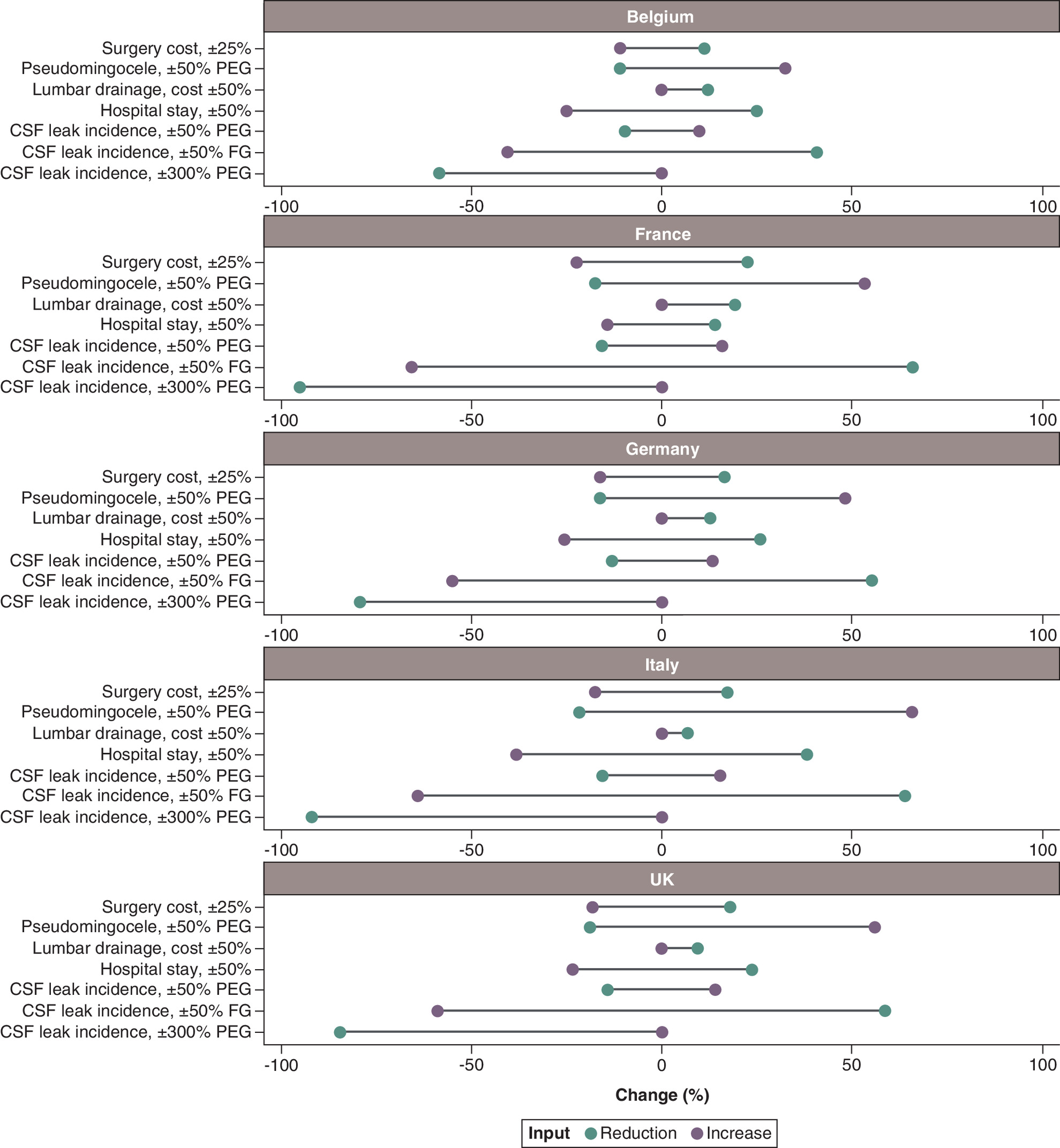
Figure 2. One-way sensitivity analysis.
Variations in expected results upon changing key input variables. For the analysis, the parameter is altered by the percentage indicated in the graph axis label. A value of -50% means that the base case parameter is halved, and a value of +100% means that the base case value is doubled.
CSF: Cerebrospinal fluid; FG: Fibrin glue; PEG: Polyethylene glycol.
Discussion
PEG hydrogels are recognized for their tangible performance edge and sealant achievement over SOC fibrin glue in general surgical practice [17,18]. Limiting to the particular case of PCF surgery, albeit meagre, the literature provides dependable leads of a significant reduction in postoperative CSF leak risk resulting from using PEG hydrogels [21]. Weaving around this premise and adapting an earlier model developed to US specifications [22], our budget impact model predicts concomitant economic benefits from adopting a PEG hydrogel in the heterogeneous context of five European countries. The national healthcare systems' peculiarities, reimbursement mechanisms, or the different shares of healthcare burden between the public and private sectors were reflected in the raw figures. Substantial savings per procedure ranged between the Italian EUR 419 and Belgian EUR 1279 extremes, respectively, with the other three countries within this range. Nevertheless, within limitations from the assumptions in the model, substantial consistency in cost reductions emerged in relative terms, at ∼22%, except for Italy at circa 15%. These results are comparable with estimates for USA [22], where cost savings approximated at 25%. The most significant component in defining PEG hydrogel-related budget cutbacks was the reduction in the incidence of postoperative CSF leaks: Increased overall patient safety is accompanied by reduced reliance on lumbar drains, reparative surgery, and shortened hospital stays. Coherently, these were the parameters to which the model was most responsive in the OWSA. Nonetheless, quantitative generalization of these findings should be approached cautiously and validated by localized real-life data analysis. Aside from the inherent constraints of any health economic model, this analysis extensively relies on Than and co-authors' data and inherits its limitations [21]. In detail, the comparability between the cohorts is limited by the shorter follow-up for the PEG hydrogel cohort, which, unlike the fibrin glue cohort, was populated prospectively. However, these potential cofounders were factored in by Carter, who introduced weighed adjustments to the incidence of complications in the PEG hydrogel cohort [22]. Besides, the demographics from input literature are centered around adult cohorts, despite a significant fraction of pediatric procedures. These may markedly differ in etiology, procedure specifics, outcomes, and, therefore, monetary aspects from interventions in adult patients. Finally, the available source data provides aggregated figures for a plenitude of procedures and does not allow for breaking down the analysis to the individual PCF surgery sub-types. Nonetheless, it is notable that the model predicted savings even upon inflating pseudomeningoceles incidence, which partially dispels doubts regarding the uncertainty from scant literature. Tentative qualitative considerations can be advanced concerning the generalizability of the model. The results are coherent with previous estimates for the US and across assessed European healthcare, despite the variance in costs and reimbursement, suggesting good extensibility of this model to comparable healthcare systems.
Conclusion
PEG hydrogels can be a viable, cost-effective alternative to fibrin glue in PCF surgery in the European context. As a direct consequence of the decreased occurrence of adverse CSF leaks, PEG hydrogels recoup higher procurement to reduce overall PCF postoperative expenses.
Summary points
•
Posterior cranial fossa (PCF) surgery is associated with operative and postoperative complications, especially cerebrospinal fluid leakage, which can be prevented by polyethylene glycol (PEG)-based hydrogels for sealing or fibrin glue.
•
As the clinical outcomes of PEG-based hydrogels compared with fibrin glue in PCF surgeries seems to be clinically superior, this work serves as a first assessment of its economic impact in Europe.
•
A health-economic model based on a published cost-benefit model from the US was developed to estimate the budget impact of switching from fibrin glue to a PEG hydrogel across five European countries (Belgium, France, Germany, Italy and UK).
•
The model results in total per patient cost savings for PCF procedures range from EUR 419 (lowest) to EUR 1279 (highest) in Italy and Belgium, respectively.
•
Preventing incisional cerebrospinal fluid (CSF) leaks only, led to cost savings between EUR 408 and EUR 790, compensating for higher costs due to more frequent pseudomeningoceles (EUR 42 to 66) and sealant procurement.
•
Comparing the five country analyses, a consistent average cost reduction per procedure of around 22% was found, except for Italy, where the analysis resulted in 15%.
•
Sensitivity analysis of the model revealed that the reduction of the incidence of postoperative CSF leaks was one of the main drivers of the model, however it did not alter the main model results in terms of PEG being cost saving compared with fibrin glue.
•
Following the results of this first analysis, to confirm the budget impact of PEG-based hydrogels across Europe and to inform decision making regarding a sealant for PCF surgery, real-world data studies from individual hospitals would be informative.
Author contributions
RT Torres led the conceptualization of the model, built the model, performed the data analysis and contributed to the writing of the manuscript. G Talamonti and JA Horaczek contributed equally to the conceptualization and clinical validation of the model, conducted background research and were major contributors to the writing of the manuscript. L Da Deppo and MJ Carter contributed to the conceptualization and validation of the model and were involved in the writing of the manuscript. All authors have read and approved the final version of the manuscript.
Financial disclosure
This study was funded by Integra LifeSciences. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
JA Horaczek is a consultant to Integra LifeSciences. RT Torres was a Coreva Scientific GmbH & Co KG employee, which received consultancy fees from Integra LifeSciences for performing, analyzing, and communicating this work. L Da Deppo is an employee at Integra LifeSciences, which funded the study. MJ Carter previously received a grant from Integra LifeSciences for developing the groundwork model in the USA. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing disclosure
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Grønbæk JK, Toescu S, Frič R et al. Postoperative speech impairment and cranial nerve deficits after secondary surgery of posterior fossa tumors in childhood: a prospective European multicentre study. Childs Nerv. Syst. 38(4), 747–758 (2022).
2.
Brell M, Ibáñez J, Caral L, Ferrer E. Factors influencing surgical complications of intra-axial brain tumors. Acta Neurochirurg. 142(7), 739–750 (2000).
3.
Lonjaret L, Guyonnet M, Berard E et al. Postoperative complications after craniotomy for brain tumor surgery. Anaesth. Crit. Care Pain Med. 36(4), 213–218 (2017).
4.
Legnani FG, Saladino A, Casali C et al. Craniotomy vs. craniectomy for posterior fossa tumors: a prospective study to evaluate complications after surgery. Acta Neurochirurg. 155(12), 2281–2286 (2013).
5.
Dubey A, Sung W-S, Shaya M et al. Complications of posterior cranial fossa surgery--an institutional experience of 500 patients. Surg. Neurol. 72(4), 369–375 (2009).
6.
Hadanny A, Rozovski U, Nossek E et al. Craniectomy versus craniotomy for posterior fossa metastases: complication profile. World Neurosurg. 89, 193–198 (2016).
7.
Slot EMH, van Baarsen KM, Hoving EW, Zuithoff NPA, van Doormaal TPC. Cerebrospinal fluid leakage after cranial surgery in the pediatric population-a systematic review and meta-analysis. Childs Nerv. Syst. 37(5), 1439–1447 (2021).
8.
Sastry RA, Walek K, Leary OP et al. Incidence, characteristics, and outcomes of pseudomeningocele and cerebrospinal fluid fistula after posterior fossa surgery. World Neurosurg. 164, e1094–e1102 (2022).
9.
Fuentes AM, Chiu RG, Nie J, Mehta AI. Inpatient outcomes of posterior fossa decompression with or without duraplasty for Chiari malformation type I. Clin. Neurol. Neurosurg. 207, 106757 (2021).
10.
Gürbüz MS, Berkman MZ, Ünal E et al. Foramen magnum decompression and duraplasty is superior to only foramen magnum decompression in Chiari malformation Type 1 associated with syringomyelia in adults. Asian Spine J. 9(5), 721–727 (2015).
11.
Hoffman H, Bunch KM, Paul T, Krishnamurthy S. Comparison of pericranial autograft and AlloDerm for duraplasty in patients with Type I Chiari malformation: retrospective cohort analysis. Oper. Neurosurg. 21(6), 386–392 (2021).
12.
Schiariti M, Acerbi F, Broggi M et al. Two alternative dural sealing techniques in posterior fossa surgery: (polylactide-co-glycolide) self-adhesive resorbable membrane versus polyethylene glycol hydrogel. Surg. Neurol. Int. 5, 171 (2014).
• Retrospective, single center study comparing the clinical safety of two alternative dural sealing techniques in posterior cranial fossa (PCF) surgery.
13.
Daudia A, Biswas D, Jones NS. Risk of meningitis with cerebrospinal fluid rhinorrhea. Ann. Otol. Rhinol. Laryngol. 116(12), 902–905 (2007).
14.
Sathaporntheera P, Saetia K. Risk factors associated with CSF leakage and complications after retrosigmoid surgery. Inter. Neurosurg. 22, 100865 (2020).
15.
Sneh-Arbib O, Shiferstein A, Dagan N et al. Surgical site infections following craniotomy focusing on possible post-operative acquisition of infection: prospective cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 32(12), 1511–1516 (2013).
16.
van Lieshout C, Slot EMH, Kinaci A et al. Cerebrospinal fluid leakage costs after craniotomy and health economic assessment of incidence reduction from a hospital perspective in The Netherlands. BMJ Open 11(12), e052553 (2021).
• Health-economic assessment from a European referral center (The Netherlands) to estimate the costs of cerebrospinal fluid (CSF) and the value of prevention.
17.
Kinaci A, van Doormaal TPC. Dural sealants for the management of cerebrospinal fluid leakage after intradural surgery: current status and future perspectives. Expert Rev. Med. Devices 16(7), 549–553 (2019).
18.
Kinaci A, Algra A, Heuts S, O'Donnell D, van der Zwan A, van Doormaal T. Effectiveness of dural sealants in prevention of cerebrospinal fluid leakage after craniotomy: a systematic review. World Neurosurg. 118, 368–376.e1 (2018).
• Systematic literature review on the prevention of CSF after PCF surgery comparing sealants and its clinical outcomes.
19.
Biscola NP, Cartarozzi LP, Ulian-Benitez S et al. Multiple uses of fibrin sealant for nervous system treatment following injury and disease. J. Venom Anim. Toxins Incl. Trop. Dis. 23, 13 (2017).
20.
Bhagat V, Becker ML. Degradable adhesives for surgery and tissue engineering. Biomacromolecules 18(10), 3009–3039 (2017).
21.
Than KD, Baird CJ, Olivi A. Polyethylene glycol hydrogel dural sealant may reduce incisional cerebrospinal fluid leak after posterior fossa surgery. Oper. Neurosurg. 63(Suppl. 1), ONS182–ONS187 (2008).
•• Study examining clinical outcomes using polyethylene glycol dural sealants compared with fibrin glue.
22.
Carter MJ. A cost-benefit analysis of using polyethylene glycol hydrogel sealant versus fibrin glue as a dural sealant for posterior fossa surgery in the United States. J. Health Econ. Outcomes Res. 5(2), 125–139 (2018).
•• This budget impact model was built on Carter's model for the US and adapted to the European setting.
23.
Caro JJ, Briggs AH, Siebert U, Kuntz KM. Modeling good research practices--overview: a report of the ISPOR-SMDM Modeling Good Research Practices Task Force--1. Value Health 15(6), 796–803 (2012).
24.
Husereau D, Drummond M, Augustovski F et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 explanation and elaboration: a report of the ISPOR CHEERS II Good Practices Task Force. Value Health 25(1), 10–31 (2022).
25.
Kshettry VR, Lobo B, Lim J, Sade B, Oya S, Lee JH. Evaluation of non-watertight dural reconstruction with collagen matrix onlay graft in posterior fossa surgery. J. Korean Neurosurg. Soc. 59(1), 52–57 (2016).
26.
INAMI. Spécialités pharmaceutiques remboursables: listes et fichiers de référence. (2022). https://www.inami.fgov.be/fr/themes/cout-remboursement/par-mutualite/medicament-produits-sante/remboursement/specialites/Pages/specialites-pharmaceutiques-remboursables-listes-fichiers-reference.aspx
27.
28.
Haute Autorité de Santé. Base des Medicaments: amoxicilline. (2022). http://www.codage.ext.cnamts.fr/codif/bdm_it/fiche/index_fic_medisoc.php?p_code_cip=3400934913174&p_site=AMELI%20Package%20of%2012%20units
29.
Haute Autorité de Santé. Tarifs MCO et HAD 2020 (2022). https://www.atih.sante.fr/tarifs-mco-et-had
30.
InEK GmbH. Fallpauschalen-Katalog 2021 (2022). https://www.g-drg.de/aG-DRG-System_2021/Fallpauschalen-Katalog/Fallpauschalen-Katalog_2021
31.
Piek J, Weber C, Kundt G et al. Pharmacoeconomical consequences of postoperative CSF leaks after intracranial surgery--a prospective analysis. J. Neurol. Surg. A Cent. Eur. Neurosurg. 73(1), 25–28 (2012).
32.
Remunerazione prestazioni di assistenza ospedaliera per acuti, assistenza ospedaliera di riabilitazione e di lungodegenza post acuzie e di assistenza specialistica ambulatoriale. In: Gazzetta Ufficiale della Repubblica Italiana (Ministero della Salute, Rome). GU Serie Generale n.23 del 28-01-2013 - Suppl. Ordinario n. 8. 1–64 (2012).
33.
Agenzia Italiana del Farmaco. Liste di trasparenza (2022). https://www.aifa.gov.it/liste-di-trasparenza
34.
NICE. Amoxicillin (2022). https://bnf.nice.org.uk/drugs/amoxicillin/
35.
NICE. Medicinal forms. Dexamethasone (2022). https://bnf.nice.org.uk/drugs/dexamethasone/medicinal-forms/
36.
NHS England. National tariffs 2020 (2022). https://www.england.nhs.uk/publication/past-national-tariffs-documents-and-policies/
37.
European Central Bank. Euro reference exchange rate: pound sterling (GBP) (2022). https://www.ecb.europa.eu/stats/policy_and_exchange_rates/euro_reference_exchange_rates/html/eurofxref-graph-gbp.en.html
Information & Authors
Information
Published In
Copyright
© 2024 Coreva Scientific GmbH & Co. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 30 March 2023
Accepted: 2 February 2024
Published online: 23 February 2024
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
PEG hydrogel sealant versus fibrin glue in posterior fossa surgery: an economic comparison across five European countries. (2024) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2023-0047
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- E.N. Kuanyshev, B.S. Syzdykova, D.K. Teltayev, K.H. Mustafin, First clinical application of autologous fibrin sealant Vivostat for neurosurgery in Kazakhstan and Central Asia, Burdenko's Journal of Neurosurgery, 10.17116/neiro20269002170, 90, 2, (70), (2026).
- Tomoko Ito, Yoshiyuki Koyama, Influence of Polyhydroxyl Additives on the Mechanical Properties of Poly(acrylic acid)/Polyvinylpyrrolidone Complex Films, Compounds, 10.3390/compounds6010005, 6, 1, (5), (2026).
- Jasjit Syan, Tobias Muench, Carla Fernández-Barceló, Rhodri Saunders, Jonah Attebery, Marco Luchetti, Mary Erslon, John Beard, Sadia Khan, Health-economic impact of implementing continuous vital sign monitoring in post-surgical patients in five European countries, Journal of Medical Economics, 10.1080/13696998.2025.2602364, 29, 1, (50-65), (2025).
- Andra Ioana Baloiu, Florin Filipoiu, Corneliu Toader, Razvan-Adrian Covache-Busuioc, Octavian Munteanu, Matei Serban, Sphenoid sinus hyperpneumatization: anatomical variants, molecular blueprints, and AI-augmented roadmaps for skull base surgery, Frontiers in Endocrinology, 10.3389/fendo.2025.1634206, 16, (2025).
- Zhanpeng Li, Yahui Xiong, Xiaogang Liu, Xiaoxiang Wang, Fan Bie, Fan Yang, Shuying Chen, Zhaoqiang Zhang, Yingbin Xu, Lei Chen, Bioengineered tetra-PEG-COLIII-SCS hydrogel: A rapid wet-adhesive multifunctional platform for scarless repair of dynamic diabetic wound, Chemical Engineering Journal, 10.1016/j.cej.2025.162931, 513, (162931), (2025).