Comparative effectiveness of trastuzumab emtansine versus lapatinib plus chemotherapy for HER2+ metastatic breast cancer
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To investigate the comparative effectiveness of trastuzumab emtansine (T-DM1) in a real-world population of HER2+ metastatic breast cancer (mBC) patients. Materials & methods: The Flatiron Health database was used to identify a cohort of HER2+ mBC patients who received first-line trastuzumab treatment and T-DM1 or lapatinib plus chemotherapy as second-line treatment. Overall survival was compared between the two groups. Results: A total of 278 patients with HER2+ mBC received second-line T-DM1 and 34 lapatinib plus chemotherapy. Overall survival was longer in patients treated with T-DM1 than those treated with lapatinib plus chemotherapy (adjusted hazard ratio: 0.56; 95% CI: 0.38–0.85). Conclusion: Real-world data supports the effectiveness of T-DM1 in the second-line treatment of HER2+ mBC patients.
Lay abstract
EMILIA was a randomized clinical trial (RCT) – a type of study designed to test whether a treatment works in a particular disease, using methods to remove possible bias. The study showed that a treatment called trastuzumab emtansine (shortened to T-DM1) improved the survival of patients with a particular type of breast cancer, known as HER2+ metastatic breast cancer (mBC). However, as clinical trials are run under controlled conditions, they do not fully reflect results under normal circumstances. In this study, we looked at the effect of treating a ‘real’ population of HER2+ mBC patients with T-DM1 in the USA. We found that T-DM1 still improved survival in these ‘real-world’ patients. Studies in the ‘real world’ can have some bias, as they are not controlled like RCTs; however, taking the results of the EMILIA RCT, along with the results of our study, supports the use of T-DM1 as a treatment option for HER2+ mBC patients.
Trastuzumab emtansine (T-DM1) is an antibody–drug conjugate that incorporates the HER2-targeted antitumor properties of trastuzumab with the cytotoxic activity of the microtubule-inhibitory agent DM1. The EMILIA Phase III trial, assessed the efficacy and safety of T-DM1, as compared with lapatinib plus chemotherapy, in patients with HER2-positive (HER2+) advanced breast cancer (BC) previously treated with trastuzumab and a taxane [1]. In the second interim analysis of the EMILIA trial, median overall survival (OS) was 30.9 months for T-DM1 as compared with 25.1 months for lapatinib plus chemotherapy; yielding a hazard ratio (HR) for death from any cause of 0.68 (95% CI: 0.55–0.85) [1].
The positive results from the EMILIA trial led to the regulatory approval and subsequent widespread use of T-DM1 in HER2+ metastatic BC (mBC). While final results from EMILIA have since confirmed the efficacy of T-DM1 over longer term follow-up [2], few studies have explored the realization of these benefits of T-DM1 in broader real-world populations. The aim of the current study was therefore to compare the real-world effectiveness of T-DM1 to lapatinib plus chemotherapy in second-line treatment of mBC using a longitudinal Electronic Health Record database compiling information from oncology practices in the US.
Materials & methods
Flatiron Health (FH) includes information from more than 265 cancer clinics across the US [3]. Data are deidentified thereby protecting patient confidentiality. Research with the database was approved by the Copernicus Group Institutional Review Board. For this study, data from 1 January 2011, through 31 July 2020, were included for patients with a confirmed diagnosis of mBC and documentation of a positive HER2 test result who were aged 18 or over at time of treatment initiation. Patients had to receive T-DM1 or lapatinib plus chemotherapy for second-line treatment of mBC, with the first line of therapy needing to be trastuzumab based. Patients had to have one or more clinic encounters occurring after initiation of second-line treatment.
Data on key baseline demographic and clinical characteristics were extracted from FH for the study population. Eastern Cooperative Oncology Group (ECOG) performance status assessments recorded following the start of first-line treatment and on or before the start of second-line treatment were used. Where there was more than one value, the maximum value was used. In defining a patient’s primary payer, the insurance payer that had a start date prior to and overlapping with the diagnosis of metastatic disease was used. If a patient had more than one payer that met the criteria, the following hierarchy was used to classify a patient: commercial health plan >Medicare >Medicaid >other government plan >patient assistance program >workers compensation >self pay. A patient was considered to have had a diagnosis of metastasis to a given site (bone, lung, liver, brain/central nervous system [CNS]) if the date of diagnosis (to a given site) occurred between the month of metastatic diagnosis and the month of second-line treatment initiation (inclusive). Each independent site of metastasis was used as a separate incident; therefore, a patient could have more than 1 site of metastasis. The number of metastatic sites was the sum of all incidences of metastatic sites identified. Visceral disease was defined as disease with lung, liver or brain metastases. The individual components of the Charlson comorbidity index with the exception of metastatic cancer, were extracted for each patient. A patient was considered to have a diagnosis of a given comorbidity if there was documentation of the diagnosis recorded at any time prior to initiation of second-line treatment, inclusive. First-line and second-line mBC treatments were identified using the derived line of treatment variables that are available in the FH dataset. These derived variables utilize an algorithm to define the timing and constituents of each line of treatment based on the raw treatment data available in the dataset. Time between first-line and second-line treatment initiation was calculated using the start dates of these treatment lines.
Baseline patient demographic and clinical characteristics were summarized using descriptive statistics. OS was defined as the time from initiation of second-line mBC treatment to death from any cause; otherwise, patients were censored at their last visit. The Kaplan–Meier method was used to evaluate median OS. To correct for potential covariate imbalances, all variables listed in Table 1 were considered for inclusion in a logistic regression model to estimate propensity scores. In line with best practice, we sought to construct a propensity score model which included all covariates that were associated with both the treatment and the outcome, or with the outcome only, while avoiding the inclusion of covariates associated with treatment only. As such, any covariate found to be significantly associated with the outcome in preliminary univariate Cox proportional hazard regression models at an alpha <0.1 were included in the propensity score model. Average Treatment effect on Treated (ATT) weights were estimated based on the propensity score and ATT weighted Cox proportional hazards models were used to determine the association of treatment choice with OS. To account for residual confounding not captured by the propensity score all variables were considered for inclusion in the ATT weighted multivariable Cox model, with those having an alpha <0.1 included in the final model.
| Variable name | Category/measure | Trastuzumab emtansine | Lapatinib plus chemo | p-value |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Age | Median (IQR†) | 60 (53–69) | 60 (54–66) | 0.64 |
| Gender | Female | 277 (99.64) | 34 (100) | 1 |
| Male | 1 (0.36) | 0 (0) | ||
| Ethnicity | White | 170 (61.15) | 21 (61.76) | 0.59 |
| Asian | 5 (1.8) | 2 (5.88) | ||
| Black or African American | 50 (17.99) | 6 (17.65) | ||
| Hispanic or Latino | 3 (1.08) | 0 (0) | ||
| Missing/others | 50 (17.99) | 5 (14.71) | ||
| ECOG‡ performance score | 0 | 63 (22.66) | 5 (14.71) | 0.73 |
| 1 | 89 (32.01) | 11 (32.35) | ||
| 2 | 50 (17.99) | 6 (17.65) | ||
| 3 | 14 (5.04) | 1 (2.94) | ||
| 4 | 2 (0.72) | 0 (0) | ||
| Missing | 60 (21.58) | 11 (32.35) | ||
| Hormone receptor status | ER+§ or PR+¶ | 161 (57.91) | 18 (52.94) | 0.63 |
| ER- and PR- | 116 (41.73) | 16 (47.06) | ||
| Unknown | 1 (0.36) | 0 (0) | ||
| Disease stage | I | 24 (8.63) | 2 (5.88) | 0.79 |
| II | 64 (23.02) | 6 (17.65) | ||
| III | 57 (20.5) | 6 (17.65) | ||
| IV | 117 (42.09) | 17 (50) | ||
| Not documented | 16 (5.76) | 3 (8.82) | ||
| Site of disease involvement | Visceral | 203 (73.02) | 31 (91.18) | 0.02 |
| Nonvisceral | 75 (26.98) | 3 (8.82) | ||
| Metastatic sites | Brain/CNS# | 62 (22.3) | 20 (58.82) | <0.0001 |
| Bone | 157 (56.47) | 21 (61.76) | 0.69 | |
| Liver | 113 (40.65) | 12 (35.29) | 0.68 | |
| Lung | 117 (42.09) | 17 (50) | 0.49 | |
| Number of metastatic sites | 1 | 82 (29.5) | 4 (11.76) | 0.07 |
| 2 | 76 (27.34) | 10 (29.41) | ||
| ≥3 | 120 (43.17) | 20 (58.82) | ||
| Median (IQR) | 2 (1–3) | 3 (2–4) | ||
| First-line treatment for mBC†† | Monotherapy: trastuzumab | 14 (5.04) | 1 (2.94) | 0.42 |
| Dual therapy: trastuzumab + taxane | 17 (6.12) | 2 (5.88) | ||
| Dual therapy: trastuzumab + targeted | 15 (5.4) | 5 (14.71) | ||
| Dual therapy: trastuzumab + other | 18 (6.47) | 4 (11.76) | ||
| Triple therapy: trastuzumab + taxane + targeted | 161 (57.91) | 16 (47.06) | ||
| Triple therapy: trastuzumab + taxane + other | 10 (3.6) | 0 (0) | ||
| Triple therapy: trastuzumab + targeted + other | 12 (4.32) | 1 (2.94) | ||
| Triple therapy: trastuzumab + other(s) | 1 (0.36) | 0 (0) | ||
| >Triple therapy | 30 (10.79) | 5 (14.71) | ||
| Time between first- and second-line treatment initiation (years) | Median (IQR) | 0.85 (0.44–1.49) | 1.05 (0.55–1.5) | 0.96 |
| Treatment initiation year | 2011 | 0 (0) | 1 (2.94) | <0.0001 |
| 2012 | 0 (0) | 3 (8.82) | ||
| 2013 | 10 (3.6) | 2 (5.88) | ||
| 2014 | 34 (12.23) | 4 (11.76) | ||
| 2015 | 40 (14.39) | 1 (2.94) | ||
| 2016 | 31 (11.15) | 2 (5.88) | ||
| 2017 | 42 (15.11) | 8 (23.53) | ||
| 2018 | 41 (14.75) | 6 (17.65) | ||
| 2019 | 67 (24.10) | 6 (17.65) | ||
| 2020 | 13 (4.68) | 1 (2.94) | ||
| Comorbidities from the Charlson comorbidity index | Myocardial infarction | 0 (0) | 0 (0) | N/A‡‡ |
| Congestive heart failure | 9 (3.24) | 1 (2.94) | 1 | |
| Peripheral vascular disease | 2 (0.72) | 0 (0) | 1 | |
| Cerebrovascular disease | 1 (0.36) | 1 (2.94) | 0.2 | |
| Dementia | 0 (0) | 0 (0) | N/A | |
| Chronic pulmonary disease | 9 (3.24) | 1 (2.94) | 1 | |
| Rheumatic disease | 3 (1.08) | 0 (0) | 1 | |
| Peptic ulcer disease | 1 (0.36) | 0 (0) | 1 | |
| Diabetes without chronic complication | 16 (5.76) | 2 (5.88) | 1 | |
| Diabetes with chronic complication | 0 (0) | 0 (0) | N/A | |
| Hemiplegia or paraplegia | 0 (0) | 0 (0) | N/A | |
| Renal disease | 9 (3.24) | 1 (2.94) | 1 | |
| AIDS/HIV | 0 (0) | 0 (0) | N/A | |
| Mild liver disease | 4 (1.44) | 2 (5.88) | 0.13 | |
| Moderate or severe liver disease | 0 (0) | 0 (0) | N/A | |
| Any comorbidity from the Charlson comorbidity index | Present | 44 (15.83) | 4 (11.76) | 0.8 |
| Not present | 234 (84.17) | 30 (88.24) | ||
| Payer category | Commercial health plan | 124 (44.6) | 19 (55.88) | 0.77 |
| Medicare | 29 (10.43) | 3 (8.82) | ||
| Medicaid | 8 (2.88) | 1 (2.94) | ||
| Other Government program | 4 (1.44) | 1 (2.94) | ||
| Patient assistance program | 8 (2.88) | 1 (2.94) | ||
| Other payer – type unknown | 34 (12.23) | 2 (5.88) | ||
| Self pay | 1 (0.36) | 0 (0) | ||
| Missing | 70 (25.18) | 7 (20.59) | ||
| Clinical practice | Academic | 14 (5.04) | 2 (5.88) | 0.69 |
| Community | 264 (94.96) | 32 (94.12) |
†
IQR.
‡
Eastern Cooperative Oncology Group.
§
Estrogen receptor.
¶
Progesterone receptor.
#
CNS.
††
Metastatic breast cancer.
‡‡
Not Applicable.
CNS: Central nervous system; IQR: Interquartile range.
Results
In total, 278 patients with HER2+ mBC received T-DM1 and 34 lapatinib plus chemotherapy. The majority of patients in the lapatinib plus chemotherapy arm received a capecitabine-based chemotherapy regimen (91.18%) with the remainder receiving vinorelbine or eribulin.
Patient characteristics are described in Table 1. In terms of their first-line treatment of mBC, the use of triple therapy with a taxane and targeted therapy alongside trastuzumab was more common in patients treated with T-DM1 (57.9%) than lapatinib plus chemotherapy (47.1%) and the use of trastuzumab monotherapy was more common in T-DM1 patients (5.0%) than lapatinib plus chemotherapy patients (2.9%). Despite this, the median time between initiation of 1L treatment and initiation of 2L treatment was greater for patients receiving lapatinib plus chemotherapy (1.05 years) than those receiving T-DM1 (0.85 years). Patients treated with lapatinib plus chemotherapy had a greater amount of visceral disease (91.2 vs 73.0% more brain metastases [58.8 vs 22.3%] and a greater number of metastatic sites (median 3 sites vs 2 sites) than T-DM1 patients.
Median follow-up was 28.4 months in the T-DM1 patients and 30.8 months in the lapatinib plus chemotherapy patients. The crude hazard of death was lower in the T-DM1 patients compared with the lapatinib plus chemotherapy patients (HR: 0.55; 95% CI: 0.36–0.85).
The following variables were found to be significantly associated with survival in univariate models and included in the logistic regression model used to estimate the propensity score: age at treatment initiation, metastatic sites (bone, brain/CNS), number of metastatic sites and time between first- and second-line treatment initiation (data not shown). Two patients were dropped from the study population in estimating the propensity score in order to improve population overlap leaving 310 patients for the adjusted analyses. Age and time between first- and second-line treatment had standardized mean differences after weighting of -0.183 and 0.274, respectively; all other variables had standardized mean differences <0.1. The final ATT weighted multivariable Cox model additionally adjusted for ECOG performance status at treatment initiation, metastatic site(s), number of metastatic sites, first-line treatment, insurance status and presence of a Charlson comorbidity. Results from this model were similar to the crude results, with the crude hazard of death lower in the T-DM1 patients compared with the lapatinib plus chemotherapy patients (HR: 0.56; 95% CI: 0.38–0.85; Table 2 & Figure 1).
| Hazard ratio (95% CI†) | ||
|---|---|---|
| Treatment | Lapatinib plus chemotherapy | Ref‡ |
| Trastuzumab emtansine | 0.56 (0.38–0.85) | |
| ECOG performance score | ≤2 | Ref |
| >2 | 1.44 (0.50–4.11) | |
| Missing | 2.06 (1.32–3.21) | |
| Metastatic site | Not present | Ref |
| Brain/CNS | 2.65 (1.50–4.66) | |
| Bone | 0.42 (0.27–0.66) | |
| Liver | 1.01 (0.65–1.55) | |
| Lung | 1.19 (0.77–1.82) | |
| Number of metastatic sites | 1 | Ref |
| 2 | 2.46 (1.29–4.69) | |
| ≥3 | 4.32 (2.01–9.31) | |
| First-line treatment for mBC | Triple therapy: trastuzumab + targeted + other | Ref |
| >Triple therapy | 6.22 (0.97–39.72) | |
| Dual therapy: trastuzumab + other | 5.27 (0.94–29.40) | |
| Dual therapy: trastuzumab + targeted | 3.23 (0.59–17.80) | |
| Dual therapy: trastuzumab + taxane | 7.15 (1.26–40.50) | |
| Monotherapy: trastuzumab | 2.17 (0.35–13.36) | |
| Trastuzumab + taxane + targeted/other | 3.31 (0.64–17.26) | |
| Any comorbidity from the Charlson comorbidity index | Not present | Ref |
| Present | 2.08 (1.19–3.63) | |
| Payer category | Missing | Ref |
| Commercial health plan | 1.89 (1.11–3.23) | |
| Medicaid | 0.31 (0.09–1.02) | |
| Medicare | 1.75 (0.78–3.93) | |
| Other Government program | 0.23 (0.06–0.87) | |
| Other payer – type unknown | 1.41 (0.74–2.68) | |
| Patient assistance program | 2.29 (0.88–6.00) |
†
CI.
‡
Reference.
CNS: Central nervous system; ECOG: Eastern Cooperative Oncology Group; mBC: Metastatic breast cancer.
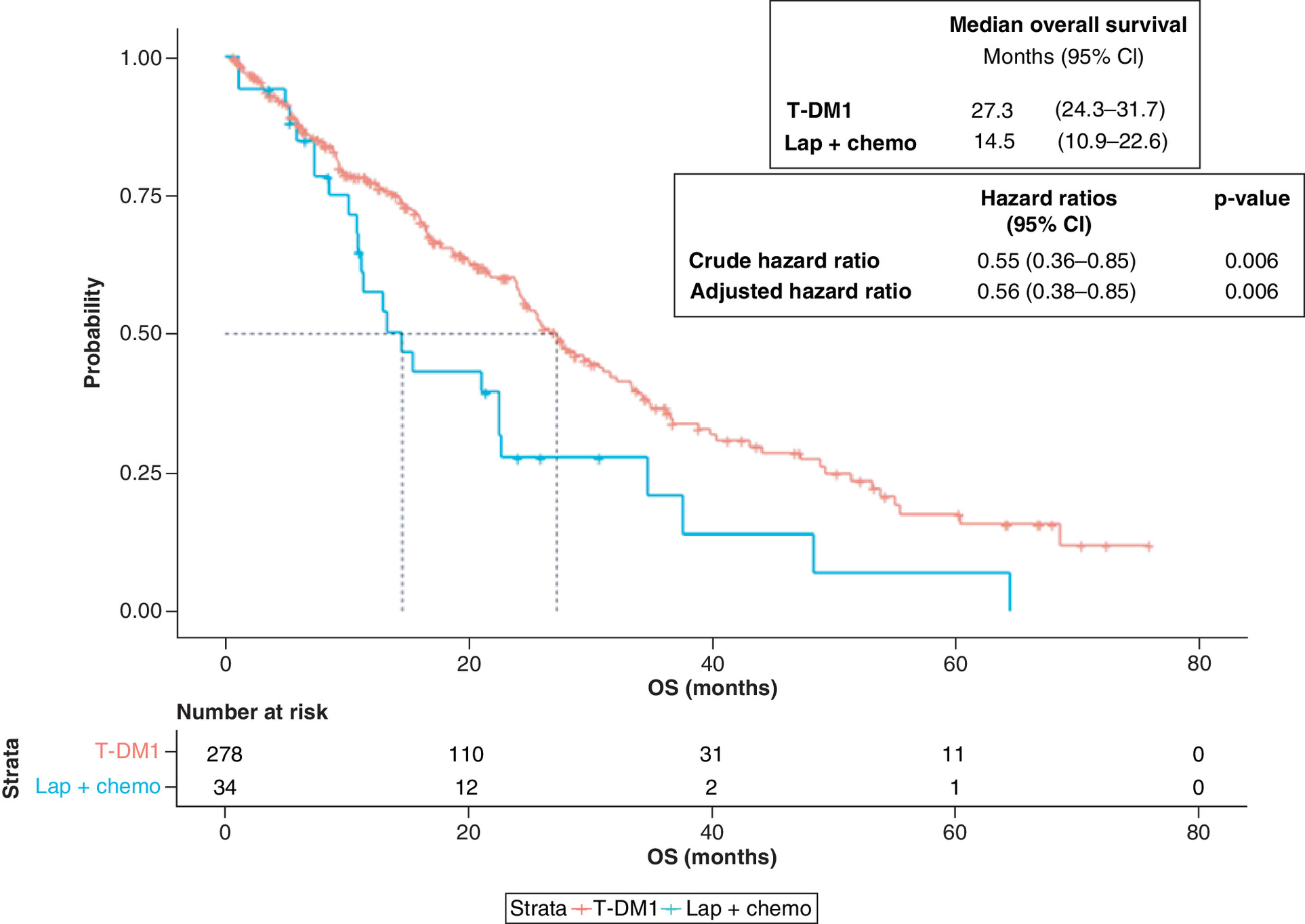
Figure 1. Kaplan–Meier estimates of overall survival for HER2+ metastatic breast cancer patients in Flatiron Health previously treated with trastuzumab.
Survival function estimates for patients receiving T-DM1 and patients receiving lapatinib plus chemotherapy are shown in red and blue, respectively.
OS: Overall survival; T-DM1: Trastuzumab emtansine.
Discussion
Overall survival in this real-world cohort of HER2+ mBC patients was significantly longer in patients treated with T-DM1 than in patients treated with lapatinib plus chemotherapy.
Direct comparison of the results presented here with those of the EMILIA trial are complicated by differences in the populations captured in each study. Individuals in the current FH study population were on an average slightly older than those in the EMILIA trial and the current study population included individuals with an ECOG greater than one where the EMILIA population did not. Another difference between the studies is that all patients in the EMILIA trial received a capecitabine-based chemotherapy regimen alongside lapatinib while only 91% of patients in the equivalent arm of our study received a capecitabine-based chemotherapy regimen. Despite these differences, our findings suggest a similar magnitude of relative benefit in those treated with T-DM1 to that reported for the EMILIA trial [1]. Notably, as the population captured in this study is broader than that in the EMILIA trial, the results go beyond those of the trial, supporting the comparative effectiveness of T-DM1 in a broader real-world population receiving a set of treatments reflective of those received in routine clinical practice.
Previous real-world studies of T-DM1 have reported absolute estimates of effectiveness in HER2+ mBC patients treated with T-DM1 and have provided comparisons of T-DM1 effectiveness between T-DM1 patients treated with different prior treatment regimens or with differing severity of disease [4–9], our study provides estimates of absolute effectiveness of T-DM1 in a larger cohort of second-line mBC patients than observed in any of these studies. Further, while these studies focused on absolute effectiveness, to our knowledge ours is the first to report on the real-world effectiveness of T-DM1 in second-line mBC relative to an alternative treatment option in this setting.
Limitations of the FH database and Electronic Health Records in general are well documented and include incomplete information on some variables such as comorbidities, metastases, performance status, date of death and adjuvant/neoadjuvant treatments [3,10]. As expected for a real-world study where treatments are not given at random, differences were observed in patient characteristics and prognostic factors between the two treatment groups. While we did our best to adjust for these in multivariable analyses, as with any nonrandomized study, the possibility of residual confounding must be considered in the interpretation of our results. Only statistical associations rather than causal relationships can therefore be concluded. Our analysis is also limited by the relatively small size of the lapatinib plus chemotherapy arm and the short median follow-up of the cohort. Our analysis should therefore be viewed as exploratory and not definitive, and further work is needed to confirm our findings. Despite these limitations, the results suggest the benefit of T-DM1 demonstrated in clinical trials is being realized in real-world populations, including populations not captured in these trials.
Conclusion
Real-world data supports the effectiveness of T-DM1 in the second-line treatment of HER2+ mBC patients previously treated with trastuzumab.
•
Positive results from the EMILIA trial have led to the widespread use of trastuzumab emtansine (T-DM1) in HER2+ metastatic breast cancer (mBC).
•
Despite this, few studies have explored the realization of these trial results in real-world populations.
•
The Flatiron Health database was used to identify a cohort of HER2+ mBC patients who received first-line trastuzumab treatment and T-DM1 or lapatinib plus chemotherapy as second-line treatment.
•
Overall survival was compared using Cox regression models adjusting for differences in patient characteristics.
•
278 patients with HER2+ mBC received second-line T-DM1 and 34 lapatinib plus chemotherapy.
•
Overall survival was longer in patients treated with T-DM1 than those treated with lapatinib plus chemotherapy (adjusted hazard ratio: 0.56; 95% CI: 0.38–0.85).
•
Real-world data supports the effectiveness of T-DM1 in the second-line treatment of HER2+ mBC patients.
Author contributions
SV Ramagopalan, J Ray and C Sammon were responsible for study conception and design; SV Ramagopalan, R Pisoni, A Zenin, J Ray, LS Rathore and C Sammon were responsible for data analysis, and drafting and revision of the manuscript.
Financial & competing interests disclosure
This study was funded by F Hoffman-La Roche. SV Ramagopalan, R Pisoni, LS Rathore and J Ray receives personal salary from F Hoffman-La Roche, A Zenin receives personal salary from Roche Moscow Ltd and C Sammon receives personal salary from PHMR. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors confirm that all the research meets the ethical guidelines, including adherence to the legal requirements of the study country.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: •• of considerable interest
1.
Verma S, Miles D, Gianni L et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N. Engl. J. Med. 367(19), 1783–1791 (2012).
2.
Diéras V, Miles D, Verma S et al. Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, Phase III trial. Lancet Oncol. 18(6), 732–742 (2017).
•• Final overall results of the EMILIA trial.
3.
Khozin S, Miksad RA, Adami J et al. Real-world progression, treatment, and survival outcomes during rapid adoption of immunotherapy for advanced non–small cell lung cancer. Cancer 125(22), 4019–4032 (2019).
4.
Conte B, Fabi A, Poggio F et al. T-DM1 efficacy in patients with HER2-positive metastatic breast cancer progressing after a taxane plus pertuzumab and trastuzumab: an Italian multicenter observational study. Clin. Breast Cancer 20(2), e181–e187 (2020).
5.
Vici P, Pizzuti L, Michelotti A et al. A retrospective multicentric observational study of trastuzumab emtansine in HER2 positive metastatic breast cancer: a real-world experience. Oncotarget 8(34), 56921–56931 (2017).
6.
Dzimitrowicz H, Berger M, Vargo C et al. T-DM1 activity in metastatic human epidermal growth factor receptor 2-positive breast cancers that received prior therapy with trastuzumab and pertuzumab. J. Clin. Oncol. 34(29), 3511–3517 (2016).
7.
Noda-Narita S, Shimomura A, Kawachi A et al. Comparison of the efficacy of trastuzumab emtansine between patients with metastatic human epidermal growth factor receptor 2-positive breast cancers previously treated with combination trastuzumab and pertuzumab and with trastuzumab only in Japanese population. Breast Cancer 26(4), 492–498 (2019).
8.
Gong IY, Yan AT, Earle CC, Trudeau ME, Eisen A, Chan KKW. Comparison of outcomes in a population-based cohort of metastatic breast cancer patients receiving anti-HER2 therapy with clinical trial outcomes. Breast Cancer Res. Treat. 181(1), 155–165 (2020).
9.
Lupichuk S, Cheung WY, Stewart D. Pertuzumab and trastuzumab emtansine for human epidermal growth factor receptor-2-positive metastatic breast cancer: contemporary population-based outcomes. Breast Cancer 13, (.2019) (Epub ahead of print).
10.
McDonald L, Schultze A, Carroll R, Ramagopalan SV. Performing studies using the UK Clinical Practice Research Datalink: to link or not to link? Eur. J. Epidemiol. 33(6), 601–605 (2018).
Information & Authors
Information
Published In
Pages: 595 - 602
PubMed: 33095031
Copyright
© 2021 Ramagopalan et al. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 15 September 2020
Accepted: 22 February 2021
Published online: 31 March 2021
Keywords:
Topics
Authors
Funding Information
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Comparative effectiveness of trastuzumab emtansine versus lapatinib plus chemotherapy for HER2+ metastatic breast cancer. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0201
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ippokratis Korantzis, Anna Koumarianou, Vassiliki Rapti, Eleni Timotheadou, Christos Christodoulou, Dimitrios Tryfonopoulos, Sofia Karageorgopoulou, Ioannis Boukovinas, Flora Zagouri, Adamantia Nikolaidi, Konstantinos Papazisis, Evangelia Razis, Vasileios Barbounis, Athina Christopoulou, Dimitrios Mavroudis, Vassilios Georgoulias, Georgios Kesisis, Emmanuel I. Papadopoulos, Rozalia Michalea, Alexandros Ardavanis, Real-world management strategies and clinical outcomes of metastatic HER2-positive breast cancer in Greece in the second-line setting and beyond (the togetHER study), BMC Cancer, 10.1186/s12885-025-14791-9, 25, 1, (2025).
- Ignacio Leiva-Escobar, Camilo Scherkl, Walter E Haefeli, Andreas D Meid, Transporting trial results to synthetic real-world populations in order to estimate real-world effectiveness of newly marketed medicines, BMJ Open, 10.1136/bmjopen-2024-089218, 15, 7, (e089218), (2025).
- H. Jourdain, I. Mansouri, A. Di Meglio, M. Zureik, N. Haddy, Utilization and safety of trastuzumab emtansine (T-DM1): a nationwide population-based study using the French National Health Data System, ESMO Real World Data and Digital Oncology, 10.1016/j.esmorw.2024.100045, 4, (100045), (2024).
- Karen Gambaro, Mélanie Groleau, Suzan McNamara, Arif Awan, Maged Salem, Mahmoud Abdelsalam, Eve St-Hilaire, François Vincent, Julie Carrier, Helen MacKay, Louise Provencher, Dominique Boudreau, Zineb Hamilou, Fred Saad, Cristiano Ferrario, Gerald Batist, Maud Marques, Third-line treatment patterns in HER2-positive metastatic breast cancer: a retrospective analysis of real-world data in Canada, Journal of Pharmacy & Pharmaceutical Sciences, 10.3389/jpps.2023.12078, 26, (2023).
- Sandhya Mehta, Jipan Xie, Raluca Ionescu-Ittu, Xiaoyu Nie, Winghan J. Kwong, Real-World Treatment Patterns and Outcomes Following First-Line Pertuzumab and Trastuzumab Among Patients with HER2+ Metastatic Breast Cancer, Oncology and Therapy, 10.1007/s40487-023-00241-8, 11, 4, (481-493), (2023).
- Carsten Bokemeyer, Noman Paracha, Ulrik Lassen, Antoine Italiano, Sean D. Sullivan, Marisca Marian, Nicoletta Brega, Jesus Garcia-Foncillas, Survival Outcomes of Patients With Tropomyosin Receptor Kinase Fusion-Positive Cancer Receiving Larotrectinib Versus Standard of Care: A Matching-Adjusted Indirect Comparison Using Real-World Data, JCO Precision Oncology, 10.1200/PO.22.00436, 7, (2023).
- Narmeen S. Rashid, Jacqueline M. Grible, Charles V. Clevenger, J. Chuck Harrell, Breast cancer liver metastasis: current and future treatment approaches, Clinical & Experimental Metastasis, 10.1007/s10585-021-10080-4, 38, 3, (263-277), (2021).