Is Medicaid expansion associated with increases in palliative treatments for metastatic cancer?
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: Medicaid expansion following the 2010 Affordable Care Act has an unknown impact on palliative treatments. Materials & methods: This registry-based study of individuals with metastatic cancer from 2010 to 2016 identified men and women with metastatic cancer in expansion and non-expansion states who received palliative treatments. A mixed effects logistic regression compared trends in expansion and non-expansion states and generated risk-adjusted probabilities or receiving palliative treatments each year. Results: Despite lower baseline use of palliative treatments, the rate of change was more rapid in expansion states (odds ratio [OR]: 1.02; 95% CI: 1.01–1.03; p < 0.001). The adjusted probability of receiving palliative treatments rose from 21.3 to 26.0% in non-expansion states, and from 19.7 to 26.9% in expansion states. Conclusion: Use of palliative treatments among metastatic cancer patients increased from 2010 to 2016 with a significantly greater increase in Medicaid expansion states, even when adjusting for demographic differences between states.
Lay abstract
Palliative treatments are a crucial tool for improving quality of life among those with advanced and incurable cancer. Increases in palliative treatments have been seen from 2010 to 2016 with a greater rate of increase in states which expanded Medicaid insurance coverage. Increases in insurance coverage in concert with policies to increase coverage of palliative and end of life care may increase access to palliative services.
The 2010 Patient Protection and Affordable Care Act (ACA) saw substantial political controversy. Some of this was related specifically to palliative care. Most notably, in 2009, several politicians and commentators wrongly claimed that the portions of the law which would have paid physicians for counseling Medicare beneficiaries about care options at the end of life would lead to government ‘panels’ that would decide whether or not to withdraw care [1].
Notwithstanding this opposition, the ACA was passed in 2010. It included both specific provisions to cover aspects of palliative care, such as end of life counseling and planning [2], as well as general provisions to improve healthcare access [3]. One key provision of the act was expansion of Medicaid, the federally funded and state-administered insurance program for low-income adults. The decision on whether (and when) to expand Medicaid was determined on a state-by-state basis and at different times for different states. A total of five states (Washington, California, New Jersey, Minnesota and Connecticut) and the District of Colombia expanded Medicaid ‘early’ - prior to 1 January 2014, and seven (New Hampshire, Indiana, Michigan, Pennsylvania, Alaska, Montana and Louisiana) expanded Medicaid ‘late’ that is between 1 January 2014 and the end of 2016. Another 19 expanded Medicaid on 1 January (Kentucky, Nevada, Colorado, Oregon, New Mexico, West Virginia, Arkansas, Rhode Island, Arizona, Maryland, Massachusetts, North Dakota, Iowa, Ohio, Illinois, Vermont, Hawaii, New York and Delaware). As of 31 December 2016, which is the final date from which the current study data were obtained, the remaining 19 had not expanded Medicaid (Virginia, Maine, Idaho, Utah, Nebraska, Oklahoma, Missouri, Wyoming, Wisconsin, South Dakota, Texas, Kansas, Tennessee, Mississippi, Alabama, Georgia, Florida, South Carolina and North Carolina). Of the 19 ‘non-expansion’ states in this study (defined based on the status in 2016), seven expanded Medicaid between 2017 and today. However, because of the study years of this analysis, these were categorized as non-expansion. These include Virginia (1 January 2019), Maine (1 October 2019), Idaho (1 January 2020), Utah (1 January 2020), Nebraska (10 January 2020), Oklahoma (planned 7 January 2021) and Missouri (planned 7 January 2021). The remaining 12 states (Wyoming, Wisconsin, South Dakota, Texas, Kansas, Tennessee, Mississippi, Alabama, Georgia, Florida, South Carolina and North Carolina) have not expanded Medicaid [4].
Policy changes of the ACA including initiatives to increase insurance coverage generally, expand Medicaid, and institute novel payment models are associated with a variety of aspects of cancer care from screening to treatment and outcomes [5–12]. The impact of Medicaid expansion on palliative treatments for cancer patients is less well studied. There is also substantial room for improvement. Despite the clear benefits of palliative care for patients with metastatic cancer [13–15], only a minority of patients with metastatic cancer receive palliative care, and there remains substantial variability in use [16].
In this setting, we examined trends in utilization of palliative treatments among adults with metastatic (stage IV) prostate, non-small-cell lung, colon and breast cancer. These are often incurable cancers and this is a category of patients which has been shown to benefit from palliative care [14]. We hypothesized that there would be an overall increase in the proportion of patients receiving palliative treatments from 2010 to 2016 and that the trends in adoption would differ based on the Medicaid expansion status of the state of diagnosis with greater rate of increase in Medicaid expansion states.
Materials & methods
The study was a retrospective cohort study of men and women diagnosed with metastatic cancer from 2010 to 2016 within a large US cancer registry. Data were extracted on adults with incident metastatic prostate, non-small-cell lung, colon and breast cancer within the National Cancer Database (NCDB), a hospital-based cancer registry covering approximately 70% of US adults diagnosed with cancer [17,18]. Adults 65 and older were excluded because at age 65, they become eligible for Medicare. Adults under 40 were also excluded because data on Medicaid expansion are not reported for this age range within the NCDB due to privacy concerns. The study period of 2010–2016 was chosen to encompass the time period of Medicaid expansion starting with the earliest state to expand Medicaid (CT, 2010).
The main independent variable was Medicaid expansion status of the state of diagnosis. Although the NCDB does not include the state of residency, it does include information about the Medicaid expansion status of the patient’s state of residency. Our dependent variable, receipt of palliative treatments, was defined using the NCDB-defined variable ‘Palliative Care’. Receipt of palliative treatments is determined by trained abstractors at participating institutions. The specific instructions for abstracting receipt of palliative treatments are included in the attached Supplementary Material 1. Patient level covariates included age at diagnosis, Charlson comorbidity index, race (Asian, Hispanic, Black, White non-Hispanic, other and unknown), cancer type (prostate, lung, colon and breast) and average income of the patient’s county of residence. The proportion of individuals in each study year who received palliative treatments was identified in expansion and non-expansion states.
A model-based approach was used to estimate the association between Medicaid expansion and the probability of receiving palliative treatments. A multilevel logistic regression model was used to test the association between Medicaid expansion status, year and receipt of palliative treatments. The model is shown in Supplementary Material 2. A facility-level random intercept was included to account for within- and between-facility variance and to account for unmeasured facility characteristics (e.g., presence of palliative care departments). Using a previously described approach [8,9,19], an interaction term between year and Medicaid expansion status was used to test whether the effect of time (per year change in odds of palliative treatments) differed between expansion and non-expansion states. Because the data include men and women with cancer who lived in states which expanded Medicaid on January 2014 and who were categorized as expanding Medicaid ‘early’ ranging from 2010 (CT) to 2016 (AK and MT) and because the state of residence is not available in the NCDB, we were not able to define a common pre-expansion/post-expansion variable for all patients in the study. A subgroup analysis was therefore, performed using only men and women who lived in states which expanded Medicaid on January 2014.
A logistic model was utilized because we were assessing a dichotomous outcome variable which was near to zero and we wanted to constrain predicted probabilities between 0 and 1. Using a linear model for this type of outcome can often yield a predicted possibility outside of the 0:1 range and we wanted to focus on predicted probabilities using a balanced covariate mix (to account for shifts in patient demographics in the category of expansion states as more states are added over the study period).
We then utilized the covariates from this model to generated risk-adjusted probabilities of receiving palliative treatments in expansion and non-expansion states in each study year. These were calculated using balanced covariate distribution for the entire study period to ensure that changes were not simply due to differences in demographic trends over time in expansion and non-expansion states (e.g., older patients being more common in Medicaid expansion states in later study years). Statistical analyses were performed with Stata version 14.0. (Stata Inc, TX, USA). The study received approval from the Brigham and Women’s Hospital IRB.
Results
There were 212,367 individuals with metastatic prostate, lung, colon and breast cancer diagnosed from 2010 to 2016. The unadjusted proportion of individuals who received palliative treatments was 24.8% (95% CI: 24.7–25.0%) for all states across the entire study period. The proportion of individuals in non-expansion states who received palliative care was 24.3% (95% CI: 22.67–26.0). The proportion of individuals in expansion states who received palliative care was 25.2% (95% CI: 23.8–26.5%). The difference was not significant (p = 0.43). The baseline characteristics of the two groups are shown in Table 1.
| Non-expansion n = 85118 (40.1) | Expansion n = 127249 (60.0) | p-value† | |
|---|---|---|---|
| Proportion receiving palliative treatments | 0.43 | ||
| 24.3% (95% CI: 22.7–26.0) | 25.2% (95% CI: 23.8–26.5) | ||
| Mean age | 0.06 | ||
| 56.1 (95% CI: 56.0–56.1) | 56.2 (95% CI: 56.2–56.2) | ||
| Age group | 0.13 | ||
| – 40–44 | 4097 (4.81) | 6128 (4.82) | |
| – 45–49 | 9029 (10.6) | 13,157 (10.3) | |
| – 50–54 | 17,246 (20.3) | 25,535 (20.1) | |
| – 55–59 | 25,155 (29.6) | 37,338 (29.3) | |
| – 60–64 | 29,591 (34.8) | 45,091 (35.4) | |
| Cancer type | 0.19 | ||
| – Prostate | 5463 (6.42) | 8521 (6.7) | |
| – Lung | 51,646 (60.7) | 76,746 (60.3) | |
| – Colorectal | 15,297 (18.0) | 22,314 (17.5) | |
| – Breast | 12,712 (14.9) | 19,668 (15.5) | |
| Race | <0.001 | ||
| – White | 59,070 (69.4) | 94,737 (74.5) | |
| – Black | 19,332 (22.7) | 18,818 (14.8) | |
| – Hispanic | 4236 (4.98) | 6084 (4.78) | |
| – Asian | 1356 (1.6) | 5422 (4.26) | |
| – Other | 753 (0.9) | 1115 (0.9) | |
| – Unknown | 371 (0.4) | 1073 (0.8) | |
| Year of diagnosis | 0.7242 | ||
| – 2010 | 11,385 (13.4) | 17,047 (13.4) | |
| – 2011 | 11,595 (13.6) | 17,397 (13.7) | |
| – 2012 | 12,062 (14.2) | 17,758 (14.0) | |
| – 2013 | 12,353 (14.5) | 18,749 (14.7) | |
| – 2014 | 12,572 (14.8) | 19,093 (15.0) | |
| – 2015 | 12,637 (14.9) | 18,829 (14.8) | |
| – 2016 | 12,514 (14.7) | 18,376 (14.4) | |
| Charlson comorbidity index | 0.001 | ||
| – 0 | 60,495 (71.1) | 93,442 (73.4) | |
| – 1 | 17,433 (20.5) | 23,935 (18.8) | |
| – 2 | 4717 (5.5) | 6454 (5.1) | |
| – 3 | 2473 (2.9) | 3418 (2.7) | |
| Family income† | <0.001 | ||
| – >US$63,000 | 15,200 (17.9) | 41,432 (32.6) | |
| – US$49,000–63,000 | 20,391 (24.0) | 34,823 (27.4) | |
| – US$38,000–48,999 | 24,197 (28.4) | 28,069 (22.1) | |
| – <US$38,000 | 25,083 (29.5) | 22,549 (17.7) | |
| – Unknown | 247 (0.3) | 376 (0.3) |
†
Chi squared test for categorical variables and F test for continuous variables. All clustered by facility with linearized standard errors.
The unadjusted proportion of patients receiving palliative care increased across the study period from 22.9% (95% CI: 21.7–24.2) in the initial study year to 26.1 (95% CI: 24.8–27.4) in the final year. In terms of expansion and non-expansion states, the unadjusted probabilities of receiving palliative care in the non-expansion and expansion states in the initial study year were 22.96 (95% CI: 21.1–24.9) and 22.89 (95% CI: 21.3–24.5), respectively. In the final year evaluated, the unadjusted probabilities of receiving palliative care in non-expansion and expansion states were 25.0% (95% CI: 23.0–27.0) and 26.9% (95% CI: 25.2–28.5), respectively. The unadjusted difference-in-differences (expansion versus non-expansion) across the entire study period was therefore, +1.97% (95% CI: 1.93–2.01).
The results of our adjusted model including patient level predictors of receiving palliative treatments are shown in Table 2. The odds of receiving palliative treatments increased by 4% each study year (OR: 1.04; 95% CI: 1.03–1.04; p < 0.001). While expansion states had overall lower adjusted odds of receiving palliative care (OR: 0.79; 95% CI: 0.69–0.91; p = 0.001), the interaction term combining year and Medicaid expansion status had a small magnitude but statistically significant positive association with receipt of palliative treatments (OR: 1.02; 95% CI: 1.01–1.03; p < 0.001), indicating a more rapid increase in use of palliative treatments in expansion states during the study period.
| Odds ratio (95% CI) | p-value | |
|---|---|---|
| Year of diagnosis | ||
| (per year) | 1.04 (1.03–1.04) | <0.001 |
| Age group | ||
| – 40–44 | Ref | |
| – 45–49 | 1.06 (0.99–1.07) | 0.08 |
| – 50–54 | 1.05 (1.00–1.12) | 0.07 |
| – 55–59 | 1.04 (0.98–1.10) | 0.18 |
| – 60–64 | 1.01 (0.96–1.07) | 0.74 |
| Race | ||
| – White | Ref | |
| – Black non-Hispanic | 1.04 (1.00–1.07) | 0.03 |
| – Hispanic | 0.99 (0.93–1.05) | 0.82 |
| – Asian | 1.02 (0.95–1.09) | 0.62 |
| – Other | 1.06 (0.95–1.20) | 0.29 |
| – Unknown | 0.78 (0.68–0.90) | 0.001 |
| Charlson comorbidity index | ||
| – 0 | Ref | |
| – 1 | 1.03 (1.00–1.06) | 0.05 |
| – 2 | 1.05 (1.00–1.10) | 0.05 |
| – ≥3 | 1.04 (0.98–1.11) | 0.23 |
| Mean family income in county of residence | ||
| – >US$63,000 | Ref | |
| – US$49,000–62,999 | 1.03 (1.00–1.07) | 0.06 |
| – US$38,000–47,999 | 0.99 (0.95–1.02) | 0.53 |
| – <US$38,000 | 1.03 (0.99–1.07) | 0.12 |
| – Unknown | 0.94 (0.77–1.16) | 0.58 |
| Medicaid expansion status | ||
| – Non-expansion | Ref | |
| – Expansion | 0.79 (0.69–0.91) | 0.001 |
| Medicaid expansion year† | ||
| 1.02 (1.01–1.03)‡ | Pinteraction < 0.001 | |
†
Estimated from American County Survey.
‡
Odds ratio corresponds to the difference in odds of palliative treatments per 1 year in the expansion group vs 1 year in the expansion group.
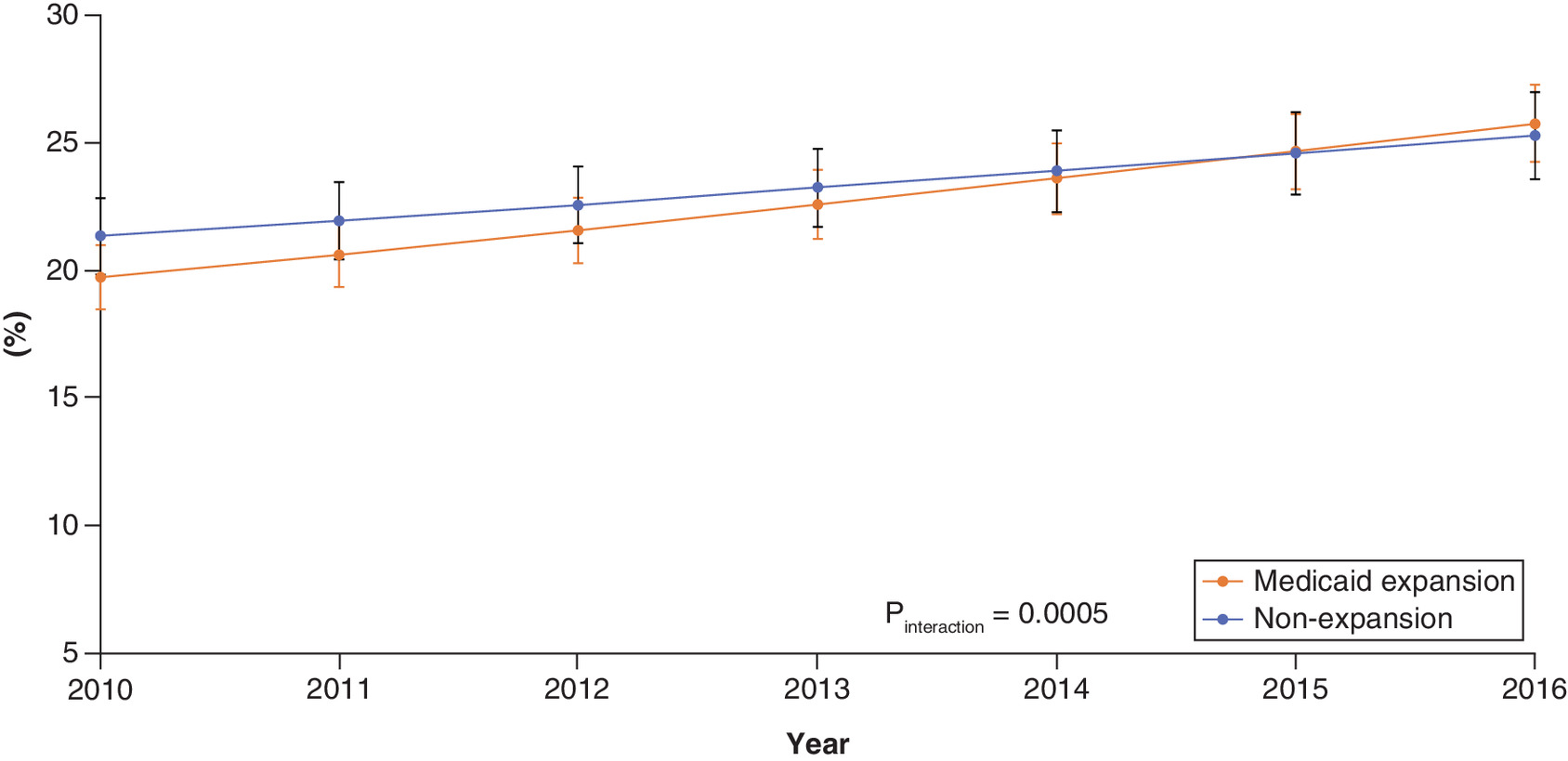
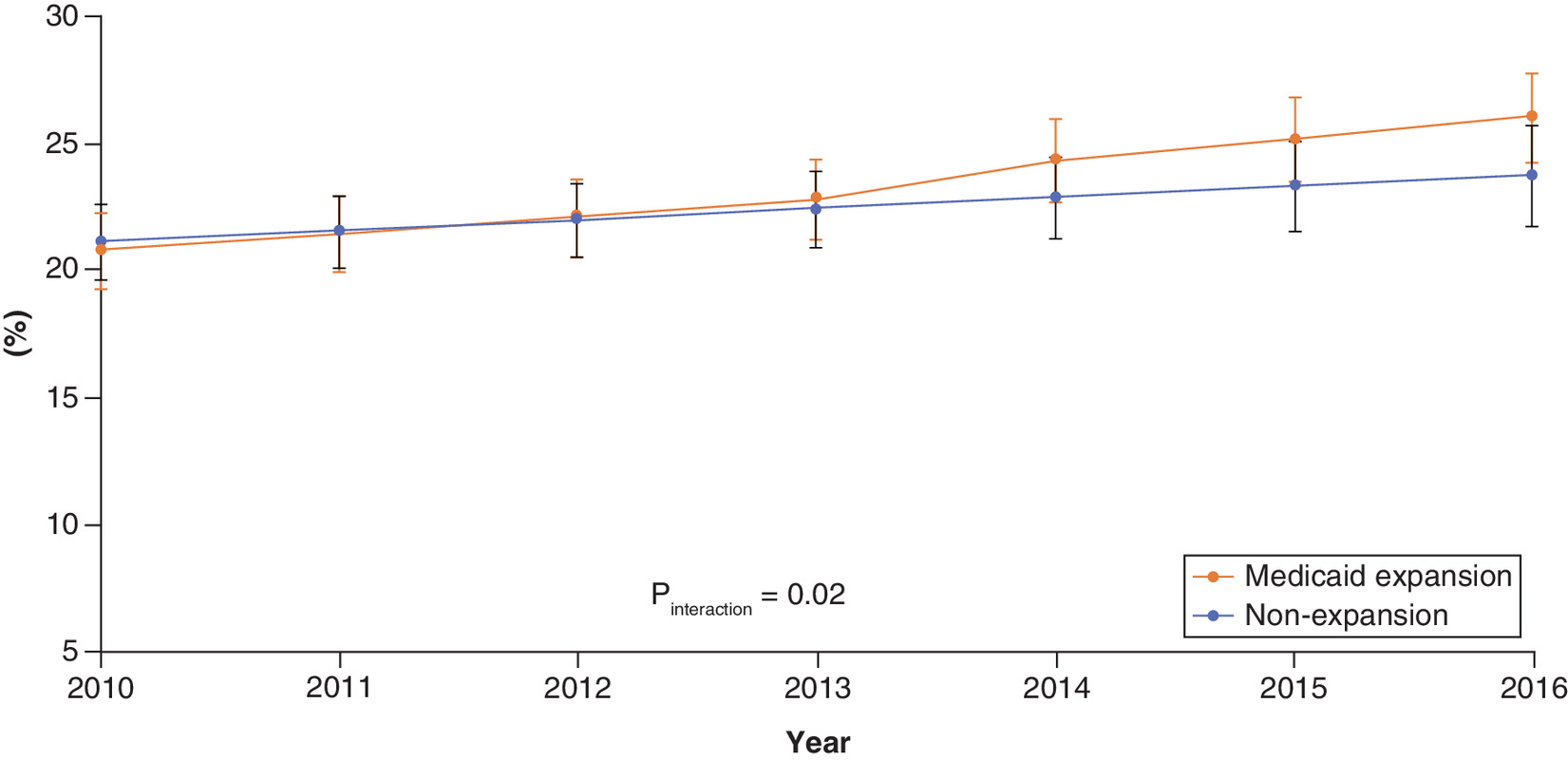
The predicted probabilities of receiving palliative treatments (using a balanced covariate mix to account for differences in state populations and differences over time) are shown in Figure 1. In non-expansion states, the predicted probability of receiving palliative treatments rose from 21.3% in 2010 to 26.0% in 2016. In Medicaid expansion states, the predicted probability of receiving palliative treatments rose from 19.7 to 26.9% over the same period (Figure 1). The results of our subgroup analysis including only states which expanded Medicaid on 1 January 2014 are shown in Figure 2. In this subgroup analysis, the interaction term between year and expansion status was again significant (OR: 1.01; 95% CI: 1.00–1.03; p = 0.03). Furthermore, the expansion and non-expansion states had similar trends pre-expansion.
Discussion
The study period from 2010 to 2016 saw an increase in palliative treatments among patients with metastatic cancer. Factors underlying this trend may include the policy changes to increase coverage of palliative treatments mandated by the ACA, popular coverage about the benefits of palliative treatments and landmark trials showing a benefit [2,14,20]. Despite starting with lower baseline utilization of palliative treatments, and having a lower odds of palliative care across the entire study period, Medicaid expansion states underwent a more rapid increase in palliative treatments during the period of medicaid expansion and eventually overtook non-expansion states.
While numerous studies have shown changes in cancer screening and treatment following the 2010 ACA, this is one of the first studies to specifically assess changes in palliative treatments. The main provisions of the Act focused on expanding insurance coverage generally. These resulted in decreases in the proportion of uninsured patients. In addition, there were certain ACA provisions which specifically strengthen hospice and palliative care reimbursements (e.g., Section 3132: Market basket cuts and productivity adjustments for hospice, Hospice payment reform) and for Medicaid expansion (e.g., Section 3202: Concurrent [curative and palliative] care for children in Medicaid and CHIP; October 2013). Taking into account the inherent limitations of this type of ecological research, our finding of a significantly greater rise in expansion states suggests that increases in insurance coverage (via Medicaid expansion) in concert with policies to ensure insurance coverage for end-of-life care may be associated with significantly greater increases in palliative treatments among those with advanced cancer.
Interestingly, there was lower baseline of use palliative treatments among the expansion states. Although the proportion of patients receiving palliative treatments in expansion states rose more rapidly than in non-expansion states, this change was not rapid enough to overcome the lower baseline use of palliative care; thus adjusted odds of palliative care in expansion states remained below that of non-expansion states for the study period viewed in toto. This finding is puzzling given that expansion states tend to be wealthier, and have a greater proportion of high income, educated and nonminority patients – all of which are factors associated with increased palliative care utilization [21]. One possible explanation is the that higher-income, nonminority patients are more likely to receive end of life care in nonhospital settings [22]. Because NCDB utilizes data from hospital systems, changes in use palliative treatments provided by hospital systems (e.g., hospital palliative care departments) would be captured but certain types of home hospice would not. If high resource patients in expansion states are more likely to die at home, then this could account for the apparent lower use of palliative care in the former group. Alternatively, it may be the case that high resource patients who receive care for metastatic cancer in hospital systems are preferentially seeking out aggressive therapies with curative intent. Both of these factors should be nonselective with respect to our main study findings, and would generally not relate to the patients most impacted by Medicaid expansion and studied in this project (e.g., low income Medicaid beneficiaries treated for advanced cancer within hospital systems).
The main limitation of this study relates to the determination of palliative treatments. Within the NCDB, data abstractors determine whether patients received ‘palliative care’ based on chart review (Supplementary Material 1). This may be less stringent that the definition in the major palliative care trials which define this using subspecialty-trained palliative care providers only. While NCDB data are abstracted from participating Commission on Cancer institutions which include both inpatient and outpatient services (e.g., clinics associated with accredited cancer centers) some standalone palliative care clinics may be under-counted. Another limitation is the potential for confounding from hospital-level characteristics (e.g., differences in charting or presence of palliative care departments) and differences in baseline demographics of each state. The use of a facility-level random intercept should reduce (but does not fully eliminate) bias due to facility characteristics and our use of a balanced covariate mix to generate our predicted probabilities will account for demographic differences.
Another limitation of the NCDB includes lack of the state of residence. Thus, it is not possible to define exact pre-expansion/post-expansion variables for those patients who were not in states that expanded Medicaid 1 January 2014. Rather than limiting our analysis to this subset, we included early and late expansion states. This is a strength compared with many studies which did not include the post-2014 expansion states [10,23,24], but limits our ability for certain types of statistical analysis (e.g., comparison of pre-expansion/post-expansion trends due to lack of a common pre-expansion period). Instead, we included all expansion states with a multilevel model-based approach (with a facility random intercept) to balance covariates across expansion and non-expansion groups and study years and account for confounding by facility characteristics. We did perform a subgroup analysis using only the 2014 expansion states which suggests similar pre-expansion trends, but of course these results cannot be extrapolated to the larger population of early and late expansion states.
Finally, there may be underlying trends in the expansion and non-expansion states, beyond Medicaid expansion itself which may account for this trend. For example, there may be a tendency for older patients to move to expansion states in later study years. We attempted to control for this in part by using a balanced covariate mix (holding all covariates at population mean) to generate the adjusted probabilities (to simulate equivalent patient demographics based on measured covariates), however, there may be unmeasured variables which differ between expansion and non-expansion states.
Conclusion
Although, the effect of Medicaid expansion on cancer care has been previously investigated in other areas of cancer, the impact of this policy on palliative treatments is unknown. This study showed an overall increase in palliative treatments in the years in which Medicaid was expanded. Despite lower baseline use of palliative care, states that expanded Medicaid saw a significantly more rapid increase in use of palliative treatments compared with those states which did not.
•
Medicaid expansion following the 2010 Affordable Care Act has an unknown impact on palliative treatments for cancer patients.
•
This registry-based study of men and women with metastatic cancer from 2010 to 2016 identified the proportion of men and women with metastatic cancer in expansion and non-expansion states who received palliative treatments in each study year.
•
Medicaid expansion states had lower baseline use of palliative treatments. Despite this, the per year rate of increase in palliative treatments for metastatic cancer patients was significantly greater in states which expanded Medicaid yielding a differential rate of change of 1.97% (95% CI: 1.93–2.01).
•
In our adjusted model, the rate of change was significantly greater in expansion states (OR per year 1.02; 95% CI: 1.01–1.03; p < 0.001).
•
In non-expansion states, the adjusted probability of receiving palliative treatments rose from 21.3% in 2010 to 26.0% in 2016. In Medicaid expansion states, the predicted probability of receiving palliative treatments rose from 19.7 to 26.9% over the same period.
•
In concert with policies to ensure coverage for palliative care, initiatives to increase insurance coverage among low-income adults may result in increased utilization of palliative treatments.
Financial & competing interests disclosure
QD Trinh supported by the Brigham Research Institute Fund to Sustain Research Excellence, the Beal Surgical Fellowship, the Genentech Bio-Oncology Career Development Award from the Conquer Cancer Foundation of the American Society of Clinical Oncology, a Health Services Research pilot test grant from the Defense Health Agency, the Clay Hamlin Young Investigator Award from the Prostate Cancer Foundation. BA Mahal is supported by the Prostate Cancer Foundation, ASTRO, Department of Defense, National Institutes of Health and the Sylvester Comprehensive Cancer Center. QD Trinh reports honoraria from Bayer and Astellas, research funding from Intuitive Surgical. AS Kibel reports honoraria from Janssen, Bayer, Bristle-Meyers Squib – DSMB AstraZeneca, General Electric, Merck, Profound, Insightec, Advantagene – DSMB. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Supplementary Material
File (suppl_file.docx)
- Download
- 19.84 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Frankford DM. The remarkable staying power of “Death Panels”. J. Health Polit. Policy Law 40(5), 1087–1101 (2015).
2.
Meier DE. Increased access to palliative care and hospice services: opportunities to improve value in health care. Milbank Q. 89(3), 343–380 (2011).
3.
Obama B. United States health care reform: progress to date and next steps. JAMA 316(5), 525–532 (2016).
4.
Foundation, Kaiser Family. Status of State Action on the Medicaid Expansion Decision (2020). www.kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act/
5.
Sun M, Cole AP, Lipsitz SL, Trinh QD. Trends in breast, colorectal, and cervical cancer incidence following the Affordable Care Act: implications for cancer screening. JAMA Oncol. 4(1), 128–129 (2018).
• Shows that the incidence of early-stage breast and colorectal cancer increased after the adoption of the Affordable Care Act which removed cost sharing for certain screening services. It did not vary for late-stage cancer. Although screening itself was not assessed, the trend is consistent with increases in colorectal and breast cancer screening following the Affordable Care Act.
6.
Sammon JD, Serrell EC, Karabon P et al. Prostate cancer screening in early Medicaid expansion states. J. Urol. 199(1), 81–88 (2018).
7.
Cole AP, Krasnova A, Ramaswamy A et al. Recommended cancer screening in accountable care organizations: trends in colonoscopy and mammography in the Medicare Shared Savings Program. J. Oncol. Pract. 15(6), e547–e559 (2019).
8.
Mahal AR, Chavez J, Yang DD et al. Early impact of the Affordable Care Act and Medicaid expansion on racial and socioeconomic disparities in cancer care. Am. J. Clin. Oncol. 43(3), 163–167 (2020).
9.
Zerhouni YA, Trinh QD, Lipsitz S et al. Effect of Medicaid expansion on colorectal cancer screening rates. Dis. Colon Rectum 62(1), 97–103 (2019).
• Reveals more rapid increase in colorectal cancer screening among low income and black individuals in early Medicaid expansion states.
10.
Liu Y, Colditz GA, Kozower BD et al. Association of Medicaid expansion under the Patient Protection and Affordable Care Act with non-small cell lung cancer survival. JAMA Oncol. 6(8), 1289–1290 (2020).
11.
Hoehn RS, Rieser CJ, Phelos H et al. Association between Medicaid expansion and diagnosis and management of colon cancer. J. Am. Coll. Surg. 232(2), 146–156; e141 (2021).
12.
Cole AP, Lu C, Krimphove MJ et al. Comparing the association between insurance and mortality in ovarian, pancreatic, lung, colorectal, prostate, and breast cancers. J. Natl Compr. Canc. Netw. 17(9), 1049–1058 (2019).
13.
Morrison RS, Dietrich J, Ladwig S et al. Palliative care consultation teams cut hospital costs for Medicaid beneficiaries. Health Affairs 30(3), 454–463 (2011).
14.
Temel JS, Greer JA, Muzikansky A et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 363(8), 733–742 (2010).
•• This landmark study reveals improved quality of life and prolonged overall survival despite less intensive care among metastatic lung cancer patients who received specialist palliative care.
15.
Kavalieratos D, Corbelli J, Zhang D et al. Association between palliative care and patient and caregiver outcomes: a systematic review and meta-analysis. JAMA 316(20), 2104–2114 (2016).
16.
Cole AP, Nguyen DD, Meirkhanov A et al. Association of care at minority-serving vs non-minority-serving hospitals with use of palliative care among racial/ethnic minorities with metastatic cancer in the United States. JAMA Netw. Open 2(2), e187633 (2019).
• Utilizes the National Cancer Database to show that hospital utilization of palliative care varied substantially between hospitals. Black patients were less likely to receive palliative care overall, however, this effect was mediated by the hospital where care was provided.
17.
Bilimoria KY, Stewart AK, Winchester DP, Ko CY. The National Cancer Data Base: a powerful initiative to improve cancer care in the United States. Ann. Surg. Oncol. 15(3), 683–690 (2008).
18.
Cole AP, Friedlander DF, Trinh QD. Secondary data sources for health services research in urologic oncology. Urol. Oncol. 36(4), 165–173 (2018).
19.
Akande M, Minneci PC, Deans KJ, Xiang H, Cooper JN. Association of Medicaid expansion under the Affordable Care Act with outcomes and access to rehabilitation in young adult trauma patients. JAMA Surg. 153(8), e181630 (2018).
20.
Gawande AA. Letting go: what should medicine do when it can't save your life? The New Yorker (2010). www.newyorker.com/magazine/2010/08/02/letting-go-2
21.
Johnson KS. Racial and ethnic disparities in palliative care. J. Palliat. Med. 16(11), 1329–1334 (2013).
22.
Ornstein KA, Roth DL, Huang J et al. Evaluation of racial disparities in hospice use and end-of-life treatment intensity in the REGARDS Cohort. JAMA Netw. Open 3(8), e2014639 (2020).
23.
Mcclintock TR, Gondi S, Wang Y et al. Association of Affordable Care Act-related Medicaid expansion with variation in utilization of surgical services. Am. J. Surg. 220(2), 441–447 (2020).
• Compares utilization of a broad array of surgical procedures among nonelderly adults within a group of state level hospital databases. There was a small but significant increase in utilization of surgical care in Medicaid Expansion states.
24.
Swaminathan S, Sommers BD, Thorsness R, Mehrotra R, Lee Y, Trivedi AN. Association of Medicaid Expansion with 1-year mortality among patients with end-stage renal disease. JAMA 320(21), 2242–2250 (2018).
Information & Authors
Information
Published In
Pages: 733 - 741
PubMed: 33880936
Copyright
© 2021 Future Medicine Ltd.
History
Received: 16 August 2020
Accepted: 26 March 2021
Published online: 21 April 2021
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Is Medicaid expansion associated with increases in palliative treatments for metastatic cancer?. (2021) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0178
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Oluwasegun Akinyemi, Mojisola Fasokun, Akachukwu Eze, Nkemdirim Ugochukwu, Sumaiyya Arshad, Orimisan Belie, Kakra Hughes, Edward Cornwell III, Gal Levy, Association of medicaid expansion with lung cancer–specific and overall mortality: A difference-in-differences analysis, PLOS One, 10.1371/journal.pone.0332292, 21, 4, (e0332292), (2026).
- Rebecca S. Arch, Enver Ozer, Amit Agrawal, Catherine T. Haring, Stephen Y. Kang, Nolan B. Seim, Matthew O. Old, James W. Rocco, Lauren E. Miller, Medicaid Expansion Status and Receipt of Palliative Care in Stage IV Oral Cavity Cancer, OTO Open, 10.1002/oto2.70184, 9, 4, (2025).
- Henrique A. Lima, Parit Mavani, Muhammad Musaab Munir, Yutaka Endo, Selamawit Woldesenbet, Muhammad Muntazir Mehdi Khan, Karol Rawicz-Pruszyński, Usama Waqar, Erryk Katayama, Vivian Resende, Mujtaba Khalil, Timothy M. Pawlik, Medicaid expansion and palliative care for advanced-stage liver cancer, Journal of Gastrointestinal Surgery, 10.1016/j.gassur.2024.01.042, 28, 4, (434-441), (2024).
- Xuesong Han, Kewei Sylvia Shi, Jingxuan Zhao, Leticia Nogueira, Ravi B. Parikh, Arif H. Kamal, Ahmedin Jemal, K. Robin Yabroff, Medicaid Expansion Associated With Increase In Palliative Care For People With Advanced-Stage Cancers, Health Affairs, 10.1377/hlthaff.2023.00035, 42, 7, (956-965), (2023).
- Karishma Khullar, Jesse J Plascak, Muhammad Hamza Habib, Samantha Nagengast, Rahul R Parikh, Extensive stage small cell lung cancer (ES-SCLC) and palliative care disparities: a national cancer database study, BMJ Supportive & Palliative Care, 10.1136/spcare-2022-004038, 14, e3, (e2694-e2699), (2022).
- Hamza Khan, Deepa Cherla, Krista Mehari, Manish Tripathi, Thomas W. Butler, Errol D. Crook, Martin J. Heslin, Fabian M. Johnston, Annabelle L. Fonseca, Palliative Therapies in Metastatic Pancreatic Cancer: Does Medicaid Expansion Make a Difference?, Annals of Surgical Oncology, 10.1245/s10434-022-12563-4, 30, 1, (179-188), (2022).