Rivaroxaban for the prevention of outcomes in patients with atrial fibrillation in clinical practice: an indirect comparison of national and international registries
Publication: Journal of Comparative Effectiveness Research
Abstract
Objective: To analyze the effectiveness and safety of rivaroxaban in patients with atrial fibrillation (AF). Methods: The clinical profile and outcomes of the EMIR study were indirectly compared with those of ROCKET-AF, eight other Spanish observational studies and XANTUS. Results: In EMIR, mean age was 74.2 years and CHA2DS2-VASc was 3.5. In the rivaroxaban arm of the ROCKET-AF trial, mean age was 73 years and CHADS2 was 3.5, whereas in the Spanish studies mean age ranged from 74.9 years to 78.4 years and CHA2DS2-VASc from 3.5 to 4.3. In EMIR, rates of stroke/systemic embolism, major adverse cardiovascular events, cardiovascular death and major bleeding were 0.57, 1.07, 0.63 and 1.04 events/100 patient-years, respectively. In ROCKET-AF, these numbers were 1.7, 3.91, 1.53 and 3.6 events/100 patient-years, respectively. In the Spanish studies, rates of stroke and major bleeding were 0–1.8 and 0.22–4.2 events/100 patient-years, respectively. In XANTUS, rates of stroke, major adverse cardiovascular events and major bleeding were 0.7, 1.8 and 2.1 events/100 patient-years, respectively. Conclusion: Despite the fact that rivaroxaban is prescribed for elderly patients with a high thromboembolic risk, rates of outcomes remain low.
Atrial fibrillation (AF) is the most common cardiac arrhythmia all around the world, currently reaching epidemic numbers [1]. Ischemic stroke is the most devastating complication associated with AF, and anticoagulation represents the cornerstone for the prevention of thromboembolic events in the AF population [2]. However, despite anticoagulation, patients remain at risk of cardiovascular complications, including myocardial infarction or cardiovascular death [3]. As a result, not only stroke but also overall cardiovascular disease prevention should be considered in the comprehensive management of the AF population [2].
Direct oral anticoagulants (DOACs) exhibit a better benefit–risk profile than vitamin K antagonists [4]. Remarkably, the greater rates of anticoagulation shown in the last years, particularly through a higher use of DOACs in clinical practice, have translated into a reduction of ischemic stroke [5,6]. Rivaroxaban is a once-daily direct anticoagulant that effectively reduces the risk of stroke with a good safety profile. The ROCKET-AF trial showed in a high-risk population that rivaroxaban was at least as effective as warfarin for the prevention of stroke or systemic embolism, with a lower risk of fatal and intracranial hemorrhages [7]. However, it is important to ascertain whether these good results can be extended to the overall real-life population with AF [8]. The EMIR study was designed to evaluate the performance of the cardiovascular risk 2MACE score in AF patients treated with rivaroxaban. Overall, this study showed that the risk of adverse events (stroke, major cardiovascular events [MACE] and bleeding) in elderly patients with many comorbidities anticoagulated with rivaroxaban in Spain was low [9].
However, in the last years a number of national and international studies on the use of rivaroxaban in clinical practice have been published [10–25]. As a result, it is important to ascertain whether the results of the EMIR study are comparable to other registries of patients anticoagulated with rivaroxaban. The aim of this narrative review was to evaluate, through indirect comparisons between different national or international real-life studies, the clinical profile and outcomes of patients with AF anticoagulated with rivaroxaban. Additionally, data from the EMIR study were compared with three other observational and prospective studies of patients treated with different DOACs [10–25].
Methods
EMIR was a noninterventional and observational study that included patients ≥18 years old with AF, taking rivaroxaban according to clinical practice ≥6 months before being enrolled. Patients with a valvular prosthesis or rheumatic mitral stenosis were excluded from the study. Patients were recruited from 79 Spanish centers (hospitals and private clinics) and followed up during 2.5 years with four visits (baseline, 12 months, 24 months and study end) that should coincide with any of the patients' routine visits. In the EMIR study, MACE were defined as a combination of nonfatal myocardial infarction, revascularization and cardiovascular death (death for coronary events, progressive heart failure death and sudden cardiac death) [9].
ROCKET-AF was a double-blind clinical trial in which 14,264 patients with nonvalvular AF who were at increased risk for stroke were randomized to receive either rivaroxaban or dose-adjusted warfarin. The median duration of treatment exposure was 590 days, with a median follow-up period of 707 days [7].
In addition to the EMIR study, eight other Spanish observational studies (one with a prospective design and seven with a retrospective design) of patients with AF taking rivaroxaban for the prevention of stroke or systemic embolism were analyzed. Brun et al. performed a retrospective study of AF patients who had started rivaroxaban therapy between May 2013 and February 2017 in the cardiology department of two hospitals from Huesca. Mean duration of treatment was 30.5 months [10]. Cerdá et al. developed an observational and prospective study of all patients with AF, with or without prior stroke, who had attended the Oral Anticoagulant Treatment Unit of the Hemostasis and Thrombosis Department of the University Hospital Vall d’ Hebron from Barcelona and who had started treatment with any DOAC between January 2015 and September 2017. Mean follow-up was 1.7 years [11]. Gavin et al. designed a retrospective study that included all patients with AF who had started treatment with rivaroxaban for the prevention of thromboembolic events in the hematology unit of a tertiary hospital between February 2012 and June 2016 (mean follow-up of 16.5 months) [12]. Pérez Cabeza et al. analyzed, in a retrospective study, the drug persistence and outcomes after 2 years of follow-up in a cohort of patients with AF in whom rivaroxaban had been prescribed during the first quarter of 2014 by cardiologists or internists, in the sanitary area of Costa del Sol (Malaga, Spain) [13]. Muñiz et al. developed a retrospective study that included all patients with AF who had started anticoagulant treatment with rivaroxaban for the prevention of stroke or systemic embolism between July 2013 and May 2017 (mean follow-up of 26.6 months) in a regional hospital in Asturias (Hospital San Agustin, Aviles, Spain) [14]. Marti et al. retrospectively analyzed patients with AF that had started treatment with rivaroxaban for the prevention of stroke from July 2012 to December 2015 (mean duration of treatment of 29.7 months) in a healthcare area of 330,000 inhabitants of Valencia (Spain) [15]. Pimentel et al. performed a retrospective study of AF patients treated with rivaroxaban in the cardiology department of the tertiary hospital San Juan de la Cruz at Ubeda (Jaen, Spain), between November 2012 and January 2017 (median follow-up of 24 months) [16]. Caro et al. developed a retrospective study that included all AF patients who had started treatment with rivaroxaban for the prevention of stroke or systemic embolism between December 2012 and December 2015 (mean follow-up period of 22.7 months) from two health areas belonging to two tertiary hospitals (Hospital Vega Baja [(]Alicante, Spain], and University Hospital Clinico Virgen de la Arrixaca [El Palmar, Spain]) [17].
Furthermore, one international study of patients taking rivaroxaban for the prevention of thromboembolic events was included. Thus, the XANTUS study was the first international, real-world, prospective, observational study of patients treated with rivaroxaban for stroke prevention in AF. This study included patients with AF newly started on rivaroxaban who were followed up at ∼3-month intervals for 1 year, or for at least 30 days after permanent discontinuation (mean treatment duration of 329 days) [21].
Additionally, in order to put into context the results of rivaroxaban compared with those of other DOACs, three prospective registries of patients with AF taking any DOAC were also included for analysis (one developed in Spain and two international studies performed in different countries across Europe). The FANTASIIA registry included consecutive AF outpatients on anticoagulant therapy, either with vitamin K antagonists or DOACs, from 50 Spanish centers between 1 June 2013 and 15 October 2014 (median follow-up of 32.4 months). For this analysis, the 533 patients receiving DOACs were included [18–20]. GLORIA-AF was a large, prospective, global registry program run in three phases, assessing the long-term safety and effectiveness of dabigatran in patients with newly diagnosed AF in clinical practice. For this analysis, patients from phase II, enrolled between 2011 and 2014 with a mean follow-up of 18.0 months, were included [22–24]. ETNA-AF-Europe was a prospective, multicenter, postauthorization, observational study enrolling patients treated with edoxaban in ten European countries. Data from 852 sites that completed the 1-year follow-up (mean and median follow-up of 352 and 366 days, respectively) were analyzed [25].
With the exception of the ROCKET-AF trial, all other studies had an observational design. All studies were approved by the appropriate clinical research ethics committees. In each study, data were collected from the medical history and physician interview. Biodemographic data, comorbidities and thromboembolic and bleeding risk were recorded if available. Information regarding thromboembolic and bleeding events, as well as death, was recorded from all studies if available and expressed as annual rates (events per 100 patient-years).
Statistical analysis
A descriptive analysis was performed. Quantitative variables were described with mean and standard deviation and qualitative variables as absolute (n) and relative (%) frequencies. Outcomes were expressed as absolute (n) and relative (%) frequencies, as well as events per 100 patient-years. The data were analyzed using the statistical package SPSS (v18.0 or superior).
Results
EMIR study versus ROCKET-AF trial
In the EMIR study, a total of 1433 patients were included. Mean age was 74.2 years, 55.5% of patients were men, mean CHA2DS2-VASc score was 3.5 and HAS-BLED score was 1.6 (Table 1). Rates of stroke, MACE, cardiovascular death and major bleeding were 0.57, 1.07, 0.63 and 1.04 events per 100 patient-years, respectively (Table 2).
| EMIR study (n = 1433) | ROCKET-AF trial (rivaroxaban arm; n = 7131) | |
|---|---|---|
| Age (years) | 74.2 | 73 |
| Sex (men), n (%) | 795 (55.5) | 4300 (60.3) |
| Permanent atrial fibrillation, n (%) | 535 (37.5) | 5786 (81.1) |
| CHA2DS2-VASc score | 3.5 | – |
| CHADS2 score | – | 3.5 |
| HAS-BLED score | 1.6 | – |
| Hypertension, n (%) | 1137 (79.3) | 6436 (90.3) |
| Diabetes, n (%) | 388 (27.1) | 2878 (40.4) |
| Previous coronary disease, n (%) | 235 (16.4) | 1182 (16.6)† |
| Prior cerebrovascular disease, n (%) | 179 (12.5) | 3916 (54.9)‡ |
| Renal insufficiency (<60 ml/min/1.73m2), n (%) | 350 (24.7) | 1474 (20.7)§ |
| Underdosing, n (%) | 138 (9.7) | 0 |
| EMIR study (n = 1433) | ROCKET-AF trial (rivaroxaban arm; n = 7131) | |
|---|---|---|
| Stroke + systemic embolism n (%) Annual rate | 23 (1.6) 0.57 | 188 (2.6)† 1.7 |
| Major bleeding n (%) Annual rate | 29 (2.0) 1.04 | 395 (5.6) 3.6 |
| MACE n (%) Annual rate | 30 (2.1) 1.07 | 433 (6.13) 3.91 |
| Myocardial infarction n (%) Annual rate | 5 (0.3) 0.16 | 101 (1.43) 0.91 |
| Cardiovascular death n (%) Annual rate | 20 (1.4) 0.63 | 170 (2.41) 1.53 |
| Death from any cause n (%) Annual rate | 87 (6.1) 2.73 | 208 (2.95) 1.87 |
†
On treatment.
In the EMIR study, MACE were defined as a combination of nonfatal myocardial infarction, revascularization, cardiovascular death (death from coronary events, progressive heart failure death and sudden cardiac death). In the ROCKET-AF trial, MACE were defined as a combination of stroke, non-central nervous system embolism, vascular death, myocardial infarction.
MACE: Major adverse cardiovascular events.
In the ROCKET-AF trial, 7131 patients were included in the rivaroxaban arm. Median age was 73 years, 60.3% of patients were men, and mean CHADS2 score was 3.5 (Table 1). Rates of stroke or systemic embolism, MACE, cardiovascular death and major bleeding were 1.7, 3.91, 1.53 and 3.6 events per 100 patient-years, respectively (Table 2).
EMIR study versus observational Spanish studies of AF patients taking rivaroxaban, including the FANTASIIA study
A total of eight studies were included. The number of patients included in these studies ranged from 111 to 732 (total number: 2516; 3949 with the EMIR study). Mean age ranged from 74.9 to 78.4 years (vs 74.2 years in the EMIR study); CHA2DS2-VASc score ranged from 3.5 to 4.3 (vs 3.5 in the EMIR study), and HAS-BLED score ranged from 1.3 to 2.3 (vs 1.6 in the EMIR study; Table 3). Rates of stroke (the definition differed between studies) ranged from 0 to 1.8 (2.3 including transient ischemic attack) events per 100 patient-years (vs 0.57 in the EMIR study); major bleeding rates ranged from 0.22 to 4.2 events per 100 patient-years (vs 1.04 in the EMIR study); only one study reported data for MACE (2.0 vs 1.07 events per 100 patient-years, respectively) and two studies reported information about the rates of cardiovascular death (2.0 vs 0.63 events per 100 patient-years; Table 4). The study of Cerdá et al. [11] included patients taking not only rivaroxaban prospectively but also other DOACs. Rates of ischemic stroke and major bleeding are reported in Figure 1.
| EMIR study (n = 1433) | Brun et al. (n = 137) | Cerdá et al. (n = 663) | Gavin et al. (n = 243) | Perez Cabeza et al. (n = 111) | Muñiz et al. (n = 189) | Marti et al. (n = 230) | Pimentel et al. (n = 211) | Caro et al. (n = 732) | FANTASIIA direct oral anticoagulants (n = 533) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 74.2 | 78.2 | 77.8 | 78.4 | 74.9 | 76.0 | 76.9 | 76.7 | 76.4 | 73.3 |
| Sex (men), n (%) | 795 (55.5) | 82 (59.9) | 299 (45.1) | 128 (52.5) | 58 (52.3) | 93 (49.2) | 126 (54.8) | 104 (49.3) | 333 (45.5) | 287 (53.8) |
| Permanent atrial fibrillation, n (%) | 535 (37.5) | 77 (56.2) | – | – | 29 (26.2) | 124 (65.6) | – | – | 341 (46.6) | 222 (41.7) |
| CHA2DS2-VASc score | 3.5 | 3.5 | 4.0 | 3.7 | 3.6 | 4.1 | 4.3 | 3.8 | 3.9 | 3.67 |
| HAS-BLED score | 1.6 | – | – | – | 1.3 | 2.1 | 1.7 | 2.0 | 2.3 | 1.95 |
| Hypertension, n (%) | 1137 (79.3) | – | 564 (85.1) | 181 (74.6) | 93 (83.8) | – | 183 (79.6) | 175 (83.0) | 640 (87.5) | 425 (79.7) |
| Diabetes, n (%) | 388 (27.1) | – | 173 (26.1) | 63 (25.8) | 28 (25.2) | – | 87 (37.8) | 61 (29.0) | 194 (26.5) | 145 (27.2) |
| Previous coronary disease, n (%) | 235 (16.4) | – | – | – | 20 (18.0) | – | – | 27 (12.8) | 83 (11.3) | 79 (14.9) |
| Prior cerebrovascular disease, n (%) | 179 (12.5) | – | 123 (18.6) | – | 16 (14.4)† | 56 (29.6)† | 40 (17.4)† | 30 (14.2) | 123 (16.8) | 111 (20.9)† |
| Renal insufficiency (estimated glomerular filtration rate <60 ml/min/1.73 m2), n (%) | 350 (24.7) | 25 (18.2)‡ | 229 (34.5)‡ | 19 (17.1) | 42 (22.2)§ | 70 (30.5)‡ | 180 (24.6)‡ | 72 (13.5) | ||
| Underdosing, n (%) | 138 (9.7) | 43 (31.4) | 20 (3.0) | – | – | 12 (6.3) | 28 (12.2) | – | 88 (12.0) | 13 (7.0)¶ |
†
Prior stroke.
‡
Creatinine clearance <50 ml/min.
§
Estimated glomerular filtration rate <50 ml/ml/1.73m2.
¶
A substudy of FANTASIIA [18] showed that among 190 patients taking rivaroxaban, 13 (7.0%) were underdosed.
Underdosing of rivaroxaban was defined as taking rivaroxaban 15 mg/daily when creatinine clearance was ≥50 ml/min.
–: Not available.
Table created with data from [9–20].
| EMIR study (n = 1433) | Brun et al. (n = 137) | Cerdá et al. (n = 663) | Gavin et al. (n = 243) | Perez Cabeza et al. (n = 111) | Muñiz et al. (n = 189) | Marti et al. (n = 230) | Pimente et al. (n = 211) | Caro et al. (n = 732) | FANTASIIA direct oral anticoagulants (n = 533) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Stroke n (%) Annual rate | 23 (1.6) 0.57 | 0 | 5 (0.7)† 0.5 | – | 4 (3.6) – | – 0.45 | 2 (0.9) 0.4 | – 2.3‡ | 25 (3.4) 1.8 | – 0.40 |
| Major bleeding n (%) Annual rate | 29 (2.0) 1.04 | 5 (3.6) 1.43 | 9 (1.3) 0.8 | 6 (2.4) 1.7 | 0 | – 0.22 | 11 (4.8) 1.9 | – 4.2 | 44 (6.0) 3.2 | – 2.13 |
| MACE n (%) Annual rate | 30 (2.1) 1.07 | – | – | 7 (2.8) 2.0 | – | – | – | – | – | – – |
| Myocardial infarction n (%) Annual rate | 5 (0.3) 0.16 | – | – | – | 0 | – | – | – | 15 (2.0) 1.0 | – – |
| Cardiovascular death n (%) Annual rate | 20 (1.4) 0.63 | – | – | – | 2 (1.8) – | – | – | – | 28 (3.8) 2.0 | – 1.20 |
| Death from any cause n (%) Annual rate | 87 (6.1) 2.73 | – | – | – | – | – | – | 76 (10.4) 5.5 | – 3.77 |
†
Ischemic stroke.
‡
Stroke + transient ischemic attack.
In the EMIR study, MACE were defined as a combination of nonfatal myocardial infarction, revascularization, cardiovascular death (death from coronary events, progressive heart failure death and sudden cardiac death). Gavin et al. MACE, stroke, transient ischemic attack, systemic embolism or myocardial infarction.
MACE: Major adverse cardiovascular events; –: Not available.
Table created with data from [9–20].
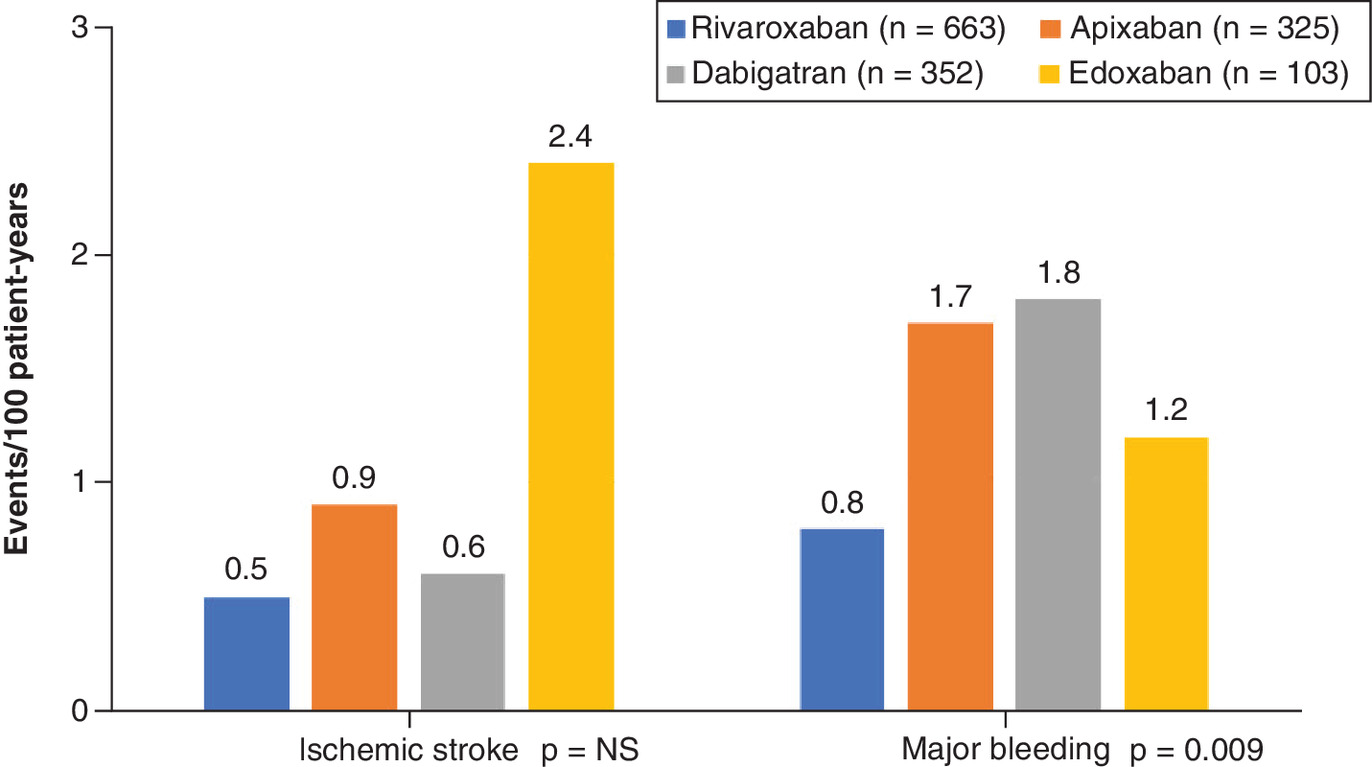
Figure 1. Main results of Cerdá et al. study.
NS: Not significant.
Figure created with data from [11].
Additionally, data from the FANTASIIA study were reported. In the FANTASIIA trial, 533 patients taking DOACs were analyzed. Mean age was 73.3 years, 53.8% of patients were men and mean CHA2DS2-VASc score was 3.67 (Table 3). Rates of stroke, cardiovascular death and major bleeding were 0.40, 1.20 and 2.13 events per 100 patient-years, respectively (Table 4).
EMIR study versus European prospective registries of patients taking DOACs
With regard to those registries of patients taking rivaroxaban, in the XANTUS study, mean age was 71.5 years (vs 74.2 years in the EMIR study) and CHA2DS2-VASc score was 3.4 (vs 3.5 in the EMIR stud; Table 5). Rates of stroke and major bleeding were 0.7 events per 100 patient-years (vs 0.57 in the EMIR study) and 2.1 events per 100 patient-years (vs 1.04 in the EMIR study), respectively. Additionally, in the XANTUS study, the rate of MACE was 1.8 events per 100 patient-years (vs 1.07 in the EMIR study; Table 6). When compared with other European studies in which other DOACs were analyzed (GLORIA-AF Europe and ETNA-AF Europe studies), mean age ranged from 73.0 years to 73.6 years (vs 74.2 years in the EMIR study), CHA2DS2-VASc score ranged from 3.0 to 3.1 (vs 3.5 in the EMIR study) and HAS-BLED score ranged from 1.0 to 2.5 (vs 1.6 in the EMIR study; Table 5). Rates of stroke (the definition differed between studies) ranged from 0.56 to 0.70 events per 100 patient-years (vs 0.57 in the EMIR study), major bleeding rates ranged from 0.87 to 1.05 events per 100 patient-years (vs 1.04 in the EMIR study) and the rates of cardiovascular death ranged from 0.92 to 1.63 events per 100 patient-years (vs 0.63 in the EMIR study; Table 6).
| EMIR, rivaroxaban (n = 1433) | XANTUS, rivaroxaban†† (n = 6784) | GLORIA-AF Europe, dabigatran‡‡ (n = 7108) | ETNA-AF Europe, edoxaban (n = 13,092) | |
|---|---|---|---|---|
| Age (years) | 74.2 | 71.5 | 73.0 | 73.6 |
| Sex (men), n (%) | 795 (55.5) | 4016 (59.2) | 3791 (53.3) | 7430 (56.8) |
| Permanent atrial fibrillation, n (%) | 535 (37.5) | 1835 (27.0) | 1019 (14.3) | 2864 (21.9) |
| CHA2DS2-VASc score | 3.5 | 3.4 | 3.0 | 3.1 |
| HAS-BLED score | 1.6 | – | 1.0 | 2.5 |
| Hypertension, n (%) | 1137 (79.3) | 5065 (74.7) | 5217 (73.4) | 10,088 (77.1) |
| Diabetes, n (%) | 388 (27.1) | 1333 (19.6) | 1510 (21.2) | 2879 (22.0) |
| Previous coronary disease, n (%) | 235 (16.4) | 688 (10.1)† | 1167 (16.4) | 560 (4.3)† |
| Prior cerebrovascular disease, n (%) | 179 (12.5) | 1291 (19.0)‡ | 1107 (15.6) | 778 (5.9)# |
| Renal insufficiency (<60 ml/min), n (%) | 350 (24.7) | 640 (9.4)§ | 89 (1.3)¶ | – |
| Underdosing, n (%) | 138 (9.7) | 572 (8.4) | – | – |
†
Myocardial infarction.
‡
Includes systemic embolism.
§
Creatinine clearance <50 ml/min.
¶
Defined as the presence of chronic dialysis or renal transplantation or serum creatinine ≥200 μmol/l.
#
Prior stroke.
††
In XANTUS, patients were enrolled from centres in Europe, Israel and Canada.
‡‡
Baseline
Characteristics correspond to the entire European population included in the study (n = 7108), not only those treated with dabigatran.
Underdosing of rivaroxaban was defined as taking rivaroxaban 15 mg/daily when creatinine clearance was ≥50 ml/min.
–: Not available.
| EMIR, rivaroxaban (n = 1433) | XANTUS, rivaroxaban‡ (n = 6784) | GLORIA-AF Europe, dabigatran (n = 2675) | ETNA-AF Europe, edoxaban (n = 13,092) | |
|---|---|---|---|---|
| Stroke n (%) Annual rate | 23 (1.6) 0.57 | 43 (0.6) 0.7 | 28 (1.0) 0.70 | 70 (0.5)† 0.56 |
| Major bleeding n (%) Annual rate | 29 (2.0) 1.04 | 128 (1.9) 2.1 | 35 (1.3) 0.87 | 132 (1.0) 1.05 |
| MACE n (%) Annual rate | 30 (2.1) 1.07 | 108 (1.6) 1.8 | – | – |
| Myocardial infarction n (%) Annual rate | 5 (0.3) 0.16 | 27 (0.4) 0.4 | 20 (0.7) 0.50 | 66 (0.5) 0.52 |
| Cardiovascular death n (%) Annual rate | 20 (1.4) 0.63 | 49 (0.7) – | 37 (1.4) 0.92 | 206 (1.6) 1.63 |
| Death from any cause n (%) Annual rate | 87 (6.1) 2.73 | 118 (1.7) 1.9 | 100 (3.7) 2.48 | 442 (3.4) 3.50 |
†
Ischemic stroke.
‡
In XANTUS, patients were enrolled from centres in Europe, Israel and Canada.
In the EMIR study, MACE were defined as a combination of nonfatal myocardial infarction, revascularization, cardiovascular death (death from coronary events, progressive heart failure death and sudden cardiac death). In the XANTUS study, MACE were defined as a combination of stroke, systemic embolism, transient ischemic attack, myocardial infarction.
MACE: Major adverse cardiovascular events; –: Not available.
Discussion
The EMIR study showed in a wide sample of real-life patients with AF that rivaroxaban was prescribed in elderly patients with a high thromboembolic risk. Despite that, rates of thromboembolic, cardiovascular and major bleeding events remained low. These numbers were in the range of or were even better than those reported in other national or international registries.
The ROCKET-AF trial was the study that included those patients with the highest thromboembolic risk and the greatest number of comorbidities when compared with the other pivotal clinical trials [7,26–28]. As a result, it was necessary to ascertain whether the results of the ROCKET-AF trial could be applied to real-life patients [8,29]. On the other hand, the clinical profile of patients for which rivaroxaban is prescribed has changed over time. Thus, as experience with rivaroxaban has increased, its prescription has been extended to the whole AF population, including those patients with a more challenging clinical profile [16,30]. In this context, the present study provided relevant and current information. In the EMIR study, patients were slightly older than in the ROCKET-AF trial, and despite the fact that they had a high thromboembolic risk and a great number of comorbidities, these were lower than in the ROCKET-AF trial [7,9]. Compared with other Spanish registries of patients taking rivaroxaban, the number of patients included in the EMIR study was markedly higher. Interestingly, overall, these studies showed that in Spain, rivaroxaban had been prescribed in elderly patients, with a high thromboembolic risk and a great number of conditions, in line with the data reported in the EMIR study [9–17]. Additionally, the XANTUS study exhibited a clinical profile similar to that of the EMIR study [21]. In summary, all these data are consistent and indicate that rivaroxaban is prescribed for the whole spectrum of the AF population, including patients with more complex disease.
In the EMIR study [9], the rate of stroke was low (0.57 events per 100 patient-years). This was much lower than that reported in the ROCKET-AF trial [7] but similar to that of the XANTUS study and other Spanish registries [10–17,21]. With regard to major bleeding, the EMIR study showed lower rates than those observed in the ROCKET-AF trial and some national and international registries of patients treated with rivaroxaban, such as the XANTUS study [7,9–17,21]. In addition, rates of stroke and bleeding events in the EMIR study were similar to those reported with other DOACs [7,18–20,22–25]. Although disparities in the clinical profiles of patients among the registries could explain, at least in part, some differences in the numbers, it should be emphasized that the EMIR study is a contemporary registry, and consequently, the more experience with the use of rivaroxaban and in the management of AF could have had some impact on the results. In fact, in the EMIR study, around 17% of patients were taking an inappropriate dose of rivaroxaban (vs 19% in the XANTUS study); underdosing was observed in 9.7% and 8.4% of patients, respectively [9,21]. In the Spanish observational studies, underdosing with rivaroxaban ranged from 3.0% to 31.4% [10–18]. These figures could be higher with other DOACs, likely related to the simplicity of dose adjustment with rivaroxaban, only depending on renal function [9,31,32]. Thus, in the FANTASIIA study, 32% of patients did not receive the proper dose [18]. In another study, underdosing was observed in one out of five patients taking DOACs [32]. This is very relevant, as underdosing is associated with an increased risk of stroke, without reducing the risk of bleeding [33,34]. As a result, prescribing the appropriate dose of DOACs according to the summary of product characteristics should be encouraged in order to provide the highest benefit [2].
The risk of MACE was specifically analyzed in the EMIR study [9]. Remarkably, despite anticoagulation, AF patients have a high risk for myocardial infarction or cardiovascular death [2,3]. In fact, the European guidelines recommend a comprehensive approach in the management of patients with AF that includes the prevention of not only thromboembolic events but also cardiovascular disease [2]. Unfortunately, this has not been fully analyzed in real-life studies. For example, only Gavin et al. and the XANTUS study specifically investigated this point, but not other registries, including those with other DOACs [12,21]. On the other hand, it is difficult to compare the rates of MACE among these studies, as the definition of MACE differed among them. In any case, the rate of MACE of the EMIR study was markedly lower than that of the ROCKET-AF trial and similar to those observed in the real-life studies with rivaroxaban [7,9,12,21]. As no head-to-head clinical trials between DOACs are available, observational studies can provide relevant information on the comparative effectiveness and safety of DOACs. However, these studies cannot be considered individually, since differences in the data can be the result of disparities in the clinical profile and methods [11,35]. By contrast, meta-analysis can show more accurate information. In this context, previous meta-analyses have reported that the use of rivaroxaban could be associated with a lower risk of ischemic events in the AF population [36–38].
This narrative review has some limitations. As no control groups are available in observational studies, no definite conclusions can be obtained from these studies (this occurred in national and international registries, including XANTUS, GLORIA-AF and ETNA-AF). However, these studies best reflect clinical practice, as no specific diagnostic or therapeutic intervention is performed for being included. On the other hand, data were taken from different studies, with particular inclusion criteria, follow-up and outcomes definitions. Therefore, only an indirect comparison can be performed between the studies and no more than hypothesis can be suggested. However, the high number of patients included throughout Spain and the robustness of the international registries may reduce these potential biases.
Conclusion
National and international registries confirm that in clinical practice, despite the fact that rivaroxaban is prescribed in elderly patients with a high thromboembolic risk and many comorbidities, rates of outcomes such as stroke, MACE, myocardial infarction, death and major bleeding are low. Therefore, rivaroxaban should be considered as a first-line therapy in the comprehensive management of patients with AF, to reduce the risk of not only thromboembolic complications but also cardiovascular disease. Using the appropriate dose of DOACs is highly recommended to obtain the maximum benefit.
Future perspective
Although the information provided by clinical trials is important, real-life studies are necessary to determine whether the results can be extended to the whole population [8]. Additionally, as observational studies cannot control all potential bias, it is important to compare data between different real-world evidence studies. In this context, as the information provided was consistent between different studies, we can conclude that rivaroxaban represents a good choice for anticoagulation in AF patients, even in elderly patients with many comorbidities.
•
The ROCKET-AF trial demonstrated that rivaroxaban was effective and safe in patients with atrial fibrillation (AF). However, it is important to analyze whether the results of the clinical trials can be extended to the real-life population.
•
The EMIR study included patients taking rivaroxaban over a 2.5-year period in Spain.
•
As observational studies cannot control all potential bias, it is also important to compare data between different real-world evidence studies.
•
This study's aim was to analyze the effectiveness and safety of rivaroxaban in patients with AF in clinical practice through different national and international registries.
•
In the EMIR study, a total of 1433 patients were included (mean age: 74.2 years; CHA2DS2-VASc: 3.5). Rates of stroke/systemic embolism, major adverse cardiovascular events, cardiovascular death and major bleeding were 0.57, 1.07, 0.63 and 1.04 events/100 patient-years, respectively.
•
Rates of outcomes were lower than those reported in the ROCKET-AF trial but were in line with those of the Spanish observational studies (rivaroxaban), XANTUS (rivaroxaban), FANTASIIA (any direct oral anticoagulant, in Spain), GLORIA-AF Europe (dabigatran) and ETNA-AF Europe (edoxaban).
•
In clinical practice, national and international registries consistently show that despite the fact that rivaroxaban is prescribed for elderly patients with a high thromboembolic risk, rates of outcomes such as stroke, major adverse cardiovascular events, myocardial infarction, death and major bleeding remain low.
Financial & competing interests disclosure
F Marín has received consultancy/lecturing fees from Bayer, Boehringer Ingelheim, Pfizer, Bristol Myers Squibb, Daiichi Sankyo and AFNET. M Sanmartín Fernández has received speaker and advisory fees from the following companies in the past 3 years: Bayer, Boehringer Ingelheim, BMS and Pfizer. I Lekuona has received honoraria for presentations from Bayer, Boehringer-Ingelheim, Daiichi Sankyo and Pfizer-BMS. F Arribas has received personal fees for educational activities or participation on boards from Daiichi Sankyo, Bayer, Boehringer Ingelheim and Bristol Myers Squibb. G Barón-Esquivas has received honoraria as advisor from Bayer, Daiichi-Sankyo, BMS-Pfizer and Rovi and honoraria as speaker from Boehringer-Ingelheim, Bayer, Daiichi-Sankyo, BMS and Pfizer. V Barrios has received consultancy/lecture fees from Bayer, BMS/Pfizer, Boehringer Ingelheim and Daiichi Sankyo. J Cosin-Sales has received consultancy/lecture fees from Bayer, BMS/Pfizer, Boehringer Ingelheim and Daiichi Sankyo. R Freixa-Pamias has received honoraria for presentations from Bayer, Boehringer-Ingelheim, Daiichi Sankyo and Pfizer-BMS. J Masjuan has received consultancy/lecturing fees from Bayer, Boehringer Ingelheim, Pfizer, Bristol Myers Squibb and Daiichi Sankyo. AI Pérez-Cabeza has received personal fees for educational activities or participation on boards from Daiichi Sankyo, Bayer, Boehringer Ingelheim and Bristol Myers Squibb. VR Schilling has received honoraria for presentations from Bayer, Boehringer-Ingelheim, Daiichi Sankyo and Pfizer-BMS. JMV Rodríguez has received lecturing fees from Bayer, Pfizer and Daiichi Sankyo. CR Priu is an employee of Bayer Hispania SL. MA Sánchez has received funding for consulting and conference services from Bayer, Daiichi-Sankyo and Pfizer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Writing and editorial assistance was provided by Content Ed Net (Madrid, Spain) with funding from Bayer Hispania.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Tsao CW, Aday AW, Almarzooq ZI et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics – 2022 update: a report from the American Heart Association. Circulation 145(8), e153–e639 (2022).
2.
Hindricks G, Potpara T, Dagres N et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio–Thoracic Surgery (EACTS). Eur. Heart J. 42(5), 373–498 (2021).
3.
Soliman EZ, Lopez F, O'Neal WT et al. Atrial fibrillation and risk of ST-segment-elevation versus non-ST-segment-elevation myocardial infarction: the Atherosclerosis Risk in Communities (ARIC) study. Circulation 131(21), 1843–1850 (2015).
• Atrial fibrillation is associated with an increased risk of incident myocardial infarction.
4.
Ruff CT, Giugliano RP, Braunwald E et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 383(9921), 955–962 (2014).
•• The benefit–risk profile of direct oral anticoagulants is superior to that of vitamin K antagonists.
5.
Cowan JC, Wu J, Hall M, Orlowski A, West RM, Gale CP. A 10-year study of hospitalized atrial fibrillation-related stroke in England and its association with uptake of oral anticoagulation. Eur. Heart J. 39(32), 2975–2983 (2018).
• The increase in anticoagulant use observed in England has been associated with a decline in hospitalized atrial fibrillation-related stroke rates.
6.
Díaz-Guzmán J, Freixa-Pamias R, García-Alegría J et al. Epidemiology of atrial fibrillation-related ischemic stroke and its association with DOAC uptake in Spain: first national population-based study 2005 to 2018. Rev. Esp. Cardiol. (Engl. Ed.) 75(6), 496–505 (2022).
• The greater use of direct oral anticoagulants has been associated with a decrease in the incidence of atrial fibrillation-related ischemic stroke in Spain.
7.
Patel MR, Mahaffey KW, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 365(10), 883–891 (2011).
•• In the ROCKET-AF trial, rivaroxaban was at least as effective as warfarin for the prevention of stroke or systemic embolism in the atrial fibrillation population, with a lower risk of fatal and intracranial bleeding.
8.
Barrios V, Escobar C. From clinical trials to clinical practice. Experience with rivaroxaban in the anticoagulant treatment of patients with non-valvular atrial fibrillation. Semergen. 43(3), 222–229 (2017).
9.
Sanmartin-Fernández M, Marín F, Rafols C et al. Thromboembolic and bleeding events with rivaroxaban in clinical practice in Spain: impact of inappropriate doses (the EMIR study). J. Comp. Eff. Res. 10(7), 583–593 (2021).
• In clinical practice, rivaroxaban is properly dosed in most patients.
10.
Brun Guinda D, Callen García Ó, Ondiviela Pérez J et al. Clinical profile, management and outcomes in a cohort of elderly and highly comorbid patients with nonvalvular atrial fibrillation treated with rivaroxaban in routine practice. Future Cardiol. 14(Suppl. 3), S39–S45 (2018).
11.
Cerdá M, Cerezo-Manchado JJ, Johansson E et al. Facing real-life with direct oral anticoagulants in patients with nonvalvular atrial fibrillation: outcomes from the first observational and prospective study in a Spanish population. J. Comp. Eff. Res. 8(3), 165–178 (2019).
12.
Gavín Sebastián O, Izuzquiza Fernández M, Martínez Fernández R, Palomera Bernal L. Anticoagulation with rivaroxaban in a hematology unit: clinical profile, events and discontinuation rates in real-life patients with nonvalvular atrial fibrillation. Future Cardiol. 14(Suppl. 3), S25–S30 (2018).
13.
Pérez Cabeza AI, González Correa JA, Chinchurreta Capote PA et al. Drug persistence and outcomes in a cohort of patients with nonvalvular atrial fibrillation treated with rivaroxaban after 2 years of follow-up in clinical practice. Future Cardiol. 14(Suppl. 3), S9–S16 (2018).
14.
Muñiz Lobato S, Tarrazo Tarrazo C, González Fernández E, Morán Alcalá M. Clinical profile, adequacy of dosage and thromboembolic and bleeding outcomes in patients with nonvalvular atrial fibrillation treated with rivaroxaban in a regional hospital of Asturias, Spain. Future Cardiol. 14(Suppl. 3), S17–S24 (2018).
15.
Martí E, Segado A, Pastor-Galán I et al. Use of rivaroxaban for the prevention of stroke in patients with nonvalvular atrial fibrillation in Spain. Future Cardiol. 14(Suppl. 3), S3–S8 (2018).
16.
Pimentel Quezada Y, Bonilla Palomas JL, Gámez López AL et al. Has the clinical profile of patients with nonvalvular atrial fibrillation treated with rivaroxaban changed in the last 5 years of use? Future Cardiol. 14(Suppl. 3), S47–S53 (2018).
17.
Caro Martinez C, Cerezo Manchado JJ, Flores Blanco PJ et al. Effectiveness and safety of rivaroxaban in nonvalvular atrial fibrillation: data from a contemporary Spanish registry. Curr. Med. Res. Opin. 35(8), 1463–1471 (2019).
18.
Ruiz Ortiz M, Muñiz J, Raña Míguez P et al. Inappropriate doses of direct oral anticoagulants in real-world clinical practice: prevalence and associated factors. A subanalysis of the FANTASIIA registry. Europace 20(10), 1577–1583 (2018).
19.
Anguita Sánchez M, Bertomeu Martínez V, Ruiz Ortiz M et al. Direct oral anticoagulants versus vitamin K antagonists in real-world patients with nonvalvular atrial fibrillation. The FANTASIIA study. Rev. Esp. Cardiol. 73(1), 14–20 (2020).
20.
Ruiz Ortiz M, Esteve-Pastor MA, Roldán I, Muñiz J, Marín F, Anguita M. FANTASIIA study investigators. Prognostic impact of inappropriate doses of direct oral anticoagulants in clinical practice. Rev. Esp. Cardiol. (Engl. Ed.) 73(4), 329–330 (2020).
21.
Camm AJ, Amarenco P, Haas S et al. XANTUS: a real-world, prospective, observational study of patients treated with rivaroxaban for stroke prevention in atrial fibrillation. Eur. Heart J. 37(14), 1145–1153 (2016).
•• XANTUS was the first international, prospective and observational study that described the use of rivaroxaban in clinical practice, showing low rates of stroke and major bleeding.
22.
Mazurek M, Teutsch C, Diener HC et al. Safety and effectiveness of dabigatran at 2 years: final outcomes from phase II of the GLORIA-AF registry program. Am. Heart J. 218, 123–127 (2019).
23.
Huisman MV, Lip GY, Diener HC et al. Design and rationale of global registry on long-term oral antithrombotic treatment in patients with atrial fibrillation: a global registry program on long-term oral antithrombotic treatment in patients with atrial fibrillation. Am. Heart J. 167(3), 329–334 (2014).
24.
Mazurek M, Huisman MV, Rothman KJ et al. Regional differences in antithrombotic treatment for atrial fibrillation: insights from the GLORIA-AF phase II registry. Thromb. Haemost. 117(12), 2376–2388 (2017).
25.
de Groot JR, Weiss TW, Kelly P et al. Edoxaban for stroke prevention in atrial fibrillation in routine clinical care: 1-year follow-up of the prospective observational ETNA-AF-Europe study. Eur. Heart. J. Cardiovasc. Pharmacother. 7(FI1), f30–f39 (2021).
26.
Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 361(12), 1139–1151 (2009).
27.
Granger CB, Alexander JH, McMurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 365(11), 981–992 (2011).
28.
Giugliano RP, Ruff CT, Braunwald E et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 369(22), 2093–2104 (2013).
29.
Barón-Esquivias G, Marín F, Sanmartín Fernandez M. Rivaroxaban in patients with atrial fibrillation: from ROCKET AF to everyday practice. Expert Rev. Cardiovasc. Ther. 15(5), 403–413 (2017).
30.
Anguita M, de la Figuera M, Cabeza AIP, Fernández CS. Clinical profile and management of rivaroxaban in patients with atrial fibrillation in routine practice in Spain: data from six nationwide studies. Drugs Context 8, 212606 (2019).
31.
Salameh M, Gronich N, Stein N et al. Stroke and bleeding risks in patients with atrial fibrillation treated with reduced apixaban dose: a real-life study. Clin. Pharmacol. Ther. 108(6), 1265–1273 (2020).
32.
Tütüncü S, Olma M, Kunze C et al. Off-label-dosing of non-vitamin K-dependent oral antagonists in AF patients before and after stroke: results of the prospective multicenter Berlin Atrial Fibrillation Registry. J. Neurol. 269(1), 470–480 (2022).
33.
Santos J, António N, Rocha M, Fortuna A. Impact of direct oral anticoagulant off-label doses on clinical outcomes of atrial fibrillation patients: a systematic review. Br. J. Clin. Pharmacol. 86(3), 533–547 (2020).
34.
Escobar C, Martí-Almor J, Pérez Cabeza A, Martínez-Zapata MJ. Direct oral anticoagulants versus vitamin K antagonists in real-life patients with atrial fibrillation. A systematic review and meta-analysis. Rev. Esp. Cardiol. (Engl. Ed.) 72(4), 305–316 (2019).
• This meta-analysis suggested that in clinical practice, only rivaroxaban significantly reduced the risk of stroke compared with warfarin.
35.
Esteve-Pastor MA, Rivera-Caravaca JM, Ruiz-Ortiz M, Muñiz J et al. A comparison of front-line oral anticoagulants for the treatment of non-valvular atrial fibrillation: effectiveness and safety of direct oral anticoagulants in the FANTASIIA registry. Expert Opin. Pharmacother. 23(12), 1457–1465 (2022).
36.
Mahaffey KW, Stevens SR, White HD et al. Ischaemic cardiac outcomes in patients with atrial fibrillation treated with vitamin K antagonism or factor Xa inhibition: results from the ROCKET AF trial. Eur. Heart J. 35(4), 233–241 (2014).
37.
Chatterjee S, Sharma A, Uchino K, Biondi-Zoccai G, Lichstein E, Mukherjee D. Rivaroxaban and risk of myocardial infarction: insights from a meta-analysis and trial sequential analysis of randomized clinical trials. Coron. Artery Dis. 24(8), 628–635 (2013).
38.
Coleman CI, Baker WL, Meinecke AK et al. Effectiveness and safety of rivaroxaban vs. warfarin in patients with non-valvular atrial fibrillation and coronary or peripheral artery disease. Eur. Heart. J. Cardiovasc. Pharmacother. 6(3), 159–166 (2020).
Information & Authors
Information
Published In
Pages: 1173 - 1184
PubMed: 36148923
Copyright
© 2022 Future Medicine Ltd.
History
Received: 14 June 2022
Accepted: 5 September 2022
Published online: 23 September 2022
Keywords:
Topics
Authors
Funding Information
Bayer Hispania: NA
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Rivaroxaban for the prevention of outcomes in patients with atrial fibrillation in clinical practice: an indirect comparison of national and international registries. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0111
Export citation
Select the citation format you wish to export for this article or chapter.