Effect of home-based exercise programs with e-devices on falls among community-dwelling older adults: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To explore the effectiveness of home-based exercise programs with e-devices (HEPEs) on falls among community-dwelling older adults. Methods: Twelve randomized controlled trials were included in the meta-analysis considering four fall-related outcomes. Results: HEPEs significantly reduced the rate of falls (risk ratio: 0.82; 95% CI: 0.72–0.95; p = 0.006) and improved lower extremity strength (mean difference: -0.94; 95% CI: -1.71 to -0.47; p < 0.001). There was a significant improvement favoring HEPEs on balance if the participants were aged >75 years (mean difference: -0.55; 95% CI: -1.05 to -0.05; p = 0.03), or the intervention duration was at least 16 weeks (mean difference: -0.81; 95% CI: -1.58 to -0.05; p = 0.04). Conclusion: HEPEs demonstrated an overall positive effect on falls among community-dwelling older adults.
Falls among older people are a worldwide public health issue. Almost one in three community-dwelling people who are aged 65 years or older will fall at least once per year [1], and the risk of falling increases to one in two adults per year among those aged 80 years or older [2]. Furthermore, fall-related injuries are the leading causes of death and disability among older adults [3]. According to the data, 40% of all kinds of injury-related deaths and over 80% of all injury admissions to hospital are caused by falls [4].
To reduce the rate of falls, many fall prevention interventions have been established and evaluated. For instance, home modification is effective in persons at higher risk for falling, including those with vision impairment [5,6]; medication reduction or withdrawal is stressed for all older people [7]; and assessment and treatment of postural hypotension should also be included for older adults [8].
In fact, it is worth noting that intervention including physical exercises is proved to be the most effective [9,10]. In other words, exercise intervention is an efficient and cost-effective way to reduce the risk of falls [11]. Strong evidence shows that exercise-based intervention can reduce falls through improving gait ability [12], balance [12,13], strength [14,15], endurance [14,16], psychosocial health [15,17] and bone metabolism [16,18]. In order to achieve these benefits, different forms of exercises have been developed and proved, mainly including physical therapy [19,20], tai chi [21], yoga [22] and group and home-based exercise programs [23]. Another review reported that group and home-based exercise programs are not only conducive to reduce the rate of falls and risk of falling, but also more suitable for most of the older people in the community compared with the others [24]. Evidence demonstrates that home-based strength and balance training programs are able to reduce falls in community-dwelling people who are at least 75 years old [25–27]. It has also been proved that implementing a personalized intervention for older adults is helpful to improve the gait speed and reduce the risk of falls [28,29]. Therefore a personalized home-based exercise program is a promising way to meet the needs of older people with different health conditions [30–32].
According to the review by Sherrington et al., a larger dose and longer intervention time lead to a better effect for the old [33]; therefore adherence to the exercise program is significant. Researchers used to utilize paper-based booklets [34], multiple home visits [35–37] or telephone calls [38] to help the older people stick to the program. While these methods may be helpful, a better intervention can further improve adherence among older through providing supervision or making the exercise more engaging and accessible [39]. The use of e-devices, including mobile phones, tablets or personal computers, may be a promising approach [40]. For example, the majority of commercially available gaming technology, as known as exergaming, used in supervised interventions, led to a high adherence [41]. Silveira et al. evaluated the effect of a tablet-based exercise application compared with a brochure-based program over 12 weeks [42,43]. The result demonstrated a higher adherence for the application programs than the paper program. Similarly, the Test-and-Exercise program allows participants to establish their own exercise plans by using a mobile application, which also showed a positive effect in fall prevention in elderly people due to better adherence [34].
Recently, the COVID-19 pandemic has negatively affected individuals’ lives. In order to decelerate the spread of COVID-19, social distancing and quarantine protocols have been established [44]. During quarantine, isolation affects the physical [45,46] and mental [47] health of the elderly. In this circumstance, medical workers should consider setting up a better way to provide answers and direction to the old based on home-based exercises [46]. With the development and generalization of e-devices, this can be a good solution because there is no need to travel a long distance to conduct a home visit for the professionals. Participants can engage in the home-based program at any time without extra labor cost or facing any risks of the pandemic [44,48].
To summarize from the current evidence, a home-based exercise program with e-devices (HEPE) can improve the participants’ adherence, reduce the harm of epidemic exposure and save the medical workers’ labor cost. However, to our knowledge, there is no meta-analysis evidence on the effects of HEPE in community-dwelling older adults. So, due to the growing importance of fall prevention and the pressure from COVID-19, the aim of this systematic review (SR) and meta-analysis was to assess the effects of HEPEs in community-dwelling older adults.
Materials & methods
This SR followed the Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) [49]. In order to prevent duplication of reviews, a search for previous and ongoing SRs similar to this study was conducted.
Search strategy
Eight online databases were searched for published works which were published until May 2022, namely: PubMed, Cochrane, CINAHL, Scopus, Ovid MEDLINE, ScienceDirect, Web of Science and Embase. In addition, ongoing and unpublished trials were searched in the Cochrane Controlled Register of Trials. The complete search strategy is summarized in Supplementary Table 1. Later, a manual search of relevant randomized controlled trials (RCTs) from reference lists was carried out, producing three additional relevant records. All the mentioned articles were written in English.
Eligibility criteria
The eligibility criteria were strictly established according to the PICOS (population, intervention, comparison, outcome and study design) framework (Table 1) [50]. The target population was older adults (aged at least 60 years) who could participate in home-based exercises after professional evaluation, living independently in communities [51]. Because of the differences in life expectancy, the definition of older adults varies from country to country. According to WHO, in most regions of the world the rates of fall-related fatalities are highest among adults over the age of 60 years [52]. Therefore we used community-dwelling adults aged 60 years or over as the target population. Interventions included HEPE alone or in combination with other multifactorial interventions. The content of the HEPE should be acceptable, feasible and safe for the elderly (including but not limited to the following: simple balance training, strength training with moderate resistance or modified comprehensive training). Meanwhile, taking the variable physical level of the elderly into consideration, the exercise programs should also be personalized or under remote supervision by professionals. Comparison included standard physiotherapy or traditional home-based exercise (including group-based exercise classes, telephone call-based exercises, home visit-based exercises or booklet-based exercises), usual medical care or no intervention. Eligible studies should contain at least one of the following outcomes: the risk or rate of falls, balance ability, lower extremity strength, cognition function, severity of falls and fear of falling. Study design should meet the standard of a RCT [53].
| Category | Inclusion criteria | Exclusion criteria |
|---|---|---|
| Population | Elder adults aged at least 60 years old who could participate in home-based exercises after evaluation, living independently in communities | Studies involving participants with a diagnosis of chronic disease (e.g., multiple sclerosis, cancer, Parkinson’s or Alzheimer’s disease) |
| Intervention | Mobile phone, tablet, personal computer and home-based exercise program, either alone or in combination with other multifactorial interventions | Exercises not performed at home (e.g., group-based exercise classes), or home-based exercises without any e-device (e.g., telephone call-based exercises, home visit-based exercises or booklet-based exercises) |
| Comparison | Standard physiotherapy or traditional home-based exercise, usual medical care or no intervention | Lack of control group |
| Outcome | To contain at least one of: risk or rate of falls, balance ability, lower extremity strength, cognition function, quality of life, severity of falls and fear of falling | Did not contain any required outcomes, absence of baseline or follow-up data |
| Study design | Randomized controlled trial | Non-randomized controlled trial |
Selection process
In this SR, the selection process was guided by the PRISMA flow diagram [50]. All articles identified from the searches were exported to EndNote v.20, and duplicates were removed automatically. The remaining articles were screened manually using the titles and abstracts. The verification of eligibility of the selected articles was done using the study titles and abstracts. Next, full texts were downloaded. Studies with inappropriate populations, interventions, comparisons and outcomes were excluded. Finally, the included studies were assessed on their suitability for meta-analysis. The number of studies included and excluded at each step and the reasons for exclusion are listed in the PRISMA diagram (Figure 1).

Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart for selection of papers.
RCT: Randomized controlled trial.
Quality assessment
The quality assessment was carried out by two raters based on the Physiotherapy Evidence Database (PEDro) scale [54,55]. This is a rating scale to assess the methodological quality of clinical trials which consists of 11 items encompassing external validity. A total score is reached by adding the ratings of items 2 to 11 for a final score of 0–10. Its authors have suggested that a PEDro score of <4 should be considered ‘poor’, 4 or 5 should be considered ‘fair’, 6–8 should be considered ‘good’ and 9 or 10 can be considered ‘excellent’ [56]. A third rater then resolved any potential disagreement.
Data extraction
The following data from each study were extracted: basic information and publication details; participants’ characteristics; intervention characteristics; comparison characteristics; and outcome measurements. When there was a missing or inconsistent outcome because of the heterogeneity of the study designs, a narrative synthesis approach was performed to examine the results, rather than a meta-analysis. Dichotomous data (fall rate during the follow-up period) and quantitative data (including the result of timed up and go [TUG], five-times sit-to-stand test [FTSST] and physiological profile assessment [PPA]) extracted were then entered into Review Manager (v. 5.3; the Cochrane Collaboration, Oxford, UK) for meta-analysis.
Data synthesis
All statistical analyses were performed with Review Manager v. 5.3. Heterogeneity was initially explored through visual inspection of the forest plots, then a test for statistical heterogeneity was carried out using the I2 and χ2 test. A p-value of < 0.05 was considered to be statistically significant. According to the percentage of I2, values greater than 50% are considered to represent substantial heterogeneity. When this occurred, we attempted to explain the cause of the variation. If the value was less than 30%, the overall estimate was produced by a fixed-effects model. Otherwise, a random-effects model was used, for which the CIs are broader than those of a fixed-effects model [57]. Stability and publication bias were tested by a one-study leave-out sensitivity analysis.
Results
Studies’ characteristics
A total of 4198 records were gathered from various databases, and three additional articles were found by hand-searching. After automatically removing the duplicates, 2231 records were kept. Then a screening according to the title and abstract was carried out by three independent authors, from which 2002 records were excluded. Finally, 229 records with corresponding full texts were further screened judging by the eligibility criteria; 12 studies (participants n = 1648) met all of the inclusion criteria and were included in the meta-analysis. The main reasons for exclusion are listed in the PRISMA diagram (Figure 1). The characteristics of the included studies are summarized in Table 2. The average age of the participants ranged from 70.22 to 85.2 years and all of them were community-dwelling older adults. The HEPEs were all personalized according to each participant’s fitness level by the professionals. The interventions required 2–7 days per week (or 60–120 min per week) and lasted from 6 weeks to 24 months. According to most of the exercise programs, 30 min per day is an average intervention intensity.
| Study (year) | Participants | Interventions | Comparison | Main outcomes | Ref. | |||
|---|---|---|---|---|---|---|---|---|
| Duration | Frequency | Modality | E-devices used | |||||
| Rosie et al. (2007) | E-device group (n = 33, mean age [years] = 85.2); control group (n = 33, mean age [years] = 85.1) | 6 weeks | 7 days/week | Home-based sit-to-stand exercises | GrandStand System (a pressure cushion with a biofeedback monitor attached connecting to a tablet) | Knee extension exercises | Gait speed; chair stand (repetitions); BBS; modified falls efficacy scale; late-life function and disability instrument | [58] |
| Haines et al. (2009) | E-device group (n = 19, mean age [years] = 80.9); control group (n = 34, mean age [years] = 80.5) | 6 months | 7 days/week | ‘Kitchen Table Exercise Program’ combining lower limb strength and balance exercises | DVD player | No intervention | Health-related quality of life; FAI; BOOMER; 15-s chair stand test; fear of falling; activity-specific balance confidence scale | [59] |
| Schoene et al. (2013) | E-device group (n = 15, mean age [years] = 77.5); control group (n = 17, mean age [years] = 78.4) | 8 weeks | 2–3 days/week | Step game based on the open-source DDR game Stepmania | A computer unit and step pad | No intervention | Choice stepping reaction time; PPA; TUG; FTSST; alternate step test | [60] |
| Gschwind et al. (2015) | E-device group (n = 78, mean age [years] = 74.7); control group (n = 75, mean age [years] = 74.7) | 16 weeks | ≥3 days/week | Comprehensive home-based exercise program including strength training and balance training exercises | The iStoppFalls program (including a PC, a Google TV set-top box, a senior mobility monitor and a Nexus 7 Android tablet) | Received an evidence-based educational booklet about general health and fall prevention | Melbourne edge test; peripheral sensation; balance; lower extremity muscle strength; hand reaction time; EQ-5D | [31] |
| Gschwind et al. (2015) | E-device group 1 (n = 24, mean age [years] = 80.1); e-device group 2 (n = 39, mean age [years] = 82.5); control group (n = 61, mean age [years] = 80.2) | 16 weeks | E-device group 1: 120 min for balance and 60 minutes for strength/week; e-device group 2: 60 min/week | E-device group 1: KIN exergames (including balance and strength exergames); e-device group 2: SMT system (targeting specific cognitive functions associated with fall risk and stepping) | KIN and SMT systems (contained an input device, a computer, universal serial bus modems and participants’ TVs) | Received an evidence-based educational booklet about health and fall prevention advice | Melbourne Edge Test; a lower limb-matching task; quadriceps strength; finger-press reaction time; postural sway | [61] |
| Boongird et al. (2017) | E-device group (n = 219, mean age [years] = 74.08); control group (n = 220, mean age [years] = 73.94) | 12 months | 120 min/week | Modified Otago exercise program including lower extremities strengthening, stretching and balance training | Video disk recorder | Only received fall prevention education | Number of reported falls; BBS; FTSST; TUG; Thai FES-I; Thai EQ-5D | [62] |
| Hong et al. (2018) | E-device group (n = 10, mean age [years] = 78.1); control group (n = 13, mean age [years] = 81.5) | 12 weeks | 3 days/week | Supervised, progressive exercise including warm-up, main exercise and cool-down activity | Web real-time communication technology based on a tablet PC | No intervention | The senior fitness test; BBS; falls efficacy; fear of falling | [63] |
| Shake et al. (2018) | E-device group (n = 60, mean age [years] = 73.59); control group (n = 45, mean age [years] = 73.22) | 10 weeks | 2 days/week | Special exercises program including cardiovascular/ balance, strength and flexibility exercises | Experimenter-provided tablets or Digiland 16GB Tablets with an app installed | Only received health education | Short performance physical battery; EXAMINER cognitive battery; health knowledge performance | [64] |
| Delbaere et al. (2021) | E-device group (n = 254, mean age [years] = 77.1); control group (n = 249, mean age [years] = 77.7) | 24 months | 120 min/week | Static balance and dynamic balance training exercises and the Standing Tall education program | Tablet PC | Only received the Standing Tall education program | Number of fallers and falls rate; static balance measures; maximal balance range test; TUG; sit-to-stand test; walking speed; stepping performance; cognitive performance and executive function; psychological assessment; health-related quality of life; physical activity levels | [65] |
| Li et al. (2021) | E-device group (n = 15, mean age [years] = 76.13); control group (n = 15, mean age [years] = 76.2) | 24 weeks | 2 days/week | Zoom-based online classes including progressive core training, interactive cognitive–physical exercises | PC, iPad or smartphone | Stretching exercises | Incidence of falls; number of fallers; four-stage balance test; 30-s chair stands; TUG | [66] |
| Yerlikaya et al. (2021) | E-device group (n = 18, mean age [years] = 70.22); control group 1 (n = 16, mean age [years] = 71.81); control group 2 (n = 16, mean age [years] = 75.62) | 8 weeks | 3 days/week | Online exercise classes via video access platforms such as WhatsApp and Google Meet | PC, tablet or smartphone | Control group 1: the same exercises but without supervision; control group 2: no intervention | BBS; TUG; Sway Balance mobile application; TAI; WHL | [67] |
| Yi et al. (2021) | E-device group (n = 35, mean age [years] = 76.11); control group (n = 35, mean age [years] = 77.31) | 8 weeks | 2 days/week | Comprehensive exercise program including warm-up, main exercise and cool-down exercises | Smartphone | No intervention | Geriatric depression scale; FTSST; handgrip strength; 10-m walk test; gait analysis; TUG; postural sway test | [44] |
BBS: Berg balance scale; BOOMER: Balance Outcome Measure for Elder Rehabilitation; DDR: Dance Dance Revolution; FAI: Frenchay Activities Index; FES-I: Fall Efficacy Scale – International; FTSST: Five-times sit-to-stand test; KIN: Microsoft Kinect®; PC: Personal computer; PPA: Physiological profile assessment; SMT: Step-mat training; TAI: Trait anxiety inventory; TUG: Timed up and go; WHL: WHO quality of life instrument (older adults module).
Quality assessment
The overall quality of the included studies could be considered as good (PEDro score: 6.83; range: 5–9; Table 3). None of the studies showed poor methodological quality. Only one study got 5 points, which should be considered as ‘fair’; besides that, ten studies had good quality and one study had excellent quality.
| Study (year) | Items | Total score† | Ref. | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Rosieet al. (2007) | + | + | – | + | + | – | – | + | + | + | + | 7 | [58] |
| Haineset al. (2009) | + | + | + | + | + | – | + | + | + | + | + | 9 | [59] |
| Schoene et al. (2013) | + | + | + | + | – | – | + | + | – | + | + | 7 | [60] |
| Gschwind t al. (2015) | + | + | + | + | + | – | – | + | + | + | + | 8 | [31] |
| Gschwind et al. (2015) | + | + | – | + | – | – | + | + | + | + | + | 7 | [61] |
| Boongird et al. (2017) | + | + | + | – | – | – | + | + | + | + | – | 6 | [62] |
| Hong et al. (2018) | + | + | – | – | – | – | + | + | + | + | + | 6 | [63] |
| Shake et al. (2018) | + | + | – | – | + | – | + | + | – | + | + | 6 | [64] |
| Delbaere et al. (2021) | + | + | + | + | – | – | + | + | + | + | + | 8 | [65] |
| Li et al. (2021) | + | + | + | – | – | – | + | + | + | + | + | 7 | [66] |
| Yerlikaya et al. (2021) | + | + | + | – | – | – | – | + | + | + | + | 6 | [67] |
| Yi et al. (2021) | + | + | – | – | – | – | – | + | + | + | + | 5 | [44] |
†
Total score is achieved by adding the ratings of items 2–11 for a combined total score between 0 and 10.
The column numbers correspond to the following criteria on the PEDro scale: 1 – eligibility criteria were specified; 2 – subjects were randomly allocated to groups; 3 – allocation was concealed; 4 – the groups were similar at baseline regarding the most important prognostic indicators; 5 – there was blinding of all subjects; 6 – there was blinding of all therapists who administered the therapy; 7 – there was blinding of all assessors who measured at least one key outcome; 8 – measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups; 9 – all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome were analyzed by ‘intention to treat’; 10 – the results of between-group statistical comparisons were reported for at least one key outcome; 11 – the study provided both point measures and measures of variability for at least one key outcome. + indicates the criterion was satisfied; – indicates that the criterion was not satisfied.
PEDro: Physiotherapy Evidence Database.
Effect of HEPE on proportion of fallers
Among the 12 included studies, six reported the proportion of fallers, while the remaining six did not mention any information about the proportion of fallers or rate of falls in the end point measurements. Therefore, a total of 1242 participants were included in the meta-analysis (Figure 2). The proportion of fallers is defined as the ratio of fallers to the total number of participants. The data were generally collected during the interventions or the follow-up period through a self-report method. A lower risk ratio indicates a reduced rate of falls. The pooled effect of HEPEs in reducing the proportion of fallers is statistically significant (risk ratio [RR]: 0.82; 95% CI: 0.72–0.95; Z = 2.11; p = 0.006), favoring HEPE groups to control groups, as determined by the fixed-effects method. Meanwhile, the heterogeneity tests indicated that nonheterogeneity was found across the six studies (I2 = 0%; χ2 = 2.20; p = 0.82).
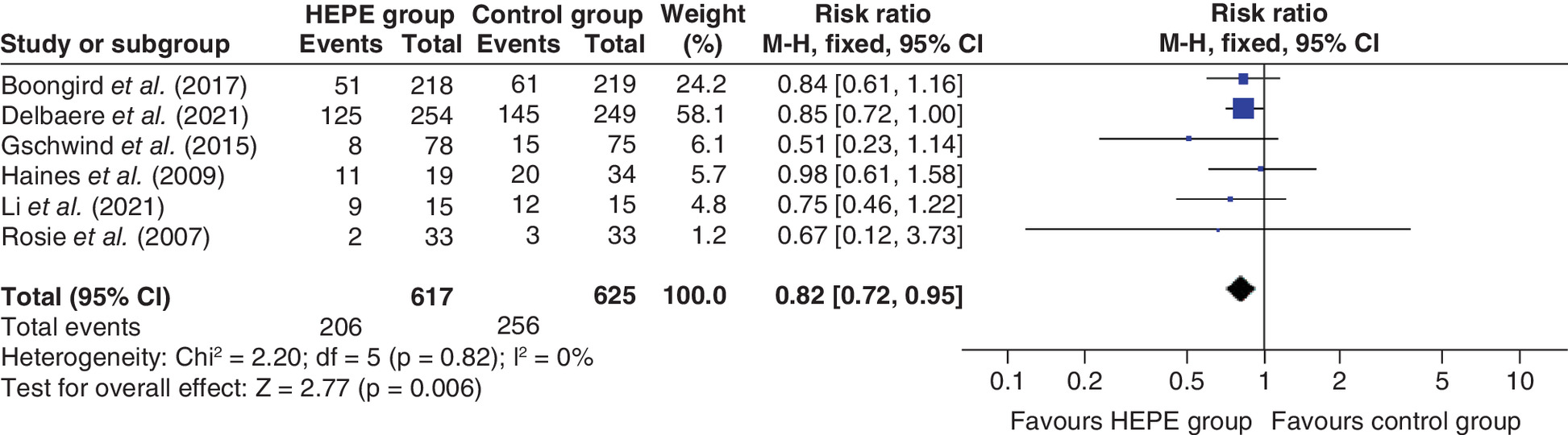
Figure 2. Forest plot of the effect of home-based exercise programs with e-devices on proportion of fallers.
HEPE: Home-based exercise program with e-device; M–H: Mantel–Haenszel statistical method.
Effect of HEPE on balance
Seven studies utilized the TUG test to estimate the balance of the participants, which were pooled in meta-analysis by a random-effects model.
TUG is a simple and widely used test of overall functional mobility, assessing the individual’s ability to transfer, walk and change direction [68]. According to the results from TUG, a shorter time taken to complete the whole test indicates better balance and functional performance [69]; therefore we took TUG as the index of balance in the meta-analysis with 865 participants included (Figure 3A). The HEPE group showed an improvement trend in balance, but without statistical significance (MD: -0.71; 95% CI: -1.47 to 0.05; Z = 1.83; p = 0.07).

Figure 3. Forest plot of the effect of home-based exercise programs with e-devices on balance.
(A) The pooled effect of HEPEs on balance. (B) The result of subgroup analysis on different ages of the participants. (C) The result of subgroup analysis on different intervention durations.
HEPE: Home-based exercise program with e-device; IV: Inverse variance statistical method; SD: Standard deviation.
Three studies (Rosie et al. [58], Boongird et al. [62] and Hong et al. [63]) used the Berg balance scale (BBS) to measure balance in the elderly. The scale consists of 14 items, scored from 0 to 4, which are added to make a total score between 0 and 56 [70]. Evidence has shown that total scores below 45 are associated with a higher risk of falls; an individual with a history of falls and a total score below 51 is highly predictive of falls; a score of less than 40 is associated with a fall risk of almost 100% [71]. Rosie et al. reported that the HEPE group had a significant within-group improvement in BBS score (mean improvement 1.67 ± 2.64 points; p = 0.001) compared with the control group [58]. Hong et al. further proved a significant interaction effect between group and time regarding the scores of BBS (p = 0.03) [63]. According to Boongird et al., the result from BBS did not show a significant improvement for the HEPE group, but maintained a fair level compared with the control group (p = 0.258) [62]. Haines et al. utilized the Balance Outcome Measure for Elder Rehabilitation to test the balance, but no statistical significance was found in their study [59]. Shake et al. [64] used the Short Physical Performance Battery in the study, which is a well-established tool to assess lower extremity muscular strength, agility and dynamic balance [72]; the composite scores of the entire battery showed only a main effect of time (F1,83 = 13.86; p < 0.001) [64].
Of note, two studies (Schoene et al. [60] and Li et al. [66]) conducted a dual-task TUG test as well; this is a modified TUG test combined with cognitive-related dual tasks. Previous research has shown that dual-task TUG may have an added value for fall prediction over TUG [73,74]. Schoene et al. found that the HEPE group improved significantly in the dual-task TUG test (F31,1 = 4.226; p = 0.049) [60]. A similar result was also shown in another study (mean difference [MD]: -2.35; p < 0.001) [66].
Meanwhile, there was high heterogeneity across the seven studies included in the meta-analysis (I2 = 80%; χ2 = 30.50; p < 0.001). The heterogeneity could be caused by different ages of the participants or the intervention duration. Thus a subgroup analysis was conducted to explain the heterogeneity.
Effect of HEPE on balance: grouping by different ages
Firstly, a subgroup analysis was carried out to investigate the influence of different ages of the participants. According to the mean ages of the participants from the included studies, we divided them into two groups: the over-75 years group (n = 2) and the under-75 years group (n = 5). There was no significant subgroup difference in MD (χ2 = 0.53; p = 0.47) across the two groups. The results indicated that the age of the participants was not the cause of the heterogeneity. Of note, a huge heterogeneity was found in the under-75 years group, and no statistically significant difference was found (MD: -3.21; 95% CI: -10.39 to 3.96; Z = 0.88; p = 0.38). Meanwhile, there was a statistically significant difference (MD: -0.55; 95% CI: -1.05 to -0.05; Z = 2.17; p = 0.03) in the over-75 years group with a fair heterogeneity (I2 = 49%; χ2 = 7.86; p = 0.10) (Figure 3B).
Effect of HEPE on balance: grouping by intervention duration
Given that the intervention duration varied greatly among studies, another subgroup analysis was then conducted. Similarly, the studies were divided into three groups based on the intervention duration: 0–8 weeks (n = 3), 8–16 weeks (n = 2) and >16 weeks (n = 2). Again, there was no significant subgroup difference in MD (χ2 = 4.47; p = 0.11) across the three groups. However, the p-value was less than the one in the age-based subgroup analysis. Relatively speaking, the result could partly explain the heterogeneity. Of note, the >16 weeks group showed a significantly improved balance (MD: -0.81; 95% CI: -1.58 to -0.05; Z = 2.09; p = 0.04), while the 0–8 (MD: -1.77; 95% CI: -4.01 to 0.47; Z = 1.55; p = 0.12) and 8–16 weeks groups (MD: 0.15; 95% CI: -0.63 to 0.93; Z = 0.38; p = 0.71) did not (Figure 3C).
Effect of HEPE on lower extremity strength
Six studies reported the changes of lower extremity strength by FTSST. Previous studies have proved the excellent reliability and validity of FTSST to assess sitting and standing performance and lower limb strength [75] in both healthy adults and those with pathologies [76,77]. The improvement of HEPE on lower extremity strength is significant (MD: -0.94; 95% CI: -1.71 to -0.47; Z = 3.93; p < 0.001) as determined by a random-effects model. The MDs ranged from -1.34 [64] to 0.40 [60]. A heterogeneity test suggested a fair heterogeneity across the studies (I2 = 42%; χ2 = 8.60; p = 0.13) (Figure 4).
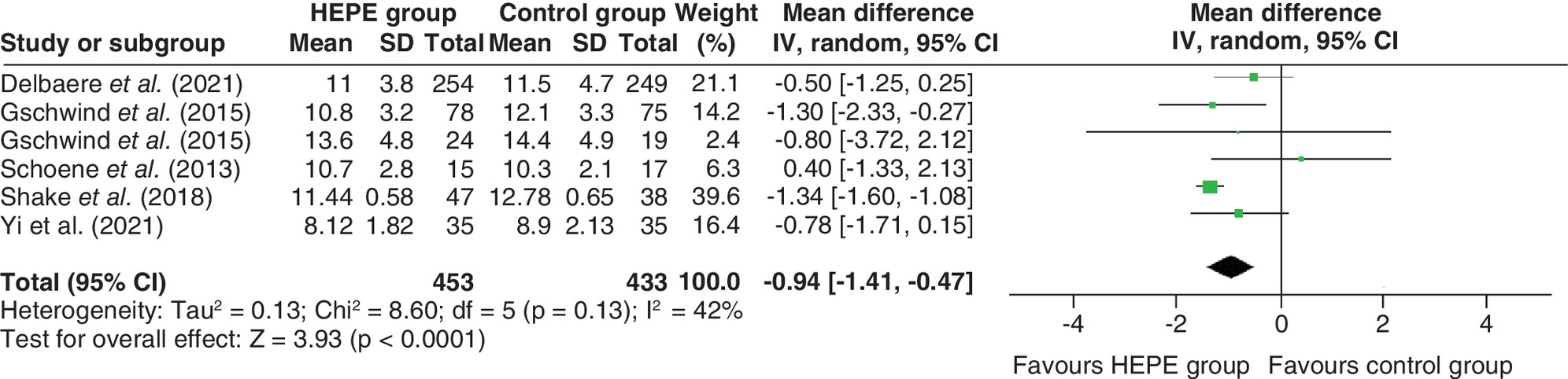
Figure 4. Forest plot of the effect of home-based exercise programs with e-devices on lower extremity strength.
HEPE: Home-based exercise program with e-device; IV: Inverse variance statistical method; SD: Standard deviation.
Effect of HEPE on fall risk & fall efficacy
Physiological fall risk was estimated using the PPA in four studies. PPA involves a series of simple tests of vision, peripheral sensation, muscle force, reaction time and postural sway, and is a useful tool in quantifying fall risks [78,79]. According to the meta-analysis results, there was no statistical significance (MD: -0.22; 95% CI: -0.46 to 0.01; Z = 1.90; p = 0.06) across the included studies with 731 participants involved, but the overall trend favored the HEPE groups. Meanwhile, a fair heterogeneity existed across the studies (I2 = 48%; χ2 = 5.73; p = 0.13) (Figure 5).
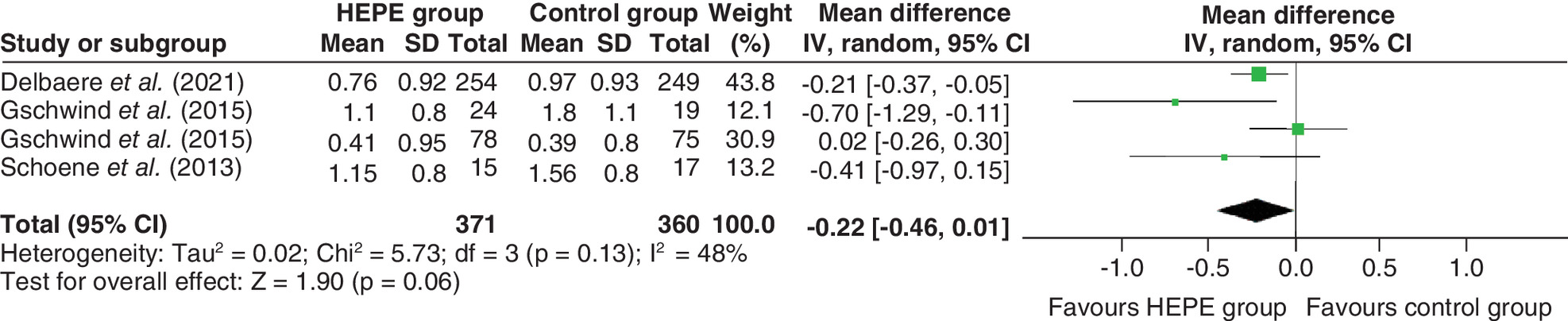
Figure 5. Forest plot of the effect of home-based exercise programs with e-devices on fall risk.
HEPE: Home-based exercise program with e-device; IV: Inverse variance statistical method; SD: Standard deviation.
The fall risk could also be measured by fall efficacy, which is related to the level of fear of falling. According to previous studies, various kinds of fall efficacy scales have been developed and proved to be accurate in predicting physiological fall risks [80]. Rosie et al. reported the fall efficacy by the modified falls self-efficacy scale, from which no statistical difference was found either in-group (p = 0.393) or between-group (p = 0.818) [58]. Haines et al. measured the fall efficacy by the activities-specific balance confidence scale [59]. Similarly, a negative result was found, according to a linear regression analysis (regression coefficient = -0.30; 95% CI: -1.49 to 0.89; p = 0.61) [59]. Boongird et al. applied the Thai fall efficacy scale to measure the fall efficacy in their trial and found that fall efficacy improved significantly in the HEPE group at the 6-month follow-up (p = 0.003) [62]. According to Hong et al., there were no changes in falls efficacy in either activities of daily living (p = 0.55) or social activities (p = 0.51) by means of the Korean falls efficacy scale [63]. However, the additional measurement of fear of falling, assessed through a fear of falling questionnaire, was carried out in their study and revealed a significant interaction effect between group and time (p = 0.009). The HEPE group showed a better fall efficacy than the control group (p = 0.008).
Discussion
This SR was carried out in the context of: the importance of fall prevention among community-dwelling older adults; the labor cost of medical workers; a shortfall in adherence of home-based exercise programs; and the special needs caused by the COVID-19 pandemic. The SR and meta-analysis was aimed at the home-based exercise program with e-devices which showed a better adherence compared with traditional home-based exercise programs [40]. We investigated the effectiveness of personalized HEPEs on the proportion of fallers, balance, lower extremity strength and fall risks.
Effectiveness of HEPE
The fall risk in the HEPE group was significantly decreased, by 18% (RR: 0.82; 95% CI: 0.72–0.95) compared with the controls according to the changes in the proportion of fallers. Notably, a previous review indicated that balance and functional exercises reduced the rate of falls by 24% (RR: 0.76; 95% CI: 0.70–0.81), while multiple types of exercise (most commonly balance and functional exercises plus resistance exercises) reduced the rate by 34% (RR: 0.66; 95% CI: 0.50–0.88) [51]. This result suggests that HEPEs may be more effective in reducing the fall rate if multiple types of exercise are applied.
Our findings suggested that the overall effect of HEPEs was not significant in improving balance as measured by TUG. A previous review indicated that elderly adults showed an age-related decline in balance and gait with increased gait variability and an associated increased risk of falls [81]. Considering that age is one of the factors that may affect the balance and intervention effect, a subgroup analysis was then carried out; we found that balance was significantly improved when the average age of involved participants was over 75. Of note, the traditional home-based interventions seemed to have limited impact on balance improvement in older adults (aged over 75). For example, a RCT enrolled 64 subjects whose average age was 75.9 years; after 15 weeks of home-based exercise, no significant improvement was found in balance as measured by TUG (p = 0.90) [82]. Therefore this is an exciting finding, because HEPE could be a more suitable intervention for older adults compared with the traditional home-based programs. On the one hand, the HEPEs took advantage of the better adherence brought by e-devices. As previous studies have shown, 67% of participants using the digital program continued to exercise regularly compared with 35% for the paper booklet (p = 0.036) [83]. Similarly, a RCT comparing adherence to laboratory-based trials using a supervised e-device versus traditional home-based trials yielded similar results [39]. Therefore a digital program was able to facilitate long-term maintenance of regular exercise so as to bring about a better curative effect on balance. On the other hand, as all the HEPEs involved were individually tailored, the exercise programs fitted the functional level of the elderly well. Evidence has shown that tailored exercise programs cause significant improvements in balance compared with fixed ones [84]. For example, in the study of Rosie et al., the results showed a significant within-group improvement in balance in the HEPE group (p = 0.001), while no change was revealed in the control group performing knee extension (p = 0.258) [58]. This aligned with another SR which found that individualized home-based exercise programs promoted autonomy and were therefore seen as superior to generic fall-prevention programs among participants at an average age of 80.1 years [85]. The mentioned two reasons might explain why the HEPEs could significantly improve balance in people over 75 years of age.
The result of another subgroup analysis based on different intervention durations suggested that >16 weeks was an appropriate intervention duration, as a significant improvement in balance was found compared with the subgroup training for less than 16 weeks. A SR aimed at dose–response relationships in balance training in older adults illustrated that balance training lasting for less than 11 weeks resulted in lower effects on balance performance [86]. Another previous review which examined the efficacy of exercise to reduce falls recommended at least 2 h of training per week for a training period of more than 6 months to reduce falls [87]. In our SR, the average amount of exercise was 121.25 min per week, which was in accordance with the analysis by Sherrington et al. [87]. These findings might indicate that an intervention period for HEPE of more than 16 weeks could be more effective in improving overall balance performance.
Muscle strength (especially in the lower extremities) is one of the factors that are closely related to falls in older adults [88]. The result found that lower extremity strength was significantly improved in HEPE groups as measured by FTSST. The positive finding might be because most of the HEPEs consisted of strength or functional training. Almost all of the studies delivered individually tailored muscle strength training, including stepping or stretching exercises that would increase in difficulty over time, as recommended by Gschwind et al. and Shake et al. [31,60,61,64,65]. A more comprehensive program including vestibular rehabilitation, core and limb strengthening exercises, joint motion range exercises and balance exercises was used in the study of Yi et al. [44]. Therefore, in order to achieve better results in improving lower limb strength, multimodal exercise programs were recommended in HEPEs.
Conversely, the effect of HEPEs on fall risk as measured by PPA was not significant. The between-trial heterogeneity (I2 = 48%) could be explained by a single study from Gschwind et al. [31]. The heterogeneity reduced to 28% (χ2 = 2.79; p = 0.25) when this trial was removed from the meta-analysis, and the overall effect of HEPEs on fall risks was then significant (MD: -0.32: 95% CI: -0.58 to -0.07; Z = 2.46; p = 0.01). According to Gschwind et al., a low adherence rate may explain the limited improvement of PPA. There was a significant three-way interaction for fall risk assessed by the PPA in a subgroup analysis between the high-adherence (>90 min of exercise per week), low-adherence (<90 min of exercise per week) and control groups (p = 0.044) [31]. In addition, two-way analysis comparing the high-adherence group with the control group revealed a significantly larger effect in favor of the high-adherence group for fall risk (p = 0.031) [31]. This result was in accordance with our finding that only a certain amount of exercise (at least 120 min per week for over 16 weeks) can achieve significant improvement in physical behavior. Our finding was better supported by the following studies which validated the dose–response relationship between fall risk and fall effectiveness. Haines et al. found a negative result of fall efficacy as measured by the activity-specific balance confidence scale after only 8 weeks of intervention (regression coefficient: -0.30; 95% CI: -1.49 to 0.89; p = 0.61) [59]. Contrary to this, another RCT suggested that a 24-week home-based tele-rehabilitation program could significantly reduce the risk of falls (RR: 0.60; 95% CI: 0.44–0.83; p < 0.001) [89].
Meanwhile, it was important to know whether exercise-induced overall physical improvement was stable over time. Evidence indicated that the fall prevention program with exercise intervention improved functional performance at 3 months in community-dwelling older adults with risk of falls, but did not reduce falls at 1-year follow-up [90]. Arkkukangas et al. conducted a trial of 12 weeks of fall prevention exercise for community-dwelling older adults, in which a significant within-group improvement was found in physical performance (p = 0.04), fall efficacy (p = 0.02) and physical activity level (p = 0.02) according to a short-term follow-up [91]. However, the positive result was not reproduced in their 2-year follow-up study [92]. Likewise, Naseri et al. found a similar time–efficacy relationship at 6-month follow-up [93]. With reference to the mentioned studies, we suggest conducting HEPEs on a permanent basis to counteract time-related declines in overall physical performance. In addition to applying different kinds of e-devices, the following improvements were adopted by the included studies to enable better long-term adherence: the exercise programs were modified and supplemented to suit the older adults in seven studies [31,44,58,61,63,64,66]; two studies provided a video of the exercises [62,67]; and three studies provided remote guidance for any possible problems [59,60,65].
Of note, the positive changes in dual-task TUG were also enlightening. As dual-task TUG is a cognitive-related test [74], this might mean that HEPEs could improve cognitive function in older adults. In addition to the studies of Schoene et al. and Li et al. [60,66], Shake et al. also paid attention to cognitive changes; these results suggested a significant main effect of group exercise (p < 0.05) and an interaction effect (p = 0.02) [64]. However, a review suggested that physical activity or exercise alone was able to improve the attentional control so as to help improve cognition in older at-risk individuals [94]. Likewise, a meta-analysis among older adults also showed that exercise training had a significant benefit for cognitive function (p < 0.001) [95]. Therefore the improvements associated with dual-task TUG or cognitive tasks were mostly attributed to the exercise itself. Whether the intervention of e-devices could improve cognitive function needed further experimental proof. So any evidence of potential benefits from HEPEs should be interpreted cautiously, given the limited evidence of changes to cognitive function.
Strengths & limitations
This review, to our knowledge, is the first SR and meta-analysis examining the effectiveness of HEPEs on fall prevention among community-dwelling older adults. Especially in the background of COVID-19, this cost-friendly and contactless intervention is worthy of being studied and popularized. Meanwhile, intervention using e-devices has solved the problem of poor adherence of home-based exercises to a great extent. A previous review proved that telehealth combined with e-devices was able to reduce fall risk and fall efficacy significantly [40], and evidence also showed that individualized home-based exercise programs can lead to significant improvements in physical activity, balance, mobility and muscle strength for older people [85]. In the review we focused on home-based exercise programs delivered by e-devices; we not only proved the effectiveness of HEPEs for fall prevention, but also reached a quantitative conclusion on the optimum exercise volume when using a HEPE. The specific volume of exercise can help healthcare providers or physiotherapist to make an informed decision for community-dwelling older adults in relation to falls. Furthermore, in addition to qualitative and quantitative perspectives, we compared HEPEs with traditional home-based exercise programs and face-to-face exercise programs in terms of fall rates. Last but not least, our findings were based on 12 studies that can be considered, on average, of good quality (PEDro score = 6.83).
This review is not without limitations. First of all, the small number of available studies and the lack of a consistent set of tests make our conclusions preliminary in essence. In fact, the sample sizes of the included studies were uneven, ranging from 30 to 503. As such, the results had smaller effect sizes and may not be representative of larger populations. Secondly, the review excluded older adults with a diagnosis of chronic diseases such as multiple sclerosis, cancer, Parkinson’s disease or Alzheimer’s disease, because these patients may have a different performance in terms of balance [96], strength [97], mobility [98] or cognitive ability [99], which increases the risk of falls and restricts the effectiveness of HEPEs. Therefore future studies should consider investigating the effects of HEPEs on older adults with different chronic diseases. Thirdly, most of the included studies were conducted in Asia and Australia; the result might be different in other regions, as many factors have been proved to influence fall risk, including ethnicity and health status [100]. Finally, almost all the studies were from developed countries, so the results might not be replicable in nondeveloped countries or remote areas.
Implications for practice & research
In terms of implications for practice, the intervention pattern of a HEPE should be personalized and contain multiple types of exercise (including balance, strength training and functional training) to achieve a better curative effect. Next, the duration of intervention should be more than 16 weeks. Besides that, a permanent exercise plan is recommended in order to counteract time-related declines in overall physical performance. The frequency of HEPE-based exercise should be at least 120 min per week. Last but not least, step-by-step instructions and important advice regarding the method of application of the e-devices are necessary to increase the acceptance of new technologies among the elderly [101].
In terms of implications for research, as we did not find significant positive results from HEPEs on cognitive performance, future studies could pay attention to the special effects of HEPEs on cognition. Furthermore, multiple test methods should be applied in any future study in order to reduce the deviation of results caused by single tests and reinforce the credibility of the results.
Conclusion
This review proved the effectiveness of HEPEs on falls among community-dwelling older adults during the COVID-19 period. The results showed that HEPEs significantly improved lower extremity strength and reduced the rate of falls among healthy older adults. Compared with those aged below 75 years, HEPEs had a positive effect on those aged over 75 years. We also found that the volume of exercise should ideally be at least 120 min per week for over 16 weeks. Despite their preliminary nature, these findings suggest that HEPEs can be promoted in the elderly as an effective fall prevention intervention due to the exponential aging of the population and the present situation caused by the COVID-19 pandemic.
Future perspective
Future studies could pay attention to investigating the effectiveness of HEPEs on other fall-related factors. Examples include, but are not limited to, cognitive performance, vision or psychological status. In the context of COVID-19 and global aging, remote health interventions can be an innovative and effective pattern to deliver healthcare to the community-dwelling older adult.
Background
•
Falls among older people are a worldwide public health issue.
•
Home-based exercise programs with e-devices (HEPEs) can improve participants’ adherence, reduce the influence of COVID-19 and save the medical workers’ labor cost.
•
This is the first meta-analysis providing evidence on the effects of HEPEs in community-dwelling older adults.
Methods
•
An extensive literature search was performed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses approach.
•
Four fall-related outcomes were evaluated in the meta-analysis: rate of falls (proportion of fallers), balance (timed up and go), lower extremity strength (five-times sit-to-stand test) and fall efficacy (physiological profile assessment). Subgroup and sensitivity analyses were conducted during the meta-analysis.
Results
•
A total of 12 studies were finally included, and their overall quality was good (average score from the Physiotherapy Evidence Database = 6.83).
•
HEPEs could significantly reduce the rate of falls and improve lower extremity strength.
•
HEPEs could improve balance if the participants were aged over 75 years or the intervention duration was at least 16 weeks.
Conclusion
•
HEPEs demonstrated an overall positive effect on falls among community-dwelling older adults.
•
Based on the results, we recommend that older adults do exercise that lasts at least 120 min per week for over 16 weeks.
Acknowledgments
The investigators wish to thank all the authors involved for their valuable contributions.
Financial & competing interests disclosure
This work was supported by National Key R&D Program of China (no. 2020YFC2008703). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Ethical approval was noted for all of the published papers included in this review.
Supplementary Material
File (supplementary data.docx)
- Download
- 16.99 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Lord SR, Ward JA, Williams P, Anstey KJ. An epidemiological study of falls in older community-dwelling women: the Randwick falls and fractures study. Aust. J. Public Health 17(3), 240–245 (1993).
2.
Phelan EA, Ritchey K. Fall prevention in community-dwelling older adults. Ann. Intern. Med. 169(11), Itc81–itc96 (2018).
3.
Alamgir H, Muazzam S, Nasrullah M. Unintentional falls mortality among elderly in the United States: time for action. Injury 43(12), 2065–2071 (2012).
4.
Peel NM. Epidemiology of falls in older age. Can. J. Aging 30(1), 7–19 (2011).
5.
Tricco AC, Thomas SM, Veroniki AA et al. Comparisons of interventions for preventing falls in older adults: a systematic review and meta-analysis. JAMA 318(17), 1687–1699 (2017).
6.
Turner S, Arthur G, Lyons RA et al. Modification of the home environment for the reduction of injuries. Cochrane Database Syst. Rev. 2011(2), Cd003600 (2011).
7.
Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J. Am. Geriatr. Soc. 59(1), 148–157 (2011).
8.
Reuben DB, Gazarian P, Alexander N et al. The strategies to reduce injuries and develop confidence in elders intervention: falls risk factor assessment and management, patient engagement, and nurse co-management. J. Am. Geriatr. Soc. 65(12), 2733–2739 (2017).
9.
Hopewell S, Adedire O, Copsey BJ et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 7(7), Cd012221 (2018).
10.
Kumar A, Delbaere K, Zijlstra GA et al. Exercise for reducing fear of falling in older people living in the community: Cochrane systematic review and meta-analysis. Age Ageing 45(3), 345–352 (2016).
• Exercise interventions probably reduce fear of falling to a small to moderate degree immediately post-intervention in community-living older people.
11.
Cvecka J, Tirpakova V, Sedliak M, Kern H, Mayr W, Hamar D. Physical activity in elderly. Eur. J. Transl. Myol. 25(4), 249–252 (2015).
12.
Cadore EL, Rodríguez-Mañas L, Sinclair A, Izquierdo M. Effects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic review. Rejuvenation Res. 16(2), 105–114 (2013).
13.
Papalia GF, Papalia R, Diaz Balzani LA et al. The effects of physical exercise on balance and prevention of falls in older people: a systematic review and meta-analysis. J. Clin. Med. 9(8), 2595 (2020).
14.
Donath L, Van Dieën J, Faude O. Exercise-based fall prevention in the elderly: what about agility? Sports Med. 46(2), 143–149 (2016).
15.
Gschwind YJ, Kressig RW, Lacroix A, Muehlbauer T, Pfenninger B, Granacher U. A best practice fall prevention exercise program to improve balance, strength/power, and psychosocial health in older adults: study protocol for a randomized controlled trial. BMC Geriatr. 13, 105 (2013).
16.
Yoo EJ, Jun TW, Hawkins SA. The effects of a walking exercise program on fall-related fitness, bone metabolism, and fall-related psychological factors in elderly women. Res. Sports Med. 18(4), 236–250 (2010).
17.
Rimer J, Dwan K, Lawlor DA et al. Exercise for depression. Cochrane Database Syst. Rev. 2012(7), CD004366 (2012).
18.
Sipilä S, Törmäkangas T, Sillanpää E et al. Muscle and bone mass in middle-aged women: role of menopausal status and physical activity. J. Cachexia Sarcopenia Muscle 11(3), 698–709 (2020).
19.
Karinkanta S, Piirtola M, Sievänen H, Uusi-Rasi K, Kannus P. Physical therapy approaches to reduce fall and fracture risk among older adults. Nat. Rev. Endocrinol. 6(7), 396–407 (2010).
20.
Hewitt J, Goodall S, Clemson L, Henwood T, Refshauge K. Progressive resistance and balance training for falls prevention in long-term residential aged care: a cluster randomized trial of the Sunbeam program. J. Am. Med. Dir. Assoc. 19(4), 361–369 (2018).
21.
Lomas-Vega R, Obrero-Gaitán E, Molina-Ortega FJ, Del-Pino-Casado R. Tai chi for risk of falls. a meta-analysis. J. Am. Geriatr. Soc. 65(9), 2037–2043 (2017).
22.
Youkhana S, Dean CM, Wolff M, Sherrington C, Tiedemann A. Yoga-based exercise improves balance and mobility in people aged 60 and over: a systematic review and meta-analysis. Age Ageing 45(1), 21–29 (2016).
23.
Kendrick D, Kumar A, Carpenter H et al. Exercise for reducing fear of falling in older people living in the community. Cochrane Database Syst. Rev. 2014(11), Cd009848 (2014).
24.
Gillespie LD, Robertson MC, Gillespie WJ et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012(9), Cd007146 (2012).
25.
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Buchner DM. Falls prevention over 2 years: a randomized controlled trial in women 80 years and older. Age Ageing 28(6), 513–518 (1999).
26.
Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ 315(7115), 1065–1069 (1997).
27.
Liu-Ambrose T, Davis JC, Best JR et al. Effect of a home-based exercise program on subsequent falls among community-dwelling high-risk older adults after a fall: a randomized clinical trial. JAMA 321(21), 2092–2100 (2019).
28.
Rincé G, Couturier C, Berrut G, Dylis A, Montero-Odasso M, Deschamps T. Impact of an individual personalised rehabilitation program on mobility performance in older-old people. Aging Clin. Exp. Res. 33(10), 2821–2830 (2021).
29.
Brodie MA, Okubo Y, Annegarn J, Wieching R, Lord SR, Delbaere K. Disentangling the health benefits of walking from increased exposure to falls in older people using remote gait monitoring and multi-dimensional analysis. Physiol. Meas. 38(1), 45–62 (2017).
30.
Netz Y, Argov E, Yekutieli Z et al. Personalized multicomponent exercise programs using smartphone technology among older people: protocol for a randomized controlled trial. BMC Geriatr. 21(1), 605 (2021).
31.
Gschwind YJ, Eichberg S, Ejupi A et al. ICT-based system to predict and prevent falls (iStoppFalls): results from an international multicenter randomized controlled trial. Eur. Rev. Aging Phys. Act. 12, 10 (2015).
32.
Yardley L, Nyman SR. Internet provision of tailored advice on falls prevention activities for older people: a randomized controlled evaluation. Health Promot. Int. 22(2), 122–128 (2007).
33.
Sherrington C, Michaleff ZA, Fairhall N et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br. J. Sports Med. 51(24), 1750–1758 (2017).
34.
Mittaz Hager AG, Mathieu N, Lenoble-Hoskovec C, Swanenburg J, De Bie R, Hilfiker R. Effects of three home-based exercise programmes regarding falls, quality of life and exercise-adherence in older adults at risk of falling: protocol for a randomized controlled trial. BMC Geriatr. 19(1), 13 (2019).
35.
Gardner MM, Buchner DM, Robertson MC, Campbell AJ. Practical implementation of an exercise-based falls prevention programme. Age Ageing 30(1), 77–83 (2001).
36.
Möller UO, Kristensson J, Midlöv P, Ekdahl C, Jakobsson U. Effects of a one-year home-based case management intervention on falls in older people: a randomized controlled trial. J. Aging Phys. Act. 22(4), 457–464 (2014).
• This traditional home-based case management intervention was not able to prevent falls or injurious falls due to poor adherence.
37.
Gallo E, Stelmach M, Frigeri F, Ahn DH. Determining whether a dosage-specific and individualized home exercise program with consults reduces fall risk and falls in community-dwelling older adults with difficulty walking: a randomized control trial. J. Geriatr. Phys. Ther. 41(3), 161–172 (2018).
• This study supports the efficacy of the experimental program in decreasing fall risk and being more effective than our usual care, as well as fostering greater compliance with an exercise regimen.
38.
Clemson L, Fiatarone Singh MA, Bundy A et al. Integration of balance and strength training into daily life activity to reduce rate of falls in older people (the LiFE study): randomised parallel trial. BMJ 345, e4547 (2012).
39.
Van Der Kolk NM, De Vries NM, Kessels RPC et al. Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: a double-blind, randomised controlled trial. Lancet Neurol. 18(11), 998–1008 (2019).
40.
Chan JKY, Klainin-Yobas P, Chi Y, Gan JKE, Chow G, Wu XV. The effectiveness of e-interventions on fall, neuromuscular functions and quality of life in community-dwelling older adults: a systematic review and meta-analysis. Int. J. Nurs. Stud. 113, 103784 (2021).
•• The aim of this review was to synthesize best available evidence concerning the effectiveness of e-interventions on fall, neuromuscular functions and quality of life in community-dwelling older adults.
41.
Valenzuela T, Okubo Y, Woodbury A, Lord SR, Delbaere K. Adherence to technology-based exercise programs in older adults: a systematic review. J. Geriatr. Phys. Ther. 41(1), 49–61 (2018).
•• This systematic review indicated that technology-based exercise interventions have good adherence and may provide a sustainable means of promoting physical activity and preventing falls in older people.
42.
Silveira P, Van De Langenberg R, Van Het Reve E, Daniel F, Casati F, De Bruin ED. Tablet-based strength-balance training to motivate and improve adherence to exercise in independently living older people: a phase II preclinical exploratory trial. J. Med. Internet Res. 15(8), e159 (2013).
43.
Van Het Reve E, Silveira P, Daniel F, Casati F, De Bruin ED. Tablet-based strength–balance training to motivate and improve adherence to exercise in independently living older people: part 2 of a phase II preclinical exploratory trial. J. Med. Internet Res. 16(6), e159 (2014).
44.
Yi D, Yim J. Remote home-based exercise program to improve the mental state, balance, and physical function and prevent falls in adults aged 65 years and older during the COVID-19 pandemic in Seoul, Korea. Med. Sci. Monit. 27, e935496 (2021).
45.
Pišot R, Marusic U, Biolo G et al. Greater loss in muscle mass and function but smaller metabolic alterations in older compared with younger men following 2 wk of bed rest and recovery. J. Appl. Physiol. (1985) 120(8), 922–929 (2016).
46.
Dwyer MJ, Pasini M, De Dominicis S, Righi E. Physical activity: benefits and challenges during the COVID-19 pandemic. Scand. J. Med. Sci. Sports 30(7), 1291–1294 (2020).
47.
Holmes EA, O'Connor RC, Perry VH et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 7(6), 547–560 (2020).
48.
Giordano A, Bonometti GP, Vanoglio F et al. Feasibility and cost–effectiveness of a multidisciplinary home-telehealth intervention programme to reduce falls among elderly discharged from hospital: study protocol for a randomized controlled trial. BMC Geriatr. 16(1), 209 (2016).
49.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med. 6(7), e1000097 (2009).
50.
Liberati A, Altman DG, Tetzlaff J et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339, b2700 (2009).
51.
Sherrington C, Fairhall NJ, Wallbank GK et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 1(1), Cd012424 (2019).
52.
World Health Organization. Falls (2021). www.who.int/news-room/fact-sheets/detail/falls
53.
Devereaux PJ, Yusuf S. The evolution of the randomized controlled trial and its role in evidence-based decision making. J. Intern. Med. 254(2), 105–113 (2003).
54.
Elkins MR, Moseley AM, Sherrington C, Herbert RD, Maher CG. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br. J. Sports Med. 47(4), 188–189 (2013).
55.
Cashin AG, Mcauley JH. Clinimetrics: Physiotherapy Evidence Database (PEDro) scale. J. Physiother. 66(1), 59 (2020).
56.
Gonzalez GZ, Moseley AM, Maher CG, Nascimento DP, Costa L, Costa LO. Methodologic quality and statistical reporting of physical therapy randomized controlled trials relevant to musculoskeletal conditions. Arch. Phys. Med. Rehabil. 99(1), 129–136 (2018).
57.
Cumpston MS, Mckenzie JE, Welch VA, Brennan SE. Strengthening systematic reviews in public health: guidance in the Cochrane Handbook for Systematic Reviews of Interventions, 2nd edition. J. Public Health (Oxf.) fdac036 (2022) (Epub ahead of print).
58.
Rosie J, Taylor D. Sit-to-stand as home exercise for mobility-limited adults over 80 years of age – GrandStand System™ may keep you standing? Age Ageing 36(5), 555–562 (2007).
59.
Haines TP, Russell T, Brauer SG et al. Effectiveness of a video-based exercise programme to reduce falls and improve health-related quality of life among older adults discharged from hospital: a pilot randomized controlled trial. Clin. Rehabil. 23(11), 973–985 (2009).
60.
Schoene D, Lord SR, Delbaere K, Severino C, Davies TA, Smith ST. A randomized controlled pilot study of home-based step training in older people using videogame technology. PLOS ONE 8(3), e57734 (2013).
61.
Gschwind YJ, Schoene D, Lord SR et al. The effect of sensor-based exercise at home on functional performance associated with fall risk in older people – a comparison of two exergame interventions. Eur. Rev. Aging Phys. Act. 12, 11 (2015).
62.
Boongird C, Keesukphan P, Phiphadthakusolkul S, Rattanasiri S, Thakkinstian A. Effects of a simple home-based exercise program on fall prevention in older adults: a 12-month primary care setting, randomized controlled trial. Geriatr. Gerontol. Int. 17(11), 2157–2163 (2017).
63.
Hong J, Kong HJ, Yoon HJ. Web-based telepresence exercise program for community-dwelling elderly women with a high risk of falling: randomized controlled trial. JMIR Mhealth Uhealth 6(5), e132 (2018).
64.
Shake MC, Crandall KJ, Mathews RP, Falls DG, Dispennette AK. Efficacy of Bingocize®: a game-centered mobile application to improve physical and cognitive performance in older adults. Games Health J. 7(4), 253–261 (2018).
65.
Delbaere K, Valenzuela T, Lord SR et al. E-health StandingTall balance exercise for fall prevention in older people: results of a two year randomised controlled trial. BMJ 373, n740 (2021).
•• The program significantly reduced the rate of falls and injurious falls over 2 years, with similar but not statistically significant effects at 12 months.
66.
Li F, Harmer P, Voit J, Chou LS. Implementing an online virtual falls prevention intervention during a public health pandemic for older adults with mild cognitive impairment: a feasibility trial. Clin. Interv. Aging 16, 973–983 (2021).
67.
Yerlikaya T, Öniz A, Özgùren M. The effect of an interactive tele rehabilitation program on balance in older individuals. Neurol. Sci. Neurophysiol. 38(3), 180–186 (2021).
68.
Choo PL, Tou NX, Jun Pang BW et al. Timed up and go (TUG) reference values and predictive cutoffs for fall risk and disability in Singaporean community-dwelling adults: Yishun cross-sectional study and Singapore longitudinal aging study. J. Am. Med. Dir. Assoc. 22(8), 1640–1645 (2021).
69.
Barry E, Galvin R, Keogh C, Horgan F, Fahey T. Is the timed up and go test a useful predictor of risk of falls in community dwelling older adults: a systematic review and meta-analysis. BMC Geriatr. 14, 14 (2014).
70.
Downs S. The Berg Balance Scale. J Physiother. 61(1), 46 (2015).
71.
Miranda-Cantellops N, Tiu TK. Berg balance testing. In: StatPearls. StatPearls Publishing LLC, FL, USA (2022).
72.
Pavasini R, Guralnik J, Brown JC et al. Short Physical Performance Battery and all-cause mortality: systematic review and meta-analysis. BMC Med. 14(1), 215 (2016).
73.
Zijlstra A, Ufkes T, Skelton DA, Lundin-Olsson L, Zijlstra W. Do dual tasks have an added value over single tasks for balance assessment in fall prevention programs? A mini-review. Gerontology 54(1), 40–49 (2008).
74.
Chen HY, Tang PF. Factors contributing to single- and dual-task timed ‘up & go’ test performance in middle-aged and older adults who are active and dwell in the community. Phys. Ther. 96(3), 284–292 (2016).
75.
Paul SS, Canning CG. Five-repetition sit-to-stand. J. Physiother. 60(3), 168 (2014).
76.
Goldberg A, Chavis M, Watkins J, Wilson T. The five-times-sit-to-stand test: validity, reliability and detectable change in older females. Aging Clin. Exp. Res. 24(4), 339–344 (2012).
77.
Muñoz-Bermejo L, Adsuar JC, Mendoza-Muñoz M et al. Test-retest reliability of five times sit to stand test (FTSST) in adults: a systematic review and meta-analysis. Biology (Basel) 10(6), 510 (2021).
78.
Lord SR, Menz HB, Tiedemann A. A physiological profile approach to falls risk assessment and prevention. Phys. Ther. 83(3), 237–252 (2003).
79.
Whitney JC, Lord SR, Close JC. Streamlining assessment and intervention in a falls clinic using the timed up and go test and physiological profile assessments. Age Ageing 34(6), 567–571 (2005).
80.
Dewan N, Macdermid JC. Fall Efficacy Scale – International (FES-I). J. Physiother. 60(1), 60 (2014).
81.
Osoba MY, Rao AK, Agrawal SK, Lalwani AK. Balance and gait in the elderly: a contemporary review. Laryngoscope Investig. Otolaryngol. 4(1), 143–153 (2019).
82.
Wu G, Keyes L, Callas P, Ren X, Bookchin B. Comparison of telecommunication, community, and home-based tai chi exercise programs on compliance and effectiveness in elders at risk for falls. Arch. Phys. Med. Rehabil. 91(6), 849–856 (2010).
83.
Mansson L, Lundin-Olsson L, Skelton DA et al. Older adults’ preferences for, adherence to and experiences of two self-management falls prevention home exercise programmes: a comparison between a digital programme and a paper booklet. BMC Geriatr. 20(1), 209 (2020).
84.
Martins AC, Santos C, Silva C, Baltazar D, Moreira J, Tavares N. Does modified Otago exercise program improves balance in older people? A systematic review. Prev. Med. Rep. 11, 231–239 (2018).
85.
Hill KD, Hunter SW, Batchelor FA, Cavalheri V, Burton E. Individualized home-based exercise programs for older people to reduce falls and improve physical performance: a systematic review and meta-analysis. Maturitas 82(1), 72–84 (2015).
86.
Lesinski M, Hortobágyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis. Sports Med. 45(12), 1721–1738 (2015).
87.
Sherrington C, Tiedemann A, Fairhall N, Close JC, Lord SR. Exercise to prevent falls in older adults: an updated meta-analysis and best practice recommendations. NSW Public Health Bull. 22(3–4), 78–83 (2011).
88.
Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J. Am. Geriatr. Soc. 52(7), 1121–1129 (2004).
89.
Bernocchi P, Giordano A, Pintavalle G et al. Feasibility and clinical efficacy of a multidisciplinary home-telehealth program to prevent falls in older adults: a randomized controlled trial. J. Am. Med. Dir. Assoc. 20(3), 340–346 (2019).
90.
Lee HC, Chang KC, Tsauo JY, Hung JW, Huang YC, Lin SI. Effects of a multifactorial fall prevention program on fall incidence and physical function in community-dwelling older adults with risk of falls. Arch. Phys. Med. Rehabil. 94(4), 606–615 (2013).
91.
Arkkukangas M, Söderlund A, Eriksson S, Johansson AC. Fall preventive exercise with or without behavior change support for community-dwelling older adults: a randomized controlled trial with short-term follow-up. J. Geriatr. Phys. Ther. 42(1), 9–17 (2019).
92.
Arkkukangas M, Johnson ST, Hellström K, Anens E, Tonkonogi M, Larsson U. Fall prevention exercises with or without behavior change support for community-dwelling older adults: a two-year follow-up of a randomized controlled trial. J. Aging Phys. Act. 28(1), 34–41 (2019).
93.
Naseri C, McPhail SM, Morris ME et al. Tailored education increased capability and motivation for fall prevention in older people after hospitalization. Front. Public Health 9, 683723 (2021).
94.
Bherer L. Cognitive plasticity in older adults: effects of cognitive training and physical exercise. Ann. NY Acad. Sci. 1337, 1–6 (2015).
95.
Falck RS, Davis JC, Best JR, Crockett RA, Liu-Ambrose T. Impact of exercise training on physical and cognitive function among older adults: a systematic review and meta-analysis. Neurobiol. Aging 79, 119–130 (2019).
96.
Sveinbjornsdottir S. The clinical symptoms of Parkinson’s disease. J. Neurochem. 139 (Suppl. 1), 318–324 (2016).
97.
García-Hermoso A, Ramírez-Vélez R, Peterson MD et al. Handgrip and knee extension strength as predictors of cancer mortality: a systematic review and meta-analysis. Scand. J. Med. Sci. Sports 28(8), 1852–1858 (2018).
98.
Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet 391(10130), 1622–1636 (2018).
99.
Ballard C, Gauthier S, Corbett A, Brayne C, Aarsland D, Jones E. Alzheimer’s disease. Lancet 377(9770), 1019–1031 (2011).
100.
Sattin RW. Falls among older persons: a public health perspective. Annu. Rev. Public Health 13, 489–508 (1992).
101.
Pilotto A, Boi R, Petermans J. Technology in geriatrics. Age Ageing 47(6), 771–774 (2018).
Information & Authors
Information
Published In
Pages: 1201 - 1217
PubMed: 36148921
Copyright
© 2022 Future Medicine Ltd.
History
Received: 17 July 2022
Accepted: 5 September 2022
Published online: 23 September 2022
Keywords:
Topics
Authors
Funding Information
National Key R&D Program of China: 2020YFC2008703
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Effect of home-based exercise programs with e-devices on falls among community-dwelling older adults: a meta-analysis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0130
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Fernanda Bueno Pilastri, Julia Fantim Lopez, Eric Nkansah Boateng, Nise Ribeiro Marques, What to Know About Falls in Older Adults? Risk Factors, Predictors, and Therapeutic Interventions, International Journal of Environmental Research and Public Health, 10.3390/ijerph22121863, 22, 12, (1863), (2025).
- Ana Isabel Martins, Rosa Andias, Diana Azedo, Frederico Baptista, Bárbara Ursine, Anabela G. Silva, Nelson Pacheco Rocha, Heuristic Evaluation of a Web-Based Application to Deliver a Home-Based Personalized Physical Exercise Program for Older Adults, Procedia Computer Science, 10.1016/j.procs.2024.06.158, 239, (158-165), (2024).