Systematic review of outcomes and patient heterogeneity in relapsed or refractory diffuse large B-cell lymphoma
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate trials of systemic therapies in transplant-ineligible or -experienced, relapsed/refractory diffuse large-B cell lymphoma and the impact of patient characteristics on overall response rate (ORR). Patients & methods: Systematically reviewed multiple databases through 22 July 2021. Analyzed variations in patient characteristics and their relationship with ORR across trials. Results: Among 17 included trials, key patient characteristics varied substantially: primary refractory (0–69%), refractory to last line of therapy (LOT) (12–100%), ≥2 prior LOTs (14–100%), ≥3 prior LOTs (0–64%), IPI ≥3 (23–73%), tumor stage III/IV (50–90%) and median age (56–74 years). ORRs varied substantially (25–83%), correlating with these characteristics. Conclusion: Differences in patient characteristics significantly contribute to the variability in ORR across these trials and should be considered when contextualizing efficacy data.
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of B-cell non-Hodgkin's lymphoma with an estimated 5.6 new cases per 100,000 individuals per year in USA [1]. Despite being an aggressive disease, over half of DLBCL cases can be cured with front-line standard of care immuno-chemotherapy (rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone [R-CHOP]) [2,3]. For the patients that do not respond to or relapse after front-line therapy, i.e., patients with relapsed/refractory (R/R) DLBCL, outcomes can vary based on factors including response to initial therapy, timing of relapse and opportunity to receive high-dose chemotherapy followed by autologous stem cell transplant (HDT-ASCT) [4].
Current treatment recommendations for R/R DLBCL differ based on whether patients are intended to receive subsequent HDT-ASCT and/or whether they relapse following ASCT. For those intended to proceed to transplant, National Comprehensive Cancer Network (NCCN)-preferred regimens include a variety of second-line platinum-based chemotherapy combinations (i.e., dexamethasone, cytarabine and cisplatin, [DHAP] ± rituximab; dexamethasone, cytarabine and oxaliplatin [DHAX] ± rituximab; gemcitabine, dexamethasone, and cisplatin or carboplatin [GDP] ± rituximab; or ifosfamide, carboplatin, and etoposide [ICE] ± rituximab) [4]. The European Society for Medical Oncology (ESMO) provides similar treatment recommendations [5]. In contrast, the optimal management of R/R DLBCL for patients who are ineligible for, or relapse after, transplant has not been established [4]. For these patients, systemic therapy regimens preferred by NCCN include gemcitabine plus oxaliplatin (GemOx) ± rituximab (i.e., R-GemOx) as well as polatuzumab vedotin ± bendamustine ± rituximab (Pola + R-Benda) and tafasitamab + lenalidomide [4]. Numerous other regimens are recommended by NCCN or deemed useful in certain circumstances. Similarly, ESMO recommends platinum- and/or gemcitabine-based regimens [5]. A review of immunochemotherapy regimens in this population found a significant gap in the availability of effective treatment options [6]. Due to the major changes in the treatment landscape for R/R DLBCL over the last 10 years, particularly the emergence of novel therapies such as chimeric antigen receptor T-cell therapies (CAR-Ts), antibody-drug conjugates and bispecific antibodies, the profile of patients enrolled into trials has evolved significantly over time. Patients enrolling in more recent R/R DLBCL trials are likely to have prior exposure to many therapeutic options, including novel therapies such as CAR-Ts. For example, both the recent LOTIS-2 and GEN3013 trials enrolled a substantial proportion of patients with prior CAR-T experience [7,8]. It can also be expected that representation of patients with prior CAR-T exposure both in clinical practice and upcoming R/R DLBCL trials of novel therapies will increase with CAR-Ts moving into earlier lines of therapy (LOTs). Similarly, the representation of patients who may have cycled through more LOTs will likely increase with increasing number of available options.
To inform clinical practice and healthcare decisions, it is important to determine the relative clinical value of available therapies. However, determination of relative clinical value is complicated by numerous issues including the lack of head-to-head clinical trial data and differences in population characteristics across trials. In a recent systematic review of clinical trial evidence specific to transplant-ineligible DLBCL patients, Thuresson et al. concluded that there is insufficient published randomized controlled trial (RCT) data to establish the comparative efficacy of treatments via network meta-analysis, and that differences in patient baseline characteristics further complicated the comparison of interventions included in their review [9]. The objective of this systematic literature review (SLR) was to synthesize outcomes from published R/R DLBCL clinical trials in patients who are ineligible for or have failed stem cell transplant, and to explore the impact of variations in trial populations on overall response rate (ORR).
Methods
This SLR was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, including the PRISMA-S checklist for literature searches. It was also conducted in alignment with EUNetHTA guidelines, using the Population, Intervention, Comparators, Outcomes and Study design (PICOS) criteria to define the scope of the SLR (Supplementary Table 1), documenting the final search strategy including the date of the search and the number of hits, use of at least two bibliographic databases, review of alternative sources (i.e., clinical trial registries and relevant documents from HTA agencies) and implementation of the Peer Review of Electronic Search Strategies (PRESS) checklist to ensure the quality of the search strategy. This review was not registered, however, the review protocol is available from the corresponding author on request.
Study eligibility & search strategy
The population of interest for this SLR were patients with R/R DLBCL ineligible for or relapsed following transplant. Included interventions were those recommended by NCCN and ESMO treatment guidelines for this patient population. The search strategy was run in MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials (CENTRAL) using Ovid and covered the period from database inception to 22 July 2021 (Supplementary Table 2). The search filter for clinical trials developed by the Scottish Intercollegiate Guidelines Network (SIGN) was used. No limits were applied to the searches. The PRESS checklist was applied by another researcher with SLR search strategy experience. In addition to databases, we searched various registries (clinicaltrials.gov, WHO-ICTRP and EU-CTR), select major HTA regulatory agencies' public reports (FDA, EMA, CADTH, Central Social Insurance Medical Council [Japan], DARE, NHS CRD HTA Database, Australia New Zealand CTR, DIMDI-AMIS [Germany]) and hand searched bibliographic references from recent related SLRs.
Study selection & data extraction
Title/abstract screening and full-text screening were both conducted in parallel by two separate reviewers. Identified clinical trials were only included if the overall study population included ≥70% of patients with DLBCL (i.e., ≤30% could have other forms of B-cell lymphoma such as high-grade B-cell lymphoma, primary mediastinal B-cell lymphoma, follicular lymphoma 3B, etc.). For individual clinical trials with multiple publications (including congress abstracts prior to journal publication), outcome data from the most recent publication was used. In cases where screening discrepancies occurred between the two reviewers, a third reviewer provided arbitration. Similarly, two separate reviewers performed parallel data extractions using a customized Microsoft® Excel® data extraction workbook, extracting all demographic, clinical and outcomes data of interest from eligible studies. Any discrepancies observed between the two extractions were resolved through arbitration from a third reviewer. Risk of bias was assessed by a single reviewer using the Cochrane Risk of Bias 2 tool [10] for RCTs and the MINORS tool [11] for single-arm trials (Supplementary Tables 3 & 4).
Evidence synthesis & analysis
Variations in patient baseline characteristics and the corresponding efficacy outcomes were described for the included trials. Pearson correlation coefficients were calculated between patient baseline characteristics and ORR across trials that evaluated the same treatment and overall. A conventional approach informed the interpretation of the correlation coefficients: moderate correlation (0.40–0.69), strong correlation (0.70–0.89) and very strong correlation (0.90–1.00) [12]. For additional context, inclusion criteria regarding reasons for transplant ineligibility and/or failure following transplant were also summarized.
Results
The search strategy yielded a total of 21,130 abstracts, 2304 of which underwent full-text screening. A total of 18 publications reporting on 17 clinical trials met the study inclusion criteria (Figure 1). These studies evaluated R-GemOx (3 studies) [13–15], rituximab plus bendamustine (R-Benda; 3 studies) [16–18], Pola + R-Benda (2 studies) [17,19], CAR-Ts (3 studies) [20–22] and seven other studies – one each for loncastuximab tesirine [7], Tafa plus Len [23], selinexor [24], rituximab plus gemcitabine (note that the rituximab plus pixantrone arm was excluded because it is not guideline recommended) [25], rituximab plus lenalidomide [26], rituximab plus etoposide/methylprednisolone/cytarabine/cisplatin [27] and gemcitabine plus vinorelbine [28]. One publication provided data for two of the above regimens [17]. One trial comprised a two-arm RCT and a single-arm extension, described in separate publications; however these three treatment arms were considered to come from the same single trial [17,29].
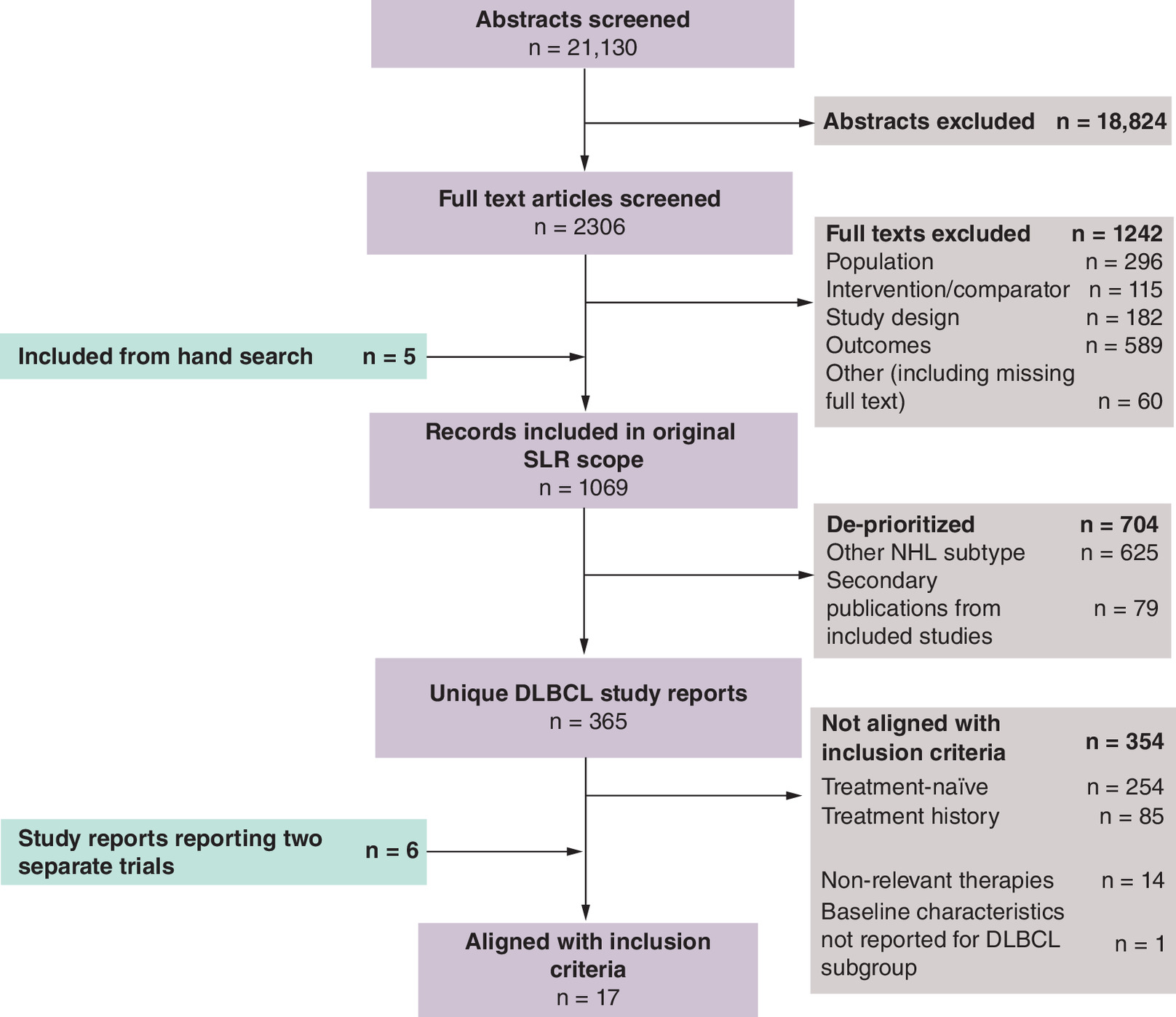
Figure 1. PRISMA diagram of study flow.
DLBCL: Diffuse large B-cell lymphoma; NHL: Non-Hodgkin's lymphoma; PRISMA: Preferred Reporting Items of Systematic reviews and Meta-Analyses; SLR: Systematic literature review.
Across all treatment regimens, the sample sizes of the trials evaluated varied substantially from 13 patients to 269 patients. When reported, key patient baseline characteristics varied widely across the trials of therapies evaluated: The proportion of patients with primary refractory disease enrolled across the evaluated trials ranged from 0 to 69% (Table 1). For almost half of the therapies evaluated, trials did not report the proportion of primary refractory patients enrolled. The proportion of patients with disease that is refractory to last LOT ranged from 12 to 100%, and the proportion of patients with three or more prior LOTs ranged from 0 to 64%. Similarly, the proportion of patients with International Prognostic Index (IPI) ≥3 ranged from 23 to 73%. Less variation was observed in the proportion of patients with ECOG≥1 (ranging only from 67 to 100%), the proportion of patients with Ann Arbor stage III/IV (ranging from 50 to 90%) and the median age of patients enrolled in trials (ranging from 56–74 years). Most of the studies had substantial proportions of patients enrolled with prior rituximab/anti-CD20 exposure, and only four trials enrolled ≥30% patients with prior ASCT. Similarly, the reported efficacy outcomes of ORR, complete response rates (CRR), duration of response (DOR), progression free survival (PFS) and overall survival (OS) all varied widely across these trials (Table 1 and Table 2).
| Study (year), design | n | Median age, years (range) | Ann Arbor tumor stage | IPI risk | ECOG PS | Prior rituximab/ anti-CD20 mAb experience | Prior ASCT experience | ≥2 prior LOT | ≥3 prior LOT | Primary refractory | Refractory to last line of therapy | ORR | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R-GemOx | |||||||||||||
| Mounier (2013), single-arm | 49 | 69 (41–77) | I/II: 12% III/IV: 88% | 0–1: 24% ≥2: 76% (Saa) | 0–1: 78% ≥2: 22% | 63% | 35% | 14% | 0% | 12% | 12% | 61% (post-induction) | [15] |
| Lopez (2008), single-arm | 32 | 69 (32–85) | I/II: 25% III/IV: 75% | 0–1: 31% ≥2: 69% (adjusted) | 0–1: 67% ≥2: 33% | 78% | NR | 44% | NR | 25% | 41% | 43% (EOT) | [14] |
| El Gnaou (2007),† single-arm | 46 | 64 (43–78) | I/II: 22% III/IV: 78% | 0–1: 63% ≥2: 37% (aa) | 0–1: 67% ≥2: 33% | 57% | 30% | 61% | NR | 13% | NR | 83% (post-induction) | [13] |
| R-Benda | |||||||||||||
| Sehn (2020) (GO29365), RCT | 40 | 71 (30–84) | I/II: 10% III/IV: 90% | 0–2: 28% ≥3: 73% | 0–1:78% 2: 20% | 100% | 15% | 70% | 48% | 68% | 85% | 25% (best) | [17] |
| Vacirca (2014), single-arm | 61 | 74 (25–90) | I/II: 10% III/IV: 89% | 0–2: 36% ≥3: 63% (revised-IPI) | 0–1: 94% 2: 6% | 95% | 8% | 49% | 28% | NR | NR | 46% (best) | [18] |
| Ohmachi (2013), single-arm | 59 | 67 (36–75) | I/II: 39% III/IV: 61% | 0–2: 69% ≥3: 31% | 0–1: 100% ≥2: 0% | 97% | 14% | 36% | 14% | NR | 14% | 63% (best) | [16] |
| Pola + R-Benda | |||||||||||||
| Terui (2021) (P-DRIVE), single-arm | 35 | 71 (46–86) | I/II: 31% III/IV: 69% | 0–1: 9% 2: 40% ≥3: 52% | 0–1: 91% 2: 9% | 97% | 11% | 66% | 43% | NR | 66% | 71% (best) | [19] |
| Sehn (2020) (GO29365); RCT | 40 | 67 (33–86) | I/II: 15% III/IV: 85% | 0–2: 45% ≥3: 55% | 0–1: 83% 2: 15% | 98% | 25% | 73% | 45% | 53% | 75% | 63% (best) | [17] |
| Sehn (2020) (GO29365), single-arm extension | 106 | 70 (24–94) | I/II: 21% III/IV: 79% | 0–2: 34% ≥3: 66% | 0–1: 87% 2: 13% | NR | NR | 65% | 40% | 69% | 76% | 57% (best) | [29] |
| CAR-T | |||||||||||||
| Abramson (2020) (TRANSCEND-NHL-001),‡ single-arm lisocabtagene maraleucel | 269 | 63 (18–86) | NR | NR | 0–1: 99% 2: 1% | 100% | 33% | 97% | 51% | NR | 67% | 73% (best) | [20] |
| Schuster (2019) (JULIET), single-arm tisagenlecleucel | 111 | 56 (22–76) | I/II: 24% III/IV: 76% | 0–1: 27% ≥2: 73% | 0–1: 100% ≥2: 0% | 100% | 49% | 95% | 52% | NR | 55% | 52% (best) | [22] |
| Neelapu (2017) (ZUMA-1), single-arm axicabtagene ciloleucel | 77 | 58 (25–76) | I/II: 13% III/IV:87% | 0–2: 52% 3–4: 48% | 0–1: 100% ≥2: 0% | NR | 21% | NR | 64% | 3% | 100% | 82% (best) | [21] |
| Others | |||||||||||||
| Caimi (2021) (LOTIS-2),§ single-arm loncastuximab tesirine | 145 | 66 (IQR: 56–71) | I/II: 23% III/IV: 77% | NR | 0–2: 100% | NR | 14% | 100% | 56% | 20% | 58% | 48% (best) | [7] |
| Salles (2020) (L-MIND), single-arm tafasitamab + lenalidomide | 81 | 72 (IQR:62–76) | I/II: 25% III/IV: 75% | 0–2: 49% 3–5: 51% | 0–1: 91% 2: 9% | 100% | 11% | 50% | 7% | 19% | 44% | 60% (best) | [23] |
| Kalakonda (2020) (SADAL), single-arm selinexor | 127 | 67 (35–87) | NR | NR | 0–1: 90% ≥2: 10% | 100% | 30% | 100% | 41% | NR | 72% | 28% (best) | [24] |
| Pettengell (2020) (PIX306), RCT R + gemcitabine | 157 | 73 (26–90) | I/II: 25% III/IV: 75% | 0–2: 46% 3–5: 54% | 0–1: 79% 2: 20% | 100% | 10% | 33% | 12% | 0% | NR | 44% (best) | [25] |
| Zinzani (2011), single-arm R + lenalidomide | 23 | 74 (NR) | I/II: 22% III/IV: 78% | 0–2: 30% ≥3: 70% | 0–2: 100% | ≥35%¶ | ≥4%¶ | 100% | ≥50%¶ | NR | NR | 35% (post-induction) | [26] |
| Harting (2007), single-arm R-ESHAP | 13 | 56 (37–70) | I/II: 23% III/IV: 77% | NR | 0–1: 100% ≥2: 0% | ≥23%¶ | NR | NR | NR | NR | 15% | 77% (best) | [27] |
| Papageorgiou (2005), single-arm gemcitabine + vinorelbine | 22 | 65 (41–82) | I/II: 50% III/IV: 50% | 0–2: 77% ≥3: 23% | 0–1: 68% ≥2: 32% | NR | 0% | 36% | 5% | NR | 36% | 50% (best) | [28] |
†
Values denote those for the entire study population (n = 46; 33 [72%] had DLBCL, 8 [17%] had follicular lymphoma and 5 [11%] had mantle cell lymphoma).
‡
Values denote those for the entire study population (n = 269; 215 [80%] had DLBCL, 36 [13%] had high-grade B-cell lymphoma with gene rearrangements in MYC and either BCL2, BCL6 or both, 15 [6%] had primary mediastinal B-cell lymphoma and 3 [1%] had follicular lymphoma grade 3B).
§
Value denotes those for the entire study population (n = 145; 127 [88%] had DLBCL, 11 [8%] had high-grade B-cell lymphoma and 7 [5%] had primary mediastinal B-cell lymphoma).
¶
Unable to calculate the exact percentage, but could confirm the minimum value from data reported in the publication.
aa-IPI: Age-adjusted IPI; ASCT: Autologous stem cell transplant; Benda: Bendamustine; CAR-T: Chimeric antigen receptor T-cell; ECOG-PS: Eastern Cooperative Oncology Group performance status; Gem/Ox: Gemcitabine + oxaliplatin; IPI: International Prognostic Index; LOT: Line of therapy; mAb: Monoclonal antibody; NR: Not reported; Pola: Polatuzumab; R: Rituximab; RCT: Randomized controlled trial; ESHAP: Etoposide + methylprednisolone + cytarabine + cisplatin; Saa-IPI: Secondary age-adjusted IPI.
| Study (year), design | Response criteria | Response assessor | ORR | CRR | DOR, median (95% CI), months | PFS, median (95% CI), months | OS, median (95% CI), months | Ref. |
|---|---|---|---|---|---|---|---|---|
| R-GemOx | ||||||||
| Mounier (2013), single-arm | Cheson/IWG (1999) [30] | Investigators | 61% (post-induction) 46% (EOT) | 44% (post-induction) 38% (EOT) | 10 (NR) | 5 (NR) | 11 (NR) | [15] |
| Lopez (2008); single-arm | Cheson/IWG (1999) [30] | Investigators | 43% (EOT) | 34% (EOT) | NR | NR | 9 (3, 15) | [14] |
| El Gnaoui (2007),† single-arm | Cheson/IWG (1999) [30] | Investigators | 83% (post-induction) 74% (EOT) | 50% (post-induction) 72% (EOT) | NR | NR | NE | [13] |
| R-Benda | ||||||||
| Sehn (2020) (GO29365), RCT | Lugano criteria (modified) [31] | IRC | 25% (best) 18% (EOT) | 23% (best) 18% (EOT) | 8 (4, 19) | 4 (2, 5) | 5 (4, 8) | [17] |
| Vacirca (2014), single-arm | Revised Cheson/IWG (2007) [32] | IRC | 46% (best) | 15% (best) | 17 (4, NE) | 4 (3, 7) | NE | [18] |
| Ohmachi (2013), single-arm | Revised Cheson/IWG (2007) [32] | IRC | 63% (best) | 37% (best) | NR | 7 (4, 14) | NR | [16] |
| Pola + R-Benda | ||||||||
| Terui (2021) (P-DRIVE), single-arm | Lugano criteria (modified) [31] | Investigators | 71% (best) 43% (EOT) | 43% (best) 34% (EOT) | 7 (4, NE) | 5 (4, NE) | NE (8, NE) | [19] |
| Sehn (2020) (GO29365), RCT | Lugano criteria (modified) [31] | IRC | 63% (best) 45% (EOT) | 50% (best) 40% (EOT) | 13 (7, NE) | 10 (6, 14) | 12 (9, NE) | [17] |
| Sehn (2021) (GO29365), single-arm extension | Lugano criteria (modified) [31] | IRC | 57% (best) 43% (EOT) | 53% (best) 40% (EOT) | 6 (5, 12) | 6 (5, 8) | 11 (8, 14) | [29] |
| CAR-T | ||||||||
| Abramson (2020) (TRANSCEND-NHL-001),‡ single-arm lisocabtagene maraleucel | Lugano criteria [31] | IRC | 73% (best) | 53% (best) | NE (9, NE) | 7 (3, 14) | 21 (13, NE) | [20] |
| Schuster (2019) (JULIET), single-arm tisagenlecleucel | Lugano criteria [31] | IRC | 52% (best) | 40% (best) | NE (10, NE) | NR | 12 (7, NE) | [22] |
| Neelapu (2017) (ZUMA-1), single-arm axicabtagene ciloleucel | Revised Cheson/IWG (2007) [32] | IRC | 82% (best) | 49% (best) | NR§ | NR§ | NR§ | [21] |
| Others | ||||||||
| Caimi (2021) (LOTIS-2),¶ single-arm loncastuximab tesirine | Lugano criteria [31] | IRC | 48% (best) | 24% (best) | 10 (7, NE) | 5 (3, 8) | 10 (7, 12) | [7] |
| Salles (2020) (L-MIND), single-arm tafasitamab + lenalidomide | Revised Cheson/IWG (2007) [32] | IRC | 60% (best) | 43% (best) | 22 (22, NE) | 12 (6, NE) | NE (18, NE) | [23] |
| Kalakonda (2020) (SADAL), single-arm selinexor | Lugano criteria [31] | IRC | 28% (best) | 12% (best) | 9 (5, 23) | 3 (2, 4) | 9 (7, 15) | [24] |
| Pettengell (2020) (PIX306), RCT R + gemcitabine | Revised Cheson/IWG (2007) [32] | IRC | 44% (best) | 22% (best) | 9 (7, 19) | 6 (4, 8) | 20 (12, 32) | [25] |
| Zinzani (2011), single-arm lenalidomide + rituximab | Revised Cheson/IWG (2007) [32] | NR | 35% (post-induction) 35% (EOT) | 30% (post-induction) 35% (EOT) | NR | NR | NR | [26] |
| Harting (2007), single-arm R-ESHAP | Cheson/IWG (1999) [30] | NR | 77% (best) | 54% (best) | 14 (NR) | NR | NR | [27] |
| Papageorgiou (2005), single-arm gemcitabine + vinorelbine | Cheson/IWG (1999) [30] | NR | 50% (best) | 14% (best) | NR | 8 (NR) | 13 (NR) | [28] |
†
Values denote those for the study entire population (n = 46; 33 [72%] had DLBCL, 8 [17%] had follicular lymphoma and 5 [11%] had mantle cell lymphoma).
‡
Values denote those for the study entire population (n = 269; 215 [80%] had DLBCL, 36 [13%] had high-grade B-cell lymphoma with gene rearrangements in MYC and either BCL2, BCL6 or both, 15 [6%] had primary mediastinal B-cell lymphoma and 3 [1%] had follicular lymphoma grade 3B).
§
DOR, PFS and OS was reported for the entire study population, but not the DLBCL subpopulation alone.
¶
Value denotes those for the entire study population (n = 145; 127 [88%] had DLBCL, 11 [8%] had high-grade B-cell lymphoma and 7 [5%] had primary mediastinal B-cell lymphoma).
Benda: Bendamustine; CAR-T: Chimeric antigen receptor T-cell; CI: Confidence interval; CRR: Complete response rate; DOR: Duration of response; EOT: End of treatment; ESHAP: Etoposide + methylprednisolone + cytarabine + cisplatin; Gem/Ox: Gemcitabine + oxaliplatin; IRC: Independent radiology review committee; IWG: International Working Group; NE: Not evaluable; NR: Not reported; ORR: Objective response rate; OS: Overall survival; PFS: Progression-free survival; Pola: Polatuzumab; R: Rituximab; RCT: Randomized controlled trial.
When all 17 studies were included, negative correlations of moderate strength were estimated between ORR and median age, as well as previous treatment with rituximab or other anti-CD20 therapy, primary refractory disease or at high-intermediate/high IPI risk (Table 3).
| Regimen (n treatment arms) | Median age | Ann Arbor tumor stage III/IV | IPI risk high-intermediate or higher | ECOG PS ≥2 | Prior rituximab/ anti-CD20 mAb failure | Prior ASCT failure | ≥2 prior LOT | ≥3 prior LOT | Primary refractory | Refractory to last line of therapy |
|---|---|---|---|---|---|---|---|---|---|---|
| R-GemOx (n = 3) | -0.89 | 0.16 | -0.81 | 0.06 | -0.96 | NA | 0.41 | NA | -0.80 | NA |
| R-Benda (n = 3) | -0.52 | -0.85 | -0.94 | -0.99 | -0.64 | -0.19 | -1.00 | -1.00 | NA | NA |
| Pola + R-Benda (n = 3) | 0.32 | -0.68 | -0.92 | -0.71 | NA | NA | 0.03 | 0.53 | NA | -0.94 |
| CAR-T (n = 3) | 0.49 | NA | NA | 0.23 | NA | -0.99 | NA | 0.68 | NA | 0.88 |
| All (n = 19) | -0.52 | -0.06† | -0.49‡ | -0.26† | -0.40‡ | 0.18§ | -0.19† | 0.11§ | -0.43¶ | -0.13§ |
Correlation coefficients between ORR and each baseline characteristic were only calculated when at least 3 individual study data values were available for the baseline characteristic; otherwise listed as NA.
†
Based on n = 17 data points.
‡
Based on n = 14 data points.
§
Based on n = 15 data points.
¶
Based on n = 10 data points.
ASCT: Autologous stem cell transplant; Benda: Bendamustine; ECOG PS: Eastern Cooperative Oncology Group performance status; GemOx: Gemcitabine + oxaliplatin; IPI: International Prognostic Index; LOT: Line of therapy; mAb: Monoclonal antibody; NA: Not available; ORR: Objective response rate; Pola: Polatuzumab; R: Rituximab.
Rituximab + Gemcitabine + Oxaliplatin
Three R-GemOx studies were identified [13–15]. One study included 28% of patients with follicular or mantle cell lymphoma [13]. All studies were small (n <50), single-arm trials published between 2007 and 2013. The widest variation in characteristics across studies was the proportion of patients with high-intermediate/high risk IPI scores (37% to 76%), the proportion with two or more prior LOT (14 to 61%) and the proportion who are refractory to their last LOT (12% to 41%). Two R-GemOx trials reported ASCT experience and both reported approximately one third of patients with prior ASCT experience (Table 1) [13,14]. Additional baseline characteristics are listed in Table 1. ORR and CRR were reported at both post-induction (i.e., after the first 4 cycles of R-GemOx) and end of treatment (EOT) timepoints (Table 2). Across the R-GemOx studies, lower response rates were reported in the studies where either majority of the cohort had high-intermediate/high IPI scores, prior anti-CD20 experience, three or more prior LOTs, or were primary refractory.
Correlations from the three R-GemOx studies revealed strong to very strong negative associations between ORR and a variety of baseline characteristics including median age, proportions of patients who were primary refractory, high-intermediate/high IPI risk, or had previous rituximab or other anti-CD20 treatment experience (Table 3). A moderate positive correlation was estimated between ORR and the proportion of patients who had received two or more prior LOTs.
Reported reasons for ASCT ineligibility varied across studies and included failure of HDT [14], age, comorbidities or prior HDT experience (Table 4) [13].
| Study (year) | Intervention | ASCT ineligibility criteria | Ref. |
|---|---|---|---|
| Mounier (2013) | R-GemOx | Relapsed/refractory; not eligible for HDT (no specific reasons given) | [15] |
| Lopez (2008) | R-GemOx | Patients who did not achieve complete response after induction or who relapsed (and hence were unable to proceed to transplant) | [14] |
| El Gnaoui (2007) | R-GemOx | Patients of any performance status were eligible for inclusion if they were unsuitable for HDT because of age, previous HDT, serious comorbidities or a combination of these factors | [13] |
| Vacirca (2014) | R-Benda | Autologous stem cell transplant-eligible patients were excluded, with the exception of those who refused ASCT. Patients with disease relapse after prior ASCT or allogeneic stem cell transplantation were allowed. Study patients were not candidates for high-dose therapy either because of advanced age, failure of salvage therapy, or comorbidities. | [18] |
| Ohmachi (2013) | R-Benda | Patients considered ASCT eligible were excluded (no specific reasons given) | [16] |
| Sehn (2020) | R-Benda (RCT) Pola + R-Benda (RCT) Pola + R-Benda (Single-arm extension) | Patients considered transplantation ineligible by the treating physician or experienced treatment failure with prior ASCT (no specific reasons given) | [17] |
| Terui (2021) | Pola + R-Benda | Patients were ineligible for ASCT as assessed by a study investigator (no specific reasons given) or experienced treatment failure with prior ASCT | [19] |
| Neelapu (2017) (ZUMA-1) | Axicabtagene ciloleucel | Refractory status as per refractory definition (includes patients who were ASCT relapsed within 12 months from transplant). | [21] |
| Schuster (2019) (JULIET) | Tisagenlecleucel | Patients had either had a relapse after or were ineligible for ASCT (no specific reasons given) | [22] |
| Abramson (2020) (TRANSCEND-NHL-001) | Lisocabtagene maraleucel | Relapsed / refractory disease after at least two systemic lines of therapy or after ASCT (based on reported baseline characteristics, included patients were either chemo-refractory or ASCT-relapsed) | [20] |
| Salles (2020) (L-MIND) | Tafasitamab + lenalidomide | Patients were not candidates for HDT and subsequent ASCT (no specific reasons given) | [23] |
| Kalakonda (2020) (SADAL) | Selinexor | Patients who progressed after, or were not candidates for, ASCT (no specific reasons given) | [24] |
| Caimi (2021) (LOTIS-2) | Loncastuximab tesirine | Not explicitly stated. Inferred based on requirement of at least two prior lines of therapy and motivation statement in intro “Outcomes for patients who are unsuitable for salvage chemotherapy and autologous haematopoietic stem-cell transplantation (HSCT) and for those who do not respond or who relapse after such treatment remain poor, despite recent approvals of novel therapeutic approaches.” | [7] |
| Pettengell (2020) | R-Gemcitabine | Patients were not eligible for HDT-SCT (no specific reasons given) | [25] |
| Zinzani (2011) | Lenalidomide + Rituximab | Inferred. Study included pretreated elderly patients | [26] |
| Harting (2007) | R-ESHAP | Eligibility for SCT was an exclusion criterion (no specific reasons given) | [27] |
| Papageorgiou (2005) | Gemcitabine + Vinorelbine | Ineligibility for ASCT due to several reasons such as age, chemorefractory disease, inadequate mobilization | [28] |
(A)SCT: (Autologous) stem cell transplant; Benda: Bendamustine; HDT: High-dose therapy; GemOx: Gemcitabine + oxaliplatin; IPI: International Prognostic Index; mAb: Monoclonal antibody; NR: Not reported; Pola: Polatuzumab; R: Rituximab; RCT: Randomized controlled trial; ESHAP: Etoposide + methylprednisolone + cytarabine + cisplatin; Saa-IPI: Secondary age-adjusted IPI.
Rituximab + Bendamustine
Three R-Benda studies were identified, two single-arm trials [16,18] and one RCT [17]. All studies were small (n ≤61) and published between 2013 and 2020. Among baseline characteristics, the widest variation was observed in the proportion of patients with Ann Arbor stages III/IV (61–90%), high-intermediate/high IPI risk scores (31–73%), two or more prior LOTs (36–70%) and refractory to last LOT (14–85%). The percentage of patients with prior ASCT experience ranged from 8 to 15% (Table 1). The best ORR ranged from 25 to 63% and CRR ranged from 15 to 37%. DOR and survival outcome data availability varied (Table 2). Across the R-Benda studies, lower response rates were reported in the studies in which the majority of the cohort had high-intermediate/high IPI scores, three or more prior LOTs and/or were primary refractory.
Correlations estimated from the three R-Benda studies revealed moderate to very strong negative associations between ORR and a variety of baseline characteristics including median age, as well as the proportion of patients who were rituximab/anti-CD20 treatment experienced, Ann Arbor stage III/IV, high-intermediate/high IPI risk, ECOG PS ≥2, had received two or more prior LOTs, or had received three or more prior LOTs (Table 3).
Polatuzumab Vedotin + Rituximab + Bendamustine
Three Pola + R-Benda studies were identified, one single-arm trial [19], one RCT [17] and a single-arm extension for the RCT [17]. The two core studies were small (n ≤40) and published between 2020–2021, while the single-arm extension included 106 patients and was published in 2020 [29]. Median patient age ranged from 67 to 71 years, most had Ann Arbor stages III/IV (69–85%), more than half were at high-intermediate/high IPI risk (52–66%) and the vast majority had previous rituximab/anti-CD20 monoclonal antibody treatment (≥97%), although the single-arm extension publication did not provide these data. The percentage of patients with prior ASCT experience was 25% in the RCT [17] and 11% in the single-arm trial (Table 1) [19]. The best ORR ranged from 57 to 71% and CRR ranged from 43 to 53%. EOT ORR for these Pola + R-Benda studies ranged from 43 to 45% and CRR ranged from 34 to 40%. DOR and survival outcome data are listed in Table 2. Across the Pola + R-Benda studies, lower response rates were reported in the studies with either higher proportions of patients that were primary refractory or refractory to last line of therapy.
Pearson correlation coefficients estimated for available data from the three Pola + R-Benda studies revealed moderate to very strong negative relationships between ORR and a variety of baseline characteristics including the proportion of patients who were Ann Arbor stage III/IVECOG PS ≥2, high-intermediate/high IPI risk, or refractory to last line of therapy. A moderate positive relationship was detected between ORR and the proportion of patients who had three or more prior LOTs (Table 3).
CAR-T
Three CAR-T studies were identified, all of which were single-arm trials published between 2017–2020 with R/R DLBCL study sample sizes that ranged from 77 to 269, although the largest of the three studies included 54 (20%) with high-grade B-cell lymphoma with gene rearrangements in MYC and either BCL2, BCL6 or both, primary mediastinal B-cell lymphoma, or follicular lymphoma grade 3B [20–22]. The majority (≥95%) of patients had two or more prior LOTs. The baseline characteristics that varied most widely across studies were the proportion of patients with high-intermediate/high IPI risk score (48–73%), prior ASCT experience (21% to 49%) and refractory to last LOT (55–100%) (Table 1). The best ORR ranged from 52 to 82% and CRR ranged from 40 to 53%. DOR and survival outcome data availability varied (Table 2).
Correlations could not be calculated for half of the baseline characteristics of interest due to a missing value from at least one of the publications. For the remaining baseline characteristics, correlations estimated from the three CAR-T studies revealed negative associations between ORR and the proportion of patients who had prior ASCT experience, as well as a positive association between ORR and median age, the proportion of patients who had three or more prior LOTs and the proportion who were refractory to last LOT (Table 3).
‘Other’ studies
Studies in the ‘other’ category evaluated interventions for which only one trial met the inclusion criteria for this review. Hence, this category contains one study each for loncastuximab tesirine(20% primary refractory patients), tafasitamab plus lenalidomide (50% second-line patients and 19% primary refractory patients), selinexor, rituximab plus gemcitabine (67% second-line patients and 0% primary refractory patients), rituximab plus lenalidomide, rituximab plus etoposide/methylprednisolone/cytarabine/cisplatin, and gemcitabine plus vinorelbine, and were published between 2005 and 2021. Study and patient characteristics are reported in Table 1 and efficacy results in Table 2.
Discussion
The current analysis indicates that the baseline characteristics of patients enrolled in trials of systemic R/R DLBCL therapies varied widely, as did the corresponding efficacy outcomes. Moreover, these variations were observed within subsets of trials investigating the same regimen, with reported ORRs negatively correlating with patient baseline characteristics.
Across each treatment class evaluated in this study, the baseline patient characteristics that were most consistently observed in cohorts with low ORRs were high-intermediate/high IPI scores, three or more prior LOTs and proportion of patients with primary refractory disease. The baseline characteristics that showed consistently strong (negative) correlations with ORR were higher ECOG PS, high-intermediate/high IPI risk and proportion of patients with primary refractory disease. Higher ECOG PS (indicating poorer patient condition) has been previously associated with poorer response rates in older patients, possibly due to the less intensive treatment regimens [33]. Patients with high IPI risk, primary refractory disease and/or more heavily pre-treated also had very poor response rates in the SCHOLAR-1 cohort (refractory DLBCL patients) [34]. Another potential source of variation in this population was in the proportion of patients who were included due to transplant-ineligibility, as opposed to being included due to relapsing following prior transplant. Further, among studies that included transplant-ineligible patients, there was a low rate of reporting specific reasons for ineligibility, potentially adding greater heterogeneity to these patient populations.
With respect to number of prior therapies, a temporal relationship was observed, with older trials (specifically those evaluating R-GemOx and R-Benda) reporting a lower proportion of heavily pre-treated patients than those conducted more recently. There is also opportunity for differences in observed efficacy that may be influenced by changes in clinical management over time; the studies included in the current analysis were published over a 16-year span (2005–2021) during which substantial changes in clinical management occurred. Another important feature to highlight, specific to this evolving clinical landscape, is the change of the patient population with respect to CAR-T experience. With the approval of the first CAR-Ts for R/R DLBCL (Yescarta [axi-cel] in 2017, followed by Kymriah [tisa-cel] in 2021 and Breyanzi [liso-cel] in 2022), upcoming clinical trials will include increasingly higher proportions of patients with CAR-T experience which is likely to affect the prognosis of these patients in a way that will make them non-comparable to trials conducted in the pre CAR-T era. While two trials published in 2021 reported that 10% of patients enrolled had prior CAR-T experience [7,8], recent R/R DLBCL trials reading out have reported substantial proportions (~40%) of patients enrolled with prior CAR-T experience [35–37].
Beyond comparability of studies on study design or population characteristics, differences in outcome assessment can also pose challenges for comparability. Included studies were heterogeneous with respect to response assessment criteria used and on the identity of the assessor (i.e., investigator vs IRC); furthermore, the timepoint of response assessment differed, with some studies reporting best ORR and others reporting EOT ORR. When these two estimates were reported for the same trial population, they showed significant variation.
The variations are particularly important considerations in clinical and healthcare decisions based on the comparisons of systemic therapies in R/R DLBCL patients ineligible for or experienced with transplant, where many of the trials are either single-arm or RCTs without a common comparator. Therefore, indirectly comparing efficacy results from these varied trials ought to use appropriate statistical techniques that take into account the differences in patient baseline characteristics across the trials [38]. Furthermore, naive indirect comparisons should be avoided as they are highly susceptible to biased assessment of comparative efficacy.
Limitations
The limited number of studies per regimen and the small sample sizes from most of the trials included is likely to have affected the robustness of the correlation coefficients exploring associations between ORR and patient baseline characteristics. Correlations were largely based on only three data points within each treatment regimen. However, our overall findings on the associations between baseline characteristics and ORR were in alignment with clinically reported prognostic factors in R/R DLBCL. In addition, several baseline characteristics of interest were not provided in all publications which limited our ability to provide a comprehensive analysis of their impact on ORR. Similarly, survival estimates were not consistently reported across trials, which prevented us from focusing on other efficacy measures. Furthermore, the limited number of studies and scant reporting of some of the end points undermined the ability to conduct multivariable assessments of the associations between patient baseline characteristics and all efficacy outcomes. These correlation analyses were not intended to be predictive and are not meant to be used in drawing firm conclusions about the relationships between these baseline characteristics and efficacy; rather, they are meant to give preliminary evidence that there are patterns of population characteristics and subsequent treatment outcomes.
Conclusion
The baseline characteristics of patients enrolled in trials evaluating the efficacy of guideline-recommended treatments for transplant-ineligible or -experienced R/R DLBCL varied widely across trials. Corresponding variations were also observed in reported efficacy outcomes from these trials. Across R/R DLBCL studies, findings indicate decreasing ORRs with higher median age of enrolled patients and with higher proportions of patients having: high-intermediate/high IPI risk, ECOG PS ≥2, prior treatment with rituximab/other anti-CD20 therapy, disease that is primary refractory and disease refractory to last LOT. Therefore, differences in the distributions of these patient baseline characteristics significantly contribute to the variability in efficacy reported across clinical trials investigating systemic therapies for R/R DLBCL and should be taken into consideration when evaluating and contextualizing treatment efficacy data.
•
Around half of patients with diffuse large B-cell lymphoma (DLBCL) relapse after or are refractory (R/R) to front-line immuno-chemotherapy.
•
Many patients with R/R DLBCL can be treated with autologous stem cell transplant (ASCT); optimal management when ASCT is not possible or fails has not been established and a variety of treatment regimens are available.
•
Among these regimes, direct comparative evidence is lacking, thus this study sought to synthesize outcomes from published clinical trials in this population and to explore the impact of variations in trial populations on overall response rate (ORR).
•
Among the 17 trials included in this systematic literature review, baseline characteristics varied widely across trials, particularly with regards to refractoriness to last line of therapy and patients' baseline International Prognostic Index (IPI), Ann Arbor stage and age.
•
Among studies reporting best ORR, rates were similar and highest in R-Benda and Pola + R-Benda treatment.
•
Across treatments, patients' age, IPI, prior exposure to ≥3 lines of therapy and in particular to rituximab / anti-CD20 mAb therapies, most frequently demonstrated correlations of at least moderate strength.
•
The limited number of trials evaluating each regimen and small sample sizes may have affected the robustness of the assessment of associations between ORR and patient baseline characteristics.
•
The widely varying baseline characteristics across trials was reflected in corresponding variations in reported efficacy outcomes from these trials; these variations should be taken into consideration when evaluating and contextualizing treatment efficacy data.
Author contributions
All authors contributed to the study conception, design and writing of the manuscript. Data analysis was performed by SD Miller and G Lozano-Ortega.
Acknowledgments
The authors thank the following for their help in the screening and data extraction of this systematic literature review: E Badillo, W Nyawade, L Hamadani, D Deighton, SA Raza and M Hughes. The authors also thank J Rodman and E Bone for their medical writing contributions.
Financial & competing interests disclosure
A Mutebi, B Elliott, O Briggs and A Kalsekar are employees of Genmab US. K Sail is an employee of AbbVie. SD Miller and G Lozano-Ortega are employees of Broadstreet HEOR, which was contracted by Genmab US for the conduct of this study. Josh Rodman and Emma Bone are employees of Apothecom which was contracted by Genmab US for medical writing support. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
SD Miller and G Lozano-Ortega (of Broadstreet HEOR) were contracted by Genmab US for the conduct of this study, including medical writing. Josh Rodman and Emma Bone (of Apothecom) were also contracted by Genmab US for additional medical writing support.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementary tables.docx)
- Download
- 41.51 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Cancer stat facts: common cancer types. https://seer.cancer.gov/statfacts/ (2022).
2.
Coiffier B, Lepage E, Briere J et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N. Engl. J. Med. 346(4), 235–242 (2002).
3.
Coiffier B, Thieblemont C, Van Den Neste E et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: a study by the Groupe d'Etudes des Lymphomes de l'Adulte. Blood 116(12), 2040–2045 (2010).
4.
B-Cell Lymphomas (Version 1.2022). www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf (2022).
5.
Tilly H, Gomes Da Silva M, Vitolo U et al. Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 26(Suppl. 5), v116–v125 (2015).
6.
Salles GA, Pettengell R, Cordoba R, Długosz-Danecka M, Jurczak W, Tilly H. Treatment of aggressive B-cell non-Hodgkin lymphoma beyond frontline therapy in patients not eligible for stem cell transplantation: a structured review. Leuk. Lymph. 60(7), 1610–1625 (2019).
7.
Caimi PF, Ai W, Alderuccio JP et al. Loncastuximab tesirine in relapsed or refractory diffuse large B-cell lymphoma (LOTIS-2): a multicentre, open-label, single-arm, Phase 2 trial. Lancet Oncol. 22(6), 790–800 (2021).
• This study is one of the most recent studies published in this population and the only study meeting our inclusion criteria that reported CAR-T in enrolled patients.
8.
Hutchings M, Mous R, Clausen MR et al. Dose escalation of subcutaneous epcoritamab in patients with relapsed or refractory B-cell non-Hodgkin lymphoma: an open-label, phase 1/2 study. Lancet 398(10306), 1157–1169 (2021).
9.
Thuresson P-O, Vander Velde N, Gupta P, Talbot J. A systematic review of the clinical efficacy of treatments in relapsed or refractory diffuse large B cell lymphoma. Adv. Ther. 37(12), 4877–489 (2020).
•• Highlighted the insufficiency of the published RCT data among transplant-ineligible DLBCL patients to establish the comparative efficacy of treatments via indirect treatment comparison and provided an impetus for this work.
10.
Sterne JaC, Savović J, Page MJ et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898 (2019).
11.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J. Surg. 73(9), 712–716 (2003).
12.
Schober P, Boer C, Schwarte LA. Correlation coefficients: appropriate use and interpretation. Anesth. Analg. 126(5), 1763–1768 (2018).
13.
El Gnaoui T, Dupuis J, Belhadj K et al. Rituximab, gemcitabine and oxaliplatin: an effective salvage regimen for patients with relapsed or refractory B-cell lymphoma not candidates for high-dose therapy. Ann. Oncol. 18(8), 1363–1368 (2007).
14.
Lopez A, Gutierrez A, Palacios A et al. GEMOX-R regimen is a highly effective salvage regimen in patients with refractory/relapsing diffuse large-cell lymphoma: a Phase II study. Eur. J. Haematol. 80(2), 127–132 (2008).
15.
Mounier N, El Gnaoui T, Tilly H et al. Rituximab plus gemcitabine and oxaliplatin in patients with refractory/relapsed diffuse large B-cell lymphoma who are not candidates for high-dose therapy. A Phase II Lymphoma Study Association trial. Haematologica 98(11), 1726–1731 (2013).
16.
Ohmachi K, Niitsu N, Uchida T et al. Multicenter phase II study of bendamustine plus rituximab in patients with relapsed or refractory diffuse large B-cell lymphoma. J. Clin. Oncol. 31(17), 2103–2109 (2013).
17.
Sehn LH, Herrera AF, Flowers CR et al. Polatuzumab vedotin in relapsed or refractory diffuse large B-cell lymphoma. J. Clin. Oncol. 38(2), 155–165 (2020).
• The pivotal trial supporting the approval of polatuzumab vedotin for R/R DLBCL; one of therapies for R/R DLBCL.
18.
Vacirca JL, Acs PI, Tabbara IA, Rosen PJ, Lee P, Lynam E. Bendamustine combined with rituximab for patients with relapsed or refractory diffuse large B cell lymphoma. Ann. Hematol. 93(3), 403–409 (2014).
19.
Terui Y, Rai S, Izutsu K et al. A Phase 2 study of polatuzumab vedotin + bendamustine + rituximab in relapsed/refractory diffuse large B-cell lymphoma. Cancer Sci. 112(7), 2845–2854 (2021).
20.
Abramson JS, Palomba ML, Gordon LI et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet 396(10254), 839–852 (2020).
21.
Neelapu SS, Locke FL, Bartlett NL et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-Cell lymphoma. N. Engl. J. Med. 377(26), 2531–2544 (2017).
• The pivotal trial supporting the approval of axicabtagene ciloleucel for R/R DLBCL; one of therapies for R/R DLBCL.
22.
Schuster SJ, Bishop MR, Tam CS et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N. Engl. J. Med. 380(1), 45–56 (2019).
• The pivotal trial supporting the approval of axicabtagene ciloleucel for R/R DLBCL; one of therapies for R/R DLBCL.
23.
Salles G, Duell J, Barca EG et al. Tafasitamab plus lenalidomide in relapsed or refractory diffuse large B-cell lymphoma (L-MIND): a multicentre, prospective, single-arm, Phase 2 study. Lancet Oncol. 21(7), 978–988 (2020).
24.
Kalakonda N, Maerevoet M, Cavallo F et al. Selinexor in patients with relapsed or refractory diffuse large B-cell lymphoma (SADAL): a single-arm, multinational, multicentre, open-label, phase 2 trial. Lancet Haematol. 7(7), e511–e522 (2020).
25.
Pettengell R, Dlugosz-Danecka M, Andorsky D et al. Pixantrone plus rituximab versus gemcitabine plus rituximab in patients with relapsed aggressive B-cell non-Hodgkin lymphoma not eligible for stem cell transplantation: a phase 3, randomized, multicentre trial (PIX306). Brit. J. Haematol. 188(2), 240–248 (2020).
26.
Zinzani PL, Pellegrini C, Gandolfi L et al. Combination of lenalidomide and rituximab in elderly patients with relapsed or refractory diffuse large B-cell lymphoma: a Phase 2 trial. Clin. Lymph. Myeloma Leuk. 11(6), 462–466 (2011).
27.
Harting R, Venugopal P, Gregory SA, O'Brien T, Bogdanova E. Efficacy and safety of rituximab combined with ESHAP chemotherapy for the treatment of relapsed/refractory aggressive B-cell non-Hodgkin lymphoma. Clin. Lymph. Myeloma 7(6), 406–412 (2007).
28.
Papageorgiou ES, Tsirigotis P, Dimopoulos M et al. Combination chemotherapy with gemcitabine and vinorelbine in the treatment of relapsed or refractory diffuse large B-cell lymphoma: a phase-II trial by the Hellenic Cooperative Oncology Group. Eur. J. Haematol. 75(2), 124–129 (2005).
29.
Sehn LH, Hertzberg M, Opat S et al. Polatuzumab vedotin plus bendamustine and rituximab in relapsed/refractory diffuse large B-cell lymphoma: updated results of a phase Ib/II randomized study and preliminary results of a single-arm extension. Blood 136(Suppl. 1), 17–19 (2020).
30.
Cheson BD, Horning SJ, Coiffier B et al. Report of an international workshop to standardize response criteria for non-Hodgkin's lymphomas. NCI Sponsored International Working Group. J. Clin. Oncol. 17(4), 1244 (1999).
31.
Cheson BD, Fisher RI, Barrington SF et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J. Clin. Oncol. 32(27), 3059–3068 (2014).
32.
Cheson BD, Pfistner B, Juweid ME et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 25(5), 579–586 (2007).
33.
Lin TL, Kuo MC, Shih LY et al. The impact of age, Charlson comorbidity index, and performance status on treatment of elderly patients with diffuse large B cell lymphoma. Ann. Hematol. 91(9), 1383–1391 (2012).
34.
Crump M, Neelapu SS, Farooq U et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood 130(16), 1800–1808 (2017).
•• SCHOLAR-1 is the largest patient-level pooled analysis of response rates among patients with refractory DLBCL ant the results provide context for the findings of this review.
35.
Bannerji R, Arnason JE, Advani RH et al. Odronextamab, a human CD20×CD3 bispecific antibody in patients with CD20-positive B-cell malignancies (ELM-1): results from the relapsed or refractory non-Hodgkin lymphoma cohort in a single-arm, multicentre, phase 1 trial. Lancet Haematol. 9(5), e327–e339 (2022).
36.
Dickinson M, Carlo-Stella C, Morschhauser F et al. Glofitamab in patients with relapsed/refractory (R/R) diffuse large B-cell lymphoma (DLBCL) and ≥2 prior therapies: pivotal Phase II expansion results. J. Clin. Oncol. 40(Suppl. 16), 7500–7500 (2022).
37.
Thieblemont C, Phillips T, Ghesquieres H et al. Primary results of subcutaneous epcoritamab dose expansion in patients with relapsed or refractory large B-cell lymphoma: a Phase 2 study. Presented at: The European Hematology Association Congress (2022).
38.
National Institute for Health and Care Excellence. Tisagenlecleucel for treating relapsed or refractory diffuse large B-cell lymphoma after 2 or more systemic therapies (TA567). Technology appraisal guidance. Available at: www.nice.org.uk/guidance/ta567 (2019).
Information & Authors
Information
Published In
Copyright
© 2022 The Authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 August 2022
Accepted: 4 November 2022
Published online: 23 November 2022
Keywords:
Topics
Authors
Funding Information
Genmab US Inc
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Systematic review of outcomes and patient heterogeneity in relapsed or refractory diffuse large B-cell lymphoma. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0146
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Hanzala Ahmed Farooqi, Muhammad Saffi Ullah, Ahmed Raza, Zain Sadiq, Wardah Ali Shaikh, Rahmah Muhammad, Muhammad Shoaib Hussain, Efficacy and safety of polatuzumab-vedotin plus bendamustine and rituximab in patients with relapsed/refractory diffuse large B-cell lymphoma: A systematic review and meta-analysis, Critical Reviews in Oncology/Hematology, 10.1016/j.critrevonc.2024.104611, 207, (104611), (2025).
- Chandler Gandy, Shadi Bazzazzadehgan, Sebastian Bruera, Yinan Huang, Evaluation of Real-World Evidence to Assess Effectiveness Outcomes of Janus Kinase Inhibitors for Rheumatoid Arthritis: A Systematic Review of US Studies, Drug, Healthcare and Patient Safety, 10.2147/DHPS.S492887, Volume 17, (25-49), (2025).
- Jiahui Pan, XueNing Chen, Nianming Ban, JiaShao He, Jiayi Chen, Haiyun Huang, Advances in P300 brain–computer interface spellers: toward paradigm design and performance evaluation, Frontiers in Human Neuroscience, 10.3389/fnhum.2022.1077717, 16, (2022).