Comparative efficacy of dabrafenib + trametinib versus treatment options for metastatic melanoma in first-line settings
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: The objective was to systematically review the literature and assess the relative efficacy of agents approved in first-line settings via network meta-analysis. Materials & methods: A literature review was conducted via searching different medical databases. The eligibility criteria included Phase II or III randomized controlled trials that had enrolled treatment-naive adult patients with advanced/metastatic melanoma. Results: The network meta-analysis results suggested that dabrafenib + trametinib significantly prolongs the survival outcomes compared with the monotherapies and had comparable efficacy profile compared with encorafenib + binimetinib and cobimetinib + vemurafenib. In comparison with immunotherapies, the results varied for progression-free survival and overall survival. Conclusion: Long-term survival data of dabrafenib + trametinib establishes the combination as one of the preferred treatment options for previously untreated melanoma patients.
Melanoma represents only 3–5% of all skin cancers, but is an aggressive form of skin cancer that may spread to any organ. Melanoma is reported as the 19th most common cancer worldwide, with estimated age-standardized incidence rates of 3.1 per 100,000 individuals [1]. As per the SEER estimates, the incidence of malignant melanoma is rapidly increasing in the US, being the fifth most common malignancy accounting for 5.6% of all new cancer cases [2]. In the US, the rate of new cases (2013–2017) of melanoma of skin was estimated at 22.7 per 100,000 men and women per year, while the death rate (2014–2018) was 2.3 per 100,000 men and women per year [2]. Cutaneous melanoma has the greatest mortality rate among all forms of melanoma, and is one of the malignancies with the highest potential of dissemination. The prognosis of patients with metastatic melanoma is grim, with a 5-year survival rate between 5 and 19%, and is dictated by the location and the number of metastases [3]. Mutations in the v-Raf murine sarcoma viral oncogene homolog B gene (BRAF) gene, which codes for a serine/threonine kinase involved in the MAPK pathway, are the most frequent mutations observed in melanoma (40–66%) and occur early in the pathogenesis of the disease [4–9]. Of the activating BRAF mutations, the BRAF V600E mutation (valine at the 600 position exchanged for glutamic acid) is reported in about 90% of cases, while the BRAF V600K mutation is reported in 5–6% of cases [10]. The BRAF V600E mutation confers the ability of BRAF to activate mitogen-activated protein kinase (MEK, the only known downstream target of BRAF) independent of RAS.
Thus, targeted inhibition of both BRAF and MEK has been of significant therapeutic interest for the treatment of melanoma, both as adjuvant and metastatic therapies [4]. Such interest has been heightened by evidence suggesting that patients with the BRAF mutation have a worse prognosis than those with the wild-type gene. Concomitant inhibition of BRAF and MEK may prevent or delay the drug resistance that arises through reactivation of the MAPK pathway. In preclinical studies, combining a BRAF inhibitor and a MEK inhibitor blocked rebound phospho-ERK (pERK) signaling in BRAF-mutant melanoma cells and enhanced cell death [11].
Since 2011, a number of targeted therapies, including BRAF inhibitors and MEK inhibitors, and checkpoint inhibitors, such as anticytotoxic T-lymphocyte-associated antigen 4 (anti-CTLA-4) antibodies and antiprogrammed (anti-PD-1) antibodies, have been approved by the US FDA in the US because of their significant survival benefit, and have emerged as new standard therapies. The treatment landscape for metastatic melanoma is changing rapidly with the recent development of newer agents that have demonstrated better efficacy than traditional chemotherapy. The first generation of agents (i.e., vemurafenib, dabrafenib and ipilimumab) demonstrated significantly improved response rates and outcomes compared with conventional therapies. Vemurafenib and dabrafenib were developed to inhibit BRAF V600 mutations. Despite high initial response rates, half of the patients treated with BRAF-targeted monotherapies relapse within 6 months due to development of drug resistance. Hence, BRAF/MEK inhibitor combination therapies with dabrafenib + trametinib, vemurafenib + cobimetinib, and the recently approved encorafenib + binimetinib improved efficacy outcomes in patients with metastatic melanoma in first-line settings. Immune checkpoint inhibitors have transformed the treatment algorithm for unresectable or metastatic disease, notably the PD-1 inhibitors pembrolizumab and nivolumab and the combined use of nivolumab and ipilimumab.
The National Comprehensive Cancer Network (NCCN) guidelines recommend BRAF/MEK inhibitor combination therapies of dabrafenib + trametinib, vemurafenib + cobimetinib and encorafenib + binimetinib for patients with BRAF V600 mutations. The guidelines also recommend immunotherapy agents (i.e., pembrolizumab, nivolumab and nivolumab + ipilimumab) for the treatment of patients with metastatic melanoma in first-line settings [12]. However, the European Society for Medical Oncology (ESMO) guidelines recommend immunotherapies upfront (i.e., pembrolizumab, nivolumab, and nivolumab + ipilimumab) in first-line settings irrespective of the BRAF mutation status, and BRAF/MEK inhibitor combination therapies of dabrafenib + trametinib, vemurafenib + cobimetinib and encorafenib + binimetinib are recommended for patients who are not suitable for immunotherapies [13].
The first-line treatment options considered for the review included targeted therapies as monotherapies (e.g., dacarbazine, vemurafenib and dabrafenib) or combination (e.g., dabrafenib + trametinib, encorafenib + binimetinib and cobimetinib + vemurafenib) and immune checkpoint inhibitors (e.g., nivolumab, pembrolizumab and nivolumab + ipilimumab). Head-to-head evidence from the RCTs between the first-line agents in metastatic melanoma is lacking and thus the optimal treatment is unknown. An understanding of the comparative efficacy of agents is important for evidence-based medicine and help in decision making for clinicians and policy-makers. Network meta-analyses (NMA) is an effective technique to assess the relative efficacy of therapeutic agents in absence of head-to-head trials. Hence, NMA methodology was utilized to achieve the estimates of the relative treatment effect of dabrafenib + trametinib versus all possible comparisons. The review also reported the qualitative safety data reported across the trials.
Materials & methods
Literature search
A systematic literature review (SLR) was conducted via a search of key biomedical databases, in other words, MEDLINE® and Embase®, and the Cochrane Central Register of Controlled Trials (CENTRAL) in May 2020. MEDLINE In-Process was also searched to ensure that nonindexed citations were retrieved. Search terms were related to each specific facet of disease, study design and interventions. The searches were limited to English-language articles only. Additionally, proceedings from selected conferences (American Society of Clinical Oncology, International Melanoma Congress of the Society for Melanoma Research and European Society for Medical Oncology) during the period from 2017–2019 were searched for abstracts to retrieve the latest studies that had not yet been published in journals as full-text articles or to supplement results of previously published studies.
Study selection
A protocol was prepared prior to conducting the systematic review defining the inclusion and exclusion criteria. The SLR included Phase II or III RCTs that had enrolled treatment-naive adult patients with unresectable lymph node metastasis (American Joint Committee on Cancer TNM stage IIIC) or distant metastatic (American Joint Committee on Cancer tumor [T] nodes [N] metastases [M] stage IV) melanoma. At least one of the interventions compared in the trial was either a targeted inhibitor (BRAF or MEK or a combination of both) or an immune checkpoint inhibitor (CTLA-4 or PD-1 or a combination of both). Although the population of interest was patients with BRAF-mutated melanoma, no restriction was applied on study eligibility by BRAF mutation status as immunotherapies have largely been assessed either in a mixed population or in a BRAF wild-type population. To identify relevant publications meeting the inclusion criteria, citations were first screened based on the abstract and title citation by two independent reviewers, and any discrepancies between the reviewers were reconciled by a third independent reviewer. Thereafter, the eligibility criteria were applied to the full text of the articles.
Data extraction
Studies that met the eligibility criteria at the second screening stage were extracted. Data extraction was done related to study and patient characteristics as well as treatments and outcomes (progression-free survival [PFS], overall survival [OS] and adverse events [AEs]). For PFS and OS, the hazard ratio (HR) and CIs were extracted wherever reported. The longest follow-up data for PFS and OS were extracted from multiple citations of the same trial and utilized for analysis.
Data analysis
The NMA allows estimation of the relative treatment effect of multiple interventions based on both head-to-head comparisons within trials and indirect comparisons across trials simultaneously. It is an extension of the classical pairwise meta-analysis. The general idea was to include all evidence at hand about a specific research question in one single model. An NMA can include all treatments as well as interventions that have not been investigated head-to-head using Bayesian method.
A set of Bayesian, hierarchical models were developed to perform the NMA analyses. Bayesian NMAs were conducted to estimate the HRs with corresponding 95% credible interval for PFS and OS. Analyses were conducted based on the reported HRs between trial arms. In the case of multi-arm trials (i.e., trials with three or more interventions), adjustments were made to reflect the correlations between relative treatment effects by converting log-HRs to log-hazards. Both fixed-effect and random-effect models were fitted to the data using the Markov Chain Monte Carlo methods and conducted under the Bayesian paradigm. The models were adapted from National Institute for Health and Care Excellence technical support document 2 [14]. A three-chain model with noninformative priors was run for 100,000 iterations with a burn-in of 30,000 model iterations. Model fit was assessed according to the deviance information criteria (DIC).
Consistency & heterogeneity test
Inconsistency was evaluated by edge-splitting, an approach that estimates relative treatment effects based on direct evidence (i.e., pairwise comparisons between treatment nodes) and indirect evidence (i.e., relative treatment effects estimated using only indirect evidence) separately. If a model is consistent, the direction and statistical importance of the effect will be maintained. Models were programmed in R v3.6.2 (www.r-project.org) using R2OpenBUGS package and Rstudio (version 1.1.456).
Study and patient characteristics that may impact treatment effects were assessed. Heterogeneity arises when treatment effects differ across studies due to observable or unobservable differences in design or population. Observable heterogeneity can be assessed by estimating the effect of study-level covariates on treatment effects. First, heterogeneity was qualitatively assessed based on the inclusion and exclusion criteria of each study. Thereafter, a meta-regression analysis was performed for the baseline characteristics of Eastern Cooperative Oncology Group performance status (ECOG PS), LDH level and BRAF mutation status. A meta-regression analysis can help explain between-study heterogeneity and minimize inconsistency.
Results
Evidence identified
Figure 1 presents the preferred reporting items for systematic reviews and meta-analyses diagram depicting the flow of studies included at each step of the review. A systematic search of the databases yielded 9826 separate references, of which 1332 references were found to be duplicates and were removed. Following the first pass of the remaining 8494 citations, 564 potentially relevant references were identified for the second stage of screening. Of these 564 citations, 404 citations were excluded for not meeting the eligibility criteria. Following full-text screening and linking of multiple publications, 15 studies (reported in 163 publications) were included for extraction. Of these 15 studies, eight studies assessed targeted therapies (monotherapies or combination therapies), while seven studies assessed immunotherapies (monotherapies, combination with chemotherapy or PD-1 inhibitor + CTLA-4 inhibitor).

Figure 1. Preferred reporting items for systematic reviews and meta-analysis study flow diagram.
CSR: Clinical study report.
Dabrafenib 150 mg twice daily (b.i.d.) + trametinib 2 mg once daily (o.d.) was assessed in three trials (COMBI-v [15], COMBI-d [16] and BRF113220 [17]), while one trial each assessed encorafenib 450 mg + binimetinib 45 mg (COLUMBUS [18]) and cobimetinib 60 mg o.d. + vemurafenib 960 mg b.i.d. (coBRIM [19]). One trial each assessed trametinib 2 mg od versus chemotherapy (METRIC), dabrafenib 150 mg b.i.d. versus dacarbazine 1000 mg/m2 (BREAK-3 [20]) and vemurafenib 960 mg b.i.d. versus dacarbazine 1000 mg/m2 (BRIM-3 [21]).
Among the immunotherapies, nivolumab 1 mg/kg every 3 weeks (q3w) + ipilimumab 3 mg/kg q3w was assessed in two trials (CheckMate 067 [22] and CheckMate 069 [23]) and ipilimumab 10 mg/kg q3w + dacarbazine 850 mg/m2 intravenous q3w was assessed in two trials (CA184-013 [24] and CA184-024 [25]). One trial assessed nivolumab 3 mg/kg every 2 weeks (q2w) versus dacarbazine 1000 mg/m2 q3w (CheckMate 066 [26]), while one trial assessed ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg [27]. In KEYNOTE-006, outcomes were reported for two doses of pembrolizumab (10 mg/kg q3w or 10 mg/kg q2w) versus ipilimumab 3 mg/kg, but a recent publication reported results for pooled doses of pembrolizumab in treatment-naive patients [28]; hence, the HRs for the pooled doses were utilized for the NMA.
Study & patient characteristics
Table 1 presents the details of RCTs and patient baseline characteristics. All the included studies were Phase III studies except three trials, BRF113220 [17], CA184-013 [24] and CheckMate 069 [23], which were Phase II studies. All the included studies had a multicenter-international setting (more than one country) except one trial, in other words, CA184-013 [24], which was conducted at multiple centers in the US. Of the included studies, seven were double-blinded, three were assessor-blinded and five were open-labeled.
| Study name | Treatment | n | Trial design | Median age (years) | Male (%) | ECOG PS (%) | LDH levels (%) | BRAF mutation status (%) | Ref. | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ECOG PS 0 | ECOG PS 1 | LDH (≤ULN) | LDH (>ULN) | Mutation positive | Mutation negative | |||||||
| CSR 2019 (COMBI-d trial) | Dabrafenib | 212 | DB, MI, AC, Phase III | 57 | 54 | 71 | 29 | 64 | 34 | 100 | – | [16] |
| Dabrafenib + trametinib | 211 | 55 | 53 | 74 | 26 | 64 | 36 | 100 | – | |||
| CSR 2019 (COMBI-v trial) | Dabrafenib + trametinib | 352 | OL, MI, AC, Phase III | 55 | 59 | 71 | 29 | 66 | 34 | 100 | – | [15] |
| Vemurafenib | 352 | 54 | 51 | 70 | 30 | 68 | 32 | 100 | – | |||
| CSR 2019 (BRF113220 trial) | Dabrafenib | 53 | OL, MI, AC, Phase II | 50 | 54 | 63 | 37 | – | 50 | 100 | – | [17] |
| Dabrafenib + trametinib | 55 | 58 | 63 | 65 | 35 | – | 41 | 100 | – | |||
| Robert 2019 (METRIC trial) | Chemotherapy | 108 | AB, MI, AC, Phase III | 54 | 49 | 64 | 36 | 61 | 39 | 100 | – | [29] |
| Trametinib | 214 | 55 | 56 | 64 | 36 | 63 | 36 | 100 | – | |||
| Liszkay 2019 (COLUMBUS trial) | Encorafenib + binimetinib | 192 | OL, MI, AC, Phase III | 57 | 60 | 71 | 29 | 71 | 29 | 100 | – | [18] |
| Encorafenib | 194 | 54 | 56 | 72 | 28 | 76 | 24 | 100 | – | |||
| Vemurafenib | 191 | 56 | 58 | 73 | 27 | 73 | 27 | 100 | ||||
| Dreno 2018 (coBRIM trial) | Cobimetinib + vemurafenib | 247 | DB, MI, AC, Phase III | 56 | 59 | 76 | 24 | – | 46 | 79 | – | [19] |
| Vemurafenib | 248 | 55 | 56 | 67 | 33 | – | 43 | 83 | – | |||
| Hauschild 2020 (BREAK-3 trial) | Dabrafenib | 187 | AB, MI, AC, Phase III | 53 | 60 | 66 | 33 | 64 | 36 | 100 | – | [20] |
| Dacarbazine | 63 | 50 | 59 | 70 | 25 | 68 | 30 | 100 | – | |||
| Chapman 2017 (BRIM-3 trial) | Dacarbazine | 338 | OL, MI, AC, Phase III | 52 | 54 | 68 | 32 | 42 | 58 | 100 | – | [21] |
| Vemurafenib | 337 | 56 | 59 | 68 | 32 | 42 | 58 | – | – | |||
| Hersh 2011 (CA184-013 trial) | Ipilimumab + dacarbazine | 35 | OL, M, AC, Phase II | 60 | 74 | – | – | 77 | 23 | – | – | [24] |
| Ipilimumab | 37 | 66 | 57 | – | – | 73 | 27 | – | – | |||
| Maio 2015 (CA184-024 trial) | Dacarbazine | 252 | DB, MI, AC, Phase III | 56 | 59 | 71 | 29 | 56 | 44 | – | – | [25] |
| Dacarbazine + ipilimumab | 250 | 58 | 61 | 71 | 29 | 63 | 37 | – | – | |||
| Larkin 2019 (CheckMate 067 trial) | Ipilimumab | 315 | DB, MI, AC, Phase III | 62 | 64 | 71 | 29 | 62 | 37 | 31 | 69 | [22] |
| Ipilimumab + nivolumab | 314 | 61 | 66 | 73 | 26 | 63 | 36 | 32 | 68 | |||
| Nivolumab | 316 | 60 | 64 | 75 | 25 | 62 | 35 | 32 | 68 | |||
| Hodi 2016 (CheckMate 069 trial) | Ipilimumab | 47 | DB, MI, AC, Phase II | 67 | 68 | 79 | 21 | 77 | 23 | 21 | 79 | [23] |
| Ipilimumab + nivolumab | 95 | 64 | 66 | 83 | 15 | 74 | 25 | 23 | 77 | |||
| Ascierto 2019 (CheckMate 066 trial) | Dacarbazine | 208 | DB, MI, AC, Phase III | 66 | 60 | 58 | 40 | 60 | 36 | – | 100 | [26] |
| Nivolumab | 210 | 64 | 58 | 70 | 29 | 57 | 38 | – | 100 | |||
| Robert 2019 (KEYNOTE-006 trial)† | Pembrolizumab 10 mg/kg q2w | 279 | AB, MI, AC, Phase III | 61 | 58 | 70 | 30 | 70 | 29 | 35 | 63 | [28] |
| Pembrolizumab 10 mg/kg q3w | 277 | 63 | 63 | 68 | 32 | 63 | 35 | 35 | 64 | |||
| Ipilimumab 3 mg/kg | 278 | 62 | 58 | 68 | 32 | 64 | 33 | 39 | 61 | |||
| Ascierto 2017† | Ipilimumab 10 mg/kg | 365 | DB, MI, AC, Phase III | 62 | 60 | 72 | 28 | 61 | 36 | 22 | 62 | [27] |
| Ipilimumab 3 mg/kg | 362 | 62 | 64 | 70 | 30 | 60 | 38 | 22 | 65 | |||
†
Data presented for overall population.
AB: Assessor blind; AC: Active controlled; BRAF: v-Raf murine sarcoma viral oncogene homolog B; CSR: Clinical study report; DB: Double-blind; ECOG PS: Eastern Cooperative Oncology Group performance status; M: Multicenter; MI: Multicenter-International; q2w: Every 2 week; q3w: Every 3 week; ULN: Upper limit of normal.
In terms of line of therapy, 11 studies had data on treatment-naive patients, while four studies had data on a mixed patient population (first- and second-line patients). Of these four studies, three reported subgroup data for first-line settings [27–29], while one study, in other words, the Columbus trial, did not report segregated data for first-line and second-line settings [18]. However, the NCCN and ESMO guidelines recommend the combination of encorafenib + binimetinib in the first-line setting; hence, this trial was included as a source for indirect comparison.
The median age of patients in all the included studies was generally >50 years, indicating a higher incidence of metastatic melanoma among the older population. ECOG PS was reported in all the included studies (except the CA184-013 trial). The majority of the patients (>60%) from the included studies had an ECOG PS of 0 or 1 at baseline, thus implying that the majority of patients in the included studies were either asymptomatic or symptomatic, but completely ambulatory. Elevated serum LDH has been identified as an independent and highly significant predictor of survival outcome among patients with stage IV disease. The proportion of patients with LDH levels more than the upper limit of normal ranged from 23.0 [23,24] to 58.0% [21]. In terms of BRAF mutation status, seven trials included populations that were entirely BRAF mutation positive, five trials included mixed patient populations, and two trials did not reported information related to BRAF mutation status [24,25]. One trial, in other words, CheckMate 066, included 100% of patients with BRAF wild-type status [26].
Clinical evidence
The SLR identified long-term PFS and OS reported in different trials (Table 2). The COMBI-d, COMBI-v, and BRF113220 trials reported landmark 5-year PFS and OS data for dabrafenib + trametinib versus the respective comparators. The 5-year analysis showed that dabrafenib + trametinib continued to demonstrate clinically meaningful reductions in the risk of progression or death compared with the BRAF inhibitors dabrafenib or vemurafenib, administered as monotherapy [15,16]. The median OS achieved by dabrafenib + trametinib treated patients was 25.8, 26.0 and 25.0 months for COMBI-d [16], COMBI-v [15] and BRF113220 [17] trial, respectively.
| Trial name | Treatment | Comparator | PFS (HR, 95% CI) | OS (HR, 95% CI) | Ref. |
|---|---|---|---|---|---|
| CSR 2019 (COMBI-d trial) | Dabrafenib + trametinib | Dabrafenib | 0.73 (0.59–0.91) | 0.80 (0.63–1.01) | [16] |
| CSR 2019 (COMBI-v trial) | Dabrafenib + trametinib | Vemurafenib | 0.62 (0.52–0.74) | 0.70 (0.58–0.84) | [15] |
| CSR 2019 (BRF113220 trial) | Dabrafenib + trametinib | Dabrafenib | 0.44 (0.28–0.67) | 0.76 (0.49–1.18) | [17] |
| Robert 2019 (METRIC trial) | Trametinib | Chemotherapy | 0.44 (0.28–0.69) | 0.81 (0.55–1.18) | [29] |
| Liszkay 2019 (COLUMBUS trial) | Encorafenib + binimetinib | Vemurafenib | 0.51 (0.39–0.67) | 0.61 (0.48–0.79) | [18] |
| Encorafenib + binimetinib | Encorafenib | 0.75 (0.56–1.00) | 0.81 (0.61–1.06) | ||
| Dreno 2018 (coBRIM trial) | Cobimetinib + vemurafenib | Vemurafenib | 0.58 (0.46–0.72) | 0.70 (0.55–0.90) | [19] |
| Hauschild 2020 (BREAK-3 trial) | Dabrafenib | Dacarbazine | 0.37 (0.23–0.57) | 0.76 (0.48–1.21) | [20] |
| Chapman 2017 (BRIM-3 trial) | Vemurafenib | Dacarbazine | 0.38 (0.32–0.46) | 0.81 (0.70–1.0) | [21] |
| Maio 2015 (CA184-024 trial) | Ipilimumab + dacarbazine | Dacarbazine | 0.76 (0.63–0.93) | 0.69 (0.57–0.84) | [25] |
| Larkin 2019 (CheckMate 067 trial) | Nivolumab + ipilimumab | Nivolumab | 0.79 (0.64–0.96) | 0.83 (0.67–1.03) | [22] |
| Nivolumab + ipilimumab | Ipilimumab | 0.42 (0.35–0.51) | 0.52 (0.42–0.64) | ||
| Hodi 2016 (CheckMate 069 trial) | Nivolumab + ipilimumab | Ipilimumab | 0.36 (0.22–0.56) | 0.74 (0.43–1.26) | [23] |
| Ascierto 2019 (CheckMate 066 trial) | Nivolumab | Dacarbazine | 0.42 (0.33–0.53) | 0.46 (0.36–0.59) | [26] |
| Robert 2019 (KEYNOTE-006 trial) | Pembrolizumab | Ipilimumab | 0.54 (0.44–0.67) | 0.73 (0.57–0.92) | [28] |
| Ascierto 2017 | Ipilimumab 10 mg/kg | Ipilimumab 3 mg/kg | _ | 0.85 (0.65–1.10) | [27] |
CSR: Clinical study report; HR: Hazard ratio; OS: Overall survival; PFS: Progression-free survival.
The COLUMBUS trial reported the 4-year landmark analysis of PFS and OS for encorafenib + binimetinib versus vemurafenib [18]. The coBRIM trial also reported 4-year survival analysis results for cobimetinib + vemurafenib versus vemurafenib monotherapy [19]. The results were found to be significantly in favor of the combination therapies.
The CheckMate 067 trial [22] recently reported 5-year PFS and OS data for nivolumab + ipilimumab versus nivolumab and ipilimumab monotherapies. The results were significantly in favor of the combination therapy versus monotherapies, with OS not yet reached with the combination therapy. The recently published KEYNOTE-006 trial [28] update analysis provided 5-year survival results for pooled doses of pembrolizumab versus ipilimumab in treatment-naive patients. Two-year PFS and OS results for the combination of nivolumab + ipilimumab versus ipilimumab monotherapy were reported in the CheckMate 069 trial. The median survival had not been reached with nivolumab + ipilimumab, significantly in favor of the combination therapy versus monotherapy. CA184-013 [24] study reported only median OS data but HR were not reported.
Network meta-analysis
Figure 2 presents the network diagram of trials contributing to the analysis for PFS and OS. A total of 13 and 14 studies contributed to the analysis for PFS and OS, respectively. In most of the cases, all comparisons were informed by a single trial.

Figure 2. Master network diagram of trials contributing to analysis for progression-free survival and overall survival.
Numerical values presents the number of studies.
OS: Overall survival; PFS; Progression-free survival.
Progression-free survival
Since data for most of the comparisons were derived from a single trial, and the DICs for the fixed-effect and random-effect models were similar, the fixed-effect model was selected as the appropriate fit. Figure 3 presents the forest plot of PFS for dabrafenib + trametinib versus the comparators.

Among the targeted therapies, the NMA results showed that dabrafenib + trametinib was associated with a significantly better PFS compared with dacarbazine (HR: 0.24 [95% CI: 0.19–0.3]), vemurafenib (HR: 0.62 [95% CI: 0.52–0.73]) and dabrafenib (HR: 0.66 [95% CI: 0.55–0.79]). The NMA results showed no significant difference in PFS between dabrafenib + trametinib and the other two BRAF/MEK inhibitor combinations, i.e, encorafenib + binimetinib (HR: 1.20 [95% CI: 0.88–1.63]) and cobimetinib + vemurafenib (HR: 1.08 [95% CI: 0.82–1.43]). It is important to highlight the heterogeneity across the trials assessing dabrafenib + trametinib and encorafenib + binimetinib, wherein the trials assessing dabrafenib + trametinib had treatment-naive populations, while the COLUMBUS trial assessing encorafenib + binimetinib had a mixed patient population, in other words, treatment-naive and pretreated patients.
The NMA results showed that dabrafenib + trametinib was associated with a significantly better PFS compared with ipilimumab (HR: 0.30 [95% CI: 0.20–0.46]), ipilimumab + dacarbazine (HR: 0.31 [95% CI: 0.23–0.42]), pembrolizumab (HR: 0.54 [95% CI: 0.34–0.88]) and nivolumab (HR: 0.57 [95% CI: 0.41–0.79]). However, the NMA results showed that the combination of dabrafenib + trametinib was associated with a numerically better PFS compared with nivolumab + ipilimumab but statistical significance was not achieved (HR: 0.73 [95% CI: 0.50–1.07]).
Overall survival
Similar to PFS, since most of the data for comparison of OS were derived from a single trial, and the DICs for the fixed-effect and random-effect models were similar, the fixed-effect model was selected as the appropriate fit. Figure 4 presents the forest plot of OS for dabrafenib + trametinib versus the comparators. Among the targeted therapies, the NMA results showed that dabrafenib + trametinib was associated with a significantly better OS compared with dacarbazine (HR: 0.59 [95% CI: 0.47–0.74]), vemurafenib (HR: 0.70 [95% CI: 0.59–0.83]) and dabrafenib (HR: 0.79 [95% CI: 0.65–0.95]). The NMA results showed no significant difference in OS between dabrafenib + trametinib and the other two BRAF/MEK inhibitor combinations, in other words, encorafenib + binimetinib (HR: 1.14 [95% CI: 0.84–1.54]) and cobimetinib + vemurafenib (HR: 1.0 [95% CI: 0.74–1.35]). Dabrafenib + trametinib was associated with a numerically better OS compared with ipilimumab 3 mg/kg (HR: 0.83 [95% CI: 0.54–1.29]) and ipilimumab + dacarbazine (HR: 0.85 [95% CI: 0.63–1.15]). However, pembrolizumab and nivolumab were numerically better compared with dabrafenib + trametinib but statistical significance was not achieved. The combination of nivolumab + ipilimumab was associated with a significantly better OS compared with dabrafenib + trametinib (HR: 1.54 [95% CI: 1.03–2.28]).
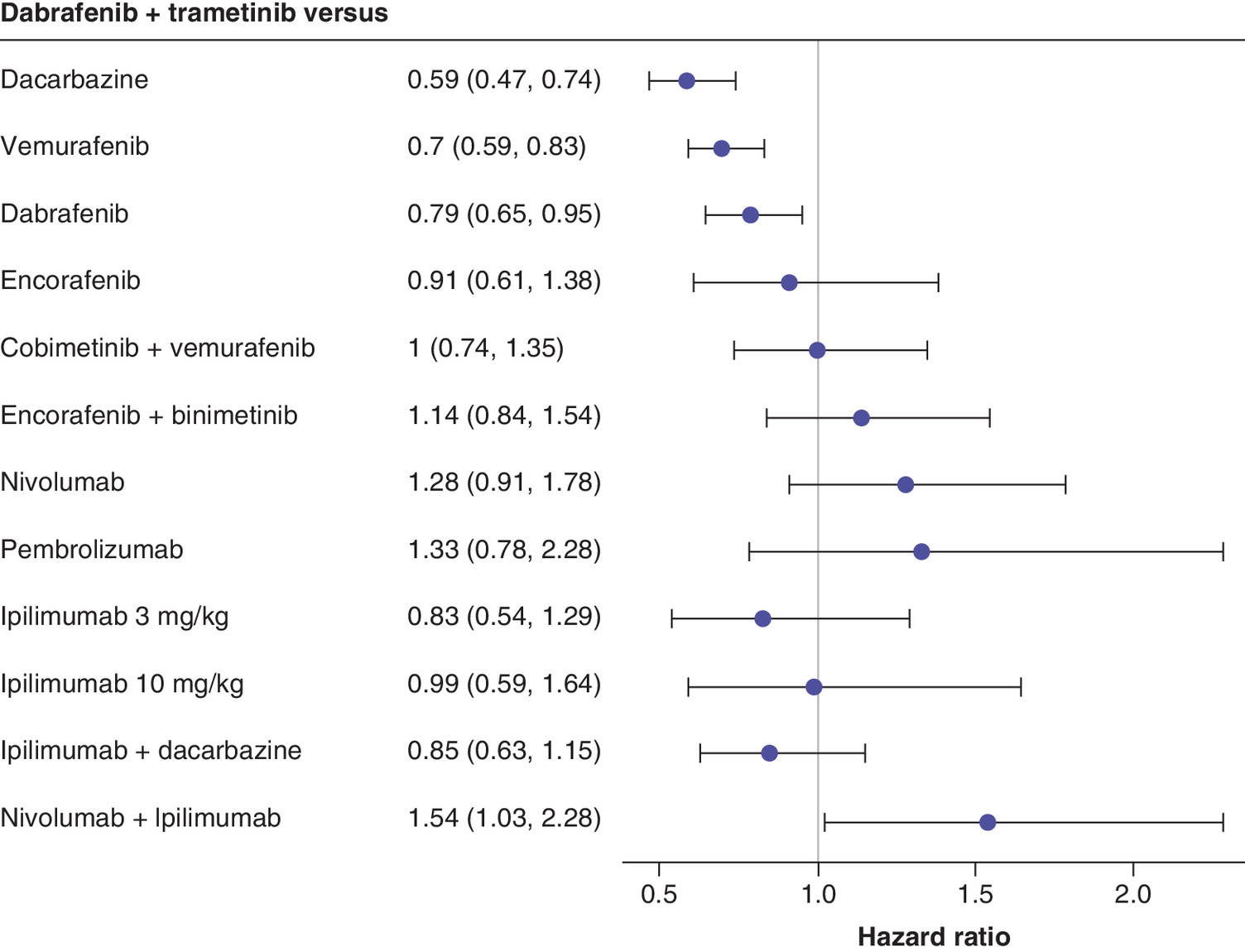
Figure 4. Summary plot of OS for dabrafenib + trametinib versus comparators (intention-to-treat population).
OS: Overall survival.
Consistency
To assess inconsistency, direct and indirect treatment effects were estimated for dabrafenib + trametinib versus vemurafenib and for dabrafenib + trametinib versus dabrafenib. The results of the edge-splitting exercise revealed evidence of inconsistency, although the mean treatment effect was similar. For both PFS and OS, HR of dabrafenib + trametinib versus vemurafenib was significant via mixed treatment comparison (MTC) approach, but significance was not achieved via indirect treatment comparison (ITC) approach. HR for PFS via MTC was found to be 1.61 (95% CI: 1.36–1.9), while HR was 1.6 (95% CI: 0.95–2.71) via ITC; for OS, HR was found to be 1.43 (95% CI: 1.2–1.7) via MTC and HR was 1.39 (95% CI: 0.82–2.37) via ITC. In addition, HR for PFS related to comparison of dabrafenib + trametinib versus dabrafenib was significant via MTC (HR: 1.51 [95% CI: 1.26–1.81) but not significant via ITC (HR: 1.52 [95% CI: 0.91–2.55]). The point estimates demonstrated a consistent direction of the effect.
To assess heterogeneity, ECOG PS, LDH level and BRAF mutation status were considered for the meta-regression analysis. None of the variables significantly affected the results except BRAF mutation status for PFS. To assess the robustness of the results in the base-case analysis, a sensitivity analysis was conducted after removing the CheckMate 066 trial that included a 100% BRAF wild-type population. Results from the sensitivity analysis were similar to the base-case results.
Safety
NMA was not performed with respect to safety outcomes, although the safety outcomes are discussed qualitatively (Table 3). The combination of BRAF + MEK inhibitors is highly effective for the treatment of metastatic melanoma; however, AEs occur with all the combinations in patients treated with combination therapies. Five-year analysis of the COMBI-d, COMBI-v and BRF113220 trials showed that the most common AEs associated with the combination therapy of dabrafenib + trametinib were pyrexia, nausea, diarrhea, chills, headache, fatigue, vomiting, hypertension and arthralgia [15–17]. The coBRIM trial illustrated that the most common AEs (≥20%, all grade) associated with the combination of vemurafenib + cobimetinib included rash, arthralgia, diarrhea, fatigue, nausea, pyrexia, decreased appetite, photosensitivity reaction, alanine aminotransferase and aspartate aminotransferase increase, and serious retinopathy [19]. The COLUMBUS trial reported that the most common AEs associated with the combination of encorafenib + binimetinib included rash, arthralgia, diarrhea, fatigue, vomiting, nausea, constipation, blood creatine phosphokinase increase and vision blurred [18]. Five-year analysis results from the CheckMate 067 trial demonstrated that most common AEs associated with nivolumab + ipilimumab were rash, pruritus, arthralgia, diarrhea, fatigue, nausea, vomiting, pyrexia, decreased appetite, photosensitivity reaction, alanine aminotransferase and aspartate aminotransferase increase, hypothyroidism, and serious retinopathy.
| Study name | Treatment | n | Any AE (%) | Any grade 3/4 AE (%) | Any SAE (%) | Any dose interruptions/ modifications (%) | Any dose reductions (%) | Ref. |
|---|---|---|---|---|---|---|---|---|
| CSR 2019 (COMBI-d trial) | Dabrafenib + trametinib | 209 | 97.0 | 51.7 | 47.0 | 56.0 | 28.0 | [16] |
| Dabrafenib | 211 | 97.0 | 51.7 | 38.0 | 37.0 | 14.0 | ||
| CSR 2019 (COMBI-v trial) | Dabrafenib + trametinib | 350 | 99.0 | 60.6 | 49.0 | 55.0 | 33.0 | [15] |
| Vemurafenib | 349 | 99.0 | 66.5 | 40.0 | 56.0 | 39.0 | ||
| CSR 2019 (BRF113220 trial) | Dabrafenib + trametinib | 55 | 100.0 | 67.3 | 71.0 | 73.0 | 60.0 | [17] |
| Dabrafenib | 53 | 100.0 | 47.2 | 28.0 | 34.0 | 25.0 | ||
| Robert 2019 (METRIC trial) | Trametinib | 211 | 99.1 | 53.0 | 24.6 | 39.0 | 33.0 | [29] |
| Chemotherapy | 99 | 92.9 | 38.0 | 20.2 | 25.3 | 10.0 | ||
| Liszkay 2019 (COLUMBUS trial) | Encorafenib + binimetinib | 192 | 98.4 | 68.2 | 34.0 | 45.8 | 11.5 | [18] |
| Encorafenib | 194 | 99.5 | 67.7 | 34.0 | 63.5 | 27.1 | ||
| Vemurafenib | 186 | 100.0 | 65.6 | 37.0 | 52.7 | 22.6 | ||
| Dreno 2018 (coBRIM trial) | Vemurafenib + cobimetinib | 247 | 99·2 | 73.0 | 37.0 | – | – | [19] |
| Vemurafenib | 246 | 98·0 | 60.0 | 28.0 | – | – | ||
| Hauschild 2020 (BREAK-3 trial) | Dabrafenib | 187 | 98.9 | 46.0 | 32.6 | 37.0 | 24.0 | [20] |
| Dacarbazine | 59 | 93.2 | 42.0 | 23.7 | 27.0 | 17.0 | ||
| Chapman 2017 (BRIM-3 trial) | Vemurafenib | 336 | 99.0 | 71.1 | 49.0 | 47.3 | 33.3 | [21] |
| Dacarbazine | 287 | 93.0 | 42.2 | 18.0 | 15.6 | 15.2 | ||
| Hersh 2011 (CA184-013 trial) | Dacarbazine + ipilimumab | 36 | – | 23.0 | – | – | – | [24] |
| Ipilimumab | 40 | – | 13.0 | – | – | – | ||
| Maio 2015 (CA184-024 trial) | Dacarbazine + ipilimumab | 247 | 98.8 | 56.3 | 68.8 | – | – | [25] |
| Dacarbazine | 251 | 94.0 | 27.5 | 48.2 | – | – | ||
| Larkin 2019 (CheckMate 067 trial) | Nivolumab + ipilimumab | 313 | 96.0 | 59.0 | – | – | – | [22] |
| Ipilimumab | 311 | 86.0 | 28.0 | – | – | – | ||
| Nivolumab | 313 | 86.0 | 22.0 | – | – | – | ||
| Hodi 2016 (CheckMate 069 trial) | Nivolumab + ipilimumab | 94 | 91.0 | 54.0 | – | – | – | [23] |
| Ipilimumab | 46 | 93.0 | 19.0 | – | – | – | ||
| Ascierto 2019 (CheckMate 066 trial) | Dacarbazine | 205 | 95.2 | 17.6 | – | – | – | [26] |
| Nivolumab | 206 | 92.7 | 15.0 | – | – | – |
AE: Adverse event; SAE: Serious adverse event.
The most common grade 3/4 AEs associated with dabrafenib + trametinib were found to be pyrexia, neutropenia and hypertension, while combination of cobimetinib + vemurafenib was associated with grade 3/4 liver toxicity, rash, arthralgia, squamous cell carcinomas and diarrhea. Combination of encorafenib + binimetinib was associated with grade 3/4 (≥5%) hypertension, blood creatine phosphokinase increase and gamma-glutamyl transferase increase. The CheckMate 067 trial reported that the most common treatment-related grade 3 AE associated with nivolumab + ipilimumab was diarrhea, while the most common grade 4 AE was increased lipase.
Discussion
Recent advances in targeted therapies and immune checkpoint inhibitors have revolutionized the treatment paradigm for patients with advanced or metastatic melanoma. Dabrafenib + trametinib has been the first choice of physicians for treating patients with advanced or metastatic melanoma in many countries; however, with the introduction of newer BRAF + MEK inhibitors and immunotherapies, it has become challenging to select the optimal therapy. Furthermore, no head-to-head trials are available to assess the efficacy and safety profile of either targeted therapies or immunotherapies among themselves. Hence, we aimed to conduct an NMA to assess the relative efficacy of the available treatment options, and an SLR was conducted with prespecified criteria to identify studies assessing agents for the treatment of metastatic melanoma in first-line settings.
This SLR identified 15 studies assessing different treatment options for patients with metastatic melanoma in first-line settings. The baseline study and patient characteristics across the studies were found to be similar except for BRAF mutation status. The SLR identified long-term survival data associated with various combination therapies, and subsequently an NMA was conducted by using the HRs reported for the latest study data cut-offs.
Dabrafenib + trametinib was found to be associated with a significantly better PFS compared with monotherapies, in other words, dacarbazine, ipilimumab, pembrolizumab, nivolumab, vemurafenib and dabrafenib. The efficacy profiles of all three BRAF + MEK inhibitor combination therapies were similar with regard to PFS and OS. These results were in line with a previously conducted meta-analysis that also reported no significant difference between the combination therapies [30]. Moreover, a recent Scottish Medicines Consortium submission also stated that the efficacy profile of encorafenib + binimetinib was similar to that of dabrafenib + trametinib [31].
Dabrafenib + trametinib was associated with a numerically better PFS compared with nivolumab and ipilimumab monotherapies but combination of nivolumab and ipilimumab was associated with a significantly better OS compared with dabrafenib + trametinib (HR: 1.54 [95% CI: 1.03–2.28]). The NMA results correspond to a recently published systematic review and meta-analysis that stated that dabrafenib + trametinib was the preferred treatment for PFS, while the combination of nivolumab + ipilimumab was the preferred option for OS [32]. However, there were few differences in this SLR versus the previously conducted NMA by Zoratti and colleagues: this NMA was not only conducted at the category level but also at the molecule level; the NMA was conducted on recent data cut-offs and the NMA involved a comparison versus encorafenib + binimetinib.
This SLR has several strengths and limitations. The strengths of this SLR involve a search of key bibliographic databases as well as searches of recent conferences. The review adopted a standard methodology following predefined eligibility criteria established in the protocol and involved two independent researchers for the identification of studies and data extraction. The SLR identified long-term survival data reported according to different data cut-offs. There were few limitations associated with the SLR, such as heterogeneous baseline parameters, in other words, the inclusion of some mixed population trials, where subgroup results were not reported separately for BRAF-mutated and BRAF wild-type patients. These trials were included to form a connected network that linked targeted therapies and immunotherapies. Additionally, evidence suggests that immunotherapies demonstrate efficacy irrespective of BRAF mutation status. Second, the inclusion of the COLUMBUS trial, which included treatment-naive and pretreated patient populations. The trial did not report segregated data for first-line and second-line settings [18]. However, the NCCN and ESMO guidelines recommend the combination of encorafenib + binimetinib in the first-line setting; hence, this trial was included to have an indirect comparison. Owing to these heterogeneous factors, the NMA results should be interpreted with caution. The results from this meta-analysis are based on a sparse network of evidence as most comparisons were informed by a single trial; hence, the results should not be generalized to a broader patient population.
The results from the NMA suggest that dabrafenib + trametinib significantly prolongs survival outcomes compared with the monotherapies and has a comparable efficacy profile versus the other two BRAF + MEK inhibitors. In comparison with immunotherapies, the results varied for PFS and OS; hence, it is difficult to derive any conclusion. The treatment landscape for metastatic melanoma has evolved; however, clinical decision-making is still based on factors, such as toxicity profile, BRAF mutation status and patient medical history (e.g., comorbidities, ECOG PS and tumor burden). This SLR may facilitate evidence-based decision-making and support the optimization of treatment and outcomes in everyday clinical practice.
Background
•
BRAF V600-mutation positive patients have worse prognosis, with higher mortality, than the general metastatic melanoma population.
•
The treatment landscape for metastatic melanoma is changing rapidly with the recent development of newer agents that have demonstrated better efficacy than traditional chemotherapy.
•
Many effective first-line treatment options are available for advanced BRAF-mutated melanoma, but there are no head-to-head randomized trials of these agents, and thus the optimal treatment is unknown.
Evidence base
•
A systematic literature review was conducted via a search of key biomedical databases on May 2020.
•
A total of 15 studies meeting the inclusion criteria were included in the review.
•
Of these 15 studies, eight studies assessed targeted therapies (monotherapies or combination therapy), while seven studies immunotherapies (monotherapies, combination with chemotherapy or PD-1 inhibitor + CTLA-4 inhibitor).
Key findings
•
Network meta-analysis results showed that dabrafenib + trametinib was associated with significantly better progression-free survival and overall survival (OS) compared with dacarbazine, vemurafenib and dabrafenib.
•
No significant difference for progression-free survival and OS between dabrafenib + trametinib and other two BRAF/MEK combinations in other words, encorafenib + binimetinib and cobimetinib + vemurafenib.
•
Combination of nivolumab and ipilimumab was associated with significantly better OS compared with dabrafenib + trametinib.
Author contributions
J Wu was responsible for providing insights and review of the analysis as well as writing/editing of manuscript. B Ratto, J Das and M Kalra were responsible for conceptualization, conducting review/analysis and writing of the manuscript.
Financial & competing interests disclosure
The review was supported by Novartis Pharmaceuticals Corporation, NJ, USA. J Wu works as a Professor with Tianjin University and received research fund from Beijing Novartis Pharma Co. Ltd. B Ratto is an employee of Novartis Pharmaceuticals Corporation, NJ, US. J Das and M Kalra are employees of Novartis Healthcare Pvt Ltd, India. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Bray F, Ferlay J, Soerjomataram I et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 68(6), 394–424 (2018).
2.
SEER. Surveillance, epidemiology, and end results program. (2020). https://seer.cancer.gov/
3.
Sandru A, Voinea S, Panaitescu E et al. Survival rates of patients with metastatic malignant melanoma. J. Med. Life 7(4), 572–576 (2014).
4.
Shtivelman E, Davies MQ, Hwu P et al. Pathways and therapeutic targets in melanoma. Oncotarget 5(7), 1701–1752 (2014).
5.
Davies H, Bignell GR, Cox C et al. Mutations of the BRAF gene in human cancer. Nature 417(6892), 949–954 (2002).
6.
Goydos JS, Mann B, Kim HJ et al. Detection of B-RAF and N-RAS mutations in human melanoma. J. Am. Coll. Surg. 200(3), 362–370 (2005).
7.
Brose MS, Volpe P, Feldman M et al. BRAF and RAS mutations in human lung cancer and melanoma. Cancer Res. 62(23), 6997–7000 (2002).
8.
Heinzerling L, Baiter M, Kuhnapfel S et al. Mutation landscape in melanoma patients clinical implications of heterogeneity of BRAF mutations. Br. J. Cancer 109(11), 2833–2841 (2013).
9.
Bruno W, Martinuzzi C, Andreotti V et al. Heterogeneity and frequency of BRAF mutations in primary melanoma: comparison between molecular methods and immunohistochemistry. Oncotarget 8(5), 8069–8082 (2017).
10.
Ascierto PA, Kirkwood JM, Grob JJ et al. The role of BRAF V600 mutation in melanoma. J. Transl. Med. 10, 85 (2012).
11.
Paraiso KH, Fedorenko IV, Cantini LP et al. Recovery of phospho-ERK activity allows melanoma cells to escape from BRAF inhibitor therapy. Br. J. Cancer 102(12), 1724–1730 (2010).
12.
NCCN. NCCN clinical practice guidelines in oncology. Cutaneous Melanoma (2019). https://www.nccn.org/store/login/login.aspx?Return
13.
Michielin O, van Akkooi A, Ascierto P et al. Cutaneous melanoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 30(12), 1884–1901 (2019).
14.
Dias S, Welton NJ, Sutton AJ et al. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. National Institute for Health and Care Excellence (NICE), UK (2014).
15.
CSR. COMBI-v: Tafinlar® (dabrafenib) and Mekinist® (trametinib): clinical overview in unresectable or metastatic melanoma with a BRAF V600 mutation: 5-year analysis. Clinical Study Report (2019).
16.
CSR. COMBI-d: Tafinlar® (dabrafenib) and Mekinist® (trametinib): clinical overview in unresectable or metastatic melanoma with a BRAF V600 mutation: 5-year analysis. (2019).
17.
CSR. BRF113220: an open-label, dose-escalation, Phase Ib/II study to investigate the safety, pharmacokinetics, pharmacodynamics and clinical activity of the BRAF inhibitor GSK2118436 in combination with the MEK inhibitor GSK1120212 in subjects with BRAF mutant metastatic melanoma. Clinical Study Report (2019).
18.
Liszkay G, Gogas H, Mandala M. Update on overall survival in COLUMBUS: a randomized Phase III trial of encorafenib (ENCO) plus binimetinib (BINI) versus vemurafenib (VEM) or ENCO in patients with BRAF V600–mutant melanoma. J. Clin. Oncol. 37(15), 9512 (2019).
•• COLUMBUS trial, a Phase III trial of encorafenib + binimetinib in metastatic melanoma.
19.
Dreno B, Antonio-Ascierto P, McArthur GA. Efficacy and safety of cobimetinib (C) combined with vemurafenib (V) in patients (pts) with BRAFV600 mutation–positive metastatic melanoma: analysis from the 4-year extended follow-up of the Phase III coBRIM study. J. Clin. Oncol. 36(15), 9522 (2018).
•• coBRIM trial, a Phase III trial of cobimetinib + vemurafenib in metastatic melanoma.
20.
Hauschild A, Ascierto P, Schadendorf D. Long-term outcomes in patients with BRAF V600-mutant metastatic melanoma receiving dabrafenib monotherapy: analysis from Phase II and III clinical trials. Eur. J. Cancer 125, 114–120 (2020).
21.
Chapman PB, Robert C, Larkin J et al. Vemurafenib in patients with BRAFV600 mutation-positive metastatic melanoma: final overall survival results of the randomized BRIM-3 study. Ann. Oncol. 28(10), 2581–2587 (2017).
22.
Larkin J, Chiarion-Sileni V, Gonzalez R et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 381(16), 1535–1546 (2019).
•• CheckMate 067 trial, a Phase III trial of ipilimumab + nivolumab in metastatic melanoma.
23.
Hodi FS, Chesney J, Pavlick AC et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, Phase II trial. Lancet Oncol. 17(11), 1558–1568 (2016).
• CheckMate 069 trial, a Phase III trial of ipilimumab + nivolumab in metastatic melanoma.
24.
Hersh EM, O'Day SJ, Powderly J et al. A Phase II multicenter study of ipilimumab with or without dacarbazine in chemotherapy-naive patients with advanced melanoma. Invest. New Drugs 29(3), 489–498 (2011).
25.
Maio M, Grob JJ, Aamdal S et al. Five-year survival rates for treatment-naive patients with advanced melanoma who received ipilimumab plus dacarbazine in a Phase III trial. J. Clin. Oncol. 33(10), 1191–1196 (2015).
26.
Ascierto PA, Long GV, Robert C et al. Survival outcomes in patients with previously untreated BRAF wild-type advanced melanoma treated with nivolumab therapy: three-year follow-up of a randomized Phase III Trial. JAMA Oncol. 5(2), 187–194 (2019).
•• CheckMate 066 trial, a Phase III trial of nivolumab in metastatic melanoma.
27.
Ascierto PA, Del Vecchio M, Robert C et al. Ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg in patients with unresectable or metastatic melanoma: a randomised, double-blind, multicentre, Phase III trial. Lancet Oncol. 18(5), 611–622 (2017).
28.
Robert C, Ribas A, Schachter J et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): post-hoc 5-year results from an open-label, multicentre, randomised, controlled, Phase III study. Lancet Oncol. 20(9), 1239–1251 (2019).
•• KEYNOTE-006 trial, a Phase III trial of pembrolizumab in metastatic melanoma.
29.
Robert C, Flaherty K, Nathan P et al. Five-year outcomes from a Phase III METRIC study in patients with BRAF V600 E/K-mutant advanced or metastatic melanoma. Eur. J. Cancer 109, 61–69 (2019).
30.
Consoli F, Bersanelli M, Perego G et al. Network indirect comparison of 3 BRAF + MEK inhibitors for the treatment of advanced BRAF mutated melanoma. Clin. Transl. Oncol. 22(6), 900–907 (2020).
31.
SMC. Encorafenib 50 mg and 75 mg hard capsules (Braftovi®) SMC2145 (2019).
32.
Zoratti MJ, Devji T, Levine O et al. Network meta-analysis of therapies for previously untreated advanced BRAF-mutated melanoma. Cancer Treat. Rev. 74, 43–48 (2019).
Information & Authors
Information
Published In
Pages: 267 - 280
PubMed: 33448878
Copyright
© 2021 Jing Wu. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 November 2020
Accepted: 1 December 2020
Published online: 15 January 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative efficacy of dabrafenib + trametinib versus treatment options for metastatic melanoma in first-line settings. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0249
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Eva Ellebaek, Michael Weichenthal, Iva Gavrilova, Nethanel Asher, Patrick Terheyden, Jochen Utikal, Amina Jalovčić Suljeviić, Claudia Pföhler, Igor Stojkovski, Rudolf Alexander Herbst, Selma Ugurel, Christina Ruhlmann, Alfonso Berrocal, Margarita Majem, Branko Dujovic, Viktor Šabarić, Tomislav Duvancic, Ainara Soria, Marco Donia, Henrik Schmidt, Rasmus B. Friis, Alexander Gerasimov, Gergana Shalamanova-Deleva, Ahmed Kontilev, Shaked Lev-Ari, Ronnie Shapira, Luisa Piccin, Alessandro Minisini, Berna C. Özdemir, Pawel Teterycz, Anna Mariuk-Jarema, Dimitrios Ziogas, Amalia Anastasopoulou, Dimitra Stefanou, Lourdes Gutiérrez, Christoffer Gebhardt, Reinhard Dummer, Axel Hauschild, Peter Mohr, Imke von Wasielewski, Friedegund Meier, John Haanen, Inge Marie Svane, Paolo A. Ascierto, Joanna Mangana, Piotr Rutkowski, Helen Gogas, Lars Bastholt, Dirk Schadendorf, Efficacy of combined BRAF-MEK inhibitor second-line therapy in patients with non-resectable or metastatic BRAFV600-positive melanoma after prior immunotherapy: A retrospective EUMelaReg multicenter study, EJC Skin Cancer, 10.1016/j.ejcskn.2025.100773, 4, (100773), (2026).
- Anne Ravix, Carole Bandiera, Evelina Cardoso, Adrian Lata-Pedreira, Haithem Chtioui, Laurent Arthur Decosterd, Anna Dorothea Wagner, Marie Paule Schneider, Chantal Csajka, Monia Guidi, Population Pharmacokinetics of Trametinib and Impact of Nonadherence on Drug Exposure in Oncology Patients as Part of the Optimizing Oral Targeted Anticancer Therapies Study, Cancers, 10.3390/cancers16122193, 16, 12, (2193), (2024).
- Andrea Boutros, Enrica Teresa Tanda, Elena Croce, Fabio Catalano, Marcello Ceppi, Marco Bruzzone, Federica Cecchi, Luca Arecco, Matteo Fraguglia, Paolo Pronzato, Carlo Genova, Lucia Del Mastro, Matteo Lambertini, Francesco Spagnolo, Activity and safety of first-line treatments for advanced melanoma: A network meta-analysis, European Journal of Cancer, 10.1016/j.ejca.2023.04.010, 188, (64-79), (2023).
- Paweł Rogala, Anna M. Czarnecka, Bożena Cybulska-Stopa, Krzysztof Ostaszewski, Karolina Piejko, Marcin Ziętek, Robert Dziura, Ewa Rutkowska, Łukasz Galus, Natasza Kempa-Kamińska, Jacek Calik, Agata Sałek-Zań, Tomasz Zemełka, Wiesław Bal, Agnieszka Kamycka, Tomasz Świtaj, Grażyna Kamińska-Winciorek, Rafał Suwiński, Jacek Mackiewicz, Piotr Rutkowski, Long-Term Outcomes of Targeted Therapy after First-Line Immunotherapy in BRAF-Mutated Advanced Cutaneous Melanoma Patients—Real-World Evidence, Journal of Clinical Medicine, 10.3390/jcm11082239, 11, 8, (2239), (2022).
- Laura Dormer, Celebrating 10 years of the Journal of Comparative Effectiveness Research, Journal of Comparative Effectiveness Research, 10.2217/cer-2021-0249, 11, 1, (1-6), (2021).
- Austin Hamp, Jarett Anderson, Torunn E Sivesind, Mindy D Szeto, Andreas Hadjinicolaou, From the Cochrane Library: Systemic Treatments for Metastatic Cutaneous Melanoma, JMIR Dermatology, 10.2196/30270, 4, 2, (e30270), (2021).