Protocol for the implementation of a statewide mobile addiction program
Publication: Journal of Comparative Effectiveness Research
Abstract
With overdose deaths increasing, improving access to harm reduction and low barrier substance use disorder treatment is more important than ever. The Community Care in Reach® model uses a mobile unit to bring both harm reduction and clinical care for addiction to people experiencing barriers to office-based care. These mobile units provide many resources and services to people who use drugs, including safer consumption supplies, naloxone, medication for substance use disorder treatment, and a wide range of primary and preventative care. This protocol outlines the evaluation plan for the Community in Care® model in MA, USA. Using the RE-AIM framework, this evaluation will assess how mobile services engage new and underserved communities in addiction services and primary and preventative care.
Background & rationale
Background
Drug overdose continues to claim the lives of individuals in MA, USA and across the country at epidemic rates. In 2020 there were an estimated 2106 deaths from opioid related overdose in MA, USA [1], nearly six deaths per day. The overdose crisis was exacerbated by the COVID-19 pandemic, with increased barriers to addiction services caused by restrictions designed to limit disease transmission as well as increased isolation due to risk of infection [2]. Evidence-based interventions proven to reduce death and disease among people who use drugs, include medications for treating opioid use disorder (MOUD) [3], distribution of naloxone (to reverse an opioid overdose) to people who use drugs and to their close contacts [4] and providing safer consumption equipment (to reduce infections such as HIV) and counseling [5]. Despite these strategies to reduce overdose death rates, people who use drugs – especially those who are unhoused – face ongoing barriers to addiction treatment and primary and preventive care. These barriers include limited access to MOUD and other addiction services [6], regulatory restrictions, competing priorities and stigma in the healthcare system experienced by people living with substance use disorder (SUD) [7,8].
In the case of MOUD, success can be measured via the ‘treatment cascade of care’ (see effectiveness component in Table 1), a framework for studying opioid use disorder (OUD) services use [9]. This framework seeks to identify transitions where patients are most likely lost to follow-up (e.g., between the receipt of prescription and prescription fill, or between filling the 2nd- and 3rd-month prescriptions) [10]. People experiencing homelessness have a high drop-off rate from office-based OUD treatment, an effective intervention to reduce mortality risk [10]. Lowering the barriers to OUD treatment, for example, by providing mobile OUD services, may lead to reduced mortality as well as building trust and greater engagement in office-based OUD treatment [10]. For health services more generally, current literature has shown that mobile health clinics are successful in reaching and delivering services to vulnerable populations and in removing barriers to care [11].
| Framework Component | Metrics | Collection method | Timeline |
|---|---|---|---|
| Reach | • n program encountersA • n patient encountersA,B • n buprenorphine patientsA • n naloxone kits distributedC | A. Monthly submissions from programs B. MDPH aggregate naloxone data C. MDPH patient data | Years 1–3 |
| Effectiveness | • OUD treatment cascade of careA: ○ n diagnosed with OUD ○ n initiated on medication for OUD ○ n retained in treatment, 28 days ○ n retained in treatment, 60 days ○ n retained in treatment, 90 days ○ n retained in treatment, 180 days • Reduced overdose rates in target areasB | A. Bi-annual submissions from programs B. MDPH overdose data | Years 2–3 |
| Adoption | • Program staff input via interviews (mobile team/IT)B • Participation and feedback from technical assistance sessionsC • Perceived community receptionB,C • Repeat visitsA | A. Monthly submissions from programs B. Program visits conducted by evaluation team C. Monthly technical assistance facilitated discussions | Years 1–3 |
| Implementation | • Mobile team impressions/feedbackB,C • Referrals made to regular care in more traditional healthcare settingsA • Community presenceB,C • Fidelity to modelB,C | A. Monthly submissions from programs B. Program visits conducted by evaluation team C. Monthly technical assistance facilitated discussions | Years 1–2 |
| Maintenance | • OUD treatment cascade of care: rate of long-term (180 days) retentionA • Program staff input via interviews (mobile team/CHC staff)B • Reduced overdose rates in target areasC,D | A. Bi-annual submissions from programs B. Program visits conducted by evaluation team C. MDPH overdose data D. Other existing data, including literature | Years 2–3 |
CHC: Community Health Center; IT: Implementation team; MDPH: Massachusetts Department of Public Health; OUD: Opioid use disorder.
Existing models
By combining elements of clinical care, harm reduction and mobility, many programs have found success at serving people living with SUDs. The Seattle-based Safe, Healthy, Empowered Clinic implemented a mobile clinic model to bring low-barrier medical care to socially marginalized women at a drop-in center, resulting in decreased emergency room services for outpatient needs and increased accessibility of medical and social services [12]. Similarly, The spot mobile clinic in Baltimore was co-located with syringe services programs (SSPs) with the objective to integrate buprenorphine (one of the three US FDA-approved MOUD) services and medical care for people who use drugs with harm reduction services already offered at the SSPs. Researchers found that individuals who received a prescription for buprenorphine at The spot mobile clinic were more likely to receive other preventative services including vaccination, naloxone distribution and HIV and sexually-transmitted infections (STI) testing [13].
Finally, the Sex Worker Promoting Action, Risk Reduction and Community Mobilization (SPARC) drop-in center in Baltimore augmented its programming with mobile outreach services, resulting in reduced incidence of HIV and sexually transmitted infections in female sex workers using drugs [14]. Despite the findings described above, concerns over mobile programs include a fear of a diminished role and funding for traditional primary care, lack of patient follow-up in mobile settings and lack of sustainability [15]. Nevertheless, mobile health services are a portal of entry for individuals at highest risk for overdose death, many of whom are not currently engaged with traditional healthcare for myriad reasons including stigma, insurance issues, lack of transportation and competing comorbidities.
Rationale
In Massachusetts, the Community Care in Reach® (CCiR) model builds on decades of mobile harm reduction and HIV services funded by the state’s Department of Public Health (DPH) and involves a mobile unit with integrated harm reduction services and clinical care for people who use drugs [16]. The infographic illustrates how CCiR combines service elements of office-based clinical care programs and harm reduction programs while eliminating barriers posed by these traditional models (Supplementary Figure 1). We note that while there are several FDA-approved medicines to treat various SUDs, we include only buprenorphine specific outcome measures. This is because OUD is a priority of this model, the restrictions on methadone provision and buprenorphine treatment is the most frequently used treatment medication provided by the programs.
The CCiR model allows for a flexible, rapid response of harm reduction and clinical services and adapts to the changing overdose geo landscape. Programs locate mobile vans in areas of greatest need based on overdose data from DPH. For example, mobile outreach sessions are often based in locations that see consistently high rates of overdose. Additionally, the schedule and location of these vans are re-evaluated when data point to a new or emerging need [16]. The model leverages its mobility, having the flexibility to alter the deployment locations and schedule to respond to the changing needs of the community in a way that traditional brick-and-mortar sites (including opioid treatment programs) cannot.
Despite the effectiveness of MOUD in preventing overdose deaths, it was estimated in 2017 over 70 percent of people who needed treatment for OUD did not receive it [17]. CCiR is designed to eliminate barriers, by mobilizing essential services such as harm reduction and clinical care including MOUD and bringing these services directly to individuals at greatest risk of near-term death from overdose. CCiR is well-suited to expand access to underused MOUD, provide a broader spectrum of services that is less frequently offered in traditional brick-and-mortar clinical care. A core element of mobile vans is the provider building a trusting relationship with the patients, thus re-engaging individuals in care who had been previously disconnected due to finances, stigma and other barriers. By prioritizing communities of color, access expansion through CCiR’s mobile programming can also reduce inequities currently seen in addiction treatment and service utilization.
The evaluation of this intervention is designed to capture the cumulative effect of combining harm reduction services, clinical addiction care and mobility to serve populations at high risk for overdose. Whereas each of these evidence-based programmatic elements have been evaluated individually [4–6,11], there is a dearth of information on the cumulative impact of combining all three elements in one service model. We outline here an analysis that uses the RE-AIM framework to measure the impact of CCiR on its target population as well as the experience of the program staff in implementing the model. The results will be essential in understanding the benefits of reducing service silos by using a more comprehensive approach to low-barrier addiction care.
Design
Overview
Based on the success of the Boston pilot [16], the CCiR model was expanded starting in 2020 to four programs across Massachusetts (Figure 1). After signing contracts that include model requirements, the new programs received funding from the Massachusetts Department of Public Health, Bureau of Substance Addiction Services (MDPH-BSAS) and technical support from The Kraft Center for Community Health at Massachusetts General Hospital (Kraft Center). Each program secured a specialized vehicle equipped to provide medical care with a sink, medical supplies, Wi-Fi and a private medical examination area. Preparation of implementation began in 2021. Data collection began in 2022 and will run through 2024.
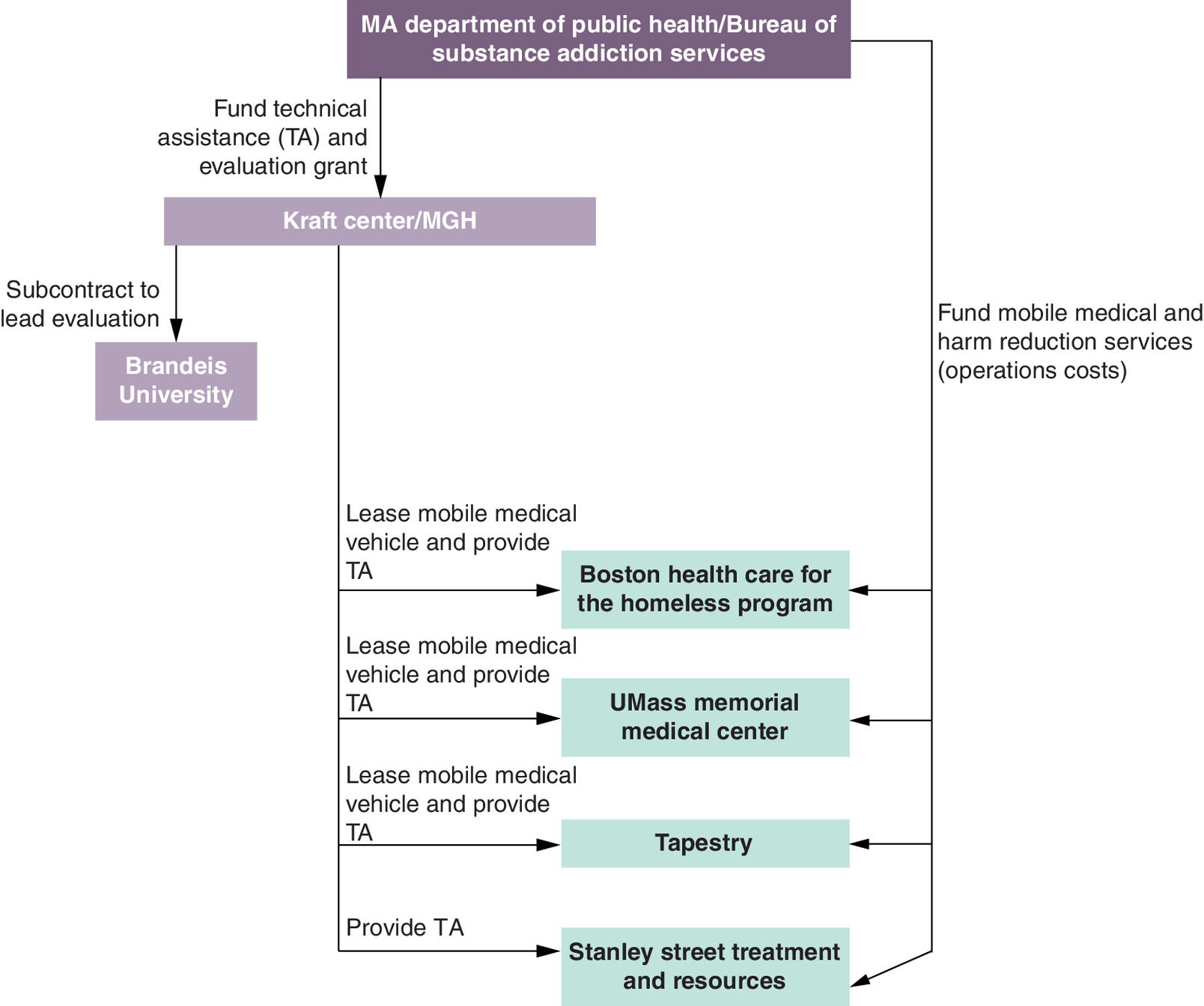
Figure 1. Stakeholders involved in the evaluation of pilot expansion of The Community Care in Reach model.
MA: Massachusetts; MGH: Massachusetts General Hospital; TA: Technical assistance.
In keeping with the CCiR model, each program’s team includes at least one clinician practiced in buprenorphine treatment and as many as three outreach workers trained in harm reduction strategies, among other support staff. Outreach workers reflect the diversity of the communities they serve and hiring decisions have prioritized staff members with lived experience with SUD. Programs that are not already SSPs themselves partner with a local agency to ensure staff receive necessary naloxone and other harm reduction trainings on an ongoing basis. The harm reduction workers and clinical practitioners provide services both near the parked mobile unit and on board the vehicle depending on the needs of the individual requesting services. Services include the prescription and initiation of MOUD such as buprenorphine; the distribution and collection of safer consumption supplies, such as syringes and glass pipes; distribution of naloxone kits; preventive care such as immunizations and screenings; provision of community drug checking services, such as fentanyl test strips; chronic disease management such as HIV treatment, hypertension management and diabetes management; skin and soft tissue infection care; and referrals for social and other medical services, including specialty care and behavioral health services [18–20].
Setting & participants
The four programs implementing the CCiR model prioritize cities, towns and neighborhoods experiencing consistently high rates of substance use and overdose. Data for siting clinic locations comes from a combination of publicly available, quarterly Massachusetts overdose reports from the Massachusetts Department of Public Health, municipal data on emergency medical services transports for narcotic related events and anecdotal information acquired from SSP staff and other addiction and homeless support services. The Kraft center receives data from Boston emergency medical services in a very timely manner through a partnership with the City of Boston. The quarterly MDPH data has a lag of approximately 4 months.
Any individuals experiencing barriers to primary care and addiction services are eligible to participate in the CCiR model, including those who are not currently engaged with the healthcare system in any capacity and those whose current care providers do not offer access to addiction services. There is no specific age requirement. Adults with SUD not currently engaged in regular care represent the core population served by the program. The staff in mobile vans identifies potential participants through: regularly canvassing areas around clinical sites; raising awareness of the program with local stakeholders and community leaders who provide referrals; and encouraging word-of-mouth promotion of the program. The CCiR model also emphasizes equity, ensuring clinical sites include locations in communities of color and that services are provided by staff that reflect the diversity of their patient population.
Implementation strategies
Implementation of the CCiR involves a several key players (Figure 1). The Kraft Center, based on its involvement with the pilot program in Boston, provides technical assistance. The Kraft Center is housed within Massachusetts General Hospital. It’s primary mission is to expand access to high quality healthcare for vulnerable populations by developing innovative programming, piloting innovations locally and disseminating effective programming state and nationwide. Kraft Center owns three of the four vehicles and leases them to the programs. The Kraft Center hosts virtual monthly technical assistance sessions to provide guidance on program specific issues, foster cross-program learning, share best practices, troubleshoot problems, hear expert speakers and explore common themes and issues. These sessions foster a learning collaborative and a supportive network. Learning collaboratives have been used for many initiatives and can improve outcomes by facilitating collaboration through sharing of resources and ideas among participants [21–25].
MDPH-BSAS funds the services provided on the vans and provides data needed for the evaluation. Brandeis University is conducting the evaluation component. Data collection tools and protocols are standardized across the four programs to allow for cross-program analysis and evaluation of fidelity to the model. Mobile van programs complete a standardized intake form on program patients for MDPH, as well as a monthly online survey (Qualtrics Survey software) for the Brandeis evaluation team that captures aggregate data for outreach encounters and clinical services provided. Once every 6 months, also via Qualtrics Survey software, programs will report on measures related to initiating and engaging patients on OUD medication treatment, (the ‘OUD treatment cascade of care’, see Table 1).
Informed consent for the evaluation is not being obtained since personal data are not collected by the Brandeis evaluation team. This protocol has been approved by the Institutional Review Boards for Massachusetts Department of Public Health and Brandeis University.
Evaluation framework & outcome measures
RE-AIM framework
The RE-AIM framework [26] informs all aspects of this evaluation (Table 1). RE-AIM identifies the components of a program that produce valued outcomes and reach the target population, while also detecting practices that may hinder or reduce health inequalities in a community [27]. The framework includes five core dimensions: ‘Reach’, ‘Effectiveness’, ‘Adoption’, ‘Implementation’ and ‘Maintenance’. Each dimension evaluates the impact of the program on either the individual and/or organization level. ‘Reach’ and ‘Effectiveness’ are individual-level measures representing the size and characteristics of the population participating in the program and highlighting whether the program impacts the health outcome. ‘Adoption’ is a measure at the organizational level that analyzes the uptake and acceptance of the program protocol among staff members, practices and settings, while ‘Implementation’ focuses on whether staff members deliver the program as intended. ‘Maintenance’ is measured at both the individual and organizational level and analyzes the extent to which the program is sustained over time [28].
Using both quantitative and qualitative methods, RE-AIM will help to evaluate the implementation of the CCiR model by the four organizations and determine its effectiveness in expanding access to addiction services, specifically MOUD in communities of color and high-risk individuals. It will also help to gain an understanding of whether buprenorphine can be successfully prescribed to the target population in a mobile setting.
Data collection challenges & processes
Data will include all individuals seeking medical or harm reduction care and each type of encounter is recorded differently. Data collection among people who use drugs and alcohol, who are often transient, and who can be skeptical of sharing personal information poses several challenges. To address this, MDPH-BSAS and evaluation staff conducted a preliminary interview of the programs implementing the CCiR model to capture their current data collection systems and best practices. Since priority for this vulnerable population is placed on building trust, developing rapport and providing ultra-low-barrier, evidence-based services that improve public health and save lives, staff would only be able to collect a limited amount of data on individuals utilizing harm reduction services. Thus, collecting variables such as sociodemographic data in a harm reduction encounter may inhibit utilization of services [29].
All encounters of clients seen for the more specific clinical care will result in generating a record in the agency Electronic Medical Record and will have those services recorded as usual in the agency Electronic Medical Record. CCiR programs will complete an intake form in a system maintained by MDPH-BSAS. This intake form includes demographic information such as gender, ethnicity, race, education, housing status, income and insurance type. No subsequent patient-level data will be collected during follow-up clinical visits for this evaluation project. MDPH will send deidentified data to the Brandeis evaluation team quarterly. No data from individuals served will be connected on an individual level to data provided by MDPH-BSAS.
Collectively, the data collection tools specifically developed for this project allow the Brandeis evaluation team to track the population accessing clinical and harm reduction services across the four programs. In addition, data specialists from the four programs will submit aggregate monthly metrics via an online survey tool developed specifically for this project by the Brandeis evaluation team. Data elements include hours of van operation, frequency of harm reduction services accessed, frequency of clinical services accessed, sexually transmitted infection tests administered, buprenorphine services provided, services most frequently requested and referrals to regular care in more traditional healthcare settings. Again, the evaluators kept the number of metrics to a minimum to maximize trust between care giver and this population. These metrics will be available to implementing programs, Kraft Center and MDPH-BSAS to see progress via a monthly ‘dashboard’ report, including the reach of both harm reduction and clinical services.
The online survey tool will also track the OUD treatment cascade of care. Programs will report on clients with new OUD diagnoses; the number that initiated medication; and the number that subsequently remained in treatment at 28, 60, 90 and 180 days. These metrics will be completed by the implementing programs every 6 months, starting in January 2023 to allow a full 180 day runout period for clients served in the first reporting period (i.e., January–June 2022).
Qualitative analysis
In addition to quantitative data, the evaluation will include qualitative data. Brandeis will conduct interviews with staff from each of the four programs. The interview protocol will follow the framework outlined in RE-AIM. The evaluators will inquire about how patients are referred in and out, how clinical and harm reduction activities are offered, barriers and facilitators to implementation of the model and perceived community reception. These questions will elucidate metrics such as fidelity to the model and community reception on both the intra-organizational level (e.g., “In what ways has the van influenced services provided by the parent organization?”) and an extra-organizational level (e.g., “How would you describe the communities’ response to your services?”).
Brandeis will also conduct a visit to each van as a non participant observer, to better understand the logistics and processes of treating people in a mobile van setting. In addition, the evaluators will attend monthly TA sessions where all four programs gather in a ‘learning collaborative’ environment. In TA sessions, program staff report their impressions and feedback regarding implementation issues at each site. For example, discussion at the TA sessions can inform the evaluators regarding difficulties in staffing issues, personal safety concerns and challenges arranging entry of study data. The evaluation team will record notes from these activities to use in qualitative data analysis.
The evaluation will use a thematic analysis approach to the data to highlight lessons learned, best practices, as well as information about staffing and community engagement. The overall qualitative analyses will help us to understand reasons for differences between the four programs, unexplained variables in the quantitative analysis, and any shifts in the implementation process.
Discussion
We have outlined here the protocol for an evaluation of a statewide effort to bring mobile addiction services to new patients in extremely vulnerable situations. Four programs across Massachusetts will provide both harm reduction services and clinical services utilizing the CCiR model. Those programs will submit demographic data to MDPH-BSAS at the individual level on an ongoing basis and aggregate benchmark data to the Brandeis evaluation team monthly. The programs will also submit aggregate data regarding initiations and retention on MOUD. Finally, the Brandeis team will collect qualitative data focused on evaluating processes and fidelity of implementation.
The importance of this evaluation is that while there have been mobile harm reduction services in operation for years [16], and more recently mobile MOUD services [16], we found only one study that evaluated a program that provided all these services via mobile vans beyond brick-and-mortar clinics [16]. It is possible that some programs are providing mobile MOUD and harm reduction services together, but to our knowledge the CCiR model is unique with its integration of treatment for various SUD, preventative and primary care and harm reduction services on mobile vans and in how it fosters partnership between clinicians and outreach staff [30]. Moreover, with opioid overdoses and overdose deaths increasing, it is more important than ever to understand the impact of mobile health services, particularly for those with the greatest barriers to care.
A randomized controlled trial (RCT) was not an option for this study, as it would be unethical to withhold MOUD, a successful and evidence-based intervention for OUD. Furthermore, an RCT was impractical given the length of time to reach the necessary number of patients (hard to reach), the homogeneity often associated with RCT participants, and the prohibitive cost. As a result, we opted for a mixed methods approach to strengthen our prospective, observational study design. We chose our key measures to be responsive to the funder’s priority areas of interest, for example, the extent to which the programs reach individuals who have yet to access any available state funded addiction services. Moreover, outcomes were narrowly targeted to bring needed sensitivity for the length of time it takes to build trust with people with such extreme levels of vulnerability, while at the same time leveraging existing data collected by the MDPH-BSAS.
Although this is an observational study with no comparison group, the evidence is so sparse for mobile addiction services delivered in this configuration, that this study represents a good first step, on which future research can build. Additionally, with the mixed methods approach we will have more insight into how a given intervention achieved its outcomes, rather than leaving this process as a ‘black box’.
Conclusion
Given the ongoing debate regarding investment in mobile SUD treatment [15], this study will help bring clarity around what benefits mobile services can and cannot deliver. Specifically, this evaluation will demonstrate the ability of mobile units to expand access to crucial addiction services (including MOUD) for people not traditionally engaged in care. It will determine if buprenorphine can be successfully prescribed in a mobile setting and how retention rates compare to published rates involving brick-and-mortar settings [31]. Finally, this study will provide new insight into how often patients can be connected to regular care in a more traditional healthcare setting.
Background & rationale
•
In 2020 there were an estimated 2106 deaths from opioid related overdose in Massachusetts, nearly six deaths per day.
•
Mobile health services like Community Care in Reach® (CCiR) are a portal of entry for individuals at highest risk for overdose death, many of whom are not currently engaged with traditional healthcare for myriad reasons including stigma, insurance issues, lack of transportation and competing comorbidities.
Design
•
In the CCiR model, harm reduction and clinical practitioners conduct outreach and provide addiction services including syringe exchange, naloxone distribution, medications for treating substance use disorder and primary care services from a mobile van.
•
The model has been replicated with state funding across four programs in Massachusetts with the goal to expand access to clinical and harm reduction services for people with addiction not currently engaged with care, particularly high-risk populations.
•
A mixed methods evaluation plan will demonstrate the model’s impact by analyzing data from standardized intake forms; collecting monthly aggregate outreach and clinical services data from programs; generating an opioid use disorder treatment cascade of care that captures the initiation and retention of patients in MOUD; and qualitative interviews and surveys across all four programs.
Outcome measures & evaluation
•
The RE-AIM framework is used to evaluate the implementation of the CCiR model across four programs to assess its effectiveness in meeting its goals.
•
Data elements for the online survey include hours of van operation, frequency of harm reduction services accessed, frequency of clinical services accessed, sexually transmitted infection tests administered, buprenorphine services provided, services most frequently requested and referrals to regular care in a traditional setting.
•
Outcome data will be collected on MOUD initiation and retention at 28, 60, 90 and 180 days.
•
Evaluators will conduct site visits and interviews with staff of each mobile van to inquire about implementation barriers, implementation facilitators and reception of the CCiR model, using a case study approach.
Discussion
•
While there have been mobile harm reduction services in operation for years, and more recently mobile MOUD services, we found only one study that evaluated a program that provided all these services via mobile vans beyond brick-and-mortar clinics.
•
The mixed methods evaluation will strengthen our prospective, observational study design.
Conclusion
•
The evaluation will demonstrate the ability of mobile units to expand access to crucial addiction services for people not previously engaged in care and communities of color, as well as compare retention rates in mobile versus traditional settings.
Author contributions
All authors (CA Tschampl, C Regis, NE Johnson, MT Davis, D Hodgkin, MF Brolin, E Do, CM Horgan, TC Green, B Reilly, MK Duska, EM Taveras) contributed to the conception and design, drafting and revising the manuscript, agreement to be accountable for all aspects of the work and ensuring integrity and accuracy, gave final approval of the manuscript to be published.
Acknowledgments
The authors thank all the staff at the four programs for their hard work and dedication.
Financial & competing interests disclosure
Funding was provided by the Massachusetts Department of Public Health (MDPH), Bureau of Substance Addiction Services (BSAS) RFQ file no. 215002240624. While the Kraft Center purchased three of the vans, and C Regis, NE Johnson, E Do and EM Taveras work or worked at the Kraft Center during the writing of this article, the evaluation is independently funded by the State of MA, USA. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The Massachusetts Department of Public Health Institutional Review Board has approved the protocol.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary infographic.png)
- Download
- 1.24 MB
{kind=link}
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Massachusetts Department of Public Health. Data brief: opioid-related overdose deaths among Massachusetts residents (2021). www.mass.gov/doc/opioid-related-overdose-deaths-among-ma-residents-november-2021/download
2.
Baumgartner JC, Radley DC, The Commonwealth Fund. Thespike in drug overdose deaths during the COVID-19 pandemic and policy options to move forward (2021). www.commonwealthfund.org/blog/2021/spike-drug-overdose-deaths-during-covid-19-pandemic-and-policy-options-move-forward
3.
Sordo L, Barrio G, Bravo MJ et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. Brit. Med. J. 357, j1550 (2017).
4.
Clark AK, Wilder CM, Winstanley EL. A systematic review of community opioid overdose prevention and naloxone distribution programs. J. Addict. Med. 8(3), 153–163 (2014).
5.
Vearrier L. The value of harm reduction for injection drug use: a clinical and public health ethics analysis. Dis. Mon. 65(5), 119–141 (2019).
6.
Shulman M, Wai JM, Nunes EV. Buprenorphine treatment for opioid use disorder: an overview. CNS Drugs 33(6), 567–580 (2019).
7.
Ross LE, Vigod S, Wishart J et al. Barriers and facilitators to primary care for people with mental health and/or substance use issues: a qualitative study. BMC Fam. Pract. 16(1), 135 (2015).
8.
Motavalli D, Taylor JL, Childs E et al. “Health Is on the Back Burner:” multilevel barriers and facilitators to primary care among people who inject drugs. J. Gen. Intern. Med. 36(1), 129–137 (2021).
9.
Williams AR, Nunes EV, Bisaga A, Levin FR, Olfson M. Development of a cascade of care for responding to the opioid epidemic. Am. J. Drug Alcohol Abuse 45(1), 1–10 (2019).
10.
Fine DR, Lewis E, Weinstock K, Wright J, Gaeta JM, Baggett TP. Office-based addiction treatment retention and mortality among people experiencing homelessness. JAMA Netw. Open 4(3), e210477 (2021).
• Aims to evaluate the retention and mortality in an office-based addiction treatment program setting for a population of homeless individuals with opioid use disorder.
11.
Yu SWY, Hill C, Ricks ML, Bennet J, Oriol NE. The scope and impact of mobile health clinics in the United States: a literature review. Int. J. Equity Health 16(1), 178 (2017).
• Reviews healthcare accessibility through Mobile Health Clinics and their use in reaching vulnerable populations by delivering curbside services.
12.
Stewart J, Stadeli KM, Ásbjörnsdóttir KH et al. Use of a community center primary care clinic and subsequent emergency department visits among unhoused women. JAMA Netw. Open 4(3), e213134 (2021).
13.
Rosecrans A, Harris R, Saxton RE et al. Mobile low-threshold buprenorphine integrated with infectious disease services. J. Subst. Abuse Treat. 133, 108553 (2022).
• This cohort analysis examines patient demographics, services provided and buprenorphine treatment retention for patients receiving care at the Spot mobile clinic, co-located with a Baltimore Syringe services program.
14.
Silberzahn BE, Tomko CA, Clouse E et al. The EMERALD (Enabling Mobilization, Empowerment, Risk Reduction, and Lasting Dignity) Study: protocol for the design, implementation, and evaluation of a community-based combination HIV prevention intervention for female sex workers in Baltimore, Maryland. JMIR Res. Protoc. 10(4), e23412 (2021).
• Examines the design, implementation and planned evaluation of a community led intervention to improve the HIV and STI incidence among female sex workers. The main components of the intervention included the SPARC (sex workers promoting action, risk reduction, and community mobilization), meant to provide low barrier harm reduction services and the mobile outreach component.
15.
Westfall JM, Nease DE, Zittleman L. Mobile van medication-assisted treatment for opioid use disorder is not enough (2022). www.healthaffairs.org/do/10.1377/forefront.20220222.646538
16.
Regis C, Gaeta JM, Mackin S, Baggett TP, Quinlan J, Taveras EM. Community care in reach: mobilizing harm reduction and addiction treatment services for vulnerable populations. Front. Public Health 8 (2020). https://www.frontiersin.org/article/10.3389/fpubh.2020.00501
•• Explores the Community Care in Reach mobile van, which addresses the prevalence of opioid overdoses in Greater Boston among vulnerable populations, and individuals experiencing homelessness. The Community Care in Reach Program provides harm reduction services, addiction treatment and primary care.
17.
Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2017 National Survey on Drug Use and Health (HHS Publication No. SMA 18-5068, NSDUH Series H-53). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, MD, USA (2018). www.samhsa.gov/data/
18.
Green TC, Park JN, Gilbert M et al. An assessment of the limits of detection, sensitivity and specificity of three devices for public health-based drug checking of fentanyl in street-acquired samples. Int. J. Drug Policy 77, 102661 (2020).
19.
Glick JL, Christensen T, Park JN, McKenzie M, Green TC, Sherman SG. Stakeholder perspectives on implementing fentanyl drug checking: results from a multi-site study. Drug Alcohol Depend. 194, 527–532 (2019).
20.
Sherman SG, Morales KB, Park JN, McKenzie M, Marshall BDL, Green TC. Acceptability of implementing community-based drug checking services for people who use drugs in three United States cities: Baltimore, Boston and Providence. Int. J. Drug Policy 68, 46–53 (2019).
21.
Rudolph L, Maizlish N, North S, Dervin K. A public health learning collaborative on climate change for Urban Health Departments, 2016–2018. Public Health Rep. 135(2), 189–201 (2020).
22.
Weinberger A, Stegmann K, Fischer F. Knowledge convergence in collaborative learning: concepts and assessment. Learn. Instr. 17(4), 416–426 (2007).
23.
Keck C, Hartley DM, Havens M, Margolis PA, Seid M. Getting what is needed, when it's needed: sharing information, knowledge, and know-how in a Collaborative Learning Health System. Learn. Health Syst. 5(3), e10268 (2021).
24.
Nicholson J, English K, Heyman M. The Parenting Well Learning Collaborative Feasibility Study: training adult mental health service practitioners in a family-focused practice approach. Community Ment. Health J. 58(2), 261–276 (2022).
25.
Cannon-Bowers JA, Salas E. Reflections on shared cognition. J. Organ Behav. 22(2), 195–202 (2001).
26.
Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am. J. Public Health 89(9), 1322–1327 (1999).
27.
Shelton RC, Chambers DA, Glasgow RE. An extension of RE-AIM to enhance sustainability: addressing dynamic context and promoting health equity over time. Front. Public Health 8, 134 (2020).
28.
Glasgow RE, Estabrooks PE. Pragmatic applications of RE-AIM for health care initiatives in community and clinical settings. Prev. Chronic. Dis. 15, E02 (2018).
•• Aims to examine the use of the RE-AIM model to evaluate public health interventions that aim to assess reach, efficacy, adoption, implementation and maintenance.
29.
Simon C, Brothers S, Strichartz K et al. We are the researched, the researchers, and the discounted: the experiences of drug user activists as researchers. Int. J. Drug Policy 98, 103364 (2021).
30.
Greater Lawrence Family Health Center. Health care on the road the importance of GLFHC's new Mobile Health Unit. InPulse 1(7), 8 (2017).
31.
Mirer AG, Tiemstra JD, Hammes NE, Cloum HM, LaFavor KJ. Integrating buprenorphine treatment for opioid use with primary care is associated with greater retention in treatment. J. Am. Board Fam. Med. 35(1), 206–208 (2022).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 27 June 2022
Accepted: 13 February 2023
Published online: 29 March 2023
Keywords:
Topics
Authors
Funding Information
Massachusetts Department of Public Health (MDPH), Bureau of Substance Addiction Services (BSAS): Grant Number (RFQ File Number): 215002240624
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Protocol for the implementation of a statewide mobile addiction program. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0117
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Cynthia A. Tschampl, Jennifer J. Wicks, Dominic Hodgkin, Craig Regis, Jadyn Baptista, Brittany P. Chapman, Madeline E. Davies, Kimberly De La Cruz, Karen Peugh, Allyson Pinkhover, Ben Plant, Priya Sarin Gupta, Sarah Mackin, Catherine E. Urquhart, Samantha Walsh, Jessie M. Gaeta, Constance Horgan, Elsie M. Taveras, Multisite Mobile Addiction Services: Four-Year Outcomes, International Journal of Environmental Research and Public Health, 10.3390/ijerph23060756, 23, 6, (756), (2026).
- Elisa Pujals, Glorimar Caraballo-Correa, Kathia Ocasio Maldonado, Yelanesse Pastrana Gonzalez, Rafael A. Torruella, Luis Román Badenas, Bridging Gaps in Care: Evaluation of a Mobile Health Model Addressing Social Determinants and Harm Reduction in Eastern Puerto Rico, International Journal of Environmental Research and Public Health, 10.3390/ijerph23040529, 23, 4, (529), (2026).
- John M Westfall, Linda Zittleman, Camille Hochheimer, David Wolff, Doug Fernald, Ben Sofie, Cory Lutgen, L Miriam Dickinson, Donald E Nease, undefined the HOMER Patient and Clinician Advisory Council, Primary care provides medication for opioid use disorder: findings from the HOMER study, Health Affairs Scholar, 10.1093/haschl/qxaf253, 4, 1, (2026).
- Irving Barrera, Grace Wang, Brammy Rajakumar, Siva Muthupalaniappan, Alexandria E. Cronin, Avik Chatterjee, Mobile addiction treatment units: a narrative review, Addiction Science & Clinical Practice, 10.1186/s13722-025-00619-1, 20, 1, (2025).
- John P. Broach, Brian Rettger, Ronald Gigliotti, Brittany P. Chapman, Jillian Joseph, Abbey Smiley, Michael Hunter, Norman Soucie, Karen Gross, Kavita M. Babu, Stacy N. Weisberg, Creating Opioid Response Specialists: A Harm Reduction Initiative, Prehospital Emergency Care, 10.1080/10903127.2025.2473682, 29, 4, (540-545), (2025).
- Jillian J Weber, Rebecca L Kinney, Jill S Roncarati, Kenneth Bruemmer, Monica Diaz, Jill Albanese, A National Mobile Medical Unit (MMU) Program to Address the Healthcare Needs of Veterans Experiencing Homelessness: An Evaluation Protocol, Health Services Insights, 10.1177/11786329251320200, 18, (2025).
- Allyson Kelley, Kellie Webb, Katherine Hirchak, Morgan Witzel, Kelsey Bajet, Sadie Posey, Tribally-led mobile outreach: improving access to harm reduction services in one rural reservation community, Frontiers in Public Health, 10.3389/fpubh.2024.1383729, 12, (2024).
- Michael D. Pepin, Jillian K. Joseph, Brittany P. Chapman, Christina McAuliffe, Logan K. O’Donnell, Ryan L. Marano, Stephanie P. Carreiro, Erik J. Garcia, Hugh Silk, Kavita M. Babu, A mobile addiction service for community-based overdose prevention, Frontiers in Public Health, 10.3389/fpubh.2023.1154813, 11, (2023).