Opicapone as an add-on to levodopa for reducing end-of-dose motor fluctuations in Parkinson’s disease: a systematic review and meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the clinical efficacy and safety profile of opicapone (25 and 50 mg once daily) versus placebo. Patients: Levodopa-treated adults with Parkinson’s disease. Material & methods: A systematic review and meta-analysis were conducted. Results: Opicapone provided a greater reduction in the absolute OFF-time, increased the chances of ≥1-h reduction in the OFF-time and ≥1-h increase in the ON-time compared with placebo. Receiving opicapone more often facilitated levodopa dose reduction versus placebo. There were no differences in the occurrence of adverse events (severe and leading to drug discontinuation), but receiving opicapone increased the frequency of dyskinesia. Conclusion: Opicapone demonstrated superior clinical efficacy to placebo, with a comparable general safety profile.
Parkinson’s disease is a slowly progressing, incurable idiopathic neurodegenerative disorder. However, early diagnosis and adequate treatment can improve the quality of life and reduce symptoms in these patients [1–3]. The disease may present with motor symptoms such as bradykinesia, rest tremor and rigidity but may also have nonmotor manifestations including anxiety, leg pain, sleep disturbances, urinary problems, concentration difficulties and fatigue [4,5]. Parkinson’s disease affects >10 million people globally (0.15–0.30% of the general population), and its incidence increases with age (only about 4% of cases are diagnosed before the age of 50). Moreover, it is diagnosed more often in men than in women [6].
The loss of dopaminergic neurons in the substantia nigra pars compacta is the main neuropathological feature of Parkinson’s disease [4]. These neurons are the main source of dopamine in the central nervous system (CNS) and are crucial for proper brain function, including control of voluntary movement, as well as control of various behavioral processes such as addiction, mood, reward or stress [7]. Currently, as there is no curative therapy targeting the loss of dopaminergic neurons, symptomatic treatment is used in patients with Parkinson’s disease. The gold standard includes long-term supplementation with levodopa, a precursor of dopamine, as dopamine itself cannot cross the blood–brain barrier [4,8,9]. Unfortunately, levodopa therapy is often associated with end-of-dose motor fluctuations, which can prolong the time patients spend in the OFF state. OFF episodes are characterized by motor symptoms such as tremor, stiffness, slowness, incoordination and weakness, and are often associated with some nonmotor symptoms such as anxiety, a change in mood, difficulty thinking, pain, urinary problems, swallowing difficulties and shortness of breath [10,11]. It was shown that after 4–6 years of levodopa therapy, about 40% of patients experienced end-of-dose motor fluctuations. Therefore, the development of novel treatment strategies aimed at reducing the rate of complications remains the crucial unmet need for patients with Parkinson’s disease [5]. However, the period when the symptoms of the disease are controlled and the levodopa is working well are referred to as the ON-time [10].
Catechol-O-methyltransferase (COMT) inhibitors are a class of drugs that reduce the metabolism of levodopa, thus prolonging its half-life. Consequently, they can be used as an addition to levodopa therapy to extend the duration of its therapeutic effect. In addition, they promote the delivery and increase the availability of levodopa in the CNS [5]. COMT inhibitors have been shown to significantly improve the condition of patients with moderate to advanced Parkinson’s disease, particularly by reducing the OFF-time and decreasing the frequency of end-of-dose motor fluctuations [5,12–16]. However, despite their considerable benefits, two currently available second-generation COMT inhibitors, entacapone and tolcapone, were reported to have some limitations. In particular, entacapone was shown to have a relatively low potency necessitating frequent administration. It is taken with each levodopa dose, which can be administered between three–five-times a day [17]. This can be inconvenient both for patients and their caretakers. Tolcapone, however, is a more potent and longer-acting drug, but its use was associated with increased risk of hepatotoxicity necessitating frequent monitoring of liver function [13].
Some alternative options used to decrease the frequency of end-of-dose motor symptoms include dopamine agonists, extended-release forms of carbidopa-levodopa and monoamine oxidase B inhibitors [18–20].
Opicapone is a COMT inhibitor that has been specifically designed to overcome the disadvantages associated with the use of older-generation drugs. It is a long-acting and peripherally selective inhibitor (increases the half-life of levodopa, whereas central inhibitors slow its metabolism within the CNS) that can be taken once daily, which makes the therapy more convenient. Additionally, it is well tolerated and associated with a reduced risk of hepatotoxicity and fulminant liver injury compared with tolcapone [9,21]. In June 2016, opicapone was approved for use by the Committee for Medicinal Products for Human Use of the European Medicines Agency [5,16]. In 2018, the International Parkinson and Movement Disorder Society described opicapone as ‘clinically useful’ in their updated evidence-based review of treatment options for motor symptoms in Parkinson’s disease [22]. However, it is still a relatively new drug, and every piece of new data regarding its clinical efficacy is extremely valuable. Moreover, considering that curative treatment is still unavailable, symptomatic treatment options should be thoroughly investigated. Detailed knowledge on a medical intervention can be derived from meta-analyses based on the results from large populations of patients included in randomized controlled trials (RCTs).
There are some network meta-analyses comparing opicapone to other COMTs [23] or istradefylline (adenosine A2A receptor antagonist) [24] or meta-analyses comparing opicapone to placebo [25]; however, they only consider one opicapone dose (50 mg daily) and/or are also limited to a few selected end points such as a change in total ON-time or OFF-time and change in Unified Parkinson’s Disease (UPDRS) part III (motor) score during the ON state. Because of limitations of current existing meta-analyses, there is still a need for preparing one with deep assessment and clarifying the relationship of the efficacy and safety of opicapone to placebo, because individual clinical trials could bring slightly different conclusions regarding the significance of the analyzed intervention. To fill up this gap, we conducted a systematic review and meta-analysis assessing the broad clinical efficacy and safety of opicapone (50 and 25 mg daily) compared with placebo in levodopa-treated adult patients with Parkinson’s disease.
Methods
Data sources & search
A systematic review of databases was conducted from 3 to 5 November 2021. Eligible studies published in English were identified in MEDLINE (via PubMed), Embase and Cochrane Library. The search strategy was created based on the medical subject heading (MeSH) terms or Emtree terms combined with Boolean logical operators (Supplementary Table 1). No restrictions with regard to end points were applied to ensure that the search returned all possible efficacy and safety results. Written informed consent from patients and ethical approval were not required, because the study did not include personal patient information and did not influence patient care.
Selection criteria
Studies were identified by two reviewers (M Żegleń and K Śladowska) using the search strategy. The third reviewer (P Kawalec) was involved to resolve potential disagreements at this stage of study selection. Studies were selected based on the title, abstract and, where necessary, the full text of the article. All relevant RCTs were selected and critically appraised according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [26].
The inclusion criteria were as follows: adult patients (18 years or older) with a clinical diagnosis of Parkinson’s disease; intervention assessed: opicapone used as an add-on to standard levodopa therapy; comparator: placebo; study: prospective RCT. Two doses of opicapone, 25 mg and 50 mg once daily, were considered in the analysis. Although the recommended dose is 50 mg once daily, 25-mg presentation is also available according to the Summary of Product Characteristics for opicapone. In addition, 25-mg presentation can be used to modify the dose for patients with increased safety risks, such as those with preexisting moderate hepatic impairment. Contraindications to use opicapone, besides hypersensitivity, include haeochromocytoma, paraganglioma or other catecholamine-secreting neoplasms, as well as the history of the neuroleptic malignant syndrome or nontraumatic rhabdomyolysis [27–29]. Full-text articles containing the required data were included in the analysis. Nonrandomized or uncontrolled studies, non-English publications, unpublished studies, poster presentations and conference abstracts were excluded.
The titles and abstracts of studies identified in the search were independently reviewed by two investigators based on prespecified inclusion and exclusion criteria. Full texts of the remaining articles were examined to determine whether they contained information relevant to the study. Possible disagreements during this stage of study selection were resolved by consensus. Nevertheless, there was a high degree of compatibility between the reviewers of search results (95%). The references of the selected articles were also hand searched to identify any potential additional studies.
Data extraction & quality assessment
Data were extracted from full-text publications independently by two reviewers (M Żegleń and K Śladowska) using predefined data extraction forms. The following information was extracted: study design (methodology), inclusion criteria, treatment regimen and duration, follow-up duration, sample and arms size, number of individuals lost to follow-up, and the number of participants who achieved predefined outcomes. Extracted data were then inspected independently by each investigator.
The risk of bias within individual studies and the methodological quality of eligible RCTs were assessed using the Cochrane Risk of Bias tool recommended by the Cochrane Collaboration. Specifically, domain-based evaluation was used, with ‘+’ denoting low risk of bias, ‘-’ denoting high risk of bias and ‘?’ denoting unclear risk of bias. Domain-based evaluation allows the assessment of specific domains, including sequence generation, allocation concealment, blinding of participants, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and ‘other issues’ [30].
Data analysis
The weighted mean difference (WMD) with 95% CIs between opicapone and placebo was used for continuous outcomes, whereas the odds ratio (OR) with 95% CIs was calculated for dichotomous outcomes. In cases where only standard errors (SEs) were available for the continuous variables, they were converted to standard deviations (SDs) according to the following formula: , where N is the number of participants in the analyzed study group.
Sensitivity analysis was performed for the primary end point (change from baseline in the time spent in the OFF state), excluding the COMFORT-PD study, which was conducted only in the Japanese population. The random effects model was applied both for dichotomous and continuous variables. A p-value < 0.05 was determined as the threshold of statistical significance. Obtained results were presented as forest plots. The I2 statistic was used to assess statistical heterogeneity. Review Manager v.5.4.1. and Microsoft Excel® were used for all analyses performed in the study.
Results
Literature search
The results of the database search are presented in Figure 1. Overall, 327 possibly relevant publications were identified, of which 316 were excluded after the screening of the titles and abstracts. Eleven articles were included in the full-text review, of which six were excluded, resulting in five references (three studies) to be included in the meta-analysis: BIPARK-1 [31,32], BIPARK-2 [33,34] and COMFORT-PD [35]. They were all double-blind, parallel-group studies, which included adult patients who had Parkinson’s disease (Hoehn-Yahr stage 1–3) for at least 3 years and who showed at least 1 year of clinical improvement following treatment with levodopa and/or a DOPA decarboxylase inhibitor. In all of the included studies, the randomized treatment period lasted 14–15 weeks (Supplementary Table 2). These three RCTs had an acceptable level of homogeneity in terms of methodology, population characteristics, selected end points and their definitions, as well as other applied methods, which allowed performing the meta-analysis.
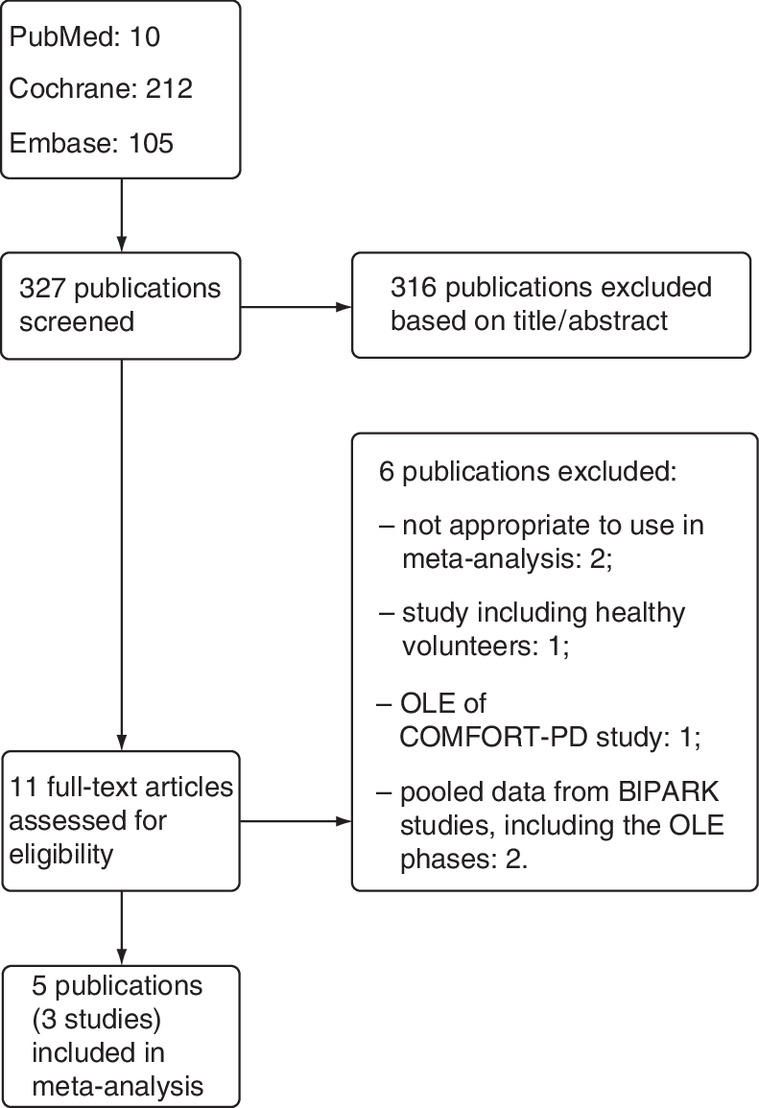
Figure 1. Results of the database search.
OLE: Open-label phase.
The methodological quality of studies included in the meta-analysis was assessed using the Cochrane Risk of Bias tool (Figure 2). In the BIPARK-1, -2 and COMFORT-PD studies, the selection bias (random sequence generation bias) was assessed as unclear due to the randomization method that included stratification and block randomization. Additionally, in BIPARK-2, there was a different measure of dispersion for the main end point given in the abstract and in the text (SE vs SD), whereas the value remained the same. Finally, there is no clear information in COMFORT-PD that the allocation code was hidden, hence the risk was assessed as unknown.

Primary end point: least-squares mean change from baseline in the absolute time in the OFF state
In all three studies, a change from baseline in the absolute time spent in the OFF state was considered a primary end point, and its analysis was based on symptom diaries completed by patients. The meta-analysis revealed that patients receiving either dose of opicapone as an add-on to their standard levodopa treatment had a significantly greater reduction in the absolute time in the OFF state at the end of the study. However, this effect was numerically stronger for the dose of 50 mg (WMD: -49.92 min [95% CI: -71.38 to -28.46]) compared with that of 25 mg (WMD: 37.76 min [95% CI: -59.21 to -16.30]; Figure 3).

Figure 3. Meta-analysis results for primary end point.
Least-squares mean change from baseline in absolute time in the OFF state for (A) 25 mg and (B) 50 mg of opicapone versus placebo.
SD: Standard deviation.
Secondary end points
The number of patients with a ≥1-h reduction in the time spent in the OFF state and an increase of ≥1 h in the time spent in the ON state was assessed in all three studies. The evaluation was based on the diaries of symptoms completed by patients.
Patients receiving either dose of opicapone as an add-on to their standard levodopa treatment were significantly more likely to achieve at least 1 h of reduction in the time spent in the OFF state as compared with the placebo group (OR: 1.60 [95% CI: 1.21–2.13] for 25 mg of opicapone and OR: 1.89 [95% CI: 1.42–2.52] for 50 mg of opicapone). Moreover, they were significantly more likely to achieve an increase in the ON-time (OR: 1.84 [95% CI: 1.39–2.45] for 25 mg of opicapone and OR: 1.91 [95% CI: 1.44–2.53] for 50 mg of opicapone). However, it should be stressed that the observed effects were dose dependent (Figure 4).
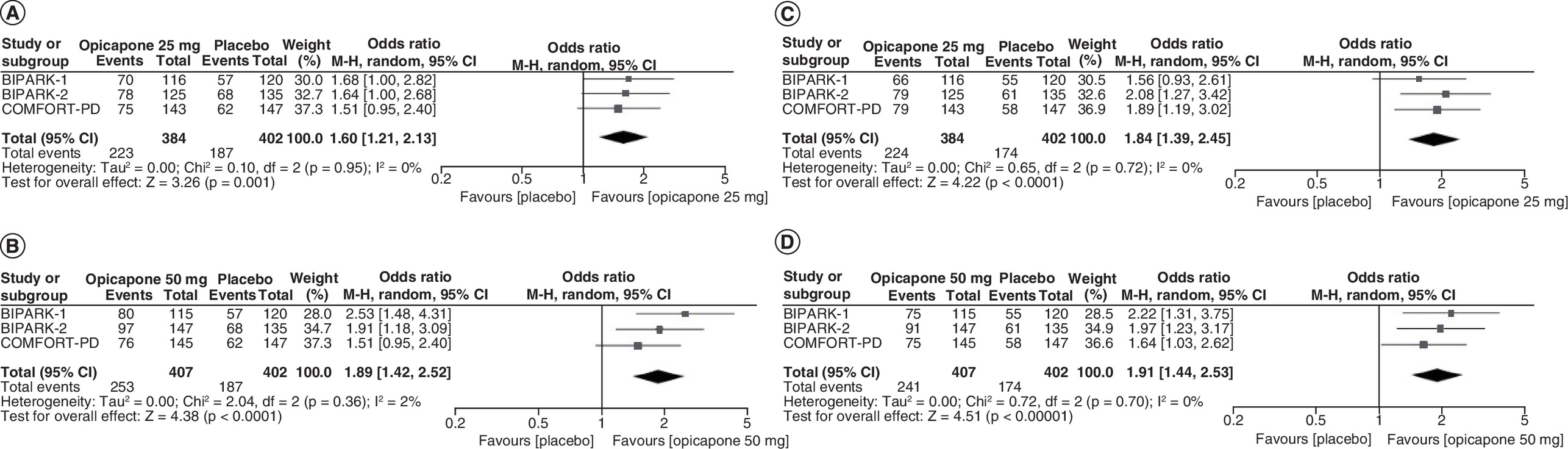
Figure 4. Meta-analysis results for the number of patients with a ≥1-h reduction in time in the OFF state.
(A) 25 mg and (B) 50 mg of opicapone versus placebo and an increase of ≥1-h in the ON state (C) 25 mg and (D) 50 mg of opicapone vs placebo.
The change from baseline in the absolute time spent in the ON state at the end of treatment was assessed in all three studies. In addition, two studies (BIPARK-1 and COMFORT-PD) analyzed the change in the time spent in the ON state with troublesome dyskinesia. The meta-analysis revealed that patients receiving either dose of opicapone had a significantly higher increase in the absolute time in the ON state at the end of the study as compared with the placebo group (WMD: 43.37 min [95% CI: 21.51–65.23] for 25 mg of opicapone and WMD: 54.63 [95% CI: 33.15–76.11] for 50 mg of opicapone). However, there were no significant differences between opicapone and placebo groups with regard to changes in the time spent in the ON state with troublesome dyskinesia (WMD: 2.09 [95% CI: -5.37–9.55] for 25 mg of opicapone and WMD: 6.15 [95% CI: -1.32–13.62] for 50 mg of opicapone; Figure 5).
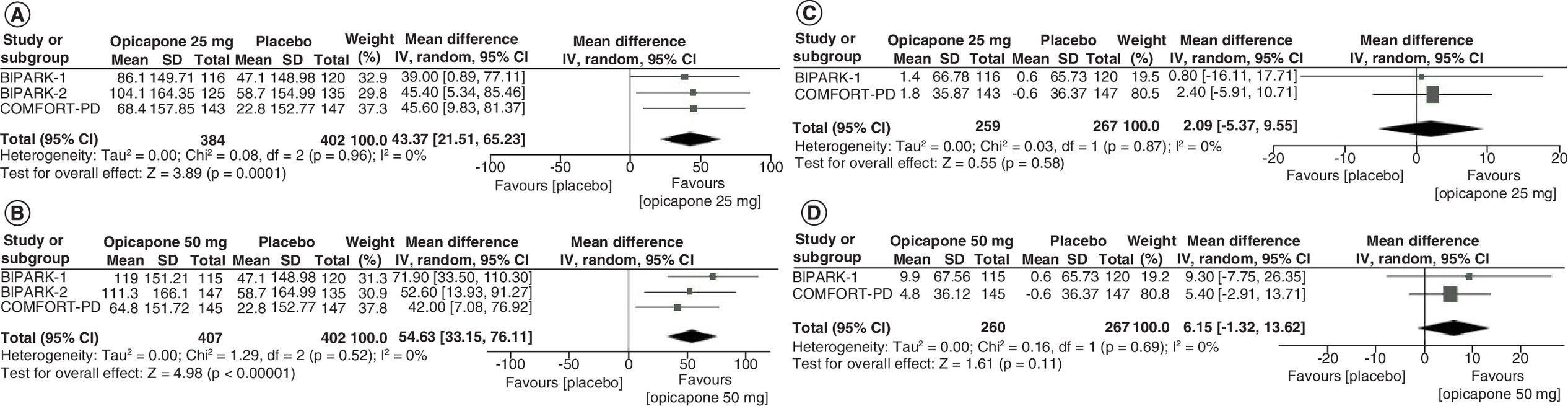
Figure 5. Meta-analysis results for the change from the baseline in absolute time in the ON state.
(A) 25 mg and (B) 50 mg of opicapone versus placebo and the ON state with troublesome dyskinesia (C) 25 mg and (D) 50 mg of opicapone versus placebo.
SD: Standard deviation.
Due to some discrepancies between studies in terms of the definition of end points, no meta-analysis has been conducted for the time without dyskinesia, but the results of individual studies indicate a significant extension of the ON-time without dyskinesia in opicapone treated patients.
Two studies (BIPARK-1 and -2) assessed the change from baseline in the percent of time spent in the OFF state. Our results suggest that patients treated with opicapone had a significantly greater reduction in the percent of the time spent in the OFF state compared with placebo (WMD: -3.73 [95% CI: -6.52 to -0.94] for 25 mg of opicapone and WMD: -5.95 [95% CI: -8.69 to -3.21] for 50 mg of opicapone; Figure 6).
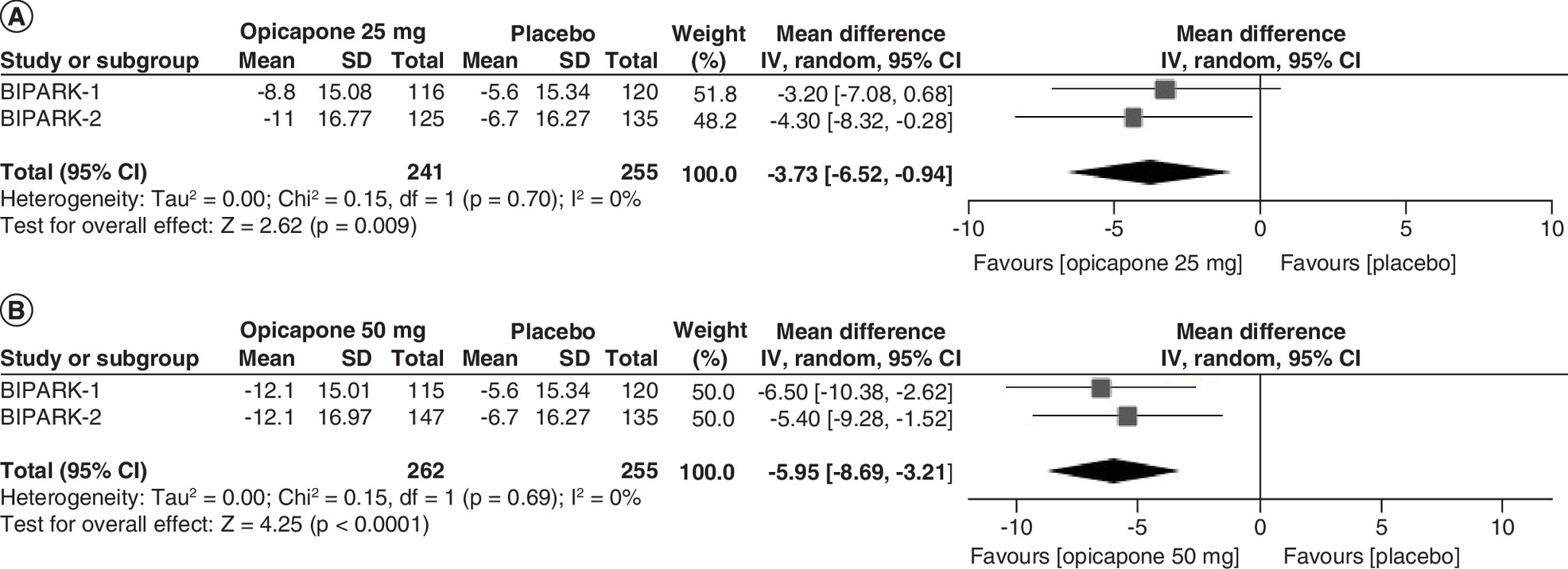
Figure 6. Meta-analysis results for change from the baseline in percentage of the time in the OFF state.
(A) 25 mg and (B) 50 mg of opicapone versus placebo.
SD: Standard deviation.
The UPDRS, Parkinson’s Disease Sleep Scale (PDSS) and Non-Motor Symptoms Scale (NMSS) scores were reported in two trials, whereas all three trials assessed the change in the Parkinson’s Disease Questionnaire (PDQ-39) score. There were no significant differences between study and placebo groups in any of the obtained scores: UPDRS (WMD: -1.16 [95% CI: -2.69–0.37] for 25 mg of opicapone and WMD: -0.20 [95% CI: -1.80–1.27] for 50 mg of opicapone), PDSS (WMD: 0.98 [95% CI: -5.98–7.93] for 25 mg of opicapone and WMD: -0.53 [95% CI: -5.13–4.08] for 50 mg of opicapone), PDQ-39 (WMD: 0.63 [95% CI: -0.61–1.87] for 25 mg of opicapone and WMD: 0.03 [95% CI: -1.26–1.33] for 50 mg of opicapone) and NMSS (WMD: 2.27 [95% CI: -0.71–5.25] for 25 mg of opicapone and WMD: 2.09 [95% CI: -1.24–5.42] for 50 mg of opicapone; Figure 7).

Figure 7. Meta-analysis results for change from the baseline in the results.
Unified Parkinson’s Disease Rating Scale – (A) 25 mg and (B) 50 mg of opicapone vs placebo, Parkinson’s Disease Sleep Scale – (C) 25 mg and (D) 50 mg of opicapone versus placebo, Non-Motor Symptoms Scale – (E) 25 mg and (F) 50 mg of opicapone versus placebo and Parkinson’s Disease Questionnaire – (G) 25 mg and (H) 50 mg of opicapone versus placebo.
SD: Standard deviation.
The number of patients receiving a reduced levodopa dose was assessed in two studies (BIPARK-1 and COMFORT-PD). Modifications of the levodopa dose were possible in the first 2–3 weeks of each study. The meta-analysis revealed that patients treated with opicapone were more likely to have their levodopa dose reduced as compared with the placebo group (OR: 3.52 [95% CI: 1.36–9.11] for 25 mg of opicapone and OR: 5.40 [95% CI: 1.42–20.60] for 50 mg of opicapone). Additionally, a trend was found in favor of the higher opicapone dose of 50 mg (Figure 8).
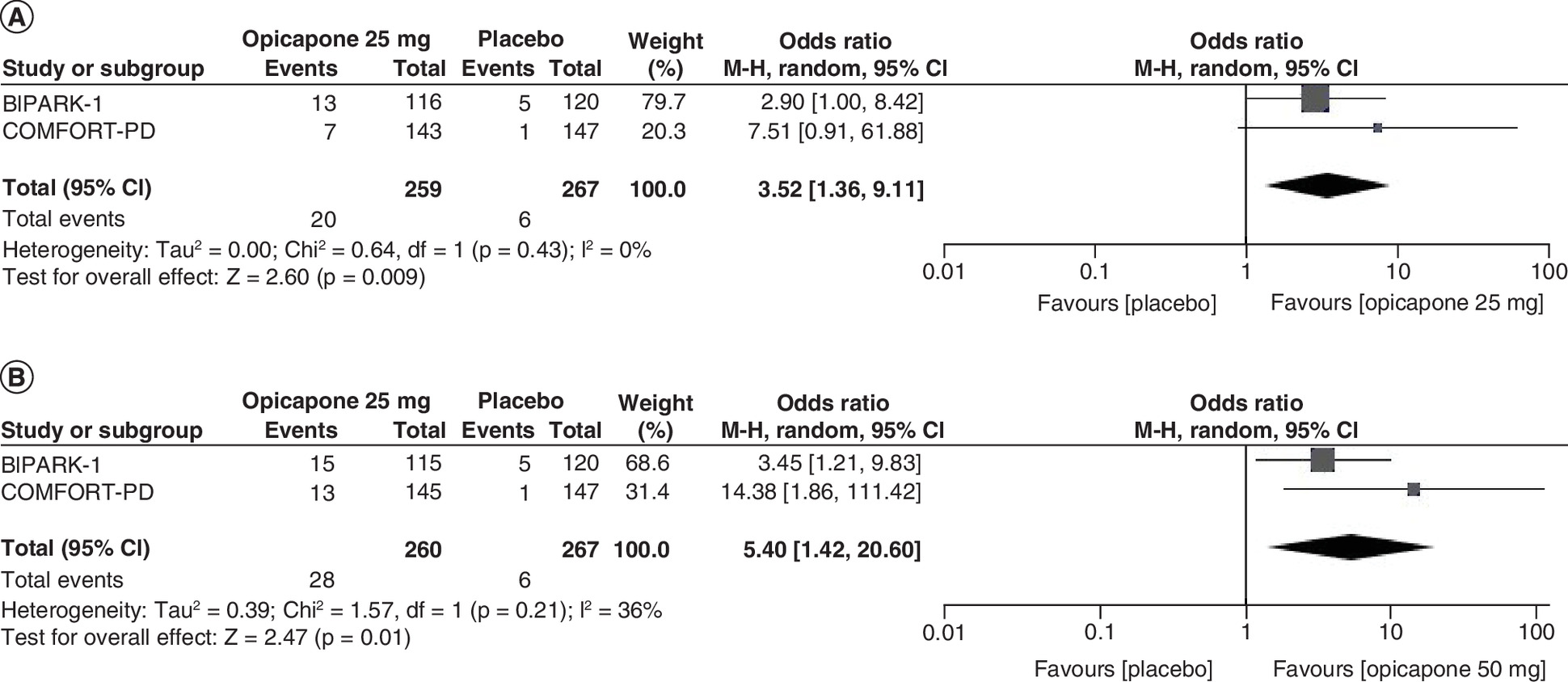
Figure 8. Meta-analysis results for the number of patients with decreased levodopa dose.
(A) 25 mg and (B) 50 mg of opicapone versus placebo.
Safety profile
The meta-analysis was performed for all treatment-emergent adverse events, serious adverse events and adverse events leading to the discontinuation of the study drug, as well as dyskinesia. It revealed no significant differences between opicapone (either dose) and placebo in terms of serious adverse events (OR: 0.95 [95% CI: 0.18–4.98] for 25 mg of opicapone and OR: 1.21 [95% CI: 0.56–2.59] for 50 mg of opicapone) and adverse events leading to discontinuation of the study drug (OR: 0.95 [95% CI: 0.46–1.93] for 25 mg of opicapone and OR: 1.49 [95% CI: 0.66–3.34] for 50 mg of opicapone). Interestingly, any treatment-emergent adverse events were more frequent in patients treated with an opicapone dose of 25 mg than in those receiving placebo (OR: 1.38 [95% CI: 1.04–1.83]).
Our results suggest that patients receiving 25 mg and 50 mg of opicapone are significantly more likely to experience dyskinesia compared with the placebo-treated group (OR: 3.08 [95% CI: 1.79–5.30] for 25 mg of opicapone and OR: 4.06 [95% CI: 2.41–6.83] for 50 mg of opicapone; Figure 9).

Figure 9. Meta-analysis results for the number of patients.
With any treatment-emergent adverse events – (A) 25 mg and (B) 50 mg of opicapone versus placebo, serious adverse events – (C) 25 mg and (D) 50 mg of opicapone versus placebo and adverse events leading to discontinuation of the study – (E) 25 mg and (F) 50 mg of opicapone versus placebo, as well as dyskinesia – (G) 25 mg and (H) 50 mg of opicapone versus placebo.
Sensitivity analysis
The results of sensitivity analysis for the primary end point, excluding the COMFORT-PD trial, were in line with the results of the main analysis. Patients receiving opicapone as an add-on to their standard levodopa treatment had a significantly greater reduction in the absolute time spent in the OFF state at the end of the study. Similar to the results of the main analysis, there was a trend in favor the opicapone dose of 50 mg (WMD: -57.63 min [95% CI: -84.82 to -30.44]) than for the dose of 25 mg (WMD: -34.02 min [95% CI: -60.84 to -7.20]).
Heterogeneity analysis
For interpretation, we quantified heterogeneity as low, moderate and high, with upper limits of 25, 50 and 75% for I2, respectively. The meta-analysis showed that there was low or moderate heterogeneity among studies for most assessed end points (including primary end point with I2 = 0%), with the exception of change from the baseline results in the PDSS for opicapone 25 mg (I2 = 74%) and the number of patients with serious adverse events for opicapone 25 mg (I2 = 67%), where the heterogeneity was high.
We conducted a sensitivity analysis excluding the COMFORT-PD study as a probable source of heterogeneity. When the study was removed, we found that the heterogeneity decreased (I2 = 43%), but there were still no differences between opicapone 25 mg and placebo in terms of serious adverse events.
Discussion
Parkinson’s disease affects 2–3% of the population aged 65 years or older, thus constituting the second most common neurodegenerative disorder. Hallmarks of the disease include striatal dopamine deficiency caused by the neuronal loss in the substantia nigra, as well as intracellular inclusions containing aggregates of α-synuclein, resulting in typical Parkinson’s symptoms [29,36]. Supplementation of levodopa is the main therapeutic strategy in Parkinson’s disease, but the end-of-dose phenomenon is the major disadvantage of this treatment. Fortunately, it can be reduced or prevented with the use of COMT inhibitors, such as opicapone [37].
The findings of this meta-analysis suggest that opicapone (25 and 50 mg once daily) used in BIPARK-1, BIPARK-2 and COMFORT-PD studies as an add-on to standard levodopa therapy resulted in a significantly greater reduction in the absolute time spent in the OFF state as compared with placebo. This is a meaningful finding, particularly for the 25-mg dose of opicapone, because the WMD for this end point did not differ significantly between study and control groups in two of the three studies. A substantial reduction in the time spent in the OFF state and a subsequent increase in the ON-time was also confirmed by the greater number of patients with a ≥1-h reduction or increase in these end points, respectively, in the opicapone compared with the placebo group. This is an important result, especially for the 25-mg dose of opicapone, because there were no significant differences when ORs for the decrease in the OFF-time were calculated for separate studies. Moreover, the meta-analysis of the BIPARK-1 and BIPARK-2 studies suggested a significantly greater reduction in the percent of the OFF-time in the study group compared with placebo, which further confirms a significant positive effect of add-on opicapone on the time spent in the OFF state.
The minimal clinically important difference for the OFF-time in Parkinson’s disease, which is about 1 h, was not reached for the opicapone dose of 25 mg. However, the sensitivity analysis revealed that the minimal clinically important difference was almost achieved for the opicapone dose of 50 mg [38].
A substantial reduction in the time spent in the OFF state and a subsequent increase in the time spent in the ON state are particularly important, because the OFF state is associated with significant impairment of mobility, thus compromising not only the activities of daily living but also the emotional well-being of patients [39]. In addition, as reported in previous research, long exposure to levodopa is typically accompanied by a reduction in the ON-time and an increase in the OFF- time [40]. Furthermore, the development of new treatments that would maximally reduce the duration of the OFF-time and delay the onset of the OFF state is consistent with the preferences of patients with Parkinson’s disease, who reported this to be one of the most important characteristics of a treatment strategy [39].
The current meta-analysis also revealed that reduced OFF-time led to a significantly higher increase in the absolute time spent in the ON state in patients receiving either dose of opicapone compared with the placebo groups. Similar results were obtained by Kwak et al. [25]. However, there were no significant differences between opicapone and placebo with regard to changes in the ON state with troublesome dyskinesia. This indicates that add-on opicapone does not increase the risk of troublesome dyskinesia, which is a promising finding. Moreover, in individual studies, there was a significant increase in the time spent in the ON state without dyskinesia. This result has important implications, especially because troublesome dyskinesia has been shown to increase the level of disability, leaving some of the patients housebound. In addition, severe dyskinesia can severely hamper a safe mobilization of patients, especially outdoors, and can as well make it extremely difficult for the patient to maintain any level of independence [41]. Thus, increasing the time spent in the ON state, particularly without aggravating troublesome dyskinesia, can prevent a reduction in the level of independence and the quality of life.
Importantly, the open-label phases of the studies included in the meta-analysis showed a consistent reduction in the OFF-time and an increase in the ON-time over a long-term treatment [42,43].
It should also be mentioned that it has been shown in previous research that switching to opicapone from other COMT inhibitors (e.g., entacapone) allows for shortening of the OFF-time while increasing the ON-time in patients with Parkinson’s disease with, as well as without, motor complications [44–47]. Therefore, it can be concluded that opicapone can be a great treatment option not only for COMT-naive patients but also for those who have not responded to previous therapy with COMT inhibitors.
In the present study, the meta-analysis of the results from two trials revealed that patients treated with opicapone were more likely to have their levodopa dose reduced as compared with the placebo groups. This suggests that adding opicapone to the therapeutic strategy can promote the safety of treatment by decreasing the incidence of adverse events associated with levodopa, among others. Moreover, this finding suggests that the use of opicapone can make it possible to tailor the levodopa regimen and thus offer a more personalized treatment to patients with Parkinson’s disease [37]. Another important advantage of using opicapone as an add-on to levodopa treatment is cost effectiveness. For example, in the UK, it allowed a significant reduction of healthcare costs related to the management of patients with Parkinson’s disease while maintaining high clinical effectiveness [48].
In our meta-analysis, there were no significant differences in UPDRS, PDSS, NMSS and PDQ-39 scores between patients receiving opicapone and placebo. This suggests that add-on opicapone does not have a significant negative effect on any of the aspects assessed by these scales. Importantly, however, as the studies included patients who were most suitable for symptomatic control with levodopa, it is not surprising that there were no considerable changes in the UPDRS score. Similarly, it should be noted that it is particularly challenging to show improvement in the quality of life in studies that include patients with quite advanced stages of the disease (and thus often heavily affected by impaired cognitive status, depression and other nonmotor symptoms) [32].
Overall, the meta-analysis revealed no significant differences between opicapone and placebo in terms of serious adverse events and events leading to the discontinuation of the study. However, it should be noted that a p-value for any adverse events for the opicapone dose of 50 mg approached statistical significance, whereas for the opicapone dose of 25 mg, adverse events were significantly more frequent compared with the control group. This suggests that opicapone-treated patients experienced more adverse effects of therapy than those receiving placebo. The most common adverse reactions associated with the use of opicapone, which were highlighted in the Summary of Product Characteristics, are nervous system disorders, with dyskinesia being the most frequently reported treatment-emergent adverse reaction (17.7%) [27].
Dyskinesia was considered an adverse event of special interest. This is due to the potent dopaminergic effect of opicapone, which can increase the risk of dyskinesia [37]. As expected, our results suggest that patients receiving either dose of opicapone were significantly more likely to suffer from dyskinesia compared with control groups. Similar results were obtained in the study of Kwak et al. [25]. However, it should be stressed that dyskinesia did not affect adherence to medication in any of the included studies. Moreover, as mentioned earlier, opicapone did not increase the time with troublesome dyskinesia in any of the studies.
The current meta-analysis has several limitations. First, studies included in the analysis had a relatively short treatment period, and the use of long-term open-label phases was not possible due to the single-armed protocol. This limitation should be considered particularly in the context of levodopa (and thus also opicapone) being a long-term treatment. Second, the number of studies included in the meta-analysis was relatively small. However, they are the only RCTs currently available on this topic. Third, the meta-analysis focused mainly on end points related to the OFF and ON states, as well as the safety profile. Nevertheless, it should be mentioned that these end points were directly related to the specific goal of using COMT inhibitors, namely a reduction in the OFF-time and a decrease of end-of-dose motor fluctuations. In addition, these end points are clinically significant and have been used in studies assessing other COMT inhibitors. Finally, due to differences in the definitions of the end point, no meta-analysis has been conducted so far for the ON-time without dyskinesia. However, the results of individual studies were reported. One more limitation is that COMFORT-PD study was conducted in Japanese population with a different formulation, and these two variables (Japanese population and different formulation) could somehow introduce bias to the analysis. However, the meta-analysis also includeso a sensitivity analysis that was carried out excluding the COMFORT-PD study. The results of sensitivity analysis were in line with the results of the main analysis. Both BIPARK-1 and BIPARK-2 studies were funded by BIAL – the marketing authorization holder of opicapone (Ongentys®), whereas the study COMFORT-PD was funded by Ono Pharmaceutical Co, Ltd (Osaka, Japan). Nevertheless, regardless of the sponsor of the study, the results are consistent.
The main strength of the study is the fact that it is the aggregation of results specifically concerning the use of opicapone in Parkinson’s disease, including the newest COMFORT-PD study and providing complex information including many end points regarding clinical effectiveness, as well as the safety profile of the analyzed drug. This gap prompted us to perform a meta-analysis, which is an objective measure of the integrated quantitative evidence. The study by Kwak et al. [25], despite the similar objective, assessed only a few efficacy end points (OFF-time change, risk of dyskinesia, ON-time without troublesome dyskinesia). In our study, we additionally conducted an extensive efficacy analysis with assessment of change from the baseline in the results in clinically relevant efficacy scales: UPDRS, PDSS, NMSS and PDQ-39, time in the ON state and also the number of patients with decreased levodopa dose. In addition, we conducted a broader safety profile analysis, including assessment of number of patients with any treatment-emergent adverse events and serious adverse events, as well as adverse events leading to discontinuation of the study, which has not been included in the study of Kwak et al. [25]. Moreover, to our knowledge, no clinical trials on large groups of patients are currently scheduled to be conducted. Therefore, a meta-analysis seems to be the optimal/best way to provide data on the efficacy and safety of opicapone versus placebo.
Conclusion
Opicapone at a dose of 25 and 50 mg once daily consistently decreased the time spent in the OFF state and increased the time spent in the ON state, including the period without troublesome dyskinesia. Importantly, it also allowed a reduction of the levodopa dose, which can be beneficial not only in clinical terms but also economically from the perspective of the national healthcare provider. Additionally, no significant differences in primary and secondary end points were discovered between active treatment doses (25 mg and 50 mg). A higher incidence of dyskinesia with opicapone than with placebo is in line with a potent dopaminergic effect of this drug. However, it should be noted that dyskinesia did not affect treatment adherence. Moreover, there were no significant differences between opicapone and placebo in terms of serious treatment-emergent adverse events and adverse events leading to the discontinuation of the study. This indicates that opicapone as an add-on to standard levodopa therapy is well tolerated and has a favorable safety profile.
Future perspective
The obtained results are essential for clinical practitioners. Further research is needed to confirm long-term effectiveness of opicaopne in real world setting, preferably large observational studies as well as studies with direct comparison with other COMT.
•
Opicapone provides a greater reduction in the absolute OFF-time compared with placebo.
•
Opicapone increases the chances of ≥1-h reduction in the OFF-time compared with placebo.
•
Opicapone increases the chances of ≥1-h increase in the ON-time compared with placebo.
•
Receiving opicapone more often facilitates levodopa dose reduction versus placebo.
•
There are no differences in the occurrence of adverse events, including severe and leading to drug discontinuation, between opicapone and placebo, but receiving opicapone increases the frequency of dyskinesia.
•
Opicapone demonstrates superior clinical efficacy to placebo and a comparable general safety profile.
Author contributions
P Kawalec and M Żegleń conceived and designed the analysis. M Żegleń and K Śladowska performed the systematic review, data extraction and calculations. M Żegleń performed the analysis, generated figures and prepared the first draft of the paper. P Kawalec, T Brzostek and K Śladowska critically reviewed and edited the paper. All authors contributed to and accepted the final version of the manuscript.
Financial & competing interests disclosure
Financed with project N43/DBS/000099 (Jagiellonian University Medical College). The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary tables.docx)
- Download
- 30.87 KB
References
1.
Mu J, Chaudhuri K, Bielza C, de Pedro-Cuesta C, Larrañaga P, Martinez-Martin P. Parkinson’s disease subtypes identified from cluster analysis of motor and non-motor symptoms. Front. Aging Neurosci. 9, 301 (2017).
2.
Baram S, Karlsborg M, Øzhayat EB, Bakke M. Effect of orofacial physiotherapeutic and hygiene interventions on oral health-related quality of life in patients with Parkinson’s disease: a randomised controlled trial. J. Oral Rehabil. 48(9), 1035 (2021).
3.
de Lau L, Breteler M. Epidemiology of Parkinson’s disease. Lancet Neurol. 5(6), 525–535 (2006).
4.
Salamon A, Zádori D, Szpisjak L, Klivényi P, Vécsei L. Opicapone for the treatment of Parkinson’s disease: an update. Expert Opin. Pharmacother. 20(18), 2201–2207 (2019).
5.
Rodrigues FB, Ferreira JJ. Opicapone for the treatment of Parkinson’s disease. Mov. Disord. 18(4), 445–453 (2017).
6.
Marras C, Beck JC, Bower JH et al. Prevalence of Parkinson’s disease across North America. NPJ Parkinsons Dis. 4, 21 (2018).
7.
Chinta S, Andersen J. Dopaminergic neurons. Int. J. Biochem. Cell Biol. 37(5), 942–946 (2005).
8.
Rogers G, Davies D, Pink J, Cooper P. Parkinson’s disease: summary of updated NICE guidance. BMJ 358, j1951 (2017).
9.
Annus Á, Vécsei L. Spotlight on opicapone as an adjunct to levodopa in Parkinson’s disease: design, development and potential place in therapy. Drug Des. Devel. Ther. 11, 143–151 (2017).
10.
European Parkinson’s Disease Association (2022). www.epda.eu.com/
11.
Olanow W, Poewe W, Rascol O, Stocchi F. From OFF to ON – treating OFF episodes in Parkinson’s disease. US Neurol. 17(1), 36 (2020).
12.
Poewe WH, Deuschl G, Gordin A, Kultalahti E-R, Leinonen M. Efficacy and safety of entacapone in Parkinson’s disease patients with suboptimal Levodopa response: a 6-month randomized placebo-controlled double-blind study in Germany and Austria (Celomen study). Acta Neurol. Scand. 105(4), 245–255 (2002).
13.
Deane K, Spieker S, Clarke CE. Catechol-O-methyltransferase inhibitors for levodopa-induced complications in Parkinson’s disease. Cochrane Database Syst. Rev. 2004(4), CD004554 (2004).
14.
Koller W, Lees A, Doder M, Hely M. Randomized trial of tolcapone versus pergolide as add-on to levodopa therapy in Parkinson’s disease patients with motor fluctuations. Mov. Disord. 16(5), 858–866 (2001).
15.
Adler CH, Singer C, O’Brien C et al. Randomized, placebo-controlled study of tolcapone in patients with fluctuating Parkinson disease treated with levodopa-carbidopa. Arch. Neurol. 55(8), 1089–1095 (1998).
16.
Fabbri M, Ferreira JJ, Lees A et al. Opicapone for the treatment of Parkinson’s disease: a review of a new licensed medicine. Mov. Disord. 33(10), 1528–1539 (2018).
17.
MedlinePlus. Levodopa and carbidopa (2021). https://medlineplus.gov/druginfo/meds/a601068.html
18.
Fernandez HH, Chen JJ. Monoamine oxidase-B inhibition in the treatment of Parkinson’s disease. Pharmacotherapy 27(12 Pt 2), 2007).
19.
Margolesky J, Singer C. Extended-release oral capsule of carbidopa-levodopa in Parkinson disease. Ther.Adv.Neurol.Disord. 11, 1756285617737728 (2018).
20.
Suski V, Stacy M. Dopamine agonists. In: Handbook of Parkinson’s Disease (5th Edition). Pahwa R, Lyons KE (Eds). CRC Press, FL, USA, 414– 429 (2021).
21.
Greenwood J, Pham H, Rey J. Opicapone: a third generation COMT inhibitor. Clin. Park. Relat. Disord. 4, 100083 (2021).
22.
Fox SH, Katzenschlager R, Lim S-Y et al. International Parkinson and Movement Disorder Society evidence-based medicine review: update on treatments for the motor symptoms of Parkinson’s disease. Mov. Disord. 33(8), 1248–1266 (2018).
23.
Song Z, Zhang J, Xue T et al. Different catechol-O-methyl transferase inhibitors in Parkinson’s disease: a Bayesian network meta-analysis. Front. Neurol. 12, 1657 (2021).
24.
Singh A, Gupta D, Dhaneria S, Sheth PG. Istradefylline versus opicapone for “off” episodes in Parkinson’s disease: a systematic review and meta-analysis. Ann. Neurosci. 28(1-2), 65–73 (2021).
25.
Kwak N, Park J, Kang H-Y, Lee M-J, Suh JK, Lee H. Efficacy and safety of opicapone for motor fluctuations as an adjuvant to levodopa therapy in patients with Parkinson’s disease: a systematic review and meta-analysis. J. Parkinsons Dis. 12(3), 773–783 (2022).
26.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int. J. Surg. 8(5), 336–341 (2010).
27.
EMA. Summary of Product Characteristics. Amsterdam, The Netherlands (2016).
28.
USFDA. Highlights of Prescribing Information MD, USA (2020).
29.
EMA. Committee for medicinal products for human use (CHIMP) assessment Report. Amsterdam, The Netherlands (2011).
30.
Higgins J. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March2011]. Cochrane Collaboration. London, UK (2011).
31.
BIPARK-1. Efficacy and Safety of BIA 9-1067 in Idiopathic Parkinson’s Disease Patients with ‘Wearing-off’ Phenomenon – Full Text View – ClinicalTrials.gov (2012). https://clinicaltrials.gov/ct2/show/NCT01568073
32.
Ferreira JJ, Lees A, Rocha J-F, Poewe W, Rascol O, Soares-Da-Silva P. Opicapone as an adjunct to levodopa in patients with Parkinson’s disease and end-of-dose motor fluctuations: a randomised, double-blind, controlled trial. Lancet Neurol. 15(2), 154–165 (2015).
33.
Lees AJ, Ferreira J, Rascol O et al. Opicapone as adjunct to levodopa therapy in patients with Parkinson disease and motor fluctuations: a randomized clinical trial. JAMA Neurol. 74(2), 197–206 (2017).
34.
BIPARK-2. Efficacy and Safety of BIA 9-1067 in Idiopathic Parkinson’s Disease Patients – Full Text View – ClinicalTrials.gov (2010). https://clinicaltrials.gov/ct2/show/NCT01227655
35.
Takeda A, Takahashi R, Tsuboi Y et al. Randomized, controlled study of opicapone in Japanese Parkinson’s patients with motor fluctuations. Mov. Disord. 36(2), 415 (2021).
36.
Poewe W, Seppi K, Tanner CM et al. Parkinson disease. Nat. Rev. Dis. Primers 3(1), 1–21 (2017).
37.
Castro Caldas A, Teodoro T, Ferreira JJ. The launch of opicapone for Parkinson’s disease: negatives versus positives. Expert Opin. Drug. Saf. 17(3), 331–337 (2018).
38.
Hauser RA, Gordon MF, Mizuno Y et al. Minimal clinically important difference in Parkinson’s disease as assessed in pivotal trials of pramipexole extended release. Parkinsons Dis. 2014, 467131 (2014).
39.
Palmer CS, Schmier JK, Snyder E, Scott B. Patient preferences and utilities for ‘off-time’ outcomes in the treatment of Parkinson’s disease. Qual. Life Res. 9(7), 819–827 (2000).
40.
Nicholas AP, Borgohain R, Chaná P et al. A randomized study of rotigotine dose response on ‘off’ time in advanced Parkinson’s disease. J. Parkinsons Dis. 4(3), 361–373 (2014).
41.
Chaudhuri KR, Jenner P, Antonini A. Should there be less emphasis on levodopa-induced dyskinesia in Parkinson’s disease? Mov. Disord. 34(6), 816–819 (2019).
42.
Ferreira JJ, Lees A, Rocha JF, Poewe W, Rascol O, Soares-da-Silva P. Long-term efficacy of opicapone in fluctuating Parkinson’s disease patients: a pooled analysis of data from two phase 3 clinical trials and their open-label extensions. Eur. J. Neurol. 26(7), 953–960 (2019).
43.
Takeda A, Takahashi R, Tsuboi Y et al. Long-term safety and efficacy of opicapone in Japanese Parkinson’s patients with motor fluctuations. J. Neural Transm. 128(3), 337–344 (2021).
44.
Ferreira JJ, Lees AJ, Poewe W et al. Effectiveness of opicapone and switching from entacapone in fluctuating Parkinson disease. Neurology 90(21), e1849–e1857 (2018).
45.
Vokurka P, Barron A, Sumaria S et al. Opicapone efficacy and tolerability in Parkinson’s disease patients reporting insufficient benefit/failure of entacapone. Mov. Disord. Clin. Pract. 7(8), 955 (2020).
46.
Reichmann H, Lees A, Rocha JF et al. Effectiveness and safety of opicapone in Parkinson’s disease patients with motor fluctuations: the OPTIPARK open-label study. Transl. Neurodegener. 9(1), 1–9 (2020).
47.
Nakamagoe K, Tsuji H, Ishii K, Tamaoka A. Remarkable clinical responses of non-fluctuating Parkinson’s disease (PD) after alternating catechol O-methyltransferase inhibitors: case series switching from entacapone 200∼300 mg/day to opicapone 25 mg/day. Neurol. Sci. 42(11), 4813–4814 (2021).
48.
Leta V, Van Wamelen DJ, Sauerbier A et al. Opicapone and levodopa-carbidopa intestinal gel infusion: the way forward towards cost savings for healthcare systems? J. Parkinsons Dis. 10(4), 1535–1539 (2020).
Information & Authors
Information
Published In
Pages: 889 - 904
PubMed: 35758044
Copyright
© 2022 Future Medicine Ltd.
History
Received: 14 February 2022
Accepted: 24 May 2022
Published online: 27 June 2022
Keywords:
Topics
Authors
Funding Information
Jagiellonian University Medical College: N43/DBS/000099
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Opicapone as an add-on to levodopa for reducing end-of-dose motor fluctuations in Parkinson’s disease: a systematic review and meta-analysis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2022-0031
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yuki Yasutaka, Takayasu Mishima, Kentaro Ogata, Akira Yokote, Hidetoshi Kamimura, Yasuhiko Baba, Factors affecting continuation rates of opicapone: A retrospective study at a single center in Japan, Clinical Neurology and Neurosurgery, 10.1016/j.clineuro.2025.108875, 252, (108875), (2025).
- Thomas Müller, Clinical pharmacokinetics of levodopa and relevant add-on therapies for Parkinson’s disease, Expert Opinion on Drug Metabolism & Toxicology, 10.1080/17425255.2024.2428831, 21, 3, (279-288), (2024).
- Wenshuo Wu, Xiaohui Lu, Liping Zhang, Du Hong, Effectiveness and safety of different catechol-o-methyl transferase inhibitors for patients with parkinson’s disease: Systematic review and network meta-analysis, Clinical Neurology and Neurosurgery, 10.1016/j.clineuro.2024.108189, 239, (108189), (2024).
- Matilde Otero-Losada, Paolo Gubellini, Francisco Capani, Santiago Perez-Lloret, Editorial: Neuroprotection and disease modification in Parkinson’s disease: Volume II, Frontiers in Pharmacology, 10.3389/fphar.2022.1121513, 13, (2023).
- Luwen Xie, Xiaoyi Qi, Xuan Wang, Bing He, Yu Wang, Wei Zhang, Zehui Yu, Mingming Deng, Sicheng Liang, Muhan Lü, Adverse event profiles of adjuvant treatment with opicapone in Parkinson’s disease: A systematic review and meta-analysis, Frontiers in Pharmacology, 10.3389/fphar.2022.1042992, 13, (2022).