Advanced or metastatic biliary tract cancer in Japan: a study using the Japan Medical Data Center payer claims database
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Biliary tract cancers are aggressive, with poor prognosis. This study describes clinical characteristics, treatment patterns and healthcare resource utilization in patients with metastatic biliary tract cancer in Japan. Materials & methods: This cohort-based study collected data from the Japan Medical Data Center claims database (2014–2018). Results: A total of 325 patients were included; 65.2% were male and the mean age was 59.2 years. A 47.6% had an Elixhauser Comorbidity Index score ≥5. Most frequent regimens were gemcitabine + cisplatin (52.9%) for first-line therapy and tegafur + gimeracil + oteracil for second-line therapy (48.6%) and third-line therapy (27.2%). Approximately 77% of patients had ≥1 hospital admission, with a median length of 57 days. Conclusion: This study provides insights on the characteristics and burden of metastatic biliary tract cancer in Japan, highlighting high disease burden in a younger population.
Biliary tract cancer (BTC) refers to a spectrum of invasive adenocarcinomas, including cholangiocarcinoma (tumor arising in the intrahepatic, perihilar or distal biliary tree), gallbladder cancer and ampullary cancer [1]. BTCs are usually diagnosed at an advanced stage, leading to a poor prognosis [2]. BTCs show a wide geographic variation and high incidence in some Asian and Latin–American regions [3]. The natural history, clinical presentation, response to treatment and prognosis differ by BTC tumor site [1].
Overall survival (OS) for metastatic biliary tract cancer (mBTC) without systemic chemotherapy is poor at 2.5–5.6 months [4]. Systemic treatment recommendations are similar across BTC tumor sites [5]. The combination of gemcitabine + cisplatin (GC) is the standard first-line (1L) therapy for mBTC, with an OS of approximately 11 months [5–7]. Several clinical trials and observational studies have investigated alternative 1L chemotherapy regimens for mBTC, including various combinations of gemcitabine, cisplatin, oxaliplatin, fluoropyrimidines and irinotecan. These studies have shown modest improvements in response rates and/or progression-free survival compared with GC but have not demonstrated a significant survival benefit [7].
No second-line (2L) therapy following disease progression has been established, although fluoropyrimidine-based regimens have been frequently used [8]. The ABC-06 trial showed improved OS with a modified leucovorin 5-fluorouracil oxaliplatin (FOLFOX) treatment versus best supportive care in patients previously treated with GC [9].
There is a growing interest in the use of immunotherapy in BTC, as it has shown promise in the treatment of other solid tumors. The use of immune checkpoint inhibitors (ICIs), such as pembrolizumab and nivolumab, either alone or in combination with chemotherapy or other agents has shown modest response rates ranging from 5.8 to 22% [10]. The use of durvalumab, an anti-PD-L1 antibody, has shown modest activity in BTC, with response rates ranging from 7 to 17% and an acceptable safety profile [11].
Healthcare resource utilization (HCRU) data for mBTC are limited. The Japan Medical Data Center (JMDC) employer-based claims database contains a comprehensive, longitudinal view of reimbursed healthcare encounters regardless of care setting (i.e., hospital and outpatient clinic). JMDC is accepted by the scientific community and health authorities as a reliable source and may provide relevant HCRU information.
This analysis describes the demographics, clinical profile, comorbidities and treatment patterns of Japanese patients with mBTC, filling the gap between randomized controlled trials and real-world data. In addition, this study assesses the impact of mBTCs on HCRU in Japan. This paper is reported in accordance with the STROBE reporting checklist [12].
Materials & methods
This cohort-based retrospective study consisted of a single cohort of incident patients diagnosed with mBTC (intrahepatic cholangiocarcinoma, extrahepatic cholangiocarcinoma, gallbladder cancer and ampullary cancer) between 1 January 2014 and 31 August 2018 (the selection period). The selected patients had ≥12 months of continuous prior insurance enrollment after mBTC diagnosis and had no other primary tumors diagnosed during the 12 month pre-index period.
Data were collected from the JMDC payer claims database, which contains anonymized claims data, including diagnoses, patient characteristics, prescriptions, medical procedures, laboratory tests, medical facility characteristics and healthcare costs associated with inpatient, outpatient and pharmacy encounters. The JMDC includes information from approximately 100 employee-based health insurance payers. The covered population comprises >16 million patients, which represents 7.9% of the Japanese population, including working adults and their dependents <75 years old. A separate public insurance system covers individuals >75 years. JMDC data is available from 2005 and is updated monthly. Mortality data are not complete for all patients: some death dates are missing because only deaths occurring in facilities covered by JMDC are captured, and deaths occurring outside these facilities are not systematically reported to JMDC.
The diagnosis of BTC was defined as ≥1 inpatient claim with a BTC diagnosis during the patient selection period or ≥2 medical claims (between 30 days and 180 days apart) with a BTC diagnosis in the outpatient setting.
International Classification of Diseases, Tenth Revision, codes C22.1, C23, C24.0, C24.1, C24.8 and C24.9 were used to identify and classify patients according to the BTC tumor type. The index date was the date of the first mBTC diagnosis. Patients were followed up until a record of death, disenrollment from insurance providing data to JMDC or data cutoff, whichever occurred first.
Treatment lines were captured based on an algorithm used in previous work to identify systemic anticancer treatment [13]. HCRU were assessed during the post-index period by treatment line via identification of claims for inpatient admissions and outpatient services, including surgeries, radiotherapy, pharmacy, laboratory tests, diagnostic imaging, home care and rehabilitation.
Baseline demographic and clinical characteristics included age, sex, whether the patient was the insurance holder or a dependent, BTC tumor sites, comorbidities and Elixhauser Comorbidity Index (ECI) scores. Treatment patterns assessed systemic anticancer regimens during the pre-index period.
Statistical analysis
Descriptive statistics were generated for all study variables, including the baseline demographic, clinical and treatment characteristics. The numbers and proportions of patients who received the most frequent treatment regimens in the 1L, 2L and third-line (3L) were reported. The duration of therapy (DOT) was summarized using standard descriptive statistics stratified by line of treatment. The median time to next treatment (TTNT) was estimated using the Kaplan–Meier method, and the first and third quartiles for median TTNT were also estimated.
Ethical statement
This study was conducted in accordance with the Declaration of Helsinki. JMDC is a fully anonymized database. Therefore, no independent ethics committee or institutional review board were required.
Results
Between 1 January 2014 and 31 July 2018, 1514 adult patients with a confirmed diagnosis of BTC were identified. Of these, 325 (21.5%) met the inclusion criteria and were included in analyses. The patient selection flowchart is presented in Figure 1.

Figure 1. Patient selection flowchart selection of patients with metastatic biliary tract carcinoma.
BTC: Biliary tract carcinoma; mBTC: Metastatic biliary tract carcinoma; NA: Not applicable.
Baseline patient characteristics are shown in Table 1. The mean age of patients with mBTC was 59.2 years, and 65.2% were male. Most patients were the insurance holders (72.3%). The most frequent BTC tumor sites were gallbladder cancer (32.6%), extrahepatic cholangiocarcinoma (32.3%) and intrahepatic cholangiocarcinoma (26.1%).
| Baseline patient characteristics† | All patients (n = 325) |
|---|---|
| Age at index date, years | |
| Mean (SD) | 59.2 (8.7) |
| Age category at index date, n (%) | |
| 18–49 years | 46 (14.1) |
| 50–59 years | 104 (32.0) |
| 60–69 years | 140 (43.1) |
| 70–75 years | 35 (10.8) |
| Sex | |
| Female | 113 (34.8%) |
| Male | 212 (65.2) |
| Insurance holder or dependent | |
| Dependent | 90 (27.7) |
| Insurance holder | 235 (72.3) |
| BTC tumor site‡ | |
| Intrahepatic cholangiocarcinoma | 85 (26.1) |
| Gallbladder cancer | 106 (32.6) |
| Extrahepatic cholangiocarcinoma | 105 (32.3) |
| Ampullary cancer | 26 (8.0) |
| Other and unspecified tumor sites | 34 (10.5) |
| Baseline comorbidities (5 most commonly occuring)§ | |
| Gastric ulcers | 144 (44.3) |
| Liver disease | 138 (42.5) |
| Hypertension | 133 (40.9) |
| Diabetes | 116 (35.7) |
| Cholangitis | 111 (34.1) |
| Comorbidities (n) | |
| Mean (SD) | 3.7 (2.4) |
| 0 | 16 (4.9) |
| 1 | 47 (14.5) |
| 2 | 50 (15.4) |
| 3 | 61 (18.8) |
| 4 | 49 (15.1) |
| ≥5 | 102 (31.4) |
| ECI score at baseline | |
| Mean (SD) | 4.5 (1.8) |
| 0 | 0 |
| 1 | 5 (1.54) |
| 2 | 34 (10.46) |
| 3 | 68 (20.92) |
| 4 | 63 (19.38) |
| ≥5 | 155 (47.69) |
†
Proportions may not sum to 100% due to rounding.
‡
Forty-nine patients had multiple primary BTC sites.
§
Patients may have had >1 comorbidity.
BTC: Biliary tract carcinoma; ECI: Elixhauser Comorbidity Index; SD: Standard deviation.
The average ECI score was 4.5, and almost half (47.7%) of patients had an ECI score ≥5. The population was characterized by a high prevalence of comorbidities at baseline and prior to the start of each treatment line. The most frequent comorbidities were gastric ulcers (44.3%), liver disease (42.3%), hypertension (40.9%), diabetes (35.7%) and cholangitis (34.2%).
(Table 2 & Figure 2) show the systemic treatments prescribed for 1L, 2L and 3L therapy. In addition, Table 2 also presents the DOT and TTNT for each line. Among 238 patients (73.2% of the total patients with mBTC) who received 1L therapy, GC was the most frequent regimen, prescribed for more than half the population (53.2%), followed by tegafur + gimeracil + oteracil (S-1; 18.5%) and gemcitabine monotherapy (10.1%).
| Treatment patterns | First line (n = 238) | Second line (n = 105) | Third line (n = 33) |
|---|---|---|---|
| Most frequent regimens, n (%)† | |||
| Gemcitabine + cisplatin | 126 (52.9) | 20 (19.0) | 8 (24.2) |
| S-1 | 44 (18.5) | 51 (48.6) | 9 (27.3) |
| Gemcitabine | 24 (10.1) | 7 (6.7) | 4 (12.1) |
| Gemcitabine + S-1 | 20 (8.4) | 13 (12.4) | 7 (21.2) |
| Other regimens | 24 (10.1) | 14 (13.3) | 5 (15.1) |
| DOT, days | |||
| Median | 94.5 | 77.0 | 59.0 |
| [Q1–Q3] | [35.0–191.0] | [36.0–163.0] | [34.0–162.0] |
| TTNT, days | |||
| Median | 114.0 | 122 | 78 |
| [Q1–Q3] | [54.0–213.0] | [64.0–198.0] | [34.0–214.0] |
†
Proportions may not sum to 100% due to rounding.
DOT: Duration of treatment; Q: Quartile; S-1: Tegafur + gimeracil + oteracil; TTNT: Time to next treatment.
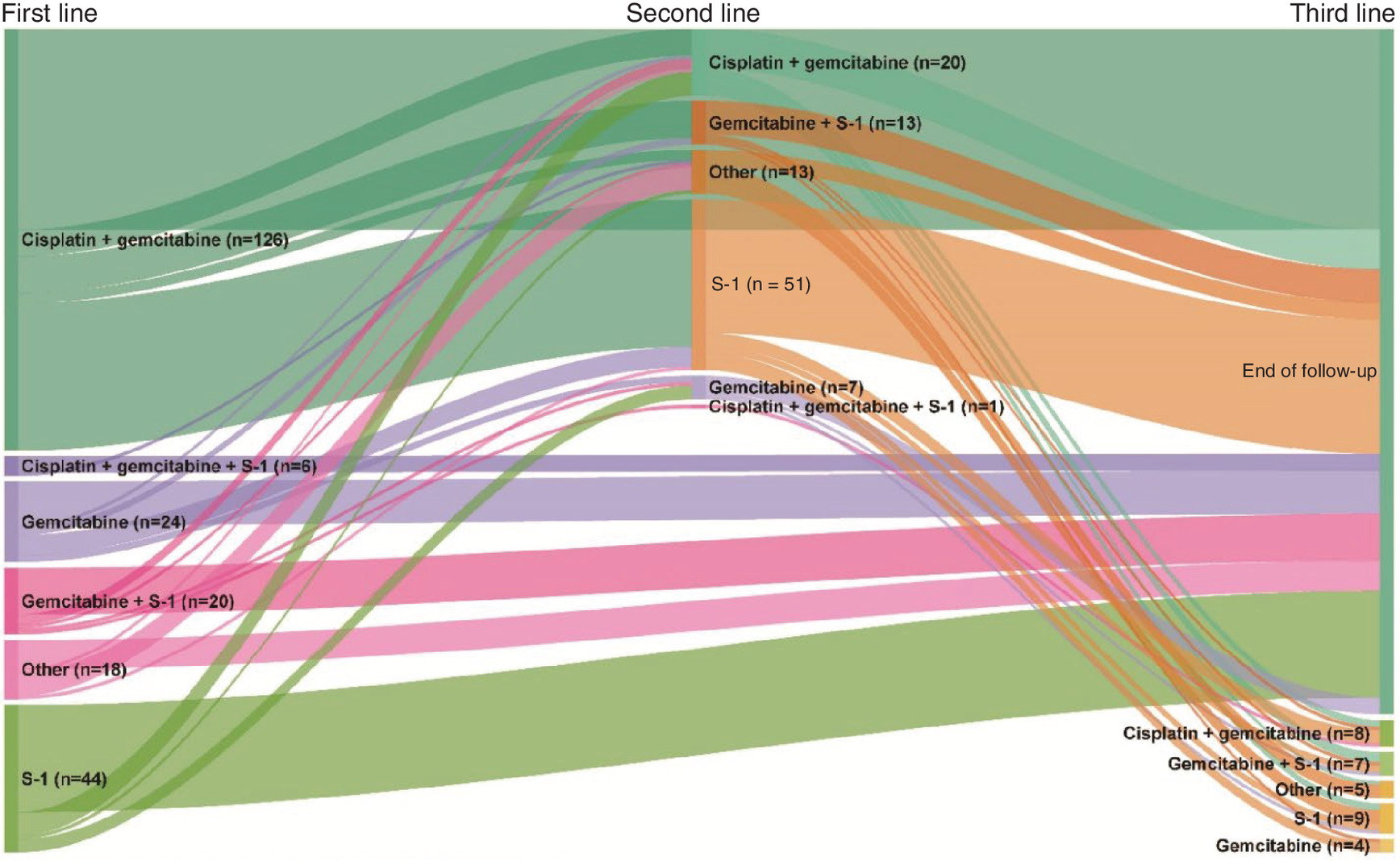
A total of 105 patients (32.3% of the total mBTC population, 44% of treated patients) received 2L therapy. S-1 was the most prescribed regimen (48.6%), followed by GC (19.0%) and gemcitabine + S-1 (12.4%).
The 3L therapy line was characterized by low patient counts (33 patients; 10.1% of the total population; 31% of 2L treated patients) and a similar prescribing pattern compared with 2L. The top three most frequent regimens were S-1 (27.3%), GC (24.2%) and gemcitabine + S-1 (21.2%).
The median DOT was 94.5 days, 77.0 and 59.0 days in the 1L, 2L and 3L, respectively, while the median TTNT was estimated at 114.0, 122.0 and 78.0 days, respectively.
Among the mBTC cohort, 84.6% of patients (n = 275) had ≥1 hospital admission, with the highest hospitalization rate recorded at 2L. The mean number of hospitalizations for the overall population was 3.2, higher for patients in 3L (3.8) compared with those in 1L (3.1) and 2L (2.9). The median length of stay was 70.0 days and varied by line of treatment (68.5, 53.0 and 63.0 days in 1L, 2L and 3L, respectively). The most common underlying medical conditions related to hospital admissions were gastroesophageal reflux disease with esophagitis, chronic pain, constipation, obstruction of bile duct, malignant neoplasm of gallbladder and cholangitis (Table 3).
| Characteristic | Total population (n = 325) | First line (n = 238) | Second line (n = 105) | Third line (n = 33) |
|---|---|---|---|---|
| Patients with ≥1 hospital admission, n (%) | 275 (84.6) | 198 (83.2) | 91 (86.7) | 27 (81.8) |
| Median hospital admissions, n | 2.0 | 2.0 | 2.0 | 3.0 |
| Median length of stay, days | 70.0 | 68.5 | 53.0 | 63.0 |
| Medical conditions related to hospital admissions (top 10 level 4 ICD 10 codes)† | ||||
| Gastroesophageal reflux disease with esophagitis | 123 (37.8) | 91 (38.2) | 39 (37.1) | 15 (45.4) |
| Other chronic pain | 113 (34.8) | 82 (34.4) | 32 (30.5) | 11 (33.3) |
| Constipation | 97 (29.8) | 67 (28.1) | 29 (27.6) | 10 (30.3) |
| Obstruction of bile duct | 89 (27.4) | 67 (28.1) | 30 (28.6) | 6 (18.2) |
| Malignant neoplasm of gallbladder | 88 (27.1) | 57 (23.9) | 23 (21.9) | 8 (24.2) |
| Cholangitis | 69 (21.2) | 56 (23.5) | 18 (17.1) | 5 (15.1) |
| Malignant neoplasm of liver and intrahepatic bile ducts/intrahepatic bile duct carcinoma | 67 (20.6) | 50 (21.0) | 22 (20.9) | 6 (18.2) |
| Secondary malignant neoplasm of respiratory and digestive organs‡/secondary malignant neoplasm of liver and intrahepatic bile duct§ | 64 (19.7) | 41 (17.2) | 22 (20.9) | 4 (12.1) |
†
Patients may have had >1 condition related to hospital admissions.
‡
Defined using ICD 10 codes C78.x.
§
Defined using ICD 10 codes C79.x.
ICD 10: International Classification of Diseases, Tenth Revision.
As presented in Figure 3, after the index date, 92.3% of the overall population had ≥1 outpatient visit (including all specialties), with a mean of 16 outpatient visits. The average number of outpatient visits decreased over time.
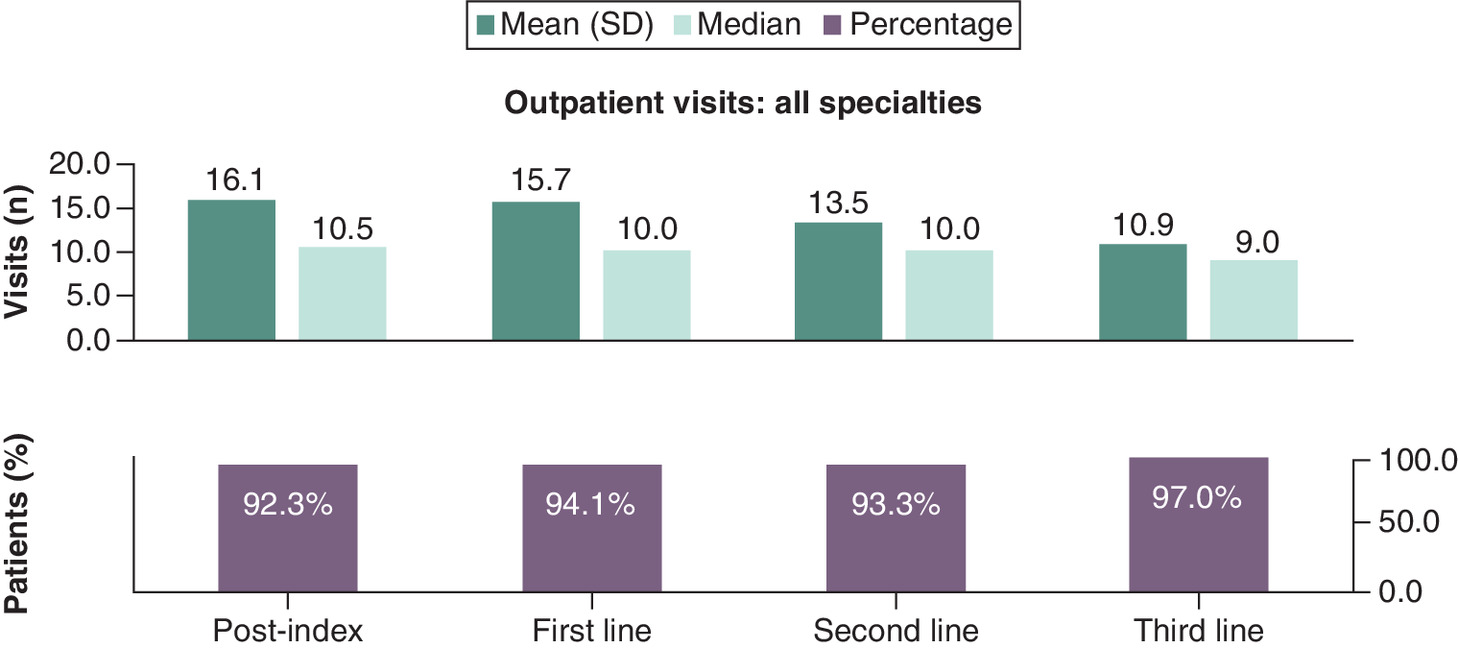
Figure 3. Outpatient visits during the post-index period.
SD: Standard deviation.
After the index date, almost all the study population had laboratory tests (96.9%; mean, 15.1) and diagnostic imaging (96.3%; mean, 8.7). The rate of resection surgeries was low (6.2%; mean, 0.1 surgeries) and 19.6% underwent radiotherapy. Almost one quarter of the total population had home care visits (23.7%; mean, 3.4 visits) and rehabilitation visits (23.1%; mean, 2.6 visits). A higher number of home care and rehabilitation visits was observed in 3L compared with 1L and 2L. Antibiotics were prescribed in 60.1% of the population during the 30 days before or after 1L initiation (50.4% of patients before; 38.7% after).
Discussion
This retrospective JMDC claims–based study described the profile of 325 patients diagnosed with mBTC in Japan, their treatment patterns and HCRU.
The baseline characteristics of patients should be interpreted considering the nature of JMDC, which covers working-age adults and their dependents. The mean age of patients at diagnosis was 59.2 years, lower than the mean age of 70 years reported in Japan by the Biliary Tract Cancer Registry (comprising data from 18,606 patients) between 2008 and 2013, likely due to an artifact of the JMDC database, which tends to reflect a younger population compared with the general population [14]. Another study using hospital-based claims in Japan also estimated a higher mean age of 73.4 years for patients with advanced mBTC [15]. The study population for this study was predominantly male (65.2%); in contrast, other studies reported a balanced distribution between sexes (male’s proportions vary between 47.8 and 56.9%) [16–18]. Tumor site distribution within this study was similar with a slightly lower proportion of extrahepatic cholangiocarcinoma (32.3%) compared with the hospital-based claims analysis by Kim et al. which reported 44.2% [15].
In this study, approximately 70% of patients received combined chemotherapy in 1L, and more than half of patients (52.9%) had received the GC combination. Since the UK ABC-02 trial in 2008, the GC regimen is considered the standard 1L therapy for mBTC, showing higher progression-free survival and OS than gemcitabine monotherapy [19]. The relatively young age of the study population may explain the frequent use of cisplatin-based combinations. The study by Danese et al. that included patients older than 66 years from the Surveillance, Epidemiology and End Results registry showed that, in 1L, only 34.2% received GC, while 35.1% received gemcitabine alone. The high median age at diagnosis (77 years) of this US population could explain the low frequency of cisplatin-based chemotherapy prescription [13]. In Japan, the FUGA-BT trial confirmed the noninferiority of 1L treatment with gemcitabine + S-1 versus GC in terms of OS [20].
In this analysis, S-1 was the second most prescribed agent in 1L. No randomized controlled trial has compared the efficacy of 1L S-1 with GC or other combinations. Patients treated with S-1 may show better compliance and higher quality of life than those who received cisplatin-based regimens [21]. The analysis by Kim et al. showed similar patterns in the hospital setting with GC being the most common 1L regimen (40.3%) followed by S-1 (27.5%) and gemcitabine monotherapy (14.3%) [15].
Real-world data regarding treatment options beyond 1L and 2L remain scarce [18]. The ABC-06 trial showed improved OS with modified leucovorin 5-fluorouracil oxaliplatin (FOLFOX) versus best supportive care in patients previously treated with GC [9]. In the present analysis, almost half of patients in 2L (48.6%) received S-1. Monotherapy was prescribed more frequently in 2L and 3L, which can be attributed to either the progressive deterioration of patients' performance status or the lack of evidence for the superiority of combination therapy over monotherapy in 2L. In addition, the patients in our analysis were treated prior to the publication of the ABC-06 trial results.
In this analysis, the median DOT was comparable to those reported by Danese et al. and Kim et al. for the 1L (94.5 and 98.5 days, respectively, vs 84 days), 2L (77 and 72 days, respectively, vs 60 days) and 3L (59 and 70 days, respectively, vs 62 days) [13,15].
The median TTNT was slightly longer for 2L than 1L (122 vs 114 days), which could be explained by the higher proportion of patients receiving S-1 in 2L and the better tolerability of this regimen compared with platinum-based regimens. In contrast, the study by Kim et al. showed that TTNT decreased with the number of lines of therapy received, lasting <1 year for each line [15].
At diagnosis, about 26.5% of overall patients with mBTC had cholecystitis, and 42.5% presented with liver disease. Biliary tract inflammation has a high recurrence rate (7–47%) and risks becoming chronic inflammation [22]. Cholangitis and cholecystitis have been associated with a higher risk of BTC [23,24]. A study evaluating the risk of cancer in 11,605 patients with liver cirrhosis found a tenfold increased risk for cholangiocarcinoma [25]. Despite the young age of the study population, the comorbidity burden was high; almost half of patients had ECI scores >5.
A substantial burden of illness is attributable to mBTC. Between 1990 and 2017, an increase of 75% in cases, 65% in deaths and 52% in disability adjusted life-years was estimated globally [26]. In the present study, about 84.6% of all patients had ≥1 hospital admission during the entire post-index period. According to the analysis by Danese et al., 78.2% of patients were hospitalized within 90 days of diagnosis, and 89% were hospitalized within 1 year of diagnosis [13]. Because Danese et al. includes a longer follow-up, the findings might be overestimated. Although data on the economic burden of BTC remain limited, several studies show that costs are driven mainly by hospital admissions. A study that evaluated cholangiocarcinoma in the US from a nationwide population-based inpatient database between 1997 and 2012 reported a significant increase in cholangiocarcinoma related hospital admissions and associated costs [27].
The median length of stay for the overall population was 70 days. Several factors contributed to the longer length of stay in Japan compared with other developed countries, including professional or cultural norms, different payment schemes and access to long-term care facilities [28,29].
Approximately 97% of patients had laboratory tests. In Japan, annual health check-up programs, especially for the working population and blood test monitoring during chemotherapy may explain the high frequency of laboratory tests.
In this study, a high rate of antibiotics use was reported in 1L. Therefore, the use of antibiotics in about 60% of patients is in line with clinical practice. Antibiotics are commonly administered to patients with BTC to treat cholangitis, prevent infections related to invasive procedures and reduce jaundice. The impact of antibiotics use in cancer patients is a recent line of research, with increasing evidence of lower efficacy of anticancer treatment and worse outcomes in some patient types. Several studies have shown that the concomitant use of antibiotics and ICIs for advanced cancers is associated with a reduced OS and less favorable response to treatment [30–34]. This impact depends on the timing of exposure to antibiotics [35]. In a pooled analysis of three clinical trials, the use of systemic antibiotics within 30 days of initiating anticancer therapy were associated with a decreased survival rate in patients treated with ICIs for advanced cancers [36].
Nearly 25% of the total population had rehabilitation visits and home care, with more visits recorded in 3L than in 1L and 2L. Even though these visits are rarely provided for patients with BTC because of the rapid progression of the disease, this finding is consistent with clinical practice in Japan. Japan’s Ministry of Health, Labor and Welfare has promoted home visits to provide better end-of-life care [37]. According to two surveys in the general population and in terminally ill cancer patients, home was the preferred place for end-of-life care [38,39]. In addition, most patients with cancer in Japan receive rehabilitation care in the early, advanced and terminal stages [40].
This study is one of the few studies that investigates real-world characteristics, treatment patterns and HCRU of patients with mBTC using a large claims database from Japan. Such real-world database studies provide information that can complement results from randomized clinical trials for mBTC. They have the potential to inform and improve clinical practice and help in development of guidelines by providing valuable insights into the actual usage and effectiveness of medical interventions in the real-world clinical setting. This could ultimately improve patient outcomes.
This study sheds light on the high burden of illness associated with mBTC, from the finding that most patients require at least one hospital admission during the post-index period and the relatively long median length of stay of 70 days. Insights into HCRU and healthcare costs can also inform healthcare policies and guide decisions on resource allocation.
One of the knowledge gaps in this study is the scarcity of real-world data regarding prescribing patterns beyond the first and second line. This suggests a need for further research in this area to better understand treatment options for patients with mBTC who have exhausted 1L and 2L therapies. Future research could further examine the reasons behind the high burden of illness and extended length of stay in mBTC patients. This could potentially lead to the development of new treatment strategies and care models to improve outcomes for patients with mBTC.
One of the limitations of this study is that cancer staging information is not available in JMDC, thus, this study used a proxy to identify patients with metastatic disease based on ICD-10 codes (C77, C78, C79) and on the presence/absence and timing of the surgery. Therefore, the study population may have some biases caused by missing or misclassified mBTC patients, which may affect the generalizability of the results to the Japanese mBTC population.
Moreover, JMDC is suitable for understanding BTC treatment and resource utilization in a younger, highly comorbid population. These patients reflect employees working in medium to large companies and their family members. Most patients with BTC are diagnosed in their 70s; thus, another limitation of this analysis is the restricted coverage of patients aged <75 years. Few people aged >65 years are expected to be active and insured by the companies that provide data for JMDC. In addition, individuals aged >75 years are not included in this data source because their health insurance is covered by a separate public system. Therefore, the JMDC population is not fully representative of the Japanese BTC population, but this study still provides insights on treatment in a younger population group. Claims-based studies have additional limitations of misclassification, particularly for administrative claims, as inaccurate coding may occur since the data analyzed is mainly used for billing purposes and is subject to interpretation by analysts. It is possible that some treatments are not reimbursed, and therefore not captured by JMDC, including very expensive drugs, experimental or alternative therapies and those administered as part of a clinical trial; this limitation is common in healthcare claims-based studies.
Conclusion
This study provides a real-world look at the clinical profile, treatment patterns and HCRU of patients diagnosed with mBTC in Japan. These data show that the most common BTC tumor sites were extrahepatic cholangiocarcinoma, gallbladder cancer and intrahepatic cholangiocarcinoma. GC was the most prescribed regimen in 1L, while the use of S-1 prevailed in 2L and 3L. Despite the young age of the study population, the clinical and economic burden attributable to mBTC was high. Results described can complement clinical trials and provide a broader clinical profile in a high-morbidity, younger population.
•
The mean age of patients at diagnosis was 59.2 years, younger than published literature. This may be an artifact of the Japan Medical Data Center database, which tends to reflect a younger population overall compared with the general population.
•
The most common tumors were gallbladder cancer (32.6%), extrahepatic cholangiocarcinoma (32.3%) and intrahepatic cholangiocarcinoma (26.1%), while ampullary cancer (8.0%) was the least frequent.
•
Approximately 70% of patients received combination chemotherapy in first-line (1L), and more than half of patients (52.9%) received gemcitabine + cisplatin combination.
•
S-1 was the second most prescribed agent in 1L. Patients treated with S-1 may show better compliance and higher quality of life than those who received cisplatin-based regimens.
•
Almost half of patients in second-line (2L) (48.6%) received S-1 in this analysis. Monotherapy was prescribed more frequently in 2L and 3L, which can be attributed to either the progressive deterioration of patients’ performance status or the lack of evidence for the superiority of combination therapy over monotherapy in 2L.
•
The median time to next treatment was slightly longer for 2L than 1L (122 vs 114 days), which could be explained by the higher proportion of patients receiving S-1 in 2L and the better tolerability of this regimen compared with platinum-based regimens.
•
Despite the young age of the study population, the comorbidity burden was high; almost half of patients had ECI scores >5.
•
In the present study, about 84.6% of all patients had ≥1 hospital admission during the entire postindex period.
•
The median length of stay for the overall population was 70 days. Several factors contributed to the longer length of stay in Japan compared with other developed countries, including professional or cultural norms, different payment schemes and access to long-term care facilities.
•
A high rate of antibiotics use was reported in 1L. Therefore, the use of antibiotics in about 60% of patients is in line with clinical practice.
Author contributions
All authors were involved in developing the content of the publication. R Argoubi: study concept, conducted analyses, data interpretation and manuscript editing. M Furegato: data interpretation and manuscript editing. P Medina: data interpretation and manuscript editing. S Bobiak: study concept, manuscript editing and critical revision. ES Reese: data interpretation, manuscript editing and critical revision.
Financial & competing interests disclosure
This study was funded by EMD Serono, MA, USA (CrossRef Funder ID no. 10.13039/100004755) and was previously part of an alliance between Merck and GlaxoSmithKline. R Argoubi, M Furegato and P Medina report employment with Cerner Enviza, which is the company supporting the execution of this EMD Serono-sponsored study. ES Reese and S Bobiak report employment with EMD Serono Research & Development Institute, Inc. (MA, USA), an affiliate of Merck KGaA. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Editorial support was provided by K Parai, ClinicalThinking, which was funded by Merck and was previously part of an alliance between Merck and GlaxoSmithKline in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Ethical conduct of research
This study was conducted in accordance with the Declaration of Helsinki. JMDC is a fully anonymized database. Therefore, no independent ethics committee or institutional review board were required.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Valle JW, Kelley RK, Nervi B, Oh DY, Zhu AX. Biliary tract cancer. Lancet 397(10272), 428–444 (2021).
2.
Cidon EU. Resectable cholangiocarcinoma: reviewing the role of adjuvant strategies. Clin. Med. Insights Oncol. 10, 43–48 (2016).
3.
Randi G, Malvezzi M, Levi F et al. Epidemiology of biliary tract cancers: an update. Ann. Oncol. 20(1), 146–159 (2009).
4.
Glimelius B, Hoffman K, Sjoden PO et al. Chemotherapy improves survival and quality of life in advanced pancreatic and biliary cancer. Ann. Oncol. 7(6), 593–600 (1996).
5.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Hepatobiliary cancers. Version 5.2021 (2021). https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf
6.
Furuse J, Takada T, Miyazaki M et al. Guidelines for chemotherapy of biliary tract and ampullary carcinomas. J. Hepatobiliary Pancreat. Surg. 15(1), 55–62 (2008).
7.
Rizzo A, Brandi G. First-line chemotherapy in advanced biliary tract cancer ten years after the ABC-02 Trial: “And Yet It Moves!”. Cancer Treat. Res. Commun. 27, 100335 (2021).
8.
Tella SH, Kommalapati A, Borad MJ, Mahipal A. Second-line therapies in advanced biliary tract cancers. Lancet Oncol. 21(1), e29–e41 (2020).
9.
Lamarca A, Palmer DH, Wasan HS et al. ABC-06 | A randomised Phase III, multi-centre, open-label study of active symptom control (ASC) alone or ASC with oxaliplatin / 5-FU chemotherapy (ASC + mFOLFOX) for patients (pts) with locally advanced / metastatic biliary tract cancers (ABC) previously-treated with cisplatin/gemcitabine (CisGem) chemotherapy. J. Clin. Oncol. 37(Suppl. 15), 4003 (2019).
10.
Ricci AD, Rizzo A, Brandi G. Immunotherapy in biliary tract cancer: worthy of a second look. Cancer Control 27(3), 1073274820948047 (2020).
11.
Rizzo A, Ricci AD, Brandi G. Durvalumab: an investigational anti-PD-L1 antibody for the treatment of biliary tract cancer. Expert Opin. Investig. Drugs 30(4), 343–350 (2021).
12.
von Elm E, Altman DG, Egger M et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J Clin Epidemiol. 61, 344–349 (2008).
13.
Danese M, Lubeck D, Gleeson M, Bobiak S. PCN322 Treatment of advanced biliary tract cancer (BTC) after progression on first-line (1L) systemic therapy. Value Health 22, S498–S499 (2019).
•• Chemotherapy use for patients with biliary tract cancer (BTC) from the Surveillance, Epidemiology and End Results (SEER) data linked with Medicare claims, was described. Variations in second-line regimens reflects a lack of consensus on how to treat older patients with advanced BTC who failed first-line treatment.
14.
Ishihara S, Horiguchi A, Miyakawa S, Endo I, Miyazaki M, Takada T. Biliary tract cancer registry in Japan from 2008 to 2013. J. Hepatobiliary Pancreat. Sci. 23(3), 149–157 (2016).
15.
Kim SW, Wang X, Chen CC, Wada S, Garside J, Reese ES. Characteristics, treatment patterns, and healthcare costs of advanced/metastatic biliary tract cancer patients in Japan. Ann. Oncol. 33, S496 (2022).
16.
Beaulieu C, Lui A, Yusuf D et al. A population-based retrospective study of biliary tract cancers in Alberta, Canada. Curr. Oncol. 28(1), 417–427 (2021).
17.
Ji JH, Song HN, Kim RB et al. Natural history of metastatic biliary tract cancer (BTC) patients with good performance status (PS) who were treated with only best supportive care (BSC). Jpn J. Clin. Oncol. 45(3), 256–260 (2015).
18.
Thol F, Gairing SJ, Czauderna C et al. Outcomes in patients receiving palliative chemotherapy for advanced biliary tract cancer. JHEP Rep. 4(3), 100417 (2022).
19.
Oneda E, Abu Hilal M, Zaniboni A. Biliary tract cancer: current medical treatment strategies. Cancers (Basel) 12(5), 1237 (2020).
20.
Morizane C, Okusaka T, Mizusawa J et al. Combination gemcitabine plus S-1 versus gemcitabine plus cisplatin for advanced/recurrent biliary tract cancer: the FUGA-BT (JCOG1113) randomized Phase III clinical trial. Ann. Oncol. 30(12), 1950–1958 (2019).
• A clinical trial of gemcitabine + S-1 versus gemcitabine + cisplatin for advanced/recurrent BTC gemcitabine + S-1 was non-inferior to gemcitabine + cisplatin in terms of overall survival and progression-free survival and was associated with less clinically significant adverse events. Both treatments were generally tolerable.
21.
Zheng W, Ying J, Zhou Y et al. The efficacy and safety of first-line chemotherapies for advanced biliary tract cancer: a network meta-analysis. J. Cancer 10(1), 257–266 (2019).
• A network meta-analysis of clinical trial on the efficacy and safety of first-line chemotherapies for advanced BTC. S-1 was associated with better compliance and quality of life than cisplatin-based regimens.
22.
Kimura Y, Takada T, Strasberg SM et al. TG13 current terminology, etiology, and epidemiology of acute cholangitis and cholecystitis. J. Hepatobiliary Pancreat. Sci. 20(1), 8–23 (2013).
23.
Ishiguro S, Inoue M, Kurahashi N, Iwasaki M, Sasazuki S, Tsugane S. Risk factors of biliary tract cancer in a large-scale population-based cohort study in Japan (JPHC study); with special focus on cholelithiasis, body mass index, and their effect modification. Cancer Causes Control 19(1), 33–41 (2008).
24.
Tsai TY, Lin CC, Peng CY et al. The association between biliary tract inflammation and risk of digestive system cancers: a population-based cohort study. Medicine (Baltimore) 95(31), e4427 (2016).
25.
Sorensen HT, Friis S, Olsen JH et al. Risk of liver and other types of cancer in patients with cirrhosis: a nationwide cohort study in Denmark. Hepatology 28(4), 921–925 (1998).
26.
Ouyang G, Liu Q, Wu Y et al. The global, regional, and national burden of gallbladder and biliary tract cancer and its attributable risk factors in 195 countries and territories, 1990 to 2017: a systematic analysis for the Global Burden of Disease Study 2017. Cancer 127(13), 2238–2250 (2021).
27.
Wadhwa V, Jobanputra Y, Thota PN, Narayanan Menon KV, Parsi MA, Sanaka MR. Healthcare utilization and costs associated with cholangiocarcinoma. Gastroenterol. Rep. (Oxf). 5(3), 213–218 (2017).
• A study of National Inpatient Sample Database of cholangiocarcinoma in the US between 1997 and 2012 reported a significant increase in cholangiocarcinoma related hospital admissions and associated costs, and a decrease in the mean length of stay and in-hospital mortality rate.
28.
Kunisawa S, Fushimi K, Imanaka Y. Reducing length of hospital stay does not increase readmission rates in early-stage gastric, colon, and lung cancer surgical cases in Japanese acute care hospitals. PLOS ONE 11(11), e0166269 (2016).
29.
Tiessen J, Kambara H, Sakai T, Kato K, Yamauchi K, McMillan C. What causes international variations in length of stay: a comparative analysis for two inpatient conditions in Japanese and Canadian hospitals. Health Serv. Manage. Res. 26(2–3), 86–94 (2013).
• Administrative patient-level data were collected from Japanese and Canadian hospitals to examine factors impacting the length of stay. Japanese length of stay was significantly longer than that in Canada. Non-clinical factors contribute to international differences in length of stay which may include professional or cultural norms, differing payment schemes and access to long-term care facilities.
30.
Chalabi M, Cardona A, Nagarkar DR et al. Efficacy of chemotherapy and atezolizumab in patients with non-small-cell lung cancer receiving antibiotics and proton pump inhibitors: pooled post hoc analyses of the OAK and POPLAR trials. Ann. Oncol. 31(4), 525–531 (2020).
31.
Derosa L, Hellmann MD, Spaziano M et al. Negative association of antibiotics on clinical activity of immune checkpoint inhibitors in patients with advanced renal cell and non-small-cell lung cancer. Ann. Oncol. 29(6), 1437–1444 (2018).
32.
Mohiuddin JJ, Chu B, Facciabene A et al. Association of antibiotic exposure with survival and toxicity in patients with melanoma receiving immunotherapy. J. Natl Cancer Inst. 113(2), 162–170 (2021).
33.
Pinato DJ, Howlett S, Ottaviani D et al. Association of prior antibiotic treatment with survival and response to immune checkpoint inhibitor therapy in patients with cancer. JAMA Oncol. 5(12), 1774–1778 (2019).
34.
Schett A, Rothschild SI, Curioni-Fontecedro A et al. Predictive impact of antibiotics in patients with advanced non small-cell lung cancer receiving immune checkpoint inhibitors: antibiotics immune checkpoint inhibitors in advanced NSCLC. Cancer Chemother. Pharmacol. 85(1), 121–131 (2020).
35.
Wilson BE, Routy B, Nagrial A, Chin VT. The effect of antibiotics on clinical outcomes in immune-checkpoint blockade: a systematic review and meta-analysis of observational studies. Cancer Immunol. Immunother. 69(3), 343–354 (2020).
36.
Vellanki PJ, Marur S, Bandaru P et al. Evaluation of the correlation between antibiotic use and survival in patients with recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC) treated with immune checkpoint inhibitors (ICIs). J. Clin. Oncol. 38(Suppl. 15), 6509–6509 (2020).
37.
Ministry of Health, Labour and Welfare. Reassuring home medical care and long-term care. Tokyo, Japan (2012). https://www.mhlw.go.jp/seisakunitsuite/bunya/kenkou_iryou/iryou/zaitaku/dl/anshin2012.pdf
38.
Hirabayashi Y, Miyashita M, Kawa M, Kazuma K, Yamashita K, Okamoto N. Factors relating to terminally ill cancer patients' willingness to continue living at home during the early phase of home care after discharge from clinical cancer centers in Japan. Palliat. Support. Care 5(1), 19–30 (2007).
• A questionnaire survey of a sample of Japanese terminally ill cancer patients and their caregivers showed that home was the preferred place for end-of-life care.
39.
Sanjo M, Miyashita M, Morita T et al. Preferences regarding end-of-life cancer care and associations with good-death concepts: a population-based survey in Japan. Ann. Oncol. 18(9), 1539–1547 (2007).
40.
Hamaguchi T, Okamura H, Nakaya N et al. Survey of the current status of cancer rehabilitation in Japan. Disabil. Rehabil. 30(7), 559–564 (2008).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 2 December 2022
Accepted: 2 May 2023
Published online: 31 May 2023
Keywords:
Topics
Authors
Funding Information
EMD Serono, Billerica, MA, USA (CrossRef Funder ID: 10.13039/100004755) and was previously part of an alliance between Merck and GlaxoSmithKline
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Advanced or metastatic biliary tract cancer in Japan: a study using the Japan Medical Data Center payer claims database. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0201
Export citation
Select the citation format you wish to export for this article or chapter.