Indirect treatment comparison of lurbinectedin versus other second-line treatments for small-cell lung cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Compare lurbinectedin versus other second-line (2L) small-cell lung cancer (SCLC) treatments. Methods: An unanchored matching-adjusted indirect comparison connected the platinum-sensitive SCLC cohort of a single-arm lurbinectedin trial to a network of three randomized controlled trials (oral and intravenous [IV] topotecan, and platinum re-challenge) identified by systematic literature review. Network meta-analysis methods estimated relative treatment effects. Results: In platinum-sensitive patients, lurbinectedin demonstrated a survival benefit and favorable safety profile versus oral and IV topotecan and platinum re-challenge (overall survival, hazard ratio [HR]: 0.43; 95% credible interval [CrI]: 0.27, 0.67; HR: 0.43; 95% CrI: 0.26, 0.70; HR: 0.42; 95% CrI: 0.30, 0.58 respectively). Conclusion: Lurbinectedin showed a robust survival benefit and favorable safety versus other SCLC treatments in 2L platinum-sensitive SCLC.
Tweetable abstract
Indirect treatment comparison analysis demonstrates robust survival benefit and safety profile for lurbinectedin monotherapy versus relevant comparators (oral and intravenous topotecan; platinum re-challenge) as second-line therapy for platinum-sensitive small-cell lung cancer
Small-cell lung cancer (SCLC) is a transcription-addicted disease that accounts for 10 to 15% of lung cancer cases [1–5]. At the time of diagnosis, nearly 70% of patients had extensive-stage disease (ES), which is defined as the presence of overt metastatic disease by imaging or physical examination (i.e., American Joint Committee on Cancer [AJCC] stage IV) [3,6,7]. The remainder of patients are classified as having limited-stage disease (LS) in which tumors are limited to the chest (i.e., AJCC stage I–III) [3,8–10]. However, regardless of the stage at diagnosis, treatment is rarely curative and SCLC is associated with poor long-term survival (5-year survival is <10%) [5].
Unlike non-SCLC, the oncogenic drivers in SCLC are relatively unexplored [11], which can make managing treatment strategy and the prognosis of patients with SCLC challenging [12]. Further, there are no approved targeted therapies for oncogenic drivers in SCLC [11,13,14]. Based on the current National Cancer Comprehensive Network (NCCN) guidelines, the recommended first-line (1L) treatment for patients with LS-SCLC is platinum-based chemotherapy (cisplatin or carboplatin + etoposide) with concomitant thoracic radiotherapy. The preferred treatment for ES-SCLC is platinum-based chemotherapy with programmed death ligand targeted immune checkpoint inhibitors, either atezolizumab or durvalumab, plus platinum plus etoposide [3]. While the initial response to 1L therapies is high, up to 80% of patients with LS-SCLC and nearly all patients with ES-SCLC relapse eventually, usually within the first year after treatment [6,15].
Choice of subsequent treatment after relapse is often guided by platinum sensitivity, with platinum-resistant disease most often defined as a chemotherapy-free interval (CTFI) of ≤90 days and platinum-sensitive as ≥90 days per the European Society for Medical Oncology (ESMO) guidelines [3,8,16]. Patients with platinum-sensitive disease are more likely to have a favorable response to second-line (2L) treatment than patients with platinum-resistant disease [17]. The NCCN guidelines for 2L treatment and beyond recommend topotecan, lurbinectedin, irinotecan, paclitaxel, docetaxel, temozolomide, pembrolizumab, vinorelbine, oral etoposide, gemcitabine, cyclophosphamide + doxorubicin + vincristine (CAV), bendamustine, or nivolumab [3].
Lurbinectedin (Zepzelca™) is a selective inhibitor of oncogenic transcription that induces immunogenic cell death, and preclinical evidence suggests it may also affect the tumor microenvironment [18]. Lurbinectedin received accelerated approval from the US Food and Drug Administration in June 2020 as a monotherapy (3.2 mg/m2 intravenous [IV] every 21 days) for adults with metastatic SCLC that has progressed on or after platinum-based chemotherapy [19,20]. This approval was based on the investigator-assessed overall response rate (ORR: 35.2%) and the duration of response (DOR: 5.3 months) observed in 105 platinum-sensitive or platinum-resistant patients with SCLC in a phase II open-label, single-arm basket trial (Study B-005: NCT02454972) of lurbinectedin monotherapy (3.2 mg/m2 IV every 21 days) [19–21].
As the phase II basket trial was a single-arm trial, the comparative efficacy and safety of lurbinectedin monotherapy in SCLC versus other 2L treatments could not be directly ascertained. Therefore, the aim of this analysis was to estimate the relative treatment effects of lurbinectedin versus relevant comparators for the treatment of SCLC that has progressed on or after platinum-based chemotherapy in terms of efficacy and safety by means of indirect comparisons of the results of the 2L lurbinectedin SCLC cohort within the phase II basket trial and published clinical trials.
Methods
Systematic literature review
A systematic literature review (SLR) was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to identify relevant clinical trials for competing interventions [22].
Studies were selected based on predefined eligibility criteria in terms of population, interventions, comparators, outcomes, and study design, and included randomized controlled trials (RCTs), non-randomized comparative trials, and single-arm trials featuring FDA-approved or NCCN-recommended therapies [3,23] for the treatment of adults with SCLC who had disease progression on or after one previous line of platinum-based chemotherapy (Supplementary Table 1). Only relevant treatment arms from RCTs were included, and non-randomized trials or single-arm trials were included only when RCTs were unavailable for an intervention of interest. Relevant trials were required to evaluate at least one efficacy outcome, including overall survival (OS), progression-free survival (PFS)/time to progression (TTP), ORR or DOR.
Database searches were conducted on 6 January 2021, using predefined searches in the Ovid platform for Excerpta Medica database (EMBASE), Medical Literature Analyses and Retrieval System Online (MEDLINE), and Cochrane Central Register of Controlled Trials (CENTRAL) (Supplementary Tables 2– 4). The following conference proceedings were also searched from 2019 to 2021: American Association for Cancer Research Annual Meeting (AACR), American Society of Clinical Oncology Annual Meeting (ASCO), and the International Association for the Study of Lung Cancer World Conference on Lung Cancer (IASLC WCLC). In addition, the US National Institutes of Health Clinical Trial Registry (clinicaltrials.gov) was searched to identify eligible trials that had not yet been published but reported results, and hand searches were performed of the bibliographies of recently published relevant systematic reviews and meta-analyses.
Study screening and data extraction were performed by two independent reviewers. Discrepancies were reconciled with involvement of a third reviewer. For all included trials, relevant patient, treatment, and study characteristics as well as outcomes of interest were extracted.
Statistical analyses
We used a statistical approach based on network meta-analysis (NMA) techniques to estimate the relative treatment effects of lurbinectedin versus key comparators of interest (i.e., carboplatin + etoposide re-challenge [from here on referred to as platinum re-challenge] and topotecan) for the following outcomes of interest – ORR, OS, PFS/TTP, hematological adverse events (AEs; grade 3/4 anemia, grade 3/4 thrombocytopenia, and grade 3/4 neutropenia). PFS was defined as the time from randomization to disease progression or death, while TTP was defined as the time from randomization to disease progression only. Safety analyses focused on hematological toxicity given that all FDA-approved 2L treatments for SCLC carry a risk of these AEs.
Since the basket trial of lurbinectedin was a single-arm trial, a standard NMA based on only RCTs could not be performed. We used a modified two-step approach that consisted of an unanchored matching-adjusted indirect comparison (MAIC) to obtain estimates of the relative treatment effect of lurbinectedin versus an alternative intervention in the network of RCTs [24] followed by an NMA based on this MAIC estimate and the RCTs for the other competing interventions.
To perform the unanchored MAIC, the RCT of a competing intervention that best matched the phase II basket trial needed to be identified. Propensity score-based weights for the basket trial were generated using its individual patient data (IPD) to match the basket trial population to each of the relevant RCTs. Since IPD were not available for the comparator trials, matching was based on aggregate study-level data for the RCTs. As the study designs and eligibility criteria of these RCTs were similar, selection of the best matching trial was based on the ability to match to the distributions of available baseline patient characteristics in the published trials, i.e., age, sex, Eastern Cooperative Oncology Group (ECOG) Performance Status, disease stage, and platinum sensitivity. The best matching trial was determined by the extent of similarity or overlap with the basket trial; an external trial resulting in a smaller change in absolute standardized differences across matching variables [25,26] and a larger effective sample size (ESS) was considered to be more similar to the basket trial. Given heterogeneity in the proportion of patients with platinum-sensitive or -resistant disease across the trials in the network, multiple sets of analyses were performed. The base case analysis focused on the platinum-sensitive (CTFI ≥90 days) subgroup of patients from the basket trial, and the external trial considered to be most similar to the basket trial was used in the MAIC. Sensitivity analysis no. 1, no. 2, and no. 3 were performed using a different external trial from the one used in the base case analysis to connect the basket trial to the network. Sensitivity analysis no. 1 focused on the basket trial's full population (including platinum sensitivity as a covariate in the MAIC model) whereas sensitivity analysis no. 2 focused on the basket trial's platinum-sensitive subgroup. In sensitivity analysis no. 3, an additional RCT which included a sicker population (patients considered unsuitable for IV chemotherapy due to comorbidities or refusal on the basis of risk of toxicity) was added to the network of RCTs, focusing on the basket trial's full population.
By connecting the basket trial to an external RCT via MAIC, the basket trial entered the network of RCTs as if it was a third arm of the external trial. The NMA for the different outcomes of interest was performed in a Bayesian framework as outlined by Dias et al. [27,28]. Since the evidence base was too limited to estimate between-trial heterogeneity for random-effects models, only fixed-effects models were used. Normal non-informative prior distributions with a mean of 0 and a variance of 10,000 were used for the nuisance and relative treatment effect parameters of the models.
For survival outcomes, the proportional hazard (PH) assumptions were tested using the Grambsch–Therneau test [29]. For OS, the PH assumption was not violated in any of the trials and the NMA of OS was performed based on constant hazard ratios (HRs). For PFS and TTP, the PH assumption was violated in some trials and a fractional polynomial NMA was performed to obtain time-varying HRs between the competing interventions [30–32]. Given differences in the PFS and TTP definitions across studies, the base-case analysis focused on PFS, which was reported in the basket trial; however, a sensitivity analysis was also performed including both PFS and TTP, assuming that relative treatment effects regarding both outcomes were comparable.
All analyses were performed using R version 4.0.3 (www.r-project.org/), JAGS version 4.2.0, and OpenBUGS version 3.2.3.
Results
Evidence base
A total of 20 citations [21,33–50] representing ten unique trials were included in the SLR (Figure 1): five RCTs (Baize et al. [33], O'Brien et al. [34], Eckardt et al. [35], von Pawel et al. [36], United Therapeutics [37]), two RCTs with only one arm of interest (Owonikoko et al. [38], CheckMate 331 [39]), two single-arm trials (phase II lurbinectedin basket trial [Trigo] [21] and Smyth [40]), and one study that included a randomized cohort and a non-randomized cohort with only one arm of interest (CheckMate 032) [41,42]. To align with the interventions of interest in Supplementary Table 1, the following treatment arms were not considered relevant: United Therapeutics 2017 (dinutuximab + irinotecan) [37], Owonikoko 2020 (alisertib + paclitaxel) [38], CheckMate 032 (nivolumab + ipilimumab) [41,42], and CheckMate 331 (investigator's choice of topotecan or amrubicin) [39]. In CheckMate 331, amrubicin was not of interest, the proportion of patients who received each treatment was not provided, and outcomes were not stratified by treatment.
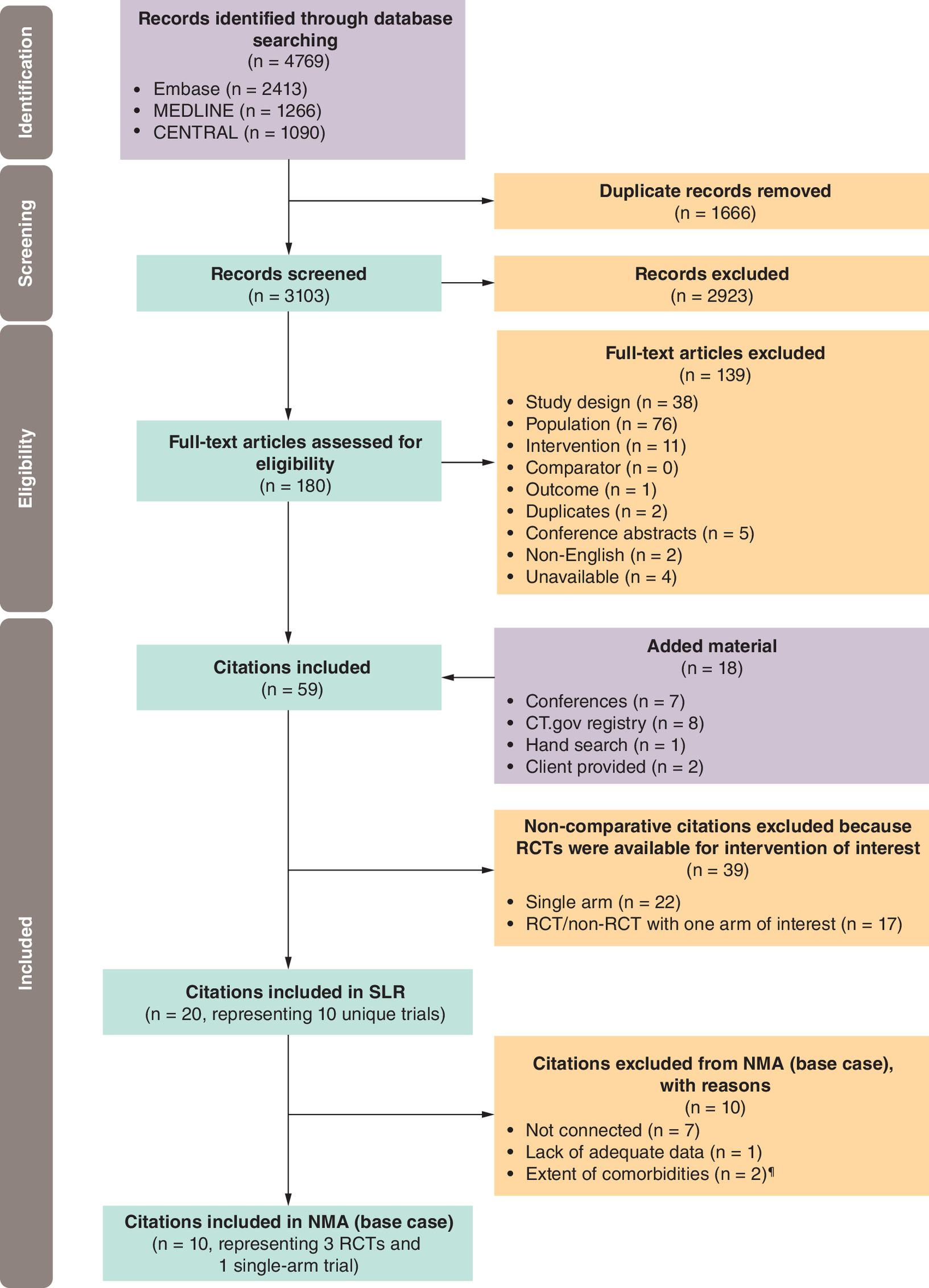
Figure 1. Study selection flow diagram based on Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Detailed descriptions of the study, patient characteristics, and study designs of the included trials are provided in Table 1 and the supplementary materials (Supplementary Figure 1). Three trials enrolled patients with sensitive disease, defined as those who had disease relapse or progression at least 90 days after completion of 1L chemotherapy treatment (CTFI ≥90 days) [33,35,36]. Six trials enrolled a broader population comprised of patients with sensitive and resistant disease (defined as those who had disease relapse or progression within 90 days after completion of 1L chemotherapy treatment; i.e., CTFI <90 days) [21,34,38], and one study did not specify patients' response to 1L treatment [40].
| Trial | Line | Study eligibility criteria | Study design | Treatment | Analyses population | n | ECOG PS, n (%) | Disease stage, n (%) | Response to 1L | Ref. | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | LS | ES | Resistant | Sensitive | |||||||||
| RCTS | |||||||||||||||
| Baize (n = 164) | 2L | Relapse ≥90 days following platinum-based 1L therapy | RCT phase III, open-label | Topotecan (oral) | ITT, CTFI ≥90 d | 81 | 26 (32.1) | 48 (59.3) | 7 (8.6) | 30 (37.0) | 51 (63.0) | 0 (0.0) | 81 (100) | [33] | |
| Platinum re-challenge (IV) | ITT, CTFI ≥90 d | 81 | 28 (34.6) | 48 (59.3) | 5 (6.2) | 29 (35.8) | 52 (64.2) | 0 (0.0) | 81 (100) | ||||||
| O'Brien (n = 141) | 2L | Progression after 1L therapy and unsuitable for IV chemotherapy. | RCT phase III, open-label | BSC | ITT | 70 | 6 (8.6) | 41 (58.6) | 23 (32.9) | 27 (38.6) | 43 (61.4) | 35 (50.0) | 35 (50.0) | [34] | |
| Topotecan (oral)/BSC | ITT | 71 | 8 (11.3) | 44 (62.0) | 19 (26.8) | 23 (32.4) | 48 (67.6) | 41 (57.7) | 30 (42.3) | ||||||
| Eckardt (n = 309) | 2L | Disease recurrence ≥90 days following 1L chemotherapy | RCT phase III, open-label | Topotecan (oral) | ITT, CTFI ≥90 d† | 153 | 48 (31.4) | 85 (55.6) | 20 (13.1) | 51 (33.3) | 102 (67.7) | 15‡ (9.5) | 134‡ (87.6) | [35] | |
| Topotecan (IV) | ITT, CTFI ≥90 d† | 151 | 35 (23.2) | 98 (64.9) | 18 (11.9) | 45 (29.8) | 106 (70.2) | 13‡ (8.6) | 137‡ (90.7) | ||||||
| von Pawel (n = 106) | 2L | Relapse ≥90 days following 1L chemotherapy | RCT phase II, open-label | Topotecan (oral) | ITT, CTFI ≥90 d§ | 52 | 10¶ (19.2) | 34¶ (65.4) | 8¶ (15.4) | 14‡ (26.9) | 37‡ (71.2) | 1 (1.9) | 51 (98.1) | [36] | |
| Topotecan (IV) | ITT, CTFI ≥90 d§ | 54 | 18¶ (33.3) | 21¶ (38.9) | 15¶ (27.8) | 14‡ (25.9) | 39‡ (72.2) | 1 (1.8) | 53 (98.1) | ||||||
| United Therapeutics (n = 483) | 2L | Progression after 1L treatment with platinum-based chemotherapy | RCT phase II/III, open-label | Irinotecan (IV) | ITT | 190 | 40 (21.1) | 150 (78.9) | 0 (0.0) | NR | NR | NR | NR | [37] | |
| Topotecan (IV) | ITT | 94 | 19 (20.2) | 75 (79.8) | 0 (0.0) | NR | NR | NR | NR | ||||||
| RCTs with only one arm of interest | |||||||||||||||
| Owonikoko (n = 178) | 2L | Progression after at least 180 days following 1L platinum-based chemotherapy | RCT phase II, double-blind | Paclitaxel (IV) | ITT | 89 | 18 (20.2) | 71 (79.8) | 0 (0.0) | 8‡ (9.0) | 62‡ (69.7) | 33‡,# (37.1) | 35‡,# (39.3) | [38] | |
| CheckMate 331 (n = 569) | 2L | Recurrence or progression following 1L platinum-based chemotherapy | RCT phase III, open-label | Nivolumab (IV) | ITT | 284 | 75 (26.4) | 209 (73.6) | 0 (0.0) | 74 (26.1) | 210 (73.9) | 121 (42.6) | 163 (57.4) | [39] | |
| Non-RCTs/RCTs with only one arm of interest | |||||||||||||||
| CheckMate 032‡‡ | Antonia 2016 (non-RCT) (n = 216) | 2L+ | Progression after 1L treatment with platinum-based chemotherapy | Non-RCT phase I/II, open-label | Nivolumab (IV) | Overall | 98†† | NR | NR | NR | NR | NR | 30‡ (30.6) | 55‡ (56.1) | [41] |
| Ready 2020 (RCT) (n = 243) | 2L+ | Progression after 1L treatment with platinum-based chemotherapy | RCT phase I/II, open-label | Nivolumab (IV) | ITT | 147†† | 49 (33.3) | 98 (66.7) | NR | NR | NR | 73‡ (49.7) | 73‡ (49.7) | [42] | |
| Single-arm trials | |||||||||||||||
| Basket trial (n = 105) | 2L | Progression after 1L treatment with platinum-based chemotherapy | Single-arm phase II | Lurbinectedin (IV) | Overall | 105 | 38 (36.2) | 59 (56.2) | 8 (7.6) | 32 (30.5) | 73 (69.5) | 45 (42.9) | 60 (57.1) | [21] | |
| Smyth (n = 34) | 1L+ | Evidence of progressive disease following 1L chemotherapy | Single-arm phase II | Docetaxel (IV) | Overall | 34 | 8¶ (23.5) | 22¶ (64.7) | 4¶ (11.8) | 0 (0) | 34 (100) | NR | NR | [40] | |
†
Approximately 10% of patients in both treatment groups had a CTFI <90 days at study entry.
‡
Missing patient data were reported.
§
Approximately 2% of patients in both treatment groups had a CTFI <90 days at study entry.
¶
WHO PS.
#
Platinum refractory, 16 (19%).
††
Mixed population, baseline characteristics for the 2L population not provided.
‡‡
Three patients in the nivolumab 3 mg/kg group did not receive 1L platinum therapy and did not meet eligibility criteria, although they were treated and included in the analysis.
1L+: First line and beyond; 2L: Second line; 2L+: Second line and beyond; BSC: Best supportive care; CTFI: Chemotherapy-free interval; ECOG: Eastern cooperative oncology group; ES: Extensive stage; ITT: Intention to treat; IV: Intravenous; LS: Limited stage; NR: Not reported; PS, Performance Status; RCT: Randomized Clinical Trial; WHO: World Health Organization.
Five RCTs (Baize [33], O'Brien [34], Eckardt [35], von Pawel [36], United Therapeutics [37]) had interventions in common such that a connected network of RCTs could be created for an NMA. However, at the time of the analysis, United Therapeutics 2017 did not provide information on the proportion of patients with platinum-sensitive or -resistant disease, and was therefore excluded from the network [37]. O'Brien [34] compared oral topotecan with best supportive care (BSC) and was the only trial in the connected network that recruited patients who were considered unsuitable for IV chemotherapy due to comorbidities or refusal on the basis of risk of toxicity. As a result, O'Brien [34] was only included in sensitivity analysis no. 3 for OS. Thus, three RCTs which compared platinum re-challenge versus oral topotecan (Baize [33]) or oral topotecan versus IV topotecan (Eckardt [35] and von Pawel [36]) were included in the connected network. There were no meaningful differences between the phase II basket trial and the three network studies with regard to study design and treatment characteristics. There were, however, differences in the patient population. The phase II basket trial enrolled patients with both platinum-sensitive and -resistant disease, while the three RCTs (Baize [33], Eckardt [35], and von Pawel [36]) were designed to enroll only platinum-sensitive patients; however, 10% of patients in Eckardt 2007 and 2% of patients in von Pawel had platinum-resistant disease [35,36].
Based on outcome availability across the four trials, ORR, OS, and PFS/TTP analyses were feasible for patients with platinum-sensitive disease and for patients with any platinum sensitivity; however, due to limitations in data availability, analyses were not feasible for the subset of patients with resistant disease (Table 2). Safety analyses were feasible for grade 3/4 anemia, grade 3/4 thrombocytopenia, and grade 3/4 neutropenia in patients with platinum-sensitive disease and any platinum sensitivity (Table 3).
| Trial ID, year | Treatment | Analyses population | n | CTFI ≥90 d, n (%) | ORR, % | Median OS, months (95% CI) | Median PFS, months (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | CTFI ≥90 d | Overall | CTFI ≥90 d | Overall | CTFI ≥90 d | ||||||
| RCTs | |||||||||||
| Baize, 2020 | Topotecan (oral) | ITT, CTFI ≥90 d | 81 | 81 (100.0) | 25.3†,‡ | 7.4 (6.0, 8.7) | 2.7† (90% CI 2.3, 3.2) | ||||
| Platinum re-challenge (IV) | ITT, CTFI ≥90 d | 81 | 81 (100.0) | 49.4†,‡ | 7.5 (5.4, 9.5) | 4.7† (90% CI 3.9, 5.5) | |||||
| O'Brien, 2006 | Topotecan (oral) + BSC | ITT | 71 | 30 (42.3) | 7.0† | 3.0† | 6.0 (4.2, 7.3) | NR | TTP: 3.8† (3.0, 4.6) | NR | |
| BSC | ITT | 70 | 35 (50.0) | NR | NR | 3.2 (2.6, 4.3) | NR | NR | NR | ||
| Eckardt, 2007 | Topotecan (oral) | ITT, CTFI ≥90 d†† | 153 | 134 (87.6) | 18.3§ | 7.6¶ (6.7, 9.8) | TTP: 2.7§,¶ (2.2, 3.2) | ||||
| Topotecan (IV) | ITT, CTFI ≥90 d†† | 151 | 137 (90.7) | 21.9§ | 8.1¶ (7.1, 8.6) | TTP: 3.4§,¶ (3.1, 4.3) | |||||
| von Pawel, 2001 | Topotecan (oral) | ITT, CTFI ≥90 d‡‡ | 52 | 51 (98.1) | 23.1§ | 7.4¶ (range: 0.1, 15.9) | TTP: 3.4§,¶ (range: 0.1, 15.9) | ||||
| Topotecan (IV) | ITT, CTFI ≥90 d‡‡ | 54 | 53 (98.1) | 14.8§ | 5.8¶ (range: 0.1, 15.0) | TTP: 3.0§,¶ (range: 0.1, 15.0) | |||||
| United Therapeutics, 2017 | Irinotecan | ITT | 190 | NR | 18.9 | NR | 7.0 (5.6, 8.9) | NR | 3.0 (2.7, 4.2) | NR | |
| Topotecan (IV) | ITT | 94 | NR | 20.2 | NR | 7.4 (6.1, 9.3) | NR | 3.4 (2.8, 4.2) | NR | ||
| RCT with only one arm of interest | |||||||||||
| Owonikoko, 2020 | Paclitaxel + placebo | ITT#, CTFI <180 d | 89 | 35 (39.3) | 18.0§ | NR | 5.42 | NR | 2.17§ | 3.34§ | |
| CheckMate 331 | Nivolumab | ITT | 284 | 163 (57.4) | 13.7† | NR | 7.5 (5.6, 9.2) | 7.6 (5.6, 11.2) | 1.4† (1.4, 1.5) | NR | |
| RCT/non-RCT with only one arm of interest | |||||||||||
| CheckMate 032 | Antonia 2016 (Non-RCT) | Nivolumab | Subgroup, 2L | 40¶¶ | NR | 10.0† | NR | NR | NR | NR | NR |
| Ready 2019 (RCT) | Nivolumab | Subgroup, 2L | NR | NR | NR | NR | 6.0 (3.8, 9.4) | NR | NR | NR | |
| Single-arm trials | |||||||||||
| Basket trial | Lurbinectedin | Overall | 105 | 60 (57.1) | 35.2† | 45.0† | 9.3 (6.3, 11.8) | 11.9 (9.7, 16.2) | 3.5† (2.6, 4.3) | 4.6† (2.8, 6.5) | |
| Smyth, 1994 | Docetaxel | Subgroup, 2L | 22§§ | NR | 18.0 | NR | NR | NR | NR | NR | |
†
Investigator assessed.
‡
Non-evaluable patients were excluded from analyses (n = 6 the in topotecan arm, n = 2 in the platinum re-challenge arm).
§
Independent review committee assessed.
¶
Median was reported in weeks in publications.
#
Protocol Amendment 2 (January 2015) corrected the stratification definition for time to relapse to follow standard guidance by counting from the date of the last dose of frontline chemotherapy as opposed to counting from initial response to first-line platinum-based chemotherapy, as originally set out in the protocol.
††
Approximately 10% of patients in both treatment groups had a CTFI <90 days at study entry.
‡‡
Approximately 2% of patients in both treatment groups had a CTFI <90 days at study entry.
§§
A total of 28 patients were evaluable; of these, 22 were second-line patients.
¶¶
3% of patients had missing data.
2L: Second line; BSC: Best supportive care; CI: Confidence interval; CTFI: Chemotherapy-free interval; ITT: Intention to treat; IV: Intravenous; NR: Not reported; ORR: Overall response rate; OS: Overall survival; PFS, Progression-free survival; RCT: Randomized controlled trial; TTP: Time to progression.
| Trial ID, year | Treatment | Analyses population | n | Anemia, n (%) | Thrombocytopenia, n (%) | Neutropenia, n (%) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Any grade | Grade 3/4 | Any grade | Grade 3/4 | Any grade | Grade 3/4 | |||||
| RCTs | ||||||||||
| Baize, 2020 | Topotecan (oral) | ITT, CTFI ≥90 days | 81 | NR | 17 (21.0) | NR | 29 (36.0) | NR | 18 (22.0) | |
| Platinum re-challenge (IV) | ITT, CTFI ≥90 days | 81 | NR | 20 (25.0) | NR | 25 (31.0) | NR | 11 (14.0) | ||
| O'Brien, 2006 | BSC | ITT | 67 | NR | NR | NR | NR | NR | NR | |
| Topotecan (oral) + BSC | ITT | 70 | NR | (25.0) | NR | (38.0) | NR | (61.0) | ||
| Eckardt, 2007 | Topotecan (oral) | ITT, CTFI ≥90 days# | 153 | NR | 34 (22.2) | NR | 73 (47.7) | NR | 109 (71.2) | |
| Topotecan (IV) | ITT, CTFI ≥90 days# | 151 | NR | 46 (30.5) | NR | 65 (43.0) | NR | 130 (86.1) | ||
| von Pawel, 2001 | Topotecan (oral) | ITT, CTFI ≥90 days†† | 52 | NR | (31.4)† | NR | (53.0)† | NR | (56.9)† | |
| Topotecan (IV) | ITT, CTFI ≥90 days†† | 54 | NR | (30.2)‡ | NR | (49.0)‡ | NR | (94.2)‡ | ||
| United Therapeutics, 2017 | Irinotecan (IV) | ITT | 187 | 55 (29.4) | NR | 13 (6.95) | NR | 47 (25.1) | NR | |
| Topotecan (IV) | ITT | 88 | 58 (65.9) | NR | 22 (25.0) | NR | 45 (51.1) | NR | ||
| RCT with only one arm of interest | ||||||||||
| Owonikoko, 2020 | Paclitaxel + Placebo (IV) | ITT, CTFI <180 days§ | 89 | 14 (16.0) | 1 (1.0)¶ | NR | NR | 7 (8.0) | 5 (6.0)¶ | |
| CheckMate, 331 | Nivolumab (IV) | ITT | 282 | 13 (4.6) | 0 (0.0) | 5 (1.8) | 0 (0.0) | 4 (1.4) | 1 (0.4) | |
| RCT/non-RCT with only one arm of interest | ||||||||||
| CheckMate 032 | Antonia 2016 (Non-RCT) | Nivolumab | Subgroup, 2L | 40 | NR | NR | NR | NR | NR | NR |
| Ready 2019 (RCT) | Nivolumab | Subgroup, 2L | NR | NR | NR | NR | NR | NR | NR | |
| Single-arm trials | ||||||||||
| Basket trial | Lurbinectedin (IV) | Treated population | 105 | 100 (95.2) | 9 (8.6) | 46 (43.8) | 7 (6.7) | 75 (71.4) | 48 (45.7) | |
| Smyth, 1994 | Docetaxel | Subgroup, 2L | 22 | NR | NR | NR | NR | NR | NR | |
Either treatment-related or any hematological AEs were extracted.
†
Grade 3 anemia, 27.5%; grade 4 anemia, 3.9%; grade 3 thrombocytopenia, 25.5%; grade 4 thrombocytopenia, 27.5%; grade 3 leukopenia, 27.5%; grade 4 leukopenia, 17.6%; grade 3 neutropenia, 21.6%; grade 4 neutropenia, 35.3%.
‡
Grade 3 anemia, 26.4%; grade 4 anemia, 3.8%; grade 3 thrombocytopenia, 24.5%; grade 4 thrombocytopenia, 24.5%; grade 3 neutropenia, 26.9%; grade 4 neutropenia, 67.3%.
§
Protocol Amendment 2 (January 2015) corrected the stratification definition for time to relapse to follow standard guidance by counting from the date of the last dose of frontline chemotherapy as opposed to counting from initial response to first-line platinum-based chemotherapy, as originally set out in the protocol.
¶
Grade 3/5 events.
#
Approximately 10% of patients in both treatment groups had a CTFI <90 days at study entry.
††
Approximately 2% of patients in both treatment groups had a CTFI <90 days at study entry.
2L: Second line; AE: Adverse event; BSC: Best supportive care; CTFI: Chemotherapy-free interval; ITT: Intention to treat; IV: Intravenous; NR: Not reported; RCT: Randomized controlled trial.
The three RCTs were possible comparator arms for the unanchored MAIC of the SCLC cohort of the basket trial in the base case analysis of platinum-sensitive patients. Of the three RCTs, Baize [33] and the basket trial had the most similar distribution of the four covariates of interest (age, sex, ECOG performance status, and disease stage), which was expected to produce the largest ESS for the basket trial; however, the ESS was slightly larger when the basket trial was matched to Eckardt [35] instead. This difference in ESS was likely attributed to the number of variables matched for the MAIC. Given that the base case analysis focused on platinum-sensitive patients only from the basket trial, an additional variable of platinum sensitivity was matched to Baize [33], which consisted of a 100% platinum-sensitive population. In contrast, platinum sensitivity could not be matched to Eckardt [35], which included a mixed population of platinum-sensitive and -resistant disease. Matching this additional variable resulted in a smaller ESS when the basket trial was matched to Baize [33] (Supplementary Table 5); however, matching to a homogeneous external trial in terms of platinum sensitivity was determined to be worth a small reduction in ESS (i.e., trade-off between matching one additional variable and reduction in ESS). Therefore, Baize [33] was selected as the RCT for the unanchored MAIC, which allowed the basket trial to be connected to the network in the base case analysis of patients with platinum-sensitive disease (Figure 2). For sensitivity analysis no. 1 based on the basket trial's full SCLC population (including patients with platinum-resistant disease), the basket trial was matched to Eckardt [35]. For a more comprehensive assessment of the relative treatment effect in the base case analysis of platinum-sensitive patients, Eckardt [35] was used as the RCT for the unanchored MAIC in sensitivity analysis no. 2. The evidence networks for these sensitivity analyses are presented in Supplementary Figure 2.

Figure 2. Evidence networks for base case analysis in patients with platinum-sensitive disease for (A) overall response rate, overall survival, grade 3/4 anemia, grade 3/4 thrombocytopenia, and grade 3/4 neutropenia.
(B) progression-free survival. Green text indicates external trial used to connect the basket trial (Trigo 2020) to the network via an unanchored MAIC; dashed line indicates pseudo-direct evidence from the MAIC.
*CTFI ≥90 d subgroup (n = 60).
CTFI: Chemotherapy-free interval; IV: Intravenous; MAIC: Matching-adjusted indirect comparison.
Relative treatment effects
Overall survival.
In the base case analysis of platinum-sensitive patients where the basket trial was connected to the network via Baize [33], lurbinectedin demonstrated a greater OS than oral topotecan (HR: 0.43; 95% CrI 0.27, 0.67), IV topotecan (HR: 0.43; 95% CrI: 0.26, 0.70), and platinum re-challenge (HR: 0.42; 95% CrI: 0.30, 0.58) (Figure 3). When the basket trial full population was connected to the network via Eckardt [35] (sensitivity analysis no. 1), the relative treatment effects of these comparisons were smaller (HR closer to 1) and no longer statistically significant. When the platinum-sensitive subgroup from the basket trial was connected to Eckardt [35] (sensitivity analysis no. 2), lurbinectedin had a greater OS benefit versus IV topotecan only (HR: 0.69; 95% CrI: 0.50, 0.96) (Supplementary Table 6). When O'Brien 2006 was added to the network including the phase II basket trial full population to assess the relative treatment effect of BSC versus lurbinectedin (sensitivity analysis no. 3), BSC had a worse OS than any of the active interventions(Supplementary Table 6).

Figure 3. Forest plot of estimated odds ratios for overall survival for the base case analysis of patients with platinum-sensitive disease.
CrI: Credible interval; HR: Hazard ratio; IV: Intravenous; OS: Overall survival.
Overall response.
Figure 4 presents the odds ratio (OR) for each intervention versus lurbinectedin for the base case analysis. Lurbinectedin was associated with a greater ORR than oral topotecan only (OR: 2.58; 95% Crl: 1.12, 5.94). Similarly, lurbinectedin demonstrated a greater ORR than oral topotecan in both sensitivity analyses no. 1 (OR: 2.94; 95% CrI: 1.54, 5.56) and no. 2 (OR: 3.22; 95% CrI: 1.60, 6.50). However, lurbinectedin was associated with a greater ORR compared with IV topotecan only in the two sensitivity analyses (Supplementary Table 6). Lurbinectedin and platinum re-challenge had comparable ORR across the three analyses.
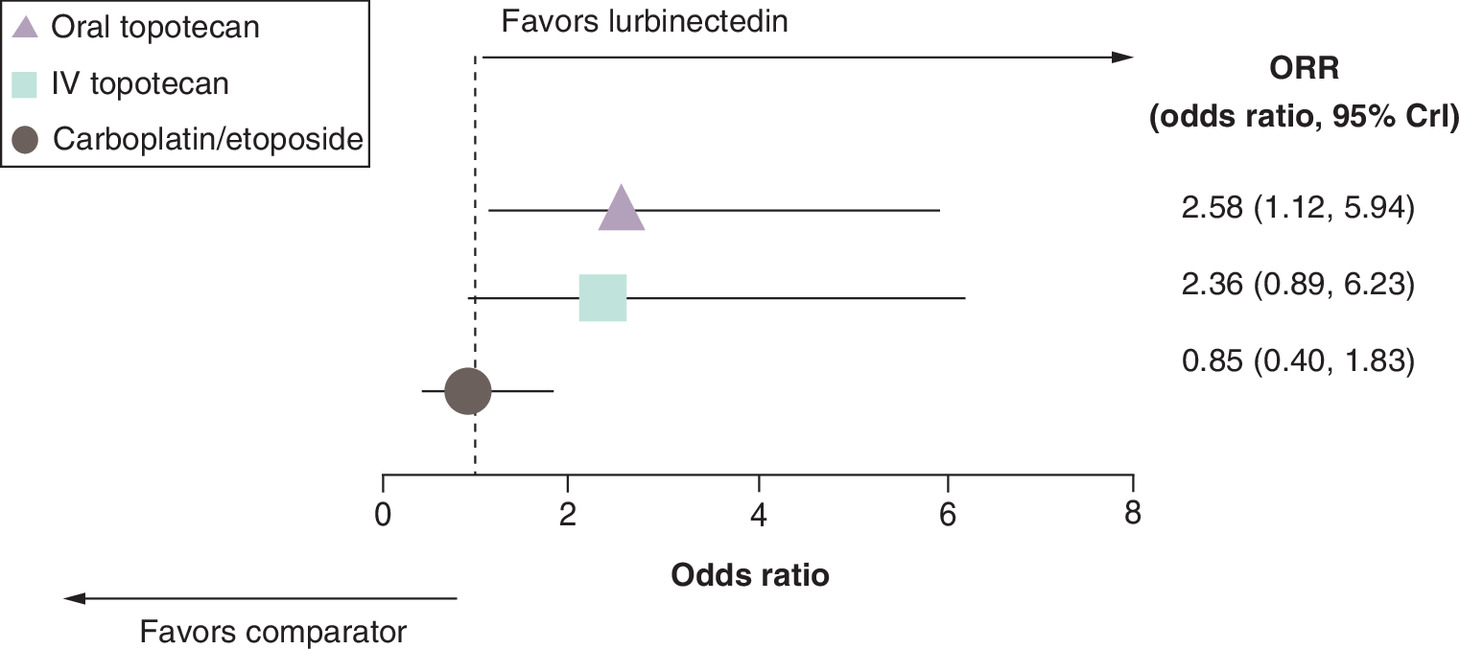
Figure 4. Forest plot of estimated odds ratios for overall response rate for the base case analysis of patients with platinum-sensitive disease.
CrI: Credible interval; IV: Intravenous; ORR: Overall response rate.
Progression-free survival & time to progression
The PFS analysis was only based on two trials (Baize [33] and the phase II basket trial) due to data availability. Figure 5 presents the time-varying HRs for two competing interventions (oral topotecan and platinum re-challenge) and the corresponding survival curves that were generated when the time-varying HRs were applied to the hazard function of oral topotecan. The time-varying HR estimates indicate that lurbinectedin was associated with a greater PFS versus oral topotecan for the first 9 months (i.e., HR <1 throughout the time period). In contrast, platinum re-challenge was comparable to lurbinectedin at first (i.e., 95% Crl included 1), but from 6 months onward, patients treated with lurbinectedin were less likely to experience progression or death than patients treated with platinum re-challenge. Similar results were observed in a scenario analysis performed by adding TTP when PFS was not available for the relevant trials (i.e., basket trial was still connected to the network via Baize [33]), with the assumption that PFS and TTP were equivalent across studies. Lurbinectedin was associated with a greater PFS/TTP than oral topotecan for the first 9 months, versus IV topotecan for at least the first 24 months, and versus platinum re-challenge from 6 months onward (Supplementary Figure 3). However, these results should be interpreted with caution due to differences in PFS/TTP definitions and differences in length of follow-up time.
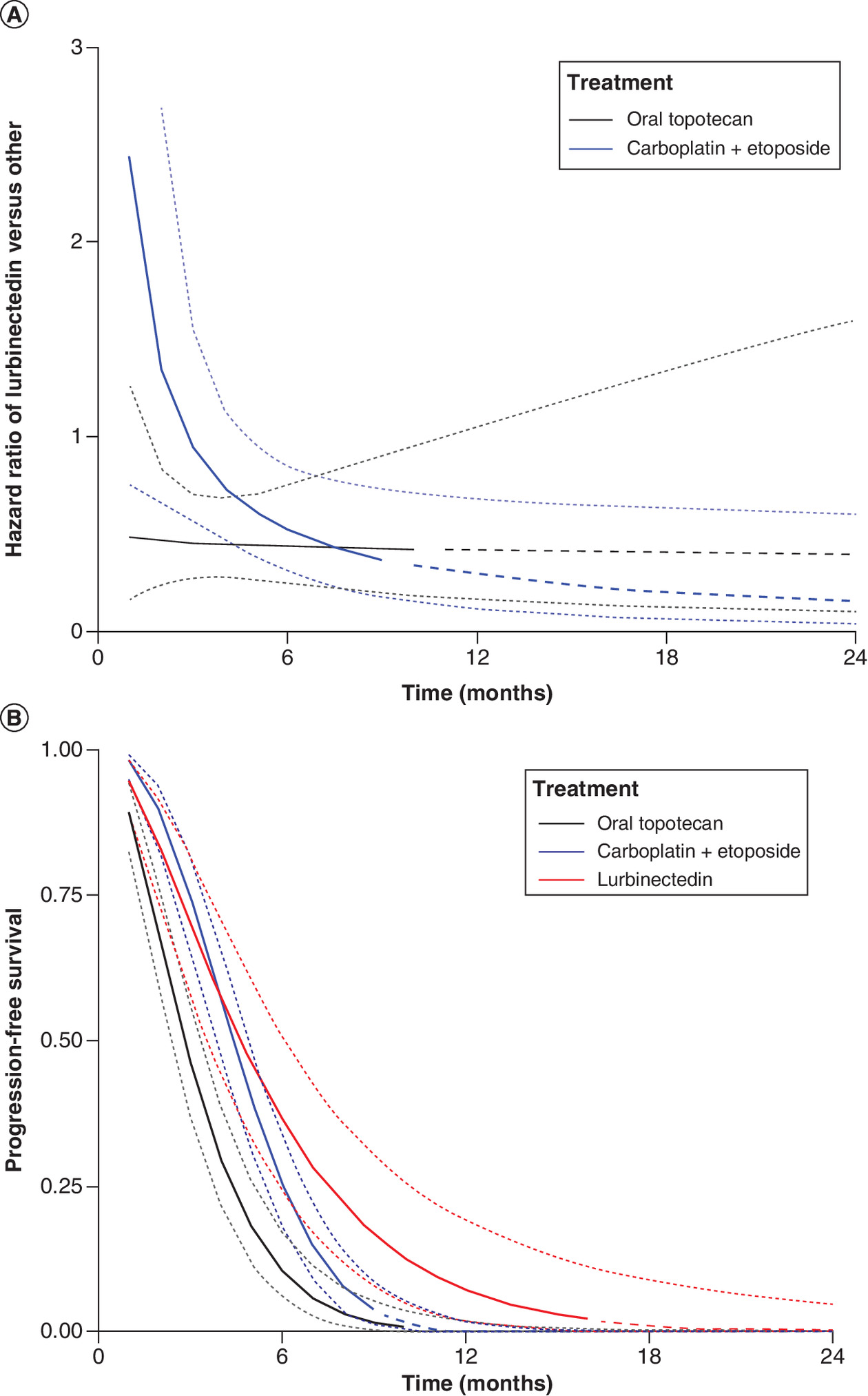
Figure 5. Results from network meta-analysis of progression-free survival.
(A) Estimated time-varying hazard ratios and 95% credible intervals for lurbinectedin versus competing interventions and (B) estimated survival curves and 95% credible intervals for lurbinectedin and competing interventions. Dashed lines at the tail of the curves represent model extrapolations. Dotted lines indicate 95% credible intervals.
Safety
Grade 3/4 anemia
In platinum-sensitive patients, lurbinectedin was associated with a lower incidence of grade 3/4 anemia compared with oral topotecan (OR: 0.28; 95% Crl: 0.09, 0.92), IV topotecan (OR: 0.21; 95% CrI: 0.06, 0.74), and platinum re-challenge (OR: 0.22; 95% CrI: 0.08, 0.61) in the base case analysis. Similar results were observed when the basket trial full population was analyzed in sensitivity analysis no. 1 where the OR for lurbinectedin was less than 0.25 versus all comparators, as well as when the basket trial platinum-sensitive subgroup was connected to the network via Eckardt [35] in sensitivity analysis no. 2 where the OR for lurbinectedin was less than 0.2 versus all comparators (Supplementary Table 7).
Grade 3/4 thrombocytopenia
In the base case analysis, lurbinectedin was associated with a lower incidence of grade 3/4 thrombocytopenia compared with oral topotecan (OR: 0.19; 95% Crl: 0.07, 0.75), IV topotecan (OR: 0.22; 95% CrI: 0.05, 0.95), and platinum re-challenge (OR: 0.23; 95% CrI: 0.08, 0.69). Similar results were observed in sensitivity analyses no. 1 and no. 2 where the OR for lurbinectedin was less than 0.15 versus all comparators (Supplementary Table 7).
Grade 3/4 neutropenia
Lurbinectedin was associated with a comparable rate of grade 3/4 neutropenia versus IV topotecan (OR: 1.19; 95% CrI: 0.45, 3.17), and a greater incidence of grade 3/4 neutropenia than oral topotecan (OR: 3.87; 95% CrI: 1.73, 8.61) and platinum re-challenge (OR: 7.05; 95% CrI: 3.09, 16.11) in the base case analysis (Supplementary Table 7) . However, in both sensitivity analyses, lurbinectedin was associated with a lower incidence of grade 3/4 neutropenia than oral topotecan (sensitivity analysis no. 1: OR: 0.37; 95% CrI: 0.20, 0.69; sensitivity analysis no. 2: OR: 0.38; 95% CrI: 0.20, 0.76) and IV topotecan (sensitivity analysis no. 1: OR: 0.11; 95% CrI: 0.06, 0.21; sensitivity analysis no. 2: OR: 0.12; 95% CrI: 0.06, 0.22), while comparable rates were observed versus platinum re-challenge (sensitivity analysis no. 1: OR: 0.68; 95% Crl: 0.24, 1.92; sensitivity analysis no. 2: OR: 0.70; 95% Crl: 0.24, 2.00).
Discussion
Lurbinectedin is the first new drug to receive FDA accelerated approval for the treatment of SCLC after platinum-based therapy in the 2L setting since topotecan was approved over 20 years ago. However, this approval was based on a Phase II basket trial without comparative efficacy and safety data. In the absence of head-to-head RCTs, indirect treatment comparisons may provide a means of estimating the relative efficacy and safety of lurbinectedin versus relevant comparators. To that end, this analysis examined the efficacy and safety of lurbinectedin compared with other FDA-approved or NCCN-recommended treatments (oral topotecan, IV topotecan, and platinum re-challenge). Using a modified two-step approach, we first performed an unanchored MAIC to connect the single-arm phase II basket trial to a network of RCTs identified from the SLR, and then performed an NMA based on this MAIC estimate and the RCTs for other competing interventions. Overall, efficacy and safety results were fairly consistent across the base case and sensitivity analyses, suggesting lurbinectedin has a survival and response advantage over other 2L treatment options in platinum-sensitive SCLC, and also has a favorable safety profile across the specific hematological AEs investigated.
Lurbinectedin had a greater OS than oral topotecan, IV topotecan, and platinum re-challenge, and PFS results were favorable for lurbinectedin across most time points, demonstrating a survival benefit in patients with platinum-sensitive disease. Of note, TTP had relatively longer follow-up time compared with PFS such that HR estimates for lurbinectedin versus oral topotecan were based on the observed data up to 21 months, in contrast to the PFS-only analysis where the HR estimates were based on the observed data up to only 9 months. Given these differences, the results of the PFS/TTP analysis should be interpreted with caution. In patients with platinum-sensitive disease, lurbinectedin was consistently associated with a greater ORR than oral topotecan; however, lurbinectedin was associated with a greater ORR compared with IV topotecan only in the two sensitivity analyses. This was possibly because when the basket trial was connected to the network via Eckardt [35], lurbinectedin became the third arm of the study that compared oral topotecan and IV topotecan, and the NMA incorporated additional evidence for the relative treatment comparison of lurbinectedin versus IV topotecan.
For grade 3/4 neutropenia, differences in results from the base case and sensitivity analyses may be explained by differences in prophylaxis requirements. Primary prophylaxis with granulocyte colony-stimulating factors (G-CSF) was recommended for all patients in Baize [33] but was not permitted in the phase II basket trial or Eckardt [35], so a comparison between the basket trial and Eckardt [35] was more appropriate. When the basket trial was connected to the network via Eckardt [35], lurbinectedin was associated with a lower incidence of grade 3/4 neutropenia versus oral topotecan and IV topotecan in patients with any platinum-sensitivity status (sensitivity analysis no. 1) and patients with platinum-sensitive disease (sensitivity analysis no. 2). Of note, EMERGE-402 (NCT04894591) [51] is an ongoing phase IV observational study assessing the effectiveness of lurbinectedin by ORR, with a secondary objective to assess the impact of G-CSF prophylaxis (primary vs secondary) in patients with ES-SCLC. This study will help guide clinical decisions regarding the routine use of G-CSF in patients with SCLC treated with lurbinectedin.
An extensive feasibility assessment was performed to evaluate differences in the distribution of study and patient characteristics across RCTs of the connected evidence network. Using the trial-specific relative treatment effects from RCTs within the NMA, we only need to ensure there are no differences in effect modifiers between these studies for valid results. There were no major differences in study characteristics between the network studies, and differences in the proportion of patients with platinum-sensitive and -resistant disease were accounted for through sensitivity analyses.
To connect the single-arm phase II basket trial to an RCT of the network as if it was an extra arm (of either Baize [33] or Eckardt [35]) and obtain credible results, between-study differences in prognostic factors and effect modifiers needed to be adjusted for. MAIC was used to achieve this goal. However, the MAIC was limited by the patient characteristics that were reported and the definitions used in the external RCTs. As a result, unmeasured confounding bias may have remained. Approximately 10% of patients in Eckardt [35] had platinum-resistant disease, which was a deviation from the inclusion criteria of the trial. Since platinum sensitivity is a known effect modifier but could not be directly accounted for in the absence of IPD, two sensitivity analyses were considered to assess the potential impact of platinum sensitivity on the estimation of relative treatment effect (i.e., including the basket trial full population or platinum-sensitive subgroup). When the basket trial platinum-sensitive subgroup was connected to the network via Eckardt [35] in sensitivity analysis no. 2, it was assumed that all patients in the network had platinum-sensitive disease. The results from this analysis are therefore expected to be more conservative, given that Eckardt [35] included a small proportion of patients with platinum-resistant disease. Limitations of the current study include that a small number of trials in the network were used; thus, only fixed-effects models were considered, which is based on a strong assumption of no between-trial heterogeneity. In addition, there were no closed loops in any evidence networks, so it was not feasible to assess the consistency between direct and indirect comparisons.
Two additional outcomes, DOR and grade 3/4 febrile neutropenia, were of interest for the analysis but had substantial limitations in data availability. Only an unanchored MAIC versus each of the three competing interventions was feasible for DOR as relative treatment effects or Kaplan-Meier curves were unavailable in the other trials. Although median DORs were reported, the corresponding standard errors were unavailable so it would need to be assumed that the difference in median DOR was normally distributed and that the standard error could be estimated based on the ranges. MAIC results from the base case analysis of platinum-sensitive patients demonstrated that the median DOR for lurbinectedin was comparable with the median DOR for oral topotecan and platinum re-challenge, as the 95% confidence intervals completely overlapped. However, the aforementioned assumption and limitations in data availability must be considered when interpreting these results. For grade 3/4 febrile neutropenia, only the basket trial and Baize [33] were included in the NMA as the outcome was not reported in other trials. Results showed lurbinectedin had a comparable incidence of grade 3/4 febrile neutropenia versus platinum re-challenge and oral topotecan (95% CrI included 1). However, in connecting the basket trial to Baize [33] through the MAIC, the network essentially only included a single trial (i.e., the basket trial was considered as the third arm of Baize [33]), so there was a lack of direct evidence to correctly estimate the indirect relative treatment effect of lurbinectedin versus relevant comparators. Results should therefore be interpreted with that in mind.
In this report, most of the included patients were not exposed to 1L immunotherapy (Table 1); however, currently the recommended 1L treatment for patients with ES-SCLC is a combination of platinum-based chemotherapy and immunotherapy [3]. Additionally, 2L treatment options after exposure to 1L immunotherapies are limited and outcomes are unclear [3,52]. This should be considered when interpreting the results of this study.
Over the past few decades, topotecan and platinum re-challenge were the only evidence-based standard of care for patients with SCLC who relapsed or had progressive disease after initial treatment with platinum-based chemotherapy. The recent FDA accelerated approval of lurbinectedin as 2L therapy in patients with SCLC is supported by the results from this analysis, which can help inform decision makers of the benefit of lurbinectedin until results from other trials become available.
Conclusion
In conclusion, using data from the single-arm phase II basket trial to estimate the comparative efficacy and safety of lurbinectedin versus oral topotecan, IV topotecan, and platinum re-challenge for SCLC that has progressed on or after platinum-based chemotherapy, results of the indirect comparison suggest that lurbinectedin has a survival and response advantage and a favorable safety profile in terms of hematological AEs for platinum-sensitive disease. The comprehensive analyses performed support the use of lurbinectedin as a 2L treatment option in SCLC. Due to the limited number of trials included in the analysis, additional RCTs may help to corroborate these findings.
Future perspective
The comparative efficacy and safety of lurbinectedin versus standard of care in the second-line SCLC setting are currently being investigated in the phase III LAGOON trial (NCT05153239) [53]. This three-arm trial will compare lurbinectedin monotherapy and the combination of lurbinectedin and irinotecan to the investigators' choice of topotecan or irinotecan in patients whose disease progressed following platinum-based chemotherapy with or without immunotherapy. In addition, there is an ongoing phase II EMERGE-201 trial (NCT05126433) [54] and phase IV EMERGE-402 observational study (NCT04894591) [51]. EMERGE-201 is a non-randomized trial designed to assess the efficacy and safety of lurbinectedin monotherapy in other advanced or metastatic solid tumors (urothelial cancer, large cell neuroendocrine tumor of the lung, and a tumor agnostic cohort of participants with homologous recombination deficient positive cancers). EMERGE-402 aims to collect data on safety (including G-CSF prophylaxis), efficacy, and health-related quality-of-life outcomes in a real-world setting among lurbinectedin-treated patients with SCLC who progressed on or after prior platinum-based chemotherapy, with or without immunotherapy. Lastly, given the hypothesized synergies between lurbinectedin and immunotherapy, the phase III IMforte trial (NCT05091567) [55] is investigating lurbinectedin plus atezolizumab versus atezolizumab alone as maintenance therapy following induction with platinum in combination with etoposide and atezolizumab in the 1L setting. Together, these studies will better define the role of lurbinectedin in the treatment paradigm for SCLC and other advanced solid tumors. Active research is also underway to understand the role of biomarkers that may be used to select patients who may benefit the most from lurbinectedin.
Background
•
Lurbinectedin is the first drug to receive accelerated approval from the Food and Drug Administration for second-line (2L) treatment of small-cell lung cancer (SCLC) since topotecan was approved >20 years ago. The approval was based on a phase II single-arm basket trial. This analysis evaluated the comparative efficacy and safety of lurbinectedin versus other 2L SCLC treatments.
Methods
Systematic literature review
•
Predefined eligibility criteria guided the identification and selection of studies. Two independent reviewers conducted study screening and data extraction.
Statistical analysis
•
Since the basket trial was a single-arm trial, a standard network meta-analysis (NMA) based on only randomized controlled trials (RCTs) could not be performed. We used a modified two-step approach consisting of an unanchored matching-adjusted indirect comparison (MAIC) to obtain estimates of the relative treatment effect of lurbinectedin versus an alternative intervention (oral topotecan, intravenous [IV] topotecan, and platinum re-challenge) for overall survival (OS), overall response rate (ORR), progression-free survival (PFS), and hematological safety outcomes. An NMA was performed based on the MAIC estimates.
•
Due to heterogeneity in the proportion of patients with platinum-sensitive or -resistant disease within the network, the base case analysis focused on the basket trial subgroup for platinum-sensitive patients.
Results
Evidence base
Relative treatment effects
•
Lurbinectedin had a greater OS than oral topotecan, IV topotecan, and platinum re-challenge in the base case NMA. The observed treatment effect was no longer statistically significant in sensitivity analysis no. 1. In sensitivity analysis no. 2, lurbinectedin had a greater OS than IV topotecan.
•
In the base case NMA, lurbinectedin had a higher ORR than oral topotecan. In the sensitivity analyses, lurbinectedin had a greater ORR than oral and IV topotecan.
•
Lurbinectedin was associated with a greater PFS versus oral topotecan from 3 months to 9 months, and versus platinum re-challenge from 6 months to 24 months.
•
Lurbinectedin was associated with a lower incidence of grade 3/4 anemia and thrombocytopenia in the base case and sensitivity analyses. When considering differences in the use of prophylactic granulocyte colony-stimulating factor, lurbinectedin was associated with a lower incidence of grade 3/4 neutropenia than oral topotecan and IV topotecan.
Conclusion
•
In this NMA, lurbinectedin showed a survival and response advantage as well as a favorable safety profile over alternative treatment options in 2L platinum-sensitive SCLC.
Financial & competing interests disclosure
This study was supported by Jazz Pharmaceuticals. R Hanvesakul, B Rengarajan, N Naveh, and A Boccuti are employees of and hold stock or stock options in Jazz Pharmaceuticals. JE Park, A Adeyemi, C Caisip, JP Jansen, and FR Wilson are employees of PRECISIONheor, which was funded by Jazz Pharmaceuticals to conduct this analysis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing support, under the direction of the authors, was provided by E Woon of CMC AFFINITY, a division of IPG Health Medical Communications, with funding from Jazz Pharmaceuticals. This was done in accordance with Good Publication Practice (GPP 2022) guidelines.
Data sharing statement
All relevant data are provided within the manuscript and supporting files.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary materials.docx)
- Download
- 1.96 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Byers LA, Rudin CM. Small cell lung cancer: where do we go from here? Cancer 121(5), 664–672 (2015).
2.
Van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet 378(9804), 1741–1755 (2011).
3.
National Cancer Comprehensive Network. Small Cell Lung Cancer, Version 2.2023. In: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) (2022). www.nccn.org
4.
Augert A, Macpherson D. Treating transcriptional addiction in small cell lung cancer. Cancer Cell 26(6), 783–784 (2014).
5.
American Cancer Society. Cancer Facts & Figures 2022. American Cancer Society, GA, USA (2022).
6.
Chan BA, Coward JI. Chemotherapy advances in small-cell lung cancer. J Thorac Dis 5(Suppl. 5), S565–S578 (2013).
7.
Simon GR, Turrisi A. Management of small cell lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 132(Suppl. 3), 324S–339S (2007).
8.
Früh M, De Ruysscher D, Popat S, Crino L, Peters S, Felip E. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 24(Suppl. 6), vi99–105 (2013).
9.
Rudin CM, Ismaila N, Hann CL et al. Treatment of small-cell lung cancer: American Society of Clinical Oncology Endorsement of the American College of Chest Physicians Guideline. J. Clin. Oncol. 33(34), 4106–4111 (2015).
10.
Micke P, Faldum A, Metz T et al. Staging small cell lung cancer: Veterans Administration Lung Study Group versus International Association for the Study of Lung Cancer–what limits limited disease? Lung Cancer 37(3), 271–276 (2002).
11.
Udyavar AR, Hoeksema MD, Clark JE et al. Co-expression network analysis identifies Spleen Tyrosine Kinase (SYK) as a candidate oncogenic driver in a subset of small-cell lung cancer. BMC Syst Biol 7(5), S1 (2013).
12.
Li L, Li W, Chen N et al. FLI1 exonic circular RNAs as a novel oncogenic driver to promote tumor metastasis in small cell lung cancer. Clin Cancer Res 25(4), 1302–1317 (2019).
13.
George J, Lim JS, Jang SJ et al. Comprehensive genomic profiles of small cell lung cancer. Nature 524(7563), 47–53 (2015).
14.
Manzo A, Sforza V, Carillio G et al. Lurbinectedin in small cell lung cancer. Front Oncol 12, 932105 (2022).
15.
Hurwitz JL, Mccoy F, Scullin P, Fennell DA. New advances in the second-line treatment of small cell lung cancer. Oncologist 14(10), 986–994 (2009).
16.
Gong J, Salgia R. Managing patients with relapsed small-cell lung cancer. J Oncol Prac 14(6), 359–366 (2018).
17.
Moser SS, Bar J, Kan I et al. Real world analysis of small cell lung cancer patients: prognostic factors and treatment outcomes. Curr Oncol 28(1), 317–331 (2021).
18.
Belgiovine C, Bello E, Liguori M et al. Lurbinectedin reduces tumour-associated macrophages and the inflammatory tumour microenvironment in preclinical models. Br. J. Cancer 117(5), 628–638 (2017).
19.
Jazz Pharmaceuticals Lurbinectedin (Zepzelca) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/213702s000lbl.pdf (Accessed 4 July 2020).
20.
Jazz Pharmaceuticals Announces U.S. FDA Accelerated Approval of Zepzelca™ (lurbinectedin) for the Treatment of Metastatic Small Cell Lung Cancer. https://www.prnewswire.com/news-releases/jazz-pharmaceuticals-announces-us-fda-accelerated-approval-of-zepzelca-lurbinectedin-for-the-treatment-of-metastatic-small-cell-lung-cancer-301077082.html (Accessed 4 July 2020).
21.
Trigo J, Subbiah V, Besse B et al. Lurbinectedin as second-line treatment for patients with small-cell lung cancer: a single-arm, open-label, Phase II basket trial. Lancet Oncol 21(5), 645–654 (2020).
•• Presents data from the basket trial (Study B-005) which was utilized to conduct the study described in this paper.
22.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol. 62(10), 1006–1012 (2009).
23.
NIH National Cancer Institute Drugs Approved for Small Cell Lung Cancer. https://www.cancer.gov/about-cancer/treatment/drugs/lung#3 (Accessed 4 July 2020).
24.
Phillippo D, Ades A, Dias S, Palmer S, Abrams K, Welton K. NICE DSU Technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICE. (2016).
• Describes the methods for matching-adjusted indirect comparisions that were used in the analyses described in this paper.
25.
Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 28(25), 3083–3107 (2009).
• Describes the methods that were used to identify the best matching trial in the analyses described in this paper.
26.
Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34(28), 3661–3679 (2015).
• Describes the methods that were used to identify the best matching trial in the analyses described in this paper.
27.
Dias S, Welton NJ, Sutton AJ, Ades AE. NICE DSU Technical Support Document 2: A Generalised Linear Modelling Framework for Pairwise and Network Meta-Analysis of Randomised Controlled Trials. National Institute for Health and Clinical Excellence, Royston, UK (2011).
28.
Dias S, Ades AE, Welton NJ, Jansen JP, Sutton AJ. Network Meta-Analysis of Survival Outcomes. In: Network Meta-Analysis for Decision-Making. Wiley, 293–322 (2018).
29.
Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 81(3), 515–526 (1994).
30.
Jansen JP. Network meta-analysis of survival data with fractional polynomials. BMC Med Res Methodol 11(1), 61 (2011).
31.
Ouwens MJ, Philips Z, Jansen JP. Network meta-analysis of parametric survival curves. Res Synth Methods 1(3–4), 258–271 (2010).
32.
Jansen JP, Cope S. Meta-regression models to address heterogeneity and inconsistency in network meta-analysis of survival outcomes. BMC Med Res Methodol 12(1), 152 (2012).
33.
Baize N, Monnet I, Greillier L et al. Carboplatin plus etoposide versus topotecan as second-line treatment for patients with sensitive relapsed small-cell lung cancer: an open-label, multicentre, randomised, phase 3 trial. Lancet Oncol 21(9), 1224–1233 (2020).
•• Presents data from Baize 2020 which was utilized to conduct the study described in this paper.
34.
O'Brien ME, Ciuleanu TE, Tsekov H et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J. Clin. Oncol. 24(34), 5441–5447 (2006).
• Presents data from O'Brien 2006 which was utilized to conduct sensitivity analysis no. 3 in this paper.
35.
Eckardt JR, Von Pawel J, Pujol JL et al. Phase III study of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer. J. Clin. Oncol. 25(15), 2086–2092 (2007).
•• Presents data from Eckardt 2007 which was utilized to conduct the study described in this paper.
36.
Von Pawel J, Gatzemeier U, Pujol JL et al. Phase ii comparator study of oral versus intravenous topotecan in patients with chemosensitive small-cell lung cancer. J. Clin. Oncol. 19(6), 1743–1749 (2001).
•• Presents data from von Pawel 2001 which was utilized to conduct the study described in this paper.
37.
United Therapeutics. Dinutuximab and irinotecan versus irinotecan to treat subjects with relapsed or refractory small cell lung cancer. ClinicalTrials.gov identifier: NCT03098030. https://clinicaltrials.gov/ct2/show/NCT03098030 (Accessed January 2023).
38.
Owonikoko TK, Niu H, Nackaerts K et al. Randomized phase II study of paclitaxel plus alisertib versus paclitaxel plus placebo as second-line therapy for small-cell lung cancer: primary and correlative biomarker analyses. J Thorac Oncol 15(2), 274–287 (2020).
39.
Spigel DR, Vicente D, Ciuleanu TE et al. Second-line nivolumab in relapsed small-cell lung cancer: checkMate331. Ann. Oncol. 32(5), 631–641 (2021).
40.
Smyth JF, Smith IE, Sessa C et al. Activity of docetaxel (Taxotere) in small cell lung cancer. The Early Clinical Trials Group of the EORTC. Eur. J. Cancer 30A(8), 1058–1060 (1994).
41.
Antonia SJ, Lopez-Martin JA, Bendell J et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol 17(7), 883–895 (2016).
42.
Ready NE, Ott PA, Hellmann MD et al. Nivolumab monotherapy and nivolumab plus ipilimumab in recurrent small cell lung cancer: Results From the CheckMate 032 Randomized Cohort. J Thorac Oncol 15(3), 426–435 (2020).
43.
Subbiah V, Paz-Ares L, Besse B et al. Antitumor activity of lurbinectedin in second-line small cell lung cancer patients who are candidates for re-challenge with the first-line treatment. Lung Cancer 150, 90–96 (2020).
44.
Baize N, Monnet I, Greillier L et al. OA15.02 Carboplatin-etoposide versus topotecan as second-line treatment for sensitive relapsed small-cell lung cancer: phase 3 trial. J Thorac Oncol 14(10), S246 (2019).
45.
Chen L, Antras L, Duh MS, Neary M, O'Brien ME. Symptom assessment in relapsed small cell lung cancer: cross-validation of the patient symptom assessment in lung cancer instrument. J Thorac Oncol 3(10), 1137–1145 (2008).
46.
Millenium Pharmaceuticals, Inc. Phase II study of alisertib (MLN8237) in combination with paclitaxel versus placebo in combination with paclitaxel as second line therapy for small cell lung cancer (SCLC). ClinicalTrials.gov identifier: NCT02038647. https://ClinicalTrials.gov/show/NCT02038647 (Accessed January 2023).
47.
Bristol-Meyers Squibb. Effectiveness study of nivolumab compared to chemotherapy in patients with relapsed small-cell lung cancer (CheckMate331). ClinicalTrials.gov identifier: NCT02481830. https://clinicaltrials.gov/ct2/show/NCT02481830 (Accessed January 2023).
48.
Trigo Perez JM, Subbiah V, Besse B et al. P1.12-03 Antitumor activity of single agent lurbinectedin in patients with relapsed SCLC occurring ≥30 days after last platinum dose. J Thorac Oncol 14(10), S535 (2019).
49.
PharmaMar S.A. Clinical study report: a multicenter phase II clinical trial of lurbinectedin (PM01183) in selected advanced solid tumors. Small cell lung cancer (SCLC) cohort. (ClinicalTrials.gov Identifier: NCT02454972). https://clinicaltrials.gov/ct2/show/NCT02454972 (Accessed January 2023).
50.
PharmaMar S.A. Addendum to the clinical study report: a multicenter phase II clinical trial of lurbinectedin (PM01183) in selected advanced solid tumors. Small cell lung cancer (SCLC) cohort. https://clinicaltrials.gov/ct2/show/NCT02454972 (Accessed January 2023).
51.
Jazz Pharmaceuticals. To assess the effectiveness and safety of Zepzelca in adult patients with extensive stage small cell lung cancer (SCLC). ClinicalTrials.gov identifier: NCT04894591. https://clinicaltrials.gov/ct2/show/NCT04894591 (Accessed January 2023).
52.
Das M, Padda SK, Weiss J, Owonikoko TK. Advances in treatment of recurrent small cell lung cancer (SCLC): insights for optimizing patient outcomes from an expert roundtable discussion. Adv Ther 38(11), 5431–5451 (2021).
53.
PharmaMar. Clinical Trial of Lurbinectedin as single-agent or in combination with irinotecan versus topotecan or irinotecan in patients with relapsed small-cell lung cancer (LAGOON). (ClinicalTrials.gov identifier: NCT05153239). https://clinicaltrials.gov/ct2/show/NCT05153239 (Accessed January 2023).
54.
Jazz Pharmaceuticals. Lurbinectedin monotherapy in participants with advanced or metastatic solid tumors. ClinicalTrials.gov identifier: NCT05126433. https://clinicaltrials.gov/ct2/show/NCT05126433 (Accessed January 2023).
55.
Hoffmann-LaRoche & Jazz Pharmaceuticals. A phase III, open-label study of maintenance lurbinectedin in combination with atezolizumab compared with atezolizumab in participants with extensive-stage small-cell lung cancer. ClinicalTrials.gov identifier: NCT05091567. https://clinicaltrials.gov/ct2/show/NCT05091567 (Accessed January 2023).
Information & Authors
Information
Published In
Copyright
© 2023 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 1 June 2022
Accepted: 6 February 2023
Published online: 20 April 2023
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect treatment comparison of lurbinectedin versus other second-line treatments for small-cell lung cancer. (2023) Journal of Comparative Effectiveness Research. DOI: 10.57264/cer-2022-0098
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jessie Wang, Rumbidzai Takundwa, Hongbo Yang, Xinglei Chai, Youfei Yu, Yuehan Zhang, Franziska Dirnberger, Erik S. Anderson, Malaika Pastel, Xerxes Pundole, Igor Gomez-Randulfe, Fiona Blackhall, Comparative efficacy of tarlatamab and second-line therapies in extensive-stage small cell lung cancer: A network meta-analysis, Lung Cancer, 10.1016/j.lungcan.2026.109465, 217, (109465), (2026).
- Franziska Dirnberger, Sachin Patel, Devon J. Boyne, Zhiyi Lan, Jenny Uyei, Jessie Wang, Seoyoon Cho, Lucy DeCosta, Ian M. Bridges, Umit Tapan, Matching-Adjusted Indirect Comparison of Tarlatamab for Patients with Platinum-Refractory or Platinum-Resistant Extensive-Stage Small-Cell Lung Cancer , Advances in Therapy, 10.1007/s12325-026-03659-4, (2026).
- V. Andreas, M. Faltys, M. Alexander, J. Rogers, S. Parakh, S. Bowyer, L. Warburton, A. Fantoni, T. Clay, S. Arulananda, I. Sullivan, S. Kao, I. Da Silva, L.J. Brown, B.G.M. Hughes, M. Itchins, B. Solomon, T. John, Second-line treatment strategies and clinical outcomes after progression on chemoimmunotherapy in extensive-stage small-cell lung cancer, Lung Cancer, 10.1016/j.lungcan.2025.108786, 209, (108786), (2025).
- Apar Kishor Ganti, Ralph B. D’Agostino, Victoria Allan, Patricia Prince, Adina Estrin, Nileesa Gautam, Anne Boccuti, Badri Rengarajan, Wenyan Li, Yanyan Cao, Xiaozhou Fan, Elizabeth M. Poole, Real-world use, effectiveness, and safety of second-line lurbinectedin monotherapy in small cell lung cancer, Future Oncology, 10.1080/14796694.2025.2499441, 21, 13, (1675-1685), (2025).
- Marcin Dzienis, Ali Mojebi, Sam Keeping, Christopher M. Black, Hilde Giezek, Niroshini Naicker, Chiara Vanetta, Julie E. Park, Keith Chan, Sanjay Merchant, Dandan Zheng, Pembrolizumab with Carboplatin and Paclitaxel Versus Alternative Systemic Treatments Recommended for the First-Line Treatment of Recurrent/Metastatic Head and Neck Cancer: An Indirect Treatment Comparison, Advances in Therapy, 10.1007/s12325-025-03144-4, 42, 6, (2690-2707), (2025).
- Jana Sawyer, Megan Banaszynski, Brian Do, Jesse Cobell, Review of outcomes in a veteran treated with lurbinectedin long-term for extensive-stage small cell lung cancer: A case report, Current Problems in Cancer: Case Reports, 10.1016/j.cpccr.2025.100350, 17, (100350), (2025).
- Manuel Dómine Gómez, Vivek Subbiah, Solange Peters, María Angeles Sala, José Trigo, Luis Paz-Ares, Antonio Nieto Archilla, Javier Gomez Garcia, Cristina Alvarez García, José Antonio López-Vilariño de Ramos, Carmen Kahatt Lopez, Cristian M. Fernandez, Lurbinectedin is an effective alternative to platinum rechallenge and may restore platinum sensitivity in patients with sensitive relapsed small cell lung cancer, Expert Review of Anticancer Therapy, 10.1080/14737140.2024.2438067, 25, 1, (27-40), (2024).
- Joo Sung Shim, Youhyun Kim, Taeho Yuh, Jii Bum Lee, Hye Ryun Kim, Min Hee Hong, Byoung Chul Cho, Sun Min Lim, Real-World Outcomes with Lurbinectedin in Second Line and Beyond for Extensive Stage Small Cell Lung Cancer in Korea, Lung Cancer: Targets and Therapy, 10.2147/LCTT.S485320, Volume 15, (149-159), (2024).
- Firas Badin, Considerations for selecting second-line treatment in patients with progressive small cell lung cancer and the use of Lurbinectedin in this setting, Cancer Treatment and Research Communications, 10.1016/j.ctarc.2024.100803, 39, (100803), (2024).