Cost–effectiveness analysis of pembrolizumab for patients with advanced esophageal cancer at PD-L1 combined positive score ≥10
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Due to the high price of pembrolizumab, it is still unknown whether the use of pembrolizumab for advanced esophageal cancer would be a cost-effective option for patients whose PD-L1 combined positive score is ≥10. Methods: A Markov simulation model was performed based on clinical trial KEYNOTE-181. Incremental cost–effectiveness ratios were calculated to compare the two treatments. Results: The total costs were US$193,575.60 and $8789.24 for pembrolizumab and chemotherapy treatment, respectively. The pembrolizumab group produced 0.93 quality-adjusted life years (QALYs), while the chemotherapy group produced 0.58 QALYs. Thus, patients in the pembrolizumab group spent an additional US$184,786.36 and produced 0.35 QALYs more than the chemotherapy group, which resulted in an incremental cost–effectiveness ratio of US$527,961.03 per QALY. Conclusion: For patients with advanced esophageal cancer whose PD-L1 combined positive score is ≥10, pembrolizumab is not a cost-effective second-line therapy versus chemotherapy from the US payer perspective.
Cancer-related death has become a great health issue in many countries and is mainly caused by rapid population growth and aging. There were 473,000 new cases of esophageal cancer (EC) and 436,000 EC-related deaths in 2017 and approximately 18,000 new cases were diagnosed in 2019 [1]. The sixth most common cause of cancer-related death worldwide is EC. Additionally, metastatic EC is a fatal disease, of which the prognosis is typically poor, with a median overall survival (OS) of less than a year. The areas with the highest prevalence of EC were Asia and Africa [2–4]. Fluoropyrimidine combined with platinum is recommended in current guidelines for first-line chemotherapy [5–7]. However, there are limited options for patients with metastatic EC after progression during first-line chemotherapy.
Anti-PD-1/PD-L1 treatments have shown significant tumor responses in patients with advanced EC [8,9]. Recently, several immune inhibitory pathway blockers, including pembrolizumab and nivolumab, targeting PD-1, as well as atezolizumab, durvalumab and avelumab, which inhibit PD-L1, have already been demonstrated to be effective and some of them have even been approved for clinical practice [10–13]. Pembrolizumab is a humanized, monoclonal anti-PD-1 antibody that has been proven to gain an obvious OS benefit with acceptable safety in patients with metastatic EC when the disease progresses during first-line therapies [14]. Recent studies have shown that pembrolizumab provides durable tumor responses in multiple tumor types [15]. The randomized phase III, open-label KEYNOTE-181 clinical trial demonstrated that pembrolizumab significantly prolonged OS and progression-free survival (PFS) versus chemotherapy for advanced EC in patients with PD-L1 combined positive score (CPS) ≥10 as second-line therapy [16].
Because pembrolizumab is expensive, it is still unknown whether the use of pembrolizumab for advanced EC would be a cost-effective option with patients whose PD-L1 CPS is ≥10. We therefore carried out this analysis to determine whether pembrolizumab was a cost-effective option from the US payer perspective.
Methods
Patients
We extracted the clinical data from the KEYNOTE-181 study. In total, 628 patients who were ≥18 years of age with histologically confirmed metastatic or locally advanced unresectable squamous cell carcinoma or adenocarcinoma of the esophagus from 154 sites in 32 countries were enrolled. A total of 314 versus 296 patients were randomly assigned to the pembrolizumab arm (PE) and chemotherapy arm (CH), respectively. There were no statistically significant differences between the two arms at baseline. The expression of PD-L1 at a CPS ≥10 was also well balanced between the two arms.
Treatment
The 314 patients in the PE group received 200 mg pembrolizumab every 3 weeks and the 296 patients in the CH group received standard chemotherapy including paclitaxel (80–100 mg/m2) on days 1, 8 and 15 of each cycle (4 weeks), docetaxel (75 mg/m2) on day 1 of each cycle (3 weeks) or irinotecan (180 mg/m2) on day 1 of each cycle (2 weeks). Patients whose PD-L1 expression was at CPS of 10 or greater were included in our analysis. Radiological examinations were performed at week 9 and every 9 weeks thereafter to assess progressive disease. The mean (standard deviation) therapeutic time was 4.0 (5.0) months versus 3.1 (2.9) months in the PE group and CH group, respectively. Treatment-related adverse events (AEs) were evaluated throughout the entire study and were graded according to the National Cancer Institute Common Terminology Criteria (version 4.0) [16].
Economic model
The decision analysis Markov model was established to assess the cost–effectiveness of pembrolizumab versus chemotherapy as second-line therapy for advanced EC from the US payer perspective. The Markov model was implemented using TreeAge Pro 2019 software (TreeAge, MA, USA) and statistical analyses were performed using R software (version 3.6.3, www.r-project.org). PFS, progressive disease (PD) and death were described as three mutually incompatible health states in the model. At the beginning, advanced EC patients with a CPS of 10 or more entered the PFS state. Patients in the PFS state can progress to the PD state or directly to death. Patients in the PD state could progress to death or stay in the same state and death was described as an absorbing state (Figure 1). The model cycle length was 1 month and the model simulation runs lasted for 10 years. Quality-adjusted life years (QALYs), incremental cost–effectiveness ratio (ICER) and total cost were the outputs of this model. ICER equals the difference in costs between the two strategic therapies divided by the difference in effects. The PE group will become cost-effective only if the ICER of the two groups was below the willingness-to-pay (WTP) threshold of US$150,000 in the US.
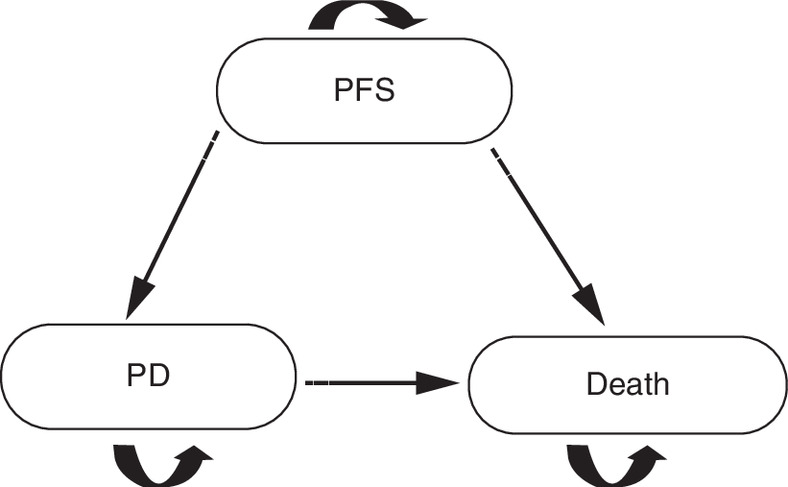
Figure 1. A Markov structure was built to compare the two treatments.
PD: Progressive disease; PFS: Progression-free survival.
We used GetData Graph Digitizer software to extract the survival curve from published OS curves from the published KEYNOTE-181 trial. Pseudoindividual patient data were generated using the algorithm derived by Hoyle and Henley, which can improve the estimation accuracy of survival time [17]. Next, 8A log-normal distribution was fitted to the OS curve in the PE group, as it provided the best fit among the exponential, log-logistic and log-normal distributions according to the Akaike information criterion, while a Weibull distribution was fitted to the CH group. We estimated the PFS curve using the same approach and log-normal distributions were fitted to both groups (Figure 2). The calculation of the time-dependent transition probability is treated in more detail in the supplement.
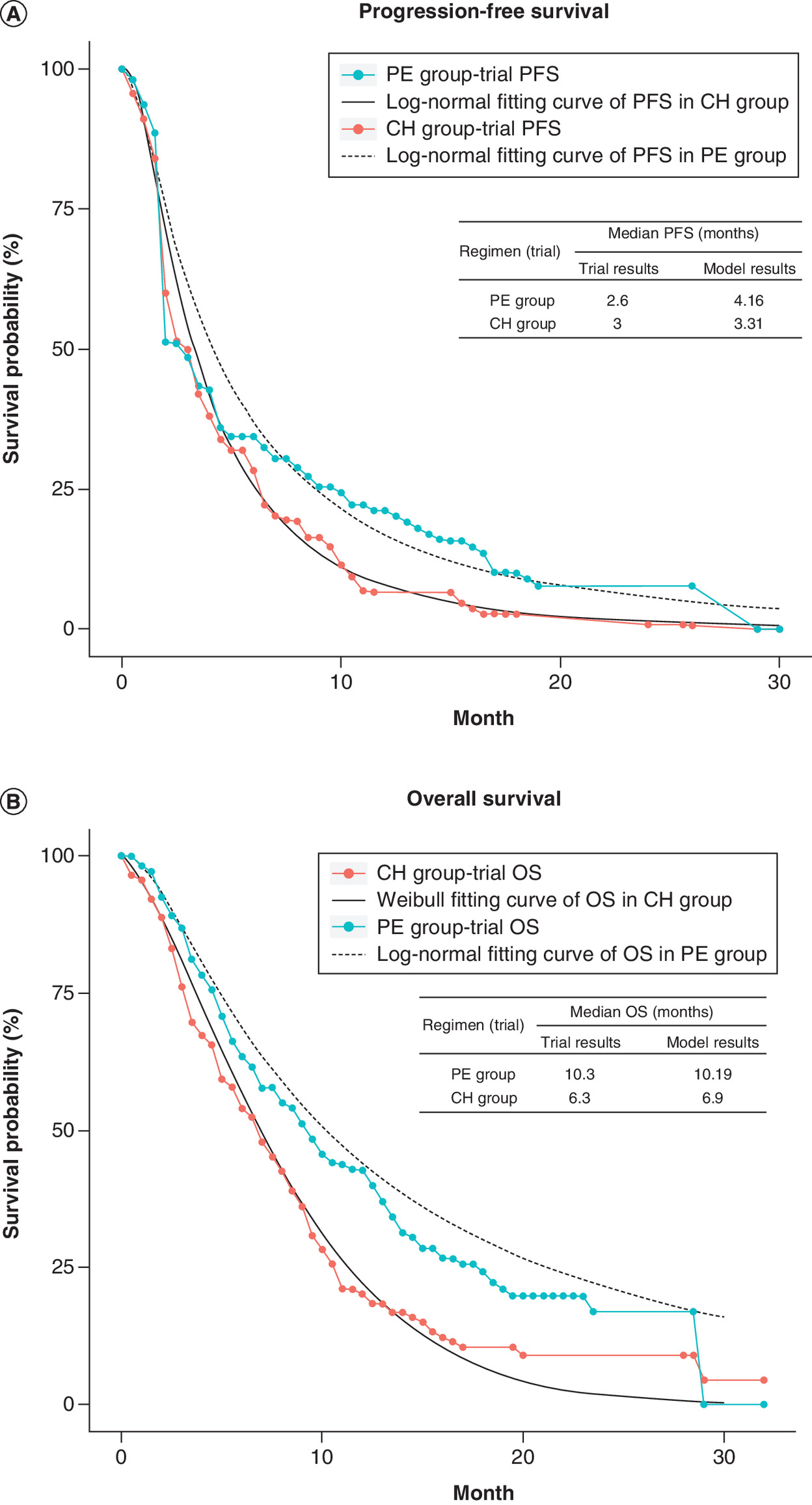
Figure 2. The original Kaplan–Meier.
(A) PFS and (B) OS curves from the KEY-NOTE181 trial. Weibull and log-normal distributions were fitted to the two groups.
CH: Chemotherapy; OS: Overall survival; PE: Pembrolizumab; PFS: Progression-free survival.
Costs & utility
Only direct costs were analysed in this study, including costs for drugs, tests (radiographic and laboratory), treatments for AEs and third-line therapy (Table 1). The prices of all the drugs were obtained on Drugs.com, 2020 [18]. In consideration of patients' geographic region in the KEYNOTE-181 study, a mean body-surface area of 1.75m2 was adopted according to published literature [19–21]. The major AEs reported in the KEYNOTE-181 study were included in our analysis. A mean cost of three different chemotherapy regimens in the CH group was adopted because the exact number of patients in each regimen was not mentioned in the KEYNOTE-181 study. All costs were measured in US dollars and a discount rate of 3% per year was adopted for both costs and outcomes [22]. Utility was applied to reflect the impact of the disease-related health states, ranging from 0 for death to 1 for the best state. Because quality-of-life data could not be obtained from the KEYNOTE-181 trial, we used utilities of 0.74 and 0.58 for the PFS and PD states, respectively, according to previously published literature [23,24].
Sensitivity analysis
One-way probabilistic sensitivity analysis was conducted to evaluate the impact of related factors in the model. To explore their impacts on ICER, input parameters were varied within a range of ±20%. Additionally, a Monte Carlo simulation with 1000 simulations with 10,000 individuals was used to assess the probabilistic sensitivity of the model. US$150,000 per QALY was set as the WTP threshold in the USA [25] (Table 1).
| Parameters | Pembrolizumab group | Chemotherapy group | Ref. |
|---|---|---|---|
| Costs per month $† | |||
| Pembrolizumab | 22,631.60 (18,105.28–27,157.92) | – | |
| Paclitaxel | – | 170.60 (136.48–204.72) | |
| Docetaxel | – | 287.30 (229.84–344.76) | |
| Irinotecan | – | 129.40 (103.52–155.28) | |
| Tests | 546 (436.80–655.20) | 546 (436.80–655.20) | [20] |
| Major AEs | 27.94 (22.35–33.53) | 316.75 (253.40–380.10) | |
| Cost of PFS | 23,205.54 (18,564.43–27,846.65) | 1058.55 (846.84–1270.26) | |
| Cost of PD | 558 (446.40–669.60) | 558 (446.40–669.60) | [31] |
| Utility | |||
| PFS | 0.74 | [23,24] | |
| PD | 0.58 | [23,24] | |
| Discount rate, % | 3 | [22] | |
†
Basis of variables, ±20% of the base-case values.
AE: Adverse event; PD: Progressive disease; PFS: Progression-free survival.
Results
Baseline analysis
The total costs were US$193,575.60 and $8,789.24 for pembrolizumab and chemotherapy treatment, respectively. The PE group produced 0.93 QALYs, while the CH group produced 0.58 QALYs. Thus, patients in the PE group spent an additional US$184,786.36 and produced 0.35 QALYs more than the CH group, which resulted in an ICER of US$527,961.03 per QALY (Table 2).
| Result | Pembrolizumab group | Chemotherapy group |
|---|---|---|
| Cost (US$) Incremental costs Effectiveness (QALYs) Incremental effectiveness ICER (US$/QALYs) | 193,575.60 184,786.36 0.93 0.35 527,961.03 | 8789.24 0.58 |
ICER: Incremental cost–effectiveness ratio; QALY: Quality-adjusted life year.
Sensitivity analyses
The one-way sensitivity analysis is displayed in Figure 3. The cost of pembrolizumab was the most sensitive parameter influencing the results, as well as the utility of PD and PFS. When the cost of pembrolizumab ranged from US$18,105.28 to $27,157.92, the ICER ranged from US$432,471.09 to $645,786.60 per QALY, which were all well above the WTP threshold of US$150,000 in the USA. Changing other parameters may somehow result in different costs and effectiveness but have little impact on the ICER. The acceptable curve shows that compared with standard chemotherapy, pembrolizumab was not a cost-effective option for patients with advanced EC with PD-L1 CPS ≥10 as second-line therapy at a WTP threshold of US$150,000 from the US payer perspective (Figure 4).
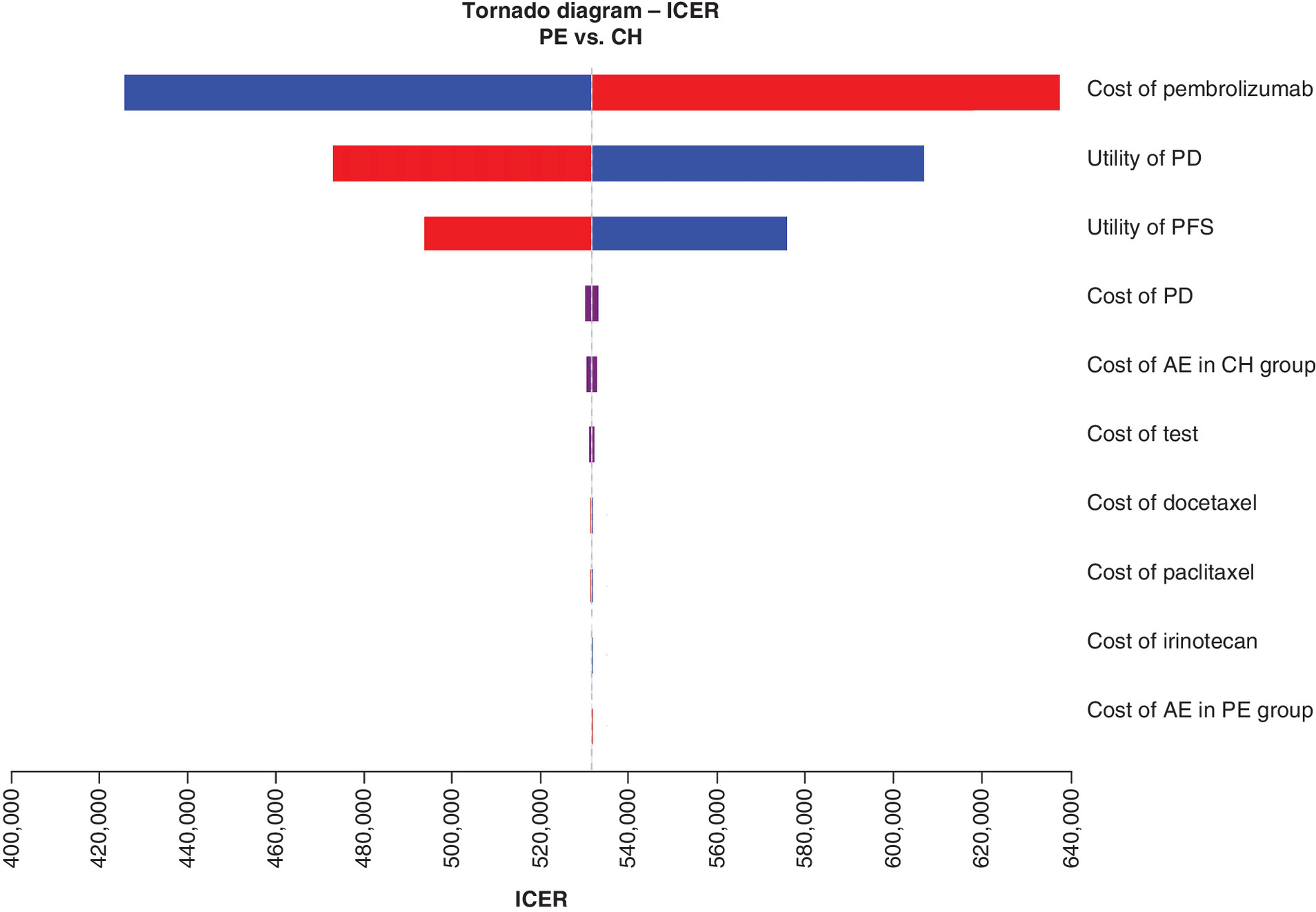
Figure 3. A one-way sensitivity analysis is shown in a tornado diagram.
The impact of each parameter on the ICER is listed.
AE: Adverse event; CH: Chemotherapy group; ICER: Incremental cost–effectiveness ratio; PD: Progressive disease; PE: Pembrolizumab group; PFS: Progression-free survival.
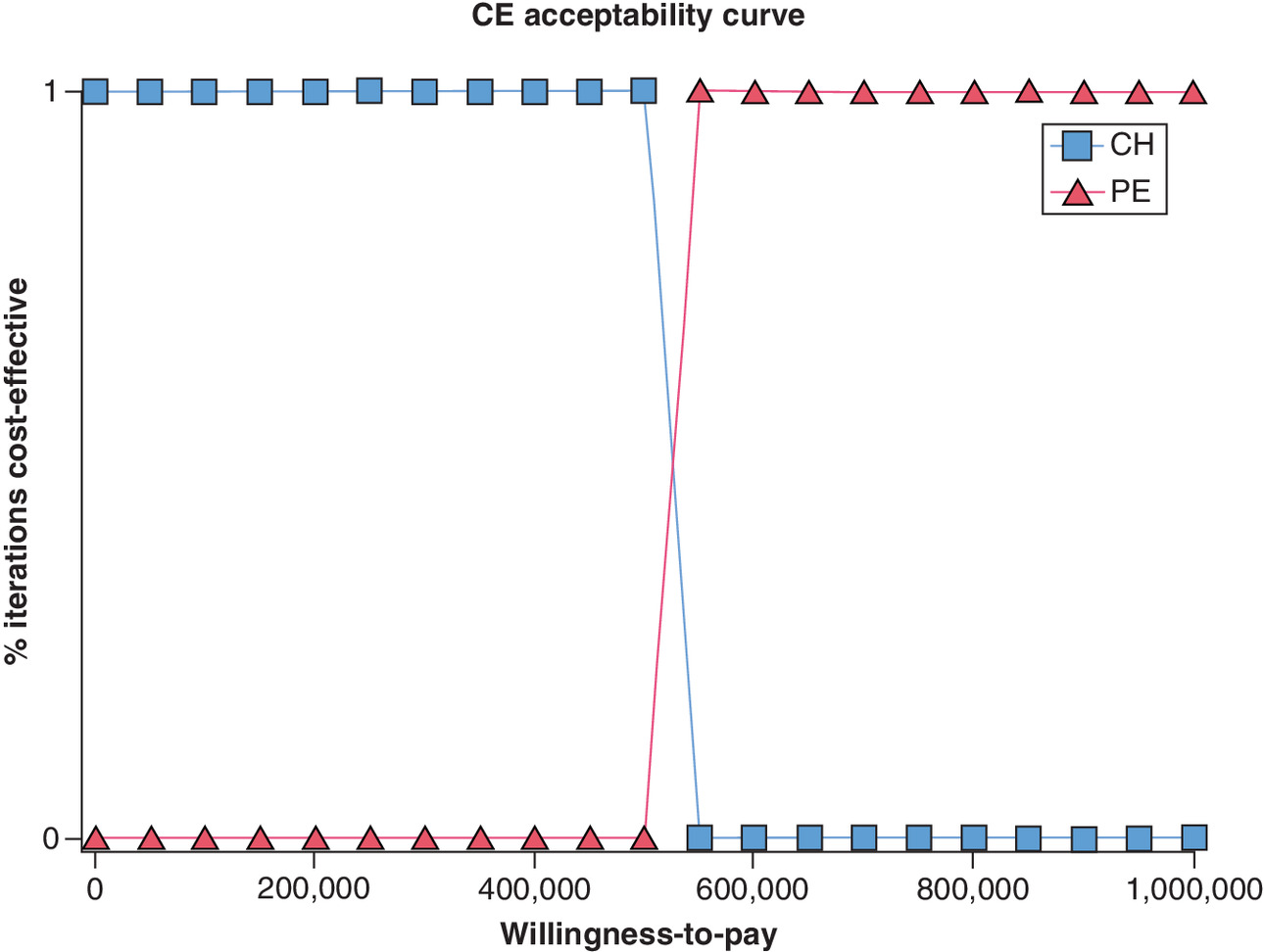
Figure 4. The acceptability curve of cost–effectiveness showed the probability at the current willingness-to-pay threshold.
CE: Cost-effective; CH: Chemotherapy group; PE: Pembrolizumab group.
Discussion
EC remains a major cause of cancer-related mortality and economic burden worldwide. Patients who progress after first-line chemotherapy still have a shortage of second-line treatment and poor prognosis. Several kinds of immune checkpoint inhibitors (ICIs) of PD-1 have shown significant effects on different types of cancers. Pembrolizumab is a highly selective humanized monoclonal antibody that can not only induce dual ligand blockade of the PD-1 protein but also inhibit the immune response [26]. The KEYNOTE-181 study reported that pembrolizumab provided a clinically meaningful PFS and OS benefit as second-line therapy compared with standard chemotherapy in patients with advanced EC whose PD-L1 CPS ≥10 [16].
According to our analysis, the ICER of the pembrolizumab group was US$527,961.03 per QALY, which was well above the current WTP of US$150,000 in the USA. Pembrolizumab will become a cost–effective option at a great reduction in pembrolizumab price. An analysis in France showed that pembrolizumab was cost–effective versus chemotherapy in the first-line therapy of patients with metastatic head and neck squamous cell carcinoma with PD-L1 expression at CPS ≥1 [27]. Similar analyses in the USA and Hong Kong showed that pembrolizumab is a cost–effective treatment when compared with platinum doublet chemotherapy as first-line treatment in non-small-cell lung cancer patients whose PD-L1 tumor proportion score was ≥50% [20,28]. A recent cost–effectiveness study showed that pembrolizumab will become cost-effective relative to chemotherapy at a price reduction of 93% or greater in patients with carcinoma in situ of the bladder, which is similar to our study [29].
Substantial progress has been made in recent years regarding ICI therapies, which provides new insights for advanced EC therapy. However, ICIs are often expensive, resulting in a significant economic burden on both patients and the health system. Therefore, our research was valuable to assess the cost-effective strategy with second-line treatment for advanced EC from a payer perspective. Despite the high cost of pembrolizumab, patients in the PE group experienced obviously lower treatment-related AEs than those in the CH group. Additionally, for patients with PD-L1 expression at CPS ≥10, the median duration of tumor response was longer in the PE group, which indicated a higher antitumor activity with pembrolizumab versus chemotherapy [16].
Nevertheless, our study has some limitations. First, our study was performed based on a published phase III trial instead of patients in the real world. Apparently, our model could not totally replicate the whole process of disease in clinical practice. For example, the dose of chemotherapy drug was calculated according to the average body surface, which varies in different individuals. Our study is focused on the analysis of patients with PD-L1 expression at CPS ≥10 and the survival data were not reported separately in patients with adenocarcinoma and squamous cell carcinoma in the KEYNOTE-181 trial. Therefore, we did not analyze the cost–effectiveness in patients with squamous cell carcinoma and patients with adenocarcinoma in the subgroup of patients with PD-L1 expression at CPS ≥10, respectively, which may lead to some bias. Second, utility scores had great influence on the results according to the sensitivity analysis. As the KEYNOTE-181 study did not publish the information, utilities applied in our study were based on the previously published literature. Additionally, subsequent treatments are not specified in the study and palliative symptomatic treatment is a recommended third-line therapy, as no drugs have been demonstrated to be effective [30]. Therefore, we assume that patients in both groups accept basic support care when the disease progresses.
Conclusion
For patients with advanced EC whose PD-L1 CPS is ≥10, pembrolizumab is not a cost-effective second-line therapy versus standard chemotherapy at the current WTP of US$150,000 from the US payer perspective.
•
Metastatic esophageal cancer (EC) is a fatal disease, of which the prognosis is typically poor, with a median overall survival (OS) of less than a year.
•
Anti-PD-1/PD-L1 treatments have shown significant tumor responses in patients with advanced EC.
•
Pembrolizumab is a humanized, monoclonal anti-PD-1 antibody that has been proven to gain an obvious OS benefit with acceptable safety in patients with metastatic EC when the disease progresses during first-line therapies.
•
The randomized phase III, open-label KEYNOTE-181 clinical trial demonstrated that pembrolizumab significantly prolonged OS and progression-free survival versus chemotherapy for advanced EC in patients with PD-L1 combined positive score (CPS) ≥10 as second-line therapy.
•
Because pembrolizumab is expensive, it is still unknown whether the use of pembrolizumab for advanced EC would be a cost-effective option with patients whose PD-L1 CPS ≥10.
•
We extracted the clinical data from the KEYNOTE-181 study and calculated the costs.
•
The decision analysis Markov model was established to assess the cost–effectiveness of pembrolizumab versus chemotherapy as second-line therapy for advanced EC from the US payer perspective.
•
Patients in the pembrolizumab group spent an additional US$184,786.36 and produced 0.35 QALYs more than the chemotherapy group, which resulted in an incremental cost–effectiveness ratio of US$527,961.03 per QALY.
•
For patients with advanced EC whose PD-L1 CPS ≥10, pembrolizumab is not a cost-effective second-line therapy versus standard chemotherapy from the US payer perspective.
Author contributions
Conception and design: X Peng, Q Xie. Development of methodology: X Peng, Q Xie. Analysis and interpretation of data: Q Xie, Y Luo.
Financial & competing interests disclosure
This work was supported by the Sichuan Province Science and Technology Support Program (grant no. 2021YFSY008) and the Technology Innovation Project of Chengdu Science and Technology Bureau (grant no. 2019-YF05-00459-SN). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (supplementary materials (9).docx)
- Download
- 13.09 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
National Cancer Institute. SEER stat fact sheet: stomach cancer (2019). https://seer.cancer.gov/statfacts/html/stomach.html
2.
Anonymous. Erratum to: Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries (CA: A Cancer Journal for Clinicians, (2018), 68, 6, (394–424), 10.3322/caac.21492). CA Cancer J. Clin. 70(4), 313 (2020).
3.
Lin Y, Totsuka Y, He Y et al. Epidemiology of esophageal cancer in Japan and China. J. Epidemiol. 23(4), 233–242 (2013).
4.
Yang S, Lin S, Li N et al. Burden, trends, and risk factors of esophageal cancer in China from 1990 to 2017: an up-to-date overview and comparison with those in Japan and South Korea. J. Hematol. Oncol. 13(1), 146 (2020).
5.
Kitagawa Y, Uno T, Oyama T et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: part 1. Esophagus 16(1), 1–24 (2019).
6.
Ajani JA, D'Amico TA, Bentrem DJ et al. Esophageal and esophagogastric junction cancers, version 2.2019, NCCN clinical practice guidelines in oncology. J. Natl Compr. Canc. Netw. 17(7), 855–883 (2019).
7.
Shah MA. Update on metastatic gastric and esophageal cancers. J. Clin. Oncol. 33(16), 1760–1769 (2015).
8.
Doi T, Piha-Paul SA, Jalal SI et al. Safety and antitumor activity of the anti-programmed death-1 antibody pembrolizumab in patients with advanced esophageal carcinoma. J. Clin. Oncol. 36(1), 61–67 (2018).
9.
Kudo T, Hamamoto Y, Kato K et al. Nivolumab treatment for oesophageal squamous-cell carcinoma: an open-label, multicentre, phase 2 trial. Lancet Oncol. 18(5), 631–639 (2017).
10.
Hellmann MD, Ciuleanu TE, Pluzanski A et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N. Engl. J. Med. 378(22), 2093–2104 (2018).
11.
Ready N, Hellmann MD, Awad MM et al. First-line nivolumab plus ipilimumab in advanced non-small-cell lung cancer (CheckMate 568): outcomes by programmed death ligand 1 and tumor mutational burden as biomarkers. J. Clin. Oncol. 37(12), 992–1000 (2019).
12.
Reck M, Rodriguez-Abreu D, Robinson AG et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375(19), 1823–1833 (2016).
13.
Nakagawa K, Yang J-H, Park K et al. Checkmate 722: a phase 3 trial of nivolumab with chemotherapy or ipilimumab vs chemotherapy in epidermal growth factor receptor (EGFR)-mutation, T790M-negative stage IV or recurrent non-small cell lung cancer (NSCLC) after EGFR tyrosine kinase inhibitor (TKI) therapy. Ann. Oncol. 27 (2016).
14.
Shah MA, Kojima T, Hochhauser D et al. Efficacy and safety of pembrolizumab for heavily pretreated patients with advanced, metastatic adenocarcinoma or squamous cell carcinoma of the esophagus: the phase 2 KEYNOTE-180 study. JAMA Oncol. 5(4), 546–550 (2019).
15.
KEYTRUDA®/TM, prescribing information. Merck, Berlin,Germany (2020). www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf
16.
Kojima T, Shah MA, Muro K et al. Randomized phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J. Clin. Oncol. (2020).
•• We obtained all the survival data from this published trial and this is the base of our study.
17.
Hoyle MW, Henley W. Improved curve fits to summary survival data: application to economic evaluation of health technologies. BMC Med. Res. Methodol. 11, 139 (2011).
• We generated pseudoindividual patient data based on the literature, which can improve the estimation accuracy of survival time.
18.
Faslodex prices, coupons and patient assistance programs (2020). www.drugs.com/price-guide/faslodex
19.
Wu Q, Zhang P, Wang X, Zhang M, Liao W, Li Q. Cost–effectiveness of capecitabine + irinotecan versus leucovorin + fluorouracil + irinotecan in the second-line treatment of metastatic colorectal cancer in China. Clin. Therapeut. 42(11), 2148–2158.e2142 (2020).
20.
She L, Hu H, Liao M et al. Cost–effectiveness analysis of pembrolizumab versus chemotherapy as first-line treatment in locally advanced or metastatic non-small cell lung cancer with PD-L1 tumor proportion score 1% or greater. Lung Cancer 138, 88–94 (2019).
21.
Fryar CD, Kruszon-Moran D, Gu Q, Ogden CL. Mean body weight, height, waist circumference, and body mass index among adults: United States, 1999–2000 through 2015–2016. Nat. Health Stat. Rep. (122), 1–16 (2018).
22.
Goldstein DA, Chen Q, Ayer T et al. First- and second-line bevacizumab in addition to chemotherapy for metastatic colorectal cancer: a United States-based cost–effectiveness analysis. J. Clin. Oncol. 33(10), 1112–1118 (2015).
23.
Adenis A, Kulkarni A, Girotto GC et al. Health-related quality of life (HRQoL) of pembrolizumab (pembro) versus physician choice single-agent paclitaxel, docetaxel, or irinotecan in subjects with advanced/metastatic adenocarcinoma (ACC) or squamous cell carcinoma (SCC) of the esophagus that has progressed after first-line standard therapy (KEYNOTE- 181). J. Clin. Oncol. 37 (2019).
• Because quality-of-life data could not be obtained from the KEYNOTE-181 trial, we obtained utilities according to the literature.
24.
Abraham P, Wang L, Jiang Z, Gricar J, Tan H, Kelly RJ. Healthcare utilization and total costs of care among patients with advanced metastatic gastric and esophageal cancer. Future Oncol. 17(3), 291–299 (2020).
• Because quality-of-life data could not be obtained from the KEYNOTE-181 trial, we obtained utilities according to the literature.
25.
Wan X, Zhang Y, Tan C, Zeng X, Peng L. First-line nivolumab plus ipilimumab vs sunitinib for metastatic renal cell carcinoma: a cost–effectiveness analysis. JAMA Oncol. 5(4), 491–496 (2019).
• The willingness-to-pay threshold in the USA adopted in our study was based on the literature.
26.
Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 12(4), 252–264 (2012).
27.
Massetti M, Even C, Geoffrois L et al. PCN81 cost-effectiveness analysis of pembrolizumab for the treatment of recurrent or metastatic head and neck squamous cell carcinoma in patients whose tumor expressed programmed death-ligand 1 at combined positive score >=1 in France. Value Health 23, S436 (2020).
28.
Loong HH, Wong CKH, Leung LKS et al. Cost–effectiveness of PD-L1-based test-and-treat strategy with pembrolizumab as the first-line treatment for metastatic NSCLC in Hong Kong. Pharmacoecon. Open 4(2), 235–247 (2020).
• Similar analyses showed that pembrolizumab is a cost-effective treatment when compared with platinum doublet chemotherapy as first-line treatment in non-small-cell lung cancer patients whose PD-L1 tumor proportion score ≥50%.
29.
Wymer KM, Sharma V, Saigal CS et al. Cost–effectiveness analysis of pembrolizumab for bcg-unresponsive carcinoma in situ of the bladder. J. Urol. 205(5), 1326–1335 (2020).
30.
Kitagawa Y, Uno T, Oyama T et al. Esophageal cancer practice guidelines 2017 edited by the Japan esophageal society: part 2. Esophagus 16(1), 25–43 (2019).
31.
Zhou K, Zhou J, Zhang M, Liao W, Li Q. Cost–effectiveness of trifluridine/tipiracil (TAS102) for heavily pretreated metastatic gastric cancer. Clin. Transl. Oncol. 22(3), 337–343 (2020).
Information & Authors
Information
Published In
Pages: 1095 - 1103
PubMed: 36043412
Copyright
© 2022 Future Medicine Ltd.
History
Received: 6 April 2022
Accepted: 8 August 2022
Published online: 31 August 2022
Keywords:
Topics
Authors
Funding Information
Sichuan Province Science and Technology Support Program: No.2021YFSY008
Technology Innovation Project of Chengdu Science and Technology Bureau: No.2019-YF05-00459-SN
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness analysis of pembrolizumab for patients with advanced esophageal cancer at PD-L1 combined positive score ≥10. (2022) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0165
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yawei Wang, Ye Hu, Yi Qin, Xiangfeng Jin, Yandong Zhao, Low Serum Interleukin-6 Levels Enhance the Efficacy of Neoadjuvant Immunotherapy in Locally Advanced Esophageal Squamous Cell Carcinoma, Cancer Biotherapy and Radiopharmaceuticals, 10.1177/10849785251360550, 40, 10, (768-777), (2025).
- Can Jiang, Kexun Zhou, Pei Shu, Cost-effectiveness analysis of pembrolizumab plus chemotherapy as first-line treatment for advanced biliary tract cancer: perspectives from US and Chinese payers, BMJ Open, 10.1136/bmjopen-2024-094047, 15, 4, (e094047), (2025).
- Shuang Liu, Linbo Zhao, Fenghao Shi, Liping Kuai, Ruizhe Liu, Jianhua Tang, Cost-effectiveness analysis of PD-1 inhibitors as second-line therapy for advanced or metastatic esophageal squamous cell carcinoma in China: an economic evaluation based on network meta-analysis, International Journal of Clinical Pharmacy, 10.1007/s11096-023-01696-5, 46, 3, (675-683), (2024).