Impact of chronic obstructive pulmonary disease on mortality in community acquired pneumonia: a meta-analysis
Publication: Journal of Comparative Effectiveness Research
Abstract
Background: The aim of the present study was to systematically review the exiting literature and to proceed a meta-analysis to determine the impact of chronic obstructive pulmonary disease (COPD) on mortality in patients with community acquired pneumonia. Materials & methods: Eligible studies were searched from PubMed, Cochrane Library and EMBASE. Odds ratios (ORs) with 95% CIs were used as effect estimates. Results: Twenty cohort studies were included. Analysis of unadjusted data revealed nonsignificant short- and long-term mortality associated with COPD. Analysis of adjusted 30-days mortality showed similarly no association between COPD and increased 30-days mortality (OR: 1.06, [0.68, 1.44]) but a positive association when COPD was confirmed spirometrically (OR: 1.84, [1.06, 2.62]). Conclusion: There is still no evidence to clear the impact of COPD on mortality in patients with community acquired pneumonia. More prospective studies with spirometrically-defined COPD and adequate adjustment for confounders are needed.
Currently, community acquired pneumonia (CAP) is one of the most common infectious diseases that contributes to substantial health and economic burden in the world [1]. In the general adult population, CAP affects about 2 to 13 cases per 1000 persons each year and remains a major cause of hospitalization and mortality, with a hospitalization rate of 22–51% and a mortality rate of 3–24% [2,3]. Chronic obstructive pulmonary disease (COPD) is featured by long-term worsening airflow, resulting in shortness of breath, cough and sputum production. COPD is one of the most common comorbidities and risk factors in patients with CAP, which is ranked as the third leading cause of death worldwide [4–6].
There are many studies analyzing whether the coexistence of COPD and CAP may cause an increased mortality rate, but to date their findings are still inconsistent and controversial. Some studies concluded that the presence of COPD as a comorbid condition was associated with increased mortality, whereas some other studies held the view that no significant link exists between presence or absence of COPD and mortality rate [7–11]. Two meta-analysis combining 13 and 11 studies, respectively demonstrated that evidence on associated mortality risk with concomitant CAP and COPD is underpowered and heterogeneous, and that additional information is needed [12,13].
Therefore, the aim of the present study was to systematically review the exiting literature and to proceed a meta-analysis to determine the impact of COPD on mortality in patients with CAP, focusing on the difference in mortality rate between COPD and non-COPD patients and whether COPD is a risk factor for mortality in CAP.
Materials & methods
This study was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement [14].
Literature search
Eligible papers were identified through computerized searching of the databases PubMed, Cochrane Library and EMBASE using the terms ‘community acquired pneumonia’ and ‘chronic obstructive pulmonary disease’, or their abbreviations, limited to English language papers until March 2020. Two independent reviewers identified possibly related studies based on titles and abstracts, and subsequently screened the articles by reading full texts to complete the literature search. In the event of any disagreement, a third reviewer was involved.
Inclusion & exclusion criteria
To minimize the influence of variation in study design, we only included cohort studies for this meta-analysis. Cohort studies were included, if they reported the mortality in COPD and non-COPD patients with CAP or addressed COPD as a factor associated with mortality in CAP in univariate or multivariate analysis; the included patients were hospitalized for CAP as primary diagnosis established by medical records or radiographic confirmation. Except for original studies, other publications such as reviews, letters, case reports or conference abstracts were excluded. If there were two studies or more enrolled overlapping participants, the one with the most sufficient data were included.
Data collection
Two reviewers independently extracted data from included papers into a predefined data collection form. The following data were collected: the name of first author, year of publication, region, study design (prospective or retrospective), subjects inclusion and exclusion criteria, type of patients source (inpatients or intensive care unit [ICU] patients), year of entry for patients, patient characteristics (sample size, age and gender) and definition of CAP and COPD. The outcomes were in-hospital, 30-days, 90-days and long-term mortality (long-term mortality was defined as death in the follow-up duration of ≥1 year). Both raw unadjusted and adjusted data on mortality in COPD versus non-COPD patients were extracted. For the study of Braeken et al. [15] reporting the results of hospitalized and outpatient cohorts, we only extracted the data on hospitalized patients. Discrepancies were resolved by consultation with a third reviewer.
Quality assessment
The critical appraisal of included studies were conducted using the Newcastle-Ottawa Scale [16]. The Newcastle-Ottawa Scale specific for cohort design consists of three domains (selection of the study groups, comparability of the groups and ascertainment of either the exposure or outcome of interest). Two authors performed the quality assessment independently, and discrepancies were resolved by discussion with a third author.
Statistical analysis
For dichotomous data, odds ratios (OR) with 95% CI were used as effect estimates. CIs are used for statistical test, with a 95% CI excluding the point of no effect indicating statistical significance. Statistical heterogeneity across studies was assessed using I2 test, with I2 >50% indicating significant heterogeneity. In data synthesis, pooled results were calculated by using a random-effects model based on Mantel–Haenszel method in the case of significant heterogeneity, while a fixed-effects model was used when no significant heterogeneity was found. Unadjusted and multivariate adjusted data were pooled and analyzed separately. For primary outcomes, subgroup analysis was performed based on study design (prospective vs retrospective), study quality (studies that met the comparability criteria vs those that did not) and sample size (>1000 vs <1000); we also performed sensitivity analysis by sequentially dropping one study at a time to determine whether removal of any one study would substantially change the effect size and the heterogeneity, and by restricting the meta-analysis to studies with spirometric definition of COPD. Begg’s and Egger’s test were performed to test publication bias, if ten studies or more were included in the meta-analysis, using a p-value < 0.05 as the threshold to indicate significant risk of publication bias [17]. We used Stata software version 15.0 (Stata Corporation, College Station, TX, USA) to proceed our data analysis.
Results
Study identification
The systematic search yielded 3097 papers, resulting in 101 potentially eligible studies. After reviewing the full text of these relevant articles, a total of 20 studies met the inclusion criteria and provided data to the meta-analysis. The search process and study identification are shown in Figure 1.
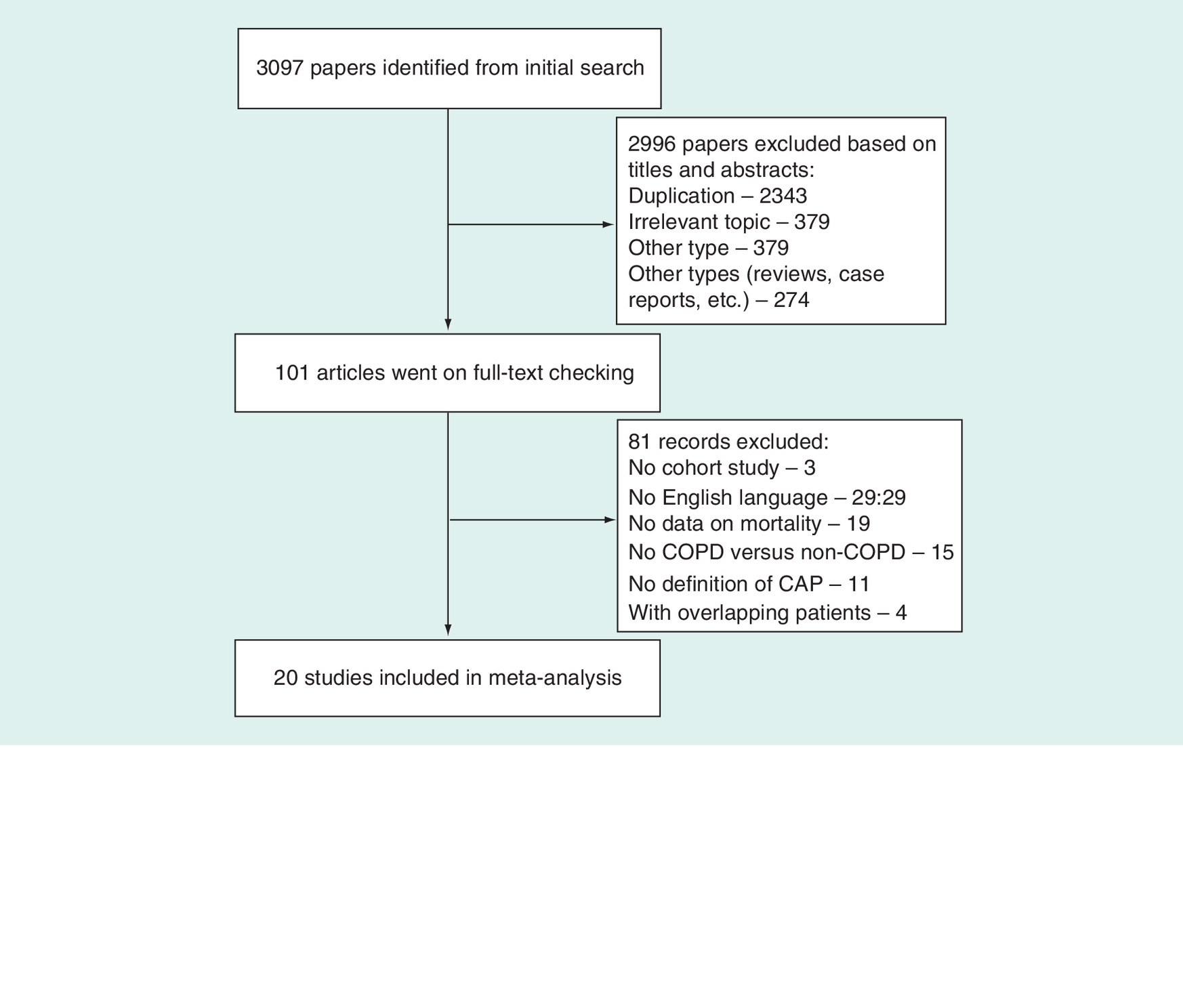
Figure 1. The search process and study identification.
CAP: Community acquired pneumonia; COPD: Chronic obstructive pulmonary disease.
Study characteristics & quality
All the included studies were published between 2006 and 2019, involving 918,449 patients hospitalized with CAP over a period of 22 years (1995–2016). A total of 304,222 and 614,227 patients were included in the COPD and non-COPD group, respectively. The mean age of the patients included varied from 54.2 to 82 years, with proportions of males ranging from 40 to 95%. Among the 20 cohort studies, 11 were prospective design [7,10,11,15,18–24], and 9 were retrospective design [8,9,25–31]. All studies were conducted in general inpatients population, except two [24,28] in ICU admissions only. Radiographically confirmed that pneumonia was reported in 18 studies, while one study [28] identified CAP according to symptoms or signs of pneumonia and medical records, and one study [29] according to the International Classification of Diseases-Ninth Revision. The definition of COPD was less certain, with only ten studies confirming COPD cases by spirometric evidence in ten studies [7,9–11,15,19,23,26,27,30]. The detailed study characteristics are presented in Table 1.
| Study (year) | Region | Study design | Sample size | Population (COPD/non-COPD) | CAP definition | CAP severity | COPD definition | Mortality | ||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean age (years) | Male (%) | ||||||||
| Bonnesen et al. (2019) | Denmark | Retrospective, multi-center | 1309 | 243/1066 | 76/71 | 48/47 | Radiological findings and clinical symptoms | CURB-65 scores 3–5: 24%/13% | Patient self-report | In-hospital, 30-days mortality |
| Braeken et al. (2015) | European | Prospective, multi-center | 1307 | 264/1043 | 71/57 | 64/55 | Radiological findings and clinical symptoms | CURB scores 2–4: 20%/9% | Spirometric evidence | 30-days, 90-days mortality |
| Crisafulli et al. (2013) | Spain | Prospective, multi-center | 367 | 117/250 | 72/64 | 95/60 | Radiological findings | PSI class IV–V: 61%/43% | Spirometric evidence | In-hospital, 30-days, 90-days, 1-year mortality |
| Dai et al. (2018) | China | Retrospective, multi-center | 520 | 230/290 | 82/79 | 74/40 | Radiological findings and clinical symptoms | PSI >130: 24%/10% | Spirometric evidence | In-hospital, 60-days mortality |
| Fujiki et al. (2007) | Japan | Prospective, single-center | 105 | 30/75 | 81.8 | 62 | Radiological findings and clinical symptoms | Pneumonia score >6: p <0.01 | Not reported | In-hospital mortality |
| Gómez-Junyent et al. (2014) | Spain | Prospective, single-center | 4121 | 983/3138 | 74/67 | 91/61 | Radiological findings and clinical symptoms | PSI class IV–V: 74%/54% | Spirometric evidence | In-hospital, 30-days mortality |
| Holter et al. (2016) | Norway | Prospective, single-center | 259 | 60/199 | 66 | 51 | Radiological findings and clinical symptoms | CURB-65 scores 3–5: 37% | Medical records and clinical symptoms | 5-years mortality |
| Ito et al. (2017) | Japan | Retrospective, single-center | 1834 | 440/1394 | 73.5 | 70 | Radiological findings and clinical symptoms | PSI class IV–V: 72% | Spirometric evidence | 30-days mortality |
| Lenz et al. (2017) | Norway | Retrospective, single-center | 173 | 67/106 | 64.9/57.2 | 49 | Medical records and clinical symptoms | SAPS II: 12%/13% | Medical records | In-hospital, 5-years mortality |
| Liapikou et al. (2012) | Spain | Prospective, single-center | 1379 | 212/1167 | 73.4/69.4 | 90/54 | Radiological findings and clinical symptoms | PSI class IV–V: 75%/66% | Spirometric evidence | 30-days mortality |
| Menendez et al. (2009) | Spain | Prospective, multi-center | 453 | 79/374 | 67.3 | 62 | Radiological findings and clinical symptoms | PSI class IV–V: 72% | Not reported | 30-days mortality |
| Miguel et al. (2017) | Spain | Retrospective, national database | 901136 | 299713/ 601423 | 75.9/75.3 | 76/53 | ICD-9 codes | Not reported | ICD-9 codes | In-hospital mortality |
| Molinos et al. (2009) | Spain | Prospective, multi-center | 710 | 244/466 | 73.7/63.6 | 85/59 | Radiological findings and clinical symptoms | PSI class IV–V: 56%/34% | Spirometric evidence | 30-days mortality |
| Neupane et al. (2010) | Canada | Prospective, multi-center | 652 | 315/337 | 79.2 | 62.5 | Radiological findings and clinical symptoms | CRB-65 scores: 1.53 ± 0.7 | Not reported | 30-days mortality |
| Restrepo et al. (2006) | USA | Retrospective, multi-center | 744 | 215/529 | 69.4/58.2 | 92/73 | Radiological findings and ICD-9 codes | PSI scores: 105 ± 32/87 ± 34 | Medical records | 30-days, 90-days mortality |
| Pifarre et al. (2007) | Spain | Prospective, single-center | 707 | 132/575 | 70.3/54.2 | 82/60 | Radiological findings and clinical symptoms | Not reported | Spirometric evidence | 30-days mortality |
| Pizzini et al. (2017) | Austria | Retrospective, single-center | 68 | 20/48 | 75/68 | 60/63 | Radiological findings and clinical symptoms | Not reported | Spirometric evidence | 30-days mortality |
| Rello et al.(2006) | Spain | Prospective, multi-center | 428 | 176/252 | 67.1/57.1 | 85/64 | Radiological findings | APS: 12.6 ± 10.1/12.4 ± 7.0 | Medical records | In-hospital mortality |
| Snijders et al. (2010) | The Netherlands | Retrospective, single-center | 262 | 95/167 | 70.4/60.8 | 64/46 | Radiological findings and clinical symptoms | PSI class IV–V: p < 0.05 | Spirometric evidence | In-hospital, 30-days mortality |
| Torner et al. (2017) | Spain | Retrospective, multi-center | 1915 | 587/1328 | ≥65 | 61 | Radiological findings and clinical symptoms | PSI class IV–V: 68% | Not reported | 30-days mortality |
APS: Acute physiological score of Acute Physiology And Chronic Health Evaluation II score; CAP: Community acquired pneumonia; COPD: Chronic obstructive pulmonary disease; CURB: Confusion, urea, respiratory rate and blood pressure; ICD-9: The International Classification of Diseases-Ninth Revision; PSI: Pneumonia Severity Index; SAPS: Simplified Acute Physiology Score.
Impact of COPD on mortality in patients with CAP
When analyzing unadjusted data on in-hospital and 30-days mortality, the pooled results from the meta-analysis of nine and 14 studies did not show any clear or consistent association between the presence of COPD and mortality in CAP (OR: 0.93 [95% CI: 0.60–1.45] and 1.06 [95% CI: 0.72–1.58], respectively) (Figures 2 & 3). Inter-study heterogeneity was high, with I2 = 85% in both in-hospital and 30-days mortality. Data synthesis found no statistically significant increase in 90-days and long-term mortality with COPD versus without COPD (OR: 0.89 [95% CI: 0.26–3.02]; I2 = 90% and 1.70 [95% CI: 0.77–3.77]; I2 = 79%, respectively; Figures 4 & 5). After adjustment, meta-analysis of seven studies with the adjusted data on 30-days mortality showed similarly no significant association between COPD and increased 30-days mortality, and the heterogeneity was high (OR: 1.06 [95% CI: 0.68–1.44]; I2 = 82%) (Figure 6). No analysis of adjusted data were available for other time-point mortality due to insufficient data.
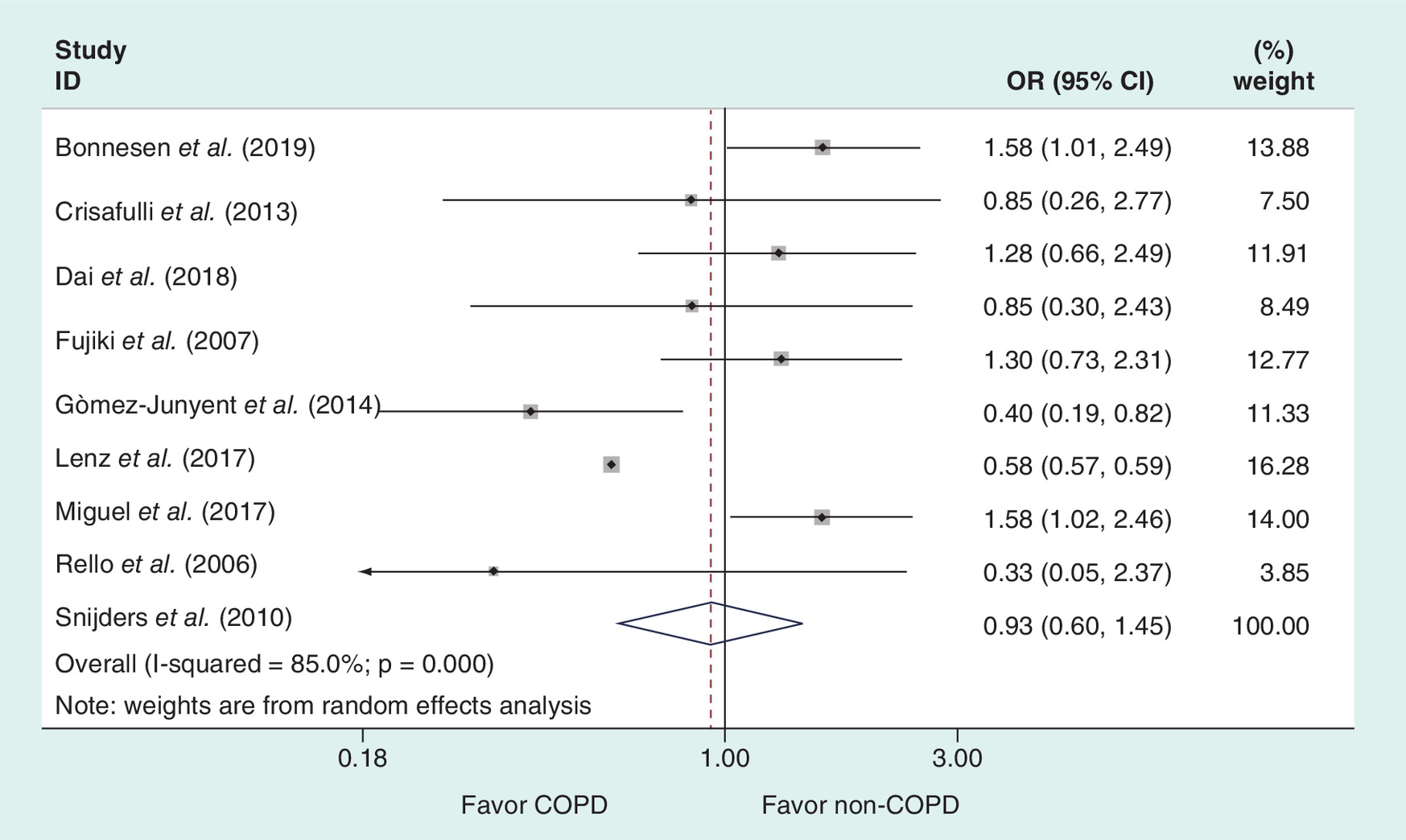
Figure 2. Meta-analysis of in-hospital mortality in patients with COPD and non-COPD.
COPD: Chronic obstructive pulmonary disease; OR: Odds ratio.
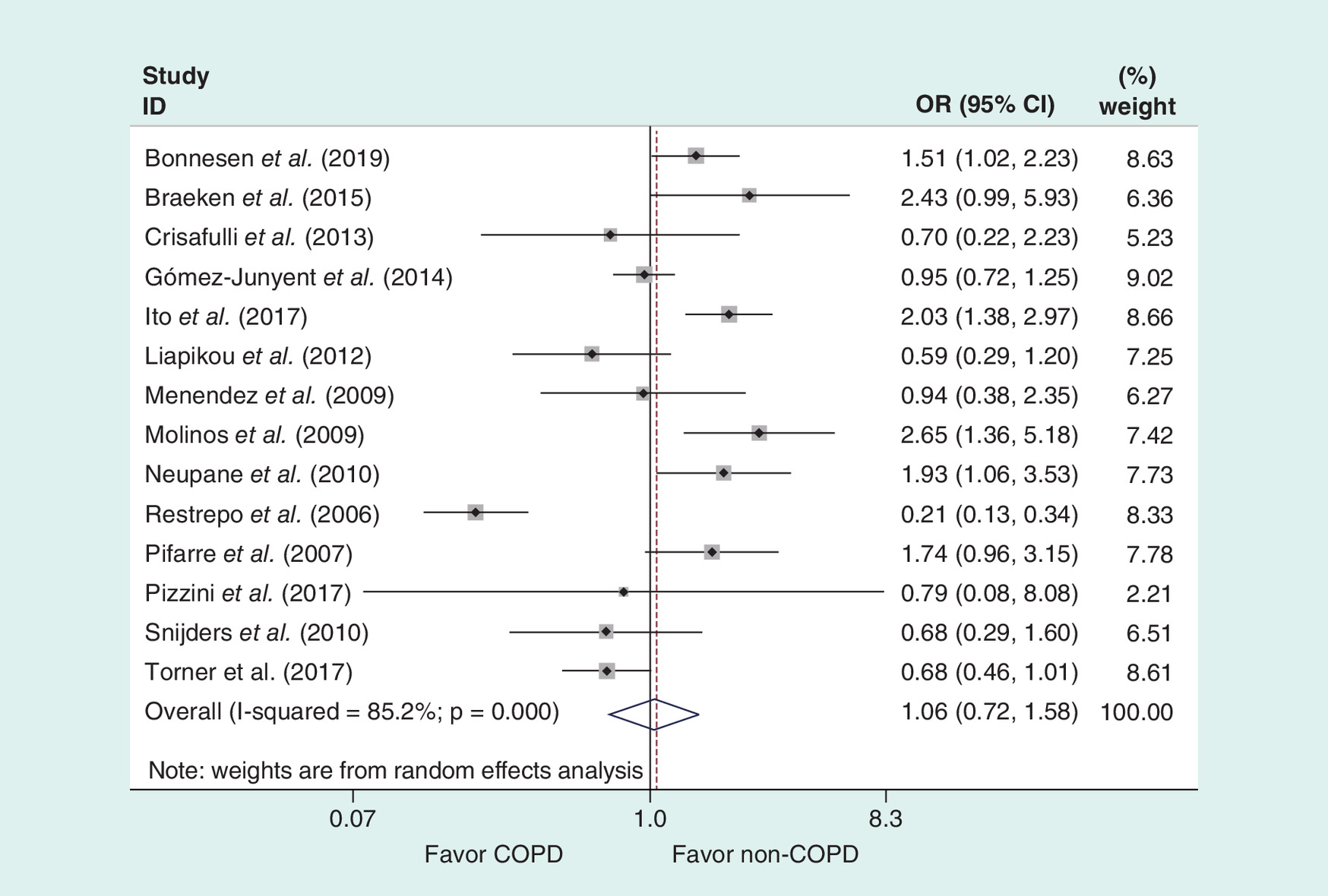
Figure 3. Meta-analysis of 30-days mortality in patients with COPD and non-COPD.
COPD: Chronic obstructive pulmonary disease; OR: Odds ratio.
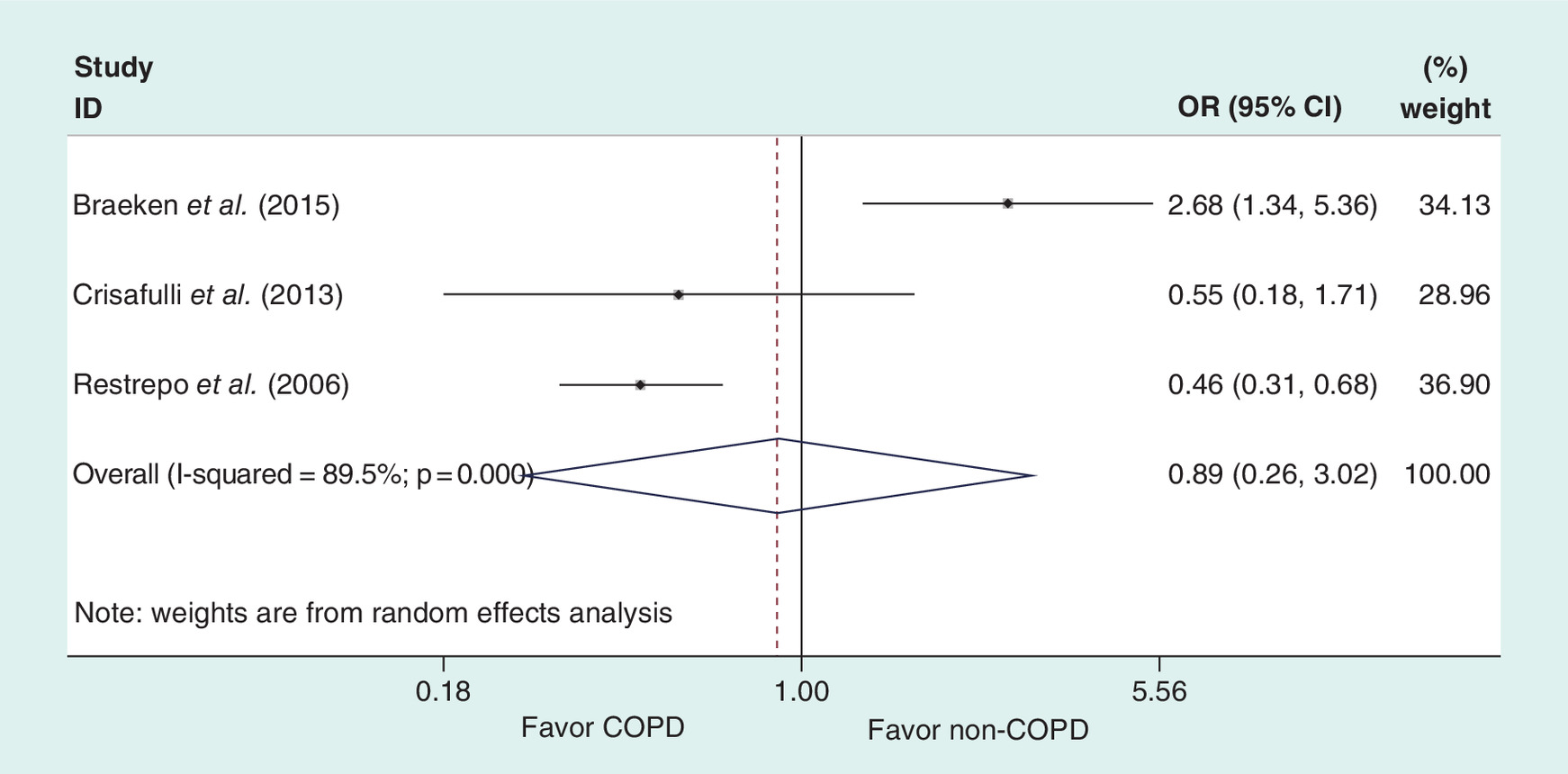
Figure 4. Meta-analysis of 90-days mortality in patients with COPD and non-COPD.
COPD: Chronic obstructive pulmonary disease; OR: Odds ratio.

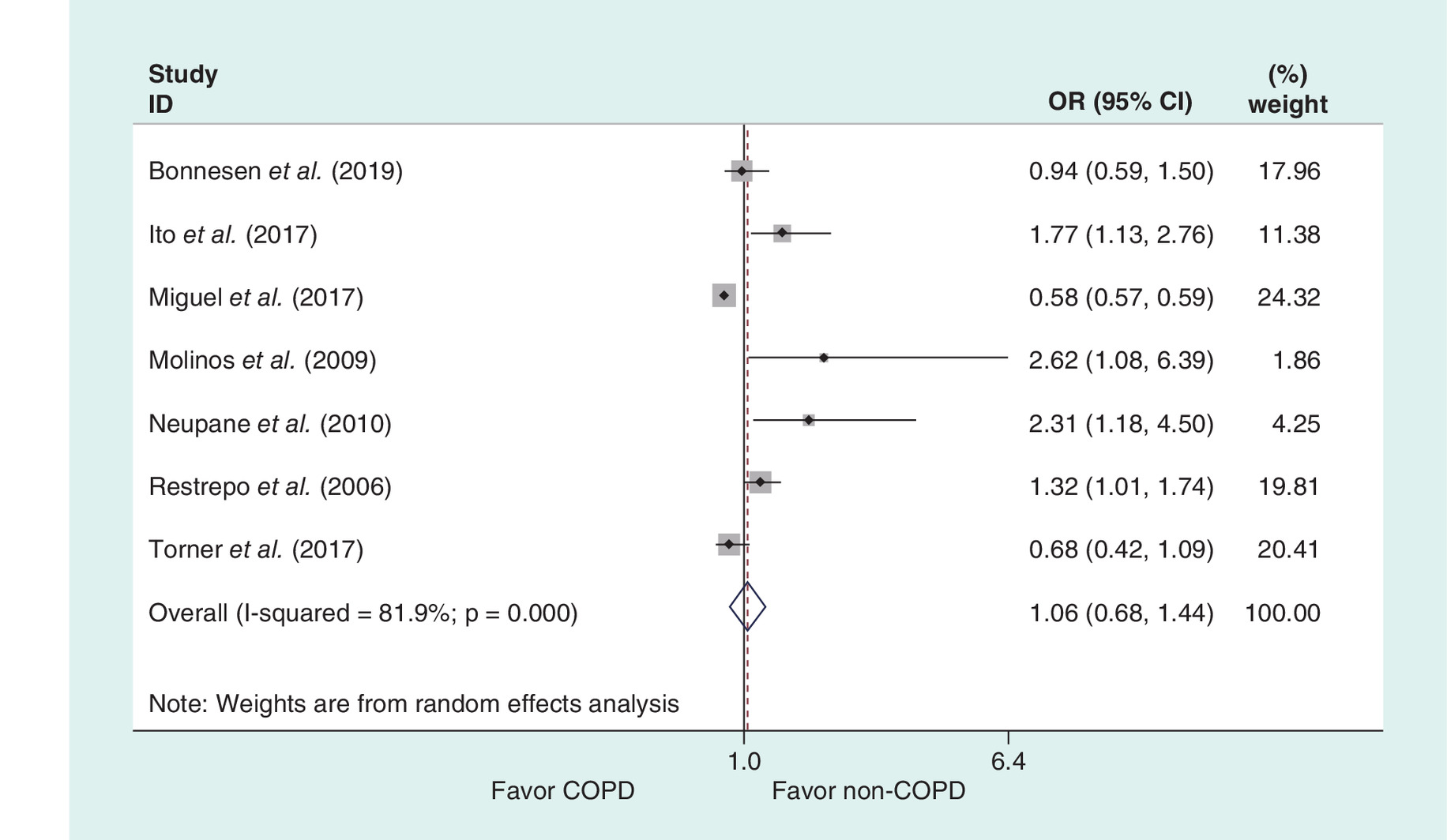
Figure 6. Meta-analysis of adjusted 30-days mortality in patients with COPD and non-COPD.
COPD: Chronic obstructive pulmonary disease; OR: Odds ratio.
Additional analysis
Additional analyses were only performed in in-hospital and 30-days mortality based on data adequacy. The subgroup analysis overall did not substantially alter the pooled estimates, except for prospective subgroup in-hospital mortality, indicating a trend toward higher mortality rate associated with COPD (OR: 1.34 [95% CI: 0.98–1.85]; I2 = 0%). The sensitivity analysis showed that no individual study had an impact on the pooled effects and heterogeneity. Restricting the meta-analysis to studies with spirometric confirmation of COPD did not cause great changes for the unadjusted in-hospital and 30-days mortality, but materially increased the overall effect size of adjusted 30-days mortality, indicating COPD was significantly associated with 30-days mortality, if confounders were controlled (OR: 1.84; 95% CI: 1.06–2.62; I2 = 0%).
Publication bias
Begg’s and Egger’s test were performed based on studies with data on the unadjusted 30-days mortality, which detected no publication bias among the included studies (p = 0.89).
Discussion
Since it is always a matter of debate whether the co-existence of COPD increased mortality in patients with CAP, we tried to draw a conclusion through combining the existing evidence. In the present meta-analysis including 20 cohort studies, we found CAP patients comorbid with COPD had the same mortality rate as patients without COPD, no matter in short-term or long-term periods. However, evident inconsistency was found among the included studies to which we should pay more attention. Results from two studies with spirometrically-defined COPD indicated higher 30-days mortality in patients with COPD and CAP compared with patients without COPD, while this evidence was weak and underpowered owing to small sample size.
In this meta-analysis, CAP patients identified with COPD were reported more likely to be males, older, associated with additional comorbidities and categorized as severe pneumonia. Incomparability of baseline characteristics may be the major reason for the divergent findings of individual studies and lead to substantial heterogeneity across studies. Although COPD patients with CAP usually develop more severe pneumonia than non-COPD patients which may suggest their poorer outcomes, the pooled effects did not demonstrate the significant association between comorbid COPD and increased mortality. To reduce confounders, multivariate adjusted data were analyzed and still failed to provide evidence of increased mortality related to the presence of COPD.
Our findings regarding mortality should be taken as hypothesis generating to help further exploration, with different possible explanations for the conflicting results. First, the use of inhaled corticosteroid were reported in several included studies, which has been shown to be a protective factor and associated with lower mortality [32–34]; but possible influence of inhaled corticosteroid therapy in our results was unknown because no clear information was given and further analysis was unavailable. Second, there was an evident association between COPD and higher CAP mortality when examining only patients with COPD and excluding other pulmonary conditions, thus the diagnosis of COPD combined with other pulmonary diseases may bias the overall impact of COPD on mortality and further investigation should minimize this bias [8,35]. Furthermore, future studies should investigate severe-to-very severe patients with COPD and comorbidities (e.g., arrhythmias) at an increased risk of exacerbations, as this population is at a higher risk of future exacerbations, hospitalizations and death [36]. Third, variation in diagnostic criteria may cause misclassification of COPD and bring difficulties to measure any association consistently. Interestingly, while considering adjustment for confounders, we used spirometrically criteria to establish the diagnosis of COPD and found that COPD population exhibited significantly higher 30-days mortality as compared with non-COPD population. However, small sample size limited the strength and validity of the result and future studies are encouraged to verify this issue.
The current meta-analysis is more critical concerning the study design, study quality and sample size than any other previous meta-analyses on this topic [12,13]. Subgroup analysis of prospective studies and studies with moderate patient comparability or with more than 1000 participants may improve our result validity and be useful for planning future studies. There was an included study by Miguel et al. having a terribly larger sample size relative to other included studies, with 901,136 patients from national database [29], and it may be worrying that it may have caused some bias; however, we found elimination of this study did not bring any changes to our findings. Overall, the meta-analysis was robust to subgroup and sensitivity analyses. On the other hand, prior published meta-analyses of COPD versus non-COPD on pneumonia mortality are less comprehensive than our current meta-analysis, as they did not include more recent cohort studies, and generally did not evaluate mortality in different time points [12,13].
This meta-analysis represents the most complete analysis for this clinical question to date. However, some limitations should be acknowledged. First, significant inconsistency was present among studies and no clear source of heterogeneity was identified, thus the interpretation of the results should be careful. Additionally, multivariate analysis adjusted by various confounders like age, sex, processes of care, other comorbidities or severity of illness could cause some bias in the adjusted 30-days mortality. Second, as a major factor, COPD severity is not well addressed by any of the currently available research. It is reasonable to expect that COPD patients with the Global initiative for chronic Obstructive Lung Disease (GOLD) stage ‘D’ or FEV1 <30% predicted have a much poorer chance of surviving a pneumonia than those with milder disease. The inability to see any impact on survival could be due to selection biases and classification errors introduced by including a high proportion of COPD cases with mild disease. Third, study population only included inpatients and ICU patients and generation to other patients should be done with caution; the included studies were conducted predominantly in Europe, therefore, geographical factor could bring some bias in the final analysis. Finally, data on 90-days and long-term mortality are sparse and more clinical evidences are required until we can draw a definite conclusion.
Conclusion
The current available evidence suggests that there is still not enough evidence to clear the impact of COPD on mortality in patients hospitalized with CAP. Future studies should prospectively assess whether clinically differences exist in pneumonia mortality between COPD and non-COPD patients by conducting adequately powered cohort studies, with adequate adjustment for confounders, spirometric confirmation of COPD and sufficient duration of follow-up to provide valid estimates.
•
Community acquired pneumonia (CAP) is one of the most common infectious diseases that contributes to substantial health and economic burden in the world.
•
Chronic obstructive pulmonary disease (COPD) is one of the most common comorbidities and risk factors in patients with CAP.
•
This study reviewed the most recent literature and aimed to determine the impact of COPD on mortality in patients with CAP.
•
In total, 20 cohort studies were included and the pooled results showed that CAP patients comorbid with COPD had similar short- and long-term mortality rate as patients without COPD.
•
Subgroup analysis on prospective studies indicated a trend toward higher in-hospital mortality rate associated with COPD.
•
COPD was significantly associated with 30-days mortality in studies with spirometric confirmation of COPD if confounders were controlled.
•
Given high inter-study heterogeneity, the evidence in this meta-analysis is still not strong enough to clear the impact of COPD on mortality in patients hospitalized with CAP.
•
More prospective studies with spirometrically-defined COPD and adequate adjustment for confounders are needed.
Author contributions
H Ma was responsible for study conception and data interpretation and was the corresponding author. T Liu and Y Zhang were responsible for literature search and data collection. Z Ye and W Jia made contribution to statistical analysis using software and the draft of manuscript. Y Li contributed to manuscript revision. All authors have read and approved the manuscript.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Reference
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Welte T, Torres A, Nathwani D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 67(1), 71–79 (2012).
2.
Ewig S, Torres A. Community-acquired pneumonia as an emergency: time for an aggressive intervention to lower mortality. Eur. Respir. J. 38(2), 253–260 (2011).
3.
Blasi F, Mantero MSP, Tarsia P. Understanding the burden of pneumococcal disease in adults. Clin. Microbiol. Infect. 18(Suppl. 5), 7–14 (2012).
4.
Cillóniz C, Polverino E, Ewig S et al. Impact of age and comorbidity on cause and outcome in community-acquired pneumonia. Chest 144(3), 999–1007 (2013).
5.
Calverley PMA, Stockley RA, Seemungal TAR et al. Reported pneumonia in patients with COPD: findings from the INSPIRE study. Chest 139(3), 505–512 (2011).
6.
Heron M. Deaths: leading causes for 2010. Natl Vital Stat. Rep. 62(6), 1–96 (2013).
7.
Molinos L, Clemente MG, Miranda B et al. Community-acquired pneumonia in patients with and without chronic obstructive pulmonary disease. J. Infect. 58(6), 417e24 (2009).
8.
Restrepo MI, Mortensen EM, Pugh JA, Anzueto A. COPD is associated with increased mortality in patients with community-acquired pneumonia. Eur. Respir. J. 28(2), 346–351 (2006).
•• This is an included study with high quality and large sample size.
9.
Snijders D, van der Eerden M, de Graaff C, Boersma W. The influence of COPD on mortality and severity scoring in community-acquired pneumonia. Respiration 79(1), 46–53 (2010).
10.
Crisafulli E, Menéndez R, Huerta A et al. Systemic inflammatory pattern of patients with community-acquired pneumonia with and without COPD. Chest 143(4), 1009–1017 (2013).
11.
Liapikou A, Polverino E, Ewig S et al. Severity and outcomes of hospitalised community-acquired pneumonia in COPD patients. Eur. Respir. J. 39(4), 855–861 (2012).
•• This is an included study with high quality and large sample size.
12.
Loke YK, Kwok CS, Wong JM, Sankaran P, Myint PK. Chronic obstructive pulmonary disease and mortality from pneumonia: meta-analysis. Int. J. Clin. Pract. 67(5), 477–487 (2013).
13.
Jiang HL, Chen HX, Liu W, Fan T, Liu GJ, Mao B. Is COPD associated with increased mortality and morbidity in hospitalized pneumonia? A systematic review and meta-analysis. Respirology 20(7), 1046–1054 (2015).
14.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol. 62(10), 1006–1012 (2009).
15.
Braeken DCW, Franssen FME, Schütte H et al. Increased severity and mortality of CAP in COPD: results from the German Competence Network, CAPNETZ. Chronic Obstr. Pulm. Dis. 2(2), 131–140 (2015).
•• This is an included study with high quality and large sample size.
16.
Wells G, Shea B, O'Connell D et al. The newcastle-ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analysis (2001). www.Ohri.Ca/programs/clinical_epidemiology/oxford.asp
17.
Ioannidis JP, Trikalinos TA. The appropriateness of asymmetry tests for publication bias in meta-analyses: a large survey. CMAJ 176(8), 1091–1096 (2007).
18.
Fujiki R, Kawayama T, Ueyama T, Ichiki M, Aizawa H. The risk factors for mortality of community-acquired pneumonia in Japan. J. Infect. Chemother. 13(3), 157–165 (2007).
19.
Gómez-Junyent J, Garcia-Vidal C, Viasus D et al. Clinical features, etiology and outcomes of community-acquired pneumonia in patients with chronic obstructive pulmonary disease. PLoS ONE 9(8), e105854 (2014).
•• This is an included study with high quality and large sample size.
20.
Holter JC, Ueland T, Jenum PA et al. Risk factors for long-term mortality after hospitalization for community-acquired pneumonia: a 5-year prospective follow-up study. PLoS ONE 11(2), e0148741 (2016).
21.
Menéndez R, Martínez R, Reyes S et al. Biomarkers improve mortality prediction by prognostic scales in community-acquired pneumonia. Thorax 64(7), 587–591 (2009).
22.
Neupane B, Walter SD, Krueger P, Marrie T, Loeb M. Predictors of inhospital mortality and re-hospitalization in older adults with community-acquired pneumonia: a prospective cohort study. BMC Geriatr. 10, 22 (2010).
23.
Pifarre R, Falguera M, Vicente-de-Vera C, Nogues A. Characteristics of community-acquired pneumonia in patients with chronic obstructive pulmonary disease. Respir. Med. 101(10), 2139–2144 (2007).
24.
Rello J, Rodriguez A, Torres A et al. Implications of COPD in patients admitted to the intensive care unit by community-acquired pneumonia. Eur. Respir. J. 27(6), 1210–1216 (2006).
25.
Bonnesen B, Baunbæk Egelund G, Vestergaard Jensen A et al. Is chronic obstructive pulmonary disease a risk factor for death in patients with community acquired pneumonia? Infect. Dis. (Lond). 51(5), 340–347 (2019).
•• This is an included study with high quality and large sample size.
26.
Dai RX, Kong QH, Mao B et al. The mortality risk factor of community acquired pneumonia patients with chronic obstructive pulmonary disease: a retrospective cohort study. BMC Pulm. Med. 18(1), 12 (2018).
27.
Ito A, Ishida T, Tokumasu H et al. Prognostic factors in hospitalized community-acquired pneumonia: a retrospective study of a prospective observational cohort. BMC Pulm. Med. 17(1), 78 (2017).
• This is an included study with large sample size.
28.
Lenz H, Norby GO, Dahl V, Ranheim TE, Haagensen RE. Five-year mortality in patients treated for severe community-acquired pneumonia - a retrospective study. Acta Anaesthesiol. Scand. 61(4), 418–426 (2017).
29.
de Miguel-Díez J, López-de-Andrés A, Hernández-Barrera V et al. Impact of COPD on outcomes in hospitalized patients with community-acquired pneumonia: analysis of the Spanish national hospital discharge database (2004–2013). Eur. J. Intern. Med. 43, 69–76 (2017).
• This is an included study with large sample size.
30.
Pizzini A, Lunger F, Sahanic A et al. Diagnostic and prognostic value of inflammatory parameters including neopterin in the setting of pneumonia, COPD, and acute exacerbations. COPD 14(3), 298–303 (2017).
31.
Torner N, Izquierdo C, Soldevila N et al. Factors associated with 30-day mortality in elderly inpatients with community acquired pneumonia during 2 influenza seasons. Hum. Vaccin. Immunother. 13(2), 450–455 (2017).
• This is an included study with large sample size.
32.
Festic E, Scanlon PD. Incident pneumonia and mortality in patients with chronic obstructive pulmonary disease. A double effect of inhaled corticosteroids? Am. J. Respir. Crit. Care Med. 191(2), 141–148 (2015).
33.
Chen D, Restrepo MI, Fine MJ et al. Observational study of inhaled corticosteroids on outcomes for COPD patients with pneumonia. Am. J. Respir. Crit. Care Med. 184(3), 312–316 (2011).
34.
Malo de Molina R, Mortensen EM, Restrepo MI, Copeland LA, Pugh MJ, Anzueto A. Inhaled corticosteroid use is associated with lower mortality for subjects with COPD and hospitalised with pneumonia. Eur. Respir. J. 36(4), 751–757 (2010).
35.
Fine MJ, Smith MA, Carson CA et al. Prognosis and outcomes of patients with community-acquired pneumonia. A meta-analysis. JAMA 275(2), 134–141 (1996).
36.
Steer J, Gibson J, Bourke SC. The DECAF Score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax 67(11), 970–976 (2012).
Information & Authors
Information
Published In
Pages: 839 - 848
PubMed: 32885988
Copyright
© 2020 Future Medicine Ltd.
History
Received: 22 April 2020
Accepted: 24 June 2020
Published online: 4 September 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of chronic obstructive pulmonary disease on mortality in community acquired pneumonia: a meta-analysis. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0061
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Xiudi Han, Hong Wang, Liang Chen, Yimin Wang, Hui Li, Fei Zhou, Xiqian Xing, Chunxiao Zhang, Lijun Suo, Jinxiang Wang, Guohua Yu, Guangqiang Wang, Xuexin Yao, Hongxia Yu, Lei Wang, Meng Liu, Chunxue Xue, Bo Liu, Xiaoli Zhu, Yanli Li, Ying Xiao, Xiaojing Cui, Lijuan Li, Xuedong Liu, Bin Cao, Impact of inhaled corticosteroid use on elderly chronic pulmonary disease patients with community acquired pneumonia, Chinese Medical Journal, 10.1097/CM9.0000000000002936, 137, 2, (241-243), (2023).
- Dong Huang, Dingxiu He, Linjing Gong, Rong Yao, Wen Wang, Lei Yang, Zhongwei Zhang, Qiao He, Zhenru Wu, Yujun Shi, Zongan Liang, A prediction model for hospital mortality in patients with severe community-acquired pneumonia and chronic obstructive pulmonary disease, Respiratory Research, 10.1186/s12931-022-02181-9, 23, 1, (2022).