Sex-based differences in the outcomes of patients with lung carcinoids
Publication: Journal of Comparative Effectiveness Research
Abstract
Objective: To assess the impact of sex on the outcomes of patients with well-differentiated lung neuroendocrine neoplasms in a real-world setting. Methods: The Surveillance, Epidemiology and End Results Research Plus database (2000–2018) was accessed, and patients with a diagnosis of typical or atypical carcinoid of the lung were reviewed. Trends in age-standardized rates (per 100,000) of the incidence of lung carcinoid tumors were reviewed among male and female patients as well as the overall population, and annual percent change (APC) was determined for the three groups. Multivariate Cox regression analysis was then used to assess the factors associated with overall and cancer-specific survival. Results: Among all patients, APC (2000–2018) for lung carcinoid diagnosis was 2.9 (95% CI: 2.4–3.5). Among male patients, APC (2000–2018) for lung carcinoid diagnosis was 1.8 (95% CI: 1.2–2.5). By contrast, among female patients, APC (2000–2018) for lung carcinoid diagnosis was 3.4 (95% CI: 2.8–4.1). Based on Kaplan–Meier survival estimates, female sex was associated with better overall survival compared with male sex (p < 0.001). Based on multivariate Cox regression analysis, the following factors were associated with worse cancer-specific survival: older age (hazard ratio [HR]: 1.036; 95% CI: 1.031–1.041), atypical carcinoid histology (HR: 3.10; 95% CI: 2.71–3.56), stage (distant vs localized stage HR: 4.05; 95% CI: 3.48–4.71), sex (male vs female sex HR: 1.76; 95% CI: 1.56–1.99) and no surgical treatment (HR: 3.77; 95% CI: 3.22–4.42). Conclusion: Female patients with lung carcinoid tumors have better overall survival compared with male patients, particularly among patients with typical carcinoid tumors.
Neuroendocrine neoplasms (NENs) represent a heterogeneous group of neoplasms with diverse anatomy, biology, histology and treatment algorithms. The lung is the second most frequent site of NENs after the digestive system [1–3]. Biologically, gastroenteropancreatic (GEP) NENs are currently classified differently than lung NENs, and this is reflected in the most recent versions of the WHO classification for both disease entities [4–6].
Sex-based differences have been observed in the etiology and outcomes of solid tumors, including some NENs [7,8]. A previous population-based study suggested that female sex is associated with better survival outcomes among patients with GEP NENs, although it is unclear if these differences are reflective of biological differences between men and women or differences in noncancer mortality between men and women [9]. Similarly, a number of other population-based studies have previously shown that female sex is associated with better outcomes among patients with all types of NENs [10,11]. However, it is unclear if the same observation would hold for patients with lung NENs. The current study will specifically focus on well-differentiated lung NENs, which are referred to in the 2015 WHO classification as carcinoid tumors (typical and atypical) [12].
The Surveillance, Epidemiology and End Results (SEER) database represents an ideal method for studying this research question given its large sample size and given the relative rarity of well-differentiated lung NENs, which makes it difficult to address this question within a smaller data set. The objective of this study was to assess the impact of sex on the outcomes of patients with well-differentiated lung NENs in a real-world setting.
Methods
Data sources
The current study is based on the SEER Research Plus database (2000–2018) [13]. This database covers approximately 28% of cancer diagnoses in the USA, and survival follow-up continues through December 2018. The current study included patients diagnosed with typical or atypical carcinoid of the lung, including International Classification of Diseases for Oncology codes 8240/3, 8241/3 and 8249/3. For patients with duplicate records/multiple primary lung carcinoid tumors, only the first reported tumor was included. For trend analysis, all patients diagnosed in this time period were included, whereas for survival analysis, only patients diagnosed 2004–2018 were included, as combined SEER summary stage was available for only this time period.
Data collection
The following data were collected from each patient where available: age at diagnosis, race, sex, histological subtype (typical vs atypical carcinoid), stage (according to combined SEER summary stage), surgery to the primary tumor, radiation therapy and chemotherapy. The reason for using combined SEER summary stage rather than American Joint Committee on Cancer stage was the change in American Joint Committee on Cancer staging systems that occurred across the course of the study (three versions were in use at various time points). SEER summary stage classifies disease into localized stage (i.e., limited to the primary site), regional stage (i.e., regional extension of the tumor and/or regional lymph node involvement) and distant stage (i.e., evidence of distant metastatic disease). End points for this study included overall survival (OS), which was defined as the time from diagnosis until death for any reason, and cancer-specific survival (CSS), which was defined as the time from diagnosis until death due to lung carcinoid.
Statistical analysis
Using SEER*Stat software, trends in age-standardized rates (per 100,000) of the incidence of lung carcinoid tumors were reviewed among male and female patients as well as the overall population. Annual percent change (APC) was calculated for each of the three categories (males, females and overall).
For the survival cohort, descriptive statistics were initially reviewed to compare baseline characteristics of male versus female patients. Chi-square testing was used for categorical variables, and independent t-test was used for continuous variables.
Kaplan–Meier survival estimates and log-rank testing were used to compare OS outcomes between male and female patients in the overall cohort as well as among substrata defined by histology (typical vs atypical carcinoid) and stage (localized/regional vs distant). Kaplan–Meier survival estimates for CSS are not shown, as these did not fulfill the assumptions of Kaplan–Meier survival estimates – specifically, patients who are censored because they died of reasons other than lung carcinoid tumors which do not have the same survival prospects as those who continued to be followed, which violates one of the basic assumptions of Kaplan–Meier estimates [14].
Multivariate Cox regression analysis was used to further assess the factors associated with OS and CSS. Factors included within Cox regression models were: age at diagnosis, race, sex, stage, histology and surgery to the primary tumor. Because of the lack of evidence of survival benefit with the use of systemic and/or radiation therapy and because of the uncertainty surrounding the reporting of these treatments in the SEER database (e.g., whether the reported systemic therapy is chemotherapy or targeted therapy, what the dose/schedule/location of the radiation therapy used is), systemic and radiation therapy was not included in the Cox regression models. The aforementioned descriptive and survival statistical analyses were conducted using SPSS Statistics 23.0 software (IBM Corporation, NY, USA).
To obtain a more robust assessment of the impact of sex on outcomes of the study cohort, a competing risk analysis was done, incorporating all factors that were included in the aforementioned multivariate Cox regression models. This was done using Stata 14.0 (StataCorp LLC, TX, USA).
Results
Trends in incidence of lung carcinoid tumors among male versus female patients
Among all patients, APC (2000–2018) for lung carcinoid diagnosis was 2.9 (95% CI: 2.4–3.5). Among male patients, APC (2000–2018) was 1.8 (95% CI: 1.2–2.5). By contrast, among female patients, APC (2000–2018) was 3.4 (95% CI: 2.8–4.1) (Figure 1A). Among patients with typical carcinoid tumors, APC (2000–2018) was 2.2 (95% CI: 1.7–2.7). Among male patients, APC (2000–2018) was 0.8 (95% CI: 0.2–1.5). By contrast, among female patients, APC (2000–2018) was 2.8 (95% CI: 2.1–3.4) (Figure 1B). APC for atypical carcinoid tumors could not be calculated because of very small numbers in some years.
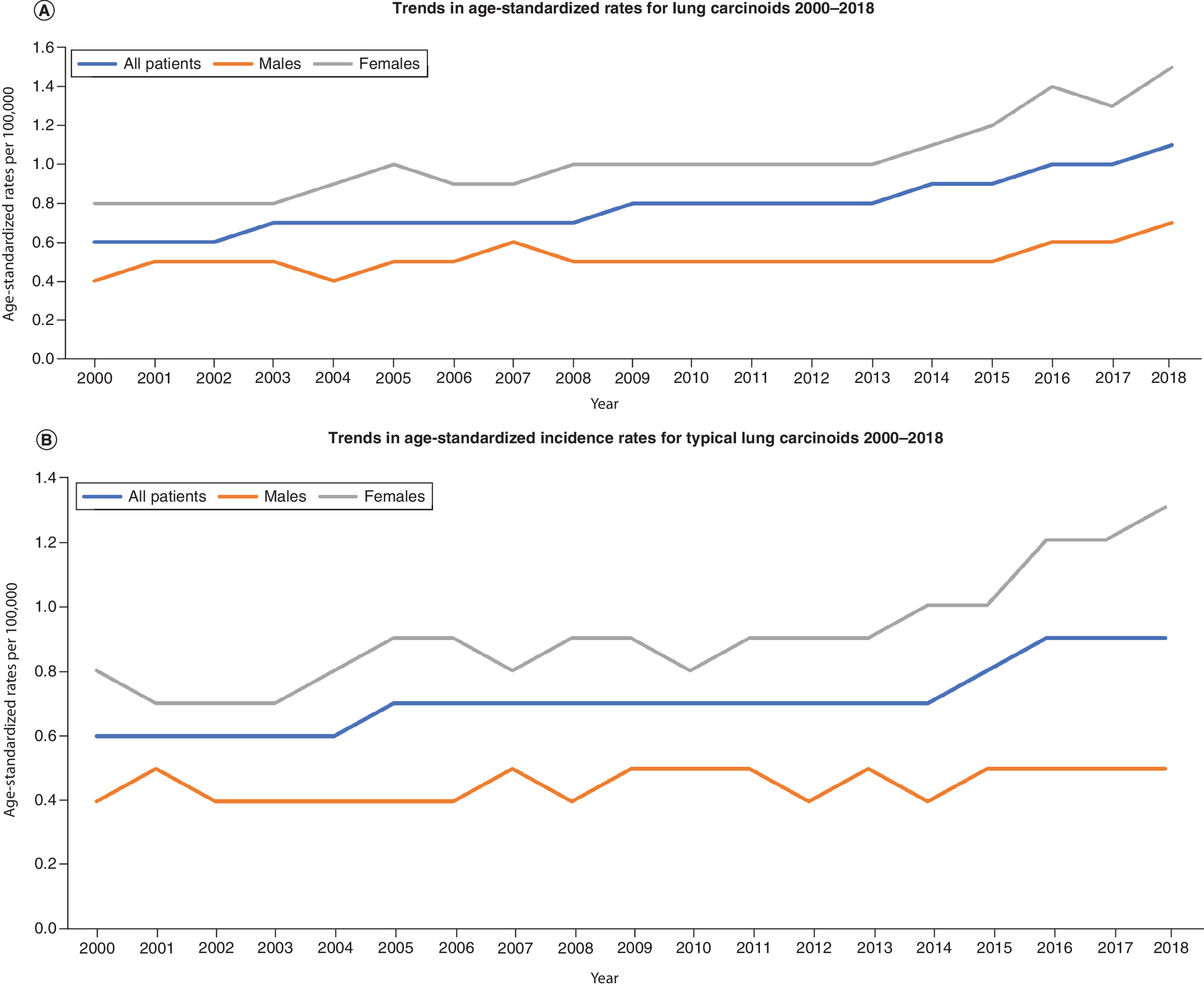
Figure 1. Trends in incidence of pulmonary carcinoid tumors among male and female patients 2000–2018.
(A) Trends for all patients. (B) Trends for typical carcinoid patients. Age-adjusted rates are calculated per 100,000.
Survival cohort
A total of 11,255 patients with lung carcinoid tumors diagnosed 2004–2018 were found to be eligible in the survival cohort and were included in the current study. This included 7909 (70.3%) female patients and 3346 (29.7%) male patients. In comparing both groups, female patients were likely to be older (p < 0.001) and White (p = 0.033) and have typical carcinoid (p = 0.001), distant stage (p = 0.012) and sublobar resection (p < 0.001) (Table 1).
| Parameter | Males (n = 3346) | Females (n = 7909) | p-value |
|---|---|---|---|
| Age, mean (SD) | 60.65 (15.41) | 63.53 (14.02) | < 0.001 |
| Race, n (%) – White – Black – Asian/Pacific Islander – American Indian – Unknown | 2940 (87.9) 274 (8.2) 101 (3) 8 (0.2) 23 (0.7) | 7073 (89.4) 577 (7.3) 198 (2.5) 29 (0.4) 32 (0.4) | 0.033 |
| Histology, n (%) – Typical carcinoid† – Atypical carcinoid | 2922 (87.3) 424 (12.7) | 7076 (89.5) 833 (10.5) | 0.001 |
| SEER summary stage, n (%) – Localized – Regional – Distant – Unknown | 2152 (64.3) 673 (20.1) 414 (12.4) 107 (3.2) | 5145 (65.1) 1428 (18.1) 1108 (14) 228 (2.9) | 0.012 |
| Surgery to the primary tumor, n (%) – None – Sublobar resection – Lobectomy – Pneumonectomy – Unknown | 865 (25.9) 621 (18.6) 1736 (51.9) 102 (3) 22 (0.7) | 1858 (23.5) 2021 (25.6) 3789 (47.9) 174 (2.2) 67 (0.8) | < 0.001 |
| Systemic treatment, n (%) – Yes – No/unknown | 263 (7.9) 3083 (92.1) | 432 (5.5) 7477 (94.5) | < 0.001 |
| Radiation therapy, n (%) – Yes – No/unknown | 241 (7.2) 3105 (92.8) | 366 (4.6) 7543 (95.4) | < 0.001 |
†
Includes patients with enterochromaffin cell carcinoid tumors. n = 11,255 patients.
SD: Standard deviation; SEER: Surveillance, Epidemiology and End Results.
Based on Kaplan–Meier survival estimates, female sex was associated with better OS compared with male sex (p < 0.001) (Figure 2A). When stratified by histology, female sex was associated with better OS among patients with typical carcinoid (p < 0.001) but not among patients with atypical carcinoid (p = 0.745) (Figure 2B & C). When stratified by stage, female sex was associated with better OS among patients with localized/regional disease (p < 0.001) as well as among patients with distant metastatic disease (p < 0.001) (Figure 2D & E).
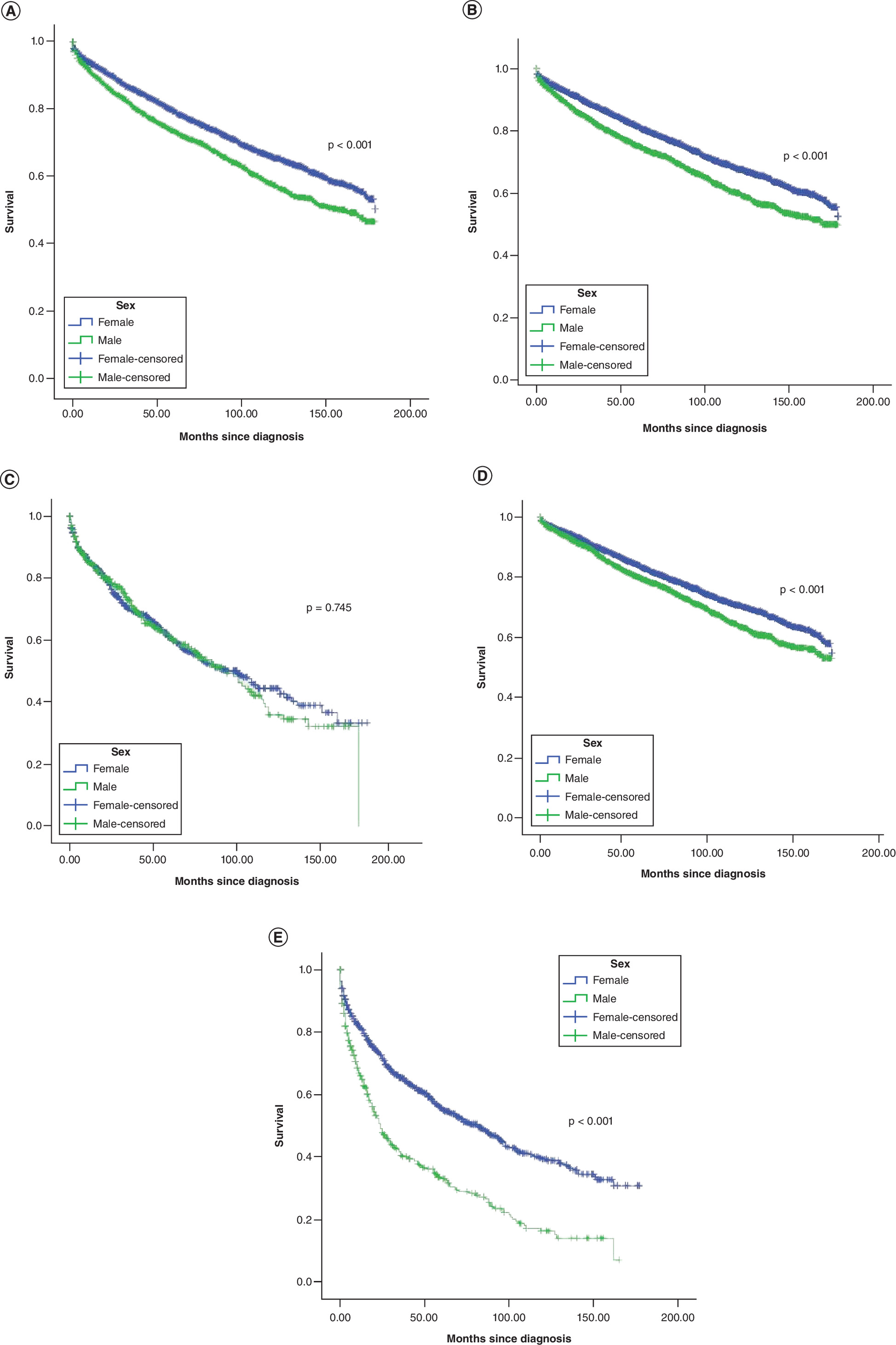
Figure 2. Overall survival according to Kaplan–Meier estimates among lung carcinoid patients.
(A) All categories. (B) Typical carcinoid. (C) Atypical carcinoid. (D) Local/regional disease. (E) Distant disease.
Based on multivariate Cox regression analysis, the following factors were associated with worse OS: older age (hazard ratio [HR]: 1.051; 95% CI: 1.047–1.055), Black race (HR: 1.20; 95% CI: 1.05–1.38), atypical carcinoid histology (HR: 2.09; 95% CI: 1.88–2.33), stage (distant vs localized stage HR: 4.05; 95% CI: 3.48–4.71), sex (male vs female sex HR: 1.59; 95% CI: 1.46–1.72) and no surgical treatment (HR: 3.14; 95% CI: 2.84–3.48). Likewise, the following factors were associated with worse CSS: older age (HR: 1.036; 95% CI: 1.031–1.041), atypical carcinoid histology (HR: 3.10; 95% CI: 2.71–3.56), stage (distant vs localized stage HR: 4.05; 95% CI: 3.48–4.71), sex (male vs female sex HR: 1.76; 95% CI: 1.56–1.99) and no surgical treatment (HR: 3.77; 95% CI: 3.22–4.42) (Table 2). Stratified analysis by histology was also performed to evaluate the association between sex and outcomes of interest. The results indicated that sex was associated with a difference in OS and CSS among patients with typical carcinoid histology but not among patients with atypical carcinoid histology (Supplementary Tables 1 & 2).
| Parameter | OS | CSS |
|---|---|---|
| HR (95% CI) | HR (95% CI) | |
| Age | 1.051 (1.047–1.055) | 1.036 (1.031–1.041) |
| Race – White – Black – Asian/Pacific Islander – American Indian | Reference 1.20 (1.05–1.38) 0.87 (0.67–1.13) 0.62 (0.28–1.37) | Reference 1.13 (0.93–1.37) 1.13 (0.80–1.59) 1.08 (0.41–2.89) |
| Histology – Typical carcinoid – Atypical carcinoid | Reference 2.09 (1.88–2.33) | Reference 3.10 (2.71–3.56) |
| SEER summary stage – Localized – Distant – Regional | Reference 1.84 (1.41–2.39) 1.26 (1.13–1.41) | Reference 4.05 (3.48–4.71) 2.18 (1.86–2.55) |
| Sex – Female – Male | Reference 1.59 (1.46–1.72) | Reference 1.76 (1.56–1.99) |
| Surgery to the primary tumor – Lobectomy – None – Sublobar resection – Pneumonectomy | Reference 3.14 (2.84–3.48) 1.26 (1.13–1.41) 1.84 (1.41–2.39) | Reference 3.77 (3.22–4.42) 1.02 (0.84–1.24) 2.17 (1.53–3.08) |
Patients with unknown race, stage or surgery were excluded from the analysis.
CSS: Cancer-specific survival; HR: Hazard ratio; OS: Overall survival; SEER: Surveillance, Epidemiology and End Results.
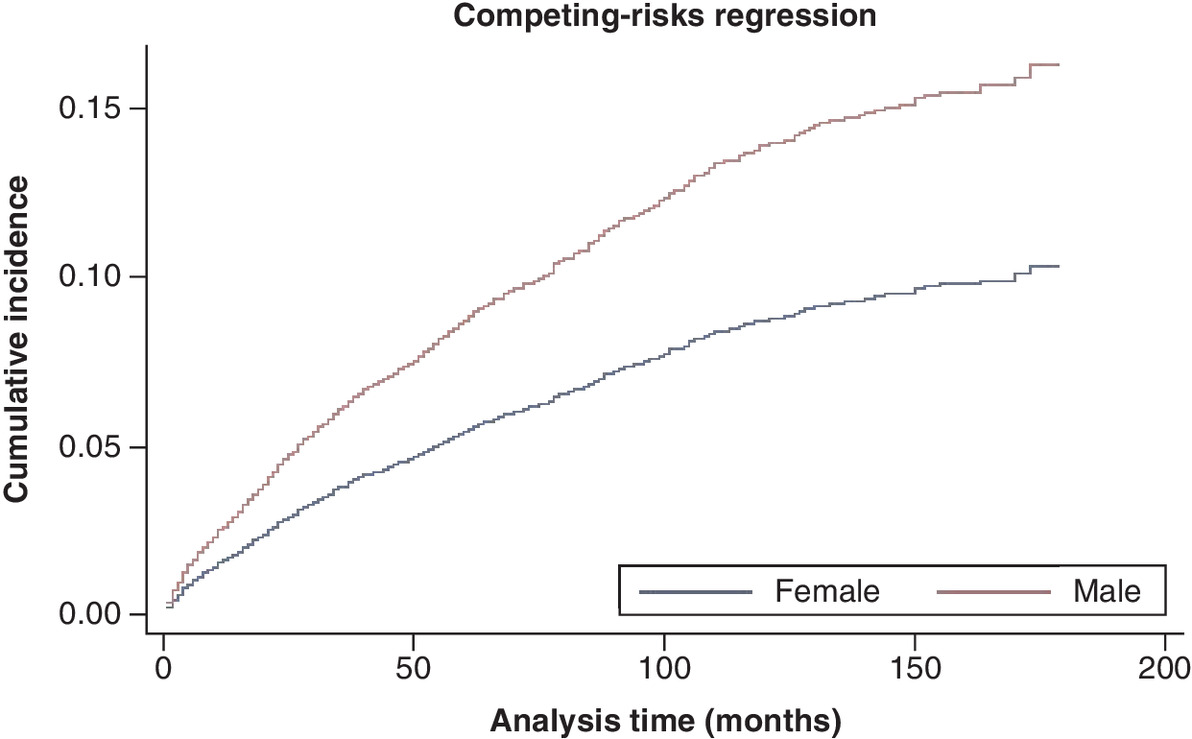
Based on competing risk analysis, and using a model adjusted for age, stage, race, surgery and histology, female sex was associated with less risk of death (female vs male patient subdistribution HR: 0.61; 95% CI: 0.53–0.69). Figure 3 shows the cumulative incidence function for female versus male patients.
Discussion
The current study evaluated the impact of sex on the outcomes of patients with lung carcinoid tumors. Within the study cohort, the proportion of male patients was less than 50% the proportion of female patients, and the APC of the incidence of lung carcinoid tumors among female patients was higher than the APC among male patients. Moreover, female patients had better OS compared with male patients, particularly among patients with typical carcinoid tumors.
Sex has been linked to differential outcomes of many solid tumors, including endocrine-sensitive and endocrine-insensitive cancers [15,16]. Sex has also been linked to differences in drug metabolism and prevalence of adverse events with systemic therapy [17]. In the context of endocrine-related cancers, including thyroid cancer, breast cancer and GEP NENs, female patients have consistently better outcomes compared with male patients [11,18]. Similarly, in patients with pulmonary endocrine-insensitive cancers (e.g., non-small and small cell lung cancer), female patients enjoy better survival outcomes compared with male patients [19,20]. Several hypotheses have been proposed to explain these observed differences. These include higher comorbidity burden among men compared with women, which is likely to affect the ability to administer aggressive treatments or undergo major surgeries. It is also possible that hormonal factors play a role in disease biology and/or response to therapy, although this is not clearly understood [21–23]. Recent preclinical data suggest that lung carcinoid tumors can be classified into a few distinct and prognostically relevant categories according to transcriptomic signatures [24–26]. Whether this biological classification might help to explain the findings of the current study is unclear.
Additionally, a recent study examined the incidence and survival outcomes of lung NENs in the US, including typical carcinoid tumors, atypical carcinoid tumors, large cell neuroendocrine carcinoma and small cell lung cancer [3]. This study also showed that female sex is associated with better outcomes. However, contrary to the current study, it was not focused on well-differentiated NENs (typical and atypical carcinoid tumors). The current study focused on this subset because the authors believe that typical and atypical carcinoid tumors represent a biologically and clinically distinct disease category compared with more aggressive subtypes of lung NENs [12]. Another recent study limited to patients with typical carcinoid tumors provided similar conclusions, with female patients having better outcomes compared with male patients [27].
With the exception of the category of atypical carcinoid tumors, better outcomes for female versus male patients were also observed in all examined substrata. One possible explanation for this might be related to the small number of patients in the atypical carcinoid subcategory, which prevented the demonstration of survival differences between female and male patients. It is interesting to note that female patients represented >70% of the survival cohort in this study, and the number of female patients was more than double the number of male patients (this difference was more pronounced within the category of typical carcinoid tumors versus the category of atypical carcinoid tumors). By contrast, recent data from the authors' group suggest that there is no such difference in incidence between male and female patients in the setting of GEP NENs [28]. The reason for this epidemiological disparity is unclear, and this needs to be further explored in future studies.
The current study has a few limitations that need to be considered. Several relevant baseline prognostic factors are not available within the SEER database (e.g., performance status, comorbidities, functional tumor status and Ki-67). Although mitotic index and necrosis were not specifically reported for each included patient, all tumors were classified as either typical or atypical carcinoid; therefore, the impact of the absence of mitotic index and necrosis information is limited. The absence of comorbidity information could raise questions regarding whether observed survival differences were related to differences in noncancer mortality rather than lung carcinoid tumor-specific outcomes. To mitigate the impact of this limitation, the authors evaluated both OS and CSS, as CSS is less likely to be impacted by noncancer mortality. Additionally, competing risk analysis for cancer-specific mortality was done to further limit the impact of missing comorbidity information. Likewise, nonsurgical treatment data are generally lacking within the SEER database. For example, hormonal treatments (e.g., somatostatin analogs) are not reported within the SEER database. Chemotherapy and radiation therapy are also of limited specificity with regard to type, schedule and duration. Therefore, and given these limitations, the results of this study would mainly inform association rather than causation, and further studies would be needed to confirm this observation and understand the potential biological basis of these observed differences.
Conclusion
The proportion of male patients in the current cohort was less than 50% the proportion of female patients, and the APC of the incidence of lung carcinoid tumors among female patients was higher than the APC among male patients. Moreover, female patients demonstrated better OS compared with male patients, particularly among patients with typical carcinoid tumors. Although noncancer mortality may be playing a role here, potential biological differences (and potential implications for treatment strategies) need to be explored between both groups.
•
The Surveillance, Epidemiology and End Results Research Plus database (2000–2018) was accessed, and patients with a diagnosis of typical or atypical carcinoid of the lung were reviewed.
•
Trends in age-standardized rates (per 100,000) of the incidence of lung carcinoid tumors were reviewed among male and female patients as well as the overall population, and annual percent change (APC) was determined for the three groups.
•
Multivariate Cox regression analysis was then used to assess the factors associated with overall and cancer-specific survival.
•
Among all patients, APC (2000–2018) for lung carcinoid diagnosis was 2.9 (95% CI: 2.4–3.5). Among male patients, APC (2000–2018) for lung carcinoid diagnosis was 1.8 (95% CI: 1.2–2.5). By contrast, among female patients, APC (2000–2018) for lung carcinoid diagnosis was 3.4 (95% CI: 2.8–4.1).
•
Based on Kaplan–Meier survival estimates, female sex was associated with better overall survival compared with male sex (p < 0.001). Based on multivariate Cox regression analysis, the following factors were associated with worse cancer-specific survival: older age (hazard ratio [HR]: 1.036; 95% CI: 1.031–1.041), atypical carcinoid histology (HR: 3.10; 95% CI: 2.71–3.56), stage (distant vs localized stage HR: 4.05; 95% CI: 3.48–4.71), sex (male vs female sex HR: 1.76; 95% CI: 1.56–1.99) and no surgical treatment (HR: 3.77; 95% CI: 3.22–4.42).
Financial & competing interests disclosure
O Abdel-Rahman is on the advisory boards and speaks publicly for Eisai Canada, Roche Canada, Bayer, Ipen, and Lilly Canada. N Fazio is on the advisory boards and speaks publicly for Novartis, Ipsen, Pfizer, Merck Serono, Advanced Accelerator Applications, Merck Sharp and Dohme Corporation and Sanofi-Aventis. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
As this study was based on a publicly available data set without identifying patient information, institutional review board approval was not required and informed consent was not needed.
Supplementary Material
File (supplementary tables.docx)
- Download
- 14.42 KB
References
Papers of special note have been highlighted as: • of interest
1.
Fazio N, Abdel-Rahman O, Spada F et al. RAF signaling in neuroendocrine neoplasms: from bench to bedside. Cancer Treat. Rev. 40(8), 974–979 (2014).
2.
Falconi M, Eriksson B, Kaltsas G et al. ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology 103(2), 153–171 (2016).
3.
Shah S, Gosain R, Groman A et al. Incidence and survival outcomes in patients with lung neuroendocrine neoplasms in the United States. Cancers (Basel) 13(8), 1753 (2021).
4.
Iyoda A, Azuma Y, Sano A. Neuroendocrine tumors of the lung: clinicopathological and molecular features. Surg. Today 50(12), 1578–1584 (2020).
5.
Abdel-Rahman O, Fouad M. Everolimus-based combination for the treatment of advanced gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): biological rationale and critical review of published data. Tumour Biol. 36(2), 467–478 (2015).
6.
Abdel-Rahman O, Fouad M. Bevacizumab-based combination therapy for advanced gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): a systematic review of the literature. J. Cancer Res. Clin. Oncol. 141(2), 295–305 (2015).
7.
Cook MB, McGlynn KA, Devesa SS, Freedman ND, Anderson WF. Sex disparities in cancer mortality and survival. Cancer Epidemiol. Biomarkers Prev. 20(8), 1629–1637 (2011).
8.
Abdel-Rahman O. Impact of sex on chemotherapy toxicity and efficacy among patients with metastatic colorectal cancer: pooled analysis of 5 randomized trials. Clin. Colorectal Cancer 18(2), 110–115.e112 (2019).
9.
Abdel-Rahman O, Fazio N. Sex-based differences in prognosis of patients with gastroenteropancreatic neuroendocrine neoplasms: a population-based study. Pancreas 50(5), 727–731 (2021).
• Evaluated the impact of sex on the prognosis of gastroenteropancreatic (GEP) neuroendocrine neoplasms (NENs).
10.
Hallet J, Law CH, Cukier M, Saskin R, Liu N, Singh S. Exploring the rising incidence of neuroendocrine tumors: a population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 121(4), 589–597 (2015).
11.
Yao JC, Hassan M, Phan A et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 26(18), 3063–3072 (2008).
12.
Travis WD, Brambilla E, Nicholson AG et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J. Thorac. Oncol. 10(9), 1243–1260 (2015).
13.
Surveillance, Epidemiology and End Results. www.seer.cancer.gov
14.
Goel MK, Khanna P, Kishore J. Understanding survival analysis: Kaplan–Meier estimate. Int. J. Ayurveda Res. 1(4), 274–278 (2010).
15.
Abdel-Rahman O. Validation of the 8th AJCC prognostic staging system for breast cancer in a population-based setting. Breast Cancer Res. Treat. 168(1), 269–275 (2018).
16.
Zahedi A, Bondaz L, Rajaraman M et al. Risk for thyroid cancer recurrence is higher in men than in women independent of disease stage at presentation. Thyroid 30(6), 871–877 (2020).
17.
Hernando-Cubero J, Grande E, Castellano DE et al. Impact of gender on multikinase inhibitors (MKIs) toxicity in patients (pts) with advanced pancreatic and gastrointestinal neuroendocrine tumors (NETs): a pooled analysis of two phase II trials with pazopanib and lenvatinib. J. Clin. Oncol. 37(Suppl. 15), 4109 (2019).
18.
Man D, Wu J, Shen Z, Zhu X. Prognosis of patients with neuroendocrine tumor: a SEER database analysis. Cancer Manag. Res. 10, 5629–5638 (2018).
19.
Singh S, Parulekar W, Murray N et al. Influence of sex on toxicity and treatment outcome in small-cell lung cancer. J. Clin. Oncol. 23(4), 850–856 (2005).
20.
Wheatley-Price P, Blackhall F, Lee SM et al. The influence of sex and histology on outcomes in non-small-cell lung cancer: a pooled analysis of five randomized trials. Ann. Oncol. 21(10), 2023–2028 (2010).
21.
Estrella JS, Ma LT, Milton DR et al. Expression of estrogen-induced genes and estrogen receptor β in pancreatic neuroendocrine tumors: implications for targeted therapy. Pancreas 43(7), 996–1002 (2014).
22.
Estrella JS, Broaddus RR, Mathews A et al. Progesterone receptor and PTEN expression predict survival in patients with low- and intermediate-grade pancreatic neuroendocrine tumors. Arch. Pathol. Lab. Med. 138(8), 1027–1036 (2014).
23.
Arnason T, Sapp HL, Barnes PJ, Drewniak M, Abdolell M, Rayson D. Immunohistochemical expression and prognostic value of ER, PR and HER2/neu in pancreatic and small intestinal neuroendocrine tumors. Neuroendocrinology 93(4), 249–258 (2011).
24.
Simbolo M, Barbi S, Fassan M et al. Gene expression profiling of lung atypical carcinoids and large cell neuroendocrine carcinomas identifies three transcriptomic subtypes with specific genomic alterations. J. Thorac. Oncol. 14(9), 1651–1661 (2019).
25.
Simbolo M, Mafficini A, Sikora KO et al. Lung neuroendocrine tumours: deep sequencing of the four World Health Organization histotypes reveals chromatin-remodelling genes as major players and a prognostic role for TERT, RB1, MEN1 and KMT2D. J. Pathol. 241(4), 488–500 (2017).
26.
Fernandez-Cuesta L, Peifer M, Lu X et al. Frequent mutations in chromatin-remodelling genes in pulmonary carcinoids. Nat. Commun. 5, 3518 (2014).
27.
Dong S, Liang J, Zhai W, Yu Z. Development and validation of an individualized nomogram for predicting overall survival in patients with typical lung carcinoid tumors. Am. J. Clin. Oncol. 43(9), 607–614 (2020).
28.
Abdel-Rahman O, North S. Patterns of cost-related medication underuse among Canadian adults with cancer: a cross-sectional study using survey data. CMAJ Open 9(2), e474–e481 (2021).
Information & Authors
Information
Published In
Pages: 523 - 531
PubMed: 35388711
Copyright
© 2022 Future Medicine Ltd.
History
Received: 26 August 2021
Accepted: 17 March 2022
Published online: 7 April 2022
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Sex-based differences in the outcomes of patients with lung carcinoids. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0205
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Chinonso A. Nwoguh, Marie Line El Asmar, Ayanna Gadsen-Jeffers, Rajaventhan Srirajaskanthan, Kandiah Chandrakumaran, John K. Ramage, Epidemiology of Neuroendocrine Neoplasia worldwide – A Review of the Literature (2012-2022), Neuroendocrinology, 10.1159/000548790, (1-31), (2025).
- Niraj Neupane, Sumeet K. Yadav, Elham Moases Ghaffary, Scott R. Houle, Umesh Ghimire, Binita Neupane, Sangharsha Thapa, Omid Mirmosayyeb, Zeni Kharel, Chengu Niu, Utsav Joshi, Survival and Chemotherapy Response in Metastatic Lung Carcinoids: Insights from the National Cancer Database, Hematology/Oncology and Stem Cell Therapy, 10.4103/hemoncstem.HEMONCSTEM-D-24-00001, 18, 1, (14-20), (2025).
- Stefano Partelli, Valentina Andreasi, Anna Battistella, Domenico Tamburrino, Nicolò Pecorelli, Stefano Crippa, Massimo Falconi, Gender and Age as Preoperative Predictors of Early Disease Progression in Patients Undergoing Surgery for Pancreatic Neuroendocrine Tumors with Liver Metastases, Annals of Surgical Oncology, 10.1245/s10434-025-17149-4, 32, 6, (4388-4395), (2025).
- Mohamed Mortagy, Marie Line El Asmar, Kandiah Chandrakumaran, John Ramage, Sex Differences in the Survival of Patients with Neuroendocrine Neoplasms: A Comparative Study of Two National Databases, Cancers, 10.3390/cancers16132376, 16, 13, (2376), (2024).
- Alessia Liccardi, Annamaria Colao, Roberta Modica, Gender Differences in Lung Neuroendocrine Tumors: A Single-Center Experience, Neuroendocrinology, 10.1159/000539412, 115, 5, (371-380), (2024).
- Anna La Salvia, Alessandra Siciliani, Maria Rinzivillo, Monica Verrico, Roberto Baldelli, Giulia Puliani, Roberta Modica, Isabella Zanata, Irene Persano, Giuseppe Fanciulli, Massimiliano Bassi, Massimiliano Mancini, Stefania Bellino, Elisa Giannetta, Mohsen Ibrahim, Francesco Panzuto, Maria Pia Brizzi, Antongiulio Faggiano, Thyroid transcription factor‐1 expression in lung neuroendocrine tumours: a gender-related biomarker?, Endocrine, 10.1007/s12020-023-03542-0, 83, 2, (519-526), (2023).
- Jorge Hernando, Maria Roca-Herrera, Alejandro García-Álvarez, Eric Raymond, Philippe Ruszniewski, Matthew H. Kulke, Enrique Grande, Rocío García-Carbonero, Daniel Castellano, Ramón Salazar, Toni Ibrahim, Alex Teule, Vicente Alonso, Nicola Fazio, Juan W. Valle, Salvatore Tafuto, Ana Carmona, Victor Navarro, Jaume Capdevila, Sex differences on multikinase inhibitors toxicity in patients with advanced gastroenteropancreatic neuroendocrine tumours, European Journal of Cancer, 10.1016/j.ejca.2023.04.013, 188, (39-48), (2023).
- Henning Jann, Sarah Krieg, Andreas Krieg, Johannes Eschrich, Tom Luedde, Karel Kostev, Sven Loosen, Christoph Roderburg, Analyses of sex-based clinicopathological differences among patients with gastrointestinal neuroendocrine neoplasms in Europe, Journal of Cancer Research and Clinical Oncology, 10.1007/s00432-023-04711-4, 149, 10, (7557-7563), (2023).
- Ahmet Sahin, Huseyin Melek, Birol Ocak, Sibel Orhan, Buket Erkan, Burcu Caner, Adem Deligonul, Erdem Cubukcu, Ahmet Bayram, Elif Akyildiz, Turkkan Evrensel, Platin‑based chemotherapy does not improve survival in patients with non‑metastatic resected typical carcinoid tumors, Molecular and Clinical Oncology, 10.3892/mco.2022.2579, 17, 4, (2022).