Indirect treatment comparison of olaparib and talazoparib in germline BRCA-mutated HER2-negative metastatic breast cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Two poly(ADP-ribose) polymerase (PARP) inhibitors olaparib and talazoparib are approved for patients with germline BRCA-mutated (gBRCAm) HER2-negative metastatic breast cancer. Methods: A Bayesian fixed-effects indirect treatment comparison (ITC) analysis was performed to simulate the comparative efficacy (primary outcome of progression-free survival [PFS]) and safety of PARP inhibitor monotherapy. Results: ITC of data from the OlympiAD (olaparib) and EMBRACA (talazoparib) studies suggested no significant difference in efficacy (PFS) between olaparib and talazoparib. However, there were differences in specific adverse events; patients receiving olaparib had a higher rate of nausea and vomiting, while those receiving talazoparib had a higher rate of alopecia and anemia. Discussion: These data support the benefit of the PARP inhibitor class in gBRCAm HER2-negative metastatic breast cancer.
Approximately 5% of all patients with breast cancer carry a deleterious germline mutation in BRCA1 and/or BRCA2 (gBRCAm), with rates higher in those with HER2-negative disease [1,2]. Patients with gBRCAm are typically diagnosed with breast cancer at a younger age than the general population [3,4], and the lifetime risk of developing breast cancer by age 80 years is approximately 70% [5]. There is a need for new treatment approaches, especially as advanced breast cancer with distant organ metastases is considered incurable with currently available therapies [6].
Poly(ADP-ribose) polymerase (PARP) inhibition targets a vulnerability in tumor cells that have homologous recombination repair gene mutations, including BRCA, most likely via multiple mechanisms, including PARP trapping [7]. The efficacy and safety of the PARP inhibitors olaparib and talazoparib given as monotherapy have been demonstrated in studies of patients with breast cancer, including those with gBRCAm HER2-negative metastatic disease [8–12]. Additionally, the preliminary efficacy and safety of veliparib monotherapy combined with chemotherapy has been demonstrated in patients with gBRCAm HER2-negative metastatic breast cancer (MBC) in the California Cancer Consortium [13] and BROCADE studies [14].
To compare the efficacy and safety of PARP inhibitor monotherapy in patients with gBRCAm HER2-negative MBC, we conducted a systematic literature review (SLR) to capture studies in patients with gBRCAm- and HER2-negative MBC. Subsequently, we undertook an indirect treatment comparison (ITC) of monotherapy PARP inhibitors that reported the primary outcome of progression-free survival (PFS) and safety data in this setting.
Methods
Systematic literature review
An SLR (cut-off date May 2019) following the guidelines published by the Cochrane Collaboration [15] was designed and conducted to identify randomized controlled trials (RCTs) that reported data on efficacy (PFS) and safety (incidence of adverse events [AEs], serious AEs [SAEs] and discontinuations due to AEs) of PARP inhibitors in patients with gBRCAm HER2-negative MBC. The following databases were searched: MEDLINE and Embase (using Embase.com), MEDLINE In-Process (using PubMed.com), and the Cochrane Library, including the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials and the Database of Abstracts of Reviews of Effectiveness. In addition, the following conference proceedings were manually searched for the years 2014–2019 (if 2019 abstracts were available at the time of analysis): San Antonio Breast Cancer Symposium, Senologic International Society, European Society for Medical Oncology, American Society of Breast Surgeons, European Breast Cancer Conference and American Society of Clinical Oncology. Searches were undertaken so that evidence up to May 2019 was retrieved with no lower date limit for the PubMed search and only studies published in English language were eligible for inclusion. The literature has subsequently been monitored to determine whether any additional relevant studies have been published since the search date. Trials had to meet the following pre-defined eligibility criteria: RCTs of interventions of interest (Table 1) in adult patients with germline BRCA1- and/or BRCA2-mutated HER2-negative MBC who are either hormone receptor (estrogen receptor and progesterone receptor) negative or positive. Publications found through electronic databases, conferences and bibliographical searches were initially reviewed for inclusion based on their title and abstract, and full-text copies were ordered for studies that potentially met the inclusion criteria. The eligibility criteria were then applied to all included full-text publications, once received. Abstract and full-text screenings were conducted by two independent reviewers, with any discrepancies between reviewers reconciled by a third independent reviewer. Data extraction was performed by an independent reviewer and quality checked by a second reviewer. Multiple publications identified for the same patient population and setting that reported data for the same intervention were linked and extracted as a single publication. Two independent reviewers undertook the screening/review of references; in the event of disagreement, a third reviewer was included to reach consensus. The identified RCTs were appraised using a comprehensive critical appraisal tool based on the National Institute for Health and Care Excellence checklist [16]. For this ITC analysis, we focus on the results of studies of gBRCAm HER2-negative MBC in line with the marketing authorizations of PARP inhibitor monotherapies in breast cancer.
| Inclusion criteria | Exclusion criteria | |
|---|---|---|
| Population (P) | Adult patients (aged ≥18 years) with HER2- or gBRCAm unresectable locally advanced BC or MBC. This includes patients with TNBC and ER+/PR+ disease The disease is also termed as: • Stage IV BC • Advanced BC Studies reporting unresectable, locally advanced, advanced, stage IV BC and MBC with unclear BRCA and unclear receptor status were included but not extracted | • Healthy volunteers • Patients aged <18 years • Diseases other than locally advanced BC or MBC • Patients with HER2+ status† • Ductal carcinoma in situ • Non-invasive or stage 0 BC • Invasive ductal carcinoma • Mucinous (colloid) carcinoma • Tubular carcinoma • Inflammatory breast cancer |
| Interventions (I) | Studies assessing at least one of the following mentioned interventions as monotherapy and/or combination therapy will be included: • Anthracyclines – Doxorubicin • Mono-chemotherapy – Capecitabine – Eribulin mesylate – Gemcitabine – Ixabepilone – Vinorelbine • Platinum drugs – Carboplatin – Cisplatin • Targeted therapy • Biological therapy (PARP inhibitors) – Olaparib – Pertuzumab – PF 01367338 (AG 014699) – Iniparib (BSI 201) – Veliparib (ABT 888) – MK 4827 – CEP 9722 – Talazoparib (BMN673, LT-673) – BSI 401 – Rucaparib (AG 014699) – Nicotinamide/nicotinamide analogues, eg 3-aminobenzamide, PD128763, NU1025 • VEGF inhibitor therapy – Bevacizumab in combination with taxane or capecitabine – Bevacizumab monotherapy • Kinase inhibitor therapy – Sorafenib • EGFR inhibitor therapy – Cetuximab • Taxanes – Abraxane® (nanoparticle albumin-bound paclitaxel, or nab-paclitaxel) – Docetaxel – Paclitaxel • Others – Cyclophosphamide + methotrexate + 5-fluorouracil | Studies that assess any one of the following interventions: • Adjuvant therapy • Endocrine/hormonal therapy – Androgens – Exemestane – Fulvestrant – Letrozole – Progestogens – Stilboestrol® – Tamoxifen – Trilostane • HER2+ targeted therapy – Trastuzumab – Lapatinib • Neoadjuvant therapy • Palliative radiotherapy • Sequential chemotherapy • Surgery |
| Comparators (C) | Comparator therapies may include one of the following: • Placebo • Any treatment listed under the interventions • Any other pharmacological treatments | • Non-pharmacological therapy (eg surgery, radiotherapy) and endocrine/hormonal therapy will be excluded • Targeted HER2+ therapies |
| Outcomes (O) | Data extraction was conducted using Excel® | – |
| Study design (S) | • RCTs – both parallel-group and crossover (double blind, single blind, open label) • Systematic reviews and meta-analyses of RCTs‡ | • In vitro studies • Preclinical studies • Non-RCTs • Observational studies • Comments, letters, editorials • Case reports, case series • Non-systematic reviews |
| Language | English language | Non-English |
| Country | No limit | – |
†
Patients with HER2+ cancer with a gBRCAm could be included but should be identified.
‡
Systematic reviews and meta-analyses of RCTs should be identified.
BC: Breast cancer; BRCA: BRCA1 and/or BRCA2; gBRCAm: Germline BRCA1 and/or BRCA2 mutation; MBC: Metastatic breast cancer; RCT: Randomized controlled trial; TNBC: Triple-negative breast cancer.
Indirect treatment comparison
Following identification of the RCTs of interest, an ITC of data from patients with gBRCAm HER2-negative MBC receiving treatment with PARP inhibitor monotherapy was performed to simulate comparative efficacy and safety. The outcomes of interest were the primary end point of PFS by blinded independent central review (BICR) and safety using data on the risk of common AEs, SAEs and SAE-related treatment discontinuations. All analyses compared the PARP inhibitor monotherapy arms in the studies of interest.
Statistical analysis
A Bayesian fixed-effects ITC of data was conducted using the gemtc package in R. The outputs of the ITC analysis included hazard ratio (HR) with 95% credible intervals (95% CrIs) for PFS by BICR and odds ratios (ORs) with 95% CrIs for AEs, SAEs and AE-related treatment discontinuations.
Results
Systematic literature review
The Preferred Reporting Items for Systematic Reviews and Meta-analysis [17] flow diagram shows the flow of studies evaluated in the SLR (Figure 1). Of the 59 publications identified, six studies provided evidence in the gBRCAm HER2-negative MBC setting. These were OlympiAD [8], EMBRACA [11], the California Cancer Consortium trial [13], BROCADE [14], CBCSG006 [18] and TNT [19]. Of these, only four studies included a PARP inhibitor arm; the TNT (carboplatin vs paclitaxel) and CBCSG006 (cisplatin plus gemcitabine vs paclitaxel plus gemcitabine) studies only included chemotherapy arms and so were not relevant for the ITC analysis. The BROCADE study did not include a PARP inhibitor monotherapy arm and the California Cancer Consortium trial did not report PFS as the primary efficacy outcome, so these were excluded from the ITC analysis (Table 2). Therefore, the OlympiAD [8] and EMBRACA [11] studies were the only two studies that met the prespecified criteria for inclusion in the ITC.

Figure 1. Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram.
†Among the 66 TNBC studies (298 publications), 61 studies (245 publication) reported only TNBC population data, whereas five studies (50 BRCA1/BRCA2 publications) reported both TNBC and BRCA1/BRCA2 population data. Hence, the 50 publications are copy duplicate between BRCA1/BRCA2 and TNBC extractions.
HTA: Health technology assessment; PARP: Poly(ADP-ribose) polymerase; PFS: Progression-free survival; SLR: Systematic literature review; TNBC: Triple-negative breast cancer.
| TNT | CBCSG006 | California Cancer Consortium | BROCADE | EMBRACA | OlympiAD | |
|---|---|---|---|---|---|---|
| Phase | III | III | II | II | III | III |
| Study design | RCT crossover trial | RCT parallel trial | RCT parallel trial | RCT parallel trial | RCT parallel trial | RCT parallel trial |
| Blinding | Open label | Open label | Open label | Partially blind† | Open label | Open label |
| Study setting | Multicenter | Multicenter | Multicenter | Multicenter, international | Multicenter, international | Multicenter, international |
| Mutation | gBRCAm (subgroup) | gBRCAm | gBRCAm | gBRCAm | gBRCAm | gBRCAm |
| Receptor status | Any | TNBC | HR+ | HR+ | HR+; TNBC | HR+; TNBC |
| Intervention | Carboplatin | Cisplatin + gemcitabine | Veliparib | Veliparib + temozolomide | Talazoparib | Olaparib |
| Comparators | Docetaxel | Paclitaxel + gemcitabine | Veliparib + carboplatin | Veliparib + carboplatin + paclitaxel; placebo + carboplatin + paclitaxel | TPC | TPC |
| Inclusion criteria | Eligible patients had ER-, PR-, HER2- BC or BC with gBRCAm with any receptor status. Patients with MBC and recurrent locally advanced BC were eligible | Eligible patients had unresectable recurrent or advanced BC; triple negative (ER-, PR-, and HER2-); ECOG performance status ≤1 | Eligible patients had MBC with gBRCAm, ECOG performance status ≤2 and measurable disease | Eligible patients had locally recurrent BC or MBC with gBRCAm and ECOG performance status 0-2 | Eligible patients had locally advanced BC and/or MBC with gBRCAm and ECOG performance status ≤2 | Eligible patients had HER2- MBC with gBRCAm |
| Exclusion criteria | Adjuvant taxane in ≤12 months or previous platinum or non-anthracyclines for MBC or ECOG performance status >2 | Symptomatic CNS metastases. Other active malignancies (including other hematological malignancies) or other malignancies except for cured non-melanoma skin cancer or cervical intra-epithelial neoplasia | Prior PARP inhibitor therapy, platinum therapy for MBC or CNS metastasis requiring therapy | >2 prior lines of cytotoxic therapy for metastatic disease, prior treatment with temozolomide, platinum, or PARP inhibitor, prior taxane for MBC; pre-existing neuropathy grade >1, and history of brain metastases or uncontrolled seizure disorder | First-line locally advanced and/or MBC with no prior adjuvant chemotherapy. Prior treatment with a PARP inhibitor (not including iniparib), HER2+ BC | Patients with HR+ BC had received at least one endocrine therapy (adjuvant therapy or therapy for metastatic disease) |
| Primary end point | Objective response rate | PFS | Confirmed response rate for single-agent veliparib in BRCA1 and BRCA2 populations | PFS | PFS | PFS |
| Reason for exclusion | No PARP inhibitor | No PARP inhibitor | Primary outcome was not PFS | No monotherapy PARP inhibitor arm | None | None |
†
The carboplatin/paclitaxel arms were double blind; treatment was open label for the veliparib with temozolomide arm.
BC: Breast cancer; CNS: Central nervous system; ECOG: Eastern Cooperative Oncology Group; gBRCAm: Germline BRCA1 and/or BRCA2 mutation; MBC: Metastatic breast cancer; PFS: Progression-free survival; RCT: Randomized controlled trial; TNBC: Triple-negative breast cancer; TPC: Treatment of physician's choice.
Studies of interest
OlympiAD (NCT02000622) was a randomized, open-label, Phase III study in patients with gBRCAm HER2-negative MBC who had received ≤2 chemotherapy lines in the metastatic setting [8]. Patients were randomized 2:1 to olaparib tablets (300 mg twice daily) or single-agent treatment of physician's choice (TPC; capecitabine, eribulin or vinorelbine in continuous 21-day cycles). The primary end point was PFS by BICR on an intention-to-treat basis.
EMBRACA (NCT01945775) was a randomized, open-label, Phase III trial in which patients with gBRCAm HER2-negative breast cancer were assigned, in a 2:1 ratio, to receive talazoparib (1 mg once daily) or single-agent TPC (capecitabine, eribulin, gemcitabine or vinorelbine in continuous 21-day cycles) [11]. The primary end point was PFS by BICR on an intention-to-treat basis.
Patient & study characteristics
There were some differences in the baseline characteristics of these two study populations (Table 3). The OlympiAD study had a higher proportion of patients with an Eastern Cooperative Oncology Group performance status of 0 (72.2%) than the EMBRACA study (53.3%) in the PARP inhibitor monotherapy arms. The EMBRACA study included patients with locally advanced and/or MBC (although only ~5% had locally advanced disease), whereas the OlympiAD study included only those with MBC. A lower proportion of patients in EMBRACA had visceral involvement at study entry (70.3 vs 80.5% in OlympiAD) and a higher proportion of patients in EMBRACA were treated in the first-line setting (38.3 vs 28.8% in OlympiAD). Gemcitabine was included in the TPC arm in the EMBRACA study but not in the OlympiAD study, and the maximum number of prior cytotoxic therapies for metastatic disease was two in the OlympiAD study and three in the EMBRACA study for advanced disease, although only a small proportion (~5%) had three therapies prior to enrolment in EMBRACA. In OlympiAD, patients had previous treatment with both a taxane and an anthracycline (if not contraindicated), whereas in EMBRACA patients had previous treatment with either a taxane, an anthracycline or both. Based on the data retrieved by the SLR, there was no evidence that the variables with imbalances were effect modifiers for the PARP inhibitors.
| Treatment/comparator group | OlympiAD | EMBRACA | ||
|---|---|---|---|---|
| Olaparib (n = 205) | TPC (n = 97) | Talazoparib (n = 287) | TPC (n = 144) | |
| Median age, years (range) | 44 (22–76) | 45 (24–68) | 45 (27–84) | 50 (24–88) |
| gBRCA1m; gBRCA2m, n (%) | 117 (57.1); 84 (41.0) Both 4 (2.0)† | 51 (52.6); 46 (47.4) | 133 (46.3); 154 (53.7) | 63 (43.8); 81 (56.2) |
| Receptor status, n (%) – TNBC – HR+ | 102 (49.8) 103 (50.2) | 48 (49.5) 49 (50.5) | 130 (45.3) 157 (54.7) | 60 (41.7) 84 (58.3) |
| Breast cancer stage, n (%) – Locally advanced – Metastatic | – 205 (100) | – 97 (100) | 15 (5.2) 271 (94.4) | 9 (6.2) 135 (93.8) |
| ECOG performance status, % – 0 – 1 – 2 | 72.2 27.8 – | 63.9 36.1 – | 53.3 44.3 2.1 | 58.3 39.6 1.4 |
| Prior chemotherapy regimen for MBC, n (%) – 0 – 1 – 2 – >3 | 68 (33.2) 80 (39.0) 57 (27.8) – | 31 (32.0) 42 (43.3) 24 (24.7) – | 111 (38.7) 107 (37.3) 57 (19.9) 12 (4.2) | 54 (37.5) 54 (37.5) 28 (19.4) 8 (5.6) |
| Prior platinum therapy, n (%) | 60 (29.3) | 26 (26.8) | 46 (16.0) | 30 (20.8) |
†
Four patients in the olaparib arm had both gBRCA1m and gBRCA2m.
ECOG: Eastern Cooperative Oncology Group; gBRCA1m: Germline BRCA1 mutation; gBRCA2m: Germline BRCA2 mutation; MBC: Metastatic breast cancer; TPC: Treatment of physician's choice; TNBC: Triple-negative breast cancer.
Outcomes of individual studies
In the OlympiAD study, PFS was statistically significantly longer with olaparib (median 7.0 months) than with TPC (median 4.2 months: HR: 0.58; 95% CI: 0.43–0.80; p < 0.001), indicating that olaparib was more efficacious than TPC [8]. At final analysis (64% maturity), median overall survival (OS) was 19.3 months for olaparib versus 17.1 months with TPC (HR: 0.90; 95% CI: 0.66–1.23; p = 0.513) [9].
The most common AEs of any grade were nausea, anemia, vomiting and fatigue in the olaparib group, and neutropenia, nausea, anemia and fatigue in the TPC group (Table 4). The incidence of alopecia during olaparib treatment was low (3.4%) compared with TPC treatment (13.2%). Overall, grade ≥3 AEs occurred more frequently with TPC than with olaparib (49.5 vs 38.0%, respectively; Table 4). The most commonly reported grade ≥3 AE was anemia in the olaparib group and neutropenia in the TPC group. The incidence of any SAE was similar in both treatment groups (16.6% for olaparib and 16.5% for TPC) and were considered treatment related in 3.4 and 6.6% of patients, respectively [9]. Extended follow-up of the OlympiAD study showed no new safety findings [9]. Dose modifications due to AEs were reported for 38.6% of patients on olaparib compared with 41.8% on TPC. The incidence of treatment discontinuation was 4.9% in the olaparib group and 7.7% in the TPC group. Gastrointestinal (GI) AEs were all grade 1 or 2 with olaparib (single events of grade 3 nausea and vomiting occurred with TPC) and were managed with dose reductions and interruptions (~2% in both groups). No patients discontinued olaparib treatment due to nausea and vomiting, but one patient discontinued TPC due to vomiting, and only 2.0% of patients in either treatment group discontinued treatment due to anemia. First onset of anemia was typically in the first 3 months of olaparib treatment and remained stable over time, and the risk of grade ≥3 anemia was low in patients who continued treatment beyond 24 months. Supportive treatment for anemia was provided for 46.3% of patients in the olaparib group; 18.0% on olaparib and 5.5% on TPC received at least one blood transfusion [9].
| Adverse events, n (%) | OlympiAD | EMBRACA | ||||||
|---|---|---|---|---|---|---|---|---|
| Olaparib (N = 205) | TPC (N = 91) | Talazoparib (N = 286) | TPC (N = 126) | |||||
| All grades | Grade ≥3 | All grades | Grade ≥3 | All grades | Grade ≥3‡ | All grades | Grade ≥3‡ | |
| Any AE | 200 (97.6) | 78 (38.0) | 87 (95.6) | 45 (49.5) | 282 (98.6) | NR | 123 (97.6) | NR |
| – Nausea | 119 (58.0) | 0 | 32 (35.2) | 1 (1.1) | 139 (48.6) | 1 (0.3) | 59 (46.8) | 2 (1.6) |
| – Anemia§ | 82 (40.0) | 33 (16.1) | 24 (26.4) | 4 (4.4) | 151 (52.8) | 112 (39.2) | 23 (18.3) | 6 (4.8) |
| – Vomiting | 66 (33.2) | 0 | 14 (15.4) | 1 (1.1) | 71 (24.8) | 7 (2.4) | 29 (23.0) | 2 (1.6) |
| – Fatigue | 61 (29.8) | 7 (3.4) | 22 (24.2) | 1 (1.1) | 144 (50.3) | 5 (1.7) | 54 (42.9) | 4 (3.2) |
| – Neutropenia¶ | 56 (27.3) | 19 (9.3) | 45 (49.5) | 24 (26.4) | 100 (35.0) | 60 (20.9) | 54 (42.9) | 44 (34.9) |
| – Diarrhea | 42 (20.5) | 1 (0.5) | 20 (22.0) | 0 | 63 (22.0) | 2 (0.7) | 33 (26.2) | 7 (5.6) |
| – Headache | 42 (20.5) | 2 (1.0) | 14 (15.4) | 2 (2.2) | 93 (32.5) | 5 (1.7) | 28 (22.2) | 1 (0.8) |
| – Thrombocytopenia | 14 (6.8) | 3 (1.5) | 5 (5.5) | 1 (1.1) | 77 (26.9) | 42 (14.7) | 9 (7.1) | 2 (1.6) |
| – Leukopenia | 23 (11.2) | 5 (2.4) | 9 (9.9) | 3 (3.3) | 49 (17.1) | 19 (6.6) | 17 (13.5) | 11 (8.7) |
| – Alopecia | 7 (3.4) | 0 | 12 (13.2) | 0 | 72 (25.2) | NA | 35 (27.8) | NA |
†
‡
For EMBRACA, overall incidence of grade ≥3 events was not reported.
Where indicated, the Medical Dictionary for Regulatory Activities preferred terms for some AEs have been combined:
§
Includes patients with reported AEs of anemia, decreased hemoglobin, decreased hematocrit, decreased red blood cell count and erythropenia for OlympiAD and anemia and decreased hemoglobin for EMBRACA.
¶
Includes patients with reported AEs of febrile neutropenia, granulocytopenia, decreased granulocyte count, neutropenia, neutropenic sepsis, decreased neutrophil count and neutropenic infection for OlympiAD and febrile neutropenia, neutropenia, decreased neutrophil count and neutropenic sepsis for EMBRACA.
AE: Adverse event; ITC: Indirect treatment comparison; NA: Not applicable; NR: Not reported; TPC: Treatment of physician's choice.
In the EMBRACA study, PFS was statistically significantly longer with talazoparib (median 8.6 months) than with standard therapy (median 5.6 months: HR: 0.54; 95% CI: 0.41–0.71; p < 0.001) [11]. At the final analysis, median OS was not significantly different between arms (19.3 months for talazoparib vs 19.5 months with TPC; HR: 0.85; 95% CI: 0.67–1.07; p = 0.17) [12].
The most common AEs of any grade were anemia, fatigue, nausea and headache in the talazoparib group and nausea, anemia, fatigue and neutropenia in the TPC group. Overall, grade ≥3 AEs were not reported for EMBRACA; however, grade ≥3 SAEs were similar in both arms (Table 4). The incidence of any SAE was similar in both treatment groups (31.8% for talazoparib and 29.4% for TPC), of which 9.1 and 8.7%, respectively, were considered treatment related. Dose modifications due to AEs were reported for 66.4% of patients on talazoparib and 59.4% on TPC, and the incidence of treatment discontinuation due to AEs was 5.9% and 8.7%, respectively. In an extended safety follow-up of the EMBRACA study [22], the cumulative risk of any-grade anemia increased more steeply than that of neutropenia and thrombocytopenia with talazoparib treatment but generally reached a plateau by week 25. Median time from first talazoparib dose to onset of first grade ≥3 episode of anemia was approximately 12 weeks, and the duration of anemia was approximately 7 days. Additionally, 38.1% of patients in the talazoparib group had blood transfusion, whereas 5.6% of the TPC-treated patients required blood transfusions.
Indirect treatment comparison
The ITC of PFS by BICR suggests no difference in efficacy between olaparib and talazoparib based on data from the primary outcome of the studies (HR: 1.09; 95% CrI: 0.72–1.65).
The ITC of overall safety end points (AEs and SAEs), as well as individual specific AEs, is shown in Figure 2. The specific AEs were those identified as the most commonly reported for olaparib and talazoparib in the OlympiAD and EMBRACA studies, respectively, and are included in their respective drug labels [20,21]. The ORs for alopecia and anemia indicated higher risk in talazoparib-treated patients than olaparib-treated patients, while those of nausea and vomiting indicated higher risk in olaparib-treated patients. The ORs for thrombocytopenia and neutropenia indicated a trend that favors olaparib, although not statistically significant. The ORs for headache, leukopenia, fatigue and diarrhea ranged from 0.85 to 1.15, suggesting no difference between the two PARP inhibitors. There was a trend favoring olaparib for any SAE or treatment-related SAE, although not statistically significant. Dose modifications due to AEs were more frequent for talazoparib in EMBRACA than olaparib in OlympiAD, which resulted in an OR of 0.68 (95% CrI: 0.35–1.33) favoring olaparib. Discontinuations due to AEs were similar for both PARP inhibitors (4.9% for olaparib and 5.9% for talazoparib) and the OR for discontinuations due to AEs was 0.93 (95% CrI: 0.26–3.45).
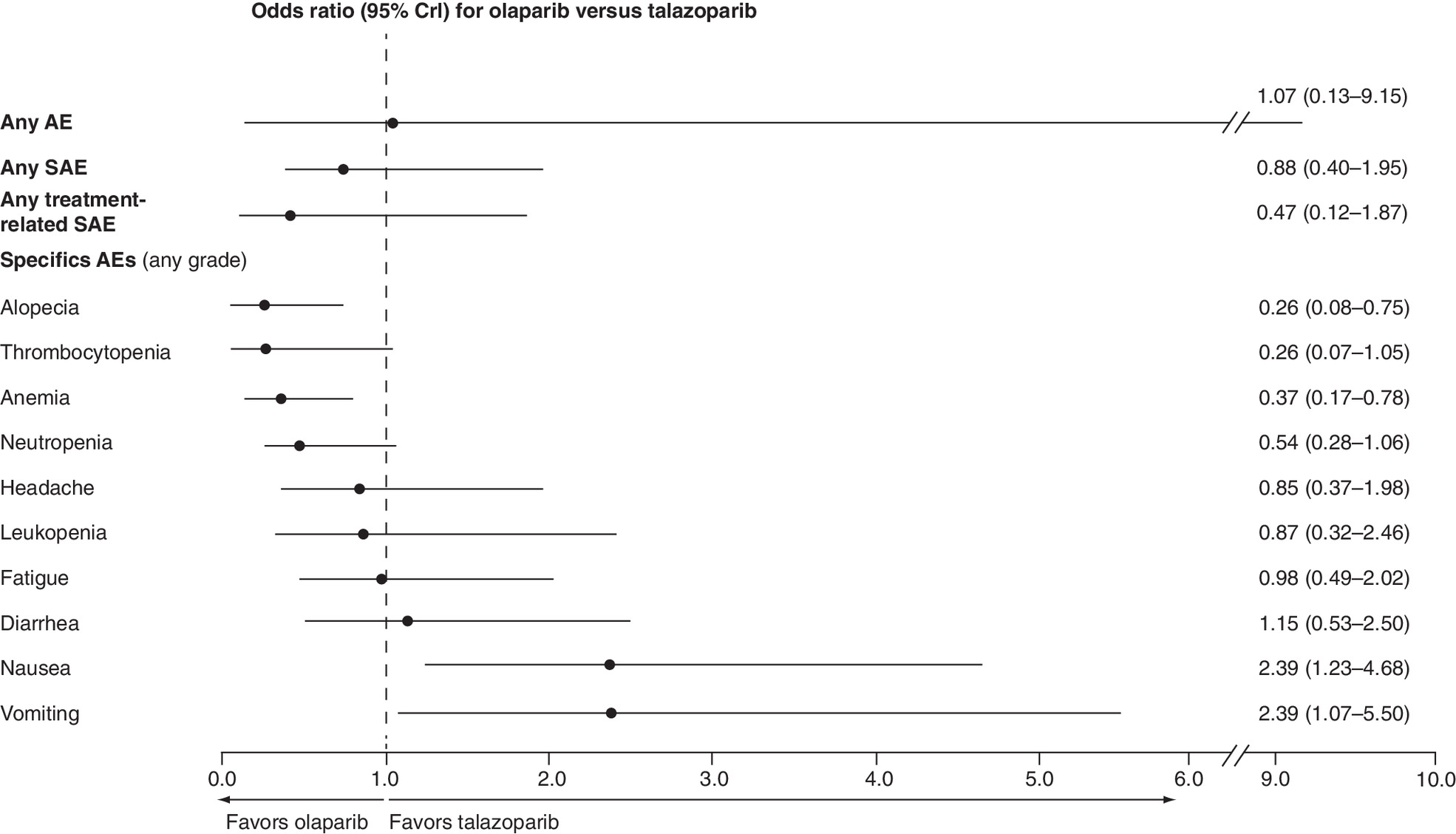
Figure 2. Forest plot of safety outcomes from ITC of olaparib versus talazoparib.
AE: Adverse event; CrI: Credible interval; ITC: Indirect treatment comparison; SAE: Serious adverse event.
Discussion
An SLR conducted to identify RCTs that included patients with gBRCAm HER2-negative advanced breast cancer and a PARP inhibitor monotherapy arm found two studies that could be considered for this ITC analysis: OlympiAD (olaparib) and EMBRACA (talazoparib). Both studies showed significant improvements in the primary end point, PFS by BICR, for the respective PARP inhibitors compared with TPC, and this ITC suggests no notable difference in efficacy between olaparib and talazoparib. The consistency of efficacy results between the OlympiAD and EMBRACA studies confirms the benefit of the PARP inhibitor class in the gBRCAm HER2-negative advanced breast cancer setting. These findings are supported by clinically significant improvements in patient-reported outcomes with olaparib and talazoparib versus TPC [23]. Median OS was not significantly different compared with TPC for olaparib in the OlympiAD study and talazoparib in the EMBRACA study, indicating no evidence of detrimental effect of PARP inhibitors versus TPC; OS was not evaluated as part of the ITC as there was no significant difference for either PARP inhibitor versus TPC [9,12]. Unlike the OlympiAD study, OS in EMBRACA was a prespecified alpha-controlled secondary end point and a larger patient population was included than in the OlympiAD study. Collectively, these findings suggest that while in vitro talazoparib has been shown to be a more effective trapper of PARP with a greater antiproliferative effect than olaparib, this did not translate into improved efficacy in MBC [24].
The ITC found no notable difference in the overall risk of any-grade AEs between olaparib and talazoparib treatment, although the CrIs were wide. There was a trend favoring olaparib in the overall risk of any SAE and treatment-related SAEs, although the differences were not statistically significant. However, the PARP inhibitors did differ in risk of specific AEs, with olaparib having an increased risk of the GI events of nausea and vomiting, but a lower risk of alopecia and anemia versus talazoparib. There was also a trend for a lower risk in thrombocytopenia and neutropenia favoring olaparib, although the differences were not statistically significant. In both PARP inhibitor studies, GI toxicities were among the most commonly reported AEs, but they were mild to moderate in severity, well managed with supportive care, and resolved without dose modification [9]. Preclinical evidence suggests that hematological toxicity may be a class effect of PARP inhibitors [25] and that they impact hematopoiesis [26], which may explain the hematological AEs observed in these studies. In both the EMBRACA and OlympiAD studies, hematological toxicities were managed by supportive care (including transfusions) and dose modifications while ensuring that the majority of patients could remain on treatment [9,22]. Overall, the risk of treatment discontinuation due to AEs for the PARP inhibitors was low (<6%) in both studies. The lower incidence of hematological grade 3 or 4 events, including anemia, neutropenia and thrombocytopenia, reported for olaparib-treated patients versus talazoparib-treated patients appeared to translate into cost savings for AE management [27].
There were several limitations of this ITC analysis, including heterogeneity in study design, differences in reporting of AEs, differences in chemotherapy agents used in the control arms of the studies, and the number of prior chemotherapies. Furthermore, although the updated SLR was undertaken in May 2019, to our knowledge there have been no additional relevant studies published for inclusion in the ITC analysis.
In conclusion, taking into account differences in study design and patient populations, the efficacy of monotherapy PARP inhibitors appears consistent, with similar outcomes reported in the EMBRACA (talazoparib) and OlympiAD (olaparib) studies. While the safety profiles of these two PARP inhibitors are similar in terms of overall AEs, there were differences in specific AEs, with the risk of GI toxicities of nausea and vomiting being higher in patients receiving olaparib compared with talazoparib, and a greater risk of alopecia, and hematological AEs, particularly anemia, thrombocytopenia and neutropenia in patients receiving talazoparib compared with olaparib.
•
To compare the efficacy and safety of PARP inhibitor monotherapy in patients with gBRCAm HER2-negative metastatic breast cancer (MBC), we conducted a systematic literature review to identify studies of interest.
•
Subsequently, an indirect treatment comparison (ITC) of data from these studies was performed to simulate comparative efficacy and safety.
•
Only two studies evaluating the efficacy and safety of PARP inhibitor monotherapy were identified; these were the OlympiAD study evaluating olaparib and the EMBRACA study evaluating talazoparib.
•
These two studies showed that olaparib and talazoparib given as monotherapy provide significant improvements in progression-free survival (PFS) compared with treatment of physician's choice in patients with gBRCAm HER2-negative MBC.
•
An ITC comparing treatment effectiveness and safety suggested no notable difference in efficacy between olaparib and talazoparib in the gBRCAm HER2-negative MBC setting.
•
The safety profiles of the two PARP inhibitors were similar in terms of overall AEs; however, there were differences in specific AEs, with the risk of nausea and vomiting being higher in patients receiving olaparib compared with talazoparib, and the risk of alopecia, anemia, thrombocytopenia, and neutropenia being higher in patients receiving talazoparib compared with olaparib.
•
These findings confirm the benefit of the PARP inhibitor class in the gBRCAm HER2-negative MBC setting.
Author contributions
C McCrea, P Gulati and R Hettle conceived and designed the study, and undertook the statistical analyses. All authors acquired and analysed the data, interpreted the results, drafted the manuscript and reviewed or revised the manuscript for important intellectual content. All authors reviewed the interim drafts and the final version of the manuscript and agreed with its content and submission.
Acknowledgments
AstraZeneca and Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, sponsored this study. The sponsors collaborated with academic advisors to design the study and gather, analyse, and interpret the results. All authors had full access to all study data and approved the decision to submit the manuscript for publication.
Financial & competing interests disclosure
This study was supported by AstraZeneca and is part of an alliance between AstraZeneca and Merck Sharp & Dohme Corp, a subsidiary of Merck & Co, Inc, Kenilworth, NJ, USA. A Taneja and P Rajora are employees of BresMed and were paid consultants for this research. C McCrea, P Gulati and R Hettle are employees and shareholders of AstraZeneca. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Juliet Fawcett, PhD, for Mudskipper Business Ltd, funded by AstraZeneca and Merck Sharp & Dohme Corp, a subsidiary of Merck & Co, Inc, Kenilworth, NJ, USA.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Malone KE, Daling JR, Doody DR et al. Prevalence and predictors of BRCA1 and BRCA2 mutations in a population-based study of breast cancer in white and black American women ages 35 to 64 years. Cancer Res. 66(16), 8297–8308 (2006).
2.
Kurian AW, Gong GD, John EM et al. Performance of prediction models for BRCA mutation carriage in three racial/ethnic groups: findings from the Northern California Breast Cancer Family Registry. Cancer Epidemiol. Biomarkers Prev. 18(4), 1084–1091 (2009).
3.
ACS. Breast Cancer Facts and Figures (2018). www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2017-2018.pdf
4.
SEER. Breast Cancer Facts (2019). https://seer.cancer.gov/statfacts/html/breast.html
5.
Kuchenbaecker KB, Hopper JL, Barnes DR et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 317(23), 2402–2416 (2017).
6.
Harbeck N, Penault-Llorca F, Cortes J et al. Breast cancer. Nat. Rev. Dis. Primers 5(1), 66 (2019).
7.
O'Connor MJ. Targeting the DNA damage response in cancer. Mol. Cell. 60(4), 547–560 (2015).
8.
Robson M, Im SA, Senkus E et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N. Engl. J. Med. 377(6), 523–533 (2017).
•• Reports the primary results from the Phase III OlympiAD study demonstrating the efficacy of olaparib in patients with gBRCAm metastatic breast cancer.
9.
Robson ME, Tung N, Conte P et al. OlympiAD final overall survival and tolerability results: olaparib versus chemotherapy treatment of physician's choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann. Oncol. 30(4), 558–566 (2019).
• Reports final overall survival data and updated tolerability findings from the OlympiAD study highlighting that olaparib is generally well tolerated in patients with gBRCAm metastatic breast cancer, but no significant difference in overall survival compared with chemotherapy.
10.
Gelmon KA, Tischkowitz M, Mackay H et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: a Phase 2, multicentre, open-label, non-randomised study. Lancet Oncol. 12(9), 852–861 (2011).
11.
Litton JK, Rugo HS, Ettl J et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N. Engl. J. Med. 379(8), 753–763 (2018).
•• Reports the primary results from the Phase III EMBRACA trial demonstrating the efficacy of talazoparib in patients with gBRCAm advanced breast cancer.
12.
Litton JK, Hurvitz SA, Mina LA et al. Talazoparib versus chemotherapy in patients with germline BRCA1/2-mutated HER2-negative advanced breast cancer: final overall survival results from the EMBRACA trial. Ann. Oncol. 31(11), 1526–1535 (2020).
• Reports the final overall survival results from the Phase III EMBRACA trial, showing no significant improvement with talazoparib compared with chemotherapy.
13.
Somlo G, Frankel PH, Arun BK et al. Efficacy of the PARP inhibitor veliparib with carboplatin or as a single agent in patients with germline BRCA1- or BRCA2-associated metastatic breast cancer: California Cancer Consortium Trial NCT01149083. Clin. Cancer Res. 23(15), 4066–4076 (2017).
14.
Han HS, Dieras V, Robson M et al. Veliparib with temozolomide or carboplatin/paclitaxel versus placebo with carboplatin/paclitaxel in patients with BRCA1/2 locally recurrent/metastatic breast cancer: randomized Phase II study. Ann. Oncol. 29(1), 154–161 (2018).
15.
Higgins JPT, Thomas J, Chandler J et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (2019). www.training.cochrane.org/handbook
16.
NICE. Single Technology Appraisal: user guide for company evidence submission template (2017). www.nice.org.uk/process/pmg24/chapter/instructions-for-companies
17.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Open Med. 3(3), e123–e130 (2009).
18.
Hu XC, Zhang J, Xu BH et al. Cisplatin plus gemcitabine versus paclitaxel plus gemcitabine as first-line therapy for metastatic triple-negative breast cancer (CBCSG006): a randomised, open-label, multicentre, Phase 3 trial. Lancet Oncol. 16(4), 436–446 (2015).
19.
Tutt A, Tovey H, Cheang MCU et al. Carboplatin in BRCA1/2-mutated and triple-negative breast cancer BRCAness subgroups: the TNT trial. Nat. Med. 24(5), 628–637 (2018).
20.
FDA. LYNPARZA (Olaparib) Prescribing Information (2014). www.accessdata.fda.gov/drugsatfda_docs/label/2020/208558s014lbl.pdf
21.
FDA. TALZEENA (Talazoparib) Prescribing Information (2018). www.accessdata.fda.gov/drugsatfda_docs/label/2018/211651s000lbl.pdf
22.
Hurvitz SA, Goncalves A, Rugo HS et al. Talazoparib in patients with a germline BRCA-mutated advanced breast cancer: detailed safety analyses from the Phase III EMBRACA trial. Oncologist 25(3), e439–e450 (2019).
• Reports detailed safety findings from the EMBRACA trial highlighting that talazoparib is generally well tolerated in gBRCAm MBC setting.
23.
Robson M, Ruddy KJ, Im SA et al. Patient-reported outcomes in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer receiving olaparib versus chemotherapy in the OlympiAD trial. Eur. J. Cancer 120, 20–30 (2019).
24.
Murai J, Huang SY, Renaud A et al. Stereospecific PARP trapping by BMN 673 and comparison with olaparib and rucaparib. Mol. Cancer Ther. 13(2), 433–443 (2014).
25.
Illuzzi G, O'Connor M, Leo E. A novel assay for PARP-DNA trapping provides insights into the mechanism of action (MoA) of clinical PARP inhibitors (PARPi). Cancer Res. 79(Suppl. 13), abstract 2077 (2019).
26.
Farres J, Martin-Caballero J, Martinez C et al. PARP-2 is required to maintain hematopoiesis following sublethal gamma-irradiation in mice. Blood 122(1), 44–54 (2013).
27.
McCrea C, MacDonald D, Hettle R et al. Cost comparison of adverse event management with poly(ADP-ribose) polymerase (PARP) inhibitors or chemotherapy in gBRCA-mutated, HER2-negative advanced breast cancer (ABC): a US and German healthcare perspective. Value Health 22, S476 (2019).
Information & Authors
Information
Published In
Pages: 1021 - 1030
PubMed: 34231369
Copyright
© 2021 Future Medicine Ltd.
History
Received: 20 April 2021
Accepted: 11 June 2021
Published online: 7 July 2021
Keywords:
Topics
Authors
Funding Information
Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Indirect treatment comparison of olaparib and talazoparib in germline BRCA-mutated HER2-negative metastatic breast cancer. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2021-0097
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Charmy Twala, Penny Govender, Ephraim Marondedze, Krishna Govender, Computational Evaluation of Novel PARP-1 Inhibitors for Breast Cancer: Docking, Molecular Dynamics, MM/GBSA, DFT and ADMET Calculations, Pharmaceuticals, 10.3390/ph19060914, 19, 6, (914), (2026).
- Nishtha Chaurawal, Amalia Ruiz Estrada, Klaus Pors, Kaisar Raza, Muhammad Wahajuddin, Innovative Nanocarriers of Sorafenib in the Optimisation of Therapeutic Outcome: Challenges and Applications in Breast Cancer, AAPS PharmSciTech, 10.1208/s12249-026-03392-9, 27, 3, (2026).
- Valeriia Lebedeva, Mira Ebbinghaus, José Villacorta Hidalgo, Olaf Hardt, Rita Pfeifer, Triple-Negative Breast Cancer Unveiled: Bridging Science, Treatment Strategy, and Economic Aspects, International Journal of Molecular Sciences, 10.3390/ijms26199714, 26, 19, (9714), (2025).
- Ayşe Hale Alkan, Demet Cansaran-Duman, Multifaceted interactions between lncRNA-associated ceRNA networks and small molecules in triple-negative breast cancer, Biomedicine & Pharmacotherapy, 10.1016/j.biopha.2025.118241, 189, (118241), (2025).
- Pablo Caballero Portero, Talazoparib en cáncer de mama y en cáncer de próstata, Panorama Actual del Medicamento, 10.63105/49.483.7, 49, 483, (511-521), (2025).
- Saif Khan, Suresh Babu Jandrajupalli, Nashwa Zaki Ali Bushara, Rama Devi Patel Raja, Shadab Mirza, Kuldeep Sharma, Rajan Verma, Ashish Kumar, Mohtashim Lohani, Targeting Refractory Triple-Negative Breast Cancer with Sacituzumab Govitecan: A New Era in Precision Medicine, Cells, 10.3390/cells13242126, 13, 24, (2126), (2024).
- Alberto Zambelli, Laura Cortesi, Mariangela Gaudio, Grazia Arpino, Giampaolo Bianchini, Francesco Caruso, Saverio Cinieri, Giuseppe Curigliano, Lucia Del Mastro, Sabino De Placido, Alessandra Fabi, Lucio Fortunato, Daniele Generali, Alessandra Gennari, Stefania Gori, Giovanni Grandi, Valentina Guarneri, Marco Klinger, Lorenzo Livi, Caterina Marchiò, Isabella Palumbo, Pietro Panizza, Gabriella Pravettoni, Giancarlo Pruneri, Fabio Puglisi, Anna Sapino, Corrado Tinterri, Daniela Turchetti, Michelino De Laurentiis, Parp-inhibitors in the therapeutic landscape of breast cancer patients with BRCA1 and BRCA2 pathogenic germline variants: An Italian consensus paper and critical review, Cancer Treatment Reviews, 10.1016/j.ctrv.2024.102815, 130, (102815), (2024).
- Banu Arun, Fergus J. Couch, Jean Abraham, Nadine Tung, Peter A. Fasching, BRCA-mutated breast cancer: the unmet need, challenges and therapeutic benefits of genetic testing, British Journal of Cancer, 10.1038/s41416-024-02827-z, 131, 9, (1400-1414), (2024).
- Emily Brugioni, Elizabeth Cathcart-Rake, Janie Metsker, Elizabeth Gustafson, Lindsey Douglass, Timothy J. Pluard, Germline BRCA-Mutated HER2-Negative Advanced Breast Cancer: Overcoming Challenges in Genetic Testing and Clinical Considerations When Using Talazoparib, Clinical Breast Cancer, 10.1016/j.clbc.2023.04.006, 23, 5, (469-477), (2023).
- Yang Luo, Ying Cheng, Chunjiao Wu, Hui Ye, Naihan Chen, Fan Zhang, Hua Wei, Binghe Xu, Pharmacokinetics, safety, and antitumor activity of talazoparib monotherapy in Chinese patients with advanced solid tumors, Investigational New Drugs, 10.1007/s10637-023-01351-w, 41, 3, (503-511), (2023).