Acute effects of resistance exercise with blood flow restriction on cardiovascular response: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the acute effects of low-load resistance training associated with blood flow restriction (LLRT-BFR) with low-load resistance training (LLRT) and high-load resistance training (HLRT) on cardiovascular outcomes in healthy individuals. Methods: This review was registered and the studies were selected using seven databases. Randomized controlled clinical trials were included that evaluated LLRT-BFR compared with LLRT and HLRT in young individuals for the cardiovascular outcomes. Results: 19 studies were included. In the comparison of LLRT-BFR with HLRT, there were significant differences for cardiac output and heart rate – with reduced values and in favor of LLRT-BFR. Conclusion: There are no greater acute effects of the addition of blood flow restriction, with the exception of the reduction in cardiac output and heart rate for LLRT-BFR compared with HLRT.
Resistance training is a training modality performed to gain muscle strength and hypertrophy in several populations, such as older adults and trained individuals [1–3]. Individuals with musculoskeletal dysfunction, in the process of rehabilitation and/or diagnosed with cardiovascular disease are not suitable to perform high-load resistance training (HLRT) [3,4]. For this reason, resistance training associated with blood flow restriction (BFR) appears as an alternative training model for strength gain and muscle hypertrophy in this population [5,6].
The methodology of low-load resistance training associated with blood flow restriction (LLRT-BFR) includes the application of a pressure cuff on the proximal portion of the limb to be trained and an exercise intensity varying between 20 and 50% of one maximum repetition (1RM) [5,6]. Although the BFR method has been used as an alternative model for patient population, it is currently also being used by active and healthy populations to optimize muscle strength and hypertrophy [7,8].
In addition, cardiovascular outcomes such as systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP) and heart rate (HR) are influenced by the BFR that is modulated by the pressor reflex of the exercise, which increases sympathetic activity and decreases parasympathetic activity by the resistance training stress [9,10]. This feedback system is necessary to perform any physical activity and is important in the adaptation of the individual to stress [9,10]. However, the cardiovascular safety must be considered, and the impact of LLRT-BFR and its training variables on cardiovascular outcomes is not yet known when applied to a healthy population.
Domingos and Polito [11] demonstrated, in a systematic review with meta-analysis, that there is a hypotensive effect for 30–60 min after resistance training associated with BFR. However, these findings were related to a heterogeneous population composed of trained older individuals [11]. Thus, the application of this exercise model on cardiovascular repercussions is still questionable, as there are gaps to be clarified for the healthy population, among which we can highlight the partial blood occlusion method (intermittent or continuous) and the region to be occluded: upper limbs or lower limbs. Understanding the cardiovascular effects of resistance training associated with BFR is necessary to better comprehend this exercise modality and to establish a better training prescription prior to prescribing it for musculoskeletal injuries as the population ages. Therefore, the objective of this systematic review with meta-analysis was to compare the acute effects of LLRT-BFR with low-load resistance training (LLRT) and HLRT on cardiovascular outcomes in healthy individuals.
Methods
This systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), and the protocol was registered in an international database of systematic reviews in health and social assistance, PROSPERO (registration number CRD42019142900, www.crd.york.ac.uk/PROSPERO/). According to Elkins [12], this process is important to increase transparency and accountability of the information presented.
Search strategies
The studies were selected from seven databases (MEDLINE, EMBASE, the Cochrane Library, Scientific Electronic Library Online [SciELO], SportDiscus, the Cumulative Index to Nursing and Allied Health Literature [CINAHL], and Physiotherapy Evidence Database [PEDro]) from the oldest record in each database until 13 January 2022. The terms and keywords used to optimize the search were related to BFR, venous occlusion, hemodynamic responses, strength training and randomized clinical trial (see details in Supplementary Material Appendix 1). There were no restrictions on the language of the studies.
Selection criteria
The selected studies involved resistance training associated with BFR in healthy participants and cardiovascular outcomes of SBP, DBP, MAP, HR, stroke volume, cardiac output, partial oxygen saturation, peripheral vascular resistance and double product (calculated by the formula SBP x HR).
To be eligible, studies were required to include the following criteria:
•
Randomized controlled clinical trials comparing LLRT-BFR versus LLRT, comparing LLRT-BFR versus HLRT or comparing LLRT-BFR versus LLRT and HLRT;
•
Studies that evaluated the acute cardiovascular effects before and after LLRT-BFR for at least one of the following cardiovascular outcomes: SBP, DBP, MAP, HR, stroke volume, cardiac output, partial oxygen saturation, peripheral vascular resistance and double product;
•
Studies with healthy participants aged 18–35 years.
Studies that did not perform a comparison between LLRT-BFR and the proposed comparators and studies composed of individuals with a cardiovascular, metabolic or musculoskeletal injury were excluded.
The study selection process was carried out initially by excluding duplicates, followed by exclusions according to the title, abstract and reading the full text. The reference lists of the selected full texts were manually reviewed to obtain potentially eligible studies that were not retrieved electronically. These steps were carried out by two independent evaluators, and in case of disagreements in the final selection of the studies, a third evaluator decided on the exclusions.
Data extraction
Outcome data, including final mean values, standard deviations and sample size, were extracted by two independent researchers. The data extraction process was carried out using a standardized form, which included details such as characteristics of the participants, procedures of resistance training regarding the volume of load and intensity of the exercise, and procedures for applying the BFR and methodological characteristics. Disagreements between authors regarding data extractions were resolved by a third reviewer. In cases where data were not reported in the article, the corresponding author was contacted by email and an email reminder was sent after 1 week. Answers or missing answers were noted. It is noteworthy that all reviewers involved in these processes were familiar with the topic investigated.
Description of interventions
Intervention information was extracted using the Template for Intervention Description and Replication (TIDieR) [13]. The TIDieR is a checklist of 12 items developed to improve the reporting of interventions.
Risk of bias assessment
All included studies were assessed for risk of bias using the PEDro scale [14], carried out by independent researchers. The PEDro scale is an 11-item scale (eligibility criteria; random allocation; hidden allocation; baseline comparability; blind participants; blind therapists and evaluators; adequate follow-up; intention-to-treat analysis; comparison between groups; point estimates and variability) – presenting a maximum score of 10 points (the item ‘eligibility criteria’ is not counted in the final score) – and is a valid tool to measure the risk of bias and the statistical analysis of clinical trials, in which the higher the score, the lower the risk of bias [15,16]. None of the included studies were indexed in PEDro; therefore, all scores were performed manually by the researchers. Methodological quality was not an inclusion criterion.
Quality of evidence
The quality of the evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation System (GRADE) [17]. The GRADE approach establishes the quality of evidence as high, moderate, low and very low. The tool includes five domains that are able to decrease the quality of the evidence: study design and risk of bias, consistency of results, directness (generalizability of the findings), precision (i.e., sufficient data to produce narrow confidence intervals) and other factors (e.g. reporting bias, publication bias). The effect of publication bias was verified through funnel plot analysis (Supplementary Material Appendix 2).
The quality of evidence was then classified for each outcome according to the following criteria: high-quality evidence (consistent findings among at least 75% of eligible studies with low risk of bias; consistent, direct and precise data and no known or suspected publication biases; further research is unlikely to change either the estimate or confidence in the results), moderate-quality evidence (one of the GRADE domains is not met; further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate), low-quality evidence (two of the GRADE domains are not met; further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate) and very low quality evidence (three of the GRADE domains are not met; we are very uncertain about the results). Single studies with a sample size smaller than the optimal information size (n = 400) were considered to yield very low quality evidence if there was also a high risk of bias (PEDro score <6) [18].
Data synthesis & analysis
Data were extracted for acute-effects follow-up (recovery period immediately after the exercise protocol and up to 60 min after the exercise). For the exploratory analyses of the present review, the data were extracted from the anatomical limb that performed the resistance training (upper limbs or lower limbs) and technique of BFR used (intermittent or continuous).
All meta-analyses were conducted using the software Review Manager – RevMan (version 5.3, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Pooled estimates were calculated using a random effect model. Data were grouped in meta-analyses and described as mean differences (MDs) with 95% CIs [17].
Results
The search identified 6166 studies from the following databases: MEDLINE (5857 studies), EMBASE (21 studies), COCHRANE (165 studies), SCIELO (27 studies), SportDiscus (26 studies), CINAHL (24 studies) and PEDro (46 studies). Of this total, 1183 duplicates were removed and 4983 studies were analyzed according to titles and abstracts. In the end, 29 studies remained for full text review. Of these studies, 19 clinical trials [19–37] met all eligibility criteria and were included for qualitative analysis. For quantitative analysis, 17 studies were included, as two studies [27–34] did not send the data for the meta-analysis.
Figure 1 shows the schematic process for selecting the studies based on a PRISMA flow chart.
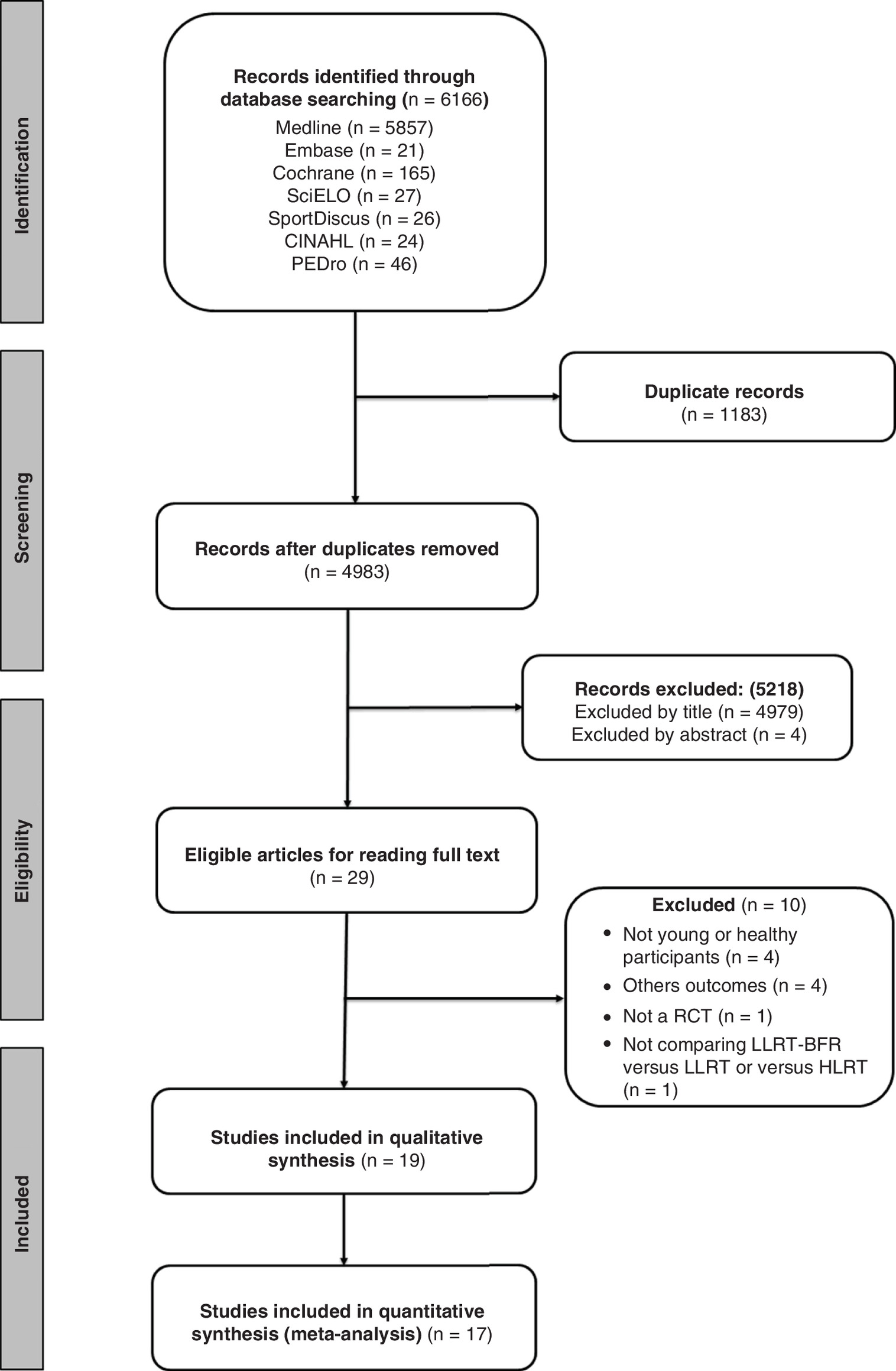
Figure 1. Flowchart of study selection.
BFR: Blood flow restriction; CINAHL: Cumulative Index to Nursing and Allied Health Literature; HLRT: High-load resistance training; LLRT: Low-load resistance training; LLRT-BFR: Low-load resistance training associated with blood flow restriction; PEDro: Physiotherapy Evidence Database; RCT: Randomized clinical trial; SciELO: Scientific Electronic Library Online.
Description of the studies
The 19 eligible studies were published between 2010 [22] and 2019 [31]. Of these, 13 studies [20–24,27,30,32–37] were randomized crossover clinical trials and six [19,25,26,28,29,31] randomized clinical trials with parallel groups. The comparison group was considered as any study group that performed some type of resistance training without BFR (LLRT, HLRT or LLRT and/or HLRT). The studies came from Australia [20], Brazil [21,23–25,27–30,32–34,36,37], the USA [22,26,31,35] and Iran [19].
The sample size of the studies ranged from eight to 90 participants with a mean (standard deviation) of 21.94 ± 22.78 participants and 472 participants. Almost all studies included young, healthy adults aged 18–35 years. Only the study of Vieira et al. [36] included healthy young and older adults – who were analyzed separately and included in this systematic review. The included studies reported the characteristics of the participants as being ‘healthy young men’ [19,23,24,27,28,30,37], ‘physically active and healthy young men’ [20,21,25,33,35], ‘healthy, trained young men’ [29,32,34] and ‘healthy men and women’ [22,26,31].
Regarding the intervention used, as a method of comparison, six studies [19,22,25,28,30,37] compared LLRT-BFR with LLRT, three studies [21,23,24] compared LLRT-BFR with HLRT and ten studies [20,26,27,29,31–36] performed both comparisons.
Regarding the training methodology, seven studies [19,20,26–28,30,34] used a wide pressure cuff, six studies [23–25,31,35,37] used a narrow pressure cuff, three studies used both [21,33,34] and three studies [22,29,36] did not report the size of the cuff.
With respect to the type of restriction, nine [21–23,30,32,33,35–37] used intermittent restriction, five [19,27,28,31,34] used continuous restriction, three studies [20,24,25] used both and two [26,29] did not report which method was used.
Considering the value of occlusion pressure used during LLRT-BFR, nine studies [19,22,25,27,28,30,32,33,36,37] used occlusion pressure <120 mm Hg, five studies [21,23,24,29,34] used pressures >120 mm Hg, three studies [20,26,35] used both occlusion pressures and only one study [31] did not report the pressure of occlusion used.
The lower limb exercises performed were ‘knee extension’ [19,21,26,34], ‘knee flexion and extension’ [22,32,33,35], ‘leg press’ [27,35], ‘squat’ [29] and ‘plantar flexion’ [35]. The upper limb exercises performed were ‘elbow flexion and extension’ [20,21,23–25,30,32,33], ‘elbow flexion’ [24,28,31,36,37], ‘bench press’ [23–25], ‘seated shoulder lift’ [30] and ‘pull down’ [23–25].
Regarding blood pressure (BP) outcomes, 17 studies [19–23,25–31,33–37] analyzed SBP and DBP, and of these, 11 [20–23,25,27,28,33,35–37] performed MAP analysis. The instruments used to measure each cardiovascular outcome were diverse. Seven studies [19,25,26,28,31,33,35] used the automatic method, five studies [20,21,23,29,37] used the auscultatory method, two studies [22,30] used the oscillometric method and three studies [27,34,36] used photoplethysmography.
For the HR, 11 studies [19–22,24,25,27,32,34–36] were found, of which seven studies [19–21,25,32,36,37] used pulse cardiofrequency, two studies [25,35] used the automatic method, one study [27] used the electrocardiogram, one study [22] used the oscillometric method and one study [34] used photoplethysmography. For the double product, six studies [21,24,29,32,36,37] measured the variable using arithmetic formulas.
Four studies [20,27,34,35] performed the analysis of cardiac output and stroke volume. To measure the cardiac output, the following were used: partial rebreathing of carbon dioxide [20], photoplethysmography [34], echocardiogram [35] and mathematical formulas [27], whereas for stroke volume, photoplethysmography [34] echocardiogram [35] and arithmetic formulas [20,27] were used.
Only three studies [27,34,35] performed analysis for the peripheral vascular resistance using arithmetic formulas [27] and photoplethysmography [34,35], whereas three studies [19,29,32] performed partial oxygen saturation measurement using a pulse oximeter. It was not possible to perform any meta-analysis for the peripheral vascular resistance and partial oxygen saturation due to the insufficient number of studies. Full descriptions of the included studies can be found in Table 1.
| Study, year | Characteristics of the participants | LLRT-BFR | Comparison group | Outcome | Analysis moments | Ref. |
|---|---|---|---|---|---|---|
| Bazgir et al., 2016 | Men 25.50 ± 3.74 years – [LLRT-BFR] 27.33 ± 3.01 years – [LLRT] | LLRT-BFR (n = 10) Knee extension – 4 sets x (INCOMPLETE DATA) 30% of MVC BFR: 90–100 mm Hg | LLRT (n = 6) Knee extension – 4 sets x (INCOMPLETE DATA) 30% of MVC | SBP, DBP, MAP, HR, partial oxygen saturation | Baseline; after 1st, 2nd, 3rd and 4th set | [19] |
| Brandner et al., 2015 | Physically active men 23.0 ± 3.0 years | LLRT-BFR continuous (n = 12) Elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 91.0 ± 2.0 mm Hg LLRT-BFR intermittent (n = 12) Elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 151.0 ± 4.0 mm Hg | HLRT (n = 12) Elbow flexion and extension – 4x 6–8 repetitions with 80% of 1RM and 30-s intervals between sets LLRT (n = 12) Elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets | SBP, DBP, MAP, HR, cardiac output, stroke volume | Baseline; after 2nd and 4th set; 5, 20, 40 and 60 min after the effort | [20] |
| Vilaça-Alves et al., 2016 | Physically active men 22.92 ± 1.96 years | LLRT-BFR continuous for upper limbs (n = 12) Elbow flexion and extension; knee flexion and extension – 30 × 15 × 15 × 15 with 20% of 1RM and 40 s of rest between sets LLRT-BFR continuous for lower limbs (n = 12) Elbow flexion and extension; knee flexion and extension – 30 × 15 × 15 × 15 with 20% of 1RM and 40 s of rest between sets BFR: 180 mm Hg for upper limbs and 220 mm Hg for lower limbs | HLRT for upper limbs (n = 12) Elbow flexion and extension; knee flexion and extension – 3 × 10 with 70% of 1RM and 90 s of rest between sets HLRT for lower limbs (n = 12) Elbow flexion and extension; knee flexion and extension – 3 × 10 with 70% of 1RM and 90 s of rest between sets | SBP, DBP, HR, double product | Baseline; immediately after the effort; 15, 30 and 45 min after the effort | [21] |
| Figueroa and Vicil, 2011 | Men and women 22.0 ± 2.0 years | LLRT-BFR (n = 12 women and 11 men) Knee flexion and extension – 3 sets to fatigue with 30% 1RM and 60-s intervals between sets BFR: 100 mm Hg | LLRT (n = 12 women and 11 men) Knee flexion and extension – 3 sets to fatigue with 30% 1RM and 60-s intervals between sets | SBP, DBP, MAP, HR | Baseline; Δ0–2 min Δ0–30 min | [22] |
| Rodrigues Neto et al., 2016 | Men (military) 19.0 ± 0.8 years | LLRT-BFR intermittent (n = 10) Bench press, pull down, elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 163.8 ± 10.5 mm Hg LLRT-BFR continuous (n = 10) Bench press, pull down, elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 160.9 ± 12.9 mm Hg | HLRT (n = 10) Bench press, pull down, elbow flexion and extension – 3 × 8 with 80% 1RM and 120-s intervals between sets LLRT (n = 10) Bench press, pull down, elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets | SBP, DBP, MAP | Baseline; immediately after the effort; 15, 30, 45 and 60 min after the effort | [23] |
| Rodrigues Neto et al., 2017 | Men (military) 19.0 ± 0.8 years | LLRT-BFR intermittent (n = 10) Bench press, pull down, elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 163.8 ± 10.5 mm Hg LLRT-BFR continuous (n = 10) Bench press, pull down, elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 160.9 ± 12.9 mm Hg | HLRT (n = 10) Bench press, pull down, elbow flexion and extension – 3 × 8 with 80% 1RM and 120-s intervals between sets LLRT (n = 10) Bench press, pull down, elbow flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets | HR, double product, TW | Baseline; immediately after the effort; 15, 30, 45 and 60 min after the effort | [24] |
| Rodrigues Neto et al., 2018 | Physically active men 23.8 ± 5.6 years (intermittent) 26.1 ± 5.0 years (continuous) | LLRT-BFR intermittent (n = 8) Bench press, pull down, elbow flexion and extension – 30 × 15 with 20% 1RM and 30-s intervals between sets BFR: 108.8 ± 9.2 mm Hg LLRT-BFR continuous (n = 9) Bench press, pull down, elbow flexion and extension – 4 × 15 with 20% 1RM and 30-s intervals between sets BFR: 117.5 ± 10.3 mm Hg | LLRT (n = 8) Bench press, pull down, elbow flexion and extension – 4 × 15 with 20% 1RM and 30-s intervals between sets | SBP, DBP, MAP, HR, TW | Baseline; immediately after the effort | [25] |
| Mattocks et al., 2018 | Men and women 18–35 years | LLRT-BFR with 40% MOP (n = 23) Knee extension – 4x to fatigue with 15% 1RM and 30-s intervals between sets BFR: 78 mm Hg LLRT-BFR with 80% MOP (n = 22) Knee extension – 4x to fatigue with 15% 1RM and 30-s intervals between sets BFR: 155.0 mm Hg | HLRT (n = 24) Knee extension – 4x to fatigue with 70% of 1RM and 30-s intervals between sets LLRT (n = 21) Knee extension – 4x to fatigue with 15% 1RM and 30-s intervals between sets | SBP, DBP | Baseline; immediately after the effort | [26] |
| Libardi et al., 2017 | Men 20.0 ± 3.0 years | LLRT-BFR (n = 12) 45° leg press – 4x fatigue with 30% 1RM and 60-s intervals between sets BFR: 75.8 ± 7.4 mm Hg | HLRT (n = 12) 45° leg press – 4x fatigue with 80% of 1RM and 60-s intervals between sets LLRT (n = 12) 45° leg press – 4x fatigue with 30% 1RM and 60-s intervals between sets | SBP, DBP, MAP, HR, stroke volume, cardiac output, peripheral vascular resistance | Between the sets; during the sets | [27] |
| Maior et al., 2015 | Men 23.4 ± 3.4 years | LLRT-BFR (n = 15) Elbow flexion – 3x fatigue with 40% 1RM and 60-s intervals between sets BFR: 109.4 ± 7.3 mm Hg | HLRT (n = 15) Elbow flexion – 3x fatigue with 80% 1RM and 60-s intervals between sets | SBP, DBP, MAP | Baseline; immediately after the effort; 10, 20, 30, 40, 50 and 60 min after the effort | [28] |
| Mota et al., 2018 | Physically active men (bodybuilders) 27.20 ± 6.89 years | LLRT-BRF (n = 10) Squats – 6 × 10-15 repetitions with 30% 1RM and 90-s intervals between sets BRF: 140–160 mm Hg | HLRT (n = 10) Squats – 6 × 10-15 repetitions with 70% 1RM and 90-s intervals between sets | SBP, DBP, double product, partial oxygen saturation | Baseline; immediately after the effort; 10 min after the effort | [29] |
| Moriggi et al., 2015 | Men 23.8 ± 4.0 years | LLRT-BFR (n = 8) Elbow flexion with free weights, elbow flexion on the scott bench, seated shoulder lift and elbow extension – 3 × 15 repetitions with 20% 1RM and 60-s intervals between each set BFR: 61.0 ± 5.0 mm Hg | HLRT (n = 8) Elbow flexion with free weights, elbow flexion on the scott bench, seated shoulder lift and elbow extension – 3 × 10 repetitions with 70% 1RM and 60-s intervals between each set | SBP, DBP | Baseline; immediately after the effort; 10, 20, 30, 40, 50 and 60 min after the effort | [30] |
| Mouser et al., 2019 | Men and women 18–35 years | LLRT-BFR with 40% MOP (n = 17) Elbow flexion – 4x to fatigue with 15% 1RM and 30-s intervals between sets BFR: 78 mm Hg LLRT-BFR with 80% MOP (n = 20) Elbow flexion – 4x to fatigue with 15% 1RM and 30-s intervals between sets BFR: 155 mm Hg | HLRT (n = 20) Elbow flexion – 4x to fatigue with 70% 1RM and 30-s intervals between sets LLRT (n = 22) Elbow flexion – 4x to fatigue with 15% 1RM and 30-s intervals between sets | SBP, DBP | Baseline; between the sets; after the effort | [31] |
| Rodrigues Neto et al., 2016 | Trained men 21.79 ± 3.21 years | LLRT-BFR (n = 24) Elbow flexion and extension; knee flexion and extension – 30 × 15 × 15 × 15 repetitions with 20% 1RM and 30-s intervals between sets BFR: 93.75 ± 12.09 mm Hg and 108.75 ± 11.53 mm Hg for upper limbs and lower limbs, respectively | HLRT (n = 24) Elbow flexion and extension; knee flexion and extension – 4 × 8 repetitions with 80% 1RM and 120-s intervals between sets LLRT (n = 24) Elbow flexion and extension; knee flexion and extension – 30 × 15 × 15 × 15 repetitions with 20% 1RM and 30-s intervals between sets | HR, double product, partial oxygen saturation | Baseline; immediately after the effort; 10, 20, 30, 40, 50 and 60 min after the effort | [32] |
| Rodrigues Neto et al., 2015 | Trained men 21.79 ± 3.21 years | LLRT-BFR (n = 24) Elbow flexion and extension; knee flexion and extension – 30 × 15 × 15 × 15 repetitions with 20% 1RM and 30-s intervals between sets BFR: 93.75 ± 12.09 mm Hg and 108.75 ± 11.53 mm Hg for upper limbs and lower limbs, respectively | HLRT (n = 24) Elbow flexion and extension; knee flexion and extension – 4 × 8 repetitions with 80% 1RM and 120-s intervals between sets LLRT (n = 24) Elbow flexion and extension; knee flexion and extension – 30 × 15 × 15 × 15 repetitions with 20% 1RM and 30-s intervals between sets | SBP, DBP, MAP, TW | Baseline; immediately after the effort; 10, 20, 30, 40, 50 and 60 min after the effort | [33] |
| Poton and Polito, 2016 | Trained men 23.4 ± 3.8 years | LLRT-BFR (n = 12) Knee extension – 3 × 15 with 20% 1RM and 45-s intervals between sets BFR: 167.9 ± 16.6 mm Hg | HLRT (n = 12) Knee extension – 3 × 8 repetitions with 80% 1RM and 60-s intervals between sets | SBP, DBP, HR, cardiac output, stroke volume, peripheral vascular resistance | Baseline; between the sets; immediately after the effort; 10 min after the effort | [34] |
| Rossow et al., 2011 | Physically active men 28.0 ± 5.0 years | LLRT-BFR (n = 10) Leg press, plantar flexion, knee flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets BFR: 200 mm Hg | HLRT (n = 10) Leg press, plantar flexion, knee flexion and extension – 3 × 10 repetitions with 70% 1RM and 60-s intervals between sets LLRT (n = 10) Leg press, plantar flexion, knee flexion and extension – 30 × 15 × 15 × 15 with 20% 1RM and 30-s intervals between sets | SBP, DBP, MAP, HR, cardiac output, stroke volume | Baseline; 30 and 60 min after the effort | [35] |
| Vieira et al., 2013 | Men 30.0 ± 3.0 years | LLRT-BFR (n = 15) Elbow flexion – 1x 3 min with 30% 1RM BFR: 120.0 mm Hg | LLRT (n = 15) Elbow flexion – 1x 3 min with 30% 1RM | SBP, DBP, MAP, HR, double product | Baseline; during exercise (1–3 min); immediately after and until 3 min after the effort | [36] |
| Bonorino et al., 2019 | Men 22.6 ± 2.0 years | LLRT-BFR (n = 10) Elbow flexion – 3 × 15 with 30% 1RM and 45-s intervals between sets BFR: 70% of SBP at rest | LLRT (n = 10) Elbow flexion – 3 × 15 with 30% 1RM and 45-s intervals between sets | SBP, DBP, MAP, HR, double product | Baseline; immediately after and until 15 min after the effort | [37] |
1RM: One maximum repetition; BFR: Blood flow restriction; DBP: Diastolic blood pressure; HLRT: High-load resistance training; HR: Heart rate; LLRT: Low-load resistance training; LLRT-BFR: Low-load resistance training associated with blood flow restriction; MAP: Mean arterial pressure; MOP: Maximum occlusion pressure; MVC: Maximum voluntary contraction; s: Second; SBP: Systolic blood pressure; TW: Total exercise work.
Quality of studies
To evaluate the methodological quality of the included studies, the PEDro scale was used, with an average of 5.05 ± 0.4 points. All studies lost points in the items: blind therapists, blind subjects, blind assessors and intention-to-treat analysis. Supplementary Material Appendix 3 shows the description of the clinical trials that met each criterion.
Regarding the evaluation of the quality of the evidence, low or very low evidence results were observed. Thus, it is quite likely that further research will have an important impact on the confidence of the estimate of the effect and may alter the estimate. Details of the evaluation of the quality of the evidence of the included studies according to the GRADE system are summarized in Supplementary Material Appendix 4.
Meta-analyses
The results of the grouped data did not show differences between LLRT-BFR compared with LLRT in the acute effects for SBP (14 studies, n = 366; MD: -1.03, 95% CI: [-4.54; 2.49]; p = 0.57; I2 = 64%), DBP (14 studies, n = 366; MD: 1.41, 95% CI: [-0.85; 3.66]; p = 0.22; I2 = 45%), MAP (ten studies, n = 231; MD: 1.57, 95% CI: [-1.07; 4.22]; p = 0.24; I2 = 44%), cardiac output (three studies, n = 56; MD: -0.02, 95% CI: [-0.36; 0.32]; p = 0.90; I2 = 37%), stroke volume (three studies, n = 56; MD: -0.77, 95% CI: [-3.31; 1.77]; p = 0.55; I2 = 0%) and HR (nine studies, n = 201; MD: 1.50, 95% CI: [-4.07; 7.07]; p = 0.60; I2 = 56%; Figure 2).
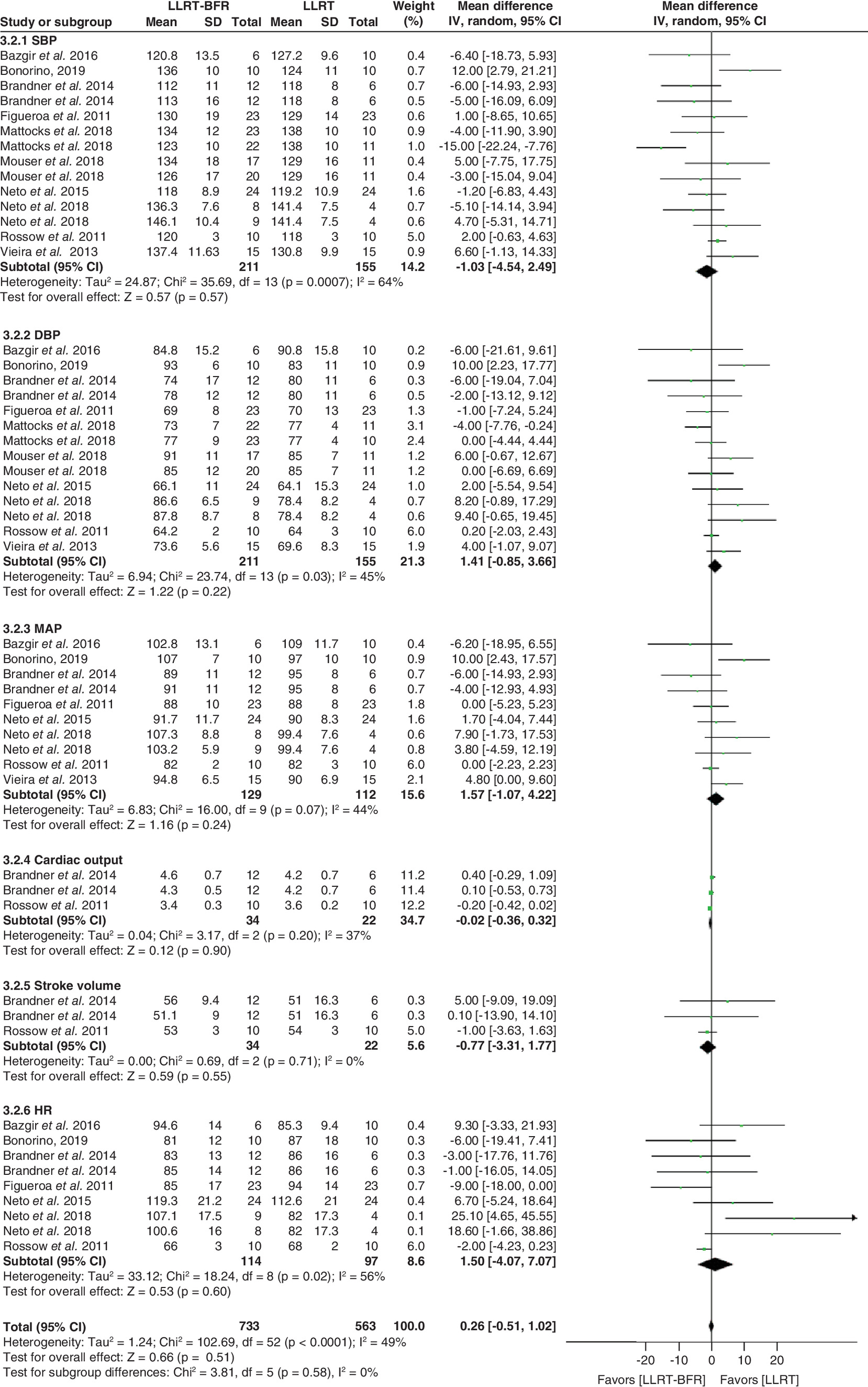
Figure 2. Forest plot illustrating the acute effects of low-load resistance training associated with blood flow restriction compared with low-load resistance training.
DBP: Diastolic blood pressure; HR: Heart rate; IV: Interval variable; LLRT: Low-load resistance training; LLRT-BFR: Low-load resistance training associated with blood flow restriction; MAP: Mean arterial pressure; SBP: Systolic blood pressure; SD: Standard deviation.
General analyses considering the comparison between LLRT-BFR and HLRT in the acute effect were performed and are described in Figure 3. The results of the grouped data demonstrated significant differences for the variables cardiac output (three studies, n = 56; MD: -0.63, 95% CI: [-0.86; -0.40]; p = 0.0001; I2 = 0%) and HR (ten studies, n = 232; MD: -15.19, 95% CI: [-24.70; -5.69]; p = 0.002; I2 = 88%). Both variables presented reduced values in favor of LLRT-BFR.
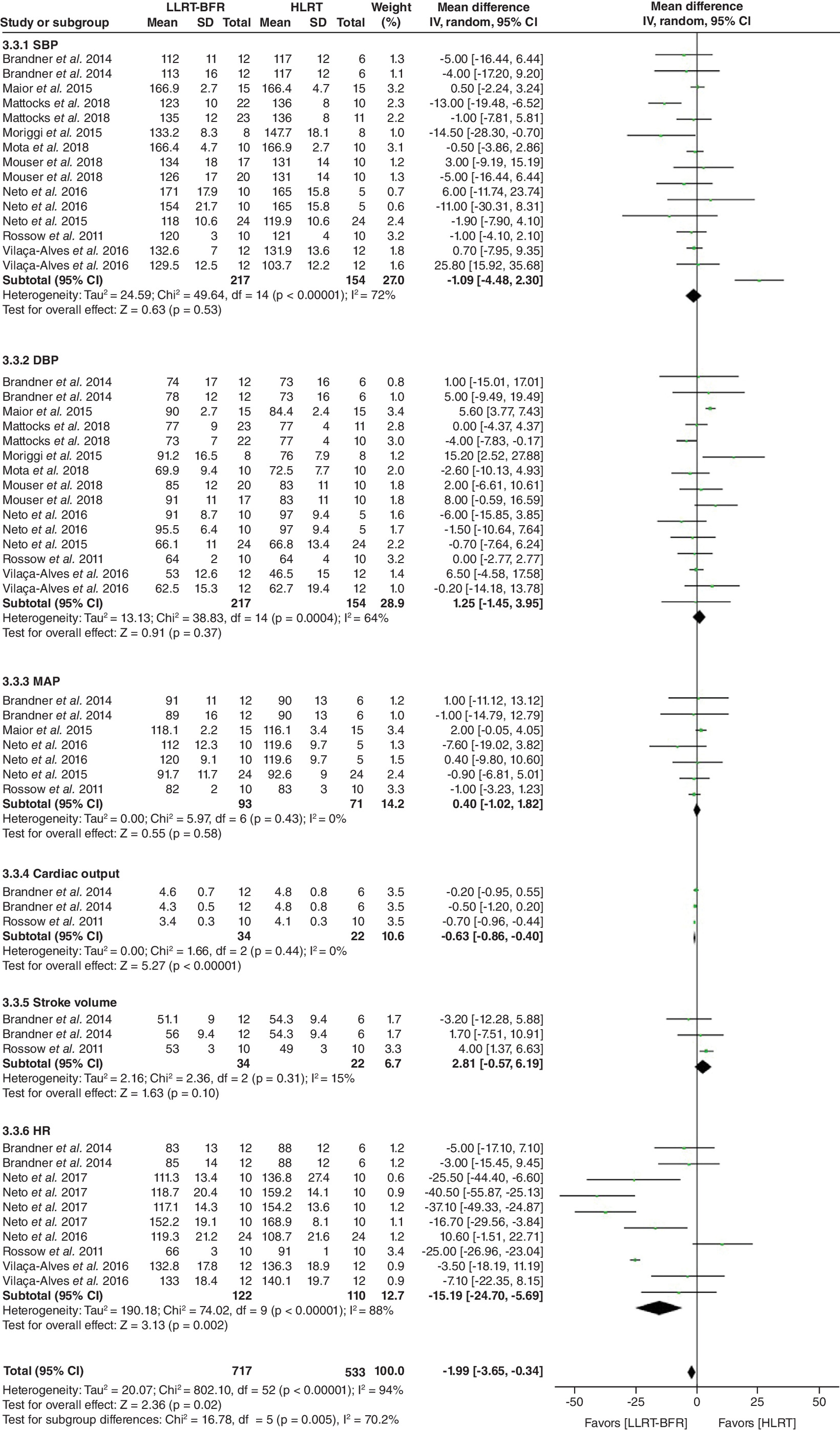
Figure 3. Forest plot illustrating the acute effects of low-load resistance training associated with blood flow restriction compared with high-load resistance training.
DBP: Diastolic blood pressure; HR: Heart rate; HLRT: High-load resistance training; IV: Interval variable; LLRT-BFR: Low-load resistance training associated with blood flow restriction; MAP: Mean arterial pressure; SBP: Systolic blood pressure; SD: Standard deviation.
For the SBP (15 studies, n = 371; MD: -1.09, 95% CI: [-4.48; 2.30]; p = 0.53; I2 = 72%), DBP (15 studies, n = 371; MD: 1.25, 95% CI: [-1.45; 3.95]; p = 0.37; I2 = 64%), MAP (seven studies, n = 164; MD: 0.40, 95% CI: [-1.02; 1.82]; p = 0.58; I2 = 0%) and stroke volume (three studies, n = 56; MD: 2.81, 95% CI: [-0.57; 6.19]; p = 0.10; I2 = 15%), there were no statistically significant differences between the two exercise modalities.
Some exploratory analyses were carried out. There was no difference of LLRT-BFR in lower limb exercises compared with LLRT and HLRT. As for upper limbs, DBP showed an increase in LLRT compared with LLRT-BFR (six studies, n = 130; MD: 4.46, 95% CI: [1.04; 7.88]; p = 0.01; I2 = 11%), whereas in comparison with HLRT, there was no difference.
For intermittent restrictions, LLRT-BFR was different from HLRT for HR (eight studies, n = 172; MD: -33.12, 95% CI: [-44.79; -21.46]; p = 0.00001; I2 = 91%). For continuous restrictions, there was difference of DBP favorable to HLRT compared with LLRT-BFR (five studies, n = 131; MD: 4.67, 95% CI: [2.15; 7.19]; p = 0.0003; I2 = 13%). The figures of these exploratory analyses can be found in Supplementary Material Appendix 5.
Discussion
The present systematic review with meta-analysis aimed to compare the acute effects of LLRT-BFR with LLRT and HLRT on cardiovascular outcomes in healthy individuals. The results of the present study demonstrated that there was no difference in the addition of BFR to resistance training for most of the cardiovascular parameters, with the exception of the cardiac output and HR, which presented lower values for LLRT-BFR compared with HLRT.
In addition, exploratory analyses showed that HR also presented lower values and was favorable to LLRT-BFR compared with HLRT for intermittent restriction, and DBP was shown to be increased for LLRT when analyzed in upper limbs and increased for HLRT when analyzed at continuous restriction.
Exercise with BFR is characterized by reduced or disrupted blood flow to a muscle group during exercise. The decrease in the supply of oxygen associated with muscle contraction provides a highly metabolic environment, which increases the afferent activity of the exercise pressor reflex, causing an increase in sympathetic nervous activity and, consequently, changes in cardiovascular responses [9].
During physical exercise, a cardiovascular imbalance occurs, mainly characterized by elevated BP. This increase occurs, in part, through activation of baroreceptors located in the carotid artery and aorta that generate action potentials [38]. These afferent signals are conducted to the central nervous system (CNS), which emits an efferent response in the heart, allowing the change in BP by sympathetic stimulation. After the end of the exercise, the suppression of the inputs coming from the CNS system and the cessation of the action of mechanoreceptors on the skeletal muscles provide a reactivation of the parasympathetic autonomic nervous system [38]. In addition, after exercise, metabolites produced by muscle contraction are removed, such as lactate and hydrogen ions, and there is a reduction in circulating catecholamines, a return of blood pH to baseline condition and normalization of temperature [38].
The regulation of these factors makes it possible to reduce the action of chemoreceptors, muscle metaboreceptors and thermoreceptors [38], producing a slow and steady decline in HR, mediated by the association of vagal reactivation [38]. In addition, the sympathetic tone for the heart and vessels is reduced, providing a decrease in cardiac contractility and in peripheral vascular resistance, leading to a reduction in BP.
However, this BP regulation is directly related to the intensity of the effort that promotes increases in cardiac output and peripheral vascular resistance, which impact on the proportional increase in SBP. Thus, when performing LLRT, lower HR values and, consequently, cardiac output, are expected during and after exertion, which justifies the findings of these favorable cardiovascular parameters for LLRT-BFR when compared with HLRT. Therefore, these findings can be explained by the intensity of the proposed exercise itself, which generates a proportional and linear increase in the face of increased metabolic demand and time of effort, a fact that also directly affects the post-exercise recovery behavior. Furthermore, this reinforces that the addition of BFR does not promote greater acute effects to HLRT in healthy individuals.
In relation to exploratory analyses, there was an increase in DBP for LLRT when analyzed in upper limbs and an increase in DBP for HLRT when analyzed with continuous restriction. The increase in DBP found in HLRT may be related to the exercise load performed, characterized by greater sensitization of the chemoreceptors located in the muscle itself during exercise and due to the high concentration of hydrogen ions and lactate during effort, as seen in the study of Rodrigues Neto et al. [25].
Another finding that deserves attention is in relation to the muscle mass involved in exercise. When analyzing the behavior in upper limbs, it is reported that BP values are higher compared with lower limb exercises [38]. This increase is due to vasoconstriction of inactive muscle groups, so the larger the muscle group involved in performing the exercise, the more arterioles will be dilated, providing lower values of peripheral vascular resistance and lower BP [38]. In addition, another plausible factor that justifies the increased DBP in LLRT is the production of nitric oxide, reducing the peripheral vascular resistance and, consequently, BP values [39].
Finally, HR also showed lower values and was favorable in LLRT-BFR compared with HLRT for intermittent restriction. It is believed that the exercise load was a determining factor for the findings of the present study since there is a proportional increase in HR with the intensity of the exercise. It is hypothesized that the application of BFR provides an increase in the action of the muscle pump by increasing the stroke volume and decreasing the HR values. Brandner et al. [20], when comparing two types of LLRT-BFR (intermittent and continuous) with HLRT and LLRT, observed that there was an increase in cardiac output in all groups, although only significant in HLRT. This increase may be linked to the increase in exercise intensity and, consequently, to the proportional increase in HR.
Regarding the clinical applicability of BFR, the results of the present review indicate that LLRT-BFR is an alternative and safe method for acute cardiovascular effects on a healthy population aged 18–35 years. However, it is necessary to highlight the limitations of the present study. Although this review included a comprehensive search in seven different databases and was composed of a large number of studies, they presented low methodological quality and low and very low levels of evidence assessed by the GRADE system. In addition, few studies investigated the effects of the variables HR, cardiac output, stroke volume, peripheral vascular resistance and partial oxygen saturation, which directly reflected on the level of evidence and, above all, on the impossibility of carrying out new exploratory analyses for these variables.
Finally, a major contributing factor that can be negatively affected by small but potentially significant differences between BRF exercises is the use of repetitions to failure versus the standard repetition scheme, so the physiological results must be interpreted with caution. Thus, attention should be paid to the criteria for the development of studies with high quality, especially, random allocation, blind advisor and intention-to-treat analysis, which would result in research with a higher level of scientific evidence. For future studies, it is recommended that clinical trials be conducted with more rigorous and robust methods in healthy populations.
Based on our knowledge, this is the first meta-analysis to investigate the effect of LLRT-BFR on acute effects of cardiovascular outcomes in healthy individuals. There are no greater effects of BFR for most cardiovascular outcomes with the exception of reduced cardiac output and HR favorable to LLRT-BFR compared with HLRT. Thus, the review’s findings indicate that LLRT-BFR appears to represent a viable alternative intervention for this kind of population.
Conclusion
The findings of the present review suggest that there are no greater acute effects of BFR to resistance exercise for most cardiovascular outcomes, with the exception of reduced cardiac output and HR favorable to LLRT-BFR compared with HLRT.
•
Low-load resistance training associated with blood flow restriction (LLRT-BFR) is an alternative training modality for strength gain and muscle hypertrophy.
•
The cardiovascular safety must be considered, and the impact of LLRT-BFR and its training variables on cardiovascular outcomes is not yet known.
•
The aim of this systematic review with meta-analysis was to compare the acute effects of LLRT-BFR with low-load resistance training and high-load resistance training (HLRT) on cardiovascular outcomes in healthy individuals.
•
This systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, and the protocol was registered in PROSPERO (no. CRD42019142900).
•
The studies were selected from seven databases from the oldest record in each database until 13 January 2022, and for quantitative analysis, 17 studies were included, as two studies did not send the data for the meta-analysis.
•
The methodological quality of the included studies was 5.05 ± 0.4 points, and the quality of the evidence was low or very low evidence.
•
The results demonstrated that there was no difference on the addition of BFR to resistance training for most of the cardiovascular parameters, with the exception of the cardiac output and heart rate, which presented lower values for LLRT-BFR compared with HLRT.
•
The review’s findings indicate that LLRT-BFR appears to represent a viable alternative intervention for this type of healthy individuals.
Financial & competing interests disclosure
This study was carried out with the support of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) – Financing Code 001 and Fundação de Amparo à Pesquisa do Estado de São Paulo (number 2020/13143-8). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
References
Papers of special note have been highlighted as: • of interest
1.
Krzysztofik M, Wilk M, Wojdała G, Gołaś A. Maximizing muscle hypertrophy: a systematic review of advanced resistance training techniques and methods. Int. J. Environ. Res. Public Health 16(24), 4897 (2019).
2.
Fortunato AK, Pontes WM, Souza DMS et al. Strength training session induces important changes on physiological, immunological, and inflammatory biomarkers. J. Immunol. Res. 2018, 9675216 (2018).
3.
American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 41(3), 687–708 (2009).
4.
Neto GR, Novaes JS, Dias I et al. Effects of resistance training with blood flow restriction on haemodynamics: a systematic review. Clin. Physiol. Funct. Imaging 37(6), 567–574 (2017).
• Haemodynamic changes promoted by low-load resistance training with blood flow restriction do not seem to differ between ages and body segments.
5.
Loenneke JP, Wilson JM, Marín PJ, Zourdos MC, Bemben MG. Low intensity blood flow restriction training: a meta-analysis. Eur. J. Appl. Physiol. 112(5), 1849–1859 (2012).
6.
Laurentino G, Ugrinowitsch C, Aihara AY et al. Effects of strength training and vascular occlusion. Int. J. Sports Med. 29(8), 664–667 (2008).
7.
Curty VM, Melo AB, Caldas LC et al. Blood flow restriction attenuates eccentric exercise-induced muscle damage without perceptual and cardiovascular overload. Clin. Physiol. Funct. Imaging 38(3), 468–476 (2018).
8.
Scott BR, Loenneke JP, Slattery KM, Dascombe BJ. Exercise with blood flow restriction: an updated evidence-based approach for enhanced muscular development. Sports Med. 45(3), 313–325 (2015).
9.
Spranger MD, Krishnan AC, Levy PD, O’Leary DS, Smith SA. Blood flow restriction training and the exercise pressor reflex: a call for concern. Am. J. Physiol. Heart. Circ. Physiol. 309(9), H1440–H1452 (2015).
• This review provides a brief yet detailed overview of the mechanisms underlying the autonomic cardiovascular response to exercise with blood flow restriction.
10.
Fu Q, Levine BD. Exercise and the autonomic nervous system. Handb. Clin. Neurol. 117, 147–160 (2013).
11.
Domingos E, Polito MD. Blood pressure response between resistance exercise with and without blood flow restriction: a systematic review and meta-analysis. Life Sci. 209, 122–131 (2018).
• Although resistance exercise with blood flow restriction resulted in greater post-exercise hypotension than traditional exercise, higher systolic blood pressure and/or diastolic blood pressure values were observed during exercise with blood flow restriction compared to traditional exercise, especially in hypertensive individuals.
12.
Elkins MR. Updating systematic reviews. J. Physiother. 64(1), 1–3 (2018).
13.
Hoffmann TC, Glasziou PP, Boutron I et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 348, g1687 (2014).
14.
Sherrington C, Herbert RD, Maher CG, Moseley AM. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man. Ther. 5(4), 223–226 (2000).
15.
Macedo LG, Elkins MR, Maher CG et al. There was evidence of convergent and construct validity of Physiotherapy Evidence Database quality scale for physiotherapy trials. J. Clin. Epidemiol. 63(8), 920–925 (2010).
16.
Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust. J. Physiother. 55(2), 129–133 (2009).
17.
Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (2011). http://handbook.cochrane.org/
18.
Guyatt GH, Oxman AD, Kunz R et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J. Clin. Epidemiol. 64(12), 1283–1293 (2011).
19.
Bazgir B, Rezazadeh Valojerdi M et al. Acute cardiovascular and hemodynamic responses to low intensity eccentric resistance exercise with blood flow restriction. Asian J. Sports Med. 7(4), e38458 (2016).
• The eccentric exercise with blood flow restriction positively regulated the hemodynamic and cardiovascular responses.
20.
Brandner C, Kidgell D, Warmington S. Unilateral bicep curl hemodynamics: low-pressure continuous vs high-pressure intermittent blood flow restriction. Scand. J. Med. Sci. Sports 25(6), 770–777 (2015).
21.
Vilaça-Alves J, Neto G, Morgado N et al. Acute effect of resistance exercises performed by the upper and lower limbs with blood flow restriction on hemodynamic responses. J. Exerc. Physiol. Online 19(3), 100–109 (2016).
22.
Figueroa A, Vicil F. Post-exercise aortic hemodynamic responses to low-intensity resistance exercise with and without vascular occlusion. Scand. J. Med. Sci. Sports 21(3), 431–436 (2011).
23.
Rodrigues Neto G, Novaes JS, Gonçalves M et al. Hypotensive effects of resistance exercise with continuous and intermittent blood flow restriction. Mot. Rev. Educ. Física. 22(3), 198–204 (2016).
24.
Rodrigues Neto G, Novaes JS, Salerno VP et al. Acute effects of resistance exercise with continuous and intermittent blood flow restriction on hemodynamic measurements and perceived exertion. Percept. Mot. Skills 124(1), 277–292 (2017).
25.
Rodrigues Neto G, Silva H, Vieira L et al. Efeito agudo e crônico do treinamento de força com restrição de fluxo sanguíneo contínua ou intermitente sobre as medidas hemodinâmicas e percepção subjetiva de esforço em homens saudáveis. Motricidade 14(2), 71–82 (2018).
26.
Mattocks K, Mouser J, Jessee M et al. Acute hemodynamic changes following high load and very low load lower body resistance exercise with and without the restriction of blood flow. Physiol. Meas. 39(12), 125007 (2018).
27.
Libardi C, Catai A, Miquelini M et al. Hemodynamic responses to blood flow restriction and resistance exercise to muscular failure. Int. J. Sports Med. 38(2), 134–140 (2017).
28.
Maior AS, Simão R, Martins MSR, de Salles BF, Willardson JM. Influence of blood flow restriction during low-intensity resistance exercise on the postexercise hypotensive response. J. Strength Cond. Res. 29(10), 2894–2899 (2015).
29.
Mota M, Fonseca J, Barbosa S et al. Physiological and hemodynamic effects of blood flow restriction training on quadriceps. J. Exerc. Physiol. Online 21(3), 79–85 (2018).
30.
Moriggi R, Mauro HD, Dias SC et al. Similar hypotensive responses to resistance exercise with and without blood flow restriction. Biol. Sport. 32(4), 289–294 (2015).
31.
Mouser JG, Mattocks KT, Dankel SJ et al. Very-low-load resistance exercise in the upper body with and without blood flow restriction: cardiovascular outcomes. Appl. Physiol. Nutr. Metab. 44(3), 288–292 (2019).
32.
Rodrigues Neto G, Sousa M, Costa e Silva G et al. Acute resistance exercise with blood flow restriction effects on heart rate, double product, oxygen saturation and perceived exertion. Clin. Physiol. Funct. Imaging. 36(1), 53–59 (2016).
33.
Rodrigues Neto G, Sousa M, Costa P et al. Hypotensive effects of resistance exercises with blood flow restriction. J. Strength Cond. Res. 29(4), 1064–1070 (2015).
34.
Poton R, Polito MD. Hemodynamic response to resistance exercise with and without blood flow restriction in healthy subjects. Clin. Physiol. Funct. Imaging 36(3), 231–236 (2016).
35.
Rossow L, Fahs C, Sherk V et al. The effect of acute blood-flow-restricted resistance exercise on postexercise blood pressure. Clin. Physiol. Funct. Imaging 31(6), 429–434 (2011).
36.
Vieira PJC, Chiappa GR, Umpierre D, Stein R, Ribeiro JP. Hemodynamic responses to resistance exercise with restricted blood flow in young and older men. J. Strength Cond. Res. 27(8), 2288–2294 (2013).
37.
Bonorino SL, De Sá CA, Corralo VS et al. Hemodynamic responses to strength exercise with blood flow restriction in small muscle groups. Rev. Bras. Cineantropom. Desempenho Hum. 21, e56258 (2019).
38.
Powers SK, Howley ET. Fisiologia do exercício: teoria e aplicação ao condicionamento e ao desempenho Manole, Sao Paulo, Brazil, 576 (2014).
39.
Viaro F, Nobre F, Evora PR. Expression of nitric oxide synthases in the pathophysiology of cardiovascular diseases. Arq. Bras. Cardiol. 74(4), 380–393 (2000).
Information & Authors
Information
Published In
Pages: 829 - 842
PubMed: 35712965
Copyright
© 2022 Future Medicine Ltd.
History
Received: 1 November 2021
Accepted: 24 May 2022
Published online: 17 June 2022
Keywords:
Topics
Authors
Funding Information
Fundação de Amparo à Pesquisa do Estado de São Paulo: 2020/13143-8
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Acute effects of resistance exercise with blood flow restriction on cardiovascular response: a meta-analysis. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0272
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- James R. Mckee, Isaac Selva Raj, Kieran J. Marston, Kristen De Marco, Michael Beere, Brook Galna, Jeremiah J. Peiffer, Kazunori Nosaka, Brendan R. Scott, Acute and Chronic Effects of High-Load Resistance Training With Blood Flow Restriction in Healthy Adults: A Systematic Review and Meta-Analysis, Journal of Strength & Conditioning Research, 10.1519/JSC.0000000000005467, 40, 7, (822-842), (2026).
- Jonathan W. Hoch, Christin Domeier, Pannonica Silvestri, Joseph C. Watso, Prognostic value of exercise blood pressure: role of fitness and exercise training, American Journal of Physiology-Heart and Circulatory Physiology, 10.1152/ajpheart.00852.2025, 330, 4, (H1025-H1047), (2026).
- Yashveer Singh, Leslie A Avila, Marty Spranger, Cardiovascular responses during blood flow-restricted resistance exercise: a systematic review with meta-analysis, BMJ Open Sport & Exercise Medicine, 10.1136/bmjsem-2025-002989, 12, 1, (e002989), (2026).
- James Brown, Jakob D. Lauver, Timothy R. Rotarius, Justin P. Guilkey, Acute responses to low-intensity aerobic exercise with continuous and intermittent blood flow restriction, Frontiers in Sports and Active Living, 10.3389/fspor.2025.1737095, 7, (2026).
- Daniel C. Ogrezeanu, Andrea Tur-Boned, Nicholas Rolnick, Juan J. Carrasco, Carlos Cruz-Montecinos, Joaquín Calatayud, Santiago Bonanad, Sofía Pérez-Alenda, Acute safety, cardiovascular, perceptual and neuromuscular responses to autoregulated and non-autoregulated blood flow restriction training during elbow rehabilitation in people with hemophilia, Frontiers in Sports and Active Living, 10.3389/fspor.2025.1587615, 7, (2025).
- Stefanos Karanasios, Thomas Sampsonis, Ioannis Lignos, George Gioftsos, The immediate effects of wrist extensor training with blood flow restriction on pain perception in middle-aged patients with lateral elbow tendinopathy: A cross-over randomized controlled trial, Sports Medicine and Health Science, 10.1016/j.smhs.2025.03.003, (2025).
- Silas de Oliveira Damasceno, Eduardo Pizzo Junior, Allysiê Priscilla de Souza Cavina, Driely Stephany Pedroso dos Santos, Maria Eduarda Lopes da Cruz, Gabriella Souza Oliveira Meireles Pimenta, Franciele Marques Vanderlei, Responses in Posttherapy Recovery-Based Virtual Reality With Blood Flow Restriction in Older Women: A Randomized Crossover Clinical Trial, Journal of Aging and Physical Activity, 10.1123/japa.2025-0027, (1-14), (2025).
- James O. Suggitt, Brock E. Eaves, Marty D. Spranger, What are the cardiovascular responses during blood flow-restricted resistance exercise?, Frontiers in Physiology, 10.3389/fphys.2024.1417855, 15, (2024).
- Ashley A. Herda, Christopher J. Cleary, Dana Young, KathleenMae B. Rogers, Santiago E. Umana Segura, Christopher Bernard, Lisa M. Vopat, Bryan G. Vopat, Blood Flow Restriction during Walking Does Not Impact Body Composition or Performance Measures in Highly Trained Runners, Journal of Functional Morphology and Kinesiology, 10.3390/jfmk9020074, 9, 2, (74), (2024).
- Joseph Mannozzi, Mohamed-Hussein Al-Hassan, Jasdeep Kaur, Beruk Lessanework, Alberto Alvarez, Louis Massoud, Kamel Aoun, Marty Spranger, Donal S. O’Leary, Blood flow restriction training activates the muscle metaboreflex during low-intensity sustained exercise, Journal of Applied Physiology, 10.1152/japplphysiol.00274.2023, 135, 2, (260-270), (2023).