Healthcare resource utilization and costs in pediatric pulmonary arterial hypertension in a third-level hospital in Mexico
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The objective of this study was to evaluate the healthcare costs and resource utilization of pediatric pulmonary arterial hypertension management at a third-level hospital in Mexico. Methods: A retrospective cohort study was conducted in a pediatric population with pulmonary arterial hypertension. Only direct medical costs, derived from pharmacological treatment, laboratory tests, physician visits and hospitalizations, were considered. From an institutional perspective, all costs were accounted for in 2019 US dollars. Results: A total of 82 patients were included. Of these, 55% were female and the mean age was 6.9 (standard deviation ± 4) years. The mean annual cost was $17,452.14 (standard deviation ± $38,944.10), with a median cost of $8832.75. Conclusion: Pulmonary arterial hypertension is a costly disease, with hospitalization and pharmacological treatment being areas with a higher economic burden. Functional class IV has greater resource utilization and costs.
Vascular pulmonary disease is associated with a high level of morbidity and mortality. The most recent National Institute for Health and Care Excellence clinical classification defines five main groups of pulmonary hypertension and pulmonary arterial hypertension (PAH) belonging to group 1 [1]. PAH can be idiopathic, hereditary or associated with other morbidities, such as congenital cardiac diseases, and it can begin at any age. It is a rare disease, with an estimated incidence/prevalence of two/two cases per million in children and 25/50 cases per million in adults. The pediatric registries of this disease remain scarce [2]. Children diagnosed with PAH have a median survival of 10 months if left untreated [3]. Clinical trials and registries have substantially progressed the knowledge of this disease in both adult and pediatric populations.
Despite innovative treatments, medication for PAH can be considered effective only in terms of mortality and morbidity reduction, as PAH remains an incurable disease. The main objective of treatment is improving survival and maintaining normal childhood activities without limitations. The pediatric treatment algorithm based on the last National Institute for Health and Care Excellence meeting in 2018 for PAH was modeled on the 2009 consensus regarding the adult treatment algorithm as well as current pediatric treatment experience [1]. Treatment for PAH can be classified as supportive or advanced therapy. Support therapy includes the use of diuretics, oxygen, anticoagulants, calcium channel blockers and digoxin [4]. Advanced therapies (also called specific treatment) have been developed focusing on the main routes through which PAH develops and include endothelin receptor antagonists, prostacyclin analogs, PDE 5 blockers and soluble guanylate cyclase stimulators [5]. For patients who are not stabilized with monotherapy, combination therapy is frequently employed.
Published research on management costs for pediatric patients with PAH is scarce and generally refers to comparisons between treatment alternatives; thus, there is a need for information regarding resource utilization in pediatric PAH management and evaluation of the effects of innovative treatment with regard to both patient health status and the economic impact on the health institutions where care is provided. The objective of the present study was to evaluate the healthcare costs and resource utilization of a cohort of pediatric patients with PAH treated in the third-level hospital (i.e., hospital with highly specialized staff and technical equipment) Centro Medico Nacional 20 de Noviembre (Mexico City, Mexico).
Methods
The authors conducted a retrospective cohort study in the pediatric cardiology service at the Centro Medico Nacional 20 de Noviembre, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado. Prior authorization by the local ethics and institutional health research committees classified the research as not posing any patient risk based on the ethical norms established in the Bylaw of the General Health Law Regarding Health Research.
Data collection
Data were collected through a clinical records review of all pediatric patients diagnosed with PAH (International Classification of Diseases, Tenth Revision code I270 and related) who met the following criteria: complete clinical record starting from the time of diagnosis and at least one evaluation by the pediatric cardiology service. A minimum of 80% of the clinical record data were required by the study collection format. The clinical record review was performed by two researchers independently: a clinical expert on pulmonary hypertension (H G Aguilar) to identify the case and an external researcher (S G Vázquez) to assess information quality. Once the designed collection format was completed, the quantity and quality of the collected data were evaluated for inclusion in the study. The following data were collected: demographic variables, medical history, pharmacological treatment, physician office visits, hospitalizations and laboratory tests.
Costs & resource utilization
Outpatient treatment costs were estimated directly from clinical records specifying the dosage, treatment duration and adjustments. Only direct institutional costs were considered. These were classified into four main groups: pharmacological treatment, laboratory tests, physician office visits and hospitalizations. From an institutional perspective, all costs were obtained from official sources and institutional tabulators and were accounted for in 2019 US dollars.
Statistical analysis
Demographic characteristics, costs and resource utilization were described as frequencies (%) for categorical variables and mean ± standard deviation (SD), median and range for continuous variables. A series of generalized linear models were performed with log link and gamma distribution for cost modeling. Two functional classes (FCs) were contrasted in each model, controlling for age, sex and treatment. Generalized linear models have the advantage of predicting the log of the mean, so there is no need to log-transform the data and the model enables zero costs [6]. A similar analysis was performed with regard to resource utilization through a series of generalized linear models with Poisson distribution, contrasting FCs and using the following covariates: age, sex and treatment. All analyses were performed with the programming language R 3.6.2 using an alpha level of 0.05.
Results
Sample characteristics
A total of 82 patients were identified at 5-year follow-up. The mean age was 6.9 (SD ± 4) years, 55 (55%) of the patients were female and the majority were FC-I (39%). During follow-up, two deaths were registered, both happening during the fourth year. The most frequent causes referenced were heartbeat alterations (47.5%) and cyanosis (39%) followed by dyspnea (35.3%). Most patients (87.8%) were diagnosed with PAH associated with congenital heart disease. The general characteristics of the patients are shown in Table 1.
| Characteristic | Patients (n = 82) |
|---|---|
| Age, years, mean (SD) | 6.9 (4) |
| Sex, n (%) | |
| – Female | 45 (55) |
| – Male | 37 (45) |
| City of origin, n (%) | |
| – Mexico City | 24 (29.3) |
| – Chiapas and Puebla | 12 (14.6) |
| – State of México | 10 (12.2) |
| – Other | 36 (43.9) |
| Motive for consultation, n (%) | |
| – Heartbeat alteration | 39 (47.5) |
| – Cyanosis | 32 (39.0) |
| – Dyspnea | 29 (35.3) |
| – Other | 20 (24.3) |
| PAH related to congenital heart disease, n (%) | 72 (87.8) |
| FC at baseline, n (%) | |
| – I | 32 (39) |
| – II | 26 (32) |
| – III | 16 (20) |
| – IV | 6 (7) |
| – Not specified | 2 (2) |
| Comorbidity, n (%) | |
| – Endocrine (hypothyroidism) | 8 (9.7) |
| – Digestive | 5 (6.1) |
| – Respiratory | 4 (4.9) |
| – Infection | 2 (2.4) |
| – Neurological | 2 (2.4) |
| – Other | 19 (23.2) |
| Previous treatment, n (%) | |
| – None | 53 (64.6) |
| – Diuretic | 29 (35.3) |
| – Digoxin | 11 (23.0) |
| – Captopril | 7 (8.5) |
| – Other | 9 (10.9) |
| Specific treatment at baseline, n (%) | |
| – Bosentan | 13 (15.85) |
| – Sildenafil | 11 (13.41) |
| – Sildenafil + bosentan | 9 (10.96) |
| – Other | 49 (59.76) |
FC: Functional class; SD: Standard deviation.
During the first year, nine (10.96%) patients were treated with bosentan and sildenafil, 13 (15.85%) were on only bosentan, 11 (13.41%) were treated with sildenafil and 49 (59.76%) were on unspecific treatment that could include digoxin, captopril, diuretics or acenocoumarol. By the fifth year, of the remaining 36 patients, 12 (33.33%) were on monotherapy (six with bosentan and six with sildenafil), two (5.56%) were on combination therapy and the remaining 22 (61.11%) were on nonspecific treatment. Patient outcomes were evaluated based on permanence of or improvement in functional classification in comparison with baseline classification, and it was found that 34 (41.5%) patients stayed in the same FC, 36 (46.9%) improved and ten (12.2%) deteriorated. Two patients had no initial functional classification (Table 2).
| Initial FC | Functional class of patients at the last evaluation | |||
|---|---|---|---|---|
| I | II | III | IV | |
| I (n = 32) | 23 | 7 | 0 | 2 |
| II (n = 26) | 15 | 10 | 1 | 0 |
| III (n = 16) | 5 | 11 | 0 | 0 |
| IV (n = 6) | 0 | 5 | 0 | 1 |
FC: Functional class.
Resource utilization
The authors analyzed the number of office visits, laboratory tests and hospitalization days during the first year of follow-up. A total of 87.37% of the overall cohort of patients required hospitalization, 84.4, 88.5 and 75% as FC-I, FC-II and FC-III, respectively. The highest proportion occurred within FC-IV, in which 100% (n = 6) of the patients required hospitalization. The annual mean hospitalization time was 17.59 days. FC-I patients had the greatest mean, although there was an outlier, as one patient remained hospitalized for 176 days. The median showed that FC-IV patients had more hospitalization days and required more laboratory tests. FC-I patients had the highest number of office visits (Table 3).
| Total (n = 82) | FC-I (n = 32) | FC-II (n = 26) | FC-III (n = 16) | FC-IV (n = 6) | No FC (n = 2) | |
|---|---|---|---|---|---|---|
| Office visits, n | ||||||
| – Mean (SD) | 4.32 (4.46) | 5.06†,§,¶ (4.87) | 3.42†,# (2.93) | 4.88#,§§ (6.12) | 3.50§,§§ (2.95) | 2.00¶ (1.41) |
| – Median | 3 | 3 | 2.5 | 2.5 | 3 | 2 |
| – Range | 1–24 | 1–18 | 1–13 | 1–24 | 1–9 | 1–3 |
| Tests, n | ||||||
| – Mean (SD) | 16.93 (17.91) | 18.41†,¶ (21.00) | 13.42†,#,†† (12.79) | 19.12#,¶¶ (20.99) | 20.50††,## (13.71) | 10.50¶,¶¶,## (6.36) |
| – Median | 10 | 11 | 8 | 13.50 | 20 | 10.50 |
| – Range | 1–89 | 2–83 | 1–50 | 3–89 | 4–39 | 6–15 |
| Hospitalization days, n | ||||||
| – Mean (SD) | 17.59 (29.66) | 21.12†,‡ (37.81) | 14.69†,#,††,‡‡ (28.78) | 15‡,#,¶¶ (17.72) | 17.50†† (9.75) | 19.50‡‡,¶¶ (17.68) |
| – Median | 8.5 | 10 | 5.5 | 9.5 | 17 | 19.50 |
| – Range | 0–176 | 0–176 | 0–143 | 0–64 | 6–31 | 7–32 |
†
Significant difference between groups FC-I and FC-II.
‡
Significant difference between groups FC-I and FC-III.
§
Significant difference between groups FC-I and FC-IV.
¶
Significant difference between groups FC-I and No FC.
#
Significant difference between groups FC-II and FC-III.
††
Significant difference between groups FC-II and FC-IV.
‡‡
Significant difference between groups FC-II and No FC.
§§
Significant difference between groups FC-III and FC-IV.
¶¶
Significant difference between groups FC-III and No FC.
##
Significant difference between groups FC-IV and No FC.
FC: Functional class; SD: Standard deviation.
Costs
Figure 1 shows the results with regard to inpatient stays costs, pharmacological costs and costs derived from laboratory tests and office visits. The annual mean cost for the entire cohort during the first year of follow-up was $17,452.14 (SD ± $38,944.10), with a median of $8,832.75. The annual median costs for hospitalization, pharmacological treatment, clinical tests and office visits were $3237.62, $643.20, $279.94 and $68.83, respectively.
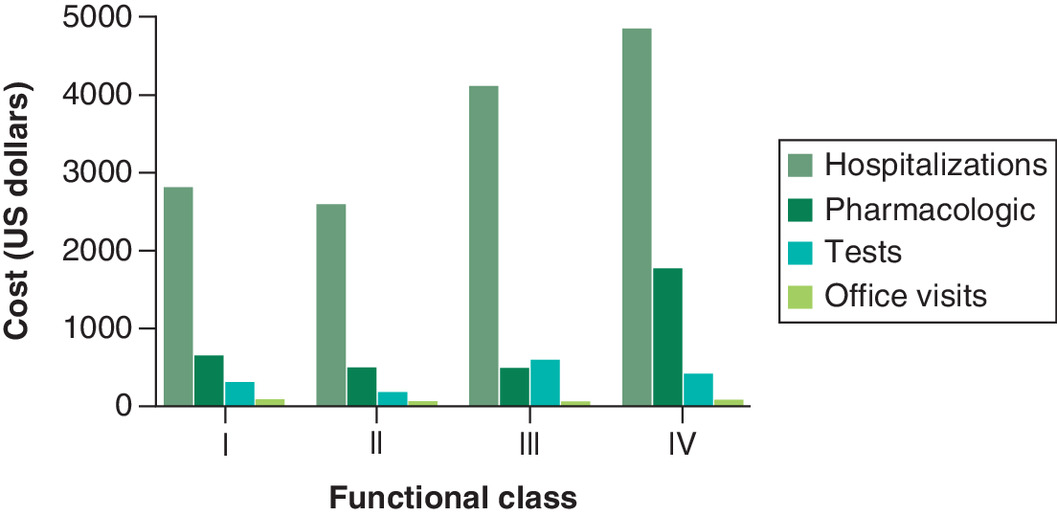
Patients had an average of 17.6 days of inpatient stays during the first year of follow-up, 80.7% of which were inpatient stays, with a unitary cost of $431.68, representing the highest proportion of spending. Because of an outlier (an FC-I patient who remained hospitalized for 176 days), the FC with the greatest hospitalization mean cost was FC-I; thus, the median provides a better description. FC-IV had a greater median cost than the other FCs. The pharmacological costs were the second highest, and FC-IV patients had the highest mean and median annual pharmacological costs (Table 4).
| Total (n = 82) | FC-I (n = 32) | FC-II (n = 26) | FC-III (n = 16) | FC-IV (n = 6) | No FC (n = 2) | |
|---|---|---|---|---|---|---|
| Mean (SD) | $17,452.14 | $23,507.27 | $15,053.01 | $11,424.13 | $14,217.18 | $9687.62 |
| ($38,944.10) | ($58,138.54) | ($22,614.31) | ($10,773.48) | ($16,678.35) | ($7783.87) | |
| – Median | $8832.75 | $9988.63 | $7608.03 | $7123.79 | $9133.77 | $9687.62 |
| – Range | $76.30–331,750.55 | $76.30–331,750.55 | $901.98–98,092.33 | $239.73–36,244.58 | $2286.11–46,887.71 | $4183.60–15,191.65 |
| Hospitalizations | ||||||
| – Mean (SD) | $10,499.08 | $16,414.28†,‡,§,¶ | $6516.22†,#,††,‡‡ | $7272.98‡,#,§§,¶¶ | $5507.14§,††,§§,## | $8417.82¶,‡‡,¶¶,## |
| ($36,242.38) | ($56,577.03) | ($12,382.64) | ($9403.94) | ($4237.13) | ($7631.15) | |
| – Median | $3237.62 | $2805.94 | $2590.10 | $4100.99 | $4848.63 | $8417.82 |
| – Range | $0.00–320,703.37 | $0.00–320,703.37 | $0.00–61,730.67 | $0.00–28,004.38 | $1262.11–11,722.19 | $3021.78–13,813.86 |
| Pharmacological | ||||||
| – Mean (SD) | $6219.19 | $6239.32†,‡,§,¶ | $8079.05†,#,††,‡‡ | $3079.31‡,#,§§,¶¶ | $8184.13§,††,§§,## | $943.33¶,‡‡,¶¶,## |
| ($11,917.96) | ($11,296.96) | ($14,586.52) | ($5593.42) | ($16,934.01) | ($69.47) | |
| – Median | $643.20 | $643.20 | $495.02 | $490.02 | $1761.57 | $943.33 |
| – Range | $0.00–62,622.74 | $0.00–42,487.71 | $14.94–62,622.74 | $0.00–20,452.66 | $132.04–42,690.33 | $894.21–992.46 |
| Tests | ||||||
| – Mean (SD) | $629.03 | $728.99† | $379.21†,# | $950.62# | $437.04 | $280.58 |
| ($1077.16) | ($1077.51) | ($365.36) | ($1826.89) | ($314.19) | ($189.74) | |
| – Median | $279.94 | $304.38 | $178.74 | $593.67 | $411.06 | $280.58 |
| – Range | $30.41–7,703.98 | $30.41–4,831.54 | $57.04–1,343.66 | $54.58–7,703.98 | $74.69–913.15 | $146.42–414.75 |
| Office visits | ||||||
| – Mean (SD) | $104.84 | $124.69†,§ | $78.53† | $121.22 | $88.88§ | $45.89 |
| ($111.98) | ($127.08) | ($69.92) | ($143.96) | ($86.73) | ($32.45) | |
| – Median | $68.83 | $74.01 | $55.37 | $58.61 | $68.83 | $45.89 |
| – Range | $22.94–529.78 | $22.94–524.79 | $22.94–298.27 | $22.94–529.78 | $22.94–256.92 | $22.94–68.83 |
All costs are in 2019 US dollars.
†
Significant difference between groups FC-I and FC-II.
‡
Significant difference between groups FC-I and FC-III.
§
Significant difference between groups FC-I and FC-IV.
¶
Significant difference between groups FC-I and No FC.
#
Significant difference between groups FC-II and FC-III.
††
Significant difference between groups FC-II and FC-IV.
‡‡
Significant difference between groups FC-II and No FC.
§§
Significant difference between groups FC-III and FC-IV.
¶¶
Significant difference between groups FC-III and No FC.
##
Significant difference between groups FC-IV and No FC.
FC: Functional class; SD: Standard deviation.
Total costs decreased by the second year, with a reduction in average inpatient stays from 17.6 days the first year to 4.3 days the second. The average total cost also decreased from $17,452.16 the first year to $9,333.48 by year five of follow-up (Table 5). This might be a consequence of health improvements in the patients; however, the authors do not have information regarding FCs from years two through five, so this cannot be proved.
| Year 1 (n = 82) | Year 2 (n = 81) | Year 3 (n = 67) | Year 4 (n = 57) | Year 5 (n = 36) | |
|---|---|---|---|---|---|
| Total costs | |||||
| – Mean (SD) | $17,452.16 ($38,944.13) | $9134.85 ($12,984.08) | $8946.13 ($13,567.47) | $7670.22 ($11,981.53) | $9333.48 ($13,498.12) |
| – Median | $8832.75 | $2838.37 | $2201.91 | $1857.43 | $1934.59 |
| – Range | $76.30–331,750.83 | $22.94–52,267.96 | $43.07–49,917.88 | $0.39–55,513.88 | $74.27–63,084.88 |
SD: Standard deviation.
Discussion
This study is a real-world evidence report. The clinical data and resources used by each patient were obtained from clinical files. Statistical analysis was performed using generalized linear models, contrasting FCs with the covariates age, sex and treatment.
The relevance of the present study must be considered, as to the best of the authors' knowledge, this is the first cost analysis of a Mexican pediatric population. The authors' findings regarding costs are difficult to compare with other studies because of the pediatric population and the differences among institutions in the Mexican public health system.
The results of this study show that hospitalization represents the biggest proportion of costs, which is also the case for adult populations with PAH [7]. This is due to the high unitary cost and the fact that patients require hospitalization several days a year, at an annual median cost of $3237.62. Pharmacological treatment represents the second highest cost. FC-IV patients required more hospitalizations and laboratory studies and had greater pharmacological treatment costs, comparable to an adult population. This shows the importance of treatments that improve FC and hospitalization risk.
There are innovative medications that may increase costs but have shown efficacy and safety in pediatric populations with PAH. For example, bosentan has proven efficacy and safety in two randomized, double-blind, placebo-controlled trials in pediatric populations [8]. These studies demonstrated statistically significant improvements (p < 0.05) compared with placebo at weeks 12 and 16 in a 6-min walk test, a standardized test that measures the distance a patient can walk briskly across a flat surface in an average of 6 min. The studies further showed that bosentan reduces the time to clinical worsening, a complex endpoint that includes death, lung transplant, PAH-related hospitalization, PAH worsening that leads to discontinuation and need for intravenous prostaglandins or atrial septostomy [9]. The arrival of macitentan has shown positive impacts on morbidity and mortality in adult populations and could be a promising treatment in children.
Current treatment guidelines and consensus documents recommend combined therapy in patients no longer responding to monotherapy. As the pathogenesis of PAH is both complex and multifactorial, it is unlikely that treatment via one pathogenic pathway will be sufficiently effective. Currently, the available data support the additional beneficial effects of combination therapy on morbidity in PAH, but the beneficial effects on mortality have yet to be proven. As combination therapy improves 6-min walk test scores, an established predictor of mortality in PAH [10], there are reasons to believe that the benefits in mortality are on their way to being confirmed conclusively. Patients on progressively more intensive combination therapy had a higher burden of the disease but had better clinical outcomes than resource use containment. This problem was managed to have expert opinions on the clinical management of PAH.
One limitation of this study is the number of patients, which resulted in a small sample when divided by FC, leading to nonrepresentative results. In addition, only data regarding the initial and final FCs were available, and some patients left the study during the 5-year follow-up, so the authors cannot prove the cause of the decreasing costs after the second year.
In the future, larger prospective studies will be required. The authors' sample included only patients receiving treatment via a specialized center that can provide the three lines of pharmacotherapy for PAH, a reality that does not apply to the rest of the country. Therefore, the authors cannot assume that the results of this study reflect the national state of pediatric PAH management.
Conclusion
The present study estimated the costs and resource utilization of a sample of Mexican pediatric patients with PAH at Centro Medico Nacional 20 de Noviembre. The mean annual cost during the first year of the study was estimated at $17,452.14 (SD ± $38,944.10), with a median of $8832.75. Hospitalization and pharmacological treatment had the highest costs, and the economic burden increased with the progression of the disease. In general, FC-IV patients had greater resource utilization and costs. Early treatment of PAH would result in economic benefits for Mexican public health institutions.
•
Pulmonary hypertension in children is associated with many diseases and can develop at any age. The causes of pulmonary hypertension in children are completely different from those in adults.
•
The methodology was conducted using a retrospective cohort study in a pediatric population with pulmonary arterial hypertension.
•
The study estimated the costs and resource utilization of a sample of pediatric patients with pulmonary arterial hypertension at Centro Medico Nacional 20 de Noviembre in Mexico City, Mexico.
•
Hospitalization and pharmacological treatment were the areas with the highest costs.
Acknowledgments
The authors would like to thank MMM Aguilar for her support.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Rosenzweig EB, Abman SH, Adatia I et al. Paediatric pulmonary arterial hypertension: updates on definition, classification, diagnostics, and management. Eur. Respir. J. 53(1), 1801916 (2019).
•• Provides updates regarding the current definition, epidemiology, classification, diagnostics and treatment of pediatric pulmonary arterial hypertension (PAH) and identifies critical knowledge gaps, which are important for understanding the background of PAH.
2.
Berger RMF, Beghetti M, Humpl T et al. Clinical features of pediatric pulmonary hypertension: a registry study. Lancet 379(9815), 537–546 (2012).
3.
Arafuri N, Murni IK, Idris NS et al. Survival of left-to-right shunt repair in children with pulmonary arterial hypertension at a tertiary hospital in a low-to-middle-income country. Glob. Heart 16(1), 25 (2021).
4.
Roofthooft MTR, van Loon RLE, Berger RMF. Management of pulmonary arterial hypertension in children. Paediatr. Respir. Rev. 11(4), 240–245 (2010).
•• Discusses the new anti-PAH drugs and the available data on their use in pediatric PAH.
5.
Ivy DD, Abman SH, Barst RJ et al. Pediatric pulmonary hypertension. J. Am. Coll. Cardiol. 62(Suppl. 25), D117–D126 (2013).
6.
Glick HA, Doshi JA, Sonnad SS, Polsky D. Economic Evaluation in Clinical Trials. Second Edition. Oxford University Press, Oxford, UK (2015).
7.
Dufour R, Pruett J, Hu N et al. Healthcare resource utilization and costs for patients with pulmonary arterial hypertension: real-world documentation of functional class. J. Med. Econ. 20(11), 1178–1186 (2017).
8.
Avitabile CM, Vorhies EE, Ivy DD. Drug treatment of pulmonary hypertension in children. Pediatr. Drugs 22(2), 123–147 (2020).
9.
Stevenson MD, MacDonald FC, Langley J, Hunsche E, Akehurst R. The cost–effectiveness of bosentan in the United Kingdom for patients with pulmonary arterial hypertension of WHO functional class III. Value Health 12(8), 1100–1105 (2009).
• Assesses whether bosentan or no active intervention, in addition to palliative care, is the more cost-effective first-line treatment option for patients with idiopathic PAH in the UK and provides important background on the use of bosentan.
10.
Small M, Piercy J, Pike J, Cerulli A. Incremental burden of disease in patients diagnosed with pulmonary arterial hypertension receiving monotherapy and combination vasodilator therapy. Adv. Ther. 31(2), 168–179 (2014).
Information & Authors
Information
Published In
Pages: 1251 - 1257
PubMed: 34585624
Copyright
© 2021 Future Medicine Ltd.
History
Received: 2 June 2021
Accepted: 26 August 2021
Published online: 29 September 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Healthcare resource utilization and costs in pediatric pulmonary arterial hypertension in a third-level hospital in Mexico. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0128
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Arturo Cortes-Telles, Yuliana Valeria Priego-Escamilla, Diana Lizbeth Ortíz-Farias, Saúl Vázquez-López, Yuri Noemí Pou-Aguilar, Esperanza Figueroa-Hurtado, Sequential Add-On Therapy Modifies Mortality Risk Stratification in Group 1.4 Pulmonary Arterial Hypertension: A Real-World, Single-Center Retrospective Cohort Study from Mexico, Journal of Clinical Medicine, 10.3390/jcm15134924, 15, 13, (4924), (2026).
- Mauricio Orozco-Levi, Rogerio Souza, Ignacio M Bluro, Julia Harley, Jose Luis Hernández Oropeza, Adrian Lescano, Gisela Meyer, Tatiana Pineda, Alicia Ramirez, Mark Small, Angelo Valencia, Tomás Pulido, Pathway to care, treatment and disease burden of pulmonary arterial hypertension: a real-world survey of physicians and patients in Latin America, BMJ Open, 10.1136/bmjopen-2024-087263, 14, 12, (e087263), (2024).