Identifying the unmet needs of individuals with Type 2 diabetes: an international web-based survey
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To identify and understand the main unmet needs of individuals with Type 2 diabetes (T2D). Materials & methods: An online survey was conducted in Brazil, China and Russia of individuals with recently diagnosed T2D. Results: The survey, involving 300 individuals with T2D, identified a need for more information regarding food/diet and for increased awareness of T2D symptoms. While most participants (94%) had experienced symptoms prior to their diagnosis, only 55% of symptomatic individuals sought medical attention. Conclusion: Novel strategies to increase awareness of diabetes should be developed and tested, and may enable earlier diagnosis and improve patients’ quality of life.
Lay abstract
Type 2 diabetes (T2D) negatively impacts an individual’s health-related quality of life and represents a significant burden of disease worldwide. Although previous studies have examined the unmet needs of patients with diabetes, no recent studies have evaluated the needs of individuals with T2D in Brazil, China or Russia. This study used an online questionnaire to identify and understand the main unmet needs of individuals who had been recently diagnosed with T2D from these countries. Several potential needs were identified, including the need for more information and support about food and diet, a new noninvasive solution for blood glucose monitoring and increased awareness of T2D symptoms. Our study also identified possible innovative solution to address these needs.
Diabetes represents a significant global burden of disease, and Type 2 diabetes (T2D) accounts for approximately 90% of all diabetes cases worldwide [1]. Globally, an estimated 463 million people aged 20–79 years had diabetes in 2019, and this number is projected to rise to 700 million by 2045. South America, Asia and Eastern Europe are emerging as three major regions with an increasing prevalence of diabetes [1]. In Brazil, the burden attributable to diabetes increased between 1990 and 2016 by 97.2% according to total years of life lost and by 117.9% according to total years of life with disability [2]. The prevalence of diabetes in Brazil is estimated to be 11.9% when diagnosed using a combination of fasting glucose levels, an oral glucose tolerance test and self-report [3]. In China, diabetes was estimated to affect approximately 129.8 million adults (70.4 million men and 59.4 million women) in 2017 [4]. Based on a population-based study, the prevalence of diabetes in Russia is estimated to be 5.4% [5]. Brazil, China and Russia are all upper middle income countries and form part of the Brazil, Russia, India, China and South Africa (BRICS) group of countries, which represent approximately 40% of the global burden of disease [6]. In the BRICS group, Brazil, China and Russia have shown better health system performance than other countries [7].
In addition to being associated with substantial economic burden, particularly in low- and middle-income countries [8], T2D has a negative impact on patient health-related quality of life (QoL) [9], with diabetic complications, hypertension and depression associated with reduced QoL [10]. T2D may also carry stigma, particularly among individuals with a high body mass index, high glycated hemoglobin (HbA1c) levels or poor blood glucose control [11].
An individual patient’s coping mechanisms for overall acceptance of T2D and its management may influence their QoL; these mechanisms differ by sex and psychosocial factors [12]. At the time of T2D diagnosis, patients often experience several emotional reactions that affect their ability to accept their diagnosis and adjust to self-management, including denial, anger, guilt and depression [13]. It is therefore important for healthcare professionals to provide appropriate psychosocial support to patients in order to improve their ability to accept responsibility for self-management of their T2D, and to adopt specific strategies based on their patients’ emotions, with the aim of improving their QoL [13].
Several studies have previously evaluated the unmet psychosocial needs of patients with diabetes, including the Diabetes Attitudes, Wishes and Needs (DAWN) and DAWN2 studies in individuals with Type 1 diabetes and T2D [14–18] and the DIABASIS study in individuals with T2D [19]. These studies highlighted the fact that psychosocial problems are common among patients with diabetes, and that diabetes is associated with a significant burden among patients, as well as their family members and healthcare professionals [14,16–19]. In particular, the lack of adequate support from healthcare systems with regard to diabetes care and self-management appeared to contribute to the development of psychosocial issues among patients with diabetes [14,16,17,19]. For example, in the French DIABASIS study, many participants reported distress and a need for more information at the time of their diagnosis, indicating a lack of proper diabetes education [19].
Several gaps exist in the literature regarding the unmet needs of patients with T2D. Of note, no recent studies have evaluated the needs of patients with T2D in Brazil, China or Russia. There is also a need for information on the sociomedical context of T2D diagnosis and patients’ needs prior to and immediately after diagnosis.
The objectives of the current study were to identify and understand the main unmet needs of individuals with T2D from Brazil, China and Russia using a unique international web-based survey. This study was focused on: understanding the burden of T2D and its impact from the patient perspective; identifying difficulties in the patient’s journey from T2D diagnosis to management; and identifying potential solutions for use in everyday life, and evaluating the patients’ perception and level of satisfaction with these solutions. The study was preceded by qualitative research exercises used to build a deeper understanding of the patient experience and to select the most appropriate language for the questionnaire to be used in the survey. Here, we report the results of the online quantitative questionnaire.
Materials & methods
Study design
This international study was performed by STETHOS International (Sèvres, France) and included individuals with recently diagnosed T2D from Brazil, China and Russia.
The preliminary qualitative phase of the study involved two successive steps: in-depth, 60-min exploratory interviews with 14 individuals from each country, conducted over the phone or face-to-face (depending on patients’ preference) between April and May 2019, to obtain key insights regarding all aspects of the participants’ life that could be potentially impacted by T2D and its treatment; 2-h face-to-face focus groups conducted in July 2019 with 12 individuals from each country (two groups of six individuals each) to expand on the potential unmet needs.
These qualitative research exercises were used to build a 50-question questionnaire (Supplementary Table 1), with the main insights being used to test the relevance and wording of the included questions, and to ensure that the appropriate list of items was used for the closed-ended questions. The goals of the 20-min web-based questionnaire, which was used to survey 100 individuals from each country, were to: quantify the main unmet needs of individuals with T2D; test and rank the final list of actionable solutions; and fine-tune specific solutions by testing different alternatives.
Study periods
The qualitative assessments (i.e., in-depth individual interviews and focus groups) were conducted between 25 April 2019 and 29 July 2019. The quantitative online questionnaires were conducted between 13 January and 11 February 2020.
Ethical considerations
Participants provided written informed consent prior to taking part in the qualitative interviews or focus groups or in the quantitative questionnaire.
The study was conducted in accordance with the appropriate regional, national or local guidelines for noninterventional studies, and used guidelines of the International Chamber of Commerce/European Society for Opinion and Marketing Research [20], the European Pharmaceutical Market Research Association [21] and Good Pharmacoepidemiology Practices [22] as a minimum standard.
Study participants
Individuals who had been recently diagnosed with T2D (between 2014 and 2019) and were currently receiving any antidiabetic therapy were eligible to participate in the online questionnaire. Eligible participants were required to have medical documentation of their T2D disease (e.g., a current prescription for an antidiabetic agent). No additional inclusion or exclusion criteria were applied. The survey participant population was designed to have a balanced mix of age groups and of males and females.
Participants were recruited through multiple channels, including healthcare professional referrals, existing panels, medical centers, social media and word-of-mouth referral. Potential participants were administered screening questions over the phone. Each participant received €10–15 for their participation in the survey.
Participant data were anonymized prior to this analysis, and the sponsor was blinded to the questionnaire responses. The sponsor’s name was not disclosed to the participants in order to avoid research bias.
Outcomes
The following data were collected from completed online questionnaires: participant baseline characteristics; details regarding the context of their T2D diagnosis, including the symptoms they experienced and the duration of these symptoms prior to diagnosis, and diabetes knowledge prior to diagnosis; details regarding their first T2D consultation, including the type of healthcare professional they saw, the duration of the visit, the diabetes information they received and their levels of satisfaction with the information and support they were given; the unmet needs of the participants based on their feelings and concerns, their ability to accept their diagnosis and impact of their T2D diagnosis on QoL.
Participant diabetes knowledge prior to diagnosis was rated on a scale of 0–10, where 0 = ‘no knowledge’ and 10 = ‘extensive knowledge’.
Participant satisfaction regarding the amount of diabetes information they received from their healthcare professional was rated on a scale of 0–10, where 0 = ‘did not meet my expectations’ and 10 = ‘fully met my expectations’.
The impact on QoL at diagnosis, at 6 months after diagnosis and at the time of the survey was rated on a scale of -5 to +5, where -5 = negative impact, 0 = no impact and +5 = positive impact.
Statistical analysis
The quantitative survey was designed to enroll 100 individuals with T2D from each of the three countries as a sample of individuals with T2D treated with oral antidiabetic therapy.
The χ2 test for qualitative data and the Student t-test for quantitative data were used, with a significance threshold of p < 0.05. All tests were two-sided. Statistical analysis was conducted by B3 TSI company using their TRAIT software.
Results
Study population
In total, 300 individuals with recently diagnosed T2D from Brazil, China and Russia (each n = 100) completed the quantitative online questionnaire and were included in this analysis. The baseline characteristics of the participants are summarized in Table 1. Overall, participants had a mean ± standard deviation age of 53 ± 10.8 years and 58% were female. There was a higher proportion of female than male participants in Brazil and Russia, while the proportions of male and female participants in China were similar. More participants in China had HbA1c levels of >8 versus ≤8% at diagnosis, whereas similar proportions of Brazilian and Russian participants had HbA1c levels >8 and ≤8%. Overall, the most common cardiovascular comorbidities reported by survey respondents were hypertension (43%) and hypercholesterolemia (27%); 55% of participants had at least one cardiovascular comorbidity.
| Characteristic, n (%) | Total (N = 300) | Brazil (N = 100)† | China (N = 100)† | Russia (N = 100)† |
|---|---|---|---|---|
| Age, years | ||||
| – <40 | 41 (14) | 21 | 12 | 8 |
| – 40–49 | 69 (23) | 26 | 25 | 18 |
| – 50–60 | 102 (34) | 28 | 34 | 40 |
| – 61–70 | 88 (29) | 25 | 29 | 34 |
| Sex | ||||
| – Male | 125 (42) | 35 | 51 | 39 |
| – Female | 175 (58) | 65 | 49 | 61 |
| Year of diagnosis | ||||
| – 2014–2015 | 130 (43) | 45 | 49 | 36 |
| – 2016–2017 | 95 (32) | 31 | 26 | 38 |
| – 2018–2019 | 75 (25) | 24 | 25 | 26 |
| HbA1c at diagnosis | ||||
| – <8% | 91 (30) | 24 | 30 | 37 |
| – ≥8% | 104 (35) | 24 | 50 | 30 |
| – Unknown | 105 (35) | 52 | 20 | 33 |
| Antidiabetic therapy | ||||
| – Oral | 233 (78) | 70 | 76 | 87 |
| – Oral + injectable | 67 (22) | 30 | 24 | 13 |
| CV comorbidities | ||||
| – Hypertension | 130 (43) | 45 | 36 | 49 |
| – Hypercholesterolemia | 81 (27) | 26 | 22 | 33 |
| – Coronary artery disease | 14 (5) | 1 | 4 | 9 |
| – Stable angina pectoris | 9 (3) | 2 | 2 | 5 |
| Digital self-monitoring tools familiarity | ||||
| – Very familiar | 157 (52) | 59 | 50 | 48 |
| – Quite familiar | 118 (39) | 31 | 49 | 38 |
| – Not familiar | 25 (8) | 10 | 1 | 14 |
†
n and percentage values are the same as there are 100 participants from each country.
CV: Cardiovascular; HbA1c: Glycated hemoglobin.
T2D diagnosis journey
Diagnosis context
Almost all (94%) of the study participants experienced decompensated diabetes-related symptoms prior to their diagnosis (93% in Brazil, 94% in China and 96% in Russia). The most common symptoms prior to diagnosis were dry mouth (58%), excessive thirst (51%) and fatigue or drowsiness (48%; Table 2) but only 55% of all participants (65% of participants in Brazil, 55% in China and 44% in Russia) sought medical attention for their symptoms leading to diabetes diagnosis. The proportion of participants who were diagnosed after presenting with symptoms was significantly higher in Brazil than in China and Russia combined (p = 0.011).
| Symptom, n (%) | Total (N = 300) | Brazil (N = 100)† | China (N = 100)† | Russia (N = 100)† |
|---|---|---|---|---|
| Dry mouth | 174 (58) | 51 | 54 | 69‡ |
| Excessive thirst | 154 (51) | 57 | 44 | 53 |
| Fatigue/drowsiness | 144 (48) | 45 | 40§ | 59‡ |
| Frequent urination | 132 (44) | 64‡ | 39 | 29§ |
| Weakness/dizziness | 104 (35) | 42 | 15§ | 47‡ |
| Blurred vision | 99 (33) | 45‡ | 23§ | 31 |
| Increased appetite | 90 (30) | 45‡ | 22§ | 23 |
| Sudden weight loss | 68 (23) | 22 | 35‡ | 11§ |
| Trembling/sweating | 67 (22) | 24 | 13§ | 30‡ |
| Itchy skin | 50 (17) | 8§ | 22 | 20 |
| Healing issues | 43 (14) | 25‡ | 4§ | 14 |
†
n and percentage values are the same as there are 100 participants from each country.
‡
Significantly higher vs other countries combined.
§
Significantly lower vs other countries combined.
The T2D diagnosis was made by chance (i.e., either during a routine medical check-up or after self-glucometer use) in 45% of all study participants, 35% of participants in Brazil, 45% in China and 56% in Russia. Of the participants who were diagnosed by chance, a routine medical check-up led to the diagnosis in most cases (92% of those diagnosed by chance in the overall study population, 94% in Brazil, 89% in China and 93% in Russia).
Regardless of how T2D was diagnosed, only a third of participants with symptoms prior to diagnosis suspected that they had T2D, mainly because of a family history of diabetes, with the highest percentage (44%) observed in China (p = 0.007; compared with 28% in Brazil and 27% in Russia).
Participants reported an average diabetes knowledge score of 4.4 (on a scale from 0 to 10) before they were diagnosed, with less than a quarter (23%) reporting a score ≥7.
After the onset of symptoms, participants sought medical attention regarding their T2D diagnosis after a mean ± standard deviation of 11.5 ± 15.0 months (10.4 ± 13.4 months in Brazil, 11.7 ± 16.6 months in China and 12.1 ± 14.7 months in Russia). The most common reasons for not seeking medical attention immediately were that the symptoms were considered mild (43%) and a fear of diagnosis (36%).
First T2D consultation
Across all three countries, 198 (66%) participants had their first T2D consultation with a diabetes specialist and 102 (34%) participants had their first visit with a general practitioner. A specialist initiated T2D treatment in the majority of participants in China (89%) and Russia (75%); however, a significantly lower proportion of participants had their first consultation with a diabetes specialist in Brazil (34%) than in China and Russia combined (p < 0.001), reflecting country-specific diabetes care pathways.
Overall, the first T2D consultation had a mean duration of 26 min (26.3 min with specialists and 25.7 min with general practitioners). The mean duration of the first visit was significantly longer among participants in Brazil versus China and Russia (31 ± 17 vs 25 ± 17 and 22 ± 10 min, respectively; p < 0.001).
Participants reported that the quality and quantity of diabetes-related information they received at their first T2D visit either ‘met their expectations’ or ‘fully met their expectations’ (corresponding to a rating of 9 or 10, respectively) in 25% of cases for disease information, 33% for lifestyle information, 34% for treatment information and 44% for blood glucose monitoring information. Using a 0–10 scale to rate their satisfaction, participants who had their first consultation with a specialist had significantly higher mean satisfaction scores for lifestyle (7.3 vs 6.7, p = 0.047) and blood glucose monitoring (7.8 vs 6.9; p = 0.004) information versus those who saw a general practitioner (Figure 1A); mean satisfaction scores for disease information (6.8 vs 6.2) and treatment information (7.4 vs 6.8) were similar between healthcare professional types. By country, significantly lower mean satisfaction scores were reported for disease information in Russia versus Brazil and China (6.1 vs 6.8 and 7.0, respectively; p = 0.011); mean satisfaction scores were similar across countries for blood glucose information (7.1–7.7), lifestyle information (6.8–7.3) and treatment information (6.9–7.3; Figure 1B).

Figure 1. Participant satisfaction.
Level of satisfaction of participants regarding the information received at the time of Type 2 diabetes diagnosis (A) by whether the first visit was conducted by a general practitioner or a specialist and (B) by country.
*Value is significantly lower versus specialists.
†Percentage is significantly lower versus other countries combined.
Overall, 57% participants were either ‘satisfied’ or ‘very satisfied’ (corresponding to a rating of 9 or 10, respectively) with the information and support they received at their first T2D consultation. Of those who saw a specialist (n = 198), 54% were satisfied or very satisfied with their consultation. Of the 102 participants who saw a general practitioner, 62% were either satisfied or very satisfied. In both situations, the proportion of patients who were satisfied or very satisfied with their consultation was significantly higher in Brazil than in China and Russia combined (for specialists: 94 vs 52 and 40%, respectively; p < 0.001; for general practitioners: 75 vs 36 and 40%, respectively; p < 0.001). On average, satisfied or very satisfied patients had longer first visits (30 min) compared with dissatisfied patients (17 min).
Participants’ feelings
At the time of their T2D diagnosis, the majority of all participants reported having felt apprehension or fear (51%) and denial or difficulty with acceptance of their diagnosis (32%; Figure 2). The most common fears and concerns at diagnosis were the risk of severe complications (63%) and multiple food restrictions (47%; Figure 3). The main diabetic complications of concern were vision impairment (67%), diabetic foot (60%) and heart disease (40%).
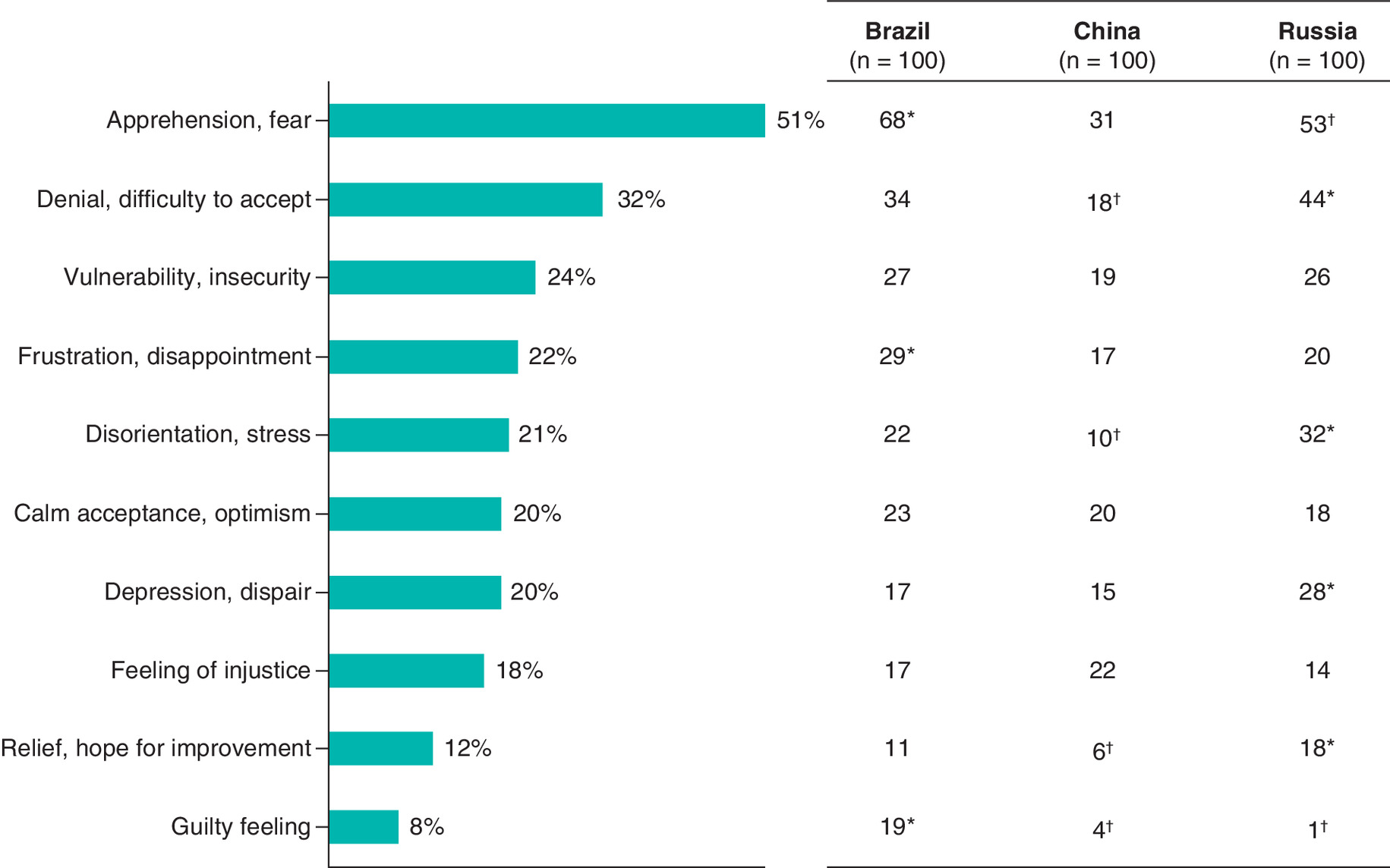
Figure 2. Most common emotions of participants at Type 2 diabetes diagnosis in the overall study population (bar graph) and in each country (table).
*Percentage is significantly higher versus other countries combined.
†Percentage is significantly lower versus other countries combined.

Figure 3. Most common fears and concerns of participants at Type 2 diabetes diagnosis.
*Percentage is significantly higher versus other countries combined.
†Percentage is significantly lower versus other countries combined.
Approximately two-thirds of all participants said they had accepted their T2D diagnosis either immediately (27%) or within a few days (20%) or weeks (19%). The remaining participants accepted their diagnosis after a few months (25%) or years (4%), or had still not accepted their diagnosis (5%). Of note, participants with a shorter time to acceptance of T2D diagnosis (within a few weeks) had a significantly greater diabetes-related knowledge prior to diagnosis (4.7/10 on average) than those who accepted the disease within a few months or years (3.9/10; p = 0.0137).
Impact on QoL
On a scale of -5 to +5, T2D diagnosis had a negative impact on QoL (score of -5/-4 or -3/-2) in 44% of all participants immediately after their diagnosis, 29% at 6 months after diagnosis and 19% at the time of the survey. The proportion of participants who reported QoL recovery or improvement (score of -1/+1, +2/+3 or +4/+5) increased from 56% immediately after diagnosis to 71% at 6 months and 81% at the time of the survey. Mean QoL scores were significantly lower in Russia than Brazil or China immediately after diagnosis (-1.6 vs -0.1 and -1.0; p = 0.001), at 6 months (-0.7 vs +0.9 and 0; p < 0.001), and at the time of the survey (-0.3 vs +1.8 and +0.3; p < 0.001).
Unmet needs in T2D
The main unmet needs identified by all participants were more information and support regarding food and diet (36%), a new solution to monitor blood glucose levels (36%) and increased awareness of T2D to facilitate earlier diagnosis (26%; Figure 4). Among those who identified a need for a new solution to monitor blood glucose levels, many participants expressed a need for a noninvasive, painless device (43%) and real-time tracking of blood glucose levels (36%).
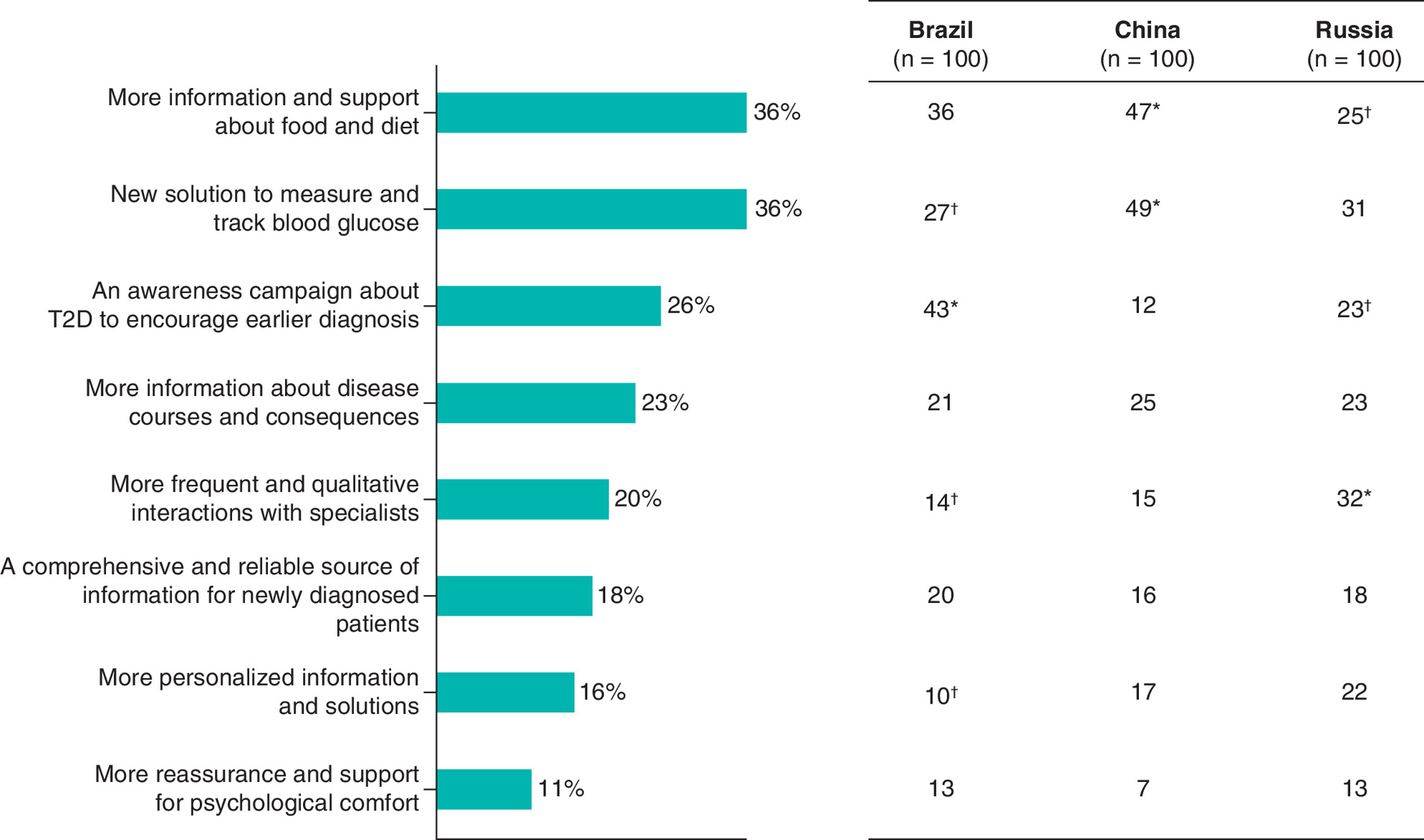
Figure 4. Main unmet needs of participants with Type 2 diabetes in the overall study population (bar graph) and in each country (table).
*Percentage is significantly higher versus other countries combined.
†Percentage is significantly lower versus other countries combined.
T2D: Type 2 diabetes.
In the first few months after their T2D diagnosis, the majority of all participants (84%) felt supported by their family and friends and 55% felt supported by their healthcare professional. Besides healthcare professionals, the main source of diabetes-related information for all participants was their family and friends (59%), followed by the internet (48%), medical television programs (25%), medical literature and press (15%) and social networks (11%). Participants used these sources mostly to look for information about food and diet (71%) and long-term disease complications (49%).
According to all participants, the most appropriate format for providing diabetes-related information and support was a smartphone application (52%), followed by patient training events (18%), a web site (17%) and printed material (13%). Similarly, most participants in Brazil and China stated that a smartphone application was the best format (59 and 65%, respectively), while opinion was more divided in Russia (29% for smartphone application, 28% for printed material, 25% for website and 18% for patient training).
More than half of all participants (58%) stated that the most appropriate channel for providing information about a new solution for individuals living with diabetes was through their healthcare professional. The majority of participants in China (57%) and Russia (67%) also stated that this information should be provided by their healthcare professional, and participants in Brazil stated that new information should be disseminated by their healthcare professional (49%) or through social networks (46%).
If a new digital solution providing diabetes information and support were to become available, most participants favored an “all-in-one” comprehensive approach with information about diabetes and other conditions associated with cardiovascular risk (85% of all participants, 89% in Brazil, 86% in China and 80% in Russia).
Discussion
This international web-based survey identified several potential patient-related concerns and unmet needs among individuals with T2D in Brazil, China and Russia.
With regard to the T2D diagnosis context, almost half of the participants (45%) were diagnosed by chance during a routine check-up, while 55% of participants sought medical attention because of diabetes-related symptoms (mainly dry mouth, excessive thirst and fatigue). Despite 94% of participants having symptoms prior to diagnosis, only a third of these participants suspected diabetes, primarily because of a family history of the disease. On average, participants waited almost 1 year after developing symptoms before seeking medical attention, mainly because they felt their symptoms were not severe enough or they were afraid of the diagnosis. These findings indicate that there is a need to disseminate general diabetes information to increase overall awareness of symptoms and the importance of visiting a healthcare professional as soon as they develop, and to address the fear induced by a diabetes diagnosis in some people.
At the time of their T2D diagnosis, most participants felt fear and apprehension, and had difficulty accepting their disease. The participants’ main concerns were the development of severe complications, including vision impairment, diabetic foot and heart disease, and multiple food restrictions, while chronic kidney disease was mentioned as a concern by a minority of patients. After diagnosis, participants reported using the internet to seek further diabetes-related information, mainly about food and diet advice and long-term disease complications.
When comparing participants’ responses between countries, more participants in Brazil than in China and Russia sought medical attention for diabetes-related symptoms, while more participants in Russia than in Brazil and China were diagnosed with T2D by chance. The proportion of participants who had their first consultation with a diabetes specialist was lower in Brazil than in other countries; however, the mean duration of the first visit was longer in Brazil than in other countries. More participants in Brazil versus other countries combined were satisfied overall with their first T2D consultation. Participants reported lower mean satisfaction scores for the amount of disease information in Russia than in other countries. Mean QoL scores were lower in Russia versus other countries immediately after diagnosis, at 6 months after diagnosis and at the time of the survey.
The participants’ perspectives in our study are consistent with and add to those of previous studies that examined the unmet needs of patients with diabetes. In the cross-national DAWN study (which included patients from 13 countries including Australia, India, Japan, the USA and a number in Europe), the majority of participants reported diabetes-related psychological problems, including anxiety, depression and stress, as well as poor psychological well-being [17]. Many healthcare professionals could not identify these psychological problems or provide the support to their patients [17]. Similarly, in the DAWN2 study (of patients in 18 countries), healthcare professionals reported that access to quality care was poor and more diabetes-related training is needed [14]. Diabetes was associated with physical, emotional, social and financial impact on the participants’ lives and presented many psychosocial challenges. The majority of participants did not feel that they received sufficient support from a healthcare professional, despite this being a high priority for most. The DAWN2 study identified unmet needs in the availability of psychosocial support, self-management education and person-centered diabetes care [14,16]. Participants also reported several challenges with regard to the impact of diabetes on work (and vice versa) [18]. In the DIABASIS study, the shortcomings of the diabetes healthcare system in France were highlighted by most participants, who reported high levels of distress at the time of their diagnosis, as well as the need for more information to help cope with this distress [19]. The importance of educational activities and the need for information at disease onset were under-recognized and routine healthcare professional visits were too short for in-depth counseling. Similar to the DAWN studies, many participants reported feelings of anxiety, depression and helplessness, fear, dismay or anger [19].
In our study, the main potential unmet needs were more information and support about food and diet, a new solution for noninvasive monitoring blood glucose levels and increased awareness of T2D symptoms to possibly allow for earlier diagnosis. Although the benefits of self-monitoring of blood glucose in patients with T2D who are not receiving insulin are questionable [23,24], noninvasive monitoring devices may address a lack of adherence due to the pain of invasive monitoring techniques [25]. In our study, most participants (78%) were not receiving injectable therapy at the time of the survey; however, our results indicate that the participants recognized the potential benefits of a noninvasive, painless device for blood glucose monitoring, particularly once insulin therapy was ultimately needed. The participants also expressed a need for consistent and detailed guidelines and support regarding their food and diet.
Our study also identified possible opportunities for innovative solutions to address these unmet needs. A smartphone application was considered the most appropriate format for providing a new solution for individuals living with T2D and other conditions associated with increased cardiovascular risk, and if available, should be recommended by healthcare professionals. The participants favored an ‘all-in-one’ approach that covers multiple topics related to disease management, including disease information, food and diet, blood glucose control, lifestyle, treatment and potential complications, rather than a diabetes-only option.
The main strengths of our study were its large study population of individuals with confirmed T2D diagnosis from three countries and its robust three-phase methodology. Using a sequential approach, our study developed a quantitative questionnaire that was built entirely from participant feedback, allowing us to form reliable conclusions from our findings. In addition, the multi-channel method of recruitment allowed us to have a varied sample of the T2D population. Participants responding to an online questionnaire are probably more willing to share their experiences as they feel free to express themselves anonymously without their doctor’s involvement. As this was a self-reported questionnaire, the main study limitations were the possibility of bias in the participant responses (i.e., sampling bias, nonresponse bias and recall bias), which is common in web-based surveys and the exclusion of individuals diagnosed with T2D before 2014. There was also the possibility of selection bias, as participants responding to an online questionnaire may be more likely to use a smart phone application for disease information and management than the general population. Another limitation is that the diagnosis and clinical data collected were not provided by healthcare professionals but rather by participants themselves (i.e., current medical prescription, diagnosis evidence), except for the individuals with T2D recruited via their practicing doctor (e.g., about 40% in Brazil), which may lead to recall bias. Further, the samples from each country were not fully representative of the general population of patients with diabetes in each country, in particular regarding the male/female ratio in the samples from China and Russia [4,5] and the age groups of the sample from Brazil [3]. However, the participant baseline characteristics were generally well balanced between countries, thus reducing the risk of major bias when comparing countries. Finally, individuals who do not have computer or internet access were excluded, which may lead to a potential recruitment bias.
Conclusion
This international web-based survey identified several potential unmet needs among individuals with T2D in Brazil, China and Russia, including the need for more information and support regarding food and diet, the need for a new solution for noninvasive monitoring blood glucose levels, and the need for increased awareness of T2D symptoms, which may facilitate earlier diagnosis. Several possible innovative solutions were identified, although further research is needed to confirm whether these solutions can help to address these needs.
•
Several gaps exist in the literature regarding the unmet needs of patients with Type 2 diabetes (T2D), particularly prior to and immediately after their diagnosis.
•
We report the results of the final phase of an online quantitative questionnaire conducted with 300 individuals with newly diagnosed T2D in Brazil, China and Russia.
•
Most participants (94%) experienced diabetes-related symptoms prior to diagnosis, but a T2D diagnosis was suspected in only a third of these participants.
•
Mean satisfaction scores were lower for disease information received at the time of T2D diagnosis by healthcare professional in Russia than in other countries.
•
Mean quality of life scores were lower in Russia than in other countries immediately after and at 6 months after diagnosis and at the time of the survey.
•
Several unmet needs were identified, including the need for more information and support about food and diet, a new solution for monitoring blood glucose levels and an increased awareness of T2D to allow for earlier diagnosis.
•
Opportunities for innovative therapeutic solutions to address the unmet needs in individuals with T2D were identified.
Author contributions
E Court was involved in the conception and design of the study, reading and revising the manuscript drafts, and approval of the final manuscript. JF Raposo, MV Shestakova, J Lu and AY Mayorov were involved in reviewing and analyzing the study results, reading and revising the manuscript drafts, and approval of the final manuscript.
Acknowledgments
The authors thanked S Greig of Springer Healthcare Communications who prepared the outline and first draft of this manuscript.
Financial & competing interests disclosure
The study was performed by STETHOS International (Sèvres, France) funded by Servier. E Court is an employee of Servier. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
This medical writing assistance was funded by Servier.
Ethical conduct of research
Participants provided written informed consent prior to taking part in the qualitative interviews or focus groups or in the quantitative questionnaire. The study was conducted in accordance with the appropriate regional, national or local guidelines for noninterventional studies and used guidelines of the International Chamber of Commerce/European Society for Opinion and Marketing Research (International Chamber of Commerce 2016), the European Pharmaceutical Market Research Association (European Pharmaceutical Market Research Association 2019) and Good Pharmacoepidemiology Practices (International Society for Pharmacoepidemiology 2015) as a minimum standard.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 17.12 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
International Diabetes Federation. IDF Diabetes Atlas (9th Edition). IDF, Brussels, Belgium (2019).
2.
GBD 2016 Brazil Collaborators. Burden of disease in Brazil, 1990–2016: a systematic subnational analysis for the Global Burden of Disease Study 2016. Lancet 392(10149), 760–775 (2018).
3.
Telo GH, Cureau FV, De Souza MS, Andrade TS, Copes F, Schaan BD. Prevalence of diabetes in Brazil over time: a systematic review with meta-analysis. Diabetol. Metab. Syndr. 8(1), 65 (2016).
4.
Li Y, Teng D, Shi X et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ 369, m997 (2020).
5.
Dedov I, Shestakova M, Benedetti MM, Simon D, Pakhomov I, Galstyan G. Prevalence of Type 2 diabetes mellitus (T2DM) in the adult Russian population (NATION study). Diabetes Res. Clin. Pract. 115, 90–95 (2016).
6.
Acharya S, Barber SL, Lopez-Acuna D et al. BRICS and global health. Bull. World Health Organ. 92(6), 386–386A (2014).
7.
Romaniuk P, Poznanska A, Brukalo K, Holecki T. Health system outcomes in BRICS countries and their association with the economic context. Front. Public Health 8, 80 (2020).
8.
Seuring T, Archangelidi O, Suhrcke M. The economic costs of Type 2 diabetes: a global systematic review. Pharmacoeconomics 33(8), 811–831 (2015).
• Systematic review of the global evidence on the costs of Type 2 diabetes (T2D), revealing the large economic cost of the disease in low-and middle-income countries (LMICs).
9.
Schram MT, Baan CA, Pouwer F. Depression and quality of life in patients with diabetes: a systematic review from the European depression in diabetes (EDID) research consortium. Curr. Diabetes Rev. 5(2), 112–119 (2009).
10.
Jing X, Chen J, Dong Y et al. Related factors of quality of life of Type 2 diabetes patients: a systematic review and meta-analysis. Health Qual. Life Outcomes 16(1), 189 (2018).
• Recent systematic review and meta-analysis of data from over 57,000 patients that identified the disease-related factors having the greatest impact on quality of life in patients with T2D.
11.
Liu NF, Brown AS, Folias AE et al. Stigma in people with Type 1 or Type 2 diabetes. Clin. Diabetes 35(1), 27–34 (2017).
12.
Mccoy MA, Theeke LA. A systematic review of the relationships among psychosocial factors and coping in adults with Type 2 diabetes mellitus. Int. J. Nurs. Sci. 6(4), 468–477 (2019).
13.
Kalra S, Jena BN, Yeravdekar R. Emotional and psychological needs of people with diabetes. Indian J. Endocrinol. Metab. 22(5), 696–704 (2018).
14.
Funnell MM, Bootle S, Stuckey HL. The Diabetes Attitudes, Wishes and Needs second study. Clin. Diabetes 33(1), 32–36 (2015).
•• Follow-up to the Diabetes Attitudes, Wishes and Needs study, which aimed to determine whether progress had been made in diabetes self-care since the publication of the original study.
15.
Peyrot M, Burns KK, Davies M et al. Diabetes Attitudes Wishes and Needs 2 (DAWN2): a multinational, multi-stakeholder study of psychosocial issues in diabetes and person-centred diabetes care. Diabetes Res. Clin. Pract. 99(2), 174–184 (2013).
16.
Tarkun I, Dumanli Ozgoksu S. Attitudes, wishes, and needs of diabetes patients and their relatives: Turkish data from the DAWN2 study. Turk. J. Med. Sci. 47(2), 447–454 (2017).
17.
Peyrot M, Rubin RR, Lauritzen T, Snoek FJ, Matthews DR, Skovlund SE. Psychosocial problems and barriers to improved diabetes management: results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diabet. Med. 22(10), 1379–1385 (2005).
•• Large, international, interview-based study of patients with diabetes (Type 1 or 2) and healthcare providers involved in their care, which aims to identify patient psychosocial problems/barriers to effective self-care and providers’ ability to address these issues.
18.
Cleal B, Willaing I, Stuckey H, Peyrot M. Work matters: diabetes and worklife in the second Diabetes Attitudes, Wishes and Needs (DAWN2) study. Diabetes Res. Clin. Pract. 150, 90–98 (2019).
• Recent sub-analysis of data from the Diabetes Attitudes, Wishes and Needs 2 study, which assessed the impact of diabetes on work-life in adults.
19.
Mosnier-Pudar H, Hochberg G, Eschwege E et al. How do patients with Type 2 diabetes perceive their disease? Insights from the French DIABASIS survey. Diabetes Metab. 35(3), 220–227 (2009).
• Large, questionnaire-based study assessing disease knowledge among French patients with T2D.
20.
International Chamber of Commerce. ICC/ESOMAR international code on market, opinion and social research and data analytics (2016). www.esomar.org/uploads/pdf/professional-standards/ICCESOMAR_Code_English_.pdf
21.
European Pharmaceutical Market Research Association. EphMRA code of conduct 2019 (2019). www.ephmra.org/media/2811/ephmra-2019-code-of-conduct-doc-f.pdf
22.
International Society for Pharmacoepidemiology. Guidelines for good pharmacoepidemiology practices (GPP) (2015). www.pharmacoepi.org/resources/policies/guidelines-08027/
23.
Benhalima K, Mathieu C. The role of blood glucose monitoring in non-insulin treated Type 2 diabetes: what is the evidence? Prim. Care Diabetes 6(3), 179–185 (2012).
24.
Xu Y, Tan DHY, Lee JY. Evaluating the impact of self-monitoring of blood glucose frequencies on glucose control in patients with Type 2 diabetes who do not use insulin: a systematic review and meta-analysis. Int. J. Clin. Pract. 73(7), e13357 (2019).
25.
Bolla AS, Priefer R. Blood glucose monitoring- an overview of current and future non-invasive devices. Diabetes Metab. Syndr. 14(5), 739–751 (2020).
Information & Authors
Information
Published In
Pages: 613 - 624
PubMed: 33769070
Copyright
© 2021 Emilie Court. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 8 December 2020
Accepted: 12 February 2021
Published online: 26 March 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Identifying the unmet needs of individuals with Type 2 diabetes: an international web-based survey. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0271
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Woorim Kim, Kyujin Chang, Soon Young Lee, Yeong Jun Ju, Association between diabetic patients’ satisfaction with local medical services and experiences of unmet healthcare needs, BMC Health Services Research, 10.1186/s12913-026-14276-w, (2026).
- Michelle D.S. Boakye, Rockson Ansong, Eyitayo O. Owolabi, Shammah O. Omololu, Hanan Abdelrahman, Christina R. Whitehouse, Understanding Immediate Concerns at Type 2 Diabetes Diagnosis: A Qualitative Comparison of Perspectives From Newly Diagnosed Adults and Clinicians, Clinical Diabetes, 10.2337/cd25-0049, 43, 5, (746-756), (2025).
- Elisabetta Maida, Paola Caruso, Simona Bonavita, Gianmarco Abbadessa, Giuseppina Miele, Miriam Longo, Lorenzo Scappaticcio, Eleonora Ruocco, Francesca Trojsi, Katherine Esposito, Luigi Lavorgna, Maria Ida Maiorino, Digital Health in Diabetes Care: A Narrative Review from Monitoring to the Management of Systemic and Neurologic Complications, Journal of Clinical Medicine, 10.3390/jcm14124240, 14, 12, (4240), (2025).
- Mengistie Yirsaw Gobezie, Nuhamin Alemayehu Tesfaye, Tewodros Solomon, Mulat Belete Demessie, Teklehaimanot Fentie Wendie, Yaschilal Muche Belayneh, Assefa Mulu Baye, Minimize Hassen, The unmet drug-related needs of patients with diabetes in Ethiopia: a systematic review and meta-analysis, Frontiers in Endocrinology, 10.3389/fendo.2024.1399944, 15, (2024).
- Miroslava Nedyalkova, Julia Romanova, Ludmila Naneva, Vasil Simeonov, Developing a questionnaire for diabetes mellitus type 2 risk effects and precondition factors – multivariate statistical paths, Physical Sciences Reviews, 10.1515/psr-2021-0158, 8, 10, (3629-3641), (2022).
- Julio Rosenstock, Stefano Del Prato, Basal weekly insulins: the way of the future!, Metabolism, 10.1016/j.metabol.2021.154924, 126, (154924), (2022).