Matching-adjusted indirect comparison of palbociclib versus ribociclib and abemaciclib in hormone receptor-positive/HER2-negative advanced breast cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Palbociclib (PAL), ribociclib (RIB) and abemaciclib (ABM), in combination with fulvestrant (FUL), are approved for the treatment of hormone receptor-positive, HER2-negative advanced breast cancer. This study aims to determine relative efficacy of PAL+FUL versus RIB+FUL and ABM+FUL using matching-adjusted indirect treatment comparisons. Patients & methods: Anchored matching-adjusted indirect treatment comparisons were conducted using individual patient data from PALOMA-3 and published summary-level data from MONARCH 2 and MONALEESA-3. The primary outcome was overall survival (OS). Results: OS was similar for PAL+FUL versus ABM+FUL (hazard ratio: 0.87; 95% CI: 0.54–1.40) and RIB+FUL (hazard ratio: 0.89; 95% CI: 0.48–1.63). Conclusion: Adjusting for cross-trial differences suggests similar OS between treatments, underscoring the importance of accounting for these differences when indirectly comparing treatments.
Lay abstract
Palbociclib (PAL), ribociclib (RIB) and abemaciclib (ABM) are used with fulvestrant to treat hormone receptor-positive, HER2-negative advanced breast cancer. This study aims to use data from clinical trials to compare how long patients live after starting treatment with PAL versus RIB and ABM. Since patients who enroll in different trials may have different characteristics, it is important to adjust for these differences for a more accurate comparison. Adjusting for these differences showed that patients with hormone receptor-positive, HER2-negative advanced breast cancer treated with PAL lived for a similar length of time compared with those treated with RIB or ABM.
Breast cancer is among the most common type of cancer among women worldwide [1,2]. Subtypes of breast cancer are classified according to hormone receptor expression and HER2 amplification or overexpression. Hormone receptor-positive, HER2-negative (HR+/HER2-) breast cancer is the most common subtype [3]; a variety of drug treatments targeting HR+ breast cancer are available, including selective estrogen receptor modulators, selective estrogen receptor degraders and aromatase inhibitors (AIs) [4].
Cell cycle checkpoints play an essential role in preventing genomic instability, which contributes to the development of breast cancer [4]. The cell cycle is tightly regulated by cyclins and their associated cyclin-dependent kinases (CDKs) [5,6]. Dysregulation of the association between D-type cyclins and two specific CDKs – CDK4 and CDK6 – plays an important role in the development and progression of breast cancer [4]. Inhibition of CDK4/6 leads to cell cycle arrest, resulting in reduced proliferation of cancer cells [6]. Three selective CDK4/6 inhibitors (CDK4/6is) are now being used in the treatment of HR+/HER2- advanced breast cancer (ABC) [6].
On 3 February 2015, palbociclib (PAL) became the first CDK4/6i approved by the US FDA, in combination with letrozole (LET), for the treatment of women with HR+/HER2- ABC [7]. The indication was extended to include PAL in combination with fulvestrant (FUL) (PAL+FUL) on 19 February 2016 [7] based on findings from a Phase III clinical trial (PALOMA-3) that demonstrated improved progression-free survival (PFS) with PAL+FUL compared with placebo (PBO) combined with FUL (PBO+FUL) [8].
Two additional CDK4/6is have since received FDA approval, in combination with AIs or FUL, for the treatment of women with HR+/HER2- ABC based on findings of improved PFS compared with PBO+FUL in Phase III trials. Ribociclib (RIB) was approved on 13 March 2017 in combination with an AI, and the indication was extended to include RIB in combination with FUL (RIB+FUL) on 18 July 2018 [9] based on findings from MONALEESA-3 (ML-3) [10]. On 28 September 2017, abemaciclib (ABM) was approved in combination with FUL (ABM+FUL) [11] based on findings from MONARCH 2 (MN 2) [12].
There is a lack of trials comparing PAL+FUL, RIB+FUL and ABM+FUL directly. In the absence of head-to-head trials comparing these therapies in the treatment of HR+/HER2- ABC, indirect treatment comparison (ITC) methods may be used to compare treatment effects using data from the PALOMA-3, MN 2 and ML-3 trials. PFS was the primary end point in each of these trials. Adjusted indirect comparisons found that PAL+FUL was similar in terms of PFS when compared with both RIB+FUL (hazard ratio [HR]: 0.78; 95% CI: 0.57–1.07) and ABM+FUL (HR: 0.84; 95% CI: 0.61–1.14) [13].
To our knowledge, ITC methods have not yet been used to compare overall survival (OS) for PAL+FUL with RIB+FUL and ABM+FUL. Each of the three approved CDK4/6is has been evaluated in reference to PBO+FUL in terms of OS in their respective randomized controlled trials. In PALOMA-3, median OS among patients treated with PAL+FUL was 34.9 months, compared with 28.0 months among those who received PBO+FUL (HR: 0.81; 95% CI: 0.64–1.03) [14]. In MN 2, median OS among patients treated with ABM+FUL was 46.7 months, compared with 37.3 months for PBO+FUL (HR: 0.76; 95% CI: 0.61–0.95) [15]. Median OS was not reached in the RIB+FUL group in ML-3, and was reported as 40.0 months in the PBO+FUL group (HR: 0.72; 95% CI: 0.57–0.92) [16].
Although PALOMA-3, ML-3 and MN 2 each investigated a CDK4/6i in combination with FUL compared with PBO+FUL, baseline characteristics differed between study populations. Notably, patients enrolled in PALOMA-3 were more heavily pretreated than those in MN 2 and ML-3. Both MN 2 and ML-3 excluded patients with any prior chemotherapy, or more than one line of prior endocrine therapy (ET), in the metastatic setting [10,12]. In contrast, PALOMA-3 included patients with up to one line of prior chemotherapy, or any prior ET, in the metastatic setting [8].
Traditional ITC methods based only on summary-level data may be biased due to such inherent differences in patient populations. Matching-adjusted indirect comparisons (MAICs) are used to indirectly compare a treatment effect across studies by leveraging individual patient data (IPD) from one study to reduce cross-trial differences. This is achieved through matching and adjusting of the IPD to the summary-level data of the comparator trial’s population. When a common comparator is present, anchored MAICs can be used to further adjust for cross-trial differences. By anchoring through the control arm, differences in known and unknown prognostic factors across trials are accounted for when determining the relative treatment effect.
The present study uses anchored MAICs, which are designed to reduce cross-trial differences that would otherwise undermine the validity of traditional ITCs. By leveraging IPD from PALOMA-3 and summary-level data from MN 2 and ML-3, separate anchored MAICs were conducted to compare PAL+FUL to ABM+FUL and RIB+FUL in terms of OS in patients with HR+/HER2- ABC.
Patients & methods
Methods for anchored MAIC analyses
IPD were available for the PALOMA-3 trial, which compared PAL+FUL to PBO+FUL. Summary-level data were available for the MN 2 and ML-3 trials, which compared ABM+FUL to PBO+FUL and RIB+FUL to PBO+FUL, respectively. Given the presence of a common comparator (PBO+FUL), an anchored MAIC is an appropriate method to compare the efficacy of PAL+FUL to ABM+FUL and RIB+FUL in the treatment of HR+/HER2- ABC.
MAICs were conducted using methods outlined by the National Institute for Health and Care Excellence [17]. The population in PALOMA-3 was ‘matched’ to the population in the comparator trial by excluding patients in the IPD who would not have met the eligibility criteria of the comparator trial. After matching, differences in patient characteristics across trials remained. These imbalances were then ‘adjusted’ for by reweighting the remaining patients in PALOMA-3 so that the means and variances of their characteristics matched those reported in the summary-level data of the comparator trial. Weights were determined by a propensity score model, in which patients in PALOMA-3 were weighted by the inverse odds of being in PALOMA-3 versus the comparator study based on the values of their baseline characteristics. A visual presentation of the steps undertaken in the MAIC method is shown in Figure 1.

Figure 1. Overview of matching & adjusting steps in a matching-adjusted indirect treatment comparison.
ESS: Effective sample size; ET: Endocrine therapy; IPD: Individual patient data; MBC: Metastatic breast cancer.
Since the MAICs were anchored through a common comparator (PBO+FUL), differences in known and unknown prognostic characteristics across trials are controlled for when comparing the relative treatment effects. That is, between-trial differences in known or unknown prognostic factors (i.e., differences in control arms) do not affect anchored ITCs due to within-trial randomization. Each active treatment is compared with PBO+FUL within their own study, and the resulting treatment effects relative to PBO+FUL are then compared across studies. Therefore, the MAICs only relied on balancing baseline characteristics that can alter the treatment effects between studies (i.e., treatment-effect modifiers). The matched and adjusted PALOMA-3 IPDs were used to compare the effect of treatment on OS across balanced trial populations. For each comparison, an HR, 95% CI and effective sample size (ESS) were derived.
Inclusion criteria of comparator trials
Before comparing treatment effects across studies, the patient population from PALOMA-3 required adjustment to align more closely with the eligibility criteria and baseline characteristics of each comparator trial. Unlike PALOMA-3 [8], MN 2 and ML-3 excluded patients with ≥2 prior therapies, or any prior chemotherapy, in the metastatic setting [10,12]. Additionally, ML-3 excluded pre/perimenopausal patients [10], while PALOMA-3 did not exclude patients based on menopausal status [8]. A comparison of the eligibility criteria across all three trials is shown in Table 1.
| PALOMA-3 | MONARCH 2 | MONALEESA-3 | Ref. [8,10,12,18] | |
|---|---|---|---|---|
| Inclusion | ||||
| – Menopausal status† | Pre, peri or post | Pre, peri or post | Post | |
| – Receptor status | HR+/HER2- | HR+/HER2- | HR+/HER2- | |
| – ECOG PS | 0, 1 | 0, 1 | 0, 1 | |
| – Measurable disease | Required‡, or bone-only disease | Required, or bone-only disease | Required‡, or ≥1 predominantly lytic bone lesion | |
| – Progressed on or after ET in the adjuvant or metastatic setting | Required | Required | Not required | |
| – Number of prior lines of ET for MBC | Any§ | ≤1 | ≤1 | |
| Exclusion | ||||
| – Visceral crisis | Excluded | Excluded | Excluded | |
| – CNS metastasis (uncontrolled/symptomatic) | Excluded | Excluded | Excluded | |
| – Prior chemotherapy for MBC | >1 excluded | Excluded | Excluded | |
| – QTc/QTcF interval¶ | >480 msec | NR | >450 msec | |
†
Pre/perimenopausal women enrolled in PALOMA-3 received the LHRH agonist goserelin for at least 4 weeks prior to and for the duration of the trial. Pre/perimenopausal women in MONARCH 2 received a GnRH agonist such as goserelin.
‡
Measurable disease defined by RECIST version 1.1.
§
In the palbociclib+fulvestrant arm, 62.2% of patients received ≤1 prior line of therapy for MBC, 25.9% received two prior lines, and 11.8% received ≥3 prior lines.
¶
Based on the value of triplicate ECGs. In MONALEESA-3, a QTcF was used at screening.
ECOG PS: Eastern Cooperative Oncology Group performance status; ET: Endocrine therapy; GnRH: Gonadotropin-releasing hormone; HR+: Hormone receptor-positive; LHRH: Luteinizing hormone-releasing hormone; MBC: Metastatic breast cancer; msec: Milliseconds; NR: Not reported; QTc: Corrected QT; QTcF: Corrected QT by Fredericia; RECIST: Response evaluation criteria in solid tumors.
Evidence-informed ranking of treatment-effect modifiers
Matching based on eligibility criteria ensures inclusion of similar patients across trials. However, it does not ensure equal spread of baseline characteristics. For example, PALOMA-3 had fewer patients with no previous lines of therapy for metastatic breast cancer (MBC; 22%) than MN 2 (61%), and PALOMA-3 had more patients with prior ET in the advanced or metastatic setting (74%) than ML-3 (26%). Differences in baseline characteristics between PALOMA-3 and each comparator trial are shown in Table 2. Since the MAIC method accounted for differences in prognostic variables across trials by anchoring through PBO+FUL, only the means and variances of treatment-effect modifiers required adjustment to those in the comparator trial.
| Characteristic | Category | PALOMA-3§ (N = 521) n (%) | MONARCH 2 (N = 669) n (%) [12] | MONALEESA-3 (N = 726) n (%) [10,16] |
|---|---|---|---|---|
| Age group† | <65 ≥65 | 392 (75) 129 (25) | 424 (63) 245 (37) | 387 (53) 339 (47) |
| Race†,‡ | White Asian Other | 385 (74) 105 (20) 29 (6) | 373 (59) 214 (34) 42 (7) | 619 (88) 63 (9) 24 (3) |
| Region†,‡ | North America Asia Pacific Other Europe Asia | 240 (46) 114 (22) 167 (32) 167 (32) 114 (22) | 178 (27) − − 279 (42) 212 (31) | 112 (15) 56 (8) 558 (77) − − |
| ECOG PS† | 1 0 | 199 (38) 322 (62) | 264 (40) 400 (60) | 256 (35) 468 (65) |
| Metastatic site†,‡ | Visceral Bone only Other | 304 (58) 124 (24) 93 (18) | 373 (56) 180 (27) 113 (17) | 439 (60) 154 (21) 133 (18) |
| Organs involved, number†,‡ | 1 2 3 ≥3 4 ≥5 | 171 (33) 146 (28) 106 (20) 201 (39) 66 (13) 29 (6) | 263 (40) 200 (30) − 203 (30) − − | 224 (31) 232 (32) 162 (22) − 72 (10) 33 (5) |
| Measurable disease† | Yes No | 405 (78) 116 (22) | 483 (73) 183 (27) | 560 (77) 166 (23) |
| Prior AI† | Yes No | 447 (86) 74 (14) | 465 (70) 204 (30) | 375 (52) 350 (48) |
| Prior chemotherapy†,‡ | Neoadjuvant or adjuvant Metastatic None | 214 (41) 177 (34) 130 (25) | 401 (60) 0 (0) 268 (40) | 405 (56) 0 (0) 321 (44) |
| Previous lines of therapy for MBC† | 0 1 ≥2 | 114 (22) 225 (43) 182 (35) | 396 (61) 256 (39) 0 (0) | 367 (52) 345 (48) 0 (0) |
| Menopausal status† | Pre/perimenopausal Postmenopausal | 108 (21) 413 (79) | 114 (17) 551 (83) | 0 (0) 726 (100) |
| ER status‡ | Negative Positive | 3 (1) 510 (99) | – – | 4 (1) 722 (99) |
| PR status | Negative Positive | 142 (28) 361 (72) | – – | 206 (28) 520 (72) |
| Disease-free Interval‡ | ≤12 months >12 months NA | 13 (2) 341 (65) 167 (32) | – – – | 31 (4) 555 (76) 140 (19) |
| Prior tamoxifen | No Yes | 207 (40) 314 (60) | – – | 428 (59) 297 (41) |
| Prior ET setting‡ | (Neo)adjuvant Advanced/metastatic | 134 (26) 387 (74) | – – | 431 (74) 150 (26) |
| Sensitivity to prior ET† | Yes No | 410 (79) 111 (21) | 489 (74)¶ 169 (26)# | – – |
Percentages are out of the total number of patients with available data for the specified variable.
†
Treatment-effect modifiers adjusted for in the MAIC with MONARCH 2.
‡
Treatment-effect modifiers adjusted for in the MAIC with MONALEESA-3.
§
Values for PALOMA-3 calculated using IPD.
¶
Secondary ET resistance used to identify sensitivity to prior ET.
#
Primary ET resistance used to identify no sensitivity to prior ET.
AI: Aromatase inhibitor; ECOG PS: Eastern Cooperative Oncology Group performance status; ER: Estrogen receptor; ET: Endocrine therapy; IPD: Individual patient data; MAIC: Matching-adjusted indirect comparison; MBC: Metastatic breast cancer; NA: Not applicable; PR: Progesterone receptor.
Treatment-effect modifiers that have the greatest influence on MAIC results are those that have a large impact on treatment effect and vary substantially across trials. Since differences in patient characteristics vary according to the populations in the comparison, a rank-ordered list of treatment-effect modifiers was produced for each of the comparisons prior to the analysis. Potential treatment-effect modifiers were first identified by reviewing the literature and consulting clinicians. Additional treatment-effect modifiers were then identified using the PALOMA-3 IPD, and all were rank ordered based on an evidence-informed process considering both extent of treatment modification and differences between trials. The final rank-ordered list of treatment-effect modifiers is shown in Supplementary Table 1. The MAIC included treatment-effect modifiers that were deemed important based on assessment of the literature and clinical opinion, extent of treatment modifications, differences in characteristics between trials, and impact on ESS.
Diagnostics assessing balance after adjustment for cross-trial differences
Each MAIC computed an ESS of the final PALOMA-3 population after matching and adjusting to the comparator trial population. The ESS is the number of nonweighted patients that would produce a treatment effect estimate with the same precision as the weighted sample estimate [17]. That is, the ESS is reduced if adjusting for larger number of, or very influential, treatment-effect modifiers. The maximum ESS occurs when all patients have equal weights, meaning that the trial populations are already similar and do not require any adjustments in baseline characteristics.
The occurrence of a small ESS is indicative of differences in patient populations between PALOMA-3 and the comparator trial. Therefore, the MAIC clearly highlights differences in patient populations, whereas other ITC methods may not be as transparent.
Scenario & sensitivity analyses
Adjusting for all predetermined treatment-effect modifiers can often lead to very low ESS of the matched and adjusted population. Scenario analyses were conducted to assess the impact on the ESS and the treatment effect estimates when adjusting for varying numbers of treatment-effect modifiers. The primary MAIC for each comparison (described as ‘scenario A’) adjusted for all selected treatment-effect modifiers with equal importance. Subsequent scenario analyses (i.e., ‘scenario B’ and onwards) removed treatment-effect modifiers one-by-one from adjustment, starting with the lowest rank-ordered factor.
Since matching the population in PALOMA-3 to the populations in MN 2 and ML-3 resulted in large sample size reductions, two sensitivity analyses were conducted. The first sensitivity analysis did not match based on eligibility criteria. Instead, eligibility factors (prior chemotherapy for MBC, previous lines of therapy for MBC and menopausal status) were redefined when possible and added as potential treatment-effect modifiers for adjustment. The second analysis matched on eligibility criteria and adjusted for the same treatment-effect modifiers as in the primary MAIC analyses, except for ‘region’ which was shown to cause a large drop in ESS.
Results
Primary results
PAL+FUL versus ABM+FUL
In the MAIC comparing PAL+FUL to ABM+FUL, the initial population size with intention to treat for PALOMA-3 was 521 patients. Removing patients with missing values in any baseline characteristics of interest resulted in an analysis dataset of 516 patients. Matching to the eligibility criteria of MN 2 reduced the total sample size to 280; 174 patients with prior chemotherapy and 180 patients with ≥2 previous lines of therapy in the metastatic setting were removed. Many patients (n = 118) were removed because they met both criteria. Of the remaining 280 patients, 183 were treated with PAL+FUL and 97 were treated with PBO+FUL. The remaining patients were reweighted by adjusting for all 12 rank-ordered treatment-effect modifiers indicated in Table 2. Fully matching and adjusting the population from PALOMA-3 to MN 2 reduced the ESS to 135. Summary statistics of baseline characteristics before and after matching and adjusting to the population of MN 2 are shown in Supplementary Table 2.
Traditional ITC results based only on summary-level data (i.e., unmatched and unadjusted) yielded similar OS for PAL+FUL compared with ABM+FUL (HR: 1.05; 95% CI: 0.76–1.44; Figure 2). Similar results were observed after matching patients in PALOMA-3 to the eligibility criteria of MN 2 (HR: 1.02; 95% CI 0.69–1.52) and after adjusting for remaining cross-trial imbalances (HR: 0.87; 95% CI: 0.54–1.40).
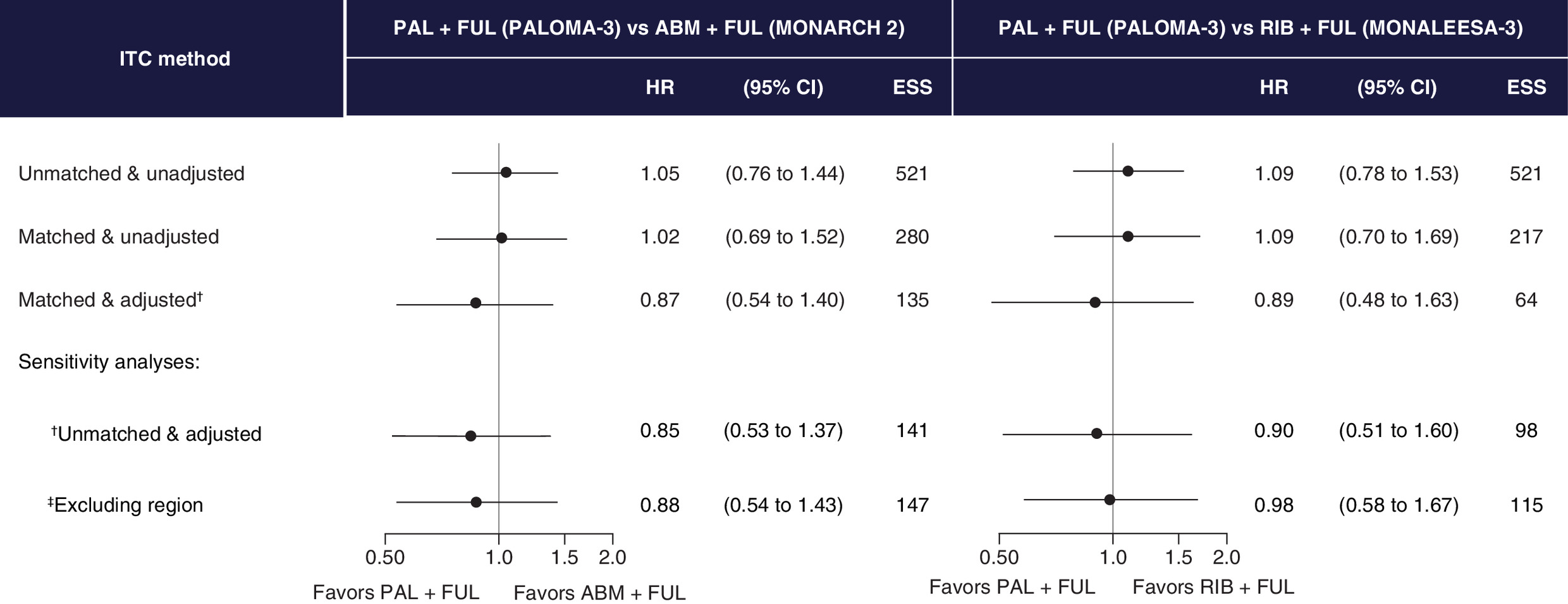
Figure 2. Executive summary of indirect treatment comparison results comparing palbociclib+fulvestrant to abemaciclib+fulvestrant & palbociclib+fulvestrant to ribociclib+fulvestrant.
Hazard ratio of <1 indicates higher OS for PAL+FUL.†The following treatment-effect modifiers are adjusted for in the MAIC with ABM+FUL: race, previous lines of therapy for MBC, number of organs involved, region, metastatic site, age group, prior chemotherapy, sensitivity to prior ET, measurable disease, ECOG PS, prior AI and menopausal status. The following treatment-effect modifiers are adjusted for in the MAIC with RIB+FUL: prior ET setting, region, number of organs involved, prior chemotherapy, ER status, race, disease-free interval and metastatic site.
‡The following treatment-effect modifiers are adjusted for in the comparison with ABM+FUL: age group, previous lines of therapy for MBC, prior chemotherapy setting (yes), race, prior AI, region, sensitivity to prior ET, number of organs involved, menopausal status, measurable disease, metastatic site, prior chemotherapy (neo)adjuvant setting and ECOG PS. The following treatment-effect modifiers are adjusted for in the comparison with RIB+FUL: age group, menopausal status, prior ET setting, previous lines of therapy for MBC (yes), prior tamoxifen, prior chemotherapy (yes) and organs involved.
ABM: Abemaciclib; AI: Aromatase inhibitor; ECOG PS: Eastern Cooperative Oncology Group performance status; ER: Estrogen receptor; ESS: Effective sample size; ET: Endocrine therapy; FUL: Fulvestrant; HR: Hazard ratio; MAIC: Matching-adjusted indirect comparison; MBC: Metastatic breast cancer; OS: Overall survival; PAL: Palbociclib; RIB: Ribociclib.
PAL+FUL versus RIB+FUL
In the MAIC comparing PAL+FUL to RIB+FUL, the analysis dataset was reduced from 521 to 492 after removing patients with missing values in any baseline characteristics of interest. After matching to the eligibility criteria of ML-3, 275 patients were removed because they received prior chemotherapy in the metastatic setting (n = 161), had ≥2 previous lines of therapy in the metastatic setting (n = 171) or had pre/perimenopausal status (n = 101). Many patients (n = 158) met more than one criterion. Of the remaining 217 patients, 142 patients were treated with PAL+FUL and 75 patients were treated with PBO+FUL. The remaining patients were reweighted by adjusting for the treatment-effect modifiers indicated in Table 2. The MAIC could not adjust for several factors (measurable disease, prior tamoxifen, age group, Eastern Cooperative Oncology Group performance status and progesterone receptor status) while maintaining sufficiently large ESS. In addition, the MAIC could not adjust for previous lines of therapy in the metastatic setting since it strongly correlated to prior ET setting after matching, or for prior aromatase inhibitor due to extreme differences across trials. Matching and adjusting the population from PALOMA-3 to ML-3 reduced the ESS to 64. Summary statistics of baseline characteristics before and after matching and adjusting to the population of ML-3 are shown in Supplementary Table 3.
Traditional ITC results based on summary-level data yielded similar OS for PAL+FUL compared with RIB+FUL (HR: 1.09; 95% CI: 0.78–1.53; Figure 2). Similar results were observed after matching patients in PALOMA-3 to the eligibility criteria of ML-3 (HR: 1.09; 95% CI: 0.70–1.69) and after adjusting for remaining cross-trial imbalances (HR: 0.89; 95% CI: 0.48–1.63).
Scenario & sensitivity analyses results
Sequentially removing treatment-effect modifiers in the scenario analyses led to comparable OS between PAL+FUL and ABM+FUL (Supplementary Figure 1), and between PAL+FUL and RIB+FUL (Supplementary Figure 2).
For each comparison, the first sensitivity analysis did not match based on eligibility criteria but considered these factors (prior chemotherapy for MBC, previous lines of therapy for MBC and menopausal status) for adjustment instead. Although this approach still resulted in substantially smaller sample sizes compared with the full study population, the ESS increased slightly compared with the primary analysis for both ABM+FUL (Figure 2 & Supplementary Figure 3) and RIB+FUL (Figure 2 & Supplementary Figure 4) comparisons. In both cases, conclusions were consistent with the primary analysis.
In the primary analysis for each comparison, the variable ‘region’ was associated with a large reduction in ESS, particularly in the comparison of PAL+FUL and RIB+FUL. Therefore, a second sensitivity analysis excluding this variable was conducted. This approach resulted in increased sample sizes compared with the primary analyses for both ABM+FUL (Figure 2 & Supplementary Figure 5) and RIB+FUL (Figure 2 & Supplementary Figure 6) comparisons. In both cases, the results were consistent with the primary analysis.
Discussion
In the absence of direct evidence from head-to-head clinical trials, ITC methods can be used to determine relative efficacy of treatments. In the present study, MAICs were conducted to compare PAL+FUL, ABM+FUL and RIB+FUL for the treatment of HR+/HER2- ABC in terms of OS.
Separate randomized controlled trials showed higher OS relative to PBO+FUL for PAL+FUL in PALOMA-3 (HR: 0.81; 95% CI: 0.64–1.03) [14], ABM+FUL in MN 2 (HR: 0.76; 95% CI: 0.61–0.95) [15] and RIB+FUL in ML-3 (HR: 0.72; 95% CI: 0.57–0.92) [16]. A naive comparison of these findings, without consideration of differences in patient populations between studies, could suggest that PAL+FUL is less effective than its competitors in terms of OS (Figures 3 & 4). However, after matching populations based on eligibility criteria, adjusting for cross-trial differences in baseline characteristics, and accounting for differences in control arms across trials, the HR was reduced from 1.05 (95% CI: 0.76–1.44) in the traditional ITC to 0.87 (95% CI: 0.54–1.40) in the MAIC with ABM+FUL, and from 1.09 (95% CI: 0.78–1.53) in the traditional ITC to 0.89 (95% CI: 0.48–1.63) in the MAIC with RIB+FUL. These results indicate that, in the absence of head-to-head clinical trials, PAL+FUL has similar OS compared with more recently approved CDK4/6is in the treatment of HR+/HER2- ABC.

Figure 3. Overall survival by treatment within each PALOMA-3 & MONARCH 2 population.
The first section shows the OS for PAL+FUL and PBO+FUL in the population from PALOMA-3 before and after reweighting patients to align with the population from MONARCH 2. The second section shows the OS of ABM+FUL and PBO+FUL in the population from MONARCH 2 [15]. The third section describes the modelled OS of PAL+FUL and ABM+FUL in the modelled population from MONARCH 2, after matching, adjusting and anchoring through PBO+FUL.
ABM: Abemaciclib; FUL: Fulvestrant; HR: Hazard ratio; OS: Overall survival; PAL: Palbociclib; PBO: Placebo.

Figure 4. Overall survival by treatment within each PALOMA-3 & MONALEESA-3 population.
The first section shows the OS for PAL+FUL and PBO+FUL in the population from PALOMA-3 before and after reweighting patients to align with the population from MONALEESA-3. The second section shows the OS of RIB+FUL and PBO+FUL in the population from MONALEESA-3 [16]. The third section describes the modelled OS of PAL+FUL and RIB+FUL in the modelled population from MONALEESA-3, after matching, adjusting and anchoring through PBO+FUL.
FUL: Fulvestrant; OS: Overall survival; HR: Hazard ratio; PAL: Palbociclib; PBO: Placebo; RIB: Ribociclib.
Although other studies have used ITC methods to compare therapies for ABC, to our knowledge, this is the first analysis to leverage IPD from the PALOMA-3 trial to compare the relative impact of PAL to either ABM or RIB in terms of OS in patients with HR+/HER2- ABC. Recently, Zhang and colleagues conducted a network meta-analysis comparing targeted therapies, in combination with FUL, in the treatment of ABC. Summary-level data from PALOMA-3, MN 2 and ML-3 were included to compare PAL, ABM and RIB in terms of PFS and objective response rate. The findings showed PAL+FUL to be superior to other targeted agents [19]. Another recent study conducted by Tremblay and colleagues used MAIC methods to compare RIB in combination with LET (RIB+LET) and PAL in combination with LET. IPD from MONALEESA-2 and published summary-level data from PALOMA-2 were used to evaluate the relative impact of these therapies on PFS, and grade 3/4 adverse events. Results showed numerical, albeit not statistically significant, favorability for RIB+LET for all outcomes [20]. The current study expands on the available literature as the first study to leverage IPD from PALOMA-3 to compare OS for PAL+FUL with RIB+FUL and ABM+FUL through MAICs.
The main strength of the present MAIC analysis is the use of IPD from PALOMA-3 to reduce heterogeneity in patient populations across trials by adjusting for treatment-effect modifiers and anchoring through PBO+FUL. Comparing the therapies in a more equal setting and within a similar population, as opposed to across studies, shows that PAL+FUL is comparable to its comparators in terms of OS (Figures 3 & 4), demonstrating the importance of conducting an anchored MAIC. In addition, these pairwise comparisons were strengthened by adjustment for a clinically relevant rank-ordered set of treatment-effect modifiers unique to each comparison, taking into consideration expert opinion, extent of treatment modification and cross-trial differences. The accompanying scenario and sensitivity analyses exploring the impact of matching and adjusting on different variables allowed for a deeper understanding of the comparisons. Therefore, these MAICs allowed for a robust comparison of PAL+FUL with ABM+FUL and RIB+FUL.
Some limitations of this study should be noted. By matching and adjusting the patient population of PALOMA-3 to those of MN 2 and ML-3, ESS is reduced, which results in broader CIs than in traditional ITCs. Furthermore, despite reducing cross-trial differences by matching on eligibility criteria and adjusting on available treatment-effect modifiers, differences between trials remained. When the comparator trial included a broader population for a given characteristic (e.g., ML-3 did not require progression on or after ET in the adjuvant or metastatic setting [10]), IPD from PALOMA-3 could not be matched. Additionally, the MAIC method assumes that all treatment-effect modifiers are balanced across trials; however, variables considered in the analysis were limited by those reported in the comparator publications. Another limitation in the comparison of PAL+FUL with RIB+FUL was that there were considerable differences between the PALOMA-3 and ML-3 study populations, which resulted in fewer adjustments of treatment-effect modifiers to preserve the ESS.
Conclusion
The results of the MAIC analyses corroborate traditional ITC results and suggest that OS for PAL+FUL is similar to ABM+FUL and RIB+FUL in patients with HR+/HER2- ABC after adjusting for cross-trial differences. Furthermore, the differences in baseline characteristics between patient populations underline the importance of conducting MAIC analyses when drawing comparisons between approved CDK4/6is.
•
Hormone receptor-positive, HER2-negative is the most common breast cancer subtype. Palbociclib (PAL)+fulvestrant (FUL), ribociclib (RIB)+FUL and abemaciclib (ABM)+FUL are cyclin-dependent kinase 4/6 inhibitors recently approved in the treatment of hormone receptor-positive, HER2-negative advanced breast cancer.
•
To date, no head-to-head clinical trials have been conducted comparing the three available cyclin-dependent kinase 4/6 inhibitors, and indirect treatment comparison methods have not yet been used to compare PAL+FUL with ABM+FUL and RIB+FUL.
•
Matching-adjusted indirect comparisons (MAICs) leverage individual patient data from one data source to better adjust for cross-trial differences between studies.
•
Individual patient data were available for PALOMA-3 and summary-level data were available for MONARCH 2 and MONALEESA-3.
•
Anchored MAICs were conducted given the inclusion of a placebo+FUL as a common comparator across all three trials.
•
Primary MAIC results suggest similar overall survival (OS) when comparing PAL+FUL versus ABM+FUL (hazard ratio: 0.87; 95% CI: 0.54–1.40) and RIB+FUL (hazard ratio: 0.89; 95% CI: 0.48–1.63).
•
These MAICs allowed for the comparison of PAL+FUL versus ABM+FUL and RIB+FUL across more similar patient populations than would be possible using summary-level data alone, but some cross-trial differences remained, and matching and adjusting resulted in reduced effective sample size.
•
These results corroborate traditional indirect treatment comparison results and suggest comparable efficacy in terms of OS for PAL+FUL in comparison to ABM+FUL and RIB+FUL.
Author contributions
HS Rugo, L Zhan, E Bananis, D Mitra and C Cameron were responsible for study conception and design. A Haltner, A Tran and B Hooper were responsible for acquisition, analysis and interpretation of data. A Haltner and B Hooper were responsible for drafting the manuscript, and all authors were responsible for revising the manuscript critically. All authors were and for final approval, agree to be held accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part are appropriately investigated and resolved.
Financial & competing interests disclosure
This study was funded by Pfizer, Inc. C Cameron is an employee and shareholder of EVERSANA™. A Haltner, A Tran and B Hooper are employees of EVERSANA. EVERSANA receives consultancy fees from major pharmaceutical and device companies, including Pfizer. D Mitra, L Zhan and E Bananis are employees of and stockholders in Pfizer, Inc. HS Rugo reports sponsored research to her institution from Eisai, Roche/Genentech, Eli Lilly, Macrogenics, Merck, Novartis, OBI Pharma, Odonate, Immunomedics, Daiichi, Seattle Genetics and Pfizer, Inc.; travel support from Mylan, Pfizer, Inc. and Novartis; and consultant fees from Puma and Samsung. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Editorial support was provided by AL Mendell of EVERSANA and was funded by Pfizer.
Data sharing statement
The authors certify that this manuscript reports the secondary analysis of clinical trial data that have been shared with them, and that the use of these shared data is in accordance with the terms agreed upon their receipt. Data were provided by Pfizer.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_data.zip)
- Download
- 1.51 MB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68(6), 394–424 (2018).
2.
Ferlay J, Colombet M, Soerjomataram I et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 144(8), 1941–1953 (2019).
3.
National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: female breast cancer (2020). https://seer.cancer.gov/statfacts/html/breast-subtypes.html
4.
Thu KL, Soria-Bretones I, Mak TW, Cescon DW. Targeting the cell cycle in breast cancer: towards the next phase. Cell Cycle 17(15), 1871–1885 (2018).
5.
Finn RS, Aleshin A, Slamon DJ. Targeting the cyclin-dependent kinases (CDK) 4/6 in estrogen receptor-positive breast cancers. Breast Cancer Res. 18(1), 17 (2016).
6.
Xu H, Yu S, Liu Q et al. Recent advances of highly selective CDK4/6 inhibitors in breast cancer. J. Hematol. Oncol. 10(1), 97 (2017).
7.
United States Food & Drug Administration. Drugs@FDA: FDA-approved drugs - palbociclib (IBRANCE) (2020). www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=207103
8.
Turner NC, Ro J, André F et al. Palbociclib in hormone-receptor–positive advanced breast cancer. N. Engl. J. Med. 373(3), 209–219 (2015).
• Presents the primary outcome and baseline characteristics of the Phase III PALOMA-3 clinical trial.
9.
United States Food & Drug Administration. Drugs@FDA: FDA-approved drugs - ribociclib (KISQALI) (2020). www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=209092
10.
Slamon DJ, Neven P, Chia S et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J. Clin. Oncol. 36(24), 2465–2472 (2018).
• Outlines the primary outcome and baseline characteristics of the Phase III MONALEESA-3 clinical trial.
11.
United States Food & Drug Administration. Drugs@FDA: FDA-approved drugs - abemaciclib (VERZENIO) (2020). www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=208716
12.
Sledge GW, Toi M, Neven P et al. MONARCH 2: abemaciclib in combination with fulvestrant in women with HR+/HER2- advanced breast cancer who had progressed while receiving endocrine therapy. J. Clin. Oncol. 35(25), 2875–2884 (2017).
• Presents the primary outcome and baseline characteristics of the Phase III MONARCH 2 clinical trial.
13.
Petrelli F, Ghidini A, Pedersini R et al. Comparative efficacy of palbociclib, ribociclib and abemaciclib for ER+ metastatic breast cancer: an adjusted indirect analysis of randomized controlled trials. Breast Cancer Res. Treat. 174(3), 597–604 (2019).
14.
Turner NC, Slamon DJ, Ro J et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer. N. Engl. J. Med. 379(20), 1926–1936 (2018).
• Highlights overall survival (OS) results from the Phase III PALOMA-3 clinical trial.
15.
Sledge GW, Toi M, Neven P et al. The effect of abemaciclib plus fulvestrant on overall survival in hormone receptor–positive, ERBB2-negative breast cancer that progressed on endocrine therapy – MONARCH 2: a randomized clinical trial. JAMA Oncol. 6(1), 116–124 (2019).
•• Describes OS results from the Phase III MONARCH 2 clinical trial.
16.
Slamon DJ, Neven P, Chia S et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N. Engl. J. Med. 382(6), 514–524 (2019).
•• Describes OS results from the Phase III MONALEESA-3 clinical trial.
17.
National Institute for Health and Care Excellence. NICE DSU Technical Support Document 18: methods for population-adjusted indirect comparisons in submission to NICE (2020). http://nicedsu.org.uk/wp-content/uploads/2018/08/Population-adjustment-TSD-FINAL-ref-rerun.pdf
•• Outlines recommendations on the methods for and use of matching-adjusted indirect comparisons.
18.
Bellet M, Ahmad F, Villanueva R et al. Palbociclib and ribociclib in breast cancer: consensus workshop on the management of concomitant medication. Ther. Adv. Med. Oncol. 11, 1–43 (2019).
19.
Zhang T, Feng F, Zhao W et al. Comparative efficacy of different targeted therapies plus fulvestrant for advanced breast cancer following progression on prior endocrine therapy: a network meta-analysis. Cancer Manag. Res. 10, 5869 (2018).
20.
Tremblay G, Chandiwana D, Dolph M, Hearnden J, Forsythe A, Monaco M. Matching-adjusted indirect treatment comparison of ribociclib and palbociclib in HR+, HER2- advanced breast cancer. Cancer Manag. Res. 10, 1319 (2018).
Information & Authors
Information
Published In
Pages: 457 - 467
PubMed: 33626934
Copyright
© 2021 Hope S Rugo. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 December 2020
Accepted: 27 January 2021
Published online: 25 February 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Matching-adjusted indirect comparison of palbociclib versus ribociclib and abemaciclib in hormone receptor-positive/HER2-negative advanced breast cancer. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0272
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- K. Jhaveri, F.C. Bidard, K. Kalinsky, P. Neven, H.S. Rugo, S.M. Tolaney, L.M. Litchfield, C.C. von Laue, S. Traore, F. Sapunar, Y. Li, J. O’Shaughnessy, Imlunestrant plus abemaciclib versus fulvestrant plus abemaciclib in ER-positive, HER2-negative advanced breast cancer: an indirect treatment comparison of three phase III trials, ESMO Open, 10.1016/j.esmoop.2026.106091, 11, 3, (106091), (2026).
- Seda Kahraman, Enes Erul, Ozge Gumusay, Deniz Can Guven, Sercan Aksoy, Gul Basaran, Mustafa Seyyar, Elif Sahin, Devrim Cabuk, Ertugrul Bayram, Semra Paydas, Burcin Cakan Demirel, Arzu Yaren, Burcu Gulbagci, Ilhan Hacibekiroglu, Naziyet Kose Baytemur, Umut Demirci, Sena Ece Davarci, Hacer Demir, Eda Eylemer Mocan, Ozlem Dogan, Ebru Cilbir, Alper Yasar, Ibrahim Vedat Bayoglu, Mutlu Hizal, Erkan Kayikcioglu, Bulent Cetin, Omer Acar, Atike Pinar Erdogan, Merve Keskinkilic, Tugba Yavuzsen, Olcun Umit Unal, Funda Yilmaz, Mutlu Dogan, Sibel Oyucu Orhan, Erdem Cubukcu, Cihan Erol, Teoman Sakalar, Ozgecan Dulgar, Yusuf Karakas, Gulhan Ozkanli, Berna Bozkurt Duman, Deniz Isik, Muge Karaoglanoglu, Sadi Kerem Okutur, Nilgun Yildirim, Esra Aydin, Basak Oyan Uluc, Murat Keser, Burak Bilgin, Asude Aksoy, Onder Eren, Nurhan Onal Kalkan, Muhammed Muhiddin Er, Hakan Yucel, Veli Sunar, Nail Paksoy, Dincer Aydin, Nazim Serdar Turhal, Serkan Menekse, Engin Kut, Musa Baris Aykan, Ozlem Ozdemir, Melike Ozcelik, Yakup Iriagac, Fatih Selcukbiricik, Ali Inal, Nuri Karadurmus, Muhammed Bulent Akinci, Mehmet Ali Nahit Sendur, Real-World Treatment Efficacy of Ribociclib or Palbociclib Plus Fulvestrant in Hormone Receptor-Positive/HER2-Negative Metastatic Breast Cancer: Turkish Oncology Group (TOG) Study, Clinical Breast Cancer, 10.1016/j.clbc.2025.03.003, 25, 5, (e635-e644), (2025).
- Cecília Menezes Farinasso, Vinícius Lins Ferreira, Flávia Cordeiro Medeiros, Aline Pereira da Rocha, Patrícia do Carmo Silva Parreira, Layssa Andrade Oliveira, Lays Pires Marra, Rosa Camila Lucchetta, Haliton Alves de Oliveira, Matching-Adjusted Indirect Comparison Studies in Oncology: A Scoping Review Focused on Reporting Quality, Value in Health Regional Issues, 10.1016/j.vhri.2025.101088, 47, (101088), (2025).
- Elena Castro, Di Wang, Sarah Walsh, Samantha Craigie, Anja Haltner, Jonathan Nazari, Alexander Niyazov, Imtiaz A. Samjoo, Matching-adjusted indirect comparison of talazoparib plus enzalutamide versus abiraterone acetate and docetaxel in mCRPC, Future Oncology, 10.1080/14796694.2025.2471200, 21, 9, (1075-1084), (2025).
- Elena Castro, Di Wang, Sarah Walsh, Samantha Craigie, Anja Haltner, Jonathan Nazari, Alexander Niyazov, Imtiaz A. Samjoo, Talazoparib plus enzalutamide versus olaparib plus abiraterone acetate and niraparib plus abiraterone acetate for metastatic castration-resistant prostate cancer: a matching-adjusted indirect comparison, Prostate Cancer and Prostatic Diseases, 10.1038/s41391-024-00924-x, 28, 3, (817-827), (2024).
- Shogo Nakamoto, Tadahiko Shien, Takayuki Iwamoto, Shinichiro Kubo, Mari Yamamoto, Tetsumasa Yamashita, Chihiro Kuwahara, Masahiko Ikeda, Absolute lymphocyte count and neutrophil-to-lymphocyte ratio as predictors of CDK 4/6 inhibitor efficacy in advanced breast cancer, Scientific Reports, 10.1038/s41598-024-60101-x, 14, 1, (2024).
- Komal Jhaveri, Joyce O’Shaughnessy, Peter A. Fasching, Sara M. Tolaney, Denise A. Yardley, Vikash Kumar Sharma, Chandroday Biswas, Astrid Thuerigen, Purnima Pathak, Hope S. Rugo, Matching-adjusted indirect comparison of PFS and OS comparing ribociclib plus letrozole versus palbociclib plus letrozole as first-line treatment of HR+/HER2− advanced breast cancer , Therapeutic Advances in Medical Oncology, 10.1177/17588359231216095, 15, (2023).
- Arnaud Serret-Larmande, Belkacem Zenati, Agnès Dechartres, Jérôme Lambert, David Hajage, A methodological review of population-adjusted indirect comparisons reveals inconsistent reporting and suggests publication bias, Journal of Clinical Epidemiology, 10.1016/j.jclinepi.2023.09.004, 163, (1-10), (2023).
- Tanju Kapagan, Nilufer Bulut, Serhat Demirer, Gokmen Umut Erdem, Ribociclib-induced visual hallucination in a patient with metastatic breast cancer, Journal of Oncology Pharmacy Practice, 10.1177/10781552231180463, 29, 6, (1529-1532), (2023).
- Ernest H Law, Chris Cameron, Letter in Reply: indirect comparison of quality-of-life scores between patients with advanced breast cancer receiving palbociclib and abemaciclib in combination with fulvestrant, Journal of Comparative Effectiveness Research, 10.57264/cer-2023-0009, 12, 6, (2023).