Do implantable loop recorders impact the survival of patients with recurrent unexplained syncope?
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: This study compares the outcomes of patients who receive an implantable loop recorder (ILR) for unexplained syncope to a control group without the diagnostic device in German claims data. Methods and materials: Patients with ILR were matched to a control group based on prior syncope events, age, gender and Charlson Comorbidity index (CCI). Survival, syncope hospitalizations, treatment and costs were compared. Results/conclusion: Four hundred and twelve ILR patients were matched with controls, mean age was 68, mean CCI was 2.7, 42% females. ILR patients lived on average 1.2 years longer than patients in the control group. Twenty-five percent of ILR patients received a therapeutic device compared with 5% in the control group. ILRs might help to diagnose and treat patients with positive impact on survival.
Syncope is a transient loss of consciousness due to cerebral hypoperfusion. Diagnosis of the underlying cause can be challenging as patients do not always have symptoms when they seek medical care. The diagnostic tests are generally undertaken when patients are asymptomatic and therefore may be normal. Therefore, syncope remains undiagnosed in up to a third of patients after initial clinical investigations [1,2].
When syncope remains undiagnosed and untreated, it can have severe consequences. Several studies have documented worse survival in patients with syncope than in a control group without syncope [3,4]. Syncope might be a first symptom of underlying cardiovascular disease. Among the types of syncope, cardiac syncope generally has the poorest prognosis as it doubles the risk of death and carries a 6-month mortality rate of greater than 10% [2].
In addition to the impact on life expectancy, patients’ quality of life has been shown to be severely affected by recurrent syncope [5–9]. Quality of life in this cohort is similar to patients with chronic diseases such as end-stage renal disease or structural heart disease [8]. Studies have shown that more than 70% of patients have anxiety or depression and require changes to daily activities such as employment or driving [6]. Syncope doubles the risk of occupational accidents termination of employment [10]. Syncope is also a well-known risk factor for falls and associated injuries; 5% of syncope patients present with a severe injury and trauma in the emergency department [11].
In order to optimize the diagnostic yield of syncope investigations, the Syncope Guidelines by the European Society of Cardiology, the Transient Loss of Consciousness guidelines by the National Institute for Health and Care Excellence as well as the Syncope Guidelines by the American College of Cardiology/American Heart Association/Heart Rhythm Society present evidence and recommendations regarding which investigations are most relevant and likely to lead to a diagnosis [1,12,13].
If the underlying cause of recurrent syncope is suspected to be cardiac, diagnostic clarification of the underlying rhythm with an implantable loop recorder (ILR) is recommended [1,12,13]. These devices enable the recording of an electrocardiogram during a syncopal event. ILRs have been shown to provide a diagnosis in 78% of cases when a syncope reoccurs and of these diagnoses, 75% were cardiac [14]. Overall, ILRs are 3.6-times more likely to reach a diagnosis than conventional testing based on a recent meta-analysis [1].
The main objective of the analysis was to compare outcomes between recurrent syncope patients who received an ILR to a control group. To be able to compare them, groups were matched based on syncope burden, age, gender and Charlson Comorbidity index (CCI).
Methods and materials
Data source
German healthcare claims data were selected for this analysis as it is possible to follow patients over a long time and we can see all healthcare utilization, costs and death. Unfortunately, there is no national claims dataset available in Germany. However, there are a few large datasets available for research purposes. For this study, we used a representative claims database of 5.7 million patients (7% of the nationwide population) in which patients can be tracked for 11 years. Health insurances keep records of their insurees over time including demographic information, healthcare utilization and associated costs, sick leave and death.
Healthcare claims data are based on codes. In order to be reimbursed, healthcare providers submit claims to health insurances, including diagnosis and procedure codes. Hospitals can code up to three primary diagnoses, designating one as the main reason for admission. In addition, there is the option to code various subdiagnoses. German healthcare claims data include the ICD-10-GM codes (International Statistical Classification of Diseases and Related Health Problems, 10th revision, German Modification) for the classification of diseases. All major medical procedures are coded using the German version of the International Classification of Procedures in Medicine codes (OPS). Patients with similar diagnoses and procedures are summarized into groups, which determine reimbursement. In the inpatient setting these codes are the German Diagnosis Related Groups (G-DRG), while in the outpatient setting these codes are called Einheitlicher Bewertungsmassstab. Similarly, there are codes for outpatient drugs prescribed (ATC codes) and medical aids (pzn codes).
The total healthcare costs of a patient include inpatient care (hospitalization), outpatient care, prescribed pharmaceuticals, sick leave pay (salary replacement after 6 weeks of absence) and medical aids (such as shoe inserts or walkers). Sick leave spells are only communicated and recorded to health insurances if they last longer than 6 weeks, since health insurances are required to compensate the salary payment thereafter.
Study population
Patients with two syncope codes within 2 years were selected for this analysis. Furthermore, the analysis is limited to patients between the age of 45–84. Patients below the age of 45 were excluded as cardiac syncope is less common at younger ages. Many young syncope patients have reflex syncope and are not the patient population of interest here. Similarly, patients older than 85 are generally not likely to still receive an ILR in clinical practice and the ones who do might be outliers.
The total time period available was 2007–2017. To leave at least 2 years of baseline period and follow-up for each patient, we included patients if they had recurrent syncope within 2 years in the time period from 2009 to 2015. Thus, the available follow-up of patients varies from 2 years (2015–2017) to 9 years (2009–2017). In order to compare survival, the total available follow-up was used in both groups. For all other outcomes, patients were only followed up for 2 years or as long as the matched patient in the other group was alive. In this way, patients have the same time at risk.
Patients with syncope were identified through the ICD-10 code R55 – Syncope and collapse. Healthcare providers generally document this code when they investigate a syncope patient. However, the diagnosis code for syncope is not always directly associated with an acute event. The code could also simply be carried forward. This is likely to be the case if the cause of the syncope is not diagnosed. It is particularly relevant in the ambulatory setting as patients might visit their general practitioner (GP) or cardiologist several times after a syncope. We therefore count the syncope code R55 in the ambulatory sector only once. Similarly, in order to ensure an R55 code reflects an actual syncope event during a hospitalization, it is only counted if it either the reason for admission (one of the main diagnosis codes) or a DRG for syncope or an injury is coded at discharge together with a secondary diagnosis code for syncope. We only included injuries typically related to a fall such as hip, knee and head injuries (please see Supplementary Table 1 for the codes included).
In the ILR group, the index event was the device implant taking place after the second syncope event, whereas in the control group, the index event was the second syncope event. The index event divides the available data into baseline period (before index event) and follow-up (the index event).
To select a group of patients with two recurrent syncope events, we identified patients who either had two hospitalizations for syncope or first an ambulatory visit followed by a hospitalization at a later point in time. In the ILR group, one of the syncope events could have been coded during the same hospitalization as the ILR implant. In order to avoid counting follow-up visits as syncope events, an ambulatory visit for syncope had to be coded before a hospitalization to be counted as syncope event (Supplementary Figure 4).
Patients with an implanted ILR were identified through the procedure code (OPS code: 5-377.8) and the diagnosis and DRG code for ILR in the indication syncope (DRG codes F12F, F12H, F12Z). There is unfortunately no ICD-10 diagnosis code for ‘unexplained’ syncope in the German setting. We therefore excluded patients if they had a documented ICD-10 diagnosis code in the baseline period which could be the cause of syncope such as epilepsy or orthostatic hypotension (Supplementary Table 2). In addition, patients with a cardiac therapeutic device (pacemaker, defibrillator, cardiac resynchronization therapy [CRT]) in the baseline period were excluded from the analysis as it was assumed that their cause of syncope had been identified.
Matching
The main objective of the analysis was to compare outcomes between recurrent syncope patients who received an ILR to a control group. Patients with ILR were matched to patients without ILR based on age, gender and CCI using mahalanobis distances and greedy nearest neighbor matching. While gender was an exact match, age and CCI were matched based on mahalanobis distances. With mahalanobis distances, each ILR patient is matched with the most similar patient in the control group with regard to age and CCI. The rational of matching was to balance potential confounding variables between the two groups as age, gender and co-morbidities are key factors for outcomes such as mortality. The CCI is a summary score that predicts 10-year mortality for a patient with a range of co-morbid conditions. The CCI includes 19 different co-morbidities including, for example, different cardiovascular conditions, diabetes and different types of cancers [15].
To assess the long-term burden of recurrent syncope for patients and the costs to the healthcare system, the following outcomes were assessed:
•
Survival
•
Percentage of patients with diagnosis in follow-up period
•
Treatment rates
•
Total healthcare costs
The amounts reimbursed by health insurances to healthcare providers were used to approximate true healthcare costs. The reimbursed amounts are based on DRG and outpatient tariffs, drug prescriptions and medical aids prescribed. The DRG and Einheitlicher Bewertungsmassstab tariffs are lump-sum reimbursements for treating groups of patients with similar treatment needs and diagnosis.
Statistics
The analysis was performed on aggregated data. Continuous data are summarized with a mean ± standard deviation, median and interquartile range. Categorical data as counts and percentages. The risk of mortality is shown as Kaplan–Meier Curves. Various types of statistical tests were employed. T-tests were used for calculating differences in means. McNemar tests were used for analysis of contingency tables. Significance was tested using the log rank test for the survival analysis. Data were stored and analyzed using Microsoft Office Excel 2014 (Microsoft Corporation, WA, USA) and SAS (Version 9.4; SAS Institute Inc., NC, USA).
Results
During the period 2009 through 2015, 82,689 patients had at least one hospital admission for syncope. Based on the total sample of 5.7 million patients, the average rate of hospital admissions for syncope was 1.88 per 1000 person-years. This result is consistent with other epidemiological data [12,25].
In line with the literature, the number of patients with repeated event is much smaller. In this dataset, 8% (6593) of the patients with one syncope admission (82,689) experience a second event within 2 years (Figure 1). When limiting this group to the age group 45–84 and excluding patients with a definite diagnosis (identified by additional documented ICD-10 diagnosis codes), the final control group with recurrent unexplained syncope includes 1920 patients. Please see Supplementary Table 2 for the percentage of excluded patients by ICD-10 code.

Figure 1. Flow chart of patient inclusion.
ILR: Implantable loop recorder.
Out of a total of 3023 patients with an ILR in this dataset, 74% (2241 patients) received the ILR for the indication syncope and 850 patients had exactly two documented syncope codes before implant using the code combinations as defined in the Methods section. Analogously to the control group, we limit the ILR group also to the age group 45–84. After excluding patients with possible diagnosis/different indication than unexplained syncope (Supplementary Table 2), there are 412 patients in total in the ILR group as shown in Figure 1. Mean follow-up time was 4.25 years in the ILR group (standard deviation [SD]: 1.8) and 4.3 in the control group (SD: 2.2).
Matching results
The 412 ILR patients were matched 1:1 to 412 control patients. Mean age was 68 years (SD: 10.7), and 42% of the patients were females. The mean CCI was 2.7 (SD: 2.4) and thus patients had on average nearly three serious co-morbidities. Around 20% of patient had congestive heart failure and 10% had myocardial infarction in both groups (Supplementary Table 3). By design, all patients had two syncope codes within 2 years in the baseline period.
Survival
The risk of death was significantly higher in the control group during follow-up as shown in Figure 2 (log rank test, p < 0.0001). Survival at 3 years was 80% in the control group, compared with 93% in the ILR group. Overall, 27% of patients in the control group died in the follow-up period compared with 12% in the ILR group. Based on the Kaplan–Meier curve, projected mean life expectancy is 7.7 years for the ILR patients and 6.5 years for the control group. Thus, ILR patients are expected to live on average 1.2 years longer than patients in the control group. Please note that the cause of death is not recorded in the dataset and thus the share of cardiovascular deaths is not known. Please also note that there were very few patients with more than 7 years follow-up and as such there are very few observations left after year 7 as shown in Figure 2.

Figure 2. Survival of implantable loop recorder patients compared with control group.
HR: Hazard ratio; ILR: Implantable loop recorder; KM: Kaplan–Meier.
Cardiac treatment & diagnoses
During the 2-year follow-up period, cardiac treatment rates were higher in the ILR group. A quarter (25%) of ILR patients received an implantable cardiac device compared with 5% in the control group (p-value McNemar test < 0.0001). Ablation rates were 4% in the ILR group compared with 1% in the control group (p-value McNemar test < 0.0027). The results are illustrated in Supplementary Figure 5. The share of ILR patients on antiarrhythmic drug therapy doubles during the follow-up period from 3 to 6% (p-value McNemar test = 0.0035), while there is no change in the control group.
In line with the higher cardiac treatment rates, patients in the ILR group were significantly more likely to receive a new cardiovascular related diagnosis in the follow-up period (Supplementary Table 4). In addition to diagnoses that are indications for a pacemaker or defibrillator, patients with an ILR were also significantly more likely to be detected with paroxysmal atrial fibrillation (PAF). The share of ILR patients diagnosed with PAF rose from 11% in baseline to 18% during follow-up, while no new diagnoses of PAF were noted in the control group that remained at 8%. Anticoagulation (OAC) prescriptions rose from 13 to 19% in the ILR group (p-value McNemar test = 0.0002), while it remained at 10% in the control group. OAC initiation is important to prevent ischemic strokes in patients with AF. Ischemic stroke rates were higher in the control group but the difference was not significant. As an ILR could also help to diagnose an underlying coronary heart disease, the application of percutaneous coronary interventions was also compared in the two groups, no difference was found.
ILR patients were more likely to have a cardiology diagnosis code already documented in the baseline period. The most common diagnosis code was ‘unspecified cardiac arrythmia.’ The code was documented for 24% of ILR patients compared with 14% of control patients (p < 0.0002). Such an unspecified code might be used when a cardiac cause of the syncope is suspected. The codes ‘supraventricular tachycardia’ and ‘unspecified atrial fibrillation’ were also more common in the ILR group than in the control group.
Healthcare costs
Figure 3 compares the mean healthcare costs between the two groups. Total healthcare costs are higher in the control group in the baseline period as a result of higher costs of drug prescriptions (paired t-test = 0.01). The difference in mean drug costs is driven by a single patient who receives the drug Remodulin during the baseline period. Overall, the patient does not appear to be an outlier, the drug therapy was discontinued before the follow-up period and the patients remain in the study over the entire follow-up time.
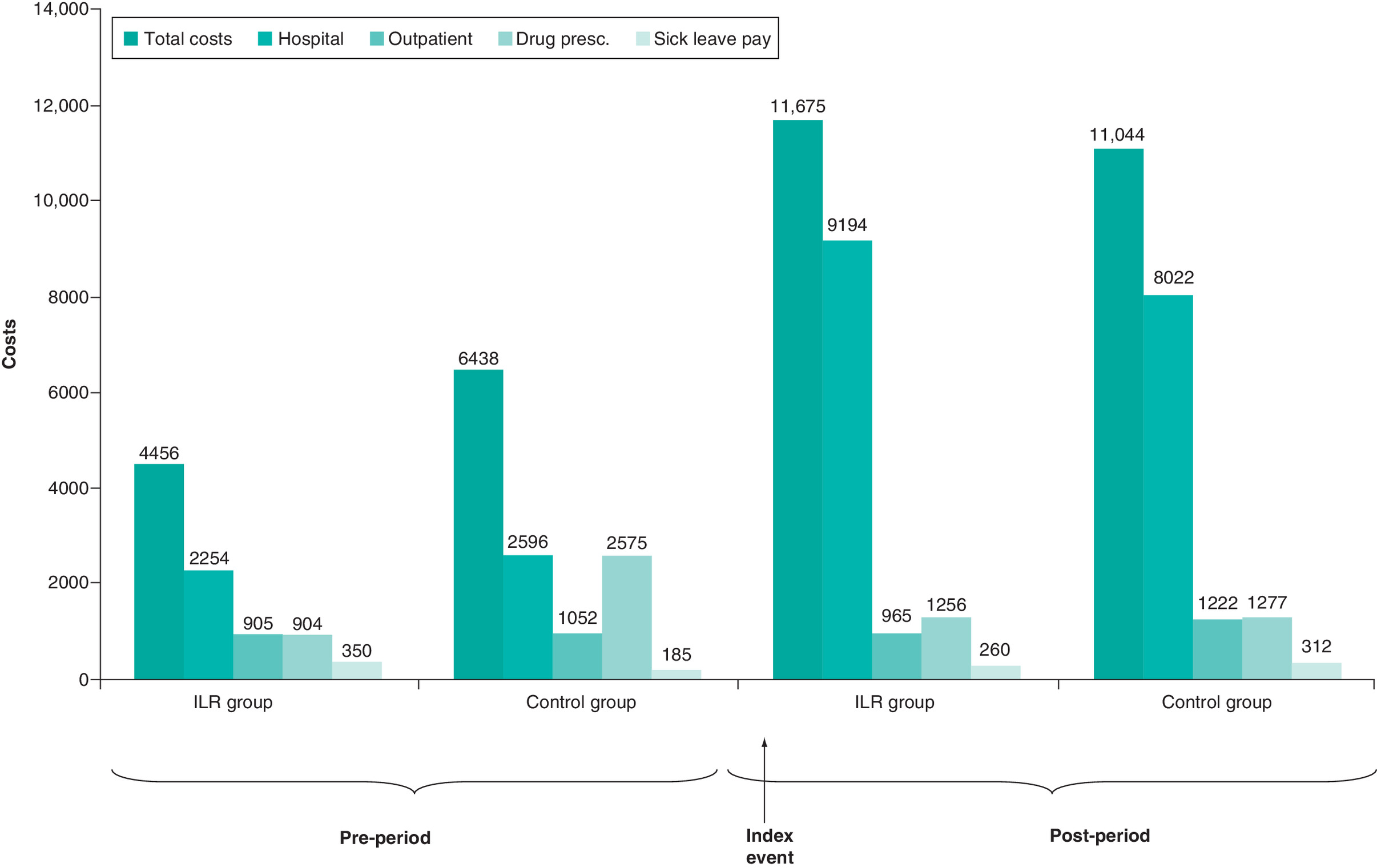
Figure 3. Comparison of mean healthcare costs.
ILR: Implantable loop recorder.
Total healthcare costs rise in both groups in the follow-up period as a result of higher hospital costs. There is no difference among the mean total healthcare costs between the two groups in the follow-up period (control = €11,043.60 vs ILR = €11,674.80, paired t-test = 0.69). The biggest share of the costs is spent on hospitalizations: 79% in the ILR group and 73% in the control group. In case of the ILR patients, the ILR implant costs are included in the follow-up costs (in Germany, ILRs are still mostly implanted in a hospitalization with overnight stay due to the lack of day case or outpatient reimbursement).
Recurrent syncope events & diagnostic tests
The number of syncope hospitalizations fell from 1.43 before the implant to 0.23 in the first year of follow-up in the ILR group. At the same time, syncope hospitalizations in the control group exhibit a similar trend, they fell from 1.3 to 0.12. Note that the syncope hospitalizations which are counted as index events are included in the baseline (Supplementary Figure 3). Both groups continue to have R55 coded in the outpatient setting: outpatient visits with a R55 code remain stable over time, at 1.5 per year for the ILR group and one visit per year in the control group. Outpatient codes do not necessarily indicate an event but could simply be carried forward. The code R55 might, for example, be coded during the follow-up of an ILR.
The control group undergoes more diagnostic testing in the follow-up period than the ILR group: 120% more 24 h Holters, 174% more MRI, 52% more computer tomography, 65% more electroencephalography (Supplementary Figure 7). Nearly all patients (99.8% in ILR group and 99% in control group) visit a specialist in the outpatient setting during follow-up. ILR patients were much more likely to see an outpatient cardiologist during follow-up (67% compared with 26% in the control group), which is likely to be connected to the follow-up of the ILR or the therapeutic device. Moreover, 43% of patients in the control group see a neurologist compared with 38% in the ILR group.
Discussion
This study analyses the survival, health careutilisations and costs of patients with recurrent syncope and compares outcomes of patients who received an ILR to a control group without ILR. Patients were followed over time and matched on syncope burden, age, gender and comorbidities. The analysis shows a remarkable difference in life expectancy between the groups. Patients with an ILR live on average 1.2 years longer than patients in the control group. The higher rates of device therapy in the ILR group are likely to be a key reason for the 1.2 life years gained as patients in the ILR group were more than 5 times more likely to receive a device therapy. The most common diagnoses resulting from an ILR are generally bradycardia resulting in a pacemaker indication and ventricular tachycardias often referred for an ICD [14]. Treatment with permanent pacemakers and defibrillators have been shown to favourably alter mortality and there are clear recommendations by clinical guidelines [16,22]. Another therapy that might contribute to the better survival is a higher treatment rate with OAC due to detection of PAF. AF is associated with increased rates of stroke and thus patients at risk of stroke are indicated for oral anticoagulation treatment if AF is detected [23]. This study adds to a recent strand of literature on life expectancy of patients with unexplained syncope. Two large claim data analysis have shown higher rates of cardiovascular death as well as all-cause mortality in patients with admission for unexplained syncope compared to a control group without syncope [3,4]. This study sheds light on the possible causes of the lower life expectancy of syncope patients and the importance of diagnosing. A selected group of syncope patients was studied to ensure comparability between ILR patients and the control group. Similar analyses are needed to replicate the results of this study to confirm the external validity. Nevertheless, the study represents an important step towards improving survival of unexplained syncope patients.
Given the difference in mortality between the matched groups, patients in the control group do not seem to receive the right care. Diagnosing and treating patients is not only important to improve life expectancy but also to enhance quality of life. Claims data unfortunately do not include information on symptoms and quality of life (QoL). Patients with untreated bradycardia have been shown to have problems carrying out daily activities, often have poor physical health, frequent fatigue and face interference with social activities [26]. Clinical studies have proven significant improvements in symptoms and quality of life from cardiac therapies such as pacemakers and ablation [16,27–30]. Claims data provide the possibility to follow patients over a long period of time and to document survival, healthcare utilization and costs. The main limitation is the observational nature of the study and the lack of detailed clinical diagnostic data, particularly electrocardiographic data. In order to compare outcomes of syncope patients, ILR patients were matched to a control group based on syncope burden, age, co-morbidities and gender. Patients with recurrent syncope and possible cardiac cause are indicated for an ILR based on guidelines. Based on the available data, it is not clear why patients in the control group did not receive an ILR. There could be various reasons such as lack of budget or awareness, patient refusal or clinical reasons unobserved in claims data. The selection for an ILR and future survival prospects could be driven by unobserved variables. This is the main limitation of every matching design.
Furthermore, claims data studies rely on the accuracy of coding. The CCI, for example, relies on a good quality of co-morbidity coding in order to accurately reflect life expectancy [31]. Furthermore, the code R55 can unfortunately only serve as proxy for syncope events. Although syncope is a well-defined term, the usage of the code R55 could be broader as the wording includes Syncope and Collapse. However, a recent validation study has shown that the administrative coding of syncope in hospital could accurately be used to identify patients with syncope event with a positive predictive value of 95% [32]. We have defined strict criteria for counting the code in the ambulatory sector. Nevertheless, it is unfortunately not possible to determine the true change in syncope events in the two groups from baseline to the follow-up period. We see a clear reduction in syncope hospitalizations in both groups while the number of outpatient visits with a diagnosis code for syncope remains stable. Since the code is likely to be carried forward, it would not be sensible to count these codes as events.
It is initially surprising that there is no difference in future hospitalizations for syncope in the control and ILR groups. The control group seems more likely to have recurrent events and to return to hospital again. However, after having been hospitalized before, patients might prefer to visit their GP or outpatient cardiologist after a new event.
Patients in the control group receive more diagnostic tests than ILR patients (Supplementary Figure 7). The diagnostic assessment of syncope is unfortunately often unsystematic, irrespective of guidelines [1]. As a consequence, patients often undergo many tests and see numerous specialists without receiving a diagnosis. Standard tests tend to be repeated many times, including various expensive diagnostic tests, which have a low diagnostic yield in unexplained syncope patients [14,24]. At the same time, ILRs are underutilized [24].
Conclusion
This study of patients with recurrent syncope shows a remarkable difference in life expectancy in patients with ILR compared with the matched control group. Two large claim data analyses have recently shown higher rates of cardiovascular death as well as all-cause mortality in patients with unexplained syncope. A more vigilant cardiac workup might be needed to identify a possible underlying cardiac condition. Following the existing guidelines for cardiac syncope with the timely indication of an ILR might lead to significant health improvements, in particular a mortality benefit. Higher rates of interventional and device therapy in the ILR group were likely to play an important role for the better life expectancy.
•
Syncope admissions have been connected to worse survival prospects in prior studies. This analysis documents the impact of different diagnostic strategies.
•
Implantable loop recorders (ILRs) are recommended in guidelines as a tool to support the diagnosis of patients with infrequent unexplained syncope.
•
First longitudinal claims data study of recurrent syncope patients compares the survival of patients who receive an ILR for diagnostic clarification to a control group.
•
The study assesses survival and costs of patients with recurrent syncope by following patients over a period of 11 years.
•
In the absence of complete data on syncope events, syncope admissions and outpatient visits are used as a proxy.
•
The analysis documents that patients who receive an ILR live on average 1.2 years longer than patients in the control group.
•
A fourth of patients in the ILR group receive a cardiac therapeutic device compared with 5% in the control groups.
•
Overall healthcare costs are the same for both groups in the follow-up period.
Financial & competing interests disclosure
Data access and statistical analysis was funded by Medtronic. C Wolff, A Witthohn and R Voss are employees of Medtronic, one of the manufacturers of implantable loop recorders. A Wilk works for Team Gesundheit, the company who performed the statistical analysis Medtronic. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (suppl_file.docx)
- Download
- 148.35 KB
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Brignole M, Moya A, de Lange FJ et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 39(21), 1883–1948 (2018).
•• The ESC Syncope Guidelines present evidence and recommendations regarding which investigations are most relevant and likely to lead to a diagnosis in syncope patients. They include a meta-analysis showing that implantable loop recorders are 3.6-times more likely to reach a diagnosis than conventional testing.
2.
Soteriades ES, Evans JC, Larson MG et al. Incidence and prognosis of syncope. N. Engl. J. Med. 347(12), 878–885 (2002).
•• Shows higher mortality for patients with recurrent syncope and a cardiac cause.
3.
Yasa E, Ricci F, Magnusson M, Sutton R, Gallina S, De Caterina R. Cardiovascular risk after hospitalisation for unexplained syncope and orthostatic hypotension. Heart 104(6), 487–493 (2018).
•• Shows that a hospitalization for unexplained syncope is associated with a higher risk of cardiovascular death and all-cause mortality. Patients have a higher risk of coronary events, strokes, heart failure and aortic stenosis.
4.
Ricci F, Sutton R, Palermi S et al. Prognostic significance of noncardiac syncope in the general population: a systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 29(12), 1641–1647 (2018).
•• Summarized the evidence for a higher all-cause mortality in patients with previous hospitalization for unexplained syncope.
5.
Sun BC. Quality-of-life, health service use, and costs associated with syncope. Prog. Cardiovasc. Dis. 55, 370–375 (2013).
6.
Linzer M, Pontinen M, Gold DT, Divine GW, Felder A, Brooks WB. Impairment of physical and psychosocial function in recurrent syncope. J. Clin. Epidemiol. 44, 1037–1043 (1991).
7.
van Dijk N, Sprangers MA, Colman N, Boer KR, Wieling W, Linzer M. Clinical factors associated with quality of life in patients with transient loss of consciousness. J. Cardiovasc. Electrophysiol. 17, 998–1003 (2006).
8.
Linzer M, Gold DT, Pontinen M, Divine GW, Felder A, Brooks WB. Recurrent syncope as a chronic disease: preliminary validation of a disease-specific measure of functional impairment. J. Gen. Intern. Med. 9(4), 181–186 (1994).
9.
Anderson JB, Czosek RJ, Knilans TK, Marino BS. The effect of paediatric syncope on health-related quality of life. Cardiol. Young. 22(5), 583–588 (2012).
10.
Numé AK, Kragholm K, Carlson N et al. Syncope and its impact on occupational accidents and employment. Circ. Cardiovasc. Qual. Outcomes 10(4), e003202 (2017).
11.
Bartoletti A, Fabiani P, Bagnoli L et al. Physical injuries caused by a transient loss of consciousness: main clinical characteristics of patients and diagnostic contribution of carotid sinus massage. Eur. Heart J. 29(5), 618–624 (2017).
12.
Rogers G, O'Flynn N. NICE guideline: transient loss of consciousness (blackouts) in adults and young people. Br. J. Gen. Pract. 61(582), 40–42 (2012).
13.
Shen WK, Sheldon RS, Benditt DG et al. 2017 ACC/AHA/HRS Guideline for the evaluation and management of patients with syncope: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 70(5), e39–e110 (2017).
14.
Edvardsson N, Frykman V, van Mechelen R et al. Use of an implantable loop recorder to increase the diagnostic yield in unexplained syncope: results from the PICTURE registry. Europace 13(2), 262–269 (2011).
•• This observational registry showed that syncope evaluations are unstructured, which results in low diagnostic yield. Some tests are repeated many times, patients undergo various expensive diagnostic tests with low diagnostic yield and see three specialists without receiving a diagnosis.
15.
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 47(11), 1245–1251 (1994).
16.
Brignole M, Auricchio A, Baron-Esquivias G et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 34(29), 2281–2329 (2013).
17.
National Institute for Health and Care Excellence (NICE). Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure. NICE Technology Appraisal Guidance 314 (2014).
18.
Priori SG, Blomström-Lundqvist C, Mazzanti A et al ; Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace 17(11), 1601–1687 (2015).
19.
Shaw DB, Kekwick CA, Veale D, Gowers J, Whistance T. Survival in second degree atrioventricular block. Br. Heart J. 53, 587–593 (1985).
20.
Shaw DB, Eraut D. Prevalence and morbidity of heart block in Devon. Br. Med. J. 1, 144–147 (1970).
21.
Simon AB, Zloto AE. Atrioventricular block: natural history after permanent ventricular pacing. Am. J. Cardiol. 41, 500–507 (1978).
22.
Connolly SJ, Hallstrom AP, Cappato R et al. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. Eur. Heart J. 21(24), 2071–2078 (2000).
23.
European Heart Rhythm Association, European Association for Cardio-Thoracic Surgery. Guidelines for the management of atrial fibrillation: the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC). Eur. Heart J. 31(19), 2369–2429 (2010).
24.
Edvardsson N, Wolff C, Tsintzos S, Rieger G, Linker NJ. Costs of unstructured investigation of unexplained syncope: insights from a micro-costing analysis of the observational PICTURE registry. Europace 17(7), 1141–1148 (2015).
25.
Vitale E, Ungar A, Maggi R et al. Discrepancy between clinical practice and standardized indications for an implantable loop recorder in patients with unexplained syncope. Europace 12(10), 1475–1479 (2010).
26.
Castelnuovo E, Stein K, Pitt M, Garside R, Payne E. The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation. Health Technol. Assess. 9(43), iii; xi–xiii, 1–246 (2005).
27.
van Eck JW, van Hemel NM, Kelder JC et al ; FOLLOWPACE Investigators. Poor health-related quality of life of patients with indication for chronic cardiac pacemaker therapy. Pacing Clin. Electrophysiol. 31(4), 480–486 (2008).
28.
Udo EO, Zuithoff NP, van Hemel NM et al. Incidence and predictors of short- and long-term complications in pacemaker therapy: the FOLLOWPACE study. Heart Rhythm 9(5), 728–735 (2012).
29.
Lamas GA, Orav EJ, Stambler BS et al. Quality of life and clinical outcomes in elderly patients treated with ventricular pacing as compared with dual-chamber pacing. Pacemaker Selection in the Elderly Investigators. N. Engl. J. Med. 338(16), 1097–1104 (1998).
30.
Kirchhof P, Benussi S, Kotecha D et al ; ESC Scientific Document Group. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 37(38), 2893–2962 (2016).
31.
Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sørensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med. Res. Methodol. 11, 83 (2011).
32.
Ruwald MH, Hansen ML, Lamberts M et al. Accuracy of the ICD-10 discharge diagnosis for syncope. Europace 15(4), 595–600 (2012).
Information & Authors
Information
Published In
Pages: 285 - 294
PubMed: 33499667
Copyright
© 2021 Claudia Wolff. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 6 November 2020
Accepted: 9 December 2020
Published online: 27 January 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Do implantable loop recorders impact the survival of patients with recurrent unexplained syncope?. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0242
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Sandeep A. Saha, Sarah Rosemas, Shantanu Sarkar, Veronica Ramos, Andrew P. Radtke, Shubha Majumder, Mirko De Melis, Jiani Zhou, J. Jason Sims, A Large, Real‐World Cohort Analysis of Arrhythmia Detection and Therapeutic Interventions in Patients With Insertable Cardiac Monitors and Long‐Term Monitoring, Journal of Cardiovascular Electrophysiology, 10.1111/jce.70214, 37, 2, (359-373), (2025).
- Lukas Duvillier, Anthony Demolder, Sally Van Renterghem, Caroline De Mey, Filip West, Jan De Pooter, Real‐world battery longevity of implantable loop recorders implanted for unexplained syncope: Results from a large single‐center registry, Journal of Cardiovascular Electrophysiology, 10.1111/jce.16420, (2024).
- Johanna Mueller-Leisse, Henrike Aenne Katrin Hillmann, Laura Iserloh, Bjoern Fruehauf, David Duncker, Diagnostic Yield and Clinical Implications of Implantable Loop Recorders in Patients with Syncope in Germany: A National Database Analysis, Journal of Clinical Medicine, 10.3390/jcm13061564, 13, 6, (1564), (2024).
- Fabio Quartieri, Manyam Harish, Leonardo Calò, Iftikhar Ebrahim, Antonio Fusco, Stephen Mester, Filippo Cauti, Seung-Jung Park, Pietro Francia, Marco Giovagnoni, Pedro Adragao, Brian Vezi, Wenjiao Lin, Chananit Sintuu Hutson, Andrea Grammatico, New insertable cardiac monitors show high diagnostic yield and good safety profile in real-world clinical practice: results from the international prospective observational SMART Registry, Europace, 10.1093/europace/euad068, 25, 5, (2023).
- Nyree Sencion-Akhtar, Aileen Ferrick, Sei Iwai, A case of an implantable cardiac monitor follow-up: Too little, too late, HeartRhythm Case Reports, 10.1016/j.hrcr.2022.06.005, 8, 9, (658-659), (2022).
- Laura Dormer, Celebrating 10 years of the Journal of Comparative Effectiveness Research, Journal of Comparative Effectiveness Research, 10.2217/cer-2021-0249, 11, 1, (1-6), (2021).
- A. Porta-Sánchez, R. Casado, O. Salvador, C. Sánchez-Enrique, S. Bayona-Horta, P. Sánchez-Borque, J.M. Rubio Campal, J.A. Cabrera, Arritmias cardíacas, Medicine - Programa de Formación Médica Continuada Acreditado, 10.1016/j.med.2021.10.011, 13, 44, (2568-2576), (2021).