Impact of perioperative chemotherapy on survival outcomes among patients with metastatic colorectal cancer to the liver
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Compare overall survival (OS) between adjuvant and neoadjuvant chemotherapy and analyze the effect of chemotherapy on OS. Materials & methods: National Cancer Database was queried for patients diagnosed with metastatic colorectal adenocarcinoma with isolated liver metastases between 2004 and 2016. We evaluated the OS and chemotherapy effect using Kaplan-Meier estimates and multivariable cox regression analyses. Results: Total 6883 patients with metastatic colorectal cancer and liver metastases were included, of which 6042 patients were treated with surgery and chemotherapy and 841 patients were treated with surgery only. Patients who received neoadjuvant chemotherapy had better OS compared with patients who received adjuvant chemotherapy. Conclusion: Patients with colorectal cancer with isolated liver metastases who were treated with neoadjuvant chemotherapy had better OS compared with adjuvant chemotherapy.
Colorectal cancer (CRC) is the third most commonly diagnosed malignancy in the USA and the world and the second leading cause of cancer death in both sexes in 2020 in the USA [1–3]. Due to the majority of the intestinal mesenteric drainage entering the hepatic portal venous system, hepatic metastases develop in approximately half of all colorectal cancer cases with nearly a fifth to a quarter of newly diagnosed metastatic CRC patients present with liver metastases at the time of primary diagnosis [2,4]. Surgical resection alone is the cornerstone of treatment for patients with liver metastases from CRC in whom there is at least a one in six chance of a cure after hepatectomy and apparent clinical cure is achieved in those who survive 10 years [5–7]. In the past 15–20 years, profound improvements in outcomes of metastatic CRC of 5-year survival have more than doubled [4,8,9]. Although new treatment options have doubled overall survival (OS) for advanced disease, survival is still best for those with non-metastatic disease [10]. While the role of surgical resection is established in metastatic disease to the liver, the potential benefit from peri-operative chemotherapy remains unclear [6,11]. While some studies have shown that perioperative chemotherapy with surgery reduced the risk of progression-free survival (PFS) events at 3 years in patients with resectable liver metastases [12], others concluded that preoperative chemotherapy did not prolong survival with colorectal cancer and resectable or marginally resectable liver metastasis [13]. Also, there's a lack of data in assessing the impact of timing of perioperative chemotherapy on survival (pre- vs post-operative), as well as in comparing the effect of single-agent versus multiagent chemotherapy on survival. We studied the survival outcomes of patients with CRC with liver metastases who underwent surgical management alone versus combined surgery and chemotherapy based on a real-world cohort. In addition to that, we assessed the effect of timing of chemotherapy on survival among patients who received chemotherapy and compared the OS between patients who received single-agent and patients who received multiagent chemotherapy as the first line of chemotherapy.
Patients & methods
Data source
The National Cancer Database (NCDB) is a nationwide database supported by the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society. About 70% of all cancer cases diagnosed in the USA from more than 1500 cancer centers are included in this database. Details of patients' demographics, malignancy staging and histological characteristics in addition to treatment and outcome information are provided in this database [14]. The CoC's NCDB and the hospitals participating in the CoC's NCDB are the sources of the de-identified data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors of the current study.
After we obtained the approval on our proposed protocol and the letter of support from the cancer committee chair at Cleveland Clinic, the NCDB was queried for patients diagnosed with metastatic colorectal adenocarcinoma between 2004 and 2016. Survival follow-up for the studied cohort is available till December 2016. It's worth mentioning that the metastatic status provided in the database is related to the status at the time of the diagnosis. NCDB doesn't provide the details about the possible non-metastatic cases that subsequently developed metastatic disease.
Patient selection
For our study, we selected the patients who were diagnosed with metastatic colorectal adenocarcinoma with liver metastases at age of 18 or older. We excluded patients with metastases to other sites other than the liver. Patients who didn't have radical surgical resection to the primary tumor and/or did not have surgery to distant metastatic sites were also excluded in addition to patients with unknown chemotherapy status. Also, we excluded patients who lost follow-up which are defined by patients with missing details about their last contact status as alive or dead, and those with missing information about their time from diagnosis to the last contact.
Variables
Using the NCDB, we included the following patient demographic variables: age, gender, race, median income, education level, insurance status, facility type (which includes community cancer program, comprehensive community cancer program, academic/research program and integrated network cancer program) in addition to the geographic area which was classified as metropolitan, urban or rural location. Also, we collected the following disease-related variables: clinical tumor and nodal categories based on American Joint Committee on Cancer staging, microsatellite instability (MSI) status, Charlson-Deyo comorbidity score and chemotherapy status.
Outcome
The primary outcome of this study was OS in months defined as the time from diagnosis to the time of death for any reason.
Statistical analysis
We compared the baseline demographics and characteristics between patients who were treated with surgery and chemotherapy versus patients who were treated with surgery only using the Pearson Chi-square test and t-test.
For OS comparisons, we split the cohort into two separate groups according to the type of treatment the patients received, the first group who was treated with surgery and chemotherapy and the second group who was treated with surgery only. Then, we compared the OS between the two groups. Moreover, we conducted additional OS comparisons (limited to patients who received perioperative chemotherapy) between patients who received adjuvant chemotherapy versus neoadjuvant chemotherapy; and between patients who received single-agent versus multiagent chemotherapy.
OS analyses were evaluated using the Kaplan-Meier survival method. A log-rank test was used to evaluate survival differences between groups. We used Cox regression analysis to conduct multivariable analyses to evaluate the factors associated with improved OS; hazard ratios (HRs) with associated 95% confidence intervals (CI) were accordingly generated, statistical significance was defined as a p-value less than 0.05 for all analyses. The following factors were included in the multivariable model: facility type, age, gender, race, median household income, education level, insurance status, area, Charlson score, clinical T stage, clinical N stage, MSI status and chemotherapy use.
All the above statistical analyses were performed using the SPSS Statistics 27.0
To further reduce any potential biases related to the variation in baseline characteristics between the patient group that received chemotherapy and the one that did not receive chemotherapy, we used nearest neighbor, 1:1, propensity score matching using RStudio Version 1.3.1093 (MA, USA).
As a sensitivity analysis, we repeated all the above analyses after excluding patients who died within 90 days of the most definitive primary site surgery (to eliminate the effect of post-surgical complication-related mortality on overall survival).
To further examine the impact of MSI status on the above survival analyses, we repeated the above survival analyses among patients with MSI-H versus those with MSI-L status. In our study, MSI-L includes MSI-stable cases.
Results
Baseline characteristics
Figure 1 provides a flowchart for patient selection within the current study. We ended up with 6883 patients with metastatic CRC and liver metastases; 6042 (87.8%) were treated with surgery and chemotherapy and 841 (12.2%) were treated with surgery only. Compared with the surgery-only group, the perioperative-chemo group was likely to be younger (58 vs 70 years old), males (55.5% vs 47.4%), and had more MSI-L status (27.8 vs 16.6%). The baseline characteristics' comparison between the two groups is summarized in Table 1.

Figure 1. Patient selection flowchart.
CRC: Colorectal cancer; NCDB: National Cancer Database.
| Characteristics | All cases (n = 6883) | Surgery only (n = 841) (12.2%) | Surgery and chemotherapy (n = 6042) (87.8%) | p-value and test |
|---|---|---|---|---|
| Mean age in years | 59.54 ± 13.05 | 70.28 ± 12.92 | 58.04 ± 12.35 | <0.001 t-test |
| Sex | <0.001; Chi-square | |||
| Female | 3130 (45.5%) | 442 (52.6%) | 2688 (44.5%) | |
| Male | 3753 (54.5%) | 399 (47.4%) | 3354 (55.5%) | |
| Race | 0.062; Chi-square | |||
| White | 5682 (82.6%) | 672 (79.9%) | 5010 (82.9%) | |
| African American | 826 (12.0%) | 124 (14.7%) | 702 (11.6%) | |
| Others | 329 (4.8%) | 38 (4.5%) | 291 (4.8%) | |
| Unknown | 46 (0.7%) | 7 (0.8%) | 39 (0.6%) | |
| Facility type | <0.001; Chi-square | |||
| Community cancer program | 443 (6.4%) | 87 (10.3%) | 356 (5.9%) | |
| Comprehensive Community Cancer Program | 2015 (29.3%) | 361 (42.9%) | 1654 (27.4%) | |
| Academic/Research Program | 3158 (45.9%) | 244 (29.0%) | 2914 (48.2%) | |
| Integrated Network Cancer Program | 835 (12.1%) | 134 (15.9%) | 701 (11.6%) | |
| Unknown | 432 (6.3%) | 15 (1.8%) | 417 (6.9%) | |
| Median household income 2012–2016 | <0.001; Chi-square | |||
| Less than US$40,227 | 1188 (17.3%) | 186 (22.1%) | 1002 (16.6%) | |
| US$40,227–$50,353 | 1501 (21.8%) | 199 (23.7%) | 1302 (21.5%) | |
| US$50,354- $63,332 | 1567 (22.8%) | 193 (22.9%) | 1374 (22.7%) | |
| US$63,333+ | 2539 (36.9%) | 254 (30.2%) | 2285 (37.8%) | |
| Unknown | 88 (1.3%) | 9 (1.1%) | 79 (1.3%) | |
| Education level 2012–2016 (percentage of not graduated from high school) | <0.001; Chi-square | |||
| 17.6% or more | 1237 (18.0%) | 217 (25.8%) | 1020 (16.9%) | |
| 10.9–17.5% | 1803 (26.2%) | 246 (29.3%) | 1557 (25.8%) | |
| 6.3%-10.8% | 2017 (29.3%) | 202 (24.0%) | 1815 (30.0%) | |
| Less than 6.3% | 1753 (25.5%) | 171 (20.3%) | 1582 (26.2%) | |
| Unknown | 73 (1.1%) | 5 (0.6%) | 68 (1.1%) | |
| Insurance status | 0.384; Chi-square | |||
| No | 225 (3.3%) | 34 (4.0%) | 191 (3.2%) | |
| Yes | 6567 (95.4%) | 795 (94.5%) | 5772 (95.5%) | |
| Unknown | 91 (1.3%) | 12 (1.4%) | 79 (1.3%) | |
| Area | 0.237; Chi-square | |||
| Metro counties | 5545(80.6%) | 697 (82.9%) | 4848 (80.2%) | |
| Rural counties | 137 (2.0%) | 17 (2.0%) | 120 (2.0%) | |
| Urban counties | 1031 (15.0%) | 112 (13.3%) | 919 (15.2%) | |
| Unknown | 170 (2.5%) | 15 (1.8%) | 155 (2.6%) | |
| Clinical T stage | <0.001; Chi-square | |||
| T0 | 18 (0.3%) | 1 (0.1%) | 17 (0.3%) | |
| T1 | 316 (4.6%) | 36 (4.3%) | 280 (4.6%) | |
| T2 | 208 (3.0%) | 17 (2.0%) | 191 (3.2%) | |
| T3 | 1617 (23.5%) | 135 (16.1%) | 1482 (24.5%) | |
| T4 | 621 (9.0%) | 115 (13.7%) | 506 (8.4%) | |
| Tis | 15 (0.2%) | 0 (0.0%) | 15 (0.2%) | |
| Unknown | 4,088 (59.4%) | 537 (63.9%) | 3551 (58.8%) | |
| Clinical N stage | <0.001; Chi-square | |||
| N0 | 2732 (39.7%) | 329 (39.1%) | 2403 (39.8%) | |
| N1 | 1694 (24.6%) | 166 (19.7%) | 1528 (25.3%) | |
| N2 | 684 (9.9%) | 98 (11.7%) | 586 (9.7%) | |
| Unknown | 1773 (25.8%) | 248 (29.5%) | 1525 (25.2%) | |
| MSI status | <0.001; Chi-square | |||
| MSI-H | 208 (3.0%) | 30 (3.6%) | 178 (2.9%) | |
| MSI-L | 1818 (26.4%) | 140 (16.6%) | 1678 (27.8%) | |
| Unknown | 4857 (70.6%) | 671 (79.8%) | 4186 (69.3%) | |
| Charlson-Deyo score | <0.001; Chi-square | |||
| 0 | 5325 (77.4%) | 523 (62.2%) | 4802 (79.5%) | |
| 1 | 1207 (17.5%) | 220 (26.2%) | 987 (16.3%) | |
| 2 | 258 (3.7%) | 71 (8.4%) | 187 (3.1%) | |
| 3 | 93 (1.4%) | 27 (3.2%) | 66 (1.1%) |
MSI: Microsatellite instability.
Next, in our sensitivity analysis, we excluded all patients who died within 90 days of most definitive primary site surgery (n = 550), which left us with 6333 patients; 5834 (92.1%) who were treated with surgery and chemotherapy, and 499 (7.9%) who were treated with surgery only. While the percentage of patients who died within the first 90 days of the primary tumor surgery is significant, we are unable to determine the cause of death if it was cancer-related, surgery-related, or due to other reason.
The baseline characteristics' comparison between the two groups is summarized in Table 2.
| Characteristics | All cases (n = 6333) | Surgery only (n = 499) (7.9%) | Surgery and chemotherapy (n = 5834) (92.1%) | p-value and test |
|---|---|---|---|---|
| Mean age in years | 58.90 ± 12.83 | 69.47 ± 13.34 | 57.99 ± 12.38 | <0.001 t-test |
| Sex | <0.001; Chi-square | |||
| Female | 2882 (45.5%) | 274 (54.9%) | 2608 (44.7%) | |
| Male | 3451 (54.5%) | 225 (45.1%) | 3226 (55.3%) | |
| Race | 0.256; Chi-square | |||
| White | 5242 (82.8%) | 401 (80.4%) | 4841 (83.0%) | |
| African American | 743 (11.7%) | 68 (13.6%) | 675 (11.6%) | |
| Others | 304 (4.8%) | 24 (4.8%) | 280 (4.8%) | |
| Unknown | 44 (0.7%) | 6 (1.2%) | 38 (0.7%) | |
| Facility type | <0.001; Chi-square | |||
| Community cancer program | 387 (6.1%) | 42 (8.4%) | 345 (5.9%) | |
| Comprehensive Community Cancer Program | 1798 (28.4%) | 200 (40.1%) | 1598 (27.4%) | |
| Academic/Research Program | 2987 (47.2%) | 171 (34.3%) | 2816 (48.3%) | |
| Integrated Network Cancer Program | 742 (11.7%) | 73 (14.6%) | 669 (11.5%) | |
| Unknown | 419 (6.6%) | 13 (2.6%) | 406 (7.0%) | |
| Median household income 2012–2016 | 0.002; Chi-square | |||
| Less than US$40,227 | 1073 (16.9%) | 105 (21.0%) | 968 (16.6%) | |
| US$40,227–$50,353 | 1377 (21.7%) | 122 (24.4%) | 1255 (21.5%) | |
| US$50,354–$63,332 | 1439 (22.7%) | 119 (23.8%) | 1320 (22.6%) | |
| US$63,333+ | 2362 (37.3%) | 147 (29.5%) | 2215 (38.0%) | |
| Unknown | 82 (1.3%) | 6 (1.2%) | 76 (1.3%) | |
| Education level 2012–2016 (percentage of not graduated from high school) | <0.001; Chi-square | |||
| 17.6% or more | 1116 (17.6%) | 128 (25.7%) | 988 (16.9%) | |
| 10.9–17.5% | 1646 (26.0%) | 145 (29.1%) | 1501 (25.7%) | |
| 6.3–10.8% | 1866 (29.5%) | 117 (23.4%) | 1749 (30.0%) | |
| Less than 6.3% | 1637 (25.8%) | 106 (21.2%) | 1531 (26.2%) | |
| Unknown | 68 (1.1%) | 3 (0.6%) | 65 (1.1%) | |
| Insurance status | 0.581; Chi-square | |||
| No | 200 (3.2%) | 19 (3.8%) | 181 (3.1%) | |
| Yes | 6049 (95.5%) | 472 (94.6%) | 5577 (95.6%) | |
| Unknown | 84 (1.3%) | 8 (1.6%) | 76 (1.3%) | |
| Area | 0.470; Chi-square | |||
| Metro counties | 5095 (80.5%) | 411 (82.4%) | 4684 (80.3%) | |
| Rural counties | 129 (2.0%) | 12 (2.4%) | 117 (2.0%) | |
| Urban counties | 952 (15.0%) | 67 (13.4%) | 885 (15.2%) | |
| Unknown | 157 (2.5%) | 9 (1.8%) | 148 (2.5%) | |
| Clinical T stage | 0.002; Chi-square | |||
| T0 | 14 (0.2%) | 0 (0.0%) | 14 (0.2%) | |
| T1 | 298 (4.7%) | 25 (5.0%) | 273 (4.7%) | |
| T2 | 199 (3.1%) | 14 (2.8%) | 185 (3.2%) | |
| T3 | 1516 (23.9%) | 86 (17.2%) | 1430 (24.5%) | |
| T4 | 540 (8.5%) | 59 (11.8%) | 481 (8.2%) | |
| Tis | 13 (0.2%) | 0 (0.0%) | 13 (0.2%) | |
| Unknown | 3753 (59.3%) | 315 (63.1%) | 3438 (58.9%) | |
| Clinical N stage | 0.008; Chi-square | |||
| N0 | 2535 (40.0%) | 219 (43.9%) | 2316 (39.7%) | |
| N1 | 1577 (24.9%) | 100 (20.0%) | 1477 (25.3%) | |
| N2 | 607 (9.6%) | 37 (7.4%) | 570 (9.8%) | |
| Unknown | 1614 (25.5%) | 143 (28.7%) | 1471 (25.2%) | |
| MSI status | <0.001; Chi-square | |||
| MSI-H | 192 (3.0%) | 20 (4.0%) | 172 (2.9%) | |
| MSI-L | 1718 (27.1%) | 92 (18.4%) | 1626 (27.9%) | |
| Unknown | 4423 (69.8%) | 387 (77.6%) | 4036 (69.2%) | |
| Charlson-Deyo score | <0.001; Chi-square | |||
| 0 | 5325 (77.4%) | 523 (62.2%) | 4802 (79.5%) | |
| 1 | 1207 (17.5%) | 220 (26.2%) | 987 (16.3%) | |
| 2 | 258 (3.7%) | 71 (8.4%) | 187 (3.1%) | |
| 3 | 93 (1.4%) | 27 (3.2%) | 66 (1.1%) |
MSI: Microsatellite instability.
Survival outcome
The entire cohort
We compared the OS between patients who were treated with surgery and chemotherapy versus patients who were treated with surgery only and found that patients who were treated with surgery and chemotherapy had better OS compared with patients who were treated with surgery only (median OS 42.9 vs 6.4 months; p < 0.001) as illustrated in the Kaplan-Meier survival curves (Figure 2). We noted the significant difference in the OS and the very short median OS for patients treated with surgery only. This could be due to multiple factors including the heterogeneity of the patients in this pool.

Propensity score matching yielded 1682 patients for analysis: 841 patients in the no chemotherapy group and 841 patients in the chemotherapy group. Comparison of baseline characteristics between the groups after propensity score matching is shown in Supplementary Table A.
We compared the OS between patients who received chemotherapy versus patients who didn't receive chemotherapy using Kaplan-Meier analysis on the propensity score-matched groups and found that patients who received chemotherapy had better OS than those who didn't receive chemotherapy as illustrated in the Kaplan-Meier survival curves (p < 0.001) (Supplementary Figure A).
Excluding patients who died within 90 days of most definitive primary site surgery
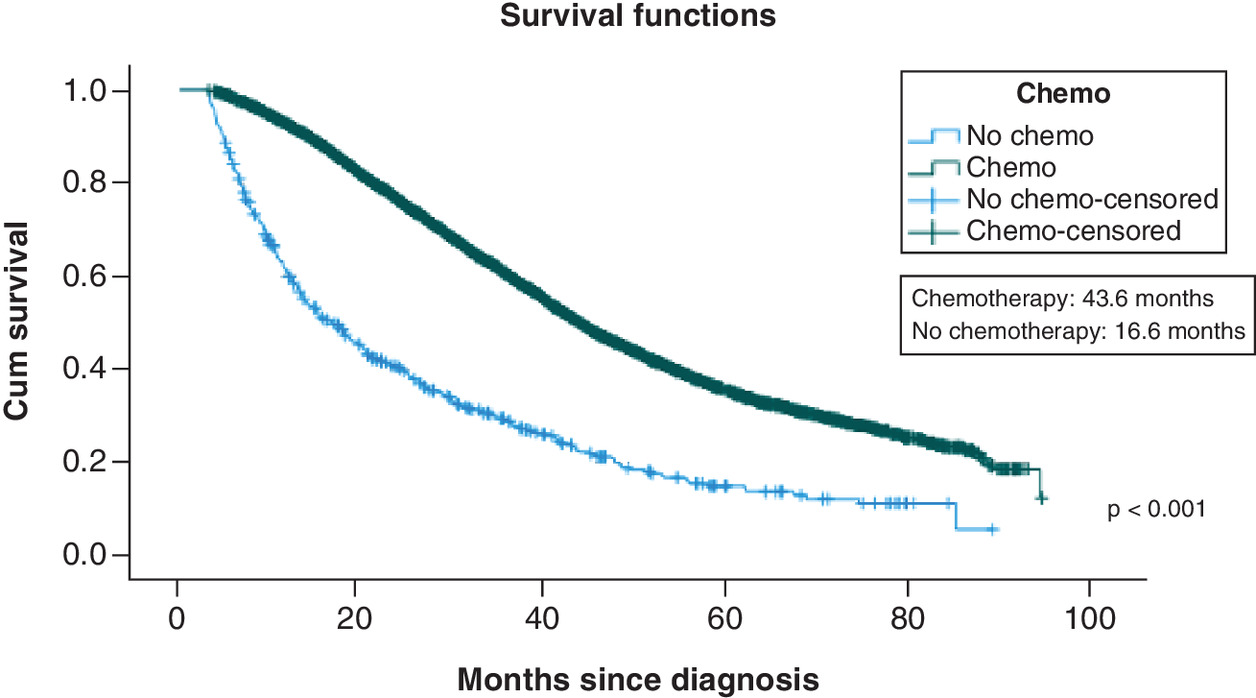
After excluding patients who died within 90 days of the most definitive primary site surgery, we compared the OS between patients who were treated with surgery and chemotherapy versus patients who were treated with surgery only. We found that patients who were treated with surgery and chemotherapy had better OS compared with patients who were treated with surgery only (median OS was 43.6 months vs 16.6 months; p < 0.001) as illustrated in the Kaplan-Meier survival curves (Figure 3).
Propensity score matching yielded 998 patients for analysis: 499 patients in the no chemotherapy group and 499 patients in the chemotherapy group. Baseline characteristics comparison between the groups after propensity score matching is shown in Supplementary Table B.
We compared the OS between patients who received chemotherapy versus patients who didn't receive chemotherapy using Kaplan-Meier analysis on the propensity score-matched groups and found that patients who received chemotherapy had better OS than those who didn't receive chemotherapy as illustrated in the Kaplan-Meier survival curves (p < 0.001) (Supplementary Figure B).
Subgroup analysis among patients who received chemotherapy
Single versus multiagent chemotherapy
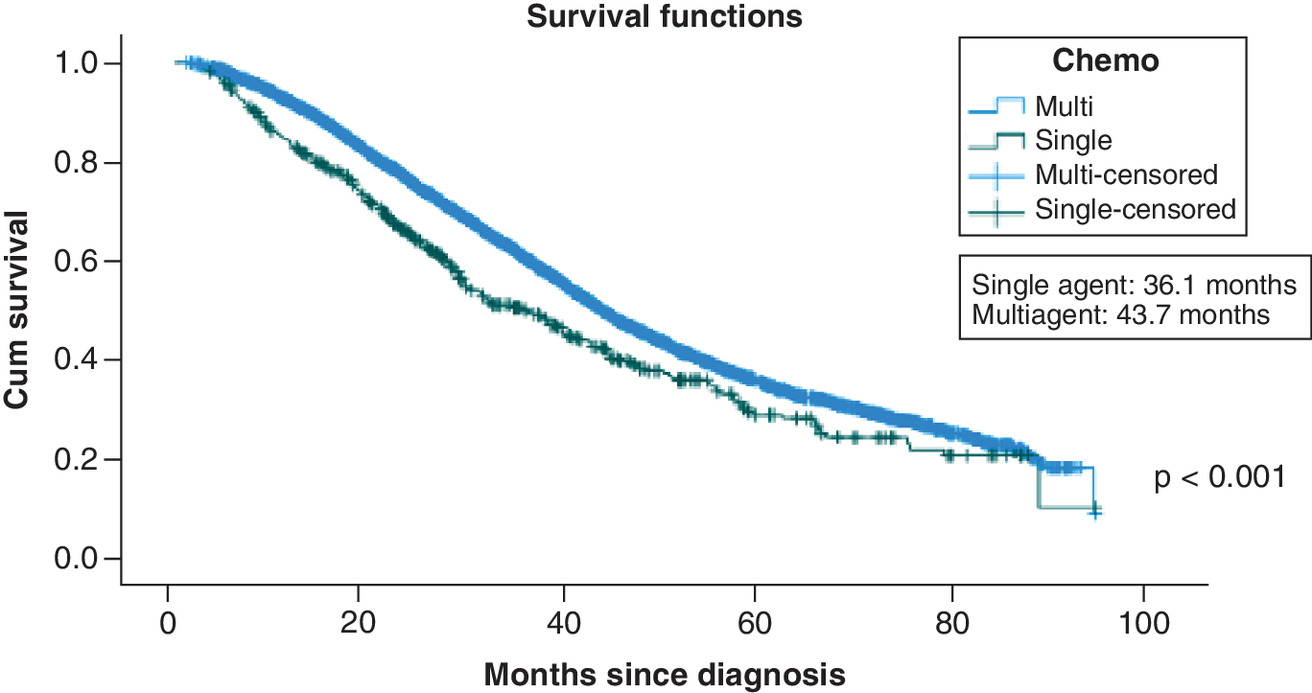
After including only patients who received chemotherapy and excluding patients with the unknown number of chemotherapy agents they received, we compared the OS between patients who received single-agent chemotherapy and patients who received multiagent chemotherapy. We found patients who received multiagent chemotherapy had statistically significant better OS compared with patients who received single-agent chemotherapy (median OS was 43.7 months vs 36.1 months; p < 0.001) as illustrated in the Kaplan-Meier survival curves (Figure 4).
Propensity score matching yielded 958 patients for analysis: 479 patients received single-agent chemotherapy and 479 patients received multiagent chemotherapy. We compared the OS between patients who received single-agent chemotherapy and patients who received multiagent chemotherapy using Kaplan-Meier analysis on the propensity score-matched groups and found that patients who received multiagent chemotherapy had statistically significant better OS compared with patients who received single-agent chemotherapy as illustrated in the Kaplan-Meier survival curves (p < 0.001) (Supplementary Figure C).
In multivariable analysis, we found multiagent chemotherapy was associated with better OS compared with single chemotherapy (HR 0.728; 95% CI 0.549–0.966; p = 0.028).
Adjuvant versus neoadjuvant chemotherapy
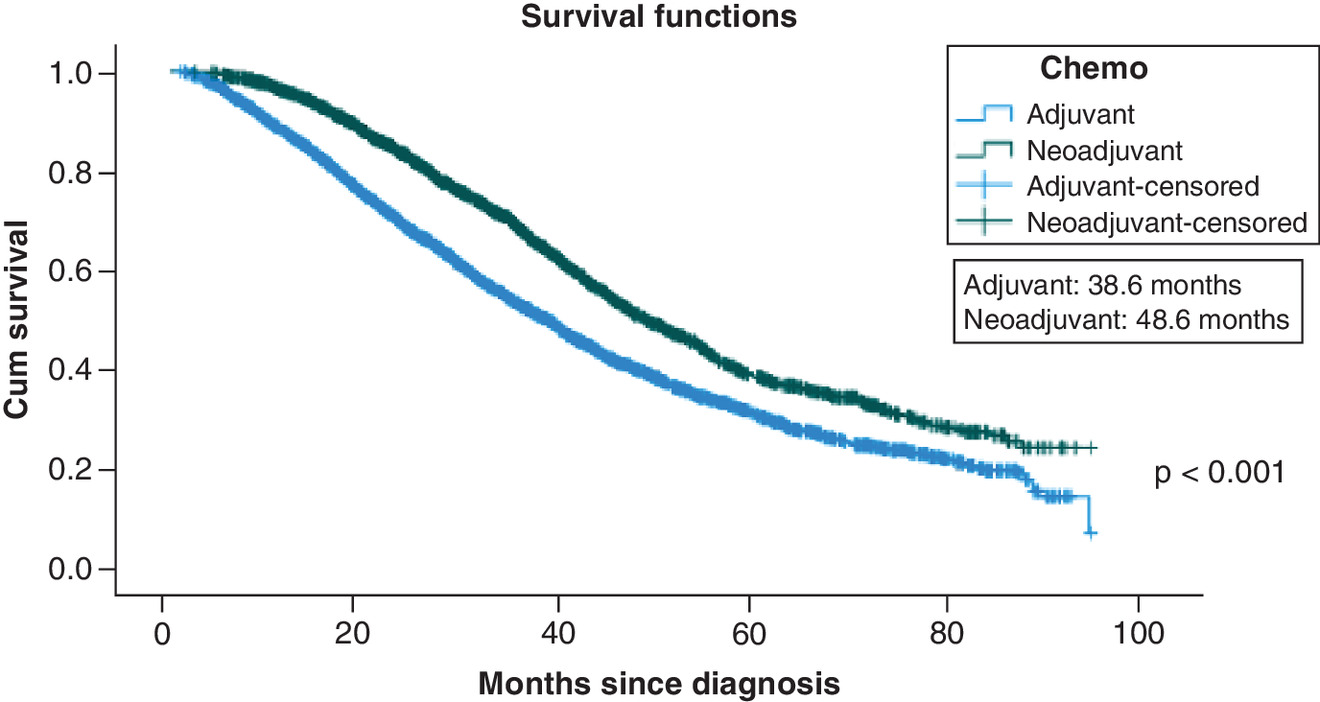
After excluding patients who did not received chemotherapy and with unknown time duration between diagnosis and surgery and time duration between diagnosis and chemotherapy, we compared the OS between patients who received neoadjuvant chemotherapy versus patients who received adjuvant chemotherapy. We found patients were treated with neoadjuvant chemotherapy had statistically significant better OS compared with patients were treated with adjuvant chemotherapy (median OS was 48.6 months vs 38.6 months; p < 0.001) as illustrated in the Kaplan-Meier survival curves (Figure 5).
Propensity score matching yielded 4428 patients for analysis: 2214 patients received chemotherapy before surgery and 2214 patients received chemotherapy after surgery. We compared the OS between patients who received chemotherapy before surgery and patients who received chemotherapy after surgery using Kaplan-Meier analysis on the propensity score-matched groups and we found that patients who received chemotherapy before surgery had statistically significant better OS compared with patients who received chemotherapy after surgery as illustrated in the Kaplan-Meier survival curves (p < 0.001) (Supplementary Figure D).
In multivariable analysis, we found no significant difference in OS between adjuvant versus neoadjuvant chemotherapy (HR 1.123; 95% CI 0.959–1.315; p = 0.150).
Subgroup analysis according to MSI status
Chemotherapy & surgery versus surgery only
After excluding patients with unknown MSI status, we ended up with 2026 metastatic CRC patients with liver metastases and known MSI status. We split the patients into two groups according to the MSI status: MIS-H group and MSI-L group, then we compared the OS between patients who were treated with surgery and chemotherapy versus patients who were treated with surgery only in each MSI group. We found that patients who were treated with surgery and chemotherapy had better OS compared with patients who were treated with surgery only in both MSI-H and MSI-L groups as illustrated in the Kaplan-Meier survival curves (Supplementary Figure E).
Single versus multiagent chemotherapy
After excluding patients with unknown MSI status, we ended up with 1789 metastatic CRC patients with liver metastases and known MSI status who received chemotherapy with a known number of chemotherapy agents they received. We split the patients into two groups according to the MSI status: MIS-H group and MSI-L group, then we compared the OS between patients who received single-agent chemotherapy and patients who received multiagent chemotherapy in each MSI group. In the MSI-L group, we found patients who received multiagent chemotherapy had statistically significant better OS compared with patients who received single-agent chemotherapy. Whereas in the MSI-H group, there was no difference in OS between the two treatment groups. This finding in the MSI-H group, could be related to the idea that our chemotherapy data is limited to the first line treatment only (Supplementary Figure F).
Adjuvant versus neoadjuvant chemotherapy
After excluding patients with unknown MSI status, we ended up with 1755 metastatic CRC patients with liver metastases and known MSI status who received chemotherapy with known time from diagnosis to surgery and time from diagnosis to chemotherapy. We split the patients into two groups according to the MSI status: MSI-H group and MSI-L group, then we compared the OS between patients who received chemotherapy before surgery and patients who received chemotherapy after surgery in each MSI group. In the MSI-L group, we found patients who received chemotherapy before surgery had statistically significant better OS compared with patients who received chemotherapy after surgery. Whereas in the MSI-H group, there was no difference in OS between the two treatment groups (Supplementary Figure G).
Multivariable analysis
Multivariable analysis was done to assess factors affecting OS. In the entire cohort, factors associated with worse OS were older age (HR 1.021; 95% CI 1.018–1.025; p < 0.001), African American race compared with Caucasian race (HR 1.171; 95% CI 1.058–1.296; p = 0.002), not having insurance (HR 1.217; 95% CI 1.027 -1.442; p = 0.024), clinical N1 and N2 stage compared with N0 stage (HR 1.224; 95% CI 1.122–1.335; p < 0.001 and HR 1.907; 95% CI 1.699 -2.141; p < 0.001, respectively), community cancer program (HR for Academic/Research Program and Integrated Network Cancer Program compared with community cancer program was 0.625; 95% CI 0.549–0.712; p < 0.001 and HR 0.842; 95% CI 0.726–0.978; p = 0.024, respectively), higher Charlson-Deyo scores (HR for Charlson-Deyo scores 0 compared with the Charlson-Deyo score of 3 was 0.768; 95% CI 0.602–0.980; p = 0.034), MSI-high (HR for MSI-stable compared with MSI-high was 0.818; 95% CI 0.677–0.988; p = 0.037) and not receiving chemotherapy (HR for receiving chemotherapy compared with not receiving chemotherapy was 0.300; 95% CI 0.275–0.328; p < 0.001) (Table 3).
| Variables | HR | 95%CI | p-value |
|---|---|---|---|
| Facility type | |||
| Community cancer program | Reference | ||
| Comprehensive Community Cancer Program | 0.973 | 0.853–1.108 | 0.676 |
| Academic/Research Program | 0.625 | 0.549–0.712 | <0.001 |
| Integrated Network Cancer Program | 0.842 | 0.726–0.978 | 0.024 |
| Unknown | 1.140 | 0.931–1.395 | 0.204 |
| Age | 1.021 | 1.018–1.025 | <0.001 |
| Gender | |||
| Female | 0.950 | 0.890–1.013 | 0.118 |
| Male | Reference | ||
| Race | |||
| African American | 1.171 | 1.058–1.296 | 0.002 |
| Others | 0.868 | 0.734–1.026 | 0.098 |
| Unknown | 0.571 | 0.363–0.898 | 0.015 |
| White | Reference | ||
| Median household income 2012–2016 | |||
| Less than US$40,227 | Reference | ||
| US$40,227–$50,353 | 1.020 | 0.917–1.136 | 0.710 |
| US$50,354–$63,332 | 0.972 | 0.867–1.089 | 0.620 |
| US$63,333+ | 0.892 | 0.787–1.011 | 0.074 |
| Unknown | 0.604 | 0.298–1.226 | 0.163 |
| Education level 2012–2016 (percentage of not graduated from high school) | |||
| 17.6% or more | Reference | ||
| 10.9–17.5% | 0.965 | 0.873–1.067 | 0.483 |
| 6.3–10.8% | 0.929 | 0.832–1.038 | 0.192 |
| Less than 6.3% | 0.965 | 0.850–1.095 | 0.579 |
| Unknown | 1.384 | 0.634–3.022 | 0.415 |
| Insurance status | |||
| No | 1.217 | 1.027–1.442 | 0.024 |
| Unknown | 0.982 | 0.740–1.303 | 0.900 |
| Yes | Reference | ||
| Area | |||
| Metro counties | Reference | ||
| Rural counties | 1.020 | 0.814–1.276 | 0.866 |
| Urban counties | 1.027 | 0.934–1.131 | 0.580 |
| Unknown | 1.089 | 0.886–1.338 | 0.417 |
| Charlson score | |||
| 0 | 0.768 | 0.602–0.980 | 0.034 |
| 1 | 0.830 | 0.646–1.067 | 0.145 |
| 2 | 1.109 | 0.837–1.468 | 0.471 |
| 3 | Reference | ||
| Clinical T stage | |||
| T0 | Reference | ||
| T1 | 0.591 | 0.311–1.122 | 0.108 |
| T2 | 0.473 | 0.246–0.911 | 0.025 |
| T3 | 0.475 | 0.253–0.889 | 0.020 |
| T4 | 0.739 | 0.393–1.390 | 0.348 |
| Tis | 0.667 | 0.262–1.696 | 0.395 |
| Unknown | 0.626 | 0.335–1.170 | 0.142 |
| Clinical N stage | |||
| N0 | Reference | ||
| N1 | 1.224 | 1.122–1.335 | <0.001 |
| N2 | 1.907 | 1.699–2.141 | <0.001 |
| Unknown | 1.325 | 1.219–1.440 | <0.001 |
| MSI status | |||
| MSI-H | Reference | ||
| MSI-L | 0.818 | 0.677–0.988 | 0.037 |
| Unknown | 0.833 | 0.695–0.999 | 0.49 |
| Chemotherapy | |||
| NO | Reference | ||
| Yes | 0.300 | 0.275–0.328 | <0.001 |
HR: Hazard ratio; MSI: Microsatellite instability.
In the sensitivity cohort (after excluding patients who died within 90 days of the most definitive primary site surgery), factors associated with worse OS were age (HR 1.021; 95% CI 1.018–1.025; p < 0.001), African American race compared with white race (HR 1.179; 95% CI 1.057–1.315; p = 0.003), community cancer program (HR for Academic/Research Program and Integrated Network Cancer Program compared with community cancer program was 0.664; 95% CI 0.576–0.766; p < 0.001 and HR 0.830; 95% CI 0.704–0.978; p = 0.026, respectively), clinical N1 and N2 stage compared with N0 stage (HR 1.206; 95% CI 1.100–1.322; p < 0.001 and HR 1.809; 95% CI 1.597 -2.050; p < 0.001, respectively), and not receiving chemotherapy (HR for receiving chemotherapy compared with not receiving chemotherapy was 0.472; 95% CI 0.422–0.529; p < 0.001) (Table 4).
| Variables | HR | 95%CI | p-value |
|---|---|---|---|
| Facility type | |||
| Community cancer program | Reference | ||
| Comprehensive Community Cancer Program | 1.012 | 0.877–1.169 | 0.867 |
| Academic/Research Program | 0.664 | 0.576–0.766 | <0.001 |
| Integrated Network Cancer Program | 0.830 | 0.704–0.978 | 0.026 |
| Unknown | 1.184 | 0.956–1.466 | 0.121 |
| Age | 1.021 | 1.018–1.025 | <0.001 |
| Gender | |||
| Female | 0.974 | 0.910–1.044 | 0.459 |
| Male | Reference | ||
| Race | |||
| African American | 1.179 | 1.057–1.315 | 0.003 |
| Others | 0.890 | 0.746–1.061 | 0.194 |
| Unknown | 0.572 | 0.354–0.923 | 0.022 |
| White | Reference | ||
| Median household income 2012–2016 | |||
| Less than US$40,227 | Reference | ||
| US$40,227–$50,353 | 1.017 | 0.907–1.139 | 0.778 |
| US$50,354–$63,332 | 0.961 | 0.851–1.085 | 0.521 |
| US$63,333+ | 0.883 | 0.773–1.009 | 0.068 |
| Unknown | 0.659 | 0.310–1.403 | 0.280 |
| Education level 2012–2016 (percentage of not graduated from high school) | |||
| 17.6% or more | Reference | ||
| 10.9%–17.5% | 0.967 | 0.868–1.077 | 0.540 |
| 6.3%–10.8% | 0.927 | 0.824–1.043 | 0.207 |
| Less than 6.3% | 0.949 | 0.829–1.087 | 0.453 |
| Unknown | 1.225 | 0.533–2.813 | 0.632 |
| Insurance status | |||
| No | 1.179 | 0.981–1.418 | 0.079 |
| Unknown | 1.007 | 0.747–1.357 | 0.965 |
| Yes | Reference | ||
| Area | |||
| Metro counties | Reference | ||
| Rural counties | 1.037 | 0.821–1.311 | 0.758 |
| Urban counties | 1.028 | 0.929–1.138 | 0.596 |
| Unknown | 1.133 | 0.913–1.407 | 0.257 |
| Charlson score | |||
| 0 | 0.870 | 0.656–1.155 | 0.335 |
| 1 | 0.928 | 0.694–1.240 | 0.613 |
| 2 | 1.299 | 0.940–1.796 | 0.113 |
| 3 | Reference | ||
| Clinical T stage | |||
| T0 | Reference | ||
| T1 | 0.820 | 0.383–1.754 | 0.609 |
| T2 | 0.652 | 0.301–1.413 | 0.279 |
| T3 | 0.643 | 0.304–1.359 | 0.247 |
| T4 | 0.981 | 0.462–2.083 | 0.960 |
| Tis | 0.844 | 0.295–2.416 | 0.752 |
| Unknown | 0.836 | 0.397–1.762 | 0.638 |
| Clinical N stage | |||
| N0 | Reference | ||
| N1 | 1.206 | 1.100–1.322 | <0.001 |
| N2 | 1.809 | 1.597–2.050 | <0.001 |
| Unknown | 1.305 | 1.195–1.427 | <0.001 |
| MSI status | |||
| MSI-H | Reference | ||
| MSI-L | 0.820 | 0.670–1.002 | 0.053 |
| Unknown | 0.835 | 0.688–1.014 | 0.068 |
| Chemotherapy | |||
| NO | Reference | ||
| Yes | 0.472 | 0.422–0.529 | <0.001 |
HR: Hazard ratio.
Discussion
To our knowledge, this is the largest real-world study that looked at the chemotherapy effect in metastatic CRC with only liver metastases who were treated with metastasectomy and compared the OS between patients who received perioperative chemotherapy versus patients treated with surgery only in addition to comparing the OS between adjuvant chemotherapy and neoadjuvant chemotherapy and comparing the OS between single-agent and multiagent chemotherapy.
Our study showed that patients with metastatic CRC with liver metastases who were treated with chemotherapy in addition to surgery had statistically significant better OS compared with patients who didn't receive chemotherapy. Also, in the multivariable analysis, we found that chemotherapy was independently associated with better OS.
There is limited data about the role of perioperative chemotherapy in patients with liver metastases from CRC. Most of the studies had a small number of patients and were designed to evaluate the effect of chemotherapy on recurrence- and PFS rather than overall survival. And the majority of the studies that evaluated the effect of chemotherapy on OS didn't report a significant difference in the OS between patients who received perioperative chemotherapy and patients who did not.
Nordlinger et al., in a European Organization for Research and Treatment of Cancer trial based on 364 patients with metastatic CRC and up to four liver metastases, who were recruited from 78 hospitals from different European countries, compared the outcomes of 182 patients who received perioperative FOLFOX-4 chemotherapy to those of 182 patients who had surgery only. Initial results showed chemotherapy was associated with better 3-year PFS compared with surgical resection alone. After a median follow-up of 8·5 years, it was found that patients who received perioperative chemotherapy had a better median OS and 5-year OS, but it wasn't statistically significant. There are multiple factors in that study that could contribute to the lack of difference in the OS between the two groups. In addition to the small number of included patients, the study was designed with PFS being the primary end point whereas OS was a secondary end point. Also, the perioperative group had a higher number of non-cancer deaths compared with the surgery-only group [12,15]. Similarly, Portier et al., in the FFCD trial compared the outcomes between patients who had surgery only versus patients who had adjuvant chemotherapy with fluorouracil and folinic acid in 173 patients with liver metastases from CRC. They found that patients who received adjuvant chemotherapy had better 5-year OS, but it wasn't statistically significant. Several factors could be behind this result, the study wasn't designed with overall survival as an end point, also recurrences in both groups were treated by second-line chemotherapy, or by repeat liver resections, which influenced the natural history of the disease [16]. Hasegawa et al., in a randomized controlled trial, assigned 180 patients with CRC liver metastasis into two groups; patients who received adjuvant chemotherapy with uracil-tegafur and leucovorin and patients who had had surgery only. They found that patients who received adjuvant chemotherapy had significantly reduced recurrence compared with the patients who had surgery only, but there was no difference in the OS (66.1% vs 66.8%; p = 0.409). Multiple limitations also may have contributed to this result; the short period of follow-up (median follow-up was less than 5 years), a small number of included patients, and the way the study was designed with recurrence-free survival as the primary end point whereas the OS was a secondary end point [17]. Kemeny et al., did a randomized trial of 75 patients with one to three hepatic metastases of CRC where patients were randomized to hepatic resection alone or resection followed by hepatic arterial infusion of floxuridine and systemic 5-FU. The results showed that patients who received chemotherapy had a better 4-year OS and median OS, but the difference wasn't statistically significant (p = 0.6) [18].
While the previously mentioned studies failed to show a significant effect of chemotherapy on OS, another study reported a positive effect of chemotherapy on OS. A pooled analysis of two trials done by Mitry et al., that included 278 patients with metastatic CRC (171 patients with liver metastases from the FFCD trial and 107 patients with liver or lung metastases from the ENG trial) and found that compared with patients who had surgery alone, patients who had adjuvant chemotherapy had better median PFS and median OS, but the differences were not statistically significant. Whereas, in multivariable analysis, they found that adjuvant chemotherapy was associated with better PFS and OS [19] which aligns with our findings.
On the other hand, Kanemitsu et al., in a randomized trial of 300 patients with metastatic CRC with an unlimited number of liver metastases, found that patients who had adjuvant modified FOLFOX6 regimen had better disease-free survival, but a numerically worse 3-year OS and worse 5-year OS compared with patients who had hepatectomy alone, but the differences were not statistically significant [20].
Among patients who received chemotherapy, we found that patients were treated with neoadjuvant chemotherapy had better OS compared with patients were treated with adjuvant chemotherapy. Also, we found patients who received multiagent chemotherapy had better OS compared with patients who received single-agent chemotherapy.
The vast majority of trials, that were done on metastatic CRC, assessed the effect of perioperative chemotherapy compared with surgical resection only, and while the comparison between adjuvant and neoadjuvant chemotherapy in non-metastatic CRC has been investigated, there are very few prospective studies done in metastatic cases. While some studies suggest neoadjuvant chemotherapy is beneficial in unresectable disease and helps in improving the complete resection success rate [21], other studies showed that neoadjuvant chemotherapy was associated with increased liver toxicity and suggest adjuvant chemotherapy was more beneficial in managing micro-metastases with less liver toxicity-related complications [22–25].
Despite its use it is not very common, using neoadjuvant chemotherapy in the sitting of unresectable colorectal liver metastases, which is referred to as conversion chemotherapy, seems to have a survival benefit in these cases. This area of interest is still under extensive study and evaluation. The ideal chemotherapy regimen has not been established yet and different matters regarding to the chemotherapy timing, dosage and live toxicity should be taken into consideration [26,27]. Adam et al., evaluated the impact of conversion chemotherapy on the outcome of 1104 patients with unresectable colorectal liver metastases. They found that conversion chemotherapy allowed 12.5% of patients with unresectable colorectal liver metastases to be rescued by liver surgery [28].
In the setting of not having a head-to-head comparison between adjuvant and neoadjuvant chemotherapy in metastatic disease [29,30], the National Comprehensive Cancer Network guidelines still recommends using peri-operative chemotherapy for a total of 6 months without a preference for adjuvant or neoadjuvant chemotherapy [31].
When it comes to the comparison between the single-agent and multiagent chemotherapy, few studies looked at that in the setting of metastatic disease. Seymour et al., evaluated 2135 patients with inoperable metastatic or locoregional CRC and compared the OS in three different chemotherapy strategies; the first group received single-agent as a first line and single-agent as a second line, the second group received single-agent as a first line and combination chemotherapy as a second line, the third group received combination chemotherapy as a first line. The study showed that the group treated with combination chemotherapy as a first line had better OS compared with the group that received single-agent chemotherapy in both first and second line. Interestingly, there was no statistically significant difference in the OS between the group that received single-agent chemotherapy as a first and second line and the group that received single-agent chemotherapy as a first line and combination chemotherapy as a second line. These results are similar to our result in one way that patients who received multiagent chemotherapy as a first line had better OS than patients who received single-agent as a first line. Unfortunately, the NCDB doesn't provide details about the second line chemotherapy to be able to compare patients according to second line chemotherapy like the mentioned study [32]. The biggest limiting factor in this study is that recruited patients were selected as a poor-prognosis group who were definitely incurable and patients with operable metastases were excluded.
Koopman et al., in phase III randomized controlled trial (CAIRO study), reported no statistically significant difference in the OS between patients with advanced CRC who received combination chemotherapy as a first line and patients who received the same chemotherapy agents but were given sequentially [33]. Similar to what we mentioned before, the chemotherapy details in NCDB are limited to first line chemotherapy.
It is worth mentioning that the two mentioned studies [32,33] enrolled metastatic CRC cases are not amenable for curative surgery, while patients in our study received surgery for the primary tumor and the metastatic liver metastases.
Our study has some limiting factors that need to be discussed; first, the type of chemotherapy that patients received was not available. This could have impacted the outcomes of some patients receiving adjuvant chemotherapy. Second, the differentiation between single-agent and multiagent chemotherapy is limited to the first line of chemotherapy not total chemotherapy the patient may have received. Third, the distribution and completeness of surgical resection of liver metastases were not specified in the database. Fourth, data about liver metastases like number, dimension, site or resectability and molecular profile (RAS/BRAF) are not available in NCDB. This is an important element that could have affected patients' outcomes if there is an imbalanced between both groups. Fifth, NCDB also doesn't have details about other oncologic end points like disease-free survival and cancer-specific survival (both represent important end points to evaluate the effect of chemotherapy). Sixth, the retrospective nature of data collection within the NCDB might have affected the veracity of the analyses as well.
It is worth mentioning as well that in our study, patients who had surgery only were older compared with patients who received perioperative chemotherapy (mean age in years 70 vs 58) which could be a significant factor that affects the difference in the OS between the two groups as older patients tend to have more comorbidities and as a result more likely not to receive chemotherapy. To account for this potential bias, we did a propensity score matching for age and Charlson comorbidity score as well as multivariable Cox regression analysis incorporating other relevant baseline factors.
Conclusion & future perspective
In conclusion, our study shows that the addition of chemotherapy to surgery improves the OS in metastatic CRC with liver metastases treated with metastasectomy. Also, neoadjuvant and multiagent chemotherapy seem to improve the OS compared with adjuvant and single-agent chemotherapy, respectively. Further large-scale studies are needed to evaluate the effect of chemotherapy role and timing not only on recurrence and PFS but also on OS.
•
Colorectal cancer (CRC) is the third most diagnosed malignancy and the second leading cause of cancer-related death in the USA.
•
About 50% of CRC cases develop liver metastases.
•
The survival benefit of perioperative chemotherapy in patients with metastatic CRC with liver metastases is still unclear.
•
We compare overall survival (OS) between adjuvant and neoadjuvant chemotherapy and analyze the effect of chemotherapy on OS.
•
We found that perioperative chemotherapy improves the OS in metastatic CRC with liver metastases.
•
In metastatic CRC with liver metastases neoadjuvant and multiagent chemotherapy improves the OS compared with adjuvant and single-agent chemotherapy, respectively.
Author contributions
F Baidoun: data analysis, data interpretation, manuscript writing. Z Merjaneh: manuscript writing. R Nanah: manuscript writing. AM Saad: manuscript editing, critical revision. O Abdel-Rahman: study concept, manuscript editing, critical revision.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
Supplementary Material
File (supplementary figure a.docx)
- Download
- 63.08 KB
File (supplementary figure b.docx)
- Download
- 62.21 KB
File (supplementary figure c.docx)
- Download
- 61.74 KB
File (supplementary figure d.docx)
- Download
- 63.16 KB
File (supplementary figure e.docx)
- Download
- 96.43 KB
File (supplementary figure f.docx)
- Download
- 94.74 KB
File (supplementary figure g.docx)
- Download
- 99.48 KB
File (supplementary table a.docx)
- Download
- 19.88 KB
File (supplementary table b.docx)
- Download
- 20.06 KB
References
1.
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J. Clin. 70(1), 7–30 (2020).
2.
Zarour LR, Anand S, Billingsley KG et al. Colorectal cancer liver metastasis: evolving paradigms and future directions. CMGH 3(2), 163–173 (2017).
3.
Baidoun F, Elshiwy K, Elkeraie Y et al. Colorectal cancer epidemiology: recent trends and impact on outcomes. Curr. Drug Targets 22(9), 998–1009 (2021).
4.
Kanas GP, Taylor A, Primrose JN et al. Survival after liver resection in metastatic colorectal cancer: review and meta-analysis of prognostic factors. Clin. Epidemiol. 4(1), 283–301 (2012).
5.
Abdalla EK, Vauthey JN, Ellis LM et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann. Surg. 239(6), 818–827 (2004).
6.
Tomlinson JS, Jarnagin WR, DeMatteo RP et al. Actual 10-year survival after resection of colorectal liver metastases defines cure. J. Clin. Oncol. 25(29), 4575–4580 (2007).
7.
Oweira H, Mehrabi A, Reissfelder C, Abdel-Rahman O. A real-world, population-based analysis of the outcomes of colorectal cancer patients with isolated synchronous liver or lung metastases treated with metastasectomy. World J. Surg. 44(5), 1604–1611 (2020).
8.
Messersmith WA. NCCN Guidelines Updates: Management of Metastatic Colorectal Cancer. J. Natl Compr. Canc. Netw. 17(55), 599–601 (2019).
9.
Chakedis J, Schmidt CR. Surgical treatment of metastatic colorectal cancer. Surg. Oncol. Clin. N. Am. 27(2), 377–399 (2018).
10.
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet 394(10207), 1467–1480 (2019).
11.
Fong Y, Fortner J, Sun RL, Brennan MF, Blumgart LH. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer. Ann. Surg. 230(3), 309 (1999).
12.
Nordlinger B, Sorbye H, Glimelius B et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet 371(9617), 1007–1016 (2008).
13.
Ichikawa N, Kamiyama T, Yokoo H et al. Preoperative chemotherapy in colorectal cancer patients with synchronous liver metastasis. Mol. Clin. Oncol. 12(4), 374–383 (2020).
14.
National Cancer Database - About the National Cancer Database. (Accessed 8 September 2020) www.facs.org/quality-programs/cancer/ncdb/about
15.
Nordlinger B, Sorbye H, Glimelius B et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 14(12), 1208–1215 (2013).
16.
Portier G, Elias D, Bouche O et al. Multicenter randomized trial of adjuvant fluorouracil and folinic acid compared with surgery alone after resection of colorectal liver metastases: FFCD ACHBTH AURC 9002 Trial. J. Clin. Oncol. 24(31), 4976–4982 (2006).
17.
Hasegawa K, Saiura A, Takayama T et al. Adjuvant oral uracil-tegafur with leucovorin for colorectal cancer liver metastases: a randomized controlled trial. PLoS ONE 11(9), e0162400 (2016).
18.
Kemeny MM, Adak S, Gray B et al. Combined-modality treatment for resectable metastatic colorectal carcinoma to the liver: surgical resection of hepatic metastases in combination with continuous infusion of chemotherapy - An intergroup study. J. Clin. Oncol. 20(6), 1499–1505 (2002).
19.
Mitry E, Fields ALA, Bleiberg H et al. Adjuvant chemotherapy after potentially curative resection of metastases from colorectal cancer: a pooled analysis of two randomized trials. J. Clin. Oncol. 26(30), 4906–4911 (2008).
20.
Kanemitsu Y, Shimizu Y, Mizusawa J et al. A randomized phase II/III trial comparing hepatectomy followed by mFOLFOX6 with hepatectomy alone for liver metastasis from colorectal cancer: JCOG0603 study. J. Clin. Oncol. 38(Suppl. 15), 4005–4005 (2020).
21.
Bismuth H, Adam R, Lévi F et al. Resection of nonresectable liver metastases from colorectal cancer after neoadjuvant chemotherapy. Ann. Surg. 224(4), 509–522 (1996).
22.
Vauthey JN, Pawlik TM, Ribero D et al. Chemotherapy regimen predicts steatohepatitis and an increase in 90-day mortality after surgery for hepatic colorectal metastases. J. Clin. Oncol. 24(13), 2065–2072 (2006).
23.
Mehta NN, Ravikumar R, Coldham CA et al. Effect of preoperative chemotherapy on liver resection for colorectal liver metastases. Eur. J. Surg. Oncol. 34(7), 782–786 (2008).
24.
Fernandez FG, Ritter J, Goodwin JW, Linehan DC, Hawkins WG, Strasberg SM. Effect of steatohepatitis associated with irinotecan or oxaliplatin pretreatment on resectability of hepatic colorectal metastases. J. Am. Coll. Surg. 200(6), 845–853 (2005).
25.
Parks R, Gonen M, Kemeny N et al. Adjuvant chemotherapy improves survival after resection of hepatic colorectal metastases: analysis of data from two continents. J. Am. Coll. Surg. 204(5), 753–761 (2007).
26.
Symonds LK, Cohen SA. Use of perioperative chemotherapy in colorectal cancer metastatic to the liver. Gastroenterol. Rep. 7(5), 301–311 (2019).
27.
Chan G, Chee CE. Perioperative chemotherapy for liver metastasis of colorectal cancer. Cancers (Basel). 12(12), 3535 (2020).
28.
Adam R, Delvart V, Pascal G et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy. Ann. Surg. 240(4), 644–658 (2004).
29.
Sauer R, Becker H, Hohenberger W et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 351(17), 1731–1740 (2004).
30.
De Gooyer JM, Verstegen MG, Lam-Boer J et al. Neoadjuvant chemotherapy for locally advanced T4 colon cancer: a nationwide propensity-score matched cohort analysis. Dig. Surg. 37(4), 292–301 (2020).
31.
NCCN Clinical Practice Guidelines in Oncology - Colon Cancer. www.nccn.org/professionals/physician_gls/pdf/colon.pdf
32.
Seymour MT, Maughan TS, Ledermann JA et al. Different strategies of sequential and combination chemotherapy for patients with poor prognosis advanced colorectal cancer (MRC FOCUS): a randomised controlled trial. Lancet 370(9582), 143–152 (2007).
33.
Koopman M, Antonini NF, Douma J et al. Sequential versus combination chemotherapy with capecitabine, irinotecan, and oxaliplatin in advanced colorectal cancer (CAIRO): a Phase III randomised controlled trial. Lancet 370(9582), 135–142 (2007).
Information & Authors
Information
Published In
Pages: 935 - 951
PubMed: 35787069
Copyright
© 2022 The Authors. This work is licensed under the Creative Commons Attribution 4.0 License
History
Received: 6 October 2021
Accepted: 15 June 2022
Published online: 5 July 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of perioperative chemotherapy on survival outcomes among patients with metastatic colorectal cancer to the liver. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0239
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Zhiguo Tang, Guojia Zhou, Yu Xu, Yang Zhang, Yinxu Zhang, Prognostic model for early-onset colorectal cancer with liver metastasis after primary tumor resection and chemotherapy, Scientific Reports, 10.1038/s41598-025-21410-x, 15, 1, (2025).