The effects of pregnancy on relapse rates, disability and peripartum outcomes in women with multiple sclerosis: a systematic review and meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Although previous cohort studies of women with multiple sclerosis (MS) yielded a reduction in relapse rate during pregnancy, the effect size has not been quantified in a comprehensive manner. In addition, the effects on disability progression and peripartum outcomes have been controversial. The purpose of this work is to assess the effect of pregnancy on disease activity, and to assess the effects of MS on pregnancy as well. Materials & methods: We searched in PubMed, Cochrane Library and EMBASE for cohort studies dealing with the effects of pregnancy on relapse rates, disability progression and peripartum outcomes in women with MS. The evaluated outcomes were: changes in the annualized relapse rate (ARR) in pregnancy and puerperium, disability worsening compared with the year before pregnancy, and peripartum outcomes, which were compared with the ones of non-MS women. In the majority of cohorts included here, the women were not under disease modifying therapies during pregnancy. Results: We found 23 cohort studies measuring changes in the ARR during pregnancy and puerperium; 12 were prospective and 11 retrospective. In 17 cohorts there was significant reduction in the ARR during pregnancy compared with prepregnancy period. The pooled mean reduction in the ARR was -0.5 (95% CI: 0.67–0.38), p < 0.001, from 15 cohorts included in meta-analysis. In 18 cohorts the ARR increased in the 3-month puerperium relative to prepregnancy year period; the pooled mean increase in the ARR was 0.22 (95% CI: 0.11–0.33), p < 0.001, from 14 cohorts included in meta-analysis. Disability worsening was addressed in 18 cohorts, and in 14 of them there were no significant changes. Peripartum complications and obstetrical outcomes were assessed in 16 cohorts, of whom 13 were retrospective, without finding significant differences. Conclusion: Pregnancy is associated with lower disease activity, and puerperium with higher disease activity. Disability does not change significantly after pregnancy. The obstetrical outcomes are not very different from those of non-MS women in most cohorts.
Multiple sclerosis (MS) is a chronic immunomediated disease of the central nervous system in which inflammation, demyelination and axonal loss occur from early stages of the disease. It mainly affects young people between 20 and 40 years of age, with predominance in the female sex [1]. The average prevalence of MS in the world is 33/100,000 people, with significant variability among countries. Europe and North America have the highest prevalence (108 and 140/ 100,000 people), while Asia and sub-Saharan Africa have the lowest (2.1 and 2.2/100,000 people) [1,2].
Depending on the onset of symptoms and their clinical course, four main different phenotypes have been described: clinical isolated syndrome, relapsing-remitting MS (the most prevalent form), primary progressive MS and secondary progressive MS [1,3]. MS affects especially young women in the age of child bearing. This fact raises doubts and concerns in those patients with gestational desire, for the fear of possible complications of pregnancy, childbirth and postpartum. Before the first epidemiological studies, >50 years ago, it was thought that pregnancy was detrimental for MS women [4–6]. However, these misconceptions have changed on the light of retrospective and prospective epidemiological studies. In addition, from an immunological viewpoint, pregnancy is considered an immunotolerant state, where the maternal immune system needs to adapt to the fetal allogeneic tissue [7], so it is expected that pregnancy may result in a decrease of autoimmune diseases activity [8]. Furthermore, in an incident cohort with 308 women, a reduced risk of MS onset was found in parous women compared with nulliparous ones [9]. However, pregnancy may also worsen or exacerbate other autoimmune diseases such as acute diseminated encephalomyelitis (ADEM) and neuromyielitis optica [10].
The interrelations between pregnancy and MS have been the focus of many published systematic reviews, but only one, published in 2011, reported a meta-analysis of disease activity changes during pregnancy and puerperium. The authors gave the overall relapse rates in prepregnancy period, pregnancy and puerperium, without statistical comparison [11].
The primary objective of this systematic review is to analyze the effects of pregnancy on the clinical course of MS (relapses and disability worsening) in a quantitative manner. The secondary objective is to analyze the effects of MS on pregnancy (peripartum complications, preterm birth and low birth weight).
Materials & methods
We made a search in PubMed, EMBASE and Cochrane Library for available evidence of the interrelations between MS and pregnancy without language restrictions, from 1967 to October 2019. We followed the PRISMA guidelines for systematic reviews. Different key words were used: ‘pregnancy and multiple sclerosis’, ‘outcomes of multiple sclerosis in pregnancy’, ‘peripartum outcomes in multiple sclerosis women’, ‘relapse rate in pregnancy in multiple sclerosis’ and ‘long-term disability in pregnant women with multiple sclerosis’.
Study selection
The studies were selected by two authors. The main criteria for study selection were: to be cohort study, and to report either pregnancy outcomes in MS women or MS outcomes in pregnant women as primary end points. We did not include cohorts of women under disease modifying therapies (DMT) during pregnancy. We rejected articles based on case reports or small case series, those not dealing with outcomes in pregnant MS women, the ones not being longitudinal in nature and cohorts under DMT. A total of 1469 abstracts were screened; 1293 articles were excluded for analysis, and 91 were deemed eligible for analysis because they were longitudinal in nature and dealt with the interactions between pregnancy and MS. Finally, 64 papers were included for qualitative and/or quantitative analysis (see Flow diagram). The selection of studies was done by consensus between two appraisers.
Data extraction
We got the annualized relapse rate (ARR) in pregnancy and 3-month puerperium in comparison with either the ARR in the year before pregnancy or ARR in nonpregnant MS women, depending on the design of the study. For meta-analysis we included studies reporting the ARR before, during pregnancy and in the 3-month postpartum, giving also either standard deviation (SD) or standard error. Disability progression was based on longitudinal assessments by means of the expanded disability status scale (EDSS). We assessed as well the influence of MS on pregnancy outcomes and peripartum complications (preterm delivery, low birth weight, infections, miscarriages, influence of epidural anesthesia, breastfeeding and assisted reproductive techniques [ARTs]).
Pooled changes in ARR before pregnancy, during and after pregnancy were calculated with a fixed effects and a random effects model meta-analysis. We used the MedCalc Statistical Software version 19.1.5 (MedCalc Software bv, Ostend, Belgium; https://www.medcalc.org; 2020). Retrospective and prospective studies were also analyzed separately. Publication bias was assessed by means of funnel plots, which depicts the symmetric/asymmetric position of positive and negative studies in each side of the midline. The more symmetric the position of the studies, the less the risk of publication bias.
Heterogeneity was assessed by Q-test and inconsistency index (I2). In the event that heterogeneity was significant (I2 being >50%), it will be addressed with subgroup analysis and by calculating the rate ratios with the number of relapses, and person-years follow-up.
Results
We found 23 longitudinal studies measuring the changes in the ARR [12–34]; 12 of them were prospective [15,17–19,21–23,26–28,32] and 11 were retrospective [12–14,16,20,24,25,29,31,33,34]. In Table 1 are given the main characteristics of every study: number of patients, design, follow-up period and main outcomes. With regard to MS phenotypes, some studies did not specify the number/percentage of patients with relapsing-remitting or progressive form. According to several studies the percentage of patients with relapsing-remitting form ranged from 87.4 to 96% [19,24,27,28,31,33]. In other studies all patients had relapsing remitting (RR) forms [16,17,20,25,29,32].
| Study (year) | Cohort type | N of patients | Outcomes | Ref. |
|---|---|---|---|---|
| Ghezzi (1981) | Retrospective, 21 months | 119 pregnant vs 100 nonpregnant MS women | ARR increased from 0.33 to 0.38, up to 1.01 in postpartum | [12] |
| Korn-Lubetzki (1984) | Retrospective, 12 months | 338 women and 199 pregnancies | ARR decreased from 0.29 to 0.14; increased ARR in postpartum to 0.82 | [13] |
| Frith (1988) | Retrospective, 15 months | 52 women and 85 pregnancies | ARR decreased from 0.53 to 0.18; down to 0.13 in postpartum | [14] |
| Bernardi (1991) | Prospective, 15 months | 52 women and 66 pregnancies | ARR decreased from 0.65 to 0.10; increased in postpartum to 0.79 | [15] |
| Nelson (1988) | Retrospective, 9 months after delivery | 191 pregnancies | AAR: 0.13 unchanged, but increased in postpartum to 0.4 | [16] |
| Roullet (1993) | Prospective, up to 6 months postpartum | 33 women and 49 pregnancies | ARR increased from 0.51 to 0.61; NS; increased in postpartum to 1.61 | [17] |
| Sadovnick (1994) | Prospective, 15 months | 47 women, 69 pregnancies and 64 controls | ARR decreased from 0.57 to 0.42; NS; rose to 0.75 in postpartum | [18] |
| Confavreux (1998) | Prospective, 12 months postpartum | 254 women with 269 pregnancies | ARR decreased from 0.7 to 0.2; rose in postpartum to 1.2 | [19] |
| Salemi (2004) | Retrospective, mean disease duration 16 years | 70 women with 98 pregnancies, vs 281 nonpregnant | ARR decreased from 0.48 to 0.36; rose to 0.84 in postpartum | [20] |
| Airas (2010) | Prospective, 6 months postpartum | 61 women | ARR decreased from 0.82 to 0.40; rose to 1.40 in puerperium | [21] |
| Portaccio (2011) | Prospective, 1 year after delivery | 298 women, 302 pregnancies | ARR decreased from 0.4 to 0.12; rose to 0.55 in postpartum | [22] |
| Keyhanian (2012) | Prospective, 6 years after delivery | 102 women | ARR decreased from 1.06 before pregnancy to 0.35; rose to 1.02 in postpartum | [23] |
| Hughes (2014) | Retrospective, 24 months postpartum | 674 women, 893 pregnancies | ARR decreased from 0.32 to 0.20; rose to 0.61 in postpartum | [24] |
| Karp (2014) | Retrospective, 3 years | 254 pregnant vs 423 nonpregnant women | ARR decreased in pregnant women; rate ratio: 0.67 (0.49–0.92) | [25] |
| Fares (2016) | Prospective, 5 years | 29 pregnant women, 64 pregnancies | ARR decreased from 0.17 to 0; rose to 0.2 at 1 year of postpartum | [26] |
| Benoit (2016) | Prospective, 1 year | 161 women, 93 with two pregnancies each | ARR decreased from 0.52 to 0.24; rose to 1.33 in postpartum | [27] |
| Cuello (2017) | Prospective, 1 year | 35 MS women and 40 pregnancies, vs 56 healthy women | ARR decreased from 0.5 to 0.3; rose to 0.4; NS | [28] |
| Jesus-Ribeiro (2017) | Retrospective, 33 months | 97 women, 127 deliveries | AAR decreased from 0.6 to 0.3; up to 0.98 in puerperium | [29] |
| Lai (2018) | Prospective, 1 year after delivery | 14 women and 15 pregnancies | ARR decreased from 0.46 to 0.07; rose to 0.55 in postpartum | [30] |
| Houtchens (2018) | Retrospective, 1 year postpartum | 2158 women | ARR decreased from 1.47 to 0.87; rose to 2.56 in postpartum | [31] |
| Bsteh (2018) | Prospective, 2 years | 239 women and 387 pregnancies | ARR decreased from 0.38 to 0.18; rose to 0.64 in postpartum | [32] |
| Alroughani (2019) | Retrospective, up to 3 months postpartum | 132 women, 164 pregnancies | ARR increased from 0.1 to 0.2 | [33] |
| MacDonald (2019) | Retrospective, up to 6 months postpartum | 1168 women | NS change, from 0.5 to 0.4; in postpartum 0.5 | [34] |
ARR: Annualized relapse rate; MS: Multiple sclerosis; NS: Not significant.
With regard to DMT, most cohorts included women not under treatment during pregnancy. In five cohorts the percentage of women exposed to DMT were: 1.2 [24], 3.7 [33], 15.3 [25], 17 [31] and 34% in a small cohort of 35 women [28].
Changes in the ARR
In 16 studies, the ARR decreased significantly in pregnancy (see Table 1), especially in the third trimester. The ARR were unchanged or not significant in four studies [16,18,28,34]. In two cohorts the ARR increased mildly, without statistical significance [12,17]. Only in one of the studies the ARR increased significantly from 0.10 to 0.20, as a consequence of DMT withdrawal before pregnancy [33]. The comparisons were made with a control group of nonpregnant MS women in five studies [12,18,20,25,28], and with the patients as self-controls in the year before pregnancy in all of the studies. In meta-analysis we included the papers giving the mean number of relapses and SD. One of the studies with small number of cases and high percentage on DMT during pregnancy was also excluded from meta-analysis [28]. The pooled mean change in the ARR from the preconception period to pregnancy was -0.5 (95% CI: 0.67–0.38) from 15 cohorts included in meta-analysis, which was significant (see Figure 1). For retrospective studies it was -0.47 (95% CI: 0.79–0.15), and -0.47 (95% CI: 0.65–0,30) for prospective studies; p < 0.001 for both analyses. Heterogeneity was present in the three analyses (I2 being >75%). Funnel plot shows also heterogeneity, without bias of publication (Figure 2).
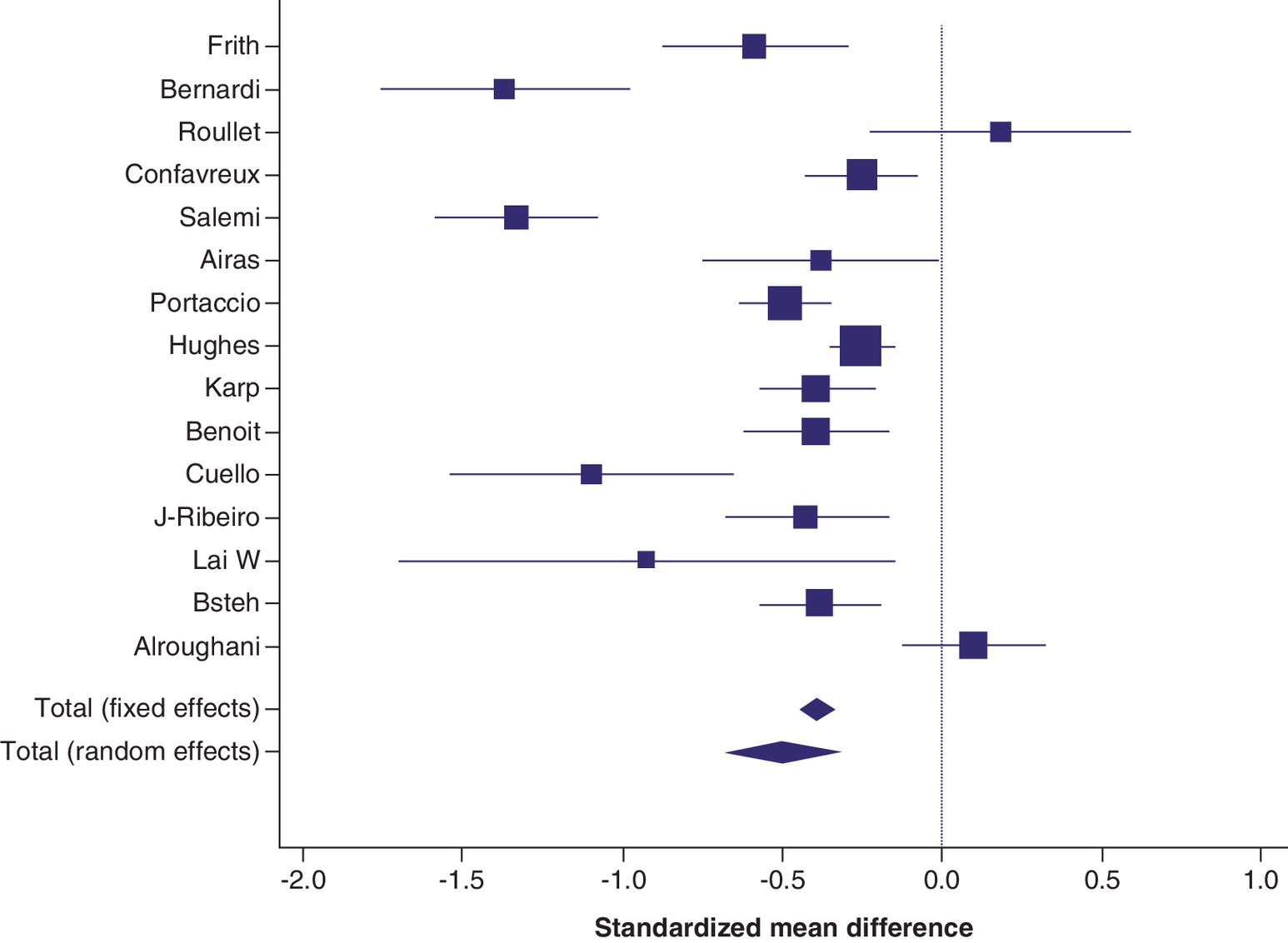
Figure 1. Meta-analysis from cohort studies giving the mean change in the annualized relapse rate before pregnancy/pregnancy.
Fixed effects model. Pooled SMD: -0.39 (95% CI: 0.44–0.34); p < 0.001. Random effects model. Pooled SMD: -0.5 (95% CI: 0.67–0.38), p < 0.001. I2: 89.7%.
I2: Inconsistency index; SMD: Standardized mean difference.
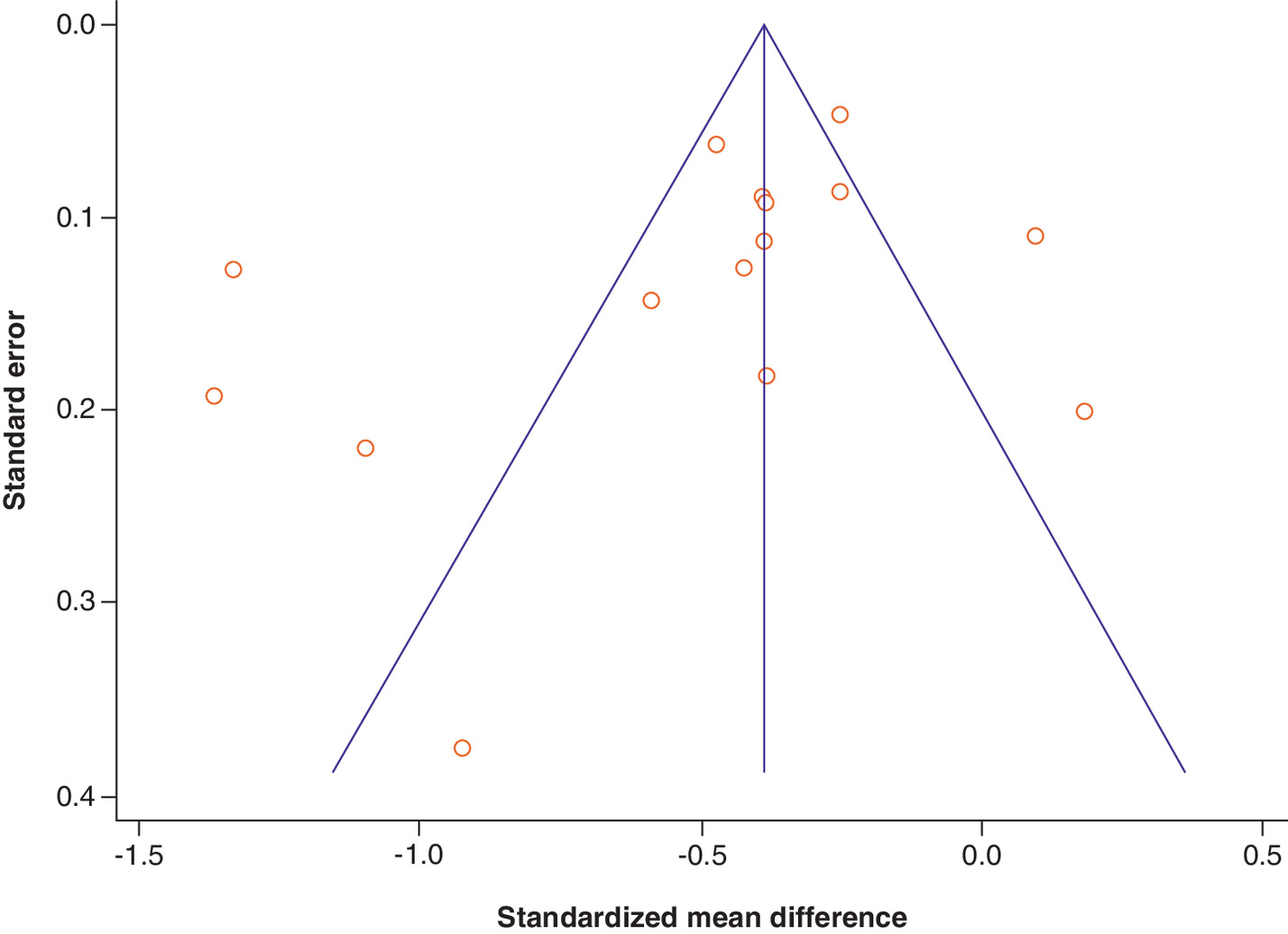
Figure 2. Funnel plot of meta-analysis showing variability of effect size among studies.
Several points out of the triangle in both sides. Small risk of publication bias, as there were studies in both sides of the midline.
In 19 studies, the ARR increased in the 3-month puerperium compared with the year before pregnancy. In one study the rate decreased [14], in another one it did not change [34] and in two studies no information was given on puerperium relapses [24,33]. Mean relapse number and SD were given in 14 studies. The pooled mean change in ARR between prepregnancy period and 3-month puerperium from these 14 studies was 0.22 (95% CI: 0.11–0.33), p < 0.001 (Figure 3), and it was similar for prospective and retrospective studies. In this analysis, heterogeneity was lower than before (I2: 73%). In the funnel plot of Figure 4, the bias of publication cannot be ruled out.
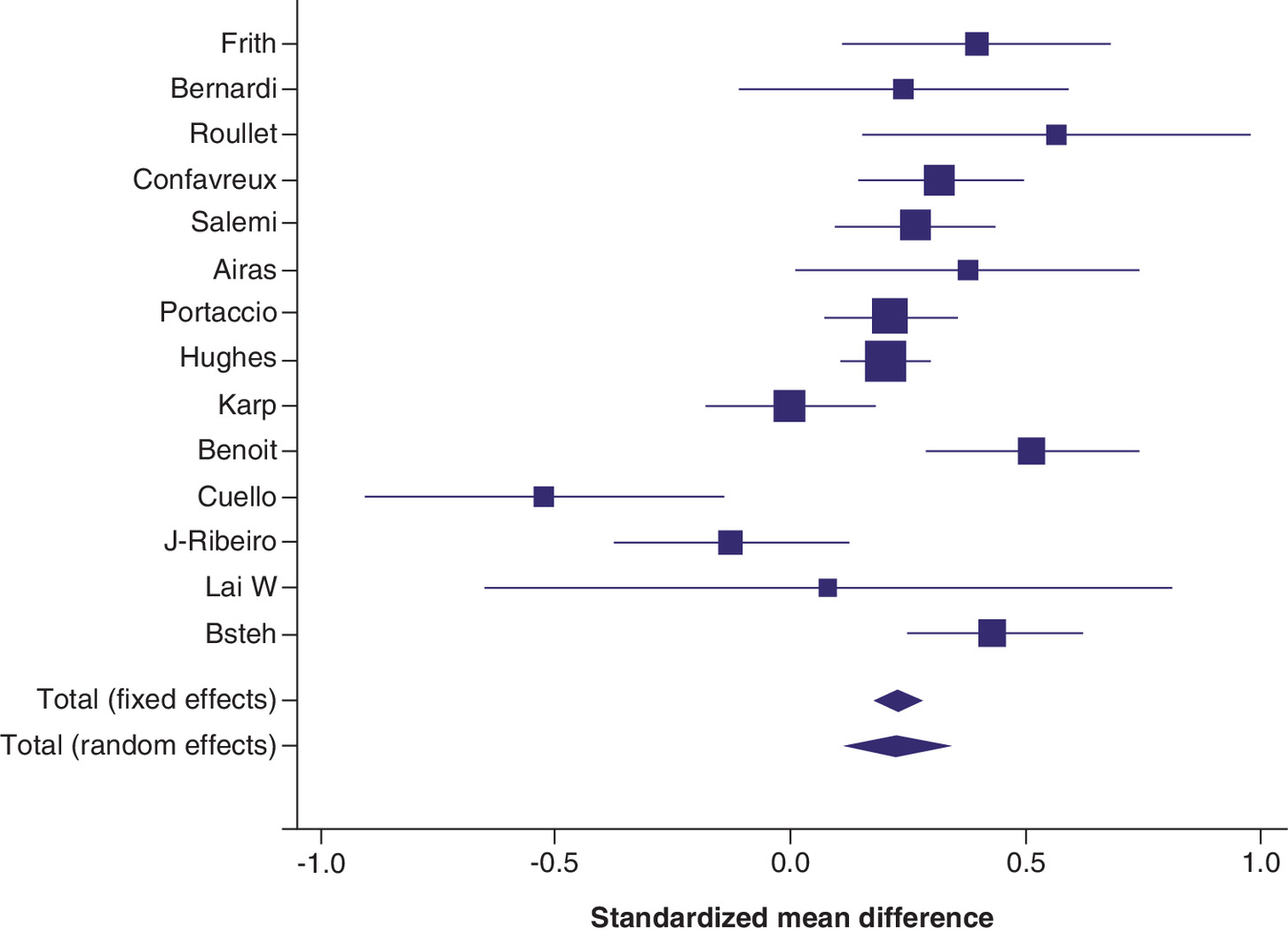
Figure 3. Meta-analysis from cohort studies giving the change in the mean annualized relapse rate pregnancy/puerperium.
Fixed effects model. Pooled SMD: 0.22 (95% CI: 0.17–0.28). Random effects model: Pooled SMD: 0.22 (95% CI: 0.116–0.336. I2 73% (53–84%).
I2: Inconsistency index; SMD: Standardized mean difference.
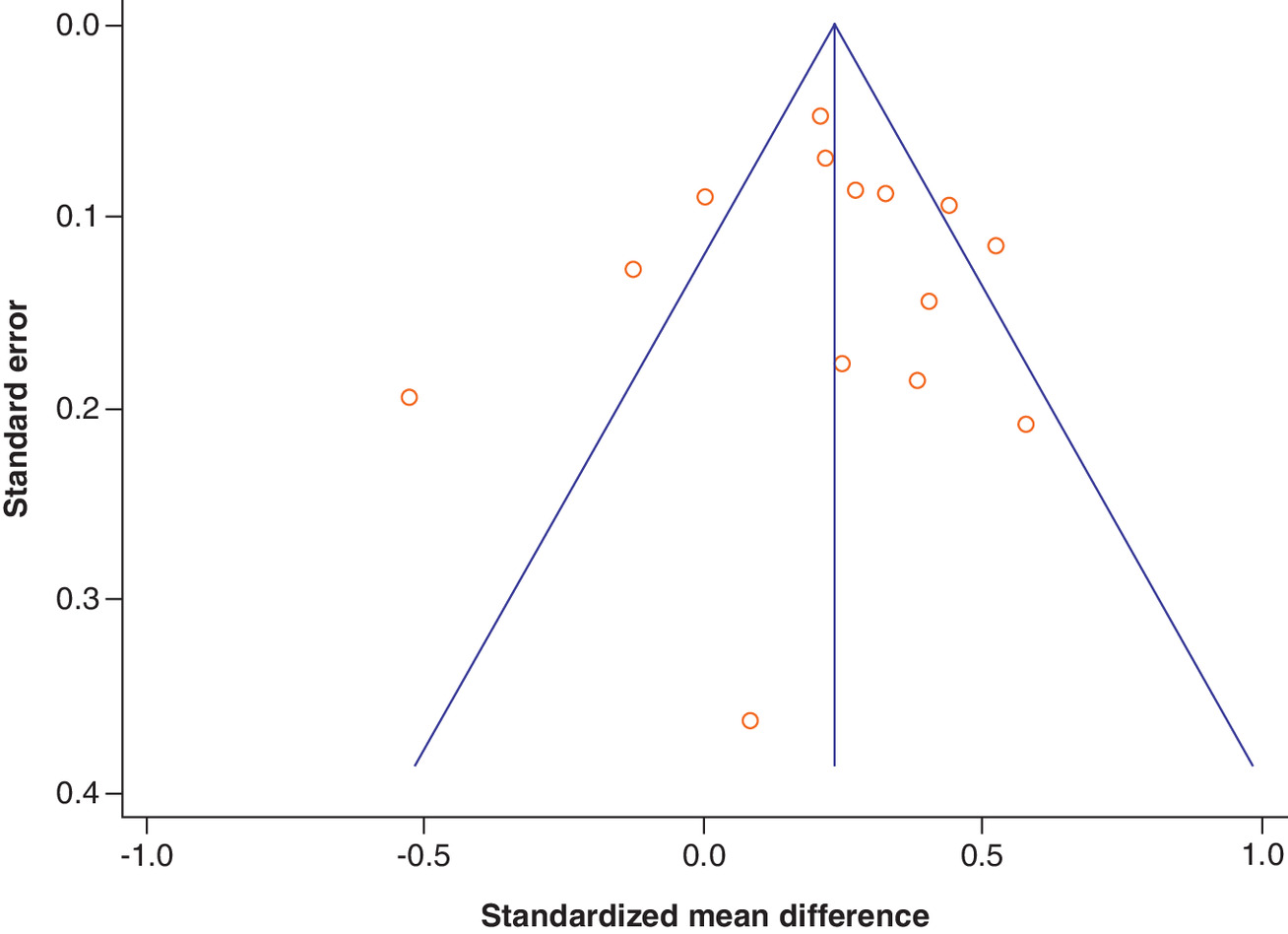
Figure 4. Funnel plot of meta-analysis of the increase in annualized relapse rate from pregnancy to puerperium.
Symmetric distribution of studies, with some outliers. Small risk of publication bias.
From the evidence presented in all of these studies, we can infer with confidence that pregnancy is associated with a decrease in the ARR in MS women relative to the preconception period, and with an increase in puerperium, especially in the 3 months after delivery. According to funnel plots, publication bias cannot be excluded.
Disability worsening
The papers dealing with disability worsening are given in Table 2. Among 18 studies, seven were prospective [9,17,23,28,30,35,36] and 11 were retrospective [24,25,37–45]. In 14 studies there was no significant disability worsening after pregnancy; in three the risk of disability worsening decreased [35,42,43] and in one it increased [30]. In the cohort of Karp et al. [25], the rate of irreversible disability at 5 and 10 years was similar, but the rates of transition to progressive forms were higher in pregnant MS women than in nonpregnant MS women. Thus, pregnancy does not increase the risk of disability worsening in MS women.
| Author (year) | Cohort and follow-up | N of patients | OR/RR and 95% CI, other measure | Ref. |
|---|---|---|---|---|
| Poser (1983) | Retrospective, 6 months after delivery | 91 women and 129 pregnancies, vs 64 MS controls | Progression index not different from controls | [37] |
| Thompson (1986) | Retrospective | 178 women | No differences in long-term disability | [38] |
| Weinshenker (1989) | Retrospective | 185 women | No differences in long-term disability | [39] |
| Roullet (1993) | Prospective, 10 years | 33 women with 49 pregnancies | Variation of EDSS: NS Transition to SPMS: 1.38 (0.68–2.78); NS | [17] |
| Verdru (1994) | Prospective, 18 years | 200 women | Mean time to wheelchair: 18.6 years for pregnant, and 12.5 for nonpregnant women† | [35] |
| Runmaker (1995) | Prospective | 308 women | Time to reach 6 points on EDSS: NS | [9] |
| Vukusic (2006) | Prospective, 2 years postpartum | 254 women | No differences in disability progression | [36] |
| Koch (2009) | Retrospective, 17 tear disease duration | 277 women | No differences in disability progression | [40] |
| Ramagopalan (2012) | Retrospective, 15 year disease duration | 2105 women | No effect on time to reach 6 points in EDSS | [41] |
| D'Hooghe (2012) | Retrospective, disease duration 19 years | 973 women | Lower risk of disability progression with two or more pregnancies; OR: 0.66† | [42] |
| Keyhanian (2012) | Prospective, 6 years after delivery | 102 women | No influence on disability progression | [23] |
| Karp (2014) | Retrospective, 5- and 10-year outcomes | 254 pregnant vs 423 nonpregnant women | – 5 Year: irreversible disability: 0.82 (0.36–1.88) – 10 Year: 4.14 (0.89–19.22) – 5 Year transition to SPMS: 2.33 (1.03–5.26)† – 10 Year transition to SPMS: 4.33 (1.1–19.96)† | [25] |
| Hughes (2014) | Retrospective, 24 months postpartum | 674 women, 893 pregnancies | EDSS unchanged | [24] |
| Masera (2015) | Retrospective, 14 year disease duration | 445 women, 184 parous | Lower risk of disease progression; OR: 0.55† to reach an EDSS of 6 points | [43] |
| Altintas (2015) | Retrospective, 13 year disease duration | 199 women and 558 pregnancies | Time to reach 6 points on EDSS not significant | [44] |
| D'Amico (2016) | Retrospective, 7 year observation period | 86 women with one or more pregnancies | No differences in time to reach 4 or 6 points in EDSS | [45] |
| Cuello (2017) | Prospective, 2 years after delivery | 35 MS women and 40 pregnancies, vs 56 healthy women | No significant changes in EDSS score | [28] |
| Lai (2018) | Prospective, 1 year after delivery | 14 women and 15 pregnancies | Mean EDSS 1 year after delivery 1.5 (SD: 1.72) vs 0.77 (SD: 1.35) before pregnancy; p = 0.045 | [30] |
†
Means significant.
‡ Means significant difference.
EDSS: Expanded disability status scale; NS: Not significant; OR: Odds ratio; SD: Standard deviation; SPMS: Secondary progressive multiple sclerosis.
Obstetrical outcomes
Seventeen studies focused specifically on the effects of MS on pregnancy with peripartum outcomes; 14 were retrospective [5,37–39,46–55] and three were prospective [28,56,57]. In 12 of them, there were no significant differences in preterm deliveries, congenital malformations, miscarriages, stillbirths and abortions (see Table 3). In two retrospective cohorts, there was an increased number of infections and preterm deliveries [34,50], an increased number of preterm deliveries and low birth weight [47], low birth weight in another one [46], and anemia and rehospitalization in one study [52] (see Table 3). The evidence found here is not strong enough to draw definitive conclusions, but the available data are reassuring in this respect. Other pregnancy-related factors influencing the clinical course of MS are breastfeeding and analgesia. There is remarkable evidence that breastfeeding does not have influence on relapse recurrence, peripartum outcomes and long-term prognosis of MS [16,21,22,29,36,58]. Epidural analgesia has not been associated either with negative outcomes in puerperium [29,36,48,55,59].
| Author (year) | N of MS patients | Results | Ref. |
|---|---|---|---|
| Liebowitz (1967); retrospective | 131 MS patients vs 523 controls | No differences in live births, stillbirths or abortions | [5] |
| Worthington (1994); prospective | 15 women vs 22 nonpregnant MS women | No effect on pregnancy No effect on peripartum children outcomes | [56] |
| Poser (1983); retrospective | 91 pregnant women vs 64 MS nonpregnant women | No effect on the risk of congenital malformation | [37] |
| Dahl (2005); retrospective | 461 women and 649 deliveries vs 2 million control births | Lower birth weight compared with controls | [46] |
| Chen (2009); retrospective | 174 MS women vs 1392 controls | Increased risk of preterm delivery and low weight | [47] |
| MacDonald (2019); retrospective | 3875 pregnancies vs controls | Increased risk of infections and preterm delivery | [34] |
| Hanulikova (2013); retrospective | 66 women vs controls | No differences in preterm deliveries or miscarriages | [48] |
| Cuello (2017); prospective | 35 MS women and 40 pregnancies, vs 56 healthy women | No differences in peripartum outcomes | [28] |
| Goldacre (2017); retrospective | 98 women and 191 pregnancies vs controls | No differences in peripartum outcomes | [49] |
| Houtchens (2018); retrospective | 2115 women vs 2115 non-MS women | Mild increased number of infections, preterm deliveries, anemia and coagulation disorders | [50] |
| Fong (2018); retrospective | 1185 deliveries vs controls | No differences in peripartum outcomes | [51] |
| Mueller (2002); retrospective | 198 MS women vs 1584 controls | Increased risk of anemia and rehospitalization | [52] |
| van der Kop (2011); retrospective | 432 MS women vs 2975 controls | No differences in peripartum outcomes | [53] |
| Kelly (2009); retrospective | 10,055 deliveries in MS women vs 18 million controls | No differences in peripartum outcomes | [54] |
| Alroughani (2019); retrospective | 164 pregnancies vs controls | No differences in peripartum outcomes | [33] |
| Jalkanen (2020); prospective | 61 women | No differences in peripartum outcomes | [57] |
| Balslev Andersen (2019); retrospective | 5760 pregnancies in MS women vs 27,664 from general population | No differences in peripartum outcomes | [55] |
MS: Multiple sclerosis.
What about ART in MS women? Some small case series yielded an increased risk of relapse after ART [60–64]. In a Bostonian cohort with 22 ART cycles, the relapse rate was not higher after ART than before, but in a meta-analysis of the same authors there was found an increase in the ARR after ART of 0.92 compared with the year before ART, but with small effect size (p = 0.01) [64].
In this systematic review, we did not analyzed pregnancy outcomes on women exposed to DMT.
Subgroup analysis, sensitivity analysis & interactions
We compared prospective with retrospective cohorts, taking into account the number of patients included in each study. With regard to relapse rate changes in pregnancy months, there is an agreement between prospective and retrospective cohorts on the decreased ARR. The increased ARR in puerperium is found in most studies, in retrospective and in prospective studies as well. The ARR change varied among studies, but with the generic inverse variance method, the results of meta-analysis were similar, and with higher degree of heterogeneity. Withdrawing cohorts before the DMT era (studies published before 1995) from analysis did not result in a lower degree of heterogeneity. The same happened when small cohorts were excluded from analysis. Given that the cohorts come from different countries in the world, heterogeneity may be explained by interactions by country.
With a different approach and other metric (rate ratios), another meta-analysis was conducted from 20 cohorts reporting the number of relapses and person-year follow-up [12–22,24,26–30,32–34] (see Table 4). In the preconception period, 2296 relapses happened for 5815 person-years, in comparison with 772 relapses for 3158 person-years in pregnancy; rate ratio: 0.61 (95% CI: 0.56–0.67). In puerperium, 1378 relapses were reported for 2380 person-years; the rate ratio preconception/puerperium was 1.46 (95% CI: 1.37–1.56); the rate ratio pregnancy/puerperium was 2.38 (95% CI: 2.16–2.59). The pooled incidence rate difference between preconception period and pregnancy was -0.15 (95% CI: 0.17–0.12), and 0.18 (95% CI: 0.15–0.21) between preconception and postpartum period, but heterogeneity remained. With this approach, we have the advantage of including more cohorts in the meta-analysis, but the main caveat is that the follow-up period of prepregnancy and puerperium varied considerably across cohorts, so heterogeneity could be explained by this fact. In general terms, the results are equivalent with both methods, which increases robustness of the conclusions.
| Cohort | Prepregnancy period, 1 year or longer | Pregnancy, 9 months | Puerperium, 3 months or longer | Ref. | |||
|---|---|---|---|---|---|---|---|
| Relapses | Person-years | Relapses | Person-years | Relapses | Person-years | ||
| Ghezzi (1981) | 301 | 947 | 34 | 89 | 91 | 30 | [12] |
| Korn-Lubetzki (1984) | 40 | 199 | 20 | 143 | 32 | 50 | [13] |
| Frith (1988) | 193 | 327 | 40 | 106 | 14 | 25 | [14] |
| Nelson (1988) | 25 | 191 | 19 | 143 | 54 | 95 | [16] |
| Salemi (2004) | 542 | 1001 | 25 | 73 | 18 | 294 | [20] |
| Bernardi (1991) | 254 | 393 | 5 | 49 | 26 | 33 | [15] |
| Hughes (2014) | 164 | 514 | 178 | 669 | 127 | 207 | [24] |
| Jesus-Ribeiro (2017) | 52 | 127 | 22 | 95 | 27 | 32 | [29] |
| Confavreux (1998) | 164 | 227 | 71 | 170 | 68 | 55 | [19] |
| Lai (2018) | 7 | 14 | 1 | 10 | 8 | 3.5 | [30] |
| Sadovnick (1994) | 39 | 69 | 22 | 52 | 26 | 34 | [18] |
| MacDonald (2019) | 117 | 292 | 140 | 876 | 93 | 292 | [34] |
| Alroughani (2019) | 17 | 164 | 25 | 130 | NA | NA | [33] |
| Cuello (2017) | 25 | 70 | 7 | 26 | 18 | 70 | [28] |
| Airas (2010) | 50 | 61 | 18 | 46 | 21 | 15 | [21] |
| Roullet (1993) | 143 | 280 | 25 | 37 | 19 | 12 | [17] |
| Portaccio (2011) | 121 | 302 | 27 | 226 | 166 | 302 | [22] |
| Benoit (2016) | 106 | 186 | 41 | 121 | 53 | 40 | [27] |
| Fares (2016) | 5 | 64 | 0 | 48 | 0 | 16 | [26] |
| Bsteh (2018) | 147 | 387 | 52 | 290 | 495 | 774 | [32] |
| Total | 2296 | 5815 | 772 | 3158 | 1378 | 2380 | |
NA: Not available.
In terms of disability worsening, most prospective and retrospective studies pointed to nonsignificant differences (Table 2). In nine out of 11 retrospective studies including a total of 4039 women, pregnancy was not associated with disability worsening. Only in two retrospective cohorts, and in one prospective totaling 1618 MS women followed-up, pregnancy was protective in comparison with controls or the same patients year before pregnancy [38,42,43]. In five out of seven prospective cohorts, disability did not change; in one cohort decreased [35] and in another cohort disability increased after pregnancy but the number of patients included were small [30]. Disability worsening was analyzed in two ways: survival time to reach an EDSS of 6 points, or the mean EDSS score comparison before and after pregnancy.
In relation with peripartum outcomes (see Table 3), although there is no enough evidence to conclude that MS pregnant women have similar rates of complications and fetal outcomes, more studies revealed no differences than those did it. In five retrospective studies totaling 6823 pregnancies, there is an increased risk of infections [34,50], preterm deliveries [34,50], low birth weight [46,47], anemia [50,52] and rehospitalization [52], compared with non-MS pregnant women, versus the rest of studies pointing to similar outcomes and that totaled 19,619 women [5,28,33,37,48,49,51,53–55,57].
Discussion
In this systematic review, we can confirm the assumption that the relapse rate decreases in MS pregnant women, and that it increases in the 3-month puerperium period. These results were obtained with two different approaches of meta-analysis (differences in the mean relapse rate, and rate ratios). Pregnancy is not associated with disability worsening. With the cumulated evidence, the misconception of the negative effect of pregnancy in MS women has disappeared, and the number of pregnancies in these women has increased over time [49]. However, there are issues pending elucidation. One of them is the risk of reactivation of MS after withdrawal of DMT in pregnancy, especially when fingolimod or natalizumab is used before pregnancy [33,66]. Second, given that the risk of relapses increases in puerperium, early resumption of treatment might reduce the risk of relapse after delivery [24,32,66,67], but additional evidence is needed [68]. In a large cohort that extended follow-up to 9–12 month puerperium, the ARR did not return to prepregnancy level, despite 17% of patients were on self-injectable DMT during pregnancy [31]. The influence of DMT drugs has not been analyzed in this review, and the subject is being investigated through data of large cohorts and registries.
There is no clear reason for an increased risk of relapse in puerperium, but it has been related with the abrupt decrease in estrogen levels and cessation of the immunotolerant state in pregnancy [69].
Some studies concluded that breastfeeding may be protective against relapse and disability [19,70–72], but it is still controversial and deserves further research.
The main strength in our meta-analysis is the large number of patients included, and the narrow confidence interval of the mean change in the ARR. The agreement between prospective and retrospective studies gives also robustness to the conclusions. In the sensitivity analysis both methods of meta-analysis (mean changes and SD in the ARR, and rate ratios according to the number of relapses for person-years) agreed in the results but also in heterogeneity. A limitation of this review is the inconsistency found among the different studies with regard to the size of ARR reduction, but not to the fact that pregnancy is associated with a reduced ARR. We tried to minimize heterogeneity by excluding studies with few cases or with largest SDs. Given that the demographic characteristics of patients are not different among cohorts analyzed, interaction by country or ethnic factors may explain the variation in the effect size found in our meta-analysis. In a recent meta-analysis focused on factors associated with relapses in MS patients, the authors found similar results pooled from four studies, with pregnancy being protective of relapses. The risk of relapses increased in puerperium according to the analysis from eight cohorts [73].
In terms of disability progression, pregnancy is too short to draw conclusions. It is worth mentioning a cohort study in which the patients with at least two pregnancies had lower risk of disability worsening [42]. However, this was not found in two cohorts of MS women with at least two pregnancies [27,40].
Conclusion
In conclusion, pregnancy in MS is associated with decreased ARR, but with increased ARR in puerperium, without influence on disability worsening. MS is not associated with poorer peripartum outcomes in comparison with non-MS women. In vitro fertilization increases the risk of relapse.
•
Pregnancy is associated with significant reduction of the relapse rate in women with multiple sclerosis. However, in the 3-month postpartum period the disease activity tends to rebound.
•
After pregnancy there is no neurological disability worsening compared with the 1-year prepregnancy period.
•
Successive pregnancies do not increase disease activity either.
•
Pregnancy is not associated with worse peripartum outcomes and obstetrical complications in comparison with women of the general population.
•
Breastfeeding per se does not increase the risk of relapses. However, it may be discouraged in women under determined disease modifying therapies.
•
Assisted reproductive techniques in women with multiple sclerosis may result in relapse recurrence.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
1.
Vidal-Jordana A, Montalban X. Multiple sclerosis: epidemiologic, clinical and therapeutic aspects. Neuroimaging Clin. N. Am. 27(2), 195–204 (2017).
2.
Galetta KM, Bhattacharyya S. Multiple sclerosis and autoimmune neurology of the central nervous system. Med. Clin. North Am. 103(2), 325–336 (2019).
3.
Katz Sand I. Classification, diagnosis, and differential diagnosis of multiple sclerosis. Curr. Opin. Neurol. 28, 193–205 (2015).
4.
Schapira K, Poskanzer D, Neill D, Miller H. Marriage, pregnancy and multiple sclerosis. Brain 89, 419–428 (1966).
5.
Liebowitz U, Antonovsky A, Kats R, Alter M. Does pregnancy increase the risk of multiple sclerosis? J. Neurol. Neurosurg. Psych. 30, 354–357 (1967).
6.
Antonovsky A, Liebowitz U, Medalie JM, Smith HA, Halpern L, Alter M. Reappraisal of possible etiologic factors in multiple sclerosis. Am. J. Public Health Nations Health 58, 836–848 (1968).
7.
Avila M, Bansal A, Culberson J, Peiris AN. The role of sex hormones in multiple sclerosis. Eur. Neurol. 80, 93–95 (2018).
8.
Tavakolpour S, Rahimzadeh G. New insights into the management of patients with autoimmune diseases or inflammatory disorders during pregnancy. Scand. J. Immunol. 84(3), 146–149 (2016).
9.
Runmaker B, Andersen O. Pregnancy is associated with a lower risk of onset and a better prognosis in multiple sclerosis. Brain 118, 253–261 (1995).
10.
Qiu K, Qiang H, Xigian C, Hui L, Shuwen D, Wei L. Pregnancy-related immune changes and demyelinating diseases of the central nervous system. Front. Neurol. 10, 1070 (2019).
11.
Finkelstejn A, Brooks JB, Paschoal FM Jr, Fragoso YD. What can we really tell women with multiple sclerosis regarding pregnancy? A systematic review and meta-analysis of the literature. BJOG 118, 790–797 (2011).
12.
Ghezzi A, Caputo D. Pregnancy: a factor influencing the course of multiple sclerosis? Eur. Neurol. 20, 115–117 (1981).
13.
Korn-Lubetzki I, Kahama E, Cooper G, Oded A. Activity of multiple sclerosis during pregnacy and puerperium. Ann. Neurol. 16, 229–231 (1984).
14.
Frith JA, McLeod JG. Pregnancy and multiple sclerosis. J. Neurol. Neurosurg. Psych. 51, 495–498 (1988).
15.
Bernardi S, Grasso MG, Bertollini R, Orzi F, Fieschi C. The influence of pregnancy on relapses in multiple sclerosis: a cohort study. Acta Neurol. Scand. 84, 403–406 (1991).
16.
Nelson LM, Franklin GM, Jones MC. Risk of multiple sclerosis exacerbation during pregnancy and breast-feeding. JAMA 259, 3441–3443 (1988).
17.
Roullet E, Verdier-Taillefer MH, Amarenco P, Gharbi G, Alperovitch A, Marteau R. Pregnancy and multiple sclerosis: a longitudinal study of 125 remittent patients. J. Neurol. Neurosurg. Psych. 56, 1062–1065 (1993).
18.
Sadovnick AD, Eisen K, Hashimoto SA et al. Pregnancy and multiple sclerosis. A prospective study. Arch. Neurol. 51, 1120–1124 (1994).
19.
Confavreux C, Hutchinson M, Hours MM, Cortinovis P, Moreau T. Rate of pregnancy-related relapse in multiple sclerosis. Pregnancy in multiple sclerosis group. N. Engl. J. Med. 339, 285–291 (1998).
20.
Salemi G, Callari G, Gammino M et al. The relapse rate of multiple sclerosis changes during pregnancy: a cohort study. Acta Neurol. Scand. 110, 23–26 (2004).
21.
Airas L, Jalkanen A, Alanen A, Pirttila T, Marttila RJ. Breastfeeding, postpartum and pregnancy disease activity in multiple sclerosis. Neurology 75, 474–476 (2010).
22.
Portaccio E, Ghezzi A, Hakki B et al. Breastfeeding is not related to postpartum relapses in multiple sclerosis. Neurology 77, 145–150 (2011).
23.
Keyhanian K, Davoudi V, Etemandifar M, Amin M. Better prognosis of multiple sclerosis in patients who experienced a full-term pregnancy. Eur. Neurol. 68, 150–155 (2012).
24.
Hughes SE, Spelman T, Gray OM et al. Predictors and dynamics of postpartum relapses in women with multiple sclerosis. Mult. Scler. 20, 739–746 (2014).
25.
Karp I, Manganas A, Sylvestre MP, Ho A, Roger E, Duquette P. Does pregnancy alter the long-term course of multiple sclerosis?. Ann. Epidemiol. 24, 504e2–508e2 (2014).
26.
Fares J, Nassar AH, Gebeily S, Kobeissy F, Fares Y. Pregnancy outcomes in Lebanese women with multiple sclerosis (the LeMS study): a prospective multicentre study. BMJ Open 6, e011210 (2016).
27.
Benoit A, Durand-Dubief F, Amato MP et al. History of multiple sclerosis in 2 successive pregnancies: a French and Italian cohort. Neurology 87, 1360–1367 (2016).
28.
Cuello JP, Martinez Ginés ML, Martin Barriga ML, de Andrés C. Multiple sclerosis and pregnancy: a single-centre prospective comparative study. Neurologia 32, 92–98 (2017).
29.
Jesus-Ribeiro J, Correia I, Martins AI et al. Pregnancy in multiple sclerosis: a Portuguese cohort study. Mult. Scler. Relat. Disord. 17, 63–68 (2017).
30.
Lai W, Kinoshita M, Peng A et al. Does pregnancy affect women with multiple sclerosis? A prospective study in Western China. J. Neuroimmunol. 321, 24–28 (2018).
31.
Houtchens MK, Edwards NC, Phillips AL. Relapses and disease-modifying drug treatment and live birth in US women with MS. Neurology 91, e1570–e1578 (2018).
32.
Bsteh G, Algrang L, Hegen H et al. Pregnancy and multiple sclerosis in the DMT era: a cohort study in Western Austria. Mult. Scler. J. 26, 79–68 (2020).
33.
Alroughani R, Akhtar S, Zeineddine M et al. Risk of relapses during pregnancy among multiple sclerosis patients. Mult. Scler. Relat. Disord. 34, 9–13 (2019).
34.
MacDonald SC, McElrath TF, Hernandez-Diaz S. Pregnancy outcomes in women with multiple sclerosis. Am. J. Epidemiol. 188, 57–66 (2019).
35.
Verdru P, Theys P, D'Hooghe MB, Carton H. Pregnancy and multiple sclerosis: the influence of long term disability. Clin. Neurol. Neurosurg. 96, 38–41 (1994).
36.
Vukusic S, Confavreux C. Pregnancy and multiple sclerosis: the children of PRIMS. Clin. Neurol. Neurosurg. 108, 266–279 (2006).
37.
Poser S, Poser W. Multiple sclerosis and gestation. Neurology 33, 1422–1427 (1983).
38.
Thompson DS, Nelson LM, Burns A, Burks JS, Franklin GM. The effects of pregnancy in multiple sclerosis: a retrospective study. Neurology 36, 1097–1099 (1986).
39.
Weinshenker BG, Hader W, Carriere W, Baskerville J, Ebers GC. The influence of pregnancy on disability from multiple sclerosis: a population-based study in Middlesex County, Ontario. Neurology 39, 1438–1440 (1989).
40.
Koch M, Uyttenboogaart M, Heersema D, Steen C, De Keyser J. Parity and secondary progression in multiple sclerosis. J. Neurol. Neurosurg. Psych. 80, 676–678 (2009).
41.
Ramagopalan S, Yee I, Byrnes J, Guimond C, Ebers G, Sadovnick D. Term pregnancies and the clinical characteristics of multiple sclerosis. A population based study. J. Neurol. Neurosurg. Psych. 83, 793–795 (2012).
42.
D'Hooghe MB, Haentjens J, Nagels G, D'Hooghe T, De Keyser J. Menarche, oral contraceptives, pregnancy, and progression of disability in relapsing onset and progressive onset multiple sclerosis. J. Neurol. 259, 855–861 (2012).
43.
Masera S, Cavalla P, Prosperini L et al. Parity is associated with a longer time to reach irreversible disability milestones in women with multiple sclerosis. Mult. Scler. J. 21, 1291–1297 (2015).
44.
Altintas A, Najar B, Gozubatik-Cellic G, Menku SF. Pregnancy data in a Turkish multiple sclerosis population. Eur. Neurol. 74, 296–302 (2015).
45.
D'Amico E, Leone C, Patti F. Offspring number does not influence reaching the disability milestones in multiple sclerosis: a seven-year follow-up study. Int. J. Mol. Sci. 17, 234 (2016).
46.
Dahl J, Myhr K, Dalveit AK, Hoff JM, Gilhus NE. Pregnancy, delivery, and birth outcome in women with multiple sclerosis. Neurology 65, 1961–1963 (2005).
47.
Chen YH, Lin HL, Lin HC. Does multiple sclerosis increase risk of adverse pregnancy outcomes: a population-based study. Mult. Scler. J. 15, 606–612 (2009).
48.
Hanulikova P, Vlk R, Meluzinova E et al. Pregnancy and multiple sclerosis-outcomes analysis. Ceska Gynekol. 78, 142–148 (2013).
49.
Goldacre A, Pakpoor J, Goldacre M. Perinatal characteristics and obstetric complications in mothers with multiple sclerosis. Mult. Scler. Relat. Disord. 12, 4–8 (2017).
50.
Houtchens MK, Edwards NC, Schneider G, Stern K, Phillips AL. Pregnancy rates and outcomes in women with and without MS in the United States. Neurology 91, e1559–e1569 (2018).
51.
Fong A, Chau CT, Quant C, Duffy J, Pan D, Ogunyemi DA. Multiple sclerosis in pregnancy: prevalence, sociodemographic features, and obstetrical outcomes. J. Matern. Fetal Neonatal Med. 31, 382–387 (2018).
52.
Mueller BA, Zhang J, Critchlow C. Birth outcomes and need for hospitalization after delivery among women with multiple sclerosis. Am. J. Obstetr. Gynecol. 186, 446–452 (2002).
53.
van der Kop ML, Pearce MS, Dahlgren L et al. Neonatal and delivery outcomes in women with multiple sclerosis. Ann. Neurol. 70, 41–50 (2011).
54.
Kelly VM, Nelson LM, Chakravarty E. Obstetric outcomes in women with multiple sclerosis and epilepsy. Neurology 73, 1831–1836 (2009).
55.
Balslev Andersen J, Iskov Kopp T, Sellebjerg F, Magyari. Pregnancy related and perinatal outcomes among Danish women with multiple sclerosis. A nationwide population-based registry study. Mult. Scler. J. 25, 619–620, Abstract 1081 (2019).
56.
Worthington J, Jones R, Crawford M, Forti A. Pregnancy and multiple sclerosis – a 3-year prospective study. J. Neurol. 241, 228–233 (1994).
57.
Jalkanen A, Alanen A, Airas L. Finnish multiple sclerosis and pregnancy study group. Mult. Scler. 16, 950–955 (2020).
58.
Flachenecker P, Hartung HP. Multiple sclerosis and pregnancy: overview and status of the European multicenter PRIMS study. Nervenarzt 66, 87–104 (1995).
59.
Lavie C, Rollot F, Durand-Dubief F et al. Neuraxial analgesia is not associated with an increased risk of post-partum relapses in MS. Mult. Scler. J. 25, 591–600 (2019).
60.
Laplaud DA, Leray E, Barriere P, Wiertlewski S, Moreau T. Increase in multiple sclerosis relapse rate following in vitro fertilization. Neurology 66, 1280–1281 (2006).
61.
Hellwig K, Beste C, Brune N et al. Increased MS relapse rate during assisted reproduction technique. J. Neurol. 255, 592–593 (2008).
62.
Michael L, Foucher Y, Vukusic S et al. Increased risk of multiple sclerosis relapse after in vitro fertilisation. J. Neurol. Neurosurg. Psych. 83, 796–802 (2012).
63.
Correale J, Farez MF, Ysrraelit MC. Increase in multiple sclerosis activity after assisted reproduction technology. Ann. Neurol. 72, 682–694 (2012).
64.
Bove R, Rankin K, Zhao C et al. Effect of assisted reproductive technology on multiple sclerosis relapses: case series and meta-analysis. Mult. Scler. J. 26, 1410–1419 (2010).
65.
Moberg JY, Laursen B, Thygesen LC, Magyari M. Reproductive history of the Danish multiple sclerosis population: a register-based study. Mult. Scler. J. 26, 902–911 (2020).
66.
Berenguer-Ruiz L, Gimenez-Martinez J, PalazonBru A, Sempere AP. Relapses and obstetric outcomes in women with multiple sclerosis planning pregnancy. J. Neurol. 266, 2512–2517 (2019).
67.
Portaccio E, Ghezzi A, Hakiki B et al. Postpartum relapses increase the risk of disability progression in multiple sclerosis: the role of disease-modifying drugs. J. Neurol. Neurosurg. 85, 845–850 (2014).
68.
Popova EV, Korobko DS, Bulatova EV et al. A retrospective analysis of the effect of pregnancy on the course of multiple sclerosis. Zh. Nevrol. Psikhiatr. Im. SS Korsakova 115, 18–21 (2015).
69.
Airas L. Hormonal and gender-related Immune changes in multiple sclerosis. Acta Neurol. Scand. 132, 62–70 (2015).
70.
Krysko KM, Rutatangwa A, Graves J, Lazar A, Waubant E. Association between breastfeeding and postpartum multiple sclerosis relapses: a systematic review and meta-analysis. JAMA Neurol. 77, 327–338 (2020).
71.
Portaccio E, Amato MP. Breastfeeding and postpartum relapses in multiple sclerosis patients. Mult. Scler. J. 25, 1211–1216 (2019).
72.
Langer-Gould A, Smith JB, Albers KB et al. Pregnancy-related relapses and breastfeeding in a contemporary multiple sclerosis cohort. Neurology 94, e1939–e1949 (2020).
73.
Xie Y, Tian Z, Han F, Liang S, Gao Y, Wu D. Factors associated with relapses in relapsing-remitting multiple sclerosis: a systematic review and meta-analysis. Medicine (Baltimore) 99, e20885 (2020).
Information & Authors
Information
Published In
Pages: 175 - 186
PubMed: 33565886
Copyright
© 2021 Future Medicine Ltd.
History
Received: 22 September 2020
Accepted: 30 November 2020
Published online: 10 February 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The effects of pregnancy on relapse rates, disability and peripartum outcomes in women with multiple sclerosis: a systematic review and meta-analysis. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0211
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Lorena Viviana López Reyes, Miguel Ángel Robles Sanchez, Montserrat Aroca Alsina, Mireia Resina Sallés, Laura Fonseca, Patricia Arrieta Perna, Cristina Calderer Suárez, Samuel Sánchez Pous, Gaizka Loyola Sanmillan, Paula Tagliani, Xavier Montalban, Mar Tintoré, Luciana Midaglia, How misinformation affects family planning choices for women with multiple sclerosis, Patient Education and Counseling, 10.1016/j.pec.2026.109632, 149, (109632), (2026).
- Ewa Krzystanek, Paweł Gęszka, Mateusz Gawin, Magdalena Fabian, Aleksandra Foryś, Anetta Lasek-Bal, The Knowledge About the Impact of Multiple Sclerosis on Pregnancy and Maternity Among Patients with Multiple Sclerosis, Journal of Clinical Medicine, 10.3390/jcm15124625, 15, 12, (4625), (2026).
- Zi-Jun Ma, Jun Chen, Chen-Xi Yang, Shun-Ping Lin, Quan Gong, Zachary Braunstein, Ying-Ying Wei, Xiao-Quan Rao, Ji-Xin Zhong, Immune microenvironment dynamics in pregnant patients with concomitant autoimmune diseases: mechanisms, challenges, and clinical significance, Military Medical Research, 10.1016/j.mmr.2026.100015, 13, 1, (100015), (2026).
- Virginie Trabaud, Appoline Zimmerman, Audrey Gnisci, Bertrand Audoin, Blandine Courbiere, Multiple sclerosis, fertility, pregnancy, and assisted reproductive technology: Current knowledge, Journal of Gynecology Obstetrics and Human Reproduction, 10.1016/j.jogoh.2025.103061, 55, 1, (103061), (2026).
- Sara Terrim, Samira Luisa Apostolos-Pereira, Thiago Ivan Vilchez Santillan, Tarso Adoni, Dagoberto Callegaro, Guilherme Diogo Silva, Risk Factors for Relapses in Multiple Sclerosis Beyond Disease-Modifying Therapy: An Umbrella Review of Systematic Reviews and Meta-Analyses, Sclerosis, 10.3390/sclerosis3040041, 3, 4, (41), (2025).
- Diego F. Wyszynski, Pregnancy and Multiple Sclerosis: A Narrative Review of Clinical Outcomes, Disease Activity, and Treatment Considerations, Multiple Sclerosis and Related Disorders, 10.1016/j.msard.2025.106643, 102, (106643), (2025).
- Manuela Andreea Ciapă, Vlad Constantin Donica, Claudia Florida Costea, Anisia Iuliana Alexa, Alexandra Lori Donica, Camelia Margareta Bogdănici, The Relationship Between OCT and VEP Parameters with Disability and Disease Duration in Relapsing–Remitting Multiple Sclerosis, Diagnostics, 10.3390/diagnostics15172181, 15, 17, (2181), (2025).
- Claire Z. Kalpakjian, Lukonde Mulenga, Shannen M. McIntosh, Jodi M. Kreschmer, Rebecca Parten, Heidi Haapala, Elizabeth S. Langen, Sara A. S. Rosenblum, Svati Pazhyanur, Susan Carlson, Maryam Berri, Susan D. Ernst, Pregnancy and physical disability: A scoping review, Women's Health, 10.1177/17455057251338424, 21, (2025).
- Salsabil Zubedi, Hana Al-Ali, Nadia Rabeh, Sara Aljoudi, Zakia Dimassi, Hamdan Hamdan, Life Chapters: Navigating Multiple Sclerosis Across Pregnancy, Breastfeeding, Epidemiology, and Beyond, Exploring the Effects of Diet on the Development and Prognosis of Multiple Sclerosis (MS), 10.1007/978-981-97-4673-6_2, (17-44), (2024).
- Shoboo Rahmati, Zahra Galavi, Batoul Kavyani, Homa Arshadi, Jaason Geerts, Hamid Sharifi, Maternal and neonatal outcomes in pregnant women with multiple sclerosis disease: A systematic review and meta-analysis, Midwifery, 10.1016/j.midw.2024.104004, 134, (104004), (2024).
- See more