Cost–effectiveness analysis of prolonged-release fampridine to treat walking disability of multiple sclerosis in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Objectives: This study evaluates the cost–effectiveness of adding prolonged-release (PR)-fampridine to best supportive care (BSC) versus BSC alone in adult multiple sclerosis patients with walking disability in China. Materials & methods: A hybrid decision tree and Markov model from both the societal and healthcare perspectives were constructed. Parameters were derived from clinical trials of PR-fampridine, published sources and clinical expert interviews. Results: Over a 10-year time horizon, adding PR-fampridine to BSC led to 0.15 quality-adjusted life year (QALY) gain and lower costs, with incremental cost–effectiveness ratios of -238,806 Chinese Yuan/QALY and -113,488 Chinese Yuan/QALY from the societal and healthcare perspectives, respectively. Conclusion: Compared with BSC alone, PR-fampridine plus BSC is considered an economically dominant strategy for the treatment of multiple sclerosis-related walking disability in China.
Multiple sclerosis (MS) is a chronic autoimmune disease characterized by the destruction of the myelin sheath within the central nervous system, affecting about 2.8 million people globally [1]. MS was listed in China's ‘First Category of Rare Disease’, which was jointly formulated by five national authorities (e.g., the National Health Commission, Ministry of Science and Technology) in 2018 and contained a total of 121 rare diseases [2]. A nationwide, population-based study based on the claims data in six provinces showed that the prevalence of MS in urban China was 2.44/100,000 in 2016 [3], which means there might be more than 30,000 patients with MS in China. Meanwhile, MS is highly prevalent in the young and middle-aged populations from 20 to 50 years old in China [4].
Walking disability is a common impairment in MS patients, with negative impact on quality of life and the activities of daily living of patients and caregivers. An online survey with 436 MS patients from six European countries showed that nearly half of patients (45%) experienced walking disability within the first month of diagnosis and almost all of them (93%) reported walking disability within the 10-year time horizon after diagnosis [5]. Several studies showed that MS caused significant economic burden to the society [6–8], especially for the direct non-medical costs and indirect costs of patients. MS interfered with patients' ability to work or made them unable to work, leading to the loss of productivity [9]. An online survey including 1011 MS patients in the USA showed that only 34% of MS patients with walking disability were employed [9]. Maintaining walking ability was identified as one of the highest priorities among MS patients [10].
Prolonged-release (PR)-fampridine was approved as the first and only pharmacotherapy for the treatment of MS-related walking disability in adult patients with Expanded Disability Status Scale (EDSS) scores 4–7 in May 2021 in China. It was listed in the National Reimbursement Drug List (NRDL) in the same year. PR-fampridine is a broad-spectrum K+ channel blocker and can increase the conduction of action potentials in demyelinated axons through inhibition of K+ channels. It can be used concomitantly with any MS disease-modifying therapy, physiotherapy and other supportive drugs in patients with any subtype of MS [11]. Before the approval of PR-fampridine, MS-related walking disability was managed by best supportive care (BSC) only. As mentioned in the Chinese Expert Consensus, BSC mainly includes other symptomatic treatment (e.g., antidepressants and antianxiety medications), rehabilitation therapy (functional rehabilitation training and MS-related outpatient treatment and hospitalization) [12].
Several clinical trials have demonstrated that PR-fampridine can improve walking ability in MS patients [13–16]. A pooled analysis of two randomized, multicenter, double-blind, controlled, phase III trials (MS-F203 and MS-F204), aiming to evaluate the efficacy and safety of PR-fampridine, showed that PR-fampridine had a significantly higher proportion of timed 25-foot walk (T25FW) responders relative to placebo (37.6 vs 8.9%; p < 0.0001) in MS patients of any phenotype [13]. Long-term extension studies (MS-F203EXT and MS-F204EXT) also provided evidence for the long-term safety and tolerability of PR-fampridine [14]. A phase II, randomized, double-blind trial (MOBILE) and a phase III, randomized, double-blind trial (ENHANCE) both used improvement in scores of the 12-item Multiple Sclerosis Walking Scale (MSWS-12) over the 24-week treatment period as the primary end point [15,16]. In the MOBILE trial, a significantly higher proportion of patients achieved clinically meaningful improvement in MSWS-12 score in the PR-fampridine group versus the placebo group (48.5 vs 28.1%; p = 0.0153). The ENHANCE trial also showed a much better result in the PR-fampridine group compared with the placebo group (43.2 vs 33.6%; p = 0.006). In addition, the results of the MOBILE trial demonstrated that PR-fampridine can bring clinically meaningful improvements to patients' quality of life [15].
A previous economic study in Sweden and two health technology appraisal reports in the UK showed that PR-fampridine improved patients' quality of life, reduced healthcare resource utilization and was considered a cost-effective treatment for MS-related walking disability [17–19]. However, the cost–effectiveness evidence is lacking for adding PR-fampridine to BSC in China. To fill this gap, the present study aims to evaluate the cost–effectiveness of adding PR-fampridine to BSC versus BSC alone for the improvement of walking ability in adult MS patients with EDSS scores 4–7 in China.
Materials & methods
Clinical experts' in-depth interviews
In order to better understand the treatment pattern, treatment pathway and utilization of healthcare resources in MS patients with walking disability in the Chinese clinical context, a structured questionnaire was designed in this study (Supplementary Material 1). The questionnaire aimed to obtain the healthcare utilization of MS walking disability, validate the structure and assumptions of the model and confirm the accuracy of the information from the literature. The questionnaire mainly involved the following contents: 1) supportive symptomatic treatments for MS patients: treatment types, proportion of usage and treatment duration; 2) utilization of healthcare resources: rehabilitation (type and frequency), outpatient visits, inpatient care, medical examinations and tests (type and frequency); 3) direct nonmedical costs and indirect costs: use of walking aids (wheelchair, crutches etc.) and productivity losses of patients and caregivers; 4) to validate the relationships of walking speed (measured by T25FW) with healthcare resource utilization, use of walking aids and productivity losses of patients and caregivers.
The interviewed physicians were selected based on their treatment experience and locations. A total of 11 clinical experts from neurology or physiatry departments of tertiary A-level hospitals in Beijing, Shanghai, Guangzhou, Tianjin, Nanjing, Chengdu and Harbin were interviewed. All interviewees were associate chief or chief physicians with above 10 years of clinical experience in diagnosing and treating MS.
Patient population
The target population for the model consisted of a cohort of Chinese adult MS patients with walking disability (EDSS scores 4–7). For the base case analysis, the starting age of the modeled cohort was calculated integrating the mean diagnosis age of MS in China from published research [20] and the mean duration of 170 months from the diagnosis of MS to the use of PR-fampridine which was reported in the ENHANCE trial [16]. Other baseline characteristics (% of males and T25FW) were derived from published literature [21] and MS-F203 and MS-F204 trials (Table 1) [22,23].
| Characteristic | Estimates | Source | Ref. |
|---|---|---|---|
| Mean diagnosis age of multiple sclerosis (years) | 34.1 | 2020 Comprehensive Social Survey Report of Multiple Sclerosis Patients in China | [20] |
| Gender (% males) | 36% | Tian et al. | [21] |
| Time from disease diagnosis to taking prolonged-release-fampridine (months) | 170 | ENHANCE trial | [16] |
| Timed 25-foot walk at baseline (feet/s) | 2.1 | Pooled results of MS-F203 and MS-F204 trials | [22,23] |
Model structure
A cost–effectiveness analysis was conducted based on a hybrid decision tree and Markov model from both the societal and healthcare perspectives in a 10-year time horizon. This took the form of a decision tree for response assessment for the first 4 weeks, followed by a Markov model with a cycle length of 4 weeks and allowed health outcomes and costs to be accumulated over time. Both quality-adjusted life year (QALY) and costs were discounted at a rate of 5%, and a half-cycle correction was applied, as recommended by the Chinese pharmacoeconomics guidelines [24].
The model structure was consistent with the previous economic study in Sweden [17], which consisted of two arms corresponding to the two treatment strategies: 1) PR-fampridine and BSC and 2) BSC alone. Patients receiving PR-fampridine could either remain in or transit to one of the three health states: ‘response to treatment’, ‘withdrawal from treatment’ or ‘death’ (the absorbing state). Patients treated with BSC could either remain in the ‘continue treatment with BSC’ health state or transition to ‘death’. The model structure is shown in Figure 1.

Figure 1. Model structure.
BSC: Best supportive care.
Clinical inputs
In the base case analysis of the model, treatment response was defined as a mean improvement in MSWS-12 scale of ≥8 points from baseline, which was reported as the primary end point in the ENHANCE trial [16]. The response rate was applied at the end of the decision tree to calculate the first 4 weeks' effectiveness of PR-fampridine.
It is worth noting that disease progression in the Markov model was measured by T25FW instead of MSWS-12. There were several reasons for this change: 1) efficacy data evaluated by MSWS-12 were limited to 24 weeks only and long-term efficacy data measured by MSWS-12 were not available; 2) T25FW is a meaningful end point of measuring walking ability and the pooled analysis of MS-F203 EXT and MS-F204 EXT reported long-term T25FW data of PR-fampridine responders up to 60 months [14]; and 3) no data showed the relationship between MSWS-12 and healthcare resource utilization. Instead, a cross-sectional, patient record-based study in five European countries demonstrated that there was a specific relationship between T25FW and healthcare resource utilization in MS patients [25]. As no clinical trial of PR-fampridine was able to provide long-term T25FW data for the BSC-alone group or patients who withdrew from PR-fampridine, T25FW data for this population were obtained from the placebo arm of the IMPACT trial and ASCEND trial [26,27]. It was assumed that the pooled results of the placebo arms in the IMPACT trial and ASCEND trial could demonstrate the natural history of MS under BSC (Figure 2). Meanwhile, as no dataset was identified to provide walking speed progression for MS patients up to 10 years, weighted linear regression was applied to extrapolate T25FW
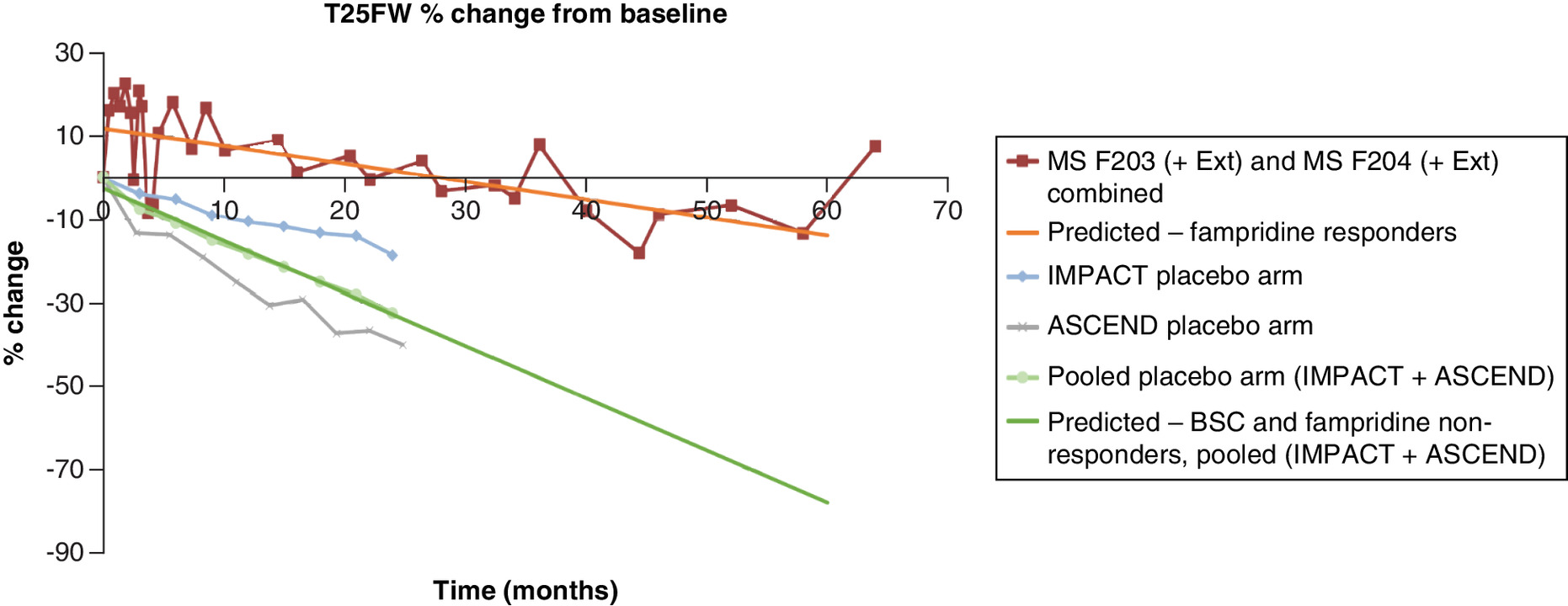
Figure 2. Long-term timed 25-foot walk extrapolated using a linear regression.
BSC: Best supportive care; MS: Multiple sclerosis.
Goodman et al., reported a pooled 5-year retention probability of PR-fampridine responders as 62.1% from the extension studies of MS-F203 and MS-F204 [14]. This 5-year probability was converted and then used to estimate the withdrawal probability for each 4-week cycle. For patients who withdrew from PR-fampridine, the present model assumed that they lost all treatment effect from PR-fampridine. In other words, the patients who withdrew from PR-fampridine were assumed to have the same utility score as the baseline value of responders at week 0.
Adverse events
Adverse event (AE) data were taken from the ENHANCE and MOBILE trials [15,16]. The criteria for AEs included in the analysis were an incidence in either group of ≥5% and incidence in the PR-fampridine group higher than that in the placebo group. In addition, there were no serious AEs in either group. Table 2 shows the pooled results of each AE during the 26-week follow-up period; the probability of each AE's occurrence per cycle was converted and used in the model.
| Urinary tract infection (%) | Fall (%) | Back pain (%) | |
|---|---|---|---|
| Prolonged-release-fampridine plus best supportive care | 12.2 | 7.3 | 5.7 |
| Best supportive care alone | 11.0 | 7.0 | 3.7 |
Health state utility values & AE disutility
The utility data were also derived from the ENHANCE and MOBILE trials [15,16]. The pooled results of these two trials were used in the model as the base case analysis. The ENHANCE trial used a three-level classification system of the EuroQol 5 dimensions (EQ-5D-3L) and collected utility at baseline and weeks 2, 4 and 24 for PR-fampridine responders, nonresponders and the placebo arm. The MOBILE trial used a five-level classification system of EQ-5D (EQ-5D-5L) and collected utility at baseline and weeks 4, 8, 12, 16 and 24 for PR-fampridine responders, non-responders and the placebo arm. Before pooling these datasets, the authors first used the crosswalk approach to map the EQ-5D-5L data in the MOBILE trial to the EQ-5D-3L value sets and then calculated the utility index score [28]. The last observation carried forward method was used to impute the missing data within 24 weeks for both the ENHANCE and MOBILE trials. The imputed value data from the ENHANCE and MOBILE trials are displayed in Supplementary Table 1. Finally, the utility value at each time point from the two trials were pooled by weighted averaging. In the model, extrapolation of utility to the selected time horizon also used the last observation carried forward method. Table 3 presents the utility of responders and non-responders/BSC used in the base case analysis.
| Time point | Prolonged-release-fampridine responders | Prolonged-release-fampridine nonresponders and the best supportive care group |
|---|---|---|
| Baseline | 0.634 | 0.601 |
| Week 2 | 0.664 | 0.637 |
| Week 4 | 0.688 | 0.621 |
| Week 8 | 0.691 | 0.618 |
| Week 12 | 0.693 | 0.616 |
| Week 16 | 0.693 | 0.613 |
| Week 20 | 0.691 | 0.617 |
| Week 24+ | 0.683 | 0.617 |
Utility decrements due to AEs were also included in the model. The utility decrements of urinary tract infection, fall and back pain were obtained from a published study with values of -0.0054, -0.1145 and -0.0866, respectively [29].
Cost inputs & resource use
Costs included in the model were categorized as drug costs, healthcare resource utilization costs, costs of walking aids and productivity loss of caregivers and patients. The latest price (as of February 2022, price after the 2021 NRDL negotiation) of PR-fampridine obtained from the provincial tendering platform was used to calculate the drug costs of PR-fampridine. The BSC consisted of other supportive drugs, examinations and lab tests, hospitalization, rehabilitation, neurologist visits and other outpatient visits. The PR-fampridine plus BSC strategy considered the drug cost and AE management cost of PR-fampridine additionally (Table 4). Costs of walking aids and productivity loss were also included in the societal perspective (Table 4). Unit costs were obtained from published sources and utilization of healthcare resources was obtained from clinical experts' in-depth interviews. All costs from previously published studies were inflated to 2021.
| Item | Unit cost (Chinese Yuan) | Source | Ref. |
|---|---|---|---|
| Drug costs | |||
| Prolonged-release-fampridine (10 mg) | 16.1 | Latest bidding price from provincial tendering platform (as of February 2022) | |
| Best supportive care costs (annual) | |||
| Neurologist visits | 920.83 | Charging standard for healthcare service in China; clinical expert interviews | |
| Rehabilitation | 42,931.04 | Charging standard for healthcare service in China; clinical expert interviews | |
| Other outpatient visits | 1146.81 | Charging standard for healthcare service in China; clinical expert interviews | |
| Multiple sclerosis-related hospitalization | 10,000.00 | Blue Book on Health Insights of Multiple Sclerosis Patients; 2021 Quality of Life Report for Multiple Sclerosis Patients in China | [4] |
| Other supportive drugs | 4377.59 | Latest bidding price from provincial tendering platform (as of February 2022); clinical expert interviews | |
| Tests and examinations | 5973.37 | Charging standard for healthcare service in China | |
| Adverse event costs (one-time) | |||
| Urinary tract infection | 120.27 | Chen et al. | [30] |
| Fall | 609.28 | Peng et al. | [31] |
| Back pain | 104.58 | Ji et al. | [32] |
| Direct nonmedical cost (annual) (societal perspective only) | |||
| Walking aids | 456.56 | The price of the product with the highest online sales | |
| Indirect cost (annual) (societal perspective only) | |||
| Loss of productivity (patients) | 7041.35 | 2020 Comprehensive Social Survey Report of Multiple Sclerosis Patients in China | [20] |
| Loss of productivity (caregivers) | 17,528.22 | Calculated based on the average salary of employees in urban nonprivate units in China in 2020 and the proportion of multiple sclerosis patients who need caregivers from clinical expert interviews | [33] |
A patient record-based study in five European countries (the Adelphi study) quantitatively analyzed the relationship between walking ability (measured by T25FW) and the costs of healthcare resource utilization and indirect costs [25]. This study collected T25FW scores in MS patients and conducted a regression analysis between healthcare resource utilization and T25FW. Patients with greater walking disability used significantly more healthcare resources (especially for caregiver support and physician visits) than those with improved walking ability. However, at present, there is a lack of data about healthcare resources at different walking ability in Chinese MS patients. According to the opinions of clinical experts, collected in the in-depth interviews, the resource use in patients with different walking ability was different indeed. Therefore, based on the regression analysis results of the frequency of healthcare resource utilization and the T25FW reported in the Adelphi study, combined with the BSC in China, the present study calculated the healthcare resource utilization of patients with different T25FW segments. The trend and relative scales were further verified in Chinese clinical expert interviews. The trend and relative scales are listed in Tables 5 & 6.
| Timed 25-foot walks | Neurologist visits (%) | Rehabilitation (%) | Other outpatient visits (%) | Multiple sclerosis-related hospitalization (%) | Other supportive drugs (%) | Tests and examinations (%) |
|---|---|---|---|---|---|---|
| 10–12 | 100 | 93 | 98 | 100 | 93 | 100 |
| 12 (baseline) | 100 | 100 | 100 | 100 | 100 | 100 |
| 12–15 | 100 | 115 | 105 | 100 | 115 | 100 |
| 16–20 | 99 | 129 | 109 | 100 | 129 | 99 |
| 21–30 | 99 | 146 | 114 | 100 | 146 | 99 |
| 31–60 | 99 | 165 | 121 | 100 | 165 | 99 |
| >60 | 99 | 187 | 128 | 100 | 187 | 99 |
The first column presents the time needed to complete 25 feet as quickly as possible.
| Timed 25-foot walks | Walking aids (%) | Loss of earnings (%) | Needs of caregivers (%) |
|---|---|---|---|
| 10–12 | 95 | 98 | 91 |
| 12 (baseline) | 100 | 100 | 100 |
| 12–15 | 110 | 104 | 119 |
| 16–20 | 117 | 106 | 136 |
| 21–30 | 126 | 109 | 153 |
| 31–60 | 134 | 112 | 172 |
| >60 | 143 | 116 | 190 |
The first column presents the time needed to complete 25 feet as quickly as possible.
Scenario analysis
Different scenarios were set to explore the impact of a longer time horizon and different sources of utility values. First, the time horizon was prolonged to 20 years to assess long-term outcomes. Also, utility data from two trials were included separately to replace the pooled utility data. The imputed utility values from the ENHANCE trial and MOBILE trial [15,16] were considered in the second and third scenarios, separately.
Sensitivity analysis
Uncertainty was assessed by one-way and probabilistic sensitivity analyses. To test an individual parameter's impact on the results, one-way sensitivity analysis was run for every parameter in the model, in which one specific parameter was varied while others were held constant each time. The ranges tested were based on the statistical uncertainty around the estimates when available. Otherwise, the variance was set as ±20% for all parameters except for the discount rate (0% and 8% were used) as recommended by the Chinese pharmacoeconomics guidelines [24].
The model also included probabilistic sensitivity analysis, in which all parameters estimated with uncertainty were independently and simultaneously varied and drawn from an appropriately assigned probability distribution. Beta distribution was assigned for effectiveness and utility values and gamma distribution was assigned for cost inputs and resource use. The resampling process was repeated for a selected number of iterations (the default setting was 5000 iterations) during the Monte-Carlo simulation. Uncertainty around model parameter estimates was based on their calculated or reported patient counts, standard deviations or ranges, depending on the parameter.
Results
Base case results
The base case analysis used a 10-year time horizon and the response rate from the ENHANCE trial. The QALY difference between PR-fampridine plus BSC and BSC alone was calculated based on the pooled EQ-5D values of the ENHANCE and MOBILE trials.
Over a 10-year time horizon, adding PR-fampridine to BSC led to an incremental QALY gain of 0.15 and lower total costs of -17,329 Chinese Yuan (CNY) from the healthcare perspective, which dominated BSC only with an incremental cost–effectiveness ratio of -113,488 CNY/QALY. The addition of PR-fampridine reduced the cost of healthcare resource utilization, especially the costs of rehabilitation and other supportive drugs (Table 7). From the societal perspective, adding PR-fampridine to BSC led to lower total costs of -36,465 CNY and dominated BSC with an incremental cost–effectiveness ratio of -238,806 CNY/QALY. The PR-fampridine plus BSC strategy presented lower costs for walking aids and productivity loss of patients and caregivers (Table 7).
| Prolonged-release-fampridine plus best supportive care | Best supportive care | |
|---|---|---|
| Prolonged-release-fampridine drug cost (CNY) | 27,769 | 0 |
| Neurologist visits (CNY) | 7119 | 7104 |
| Rehabilitation (CNY) | 493,090 | 533,815 |
| Other outpatient visits (CNY) | 10,282 | 10,627 |
| Tests and examinations (CNY) | 46,180 | 46,081 |
| Other supportive drugs (CNY) | 50,279 | 54,432 |
| Multiple sclerosis-related hospitalization (CNY) | 78,050 | 78,069 |
| Adverse event costs (CNY) | 977 | 947 |
| Total costs from the healthcare perspective (CNY) | 713,746 | 731,075 |
| Loss of productivity in patients (CNY) | 54,646 | 55,824 |
| Loss of productivity in caregivers (CNY) | 206,720 | 224,455 |
| Walking aids (CNY) | 4439 | 4662 |
| Total costs from the societal perspective (CNY) | 979,551 | 1,016,016 |
| Total QALY (QALYs) | 4.94 | 4.79 |
| Incremental | ||
| Δ Cost from the healthcare perspective (CNY) | -17,329 | / |
| Δ Cost from the societal perspective (CNY) | -36,465 | / |
| Δ QALY (QALYs) | 0.15 | / |
| Incremental cost–effectiveness ratio from the healthcare perspective (CNY/QALY) | Dominant (-113,488) | / |
| Incremental cost–effectiveness ratio from the societal perspective (CNY/QALY) | Dominant (-238,806) | / |
CNY: Chinese Yuan; QALY: Quality-adjusted life year.
Scenario analysis results
The results of longer time horizon and different utility data from the healthcare and societal perspectives are reported in Table 8. In all scenarios, PR-fampridine plus BSC dominated BSC alone. When the utilities at different time points were obtained from the MOBILE trial, adding PR-fampridine to BSC led to more incremental QALY gain (0.39 QALY) than that in the base case (0.15 QALY).
| Prolonged-release-fampridine plus best supportive care | Best supportive care | |
|---|---|---|
| Scenario 1: 20-year time horizon | ||
| Total costs from the healthcare perspective (CNY) | 1,175,633 | 1,193,502 |
| Total costs from the societal perspective (CNY) | 1,586,671 | 1,625,765 |
| Total QALY (QALYs) | 7.63 | 7.45 |
| ICER from the healthcare perspective (CNY/QALY) | Dominant (-96,522) | / |
| ICER from the societal perspective (CNY/QALY) | Dominant (-211,175) | / |
| Scenario 2: utilities from ENHANCE trial | ||
| Total costs from the healthcare perspective (CNY) | 713,746 | 731,075 |
| Total costs from the societal perspective (CNY) | 979,551 | 1,016,016 |
| Total QALY (QALYs) | 5.02 | 4.92 |
| ICER from the healthcare perspective (CNY/QALY) | Dominant (-169,756) | / |
| ICER from the societal perspective (CNY/QALY) | Dominant (-357,210) | / |
| Scenario 3: utilities from MOBILE trial | ||
| Total costs from the healthcare perspective (CNY) | 713,746 | 731,075 |
| Total costs from the societal perspective (CNY) | 979,551 | 1,016,016 |
| Total QALY (QALYs) | 4.53 | 4.14 |
| ICER from the healthcare perspective (CNY/QALY) | Dominant (-44,251) | / |
| ICER from the societal perspective (CNY/QALY) | Dominant (-93,115) | / |
CNY: Chinese Yuan; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Sensitivity analysis results
The results of the one-way sensitivity analysis are presented in Figure 3. The cost–effectiveness results were most sensitive to the cost of rehabilitation and the utility value assigned to the BSC group at week 24 and later. Within the range changed in one-way sensitivity analysis, the results showed the consistency of dominant results no matter which parameter was changed.

Figure 3. Tornado diagrams.
(A) Healthcare perspective and (B) societal perspective.
AE: Adverse event; BSC: Best supportive care; CNY: Chinese Yuan; ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Figure 4 presents graphical illustrations of the probabilistic sensitivity analysis results, showing 100% probabilities of PR-fampridine plus BSC being considered to be cost-effective versus BSC alone using a threshold of 80,976 CNY per QALY gained (gross domestic product per capita in 2021 in China).
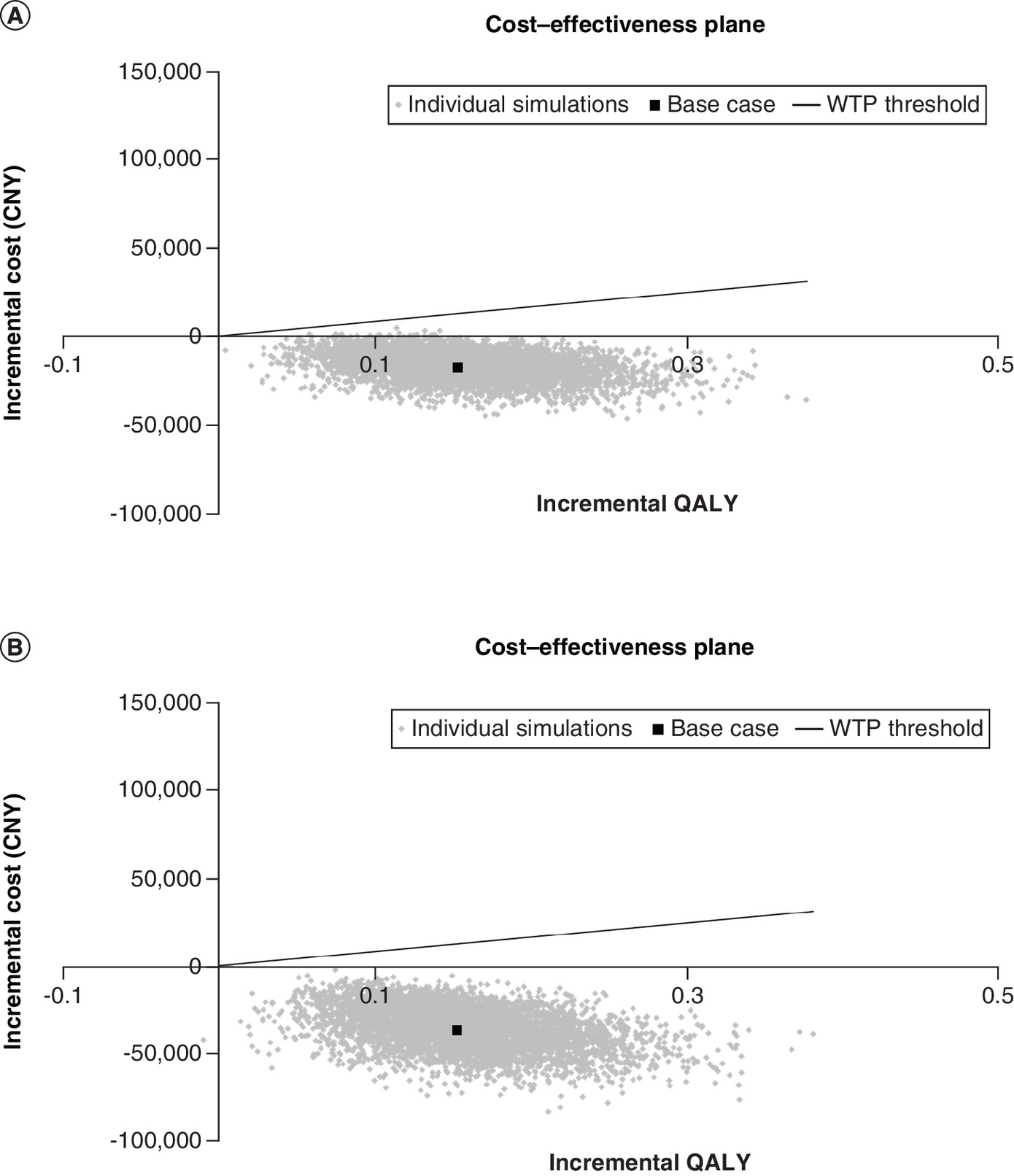
Figure 4. Cost–effectiveness planes and scatter plots.
(A) Healthcare perspective and (B) societal perspective.
CNY: Chinese Yuan; QALY: Quality-adjusted life year; WTP: Willingness-to-pay.
Discussion
This model compared the cost–effectiveness of PR-fampridine plus BSC versus BSC alone for the improvement of walking ability in MS patients in China. As the first and only approved symptomatic drug to improve MS-related walking disability in China, PR-fampridine was listed in the NRDL in 2021 considering its cost-effective advantage and clinical benefits to address unmet needs. This study showed that based on the 2021 NRDL negotiated price, PR-fampridine plus BSC was a dominant treatment strategy from both the Chinese healthcare perspective and the societal perspective when compared with BSC alone. From the healthcare perspective, the use of PR-fampridine improved walking ability and thus saved costs for rehabilitation, other supportive drugs and outpatient visits. PR-fampridine plus BSC led to an incremental QALY gain of 0.15 over BSC alone and a cost saving of 17,329 CNY. When considered from the societal perspective, the use of PR-fampridine could save walking aid costs and reduce the productivity losses for patients and caregivers. The cost–effectiveness benefit of using PR-fampridine was even greater with lower costs (-36,465 CNY) and higher QALYs (+0.15 QALYs).
Most of the published cost–effectiveness analysis studies in MS focused on disease-modifying therapies, while PR-fampridine is a symptomatic drug rather than a disease-modifying therapy. As seen in the clinical trials, the efficacy of PR-fampridine was mainly reflected in improving the walking speeds of patients and the changes in EDSS score could not indicate the real effect of PR-fampridine, so this study did not use the classical EDSS progression model but used the hybrid decision tree and Markov model. As mentioned in the methods section, the response rate of PR-fampridine plus BSC was evaluated based on MSWS-12 and obtained from the ENHANCE trial, while the relationship between walking ability and healthcare resource utilization was evaluated based on T25FW. T25FW was a convenient walking test and represented the patients' walking ability by measuring the time needed to walk 25 feet at the maximum speed [34]. The study has demonstrated that T25FW is suitable for different clinical settings and was recognized as the most well-characterized objective and specific assessment method of walking disability [35]. Based on that, the authors think it is reasonable to use T25FW to describe the change in walking speed and reflect the relationship between walking ability and healthcare resource utilization.
There are several economic evaluations conducted for PR-fampridine globally. A published economic study showed that PR-fampridine led to an incremental QALY gain of 0.12 over BSC and was a cost-effective treatment from the Swedish societal perspective [17]. Moreover, health technology appraisal reports from the All Wales Therapeutics & Toxicology Centre and Scottish Medicines Consortium also showed that PR-fampridine led to an incremental QALY gain of 0.15 and 0.16, respectively [18,19]. The comparator, model structure, cycle length and cost items in these studies are basically consistent with the present study and the estimated QALY gain of adding PR-fampridine to BSC is well aligned. Since PR-fampridine was included in the NRDL in 2021 with a price cut, this study presented an even greater economic benefit of PR-fampridine, which was an economically dominant strategy.
To improve the accuracy of the analysis and to better fit Chinese clinical practice, this study made some adjustments to the study design based on globally conducted cost–effectiveness analyses for PR-fampridine. One of the adjustments is that this study used a weighted average method to calculate the utility value in the model. Considering that both ENHANCE and MOBILE trials had missing utility data at different time points, in order to ensure data consistency and obtain the results with a larger sample size, the weighted average utility values of the ENHANCE and MOBILE trials [15,16] were used as the base case scenario. Scenario analyses were also conducted based on utility data from two trials separately. A greater QALY gain was observed by applying the utility data from the MOBILE trial, which might be due to the more sensitive questionnaire used (EQ-5D-5L in the MOBILE trial vs EQ-5D-3L in the ENHANCE trial). Additionally, the cost calculation method was adapted in in the present study based on the Swedish economic study [17]. The resource use in the Swedish economic study was informed by the relationship between healthcare resource utilization and walking speed, as measured by the T25FW, collected in the Adelphi MS disease-specific program directly [25]. The formulas representing the relationship between T25FW and healthcare resource utilization were analyzed based on the European population and may not fit the Chinese setting. Meanwhile, it is difficult to verify these formulas with clinical experts in China directly. Therefore, the present study used different speed segments to reflect the relationship between walking speed and healthcare resource utilization and verified this relationship with Chinese clinical experts. The authors collected the baseline annual costs of different healthcare resource utilization items for Chinese MS patients through clinical expert interviews, such as neurologist visits, rehabilitation, MS-related hospitalization and so on. Then based on the verified relationship between walking speed and healthcare resource utilization, the subsequent annual costs were calculated. Further, to get the long-term progression trend of T25FW scores over time in the placebo arm, the Swedish economic study chose the data of the placebo arm in the IMPACT trial only [26]. In contrast, the present study chose the IMPACT and ASCEND trials [26,27]. Both of them had baseline characteristics similar to those of the MS-F203 and MS-F204 trials of PR-fampridine [22,23]. The T25FW scores of the placebo arm in these two trials were pooled to obtain trends and the extrapolation data of T25FW scores. The authors believe the addition of the ASCEND trial's placebo arm may help provide a more robust estimation of MS natural history.
Some limitations and potential future improvements of the analysis should be acknowledged. First, considering that long-term efficacy data of MSWS-12 was not available, disease progression in the Markov model was measured by T25FW instead of MSWS-12 used in the decision tree. This might be a limitation despite the fact that T25FW is also a meaningful end point of measuring walking disability. Second, in the absence of the relationship between healthcare resource utilization and walking ability in MS patients in China, this study used the relationship of healthcare resource utilization and T25FW scores found in European studies as a substitution. Although this study verified this relationship via clinical expert interviews, once relevant data collected in the Chinese population are available in the future, the study results should be further updated. Third, the sample size of the clinical expert interviews might be limited, although the authors invited experts from several representative cities and performed sensitivity analyses for all the cost parameters to test the robustness of the results. Finally, because there were no available data regarding the utilities for PR-fampridine responders and BSC beyond 24 weeks, the authors assumed that there were no utility changes for patients in the subsequent weeks. Considering that there was some variation in the utility value, the dynamic change of the utility value can be explored in the future when the data become available.
Almost all MS patients will eventually experience walking disability [35]. This clinical outcome not only limits their ability to work but also puts a heavy psychological burden on patients and their families. These results showed that the use of PR-fampridine can save the cost of other supportive drugs and rehabilitation therapy and therefore save the medical insurance fund and promote clinical drug management. To the authors' knowledge, this is the first study to evaluate the cost–effectiveness of a symptomatic drug for the treatment of MS-related walking disability in China. The results fill the evidence gap in China and can provide more information for the clinical management of MS-related walking disability.
Conclusion
Compared with BSC alone, PR-fampridine plus BSC can provide more QALYs and reduce the cost of healthcare resource utilization and productivity losses of patients and their caregivers. The incremental cost–effectiveness ratios were -238,806 CNY/QALY and -113,488 CNY/QALY from the Chinese societal and healthcare perspectives, respectively. Our study showed that PR-fampridine plus BSC is considered an economically dominant strategy for adult MS patients with walking disability (EDSS scores 4–7) in China.
Future perspective
Real-world studies and relevant data related to the Chinese population on the relationship between healthcare resource utilization and MS-related walking disability in China could be further updated.
•
Prolonged-release (PR)-fampridine is the only approved symptomatic drug to improve multiple sclerosis (MS)-related walking disability globally.
•
This study aimed to evaluate the cost–effectiveness of adding PR-fampridine to best supportive care (BSC) versus BSC alone for the improvement of walking ability in adult MS patients with Expanded Disability Status Scale scores 4–7 in China.
•
A cost–effectiveness analysis was conducted based on a hybrid decision tree and Markov model from both the societal and healthcare perspectives in China.
•
The modeled treatment effect and utility data were derived from the clinical trials of PR-fampridine.
•
The BSC consisted of other supportive drugs, outpatient visits, examinations and lab tests, hospitalization and rehabilitation. The PR-fampridine plus BSC strategy considered the drug cost and adverse event management cost of PR-fampridine as well.
•
The costs of walking aids and productivity loss were also included in the societal perspective. Unit costs and utilization of healthcare resources were obtained from published sources or clinical experts' interviews.
•
Both quality-adjusted life years and costs were discounted at a rate of 5%, and a half-cycle correction was applied. Uncertainty was assessed by one-way and probabilistic sensitivity analyses.
•
Over a 10-year time horizon, adding PR-fampridine to BSC led to an incremental quality-adjusted life year gain of 0.15 and lower total costs from both perspectives.
•
The addition of PR-fampridine reduced the cost of healthcare resource utilization, especially the costs of rehabilitation, other supportive drugs and outpatient visits. In addition, the PR-fampridine plus BSC strategy presented lower costs of walking aids and productivity loss of patients and caregivers from the societal perspective.
•
Sensitivity analyses confirmed the robustness of the results.
•
Compared with BSC alone, PR-fampridine plus BSC is considered an economically dominant strategy (better effectiveness and lower costs) for adult MS patients with walking disability (Expanded Disability Status Scale scores 4–7) in China.
Financial & competing interests disclosure
This study was funded by Biogen China. Funding was not contingent upon publication of the manuscript. X Zhao, H Yang, T Wei, J Zhao and J Liu are employees of IQVIA, Real World Solutions, China, which received consulting fees from Biogen for adapting the model and running the analyses. Z Huang and L Zhu are employees of Biogen. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary materials (6).docx)
- Download
- 51.59 KB
References
1.
Walton C, King R, Rechtman L et al. Rising prevalence of multiple sclerosis worldwide: insights from the atlas of MS, third edition. Mult. Scler. 26(14), 1816–1821 (2020).
2.
National Health Commission of the People's Republic of China. Notice on publishing the first category of rare diseases (2018). www.nhc.gov.cn/yzygj/s7659/201806/393a9a37f39c4b458d6e830f40a4bb99.shtml
3.
Xu L, Chen L, Wang S-O et al. Urban prevalence of multiple sclerosis in China: a population-based study in six provinces. Eur. J. Neurol. 28(5), 1636–1644 (2021).
4.
China Alliance for Rare Disease. Blue Book on Health Insights of Multiple Sclerosis Patients and 2021 Quality of Life Report for Multiple Sclerosis Patients in China. Beijing, China (2021).
5.
Asch PV. Impact of mobility impairment in multiple sclerosis 2 – patient perspectives. Eur. Neurol. Rev. 6(2), 115–120 (2011).
6.
Kobelt G. Economic evidence in multiple sclerosis: a review. Eur. J. Health Econ. 5(Suppl. 1), S54–S62 (2004).
7.
Kobelt G, Berg J, Lindgren P, Fredrikson S, Jonsson B. Costs and quality of life of patients with multiple sclerosis in Europe. J. Neurol. Neurosurg. Psychiatry 77(8), 918–926 (2006).
8.
Rotstein Z, Hazan R, Barak Y, Achiron A. Perspectives in multiple sclerosis health care: special focus on the costs of multiple sclerosis. Autoimmun. Rev. 5(8), 511–516 (2006).
9.
Larocca NG. Impact of walking impairment in multiple sclerosis: perspectives of patients and care partners. Patient 4(3), 189–201 (2011).
10.
Yildiz M. The impact of slower walking speed on activities of daily living in patients with multiple sclerosis. Int. J. Clin. Pract. 66(11), 1088–1094 (2012).
11.
Mathiesen HK, Sorensen PS. Prolonged-release fampridine improves walking in a proportion of patients with multiple sclerosis. Expert Rev. Neurother. 13(12), 1309–1317 (2013).
12.
Immunology NBOCSF, Association NGONBOCM. Chinese expert consensus on diagnosis and treatment of multiple sclerosis (2018 edition). Chinese Journal of Neuroimmunology and Neurology 25(6), 387–394 (2018).
13.
Goodman AD, Brown TR, Schapiro RT, Klingler M, Cohen R, Blight AR. A pooled analysis of two phase 3 clinical trials of dalfampridine in patients with multiple sclerosis. Int. J. MS Care 16(3), 153–160 (2014).
14.
Goodman AD, Bethoux F, Brown TR et al. Long-term safety and efficacy of dalfampridine for walking impairment in patients with multiple sclerosis: results of open-label extensions of two phase 3 clinical trials. Mult. Scler. 21(10), 1322–1331 (2015).
15.
Hupperts R, Lycke J, Short C et al. Prolonged-release fampridine and walking and balance in MS: randomised controlled MOBILE trial. Mult. Scler. 22(2), 212–221 (2016).
16.
Hobart J, Ziemssen T, Feys P et al. Assessment of clinically meaningful improvements in self-reported walking ability in participants with multiple sclerosis: results from the randomized, double-blind, phase III ENHANCE trial of prolonged-release fampridine. CNS Drugs 33(1), 61–79 (2019).
17.
Acosta C, Gianinazzi M, Dort T et al. Modeling the cost–effectiveness of prolonged-release fampridine for the treatment of walking impairment in patients with multiple sclerosis in Sweden. J. Med. Econ. 24(1), 770–780 (2021).
18.
All Wales Therapeutics & Toxicology Centre (AWTTC). AWMSG secretariat assessment report. Fampridine (Fampyra®) 10mg prolonged release. Reference number: 3942 (2019). https://awmsg.nhs.wales/files/appraisals-asar-far/appraisal-report-fampridine-fampyra-3942/
19.
Scottish Medicines Consortium (SMC). Fampridine 10mg prolonged-release tablet (Fampyra®) (2020). www.scottishmedicines.org.uk/media/5165/fampridine-fampyra-final-march-2020-for-website.pdf
20.
China Alliance for Rare Disease. 2020 Comprehensive Social Survey Report of Multiple Sclerosis Patients in China. Beijing, China (2020).
21.
Tian DC, Zhang C, Yuan M et al. Incidence of multiple sclerosis in China: a nationwide hospital-based study. Lancet Reg. Health West. Pac. 1, 100010 (2020).
22.
Goodman AD, Brown TR, Krupp LB et al. Sustained-release oral fampridine in multiple sclerosis: a randomised, double-blind, controlled trial. Lancet 373(9665), 732–738 (2009).
23.
Goodman AD, Brown TR, Edwards KR et al. A phase 3 trial of extended release oral dalfampridine in multiple sclerosis. Ann. Neurol. 68(4), 494–502 (2010).
24.
Liu GN, Hu SL, Wu JH, Wu J, Dong ZH, Li HC. China Guidelines for Pharmacoeconomic Evaluation (Chinese–English Version). China Market Press, Beijing, China (2020).
25.
Pike J, Jones E, Rajagopalan K, Piercy J, Anderson P. Social and economic burden of walking and mobility problems in multiple sclerosis. BMC Neurol. 12, 94 (2012).
26.
Cohen JA, Cutter GR, Fischer JS et al. Benefit of interferon beta-1a on MSFC progression in secondary progressive MS. Neurology 59(5), 679–687 (2002).
27.
Kapoor R, Ho PR, Campbell N et al. Effect of natalizumab on disease progression in secondary progressive multiple sclerosis (ASCEND): a phase 3, randomised, double-blind, placebo-controlled trial with an open-label extension. Lancet Neurol. 17(5), 405–415 (2018).
28.
Van Hout B, Janssen MF, Feng YS et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 15(5), 708–715 (2012).
29.
Sullivan PW, Ghushchyan VH. EQ-5D scores for diabetes-related comorbidities. Value Health 19(8), 1002–1008 (2016).
30.
Chen L, Zou MJ. Efficacy and cost–effectiveness ratio of moxifloxacin and gatifloxacin in the treatment of urinary tract infection. Contemporary Medicine Forum 18(7), 121–122 (2020).
31.
Peng K, Lei L, Feng NP, Zeng NB, Li HC, Zhou HB. Prevalence of falls and direct disease burden in the elderly in Shenzhen. Chinese J. Prevention Control of Chronic Diseases 24(2), 122–124 (2016).
32.
Ji J, Zhang H, Lv YY. Analysis on the use of oral non-steroidal anti-inflammatory drugs in a hospital from 2015 to 2017. Anhui Medical and Pharmaceutical J. 24(1), 201–205 (2020).
33.
National Bureau of Statistics. The average salary of employees in urban non-private units in China in 2020 (2021). www.stats.gov.cn/xxgk/sjfb/zxfb2020/202105/t20210519_1817689.html
34.
Phan-Ba R, Calay P, Grodent P et al. A corrected version of the timed-25 foot walk test with a dynamic start to capture the maximum ambulation speed in multiple sclerosis patients. NeuroRehabilitation 30(4), 261–266 (2012).
35.
Kieseier BC, Pozzilli C. Assessing walking disability in multiple sclerosis. Mult. Scler. 18(7), 914–924 (2012).
Information & Authors
Information
Published In
Pages: 1057 - 1069
PubMed: 35894120
Copyright
© 2022 Future Medicine Ltd.
History
Received: 13 June 2022
Accepted: 14 July 2022
Published online: 27 July 2022
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness analysis of prolonged-release fampridine to treat walking disability of multiple sclerosis in China. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0109
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Tobias Sydendal Grand, Shijie Ren, Praveen Thokala, Stefano Zanigni, Daniel Oudin Åström, Aroussi Bidani, Günter Höglinger, Werner Poewe, Florian Krismer, Stephane Regnier, Cost-Effectiveness Modelling of Multiple System Atrophy for Early Health Technology Assessment, PharmacoEconomics - Open, 10.1007/s41669-025-00609-8, 10, 1, (179-196), (2025).