Cost-minimization analysis of teledermatology versus conventional care in the Brazilian National Health System
Publication: Journal of Comparative Effectiveness Research
Abstract
Aims: Cost-minimization analysis (CMA) comparing the teledermatology service of the State of Santa Catarina, Brazil with the provision of conventional care, from the societal perspective. Patients & methods: All costs related to direct patient care were considered in calculation of outpatient costs. The evaluation was performed using the parameters avoided referrals and profile of hospitalizations. The economic analysis was developed through a decision tree. Results: Totally, 40% of 79,411 tests performed could be managed in primary care, avoiding commuting and expanding the patients’ access. The CMA showed the teledermatology service had a cost per patient of US$196.04, and the conventional care of US$245.66. Conclusion: In this scenario, teledermatology proved to be a cost-saving alternative to conventional care, reducing commuting costs.
Lay abstract
Diagnosis and treatment of skin diseases through teledermatology avoid patient referrals, improves accessibility to specialized care, as well as the skin care provided by physicians. This study compared the costs of the teledermatology service of the State of Santa Catarina, Brazil with the costs of the provision of conventional care, to check which of them was more efficient. All costs related to direct patient care were considered in the calculation of costs. Totally, 40% of 79,411 dermatological tests performed could be locally managed in primary care, avoiding commuting, and expanding the patients’ access to care. The teledermatology service had a cost per patient of US$196.04, compared with the cost of conventional care of US$245.66. In this evaluation, teledermatology proved to be cheaper than conventional care, reducing commuting costs.
Background
Teledermatology has been constantly expanding in global health systems. The development of technological advances combined with the increased demand for dermatological care have led to the implementation and growth of this area. Teledermatology services have become a reliable and cost-effective access alternative for populations in need of dermatological care [1]. A literature review focusing on diagnosis and treatment of skin diseases through teledermatology confirmed the effectiveness of this alternative to improve accessibility to specialized care, as well as in diagnostic and therapeutic agreement, and in skin care provided by physicians, while reducing costs [2,3]. What makes it attractive is the optimization of care processes, resulting in more efficient use of resources, both financial and human [4]. The exchange of information about a patient between a nondermatologist and a dermatologist found good diagnostic efficiency and accuracy, with reduced costs and improved quality of life for patients [5]. On the other hand, a systematic review of economic evaluations focusing on telemedicine confirmed that it is cost–effective for applying in major medical fields, but in dermatology, studies could not confirm the positive capability of telemedicine. The authors pointed out that the evidence they analyzed was inconsistent, across a wide range of fields [6]. Nevertheless, the limited literature evaluating the economic consequences of teledermatology suggests that teledermatology may be cost–effective [7].
Brazil is a country of continental dimensions, and telehealth is a necessity and a solution for the integration of assistance networks, as well as for the coordination among the levels of care in the Brazilian National Health System (known by its acronym SUS). An integrated health system shows better results in terms of quality and efficiency [8]. The Telehealth Center of the State of Santa Catarina (TCSC) is one of the centers of the Brazilian Telehealth Program, an initiative of the Ministry of Health. Developed by the Federal University of Santa Catarina, in partnership with local government secretariat and municipalities, the TCSC telemedicine service aims to offer citizens better access to medical examinations, including dermatological, through a technological infrastructure that supports the performance of these examinations in the municipalities and their subsequent submission to the TCSC, meeting the needs of local professionals and strengthening primary care and the SUS [9]. A cost-minimization analysis (CMA) was conducted with 79,411 patients referred to the TCSC teledermatology service, in Santa Catarina State, Brazil, between January 1st, 2016 and December 31st, 2018. A decision tree model was performed to compare the cost of managing patients’ care in this teledermatology service versus the cost for the provision of conventional care. The economic analysis was carried out from the societal perspective.
Methods
The TCSC system
The system adopted by the teledermatology service is store-and-forward (asynchronous). Images are captured by dermatoscopes and digital cameras at the primary care level, stored and sent to dermatologists for analysis and diagnostic report. The exams received are classified using a color system, according to severity and need for intervention [9]. White is the least severe and does not require intervention by the primary care physician. Blue means low risk and no need for referral, amenable to treatment at primary care and the dermatologist suggests the management to the attending physician. Exams classified as green require referral to secondary care, and yellow, more severe cases, are referred to tertiary care.
Data collection
The CMA compared the teledermatology service with the provision of conventional care, for the period January 2016 to December 2018. The analysis was carried out from the societal perspective. To this end, an unidentified database was used containing the following information for each patient: date of the report, sex, date of birth, municipality of origin, municipality of reference in SUS, diagnosis of the report and risk classification. Additionally, hospital admissions in Santa Catarina were identified, whose dermatological diagnoses were similar to those reported as a yellow classification. Hospitalizations and days of stay were collected in the hospital information system (SIH, acronym in Portuguese) of SUS, from 2013 to 2018.
Ethical aspects and confidentiality were strictly safeguarded, insofar as the data from a secondary source were not identified, access to them remained restricted to researchers, and results were presented exclusively in an aggregated manner. The principles outlined in the Declaration of Helsinki have been followed.
Estimation of costs
The measurement of outpatient costs included all costs related to direct patient care (primary and secondary care), in addition to the cost of commuting to the reference municipality, and the opportunity cost of the patient and companion. Maintenance costs of the teledermatology service (equipment, infrastructure, imaging storage, dermatologists, secretary, patient support and communication) were also considered.
To calculate the number of hours spent by the patient (and companion, when appropriate) for outpatient treatment outside the city of residence, the following were considered:
i.
The average speed of 60 km/h, to calculate travel time between cities.
ii.
Four-hour stay in the city where the service is available.
iii.
One overnight stay when the commuting time added to the length of stay was ≥9 h.
iv.
Percentage of patients with a companion (27%).
The costs related to the patient’s outpatient care are described in Table 1.
| Category | Parameter | Description | Source | Value (US$) |
|---|---|---|---|---|
| Primary care medical consultation | Value of consultation | 1/3 of payment for medical services in the public sector per hour | RAIS/MTE | 15.19 |
| Dermatology medical consultation | Dermatology consultation fee | 1/3 of payment for medical services in the public sector per hour | RAIS/MTE | 19.93 |
| Per diem without overnight stay for the patient (or companion) | Food expenses | Daily remuneration value without overnight stay | SIGTAP – codes 08.03.01.002.8 or 08.03.01.005.2 | 4.11 |
| Per diem with overnight stay for the patient (or companion) | Food and accommodation expenses | Daily remuneration value with overnight stay | SIGTAP – codes 08.03.01.001.0 or 08.03.01.004.4 | 12.11 |
| Patient opportunity cost | Patient hours | Number of hours spent by the patient to undergo the procedure | Estimated from the patient’s place of residence | N/A |
| Patient opportunity cost | Hourly wage | Hourly income based on per capita nominal monthly family income in Santa Catarina | IBGE 2018 | 5.08 [812.13/month] |
| Companion opportunity cost | Companion hours | Number of hours spent by companion of patient undergoing a procedure | Estimated from the patient's place of residence | N/A |
| Companion opportunity cost | Hourly wage | Hourly income based on per capita nominal monthly family income in Santa Catarina | IBGE 2018 | 5.08 [812.13/month] |
| Salary – an hour of the driver | Hourly wage amount | Usual average real income from the main job of persons aged 14 years and over, employed in the week of reference in formal jobs in Santa Catarina | IBGE 2018 | 7.43 [1189.33/month] |
| Driver working hours | Driver hours per patient | 1/3 of the number of hours spent by the driver to make a trip (considering three people transported on average, per trip) | Estimated from the total travel period | N/A |
| Remuneration unit for the patient and/or companion travel by land transport | Spending on the patient and/or companion travel | Mileage compensation amount between cities (per km driven) | CREA/SC | 0.46 |
CREA/SC: Conselho Regional de Engenharia e Agronomia/Santa Catarina (Regional Council of Engineering and Agronomy of Santa Catarina; https://portal.crea-sc.org.br); IBGE: Instituto Brasileiro de Geografia e Estatistica (Brazilian Institute of Geography and Statistics; https://cidades.ibge.gov.br/brasil/sc/panorama); N/A: Not applicable; PPP: Purchasing power parity, expressed in US dollars – 1 PPP dollar = R$2.044 (2018); RAIS/MTE: Relação Anual de Informações Sociais/Ministério do Trabalho e Emprego (Annual List of Social Information/Ministry for Labor and Employment; http://trabalho.gov.br/rais); SIGTAP/SUS: Sistema de Gerenciamento da Tabela Unificada de Procedimentos/Sistema Único de Saúde (SUS’s System of Management of the Table of Procedures, Medications, Orthotics, Prosthetics and Special Materials; http://sigtap.datasus.gov.br).
Hospital costs were obtained from SIH/SUS, and the recorded values during the hospitalization period were collected. In addition to hospitalization costs, the following were considered:
i.
Travel costs with a calculation similar to that of outpatient care.
ii.
Two nights with an overnight stay for a companion, if the hospital stay exceeded 24 h.
iii.
The opportunity cost of the patient, corresponding to the number of days of hospitalization.
iv.
Companion’s opportunity cost, when their stay in the hospital was registered at the SIH. Patients admitted to the municipality where they lived did not add travel costs.
All costs were adjusted to December 2018 based on the Extended National Consumer Price Index (IPCA-IBGE) and converted to the US dollar adjusted by purchasing power parities (PPP) for the 2018 calendar year. It is worth pointing out that many of the estimated costs were extrapolated from government databases and may not fully match the real costs.
Effectiveness
There is evidence that the effectiveness of the alternatives teledermatology or conventional care is similar [10] and corresponds to the patient seen at any level of care.
The following assumptions were adopted in the model:
i.
Secondary care dermatologists have the same clinical management capacity as telediagnosis experts [10–13].
ii.
The costs of maintaining care network are similar in both alternatives. However, the maintenance costs of the teledermatology service were added to this alternative.
Teledermatology service was considered fully implemented as of 2016. Thus, hospitalizations in the 2013–2015 triennium corresponded to the conventional alternative and those in the 2016–2018 triennium to the teledermatology alternative. For modeling, the proportional distribution of diagnoses in the two trienniums was considered.
Model development
The CMA was developed through a decision tree model, considering the transition possibilities for the alternatives teledermatology or conventional care (Figure 1). Teledermatology care can result in the resolution of cases with no need for referral. When a referral is required, it can be to secondary or tertiary care, depending on the complexity of the case. In conventional care, patients are always referred to secondary care, where they are seen or referred to tertiary care. For modeling, the proportional distribution of diagnoses of hospitalization in the two trienniums was considered.
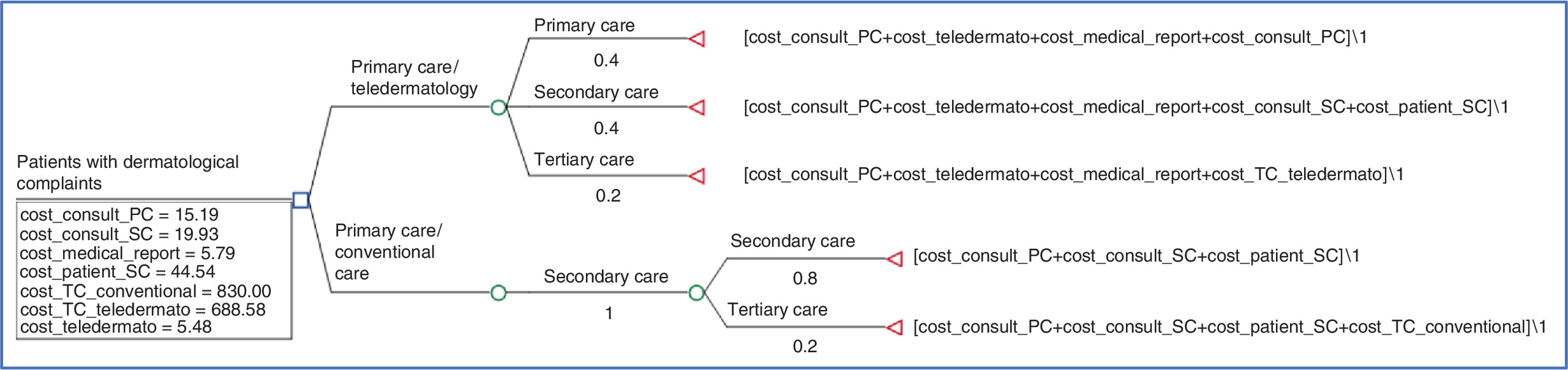
Figure 1. Decision tree with the parameters used for cost-minimization analysis.
Consult: Medical consultation; PC: Primary care; SC: Secondary care; TC: Tertiary care.
Data analysis
We calculated the frequency distributions for the categorical variables; and means, standard deviation and medians for the continuous variables. Trends over time in hospitalization with the selected diagnoses were examined. The difference in costs between trienniums was calculated using the Mann–Whitney test, as the data were not normally distributed, according to the Kolmogorov–Smirnov test. The decision-tree model consists of a hypothetical cohort of individuals who seek primary care with a complaint of dermatological problems. When patients are seen in a service with teledermatology, clinicians may consult this service. Based on the data available, the model predicts that, of the patients seen in primary care, 20% are referred to tertiary care, 40% to secondary care and 40% remain in primary care. When treated in a conventional service, 100% of patients are referred to secondary care and, after being seen by a specialist, 20% are referred to tertiary care and the rest remain in secondary care. Figure 1 shows the decision tree with the parameters used for CMA, comparing the alternative teledermatology with conventional care. The mean value of hospitalization, including travel and opportunity costs, was the parameter used in the decision tree for tertiary care in each period. All analyses were conducted using TreeAge® Pro Healthcare software version 2020R1.2 (MA, USA).
Sensitivity analysis
A univariate deterministic sensitivity analysis assessed the model’s uncertainties and identified which variables most impacted the results obtained in terms of incremental costs. The sensitivity analysis by the Tornado diagram was performed varying the estimates of costs. The values related to medical consultation, medical report and teledermatology cost were varied by 20% more and less. We used the minimum and maximum values of patient’s outpatient care and the costs of tertiary care were varying according to the lower and upper CIs of costs.
We performed an additional sensitivity analysis in order to assess the impact of the cost of hospitalizations on the total cost, in the teledermatology period (2016–2018). The objective was to evaluate whether the reduction in the cost of hospitalizations for this period is driving the findings of an overall cost reduction for the teledermatology. Thus, we perform this sensitivity analysis using a 20% increase in the cost of hospitalization in the teledermatology arm.
Results
During the period, 79,411 exams were performed at the teledermatology service; in that, 29.2% in 2016, 28.9% in 2017 and 42.0% in 2018. Most patients were female (63.7%), with a mean age of 50.4 (±20) years.
There was an increase of 43.8% in the examinations performed by the teledermatology service, from 2016 to 2018. In 2016, 9737 patients were classified in the categories white and blue, and this number increased to 13,179 in 2018. Between the years 2016 and 2018, 40.2% of exams were classified as a white or blue risk category, 40.0% as green and 19.8% as yellow. There were no significant differences in the distribution of categories between the years observed. Of the 15,693 exams classified as yellow and referred to tertiary care, 75.2% were suspected of having nonmelanoma skin cancer, 8.6% moderate-to-severe psoriasis, and 6.6% melanoma skin cancers.
In the 2013–2015 triennium, there were 7597 hospitalizations due to any of the selected dermatological diagnoses. In the 2016–2018 triennium, this figure rose to 10,751 hospitalizations. There was a decrease in the mean number of days spent at the hospital, which fell from 3.71 days in the first 3 years to 1.92 days in the second triennium (p < 0.001).
Cost measurement
Table 2 presents the values of patients commuting to outpatient care, considering 79,411 exams performed by the teledermatology service, between January 2016 and December 2018.
| Variables | Mean | Standard deviation | Minimum | Maximum |
|---|---|---|---|---|
| Travel and stay time (days) | 2.58 | 0.80 | 1.96 | 5.45 |
| Cost of patient travel (PPP US$) (a) | 14.81 | 19.00 | 0.00 | 83.21 |
| Patient opportunity cost (PPP US$) (b) | 26.76 | 8.27 | 20.31 | 56.54 |
| Daily cost (PPP US$) (c) | 2.47 | 2.79 | 0.00 | 12.11 |
| Companion cost (PPP US$) (d) | 11.89 | 7.80 | 0.00 | 41.00 |
| Total cost (a + b + c + d)† | 44.54 | 29.97 | 20.31 | 156.33 |
†
Total cost in PPP expressed in US dollars Exchange rate: 1 PPP dollar = R$ 2.044 (2018).
PPP: Purchasing Power Parity.
Table 3 shows the mean and median values, in PPP expressed in US dollars, of hospitalizations that occurred in the 2013–2015 and 2016–2018 3-year periods, including travel and opportunity costs. The mean values of hospitalization, in PPP expressed in US dollars, decreased in the second triennium (688.58 ± 910.85) when compared with the first triennium (830.00 ± 886.36). Accordingly, the median values also decreased from the first to the second triennium (p < 0.001).
| Period | n | Mean | Standard deviation | 95% CI | Median‡ | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||||
| 2013–15 | 7597 | 830.00 | 886.36 | 810.07 | 849.93 | 469.76 | 32.32 | 20,802.27 |
| 2016–18 | 10751 | 688.58 | 910.85 | 671.36 | 705.80 | 364.33 | 30.46 | 31,335.14 |
| Total | 18348 | 747.14 | 903.45 | 734.06 | 760.83 | 408.08 | 30.46 | 31,335.14 |
†
Purchasing Power Parities Exchange rate: 1 purchasing power parity dollar = R$ 2.044 (2018).
‡
p < 0.001 (test U of Mann–Whitney).
The monthly estimate of total maintenance costs for the TCSC is US$135,083.60. Considering an average monthly production of 24,625 activities in the period, each activity produced generated a maintenance cost of US$5.48.
Cost-minimization analysis
The CMA shows the service using the teledermatology strategy has a cost per patient of US$196.04, whereas the use of conventional services has a cost of US$245.66. Based on the assumption that the services have an equal capacity for patient care, there are only differences in costs, resulting in an additional US$49.62 for conventional patient care, which makes teledermatology the alternative cost-saving compared with the conventional patient care. A sensitivity analysis assessed the model’s uncertainties and verified whether changes in the values used could alter the incremental cost found. The sensitivity analysis confirmed the robustness of the main results. Figure 2, of the tornado analysis, shows the values that most impact the results are the total cost of the patient in secondary care, followed by the total cost in teledermatology tertiary care.
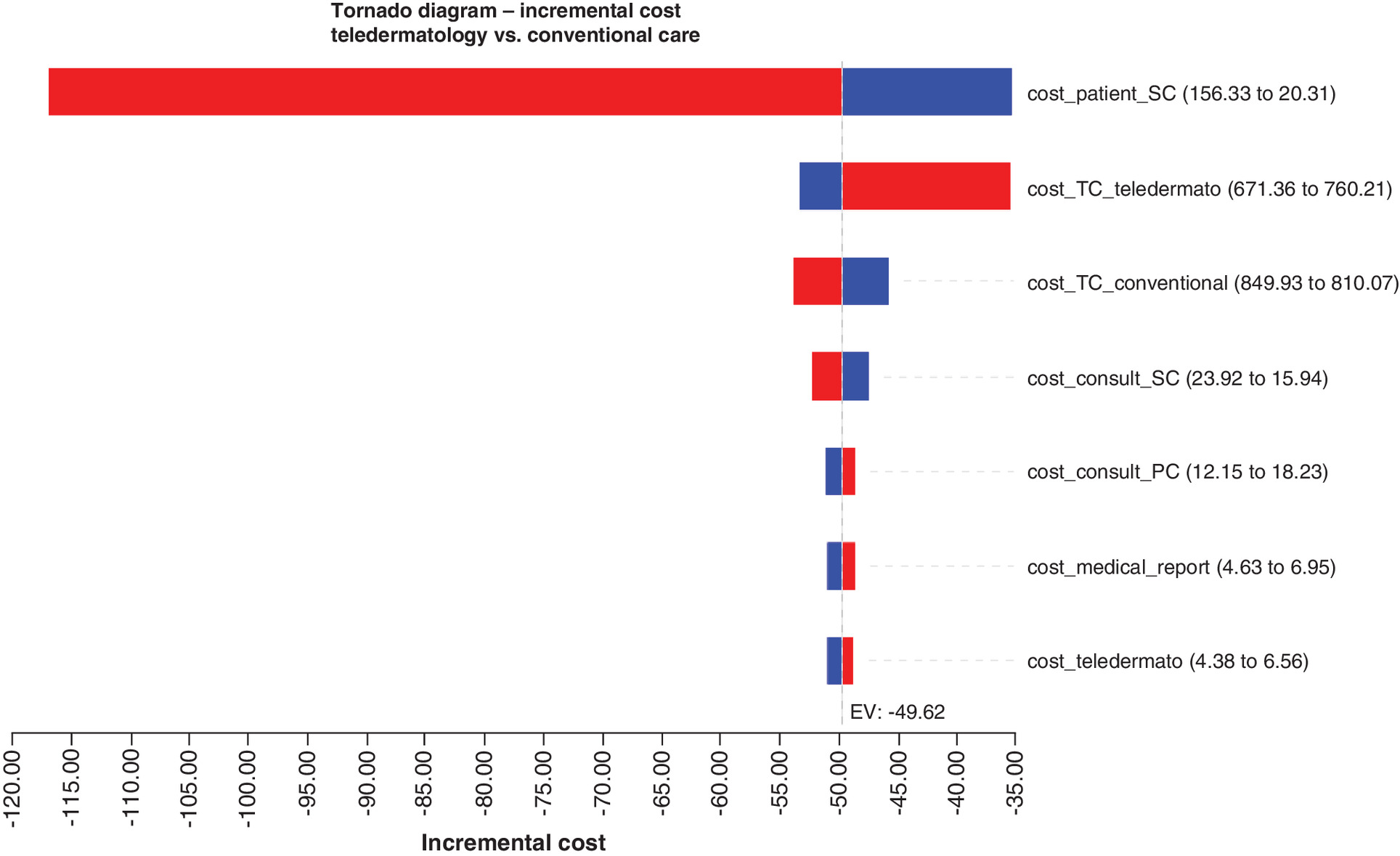
Figure 2. Tornado analysis of the incremental cost relation between teledermatology and conventional care.
Consult: Medical consultation; PC: Primary care; SC: Secondary care; TC: Tertiary care.
In the additional sensitivity analysis, the cost of hospitalization in the teledermatology arm was increased by 20% (US$826.30). In this setting, the result showed an additional cost of US$22.08 for conventional patient care, which means that the cost of hospitalization had an important contribution to the overall cost. Despite this, the cost difference between the alternatives is maintained.
Discussion
An important aspect to be emphasized in this evaluation refers to the innovation caused by teledermatology in the organization of health actions and services in the state of Santa Catarina. This organization proposal aimed to reduce unnecessary referrals and reduce the waiting time for consultation with specialists. In addition, it sought to provide support to the primary care professional in patient management [8,9,14].
A reduction of unnecessary referrals was observed in the 2016–2018 3-year period, and more patients could have been managed in primary care, avoiding commuting and expanding the access of more severe patients to the specialist. After the implementation of the teledermatology service in 2015, there was a significant drop in the number of patients on the waiting list, from 4080 to 98 patients, as well as in the average waiting time, from more than 1000 to 20 days, when comparing 2013 with 2017 [15]. Reductions in waiting list time after implementing teledermatology were also seen in Spain and the USA [16,17]. Moreover, it was found that teledermatology increased access to face-to-face dermatological care [17], and the mean rate of dermatological consultations avoided ranged from 45.5% to 57.0% when adopting the asynchronous system (store and forward), which reinforces its feasibility and importance, helping the general physicians to manage such conditions and optimizing medical hours and costs, especially in the public system [18,19]. A systematic review estimated the use of asynchronous teledermatology was associated with 43% of avoided trips [20]. These proportions reported in the literature are very close to those observed in the teledermatology service in Santa Catarina, which also adopts the asynchronous model.
The highest number of patients with their dermatological problems solved in primary care may be related to a higher qualification of care at this level. The educational benefit derived from the content of the teledermatology consultation is mentioned in the literature as a useful resource, with feedback many times faster than through traditional consultation processes [18], observing better knowledge of dermatology among primary care physicians who used this referral system [21,22].
Another aspect that deserves to be highlighted is the growth in the number of hospitalizations due to selected dermatological conditions, during the period 2016–2018, which occurred simultaneously with a significant decrease in the mean number of days spent at the hospital. A possible explanation for this, although not exhaustive, refers to the reduction of barriers to access to care. However, we have assumed that patients with the same diagnosis of hospitalization in different periods are matching cases, which is a limitation of this study. In addition, any change in the dermatological practice between the time periods could have contributed to differences seen in model parameters, although the teledermatology service team had not reported significant changes in this practice. A prospective study in university hospitals found teledermatology reduces the time required for a dermatologist to respond and the time required for a primary care team to receive an answer for a consultation to define the need for hospitalization. These findings suggest teledermatology as a tool to improve access to tertiary-level dermatological care [23]. In addition, teledermatology is a valuable mechanism for dermatologists to screen appointments and increase efficiency, thus expanding access to specialized care for hospitalized patients [24].
Teledermatology increases access to care without increasing cost [25]. A cost-minimization analysis was conducted to compare the organization-wide cost of managing referred dermatology patients within a teledermatology triage system versus a conventional dermatology care model at a general hospital. The study suggests that using teledermatology to triage and manage dermatology patients within a capitated healthcare system may be associated with significant cost savings [26]. Telemedicine usually avoids the overhead costs in the healthcare system that are associated with conventional in-person care. However, we also must consider societal costs [27].
The economic evaluation developed in this study adopted the societal perspective and included the use of direct medical resources in the production of procedures, in addition to commuting costs from the municipality of residence to the service, per diem and opportunity costs for the patient and companion, when applicable. In the scenario assessed here, teledermatology proved to be a cost-saving alternative to conventional care. The sensitivity analysis shows that incremental costs could vary according to the amounts spent on patients in secondary care. This finding reinforces the importance of teledermatology in reducing commuting costs and productivity loss for patients since it avoids unnecessary expenses [3,28]. In a country of continental dimensions such as Brazil, where distances separating rural and urban areas can be very large, the use of teledermatology has the potential to generate substantial savings in resources, as well as greater patients satisfaction.
Given that asynchronous teledermatology has the potential to reduce commuting and offers greater convenience to the patient, these gains can be addressed more holistically from a societal perspective [29,30].
The available current economic evidence is sparse, but suggested the asynchronous store-and-forward teledermatology may be cost-effective, especially when used as a screening mechanism to reduce the demand for face-to-face consultations and when considering the costs associated with productivity loss [7,29,31–33]. In this sense, our results are in line with the literature. However, because of country-specific variations in the health systems, it is problematic to generalize economic evaluations of telemedicine interventions from one country to another [6].
According to Landow et al. [32], by maximizing the time of a scarce resource, such as dermatologists, teledermatology provides improved access by increasing the number of patients evaluated and treated, and avoiding unnecessary and time-consuming face-to-face consultations. In this way, it fulfills three promises it makes about dermatological care: to be better, cheaper and faster. It is ‘better’ because, although it cannot offer the patient as much as a traditional visit, it extends the dermatologist’s reach to places and in ways that were previously not possible due to time and place limitations. It is ‘cheaper and faster’ for having the potential to reduce costs and increase the efficiency of patients and providers, by resulting in less time away from work and faster service. The results obtained by the present economic evaluation, focusing on the teledermatology service in Santa Catarina, are consonant with the fulfillment of these promises
Conclusion
A cost-minimization analysis was performed comparing the teledermatology service of the State of Santa Catarina, Brazil with the provision of conventional care. This economic evaluation adopted the societal perspective and included the use of direct medical resources in the production of procedures, in addition to commuting costs from the municipality of residence to the service, per diem and opportunity costs for the patient and companion, when applicable. In the scenario assessed here, teledermatology proved to be a cost-saving alternative to conventional care. This finding reinforces the importance of teledermatology in reducing commuting costs and productivity loss for patients since it avoids unnecessary expenses.
•
The limited literature evaluating the economic consequences of teledermatology suggests that teledermatology may be cost-effective.
•
There is evidence that the effectiveness of the alternatives teledermatology or conventional care is similar and corresponds to the patient seen at any level of care.
•
This article presents a cost-minimization analysis comparing the teledermatology service of the State of Santa Catarina, Brazil with the provision of conventional care.
•
The economic evaluation adopted the societal perspective and included the use of direct medical resources in the production of procedures, in addition to commuting costs from the municipality of residence to the service, per diem and opportunity costs for the patient and companion, when applicable.
•
During the period 2016–2018, 79,411 exams were performed at the teledermatology service. Most patients were female (63.7%), with a mean age of 50.4 (±20) years.
•
The cost-minimization analysis shows the service using the teledermatology strategy has a cost per patient of US$196.04, whereas the use of conventional services has a cost of US$245.66, resulting in an additional US$49.62 for conventional patient care.
•
The sensitivity analysis confirmed the robustness of the main results.
•
In the scenario assessed here, teledermatology proved to be a cost-saving alternative to conventional care. This finding reinforces the importance of teledermatology in reducing commuting costs and productivity loss for patients since it avoids unnecessary expenses.
•
In a country of continental dimensions such as Brazil, where distances separating rural and urban areas can be very large, the use of teledermatology has the potential to generate substantial savings in resources, as well as greater patients satisfaction.
Author contributions
FA Acurcio, AA Guerra Junior and JA Teodoro designed the study, collected and analyzed the data and wrote the manuscript. MM Garcia and RG Pereira collected data, contributed with the discussion and reviewed the manuscript. M Akerman, LF Spinel, IC Borysow, RR Silva, PS Azevedo and PCIC Gomes contributed with the discussion and reviewed the manuscript. MCM Calvo and DH Nunes designed the study, contributed with the discussion and reviewed the manuscript. All authors approved the final version of the manuscript.
Acknowledgments
The authors are indebted to the team of the Telehealth Center of the State of Santa Catarina (TCSC) for their research support.
Financial & competing interests disclosure
This study was supported by the Project ‘Diagnostic Evaluation of the Brazil Telehealth Program Networks,’ developed by the Hospital Alemão Oswaldo Cruz (HAOC), based on an agreement established with the Ministry of Health, under the Institutional Development Program of the Brazilian National Health System (PROADI-SUS). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
Ethical aspects and confidentiality were strictly safeguarded, insofar as the data from a secondary source were not identified, access to them remained restricted to researchers, and results were presented exclusively in an aggregated manner. The principles outlined in the Declaration of Helsinki have been followed.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Campagna M, Naka F, Lu J. Teledermatology: an updated overview of clinical applications and reimbursement policies. Int. J. Womens Dermatol. 3(3), 176–179 (2017).
2.
Bashshur RL, Shannon GW, Tejasvi T, Kvedar JC, Gates M. The empirical foundations of teledermatology: a review of the research evidence. Telemed. J. E Health 21(12), 953–979 (2015).
3.
Eminović N, Dijkgraaf MG, Berghout RM, Prins AH, Bindels PJE, Keizer NF. A cost-minimization analysis in teledermatology: model-based approach. BMC Health Serv. Res. 10, 251 (2010).
•• A cost-minimization study design (a model-based approach) was applied to compare teledermatology and conventional process costs per dermatology patient care episode, from the societal perspective. The results showed that savings by teledermatology can be achieved if the distance to a dermatologist is larger (≥75 km) or when more consultations (≥37%) can be prevented due to teledermatology.
4.
Datta SK, Warshaw EM, Edison KE et al. Cost and utility analysis of a store-and-forward teledermatology referral system: a randomized clinical trial. JAMA Dermatol. 151(12), 1323–1329 (2015).
5.
Yarak S, Ruiz EES, Pisa IT. Teledermatology in medical practice. Rev. Bras. Educ. Med. 41(2), 346–355 (2017).
6.
Delgoshaei B, Mobinizadeh M, Mojdekar R, Afzal E, Arabloo J, Mohamadi E. Telemedicine: a systematic review of economic evaluations. Med. J. Islam. Repub. Iran. 31, 113 (2017).
7.
Wang RH, Barbieri JS, Nguyen HP et al. Clinical effectiveness and cost-effectiveness of teledermatology: where are we now, and what are the barriers to adoption? J. Am. Acad. Dermatol. 83(1), 299–307 (2020).
•• Updated paper reviews the evidence on the clinical and cost–effectiveness of teledermatology and discusses system-level and practice-level barriers to successful teledermatology implementation.
8.
Maeyama MA, Calvo MCM. Integration of telehealth in regulation centrals: the teleconsulting as a mediator between primary care and specialized care. Rev. Bras. Educ. Med. 42(2), 63–72 (2018).
9.
von Wangenheim A, Nunes DH. Creating a web infrastructure for the support of clinical protocols and clinical management: an example in teledermatology. Telemed. J. E Health 25(9), 781–790 (2019).
10.
Ekeland AG, Bowes A, Flottorp S. Effectiveness of telemedicine: a systematic review of reviews. Int. J. Med. Inform. 79(11), 736–771 (2010).
11.
Pak H, Triplett CA, Lindquist JH, Grambow SC, Whited JD. Store-and-forward teledermatology results in similar clinical outcomes to conventional clinic-based care. J. Telemed. Telecare. 13(1), 26–30 (2007).
12.
Levin YS, Warshaw EM. Teledermatology: a review of reliability and accuracy of diagnosis and management. Dermatol. Clin. 27(2), 163–176 (2009).
13.
Whited JD, Warshaw EM, Kapur K et al. Clinical course outcomes for store and forward teledermatology versus conventional consultation: a randomized trial. J. Telemed. Telecare. 19(4), 197–204 (2013).
14.
Piccoli MF, Amorim BDB, Wagner HM, Nunes DH. Teledermatology protocol for screening of skin cancer. An. Bras. Dermatol. 90(2), 202–210 (2015).
15.
Ferreira I, Godoi D, Perugini E, Lancini AB, Zonta R. Teledermatology: an interface among primary and specialized care in Florianopolis. Rev. Bras. Med. Fam. Comunidade 14(41), 2003 (2019).
16.
Vidal Alaball J, Álamo Junquera D, López-Aguilá S, Garcia-Altés A. Evaluation of the impact of teledermatology in decreasing the waiting list in the Bages region (2009–2012). Aten. Primaria. 47(5), 320–321 (2015).
17.
Raugi GJ, Nelson W, Miethke M et al. Teledermatology Implementation in a VHA secondary treatment facility improves access to face-to-face care. Telemed. J. E Health 22(1), 12–17 (2016).
18.
Whited JD. Teledermatology. Med. Clin. North Am. 99(6), 1365–1379 (2015).
• An overview of teledermatology with an emphasis on the evidence most relevant to referring clinicians. The paper discusses the different modalities used for teledermatology and their diagnostic reliability, diagnostic accuracy, impact on in-person dermatology visits, clinical outcomes and user satisfaction.
19.
Giavina-Bianchi M, Santos AP, Cordioli E. Teledermatology reduces dermatology referrals and improves access to specialists. EClinicalMedicine. 29–30, 100641 (2020).
20.
Wootton R, Bahaadinbeigy K, Hailey D. Estimating travel reduction associated with the use of telemedicine by patients and healthcare professionals: proposal for quantitative synthesis in a systematic review. BMC Health. Serv. Res. 11, 185 (2011).
21.
McFarland LV, Raugi GJ, Taylor LL, Reiber GE. Implementation of an education and skills programme in a teledermatology project for rural veterans. J. Telemed. Telecare. 18(2), 66–71 (2012).
22.
Mohan G, Molina GE, Stavert R. Store and forward teledermatology improves dermatology knowledge among referring primary care providers: a survey-based cohort study. J. Am. Acad. Dermatol. 79(5), 960–961 (2018).
23.
Sharma P, Kovarik CL, Lipoff JB. Teledermatology as a means to improve access to inpatient dermatology care. J. Telemed. Telecare. 22(5), 304–310 (2016).
24.
Barbieri JS, Nelson CA, James WD et al. The reliability of teledermatology to triage inpatient dermatology consultations. JAMA Dermatol. 150(4), 419–424 (2014).
25.
Jariwala NN, Snider CK, Mehta SJ et al. Prospective implementation of a consultative store-and-forward teledermatology model at a single urban academic health system with real cost data subanalysis. Telemed. J. E Health. (2020). (Epub ahead of print).
26.
Zakaria A, Miclau TA, Maurer T, Leslie KS, Amerson E. Cost minimization analysis of a teledermatology triage system in a managed care setting. JAMA Dermatol. 157(1), 52–58 (2021).
•• A retrospective cost minimization analysis comparing the organization-wide cost of managing referred patients within a teledermatology triage system versus a conventional dermatology care model. Managed healthcare settings may experience significant cost savings from using teledermatology to triage and manage patients.
27.
Maddukuri S, Patel J, Lipoff JB. Teledermatology addressing disparities in health care access: a review. Curr. Derm. Rep. 10, 40–47 (2021).
28.
Tensen E, van der Heijden JP, Jaspers MW, Witkamp L. Two decades of teledermatology: current status and integration in national healthcare systems. Curr. Dermatol. Rep. 5, 96–104 (2016).
29.
Snoswell C, Finnane A, Janda M, Soyer HP, A Whitty JA. Cost–effectiveness of store-and-forward teledermatology: a systematic review. JAMA Dermatol 152(6), 702–708 (2016).
•• Summarizes and evaluates the current economic evidence comparing store-and-forward teledermatology with conventional face-to-face care. Teledermatology appears to be cost-effective when used as a triage mechanism to reduce face-to-face appointment requirements. Its cost–effectiveness increases when patients are required to travel farther distances to access dermatology services.
30.
Vidal-Alaball J, Garcia Domingo JL, Garcia Cuyàs F et al. A cost savings analysis of asynchronous teledermatology compared to face-to-face dermatology in Catalonia. BMC Health Serv. Res. 18, 650 (2018).
31.
Pak HS, Datta SK, Triplett CA, Lindquist JH, Grambow SC, Whited JD. Cost minimization analysis of a store-and-forward teledermatology consult system. Telemed. J. E Health. 15(2), 160–165 (2009).
32.
Landow SM, Mateus A, Korgavkar K et al. Teledermatology: Key factors associated with reducing face-to-face dermatology visits. J. Am. Acad. Dermatol. 71(3), 570–576 (2014).
• Highlights factors that are associated with a higher number of face-to-face appointments avoided by teledermatology programs: effective preselection of patients for teleconsultation, high-quality photographic images, dermoscopy if pigmented lesions are evaluated and effective infrastructure and culture in place to implement teleconsultation recommendations.
33.
Livingstone J, Solomon J. An assessment of the cost–effectiveness, safety of referral and patient satisfaction of a general practice teledermatology service. London J. Prim. Care. 7(2), 31–35 (2015).
Information & Authors
Information
Published In
Pages: 1159 - 1168
PubMed: 34494888
Copyright
© 2021 Future Medicine Ltd.
History
Received: 27 May 2021
Accepted: 4 August 2021
Published online: 8 September 2021
Keywords:
Topics
Authors
Funding Information
Institutional Development Program of the Brazilian National Health System (PROADI-SUS), Hospital Alemão Oswaldo Cruz: NUP: 25000.018744/2018-49
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost-minimization analysis of teledermatology versus conventional care in the Brazilian National Health System. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0124
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Monica L. Taylor, Preksha Machaiya Kuppanda, Annie Bygraves, Cathy Baynie, Haley Bennett, H. Peter Soyer, Liam J. Caffery, Making Teledermatology Services Work: A Realist Review of Success Factors, Australasian Journal of Dermatology, 10.1111/ajd.70183, (2026).
- Camila Acordi da Silva, Andressa Konrad Corcetti, Franciele Cascaes da Silva, Oscar Cardoso Dimatos, DISTRIBUIÇÃO DOS DERMATOLOGISTAS NO ESTADO DE SANTA CATARINA, Arquivos Catarinenses de Medicina, 10.63845/dhk35997, 54, 4, (115-127), (2026).
- Júlia Meller Dias de Oliveira, Eduarda Talita Bramorski Mohr, Daniel Henrique Scandolara, Mariano Felisberto, Ianka Cristina Celuppi, Isis Gualdi Vasconcelos da Silva, Wagner Luiz Zanotto, Miliane dos Santos Fantonelli, Célio Luiz Cunha, Jades Fernando Hammes, Raul Sidnei Wazlawick, Eduardo Monguilhott Dalmarco, The Brazilian telehealth systems: a scoping review, Health and Technology, 10.1007/s12553-025-01047-6, (2026).
- Kevin Yun Kim, Lung Wen Chao, Cyro Festa Neto, História da Teledermatologia e sua evolução, aspectos práticos e perspectivas futuras no Brasil, Anais Brasileiros de Dermatologia (Versão em Português), 10.1016/j.abdp.2025.501208, 100, 6, (501208), (2025).
- Kevin Yun Kim, Lung Wen Chao, Cyro Festa Neto, The history of Teledermatology and its evolution, practical aspects, and prospects in Brazil, Anais Brasileiros de Dermatologia, 10.1016/j.abd.2025.501208, 100, 6, (501208), (2025).
- Sei-Jong Baek, Jeong-Ah Choi, Jin-Won Noh, Hyoung-Sun Jeong, A Cost-Minimization Analysis of Teleconsultation Versus In-Person Care for Chronic Diseases and Rehabilitation in Medically Underserved Areas of South Korea, Healthcare, 10.3390/healthcare13050445, 13, 5, (445), (2025).
- Sonya Ahuja, Shanelle Mariah Briggs, Sigrid Marie Collier, Teledermatology in Rural, Underserved, and Isolated Environments: A Review, Current Dermatology Reports, 10.1007/s13671-022-00377-2, 11, 4, (328-335), (2022).
- Petre Ilie, Simina Stefanescu, Jane Aldridge, Philip Gaffney, James Belcher, Lee Smith, Value of DermaCheckup as a novel dedicated digital health solution for teledermatology, Medicine International, 10.3892/mi.2022.30, 2, 1, (2022).