Advantages of robotic arm-assisted total hip arthroplasty: a 90-day episode-of-care clinical utility and cost analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Determine the clinical utility and economic differences over a 90-day period between robotic arm-assisted total hip arthroplasty (RATHA) and manual total hip arthroplasty (MTHA). Methods: Leveraging a nationwide commercial payer database, pre-covid THA procedures were identified. Following a 1:5 propensity score match, 1732 RATHA and 8660 MTHA patients were analyzed. Index costs, index lengths of-stay, and 90-day episode-of-care utilization and costs were evaluated. Results: Episode of care costs for RATHA was found to be $1573 lower compared with MTHA (p < 0.0001). Post-index hospital utilization was significantly less likely to occur for RATHA compared with MTHA. Total index costs were also significantly lower for RATHA versus MTHA (p < 0.0001). Conclusion: Index and post-index EOC hospital utilization and costs were lower for RATHA compared with MTHA.
Tweetable abstract
A 90-day episode-of-care analysis of 1732 robotic arm-assisted and 8660 manual THAs reveals costs were $1573 lower for RATHA compared with MTHA and hospital utilization was less.
#stryker #makosmartrobotics #orthopaedics #totalhipreplacement
Total hip arthroplasty (THA) is one of the most successful operations provided to patients. One study found that 58% of THAs should last at least 25 years, indicating strong long-term implant survivorship [1]. However, there are still some common complications, such as component malpositioning that surgeons need to be highly cognizant of during both preoperative planning and surgery [2]. To help optimize implant positioning and restore leg length, several different technological devices are available [3]. Robotic arm-assisted total hip arthroplasty, in particular, helps facilitate acetabular component placement in the desired position for each individual patient. In fact, studies have shown that robotic arm-assisted hip arthroplasties are associated with a greater chance of placing components in the universally accepted hip safe zones [4]. In association with real time haptic feedback, CT scan-based robotic arm-assisted THA (RATHA) can more reliably reproduce and is more accurate and precise in achieving the planned hip center of rotation [5]. Although robotic technology can have potential intraoperative and patient specific advantages, a major consideration, especially given today's healthcare climate, is the economic impact of using this technology versus simply using manual techniques.
The evaluation of the economic impact of changes in care delivery is playing a larger role in healthcare decision making today. A substantial emphasis is placed on providing patients with the most appropriate level of care while ensuring that there is a fair assessment of value of that care [6]. This emphasis is even greater for total joint arthroplasty, given that these surgeries are performed often and on an elective basis. Although there is limited cost-consideration-based data for RATHA, several studies have shown cost savings as well as patient outcome advantages when utilizing robotic arm assistance for total knee arthroplasty [7,8]. In one study by Gregory et al., the authors utilized a large national database comparing robotic-assisted (n = 4135) versus manual (n = 4135) total knee arthroplasties and found significant cost savings based on a 90-day episode of care (EOC) analysis ($29,984 vs $31,280, p < 0.0001) [9]. In another study, Cool et al., also found significant 90-day EOC cost savings for patients who underwent robotic-assisted versus manual total knee arthroplasty ($2391 less for robotic TKA [p < 0.0001]) [8]. The authors also identified that a major reason driving these cost savings for robotic-assisted TKA patients was the overall decreased utilization of post-acute services.
Given that patients more commonly report higher satisfaction with their hip arthroplasties as compared with their knee arthroplasties [10], and given the intraoperative advantages of more accurately placing implants leading to potentially improve postoperative function, there is reason to believe that incorporating robotic technology in total hip arthroplasty can further help increase the economic advantages. The purpose of this study was to perform a 90-day EOC clinical utility and cost analysis study of CT scan-based RATHA versus manual total hip arthroplasty (MTHA) patients, with a focus on the payer perspective and reduced use of the expensive hospital setting during both the index and post-index periods. Specifically, we evaluated: 1) Index costs; 2) Index lengths-of-stay; 3) 90-day post-index resource utilization and costs; and 4) Overall 90-day EOC costs.
Materials & methods
Data source
In order to capture the cost impact from a payer perspective, The Blue Health Intelligence (BHI) nationwide commercial insurance database (Health Intelligence Company, LLC, IL, USA) was utilized to capture all patient data. This database contains data regarding medical and pharmacy services provided to more than 234 million unique patients' medical and pharmaceutical claims. Utilizing a medical claims database provides the unique advantage of being able to capture all billable aspects of the longitudinal patient journey, which is not necessarily possible with hospital-specific or index-focused datasets. This data source contains a population of commercially insured patients, with over 90% being less than 65 years old.
Patient Selection
All patients who had hospital admissions under DRG codes 469 and 470 were isolated, yielding a total of 185,181 patients. Patients were then filtered directly based on the following ICD codes for THA: 0SR9019, 0SR901A, 0SR901Z, 0SR9029, 0SR902A, 0SR902Z, 0SR9039, 0SR903A, 0SR903Z, 0SR9049, 0SR904A, 0SR904Z, 0SR90J9, 0SR90JA, 0SR90JZ, 0SRB019, 0SRB01A, 0SRB01Z, 0SRB029, 0SRB02A, 0SRB02Z, 0SRB039, 0SRB03A, 0SRB03Z, 0SRB049, 0SRB04A, 0SRB04Z, 0SRB0J9, 0SRB0JA, and 0SRB0JZ, yielding 152,570 patients. Further selection was performed for patients who underwent their THA between 1 April 2018 and 30 September 2019, extracting 56,433 patients from the database. Next, patients who did not have an inpatient admission for DRG 469 and 470 within 60 days prior or 90 days after their THA were selected for inclusion (n = 53,515).
From this cohort of 53,515 THA patients, two study populations were identified: a CT scan-based robotic arm-assisted THA (RATHA) cohort and a manual THA (MTHA) cohort. The RATKA population was identified through an ICD-10 code indicative of a robotic-assisted procedure and a CT scan within 60 days prior to the THA procedure. Patients who did not have a robotic-assisted procedure and a CT scan were deemed manual cases. The patient population was further limited to the first THA event during the study timeframe and those that had continuous enrollment during the post-operative 90-day follow-up. Patients were required to have at least one follow-up service on a post-index basis. Finally, patients who had an index admission cost of at least $12,000 for MS-DRG 470 or at least $19,000 for MS-DRG 469 were selected (Figure 1). This threshold was selected to ensure that the payer cost was at or above the average Medicare payment in order to avoid scenarios associated with major patient responsibilities or other underpayment situations that could not be controlled for in the study.
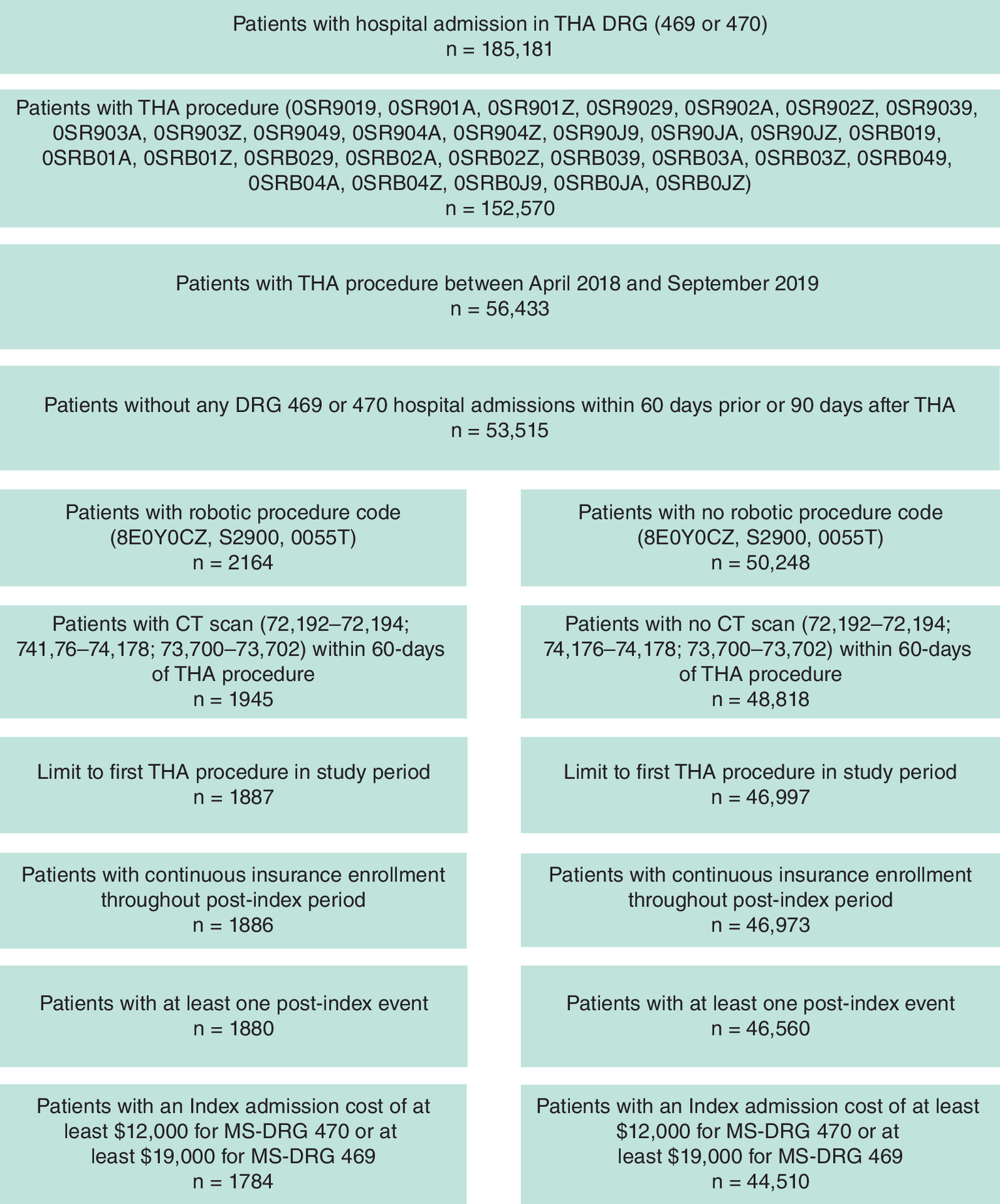
Figure 1. Patient selection for the robotic and manual cohorts.
THA: Total hip arthroplasty.
Propensity score matching
Patients in each cohort were propensity score matched (PSM) in a 1:5 ratio of robotic to manual cases using the greedy nearest-neighbor algorithm applied to propensity score probabilities estimated by logistic regression with independent variables based on age, sex, comorbidities, census division based on US Census bureau divisions (i.e., New England, Middle Atlantic, East North Central, etc.), and geography (i.e., urban, rural, etc.). Comorbidities included: chronic obstructive pulmonary disease; diabetes; coronary artery disease; cancer; smoking; obesity; hypertension; bone density issues; osteoarthritis; and functional mobility issues. (Table 1).
| Characteristics | Pre-match characteristics | Post-match characteristics | ||||||
|---|---|---|---|---|---|---|---|---|
| RATHA (n = 1784) | MTHA (n = 44,510) | % difference (% points) | p-value | RATHA (n = 1732) | MTHA (n = 8660) | % difference (% points) | p-value | |
| Age group (years) | ||||||||
| <40 | 3.53% | 2.85% | 24 | 0.0112 | 3.52% | 3.34% | 5 | 0.9957 |
| 40–49 | 11.60% | 10.29% | 13 | 11.72% | 11.91% | -2 | ||
| 50–54 | 15.58% | 14.22% | 10 | 15.59% | 16.09% | -3 | ||
| 55–59 | 26.85% | 26.13% | 3 | 26.96% | 27.07% | 0 | ||
| 60–64 | 31.61% | 33.61% | -6 | 31.52% | 31.26% | 1 | ||
| 65–69 | 8.13% | 9.38% | -13 | 8.08% | 7.90% | 2 | ||
| 70+ | 2.69% | 3.52% | -24 | 2.60% | 2.45% | 6 | ||
| Men | 50.28% | 51.41% | -2 | 0.3587 | 50.35% | 51.11% | -1 | 0.5626 |
| Comorbidities | ||||||||
| Chronic obstructive pulmonary disease | 4.04% | 4.19% | -4 | 0.8094 | 3.81% | 2.89% | 32 | 0.0460 |
| Diabetes | 11.43% | 13.48% | -15 | 0.0130 | 11.09% | 10.98% | 1 | 0.8996 |
| Coronary artery disease | 7.79% | 7.70% | 1 | 0.8919 | 7.79% | 7.41% | 5 | 0.5821 |
| Cancer | 0.78% | 1.11% | -30 | 0.2447 | 0.69% | 0.48% | 44 | 0.2720 |
| Smoking | 12.72% | 12.83% | -1 | 0.9424 | 12.41% | 11.71% | 6 | 0.4150 |
| Obesity | 31.17% | 32.19% | -3 | 0.3795 | 31.12% | 31.55% | -1 | 0.7339 |
| Hypertension | 54.65% | 54.69% | 0 | 0.9807 | 54.56% | 55.21% | -1 | 0.6339 |
| Bone density issues | 4.93% | 3.73% | 32 | 0.0113 | 4.85% | 4.57% | 6 | 0.6159 |
| Osteoarthritis | 99.33% | 97.65% | 2 | <0.0001 | 99.48% | 99.69% | 0 | 0.1797 |
| Functional mobility issues | 8.63% | 7.23% | 19 | 0.0289 | 8.66% | 7.77% | 11 | 0.2229 |
| Census Division | ||||||||
| New England | 8.80% | 6.18% | 42 | <0.0001 | 8.66% | 8.71% | -1 | 0.9969 |
| Middle Atlantic | 15.19% | 16.08% | -6 | 15.18% | 15.46% | -2 | ||
| East North Central | 13.00% | 17.24% | -25 | 12.70% | 12.15% | 5 | ||
| West North Central | 3.59% | 7.68% | -53 | 3.52% | 3.63% | -3 | ||
| South Atlantic | 10.71% | 20.69% | -48 | 10.91% | 11.28% | -3 | ||
| East South Central | 15.02% | 7.89% | 90 | 15.36% | 14.99% | 2 | ||
| West South Central | 20.63% | 10.87% | 90 | 20.79% | 21.34% | -3 | ||
| Mountain | 5.55% | 5.07% | 9 | 5.60% | 5.20% | 8 | ||
| Pacific | 7.29% | 8.01% | -9 | 7.04% | 7.06% | 0 | ||
| Unknown | 0.22% | 0.28% | -21 | 0.23% | 0.20% | 15 | ||
| Geography | ||||||||
| Urban | 87.11% | 88.83% | -2 | 0.0490 | 87.12% | 88.52% | -2 | 0.0513 |
| Rural | 9.59% | 8.00% | 20 | 9.58% | 9.15% | 5 | ||
| Unknown | 3.31% | 3.17% | 4 | 3.29% | 2.33% | 41 | ||
MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty.
Outcomes evaluated
The outcomes evaluated in this study was 90-day episode-of-care costs, utilization trends, and index lengths-of-stay. These costs consisted of index facility and professional fees, CT-scan costs, as well as post-index costs, such as inpatient, outpatient, pharmacy, professional, and other costs. ‘Other costs’ involved patient utilization of any of the following resources: emergency rooms, ambulatory surgical centers, independent clinics, skilled nursing facilities, home health usages, inpatient psychiatric facilities, comprehensive inpatient and outpatient rehabilitation centers, and/or independent laboratory testings.
Data analyses
All data were extracted from the BHI database and evaluated utilizing SAS Enterprise Guide 7.1 (SAS Institute Inc., NC, USA). Descriptive analyses were performed for qualitative variables. Mann–Whitney U tests were performed to compare differences between cohorts for the above listed outcomes evaluated. Outliers were identified and removed by converting episode of care costs to natural logarithm values and were assumed to be distributed as log-normal. An interquartile based method was used with a cutoff point as 1.5-times the interquartile range at both the upper and lower bound.
Results
Index costs
The overall mean index costs for the RATHA cohort was found to be $1,297 lower than that of the MTHA cohort ($31,507 vs $32,804; p < 0.0001). This trend in costs persisted when comparing mean facility fees ($27,103 vs $28,839; difference: $1736; p < 0.0001), and professional fees ($3902 vs $3965; difference: $63; p = 0.0007). The further breakdown of these costs is represented in Table 2.
| Cost measurement | RATHA costs (n = 1732) | MTHA costs (n = 8660) | Cost difference (RATHA–MTHA) | Std mean difference | p-value | |
|---|---|---|---|---|---|---|
| Index THA admission – facility | $27,103 | $28,839 | -$1736 | -6.02% | -0.1806 | <0.0001 |
| Index THA admission – professional | $3902 | $3965 | -$63 | -1.59% | -0.0314 | 0.0007 |
| CT Scan | $502 | – | – | – | – | – |
| Total index costs | $31,507 | $32,804 | -$1297 | -3.95% | -0.1266 | <0.0001 |
MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty; THA: Total hip arthroplasty.
On Mann–Whitney U Testing, index costs facility and professional, total index costs, all tended to be significantly lower for the robotic as compared with the manual cohort (Table 2).
Lengths-of-Stay
RATHA patients were found to be associated with a shorter length-of-stay as compared with MTHA patients (1.51 vs 1.71 days; p < 0.0001) (Table 3). Moreover, one-day stays were significantly more prevalent for RATHA patients (65.24 vs 58.98%; p < 0.0001), while stays of 3+ days were significantly less prevalent (7.97 vs 11.34%; p < 0.0001) (Table 4).
| RATHA LOS (n = 1732) | MTHA LOS (n = 8660) | LOS difference (RATHA–MTHA) | Std mean difference | p-value | |
|---|---|---|---|---|---|
| 1.51 | 1.71 | -0.20 | -11.66% | -0.1379 | <0.0001 |
LOS: Length of stay; MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty.
| LOS | RATHA (n = 1732) | MTHA (n = 8660) | p-value |
|---|---|---|---|
| 1 day | 1130 (65.24%) | 5108 (58.98%) | <0.0001 |
| 2 days | 464 (26.79%) | 2570 (29.68%) | 0.0163 |
| 3+ days | 138 (7.97%) | 982 (11.34%) | <0.0001 |
LOS: Length of stay; MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty.
90-day post-index resource utilization & costs
For inpatient services, 31.66% fewer RATHA patients needed inpatient care (p 0.0203), resulting in 35.93% fewer readmissions (p = 0.0204) for this cohort. Moreover, 7.85% fewer patients needed hospital outpatient services (p = 0.0038), leading to 22.25% fewer hospital outpatient encounters (p = 0.0002) across the RATHA cohort. The reduction in hospital costs (both inpatient and hospital outpatient services) were driven by reduced post-index utilization of these services in the RATHA cohort compared with the manual cohort (Table 5). Overall, the RATHA cohort had lower costs associated with 90-day post-index resource utilization ($3929 vs $4205; difference: $276; p = 0.1086). Specifically, the RATHA cohort had fewer inpatient ($377 vs $506; difference: $129; p = 0.0160), outpatient ($801 vs $999; difference: $198; p = 0.0010) and pharmacy ($418 vs $454; difference: $37; p = 0.1242) costs compared with MTHA. Higher costs associated with RATHA were professional ($1691 vs $1641; difference: $42; p = 0.0001) and other costs ($643 vs $597; difference: $46; p < 0.0001) (Table 6).
| Place of service | RATHA utilization (n = 1732) | MTHA utilization (n = 8660) | Utilization difference (% difference) | p-value | ||||
|---|---|---|---|---|---|---|---|---|
| Patients | Avg visits per patient | Patients | Avg visits per patient | Patients | Avg visits per patient | Patients, % | Avg visits per patient | |
| Inpatient | 2.31% | 0.0266 | 3.38% | 0.0415 | -31.66% | -35.93% | 0.0203 | 0.0204 |
| Hospital Outpatient | 44.98% | 1.1917 | 48.81% | 1.5327 | -7.85% | -22.25% | 0.0038 | 0.0002 |
| Pharmacy | 62.99% | 6.3129 | 60.83% | 5.6236 | 3.55% | 12.26% | 0.0941 | 0.0006 |
| Professional | 99.31% | 13.0676 | 98.90% | 11.8703 | 0.41% | 10.09% | 0.1509 | <0.0001 |
| Other† | 47.52% | 1.1391 | 37.88% | 0.9514 | 25.45% | 19.74% | <0.0001 | <0.0001 |
†
Other settings include: emergency room, skilled nursing facilities, home health, ambulatory surgical centers, independent clinics, inpatient psychiatric facilities, comprehensive inpatient rehabilitation, comprehensive outpatient rehabilitation, independent labs and other facility services.
Avg: average; MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty.
| Place of service | RATHA costs (n = 1732) | MTHA costs (n = 8660) | Cost differences (RATHA–MTHA) | Std mean difference | p-value | |
|---|---|---|---|---|---|---|
| Inpatient | $377 | $506 | -$129 | -25.59% | -0.0410 | 0.0160 |
| Hospital Outpatient | $801 | $999 | -$198 | -19.83% | -0.0895 | 0.0010 |
| Pharmacy | $418 | $454 | -$37 | -8.09% | -0.0215 | 0.1242 |
| Professional | $1691 | $1649 | $42 | 2.56% | 0.0196 | 0.0001 |
| Other† | $643 | $597 | $46 | 7.64% | 0.0335 | <0.0001 |
| Total Post-Index Costs | $3929 | $4205 | -$276 | -6.56% | -0.0490 | 0.1086 |
†
Other settings include: emergency room, skilled nursing facilities, home health, ambulatory surgical centers, independent clinics, inpatient psychiatric facilities, comprehensive inpatient rehabilitation, comprehensive outpatient rehabilitation, independent labs and other facility services.
MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty.
Overall Index plus 90-Day Episode-of-Care Costs
Total index costs (facility, professional, CT-scan costs) plus post-index resource utilization costs were $1573 lower for the RATHA cohort compared with MTHA ($35,436 vs $37,009; p < 0.0001) (Table 7).
| RATHA costs (n = 1732) | MTHA costs (n = 8660) | Cost difference (RATHA–MTHA) | Std mean difference | p-value | ||
|---|---|---|---|---|---|---|
| Total EOC costs (index + 90-Day) | $35,436 | $37,009 | -$1573 | -4.25% | -0.1345 | <0.0001 |
MTHA: Manual total hip arthroplasty; RATHA: Robotic arm-assisted total hip arthroplasty.
Discussion
Robotic arm-assisted total hip arthroplasty has been shown to have several intraoperative advantages leading to more optimal and reliably reproducible component positioning [11]. Additionally, clinical studies have shown improved patient reported outcomes and satisfaction scores for RATHA compared with MTHA as well as reductions in adverse events such as post-operative dislocation [4,12,22]. Currently, there are limited data comparing the clinical utility and costs of care using this technology-assisted surgery as compared with traditional manual techniques. Therefore, this study compared overall 90-day episode of care costs including index costs, post-index resource utilization and costs and lengths-of-stays between CT scan-based RATHA versus MTHAs. The data from this study indicate significant cost savings to the payer for patients who underwent RATHA as compared with MTHA patients. These patients tended to have lower associated postoperative resource utilization, specifically around post-index use of the hospital, and shorter index lengths-of-stays. The lengths-of-stays found in this study represent more modern lengths-of-stay with contemporary postoperative protocols compared with what has been presented in prior studies. Specifically, robotic-assisted care was associated with significantly more single day stays than the manual cohort, as well as significantly fewer stays of three days or more. It is notable that this LOS profile lends itself to a meaningful and imminent transition to outpatient THAs and the associated cost-efficiencies of this less restrictive setting. Therefore, these data are likely more representative of current costs in today's healthcare climate.
We suspect that in addition to the potential cost savings from decreased post-index hospital utilizations and shorter lengths-of-stay, the intra-operative advantages involved with robotic arm-assisted technology may also play a role in facilitating a more expedited postoperative recovery. The advantages include more optimal component planning and positioning, and ability to prepare the acetabulum in a more controlled manner due to the robotic arm minimizing inadvertent surrounding bony or soft tissue damage, as well as the ability to perform a single reaming as opposed to multiple reaming in MTHA, while still ensuring that the acetabular component is appropriately medialized [12]. These benefits in surgical technique may potentially help the body more quickly acclimate to the new prosthesis and therefore improve post-operative recovery [11–14]. Studies have shown reduced blood loss, greater acetabular bone preservation, and better restoration of the hip center-of-rotation for RATHA compared to MTHA. Shibanuma and colleagues compared the early recovery of 30 RATHA patients with 30 computer-navigated THAs (CNTHA) and found that RATHA patients had improved early clinical recovery including reduced pain on post-operative days 7, 10 and 14, fewer days to independent walking, and significantly higher Harris Hip scores compared to CNTHA [14].
There are some limitations to this study. As a large database study, there are always the potential errors for data entry and coding. Additionally, since multiple codes are needed to identify robotic THA patients, there is a chance that some patients were missed during the initial data collection phase. This study was also retrospective in nature, so the selection of patients to undergo robotic versus manual THAs could not be controlled. Furthermore, other important peri-operative factors were not included for analysis, such as anesthesia type, pain management, and/or physical therapies provided. Nevertheless, this study represents a large, nationwide sample indicative of the current state of robotic THA clinical utility and economics. Notably, since this data was collected from a large insurance database a true, real world cost analysis could be performed, further helping to substantiate the findings.
There are other studies in the literature that support the findings from this analysis. In a study by Pierce et al., 938 RATHAs from a private payer database were propensity score matched to 4670 MTHAs and compared based on 90-day episode of care costs, index costs, lengths-of-stay, and post-index rehabilitation utilizations [15]. The authors found that RATHA was significantly associated with fewer instances of post-index inpatient rehabilitation or skilled nursing facility admissions compared with MTHA. RATHA patients also utilized fewer home health agency visits compared with MTHA patients in their analysis. Overall, they found that total 90-day EOC costs for RATHA patients were significantly less than that of MTHA patients (difference: $785; p = 0.0095).
In another study by Maldonado et al., the authors created a Markov model to analyze cumulative costs and utilities between RATHA versus MTHAs [16]. The group found that the RATHA cohort was more cost effective relative to MTHA for cumulative medical and private insurance payer costs over a 5-year period. For Medicare patients, RATHAs saved a mean of $945, and for private insurance saved payers $1810 compared with MTHA. Additionally, RATHA had slightly more health utility (0.04 quality-adjusted life year).
In a study by Clement et al. the authors compared 40 RATHA patients versus 80 propensity score matched MTHA patients and compared several patient satisfaction outcome surveys as well as component placement based on the Lewinnek and Callanan safe zones, as well as ability to restore leg lengths [17]. The group found that the Oxford hip and Forgotten Joint Scores were significantly greater in the RATHA cohort as compared with the MTHA cohort. Importantly, no patients in the RATHA cohort were dissatisfied, however, 6 MTHA patients were dissatisfied. Overall, RATHA was associated with a greater rate of safe zone component positioning (p ≤ 0.003) as well as leg length restoration (p < 0.001) compared to MTHA.
Some studies in the literature have identified a lack of advantage for RATHA. A study by Emara et al., found RATHAs to potentially be more costly than MTHAs (robotic: $18,416 vs manual: $17,266; p < 0.001) [18]. However, the data were from the National Inpatient Sample which only evaluates the in-hospital period, and not cumulative episode-of-care costs, which is widely considered a better overall economic marker of value. Additionally, this study revealed a mean length-of-stay for robotic THA patients to be 2.2 days and manual THA patients to be 2.3 days, which is substantially longer than the lengths-of-stay identified in our report and is less representative of modern THA care pathways. In a study by Kirchner et al., the authors utilized the same database as the aforementioned study and similarly found mean RATHA index costs to be greater than that for MTHA patients [19]. Although the lengths-of-stay for the robotic cohort was shorter than that for the manual cohort, the costs reported only represent inpatient hospital costs, and not overall 90-day episode-of-care costs, which are a better economic indicator in today's value-based world. Furthermore, all of these studies do not account for the fact that new technologies can assist in shifting inpatient surgical cases to the outpatient arena which further decreases cost, but is not captured in these inpatient analyses.
Conclusion
Robotic arm-assisted total hip arthroplasty has been shown in the literature to have several intraoperative advantages, especially pertaining to optimal component positioning [11]. The added benefits of more precise and accurate acetabular cup placement have also been shown to help improve component survivorship, decrease complications, and likely influence greater patient satisfaction [20,21]. Additionally, the literature has shown less complication rates for adverse events such as dislocation between robotic-assisted and manual THAs [22]. What has not been well-elucidated are the potential clinical utility and economic benefits of this technology. Our study revealed that RATHA patients used fewer hospital services in the post-index period, had greater average cost savings based on their 90-day episodes of care, as well as shorter index lengths-of-stay compared with MTHA. In an era of increased focus on value in healthcare, CT-based robotic assisted surgery appears to both improve quality and decrease costs. Based on these data, RATHA shows not only advantages for component placement and improved outcomes for patients, but also advantages for the costs of care over a 90-day time period. Furthermore, our results are in agreement with similar payer perspective analyses. Overall, RATHA shows promising advancements for clinical and economic optimization of THA. Payers would likely benefit from encouraging the use of CT-based robotic technology in THA.
•
Total hip arthroplasty procedures provide strong long-term implant survivorship, however, there are still complications that can be limited and efficiencies gained in care delivery with technological devices, such as robotic technology.
•
Even though robotic technology can have potential intraoperative and patient-specific advantages, the economic burden to health plans needs to be considered.
•
Robotic arm-assisted total hip arthroplasty helps facilitate acetabular component placement in the desired position for each individual patient.
•
The economic value of robotic arm-assisted total hip arthroplasty (RATHA) for Medicare patients has been previously quantified, but the impact to commercial insurers has yet to be determined.
•
This analysis of health plan costs over the total episode-of-care showed RATHA to be statistically significantly lower than procedures performed manually.
•
During the post 90-day period, fewer RATHA patients required inpatient or outpatient hospital care compared to manual total hip arthroplasty and utilized statistically significantly fewer services across these settings.
•
This study shows that commercial payers would benefit financially from the use of CT-scan-based robotic technologies for total hip arthroplasties.
Acknowledgments
The authors acknowledge L Mills (Baker Tilly, US, LLP).
Financial & competing interests disclosure
This study was sponsored by Stryker. W Barsoum is a paid consultant of Stryer and receives royalties from Stryker, Zimmer, Biomet and Arthrex. D Gregory is a Principal and K Needham is an employee of Baker Tilly US, LLP, which received consulting fees from the sponsor. M Mont and D Jacofsky are paid consultants of Stryker. A Coppolecchia is an employee of Stryker and owns stock in Stryker. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Institutional review board is not required for this type of study and specific human subjects were not investigated; therefore, informed consent was not required.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Sodhi N, Mont MA. Survival of total hip replacements. Lancet 393, 613 (2019).
2.
Healy WL, Iorio R, Clair AJ, Pellegrini VD, della Valle CJ, Berend KR. Complications of total hip arthroplasty: standardized list, definitions, and stratification developed by The Hip Society. Clin. Orthop. Relat. Res. 474, 357 (2016).
3.
Fontalis A, Epinette JA, Thaler M, Zagra L, Khanduja V, Haddad FS. Advances and innovations in total hip arthroplasty. SICOT J. 7, 26 (2021).
4.
Domb BG, El Bitar YF, Sadik AY, Stake CE, Botser IB. Comparison of robotic-assisted and conventional acetabular cup placement in THA: a matched-pair controlled study. Clin. Orthop. Relat. Res. 472, 329–336 (2014).
5.
Kayani B, Konan S, Ayuob A, Ayyad S, Haddad FS. The current role of robotics in total hip arthroplasty. EFORT Open Rev. 4, 618 (2019).
6.
Sodhi N, Piuzzi NS, Khlopas A et al. Are we appropriately compensated by relative value units for primary vs revision total hip arthroplasty? J. Arthroplasty 33(2), 340–344 (2018).
7.
Mont MA, Cool C, Gregory D, Coppolecchia A, Sodhi N, Jacofsky DJ. Health care utilization and payer cost analysis of robotic arm assisted total knee arthroplasty at 30, 60, and 90 days. J. Knee Surg. 34, 328–337 (2021).
• Analysis of health care utilization trends over 30, 60 and 90 days between 519 robotic-assisted TKAs and 2595 manual TKAs showing reduced day episode of care (EOC) costs at 30, 60 and 90 days and reduced services utilization in areas such as SNF, home health, emergency room and readmissions.
8.
Cool CL, Jacofsky DJ, Seeger KA, Sodhi N, Mont MA. A 90-day episode-of-care cost analysis of robotic-arm assisted total knee arthroplasty. J. Comp. Eff. Res. 8(5), 327–336 (2019).
• Comparison of Medicare costs for 519 robotic-assisted versus 2595 manual total knee arthoplasties over 90 days, showing reduced lengths of stay, increase in home discharge, reduced readmissions and average savings for the robotic-assisted procedure over a 90-EOC.
9.
Gregory DA, Coppolecchia A, Scotti DJ, Chen Z, Mont MA, Jacofsky D. A 90-day episode-of-care analysis including computed tomography scans of robotic-arm assisted versus manual total knee arthroplasty. J. Knee Surg. (2022) (Epub ahead of print).
• Comparison of private payer costs including CT scans for 4135 robotic-assisted TKAs matched with 4135 manual TKAs found reduced costs for index procedure, inaptient admissions, hospital outpatient visits and SNF stays as well as lower overall 90-day EOC care cost for robotic- assisted compared to manual.
10.
de Beer J, Petruccelli D, Adili A, Piccirillo L, Wismer D, Winemaker M. Patient perspective survey of total hip vs total knee arthroplasty surgery. J. Arthroplasty 27(6), 865–9.e1–5 (2012).
11.
Kayani B, Konan S, Thakrar RR, Huq SS, Haddad FS. Assuring the long-term total joint arthroplasty: a triad of variables. Bone Joint J. 101-B, 11–18 (2019).
12.
Bukowski BR, Anderson P, Khlopas A, Chughtai M, Mont MA, Illgen RL. Improved functional outcomes with robotic compared with manual total hip arthroplasty. Surg. Technol. Int. XXIX, 303–308 (2016).
•• A comparison of 100 robotic arm-assisted total hip arthroplasty (RATHA) patients versus 100 manual total hip arthroplasty (MTHA) patients from a single institution showed reduced blood loss and higher mean PROMs at 1 year for RATHA compared to MTHA.
13.
Suarez-Ahedo C, Gui C, Martin TJ, Chandrasekaran S, Lodhia P, Domb BG. Robotic-arm assisted total hip arthroplasty results in smaller acetabular cup size in relation to the femoral head size: a matched-pair controlled study. Hip Int. 27, 147–152 (2017).
14.
Shibanuma N, Ishida K, Matsumoto T et al. Early postoperative clinical recovery of robotic arm-assisted vs. image-based navigated total hip arthroplasty. BMC Musculoskelet. Disord. 22(1), 314 (2021).
15.
Pierce J, Needham K, Adams C, Coppolecchia A, Lavernia C. Robotic-assisted total hip arthroplasty: an economic analysis. J. Comp. Eff. Res. 10(16), 1225–1234 (2021).
•• A 90-day EOC analysis of 938 robotic-assisted THAs compared with 4670 manual THAs from the 100% Medicare dataset showing RATHA patients used fewer home health visits, were less likely to have post index inpatient rehabilitation or SNF admissions and reduced 90-day EOC costs.
16.
Maldonado DR, Go CC, Kyin C et al. Robotic arm-assisted total hip arthroplasty is more cost-effective than manual total hip arthroplasty: a Markov model analysis. J. Am. Acad. Orthop. Surg. 29, e168–e177 (2021).
•• A Markov model analysis comparing RATHA and MTHA showing RATHA was cost saving compared to MTHA for both Medicare and private payers over a 5-year period.
17.
Clement ND, Gaston P, Bell A et al. Robotic arm-assisted versus manual total hip arthroplasty. Bone Joint Res. 10, 22–30 (2021).
18.
Emara AK, Zhou G, Klika AK et al. Is there increased value in robotic arm-assisted total hip arthroplasty?: a nationwide outcomes, trends, and projections analysis of 4,699,894 cases. Bone Joint J. 103-B, 1488–1496 (2021).
19.
Kirchner GJ, Lieber AM, Haislup B, Kerbel YE, Moretti VM. The cost of robot-assisted total hip arthroplasty: comparing safety and hospital charges to conventional total hip arthroplasty. J. Am. Acad. Orthop. Surg. 29, 609–615 (2021).
20.
Knight SR, Aujla R, Biswas SP. Total hip arthroplasty – over 100 years of operative history. Orthop. Rev. (Pavia) 3, 16 (2011).
21.
Callanan MC, Jarrett B, Bragdon CR et al. The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital. Clin. Orthop. Relat. Res. 469, 319–329 (2011).
22.
Bendich I, Vigdorchik JM, Sharma AK et al. Robotic assistance for posterior approach total hip arthroplasty is associated with lower risk of revision for dislocation when compared to manual techniques. J. Arthroplasty 37, 1124–119 (2022).
•• An analysis of 13,802 THAs from a single institution found that RATHA was associated with lower risk of revision for dislocation within 1 year of index surgery when compared to MTHA.
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 11 December 2022
Accepted: 15 March 2023
Published online: 5 May 2023
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Advantages of robotic arm-assisted total hip arthroplasty: a 90-day episode-of-care clinical utility and cost analysis. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0208
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jenna Bernstein, Jean-Baptiste Trouiller, Mina Kabiri, William G. Hamilton, Cost-Effectiveness of Computer-Assisted Fluoroscopic Navigation in Primary Total Hip Arthroplasty Compared With Robotic or Manual Techniques, JAAOS: Global Research and Reviews, 10.5435/JAAOSGlobal-D-25-00404, 10, 6, (2026).
- Warran Wignadasan, Christos Dragonas, Andreas Fontalis, Marc Jean Berna, Pit Putzeys, Romir Patel, Fares S Haddad, Economic evaluation of robotic-assisted versus manual total hip arthroplasty: a systematic review of cost and clinical outcomes, EFORT Open Reviews, 10.1530/EOR-2025-0179, 11, 6, (553-560), (2026).
- Michael S. Kim, Deeyana Roshanzaer, Melissa R. Romoff, Kylen Soriano, Ryan DiGiovanni, Russell Stitzlein, Steven Yang, Peter Hsiue, Utilization Trends and Surgical Outcomes of Technology-Assisted Total Hip Arthroplasty in the United States From 2014 Through 2024, Arthroplasty Today, 10.1016/j.artd.2026.101983, 39, (101983), (2026).
- Ka Lee Li, Sai Ka Li, Lawrence Chun Man Lau, Amy Cheung, Michelle Hilda Luk, Henry Fu, Thomas Ka Chung Leung, Kwong Yuen Chiu, Ping Keung Chan, Using a robotic-arm assisted system in revision total hip arthroplasty: surgical technique and a case series, HIP International, 10.1177/11207000251401840, 36, 2, (249-258), (2026).
- Wissem Tafat, Marcin Budka, David McDonald, Robert G. Middleton, Findlay Welsh, Thomas W. Wainwright, Robotic-assisted hip and knee replacement in NHS scotland: trends and efficiency implications (2020–2024), Journal of Robotic Surgery, 10.1007/s11701-025-03086-7, 20, 1, (2026).
- Yajing Gao, Yi Yang, Zhuofu Li, Bai Zang, Chengfengyi Yang, Feifei Zhou, Qiaoqin Wan, Systematic review of health economic evaluation of robot-assisted hip and knee arthroplasty, Health Economics Review, 10.1186/s13561-025-00701-z, 16, 1, (2025).
- Perry L. Lim, Marcos R. Gonzalez, Kevin Y. Wang, Nicholas Sauder, Hany S. Bedair, Christopher M. Melnic, Does Robotic Assistance Increase the Likelihood of Achieving the Minimal Clinically Important Improvement Following Total Hip Arthroplasty? Findings From a Propensity Score Matched Analysis of 1,364 Procedures, The Journal of Arthroplasty, 10.1016/j.arth.2025.05.015, 40, 11, (2930-2937), (2025).
- Perry L. Lim, Graham S. Goh, Hany S. Bedair, Christopher M. Melnic, Robotic Versus Manual Total Hip Arthroplasty: A Marginal Time-driven Activity-based Costing Analysis, Journal of the American Academy of Orthopaedic Surgeons, 10.5435/JAAOS-D-24-01498, 34, 2, (e227-e234), (2025).
- Alexander F. Heimann, William S. Murphy, Daniel C. Sun, Stephen B. Murphy, Accuracy of Acetabular Component Positioning Using a Mixed Reality-Guided Navigation System During Total Hip Arthroplasty, JBJS Open Access, 10.2106/JBJS.OA.24.00144, 10, 1, (2025).
- Jenna Bernstein, Anshu Gupta, Mina Kabiri, Jill W. Ruppenkamp, Laura Goldstein, Rodrigo Diaz, All Enabling Technology Is Not Created Equal: Comparing Outcomes of Computer-Assisted Fluoroscopic Navigation Versus Robotic-Assisted Total Hip Arthroplasty, JAAOS: Global Research and Reviews, 10.5435/JAAOSGlobal-D-24-00324, 8, 12, (2024).
- See more