Minimally invasive surgery for low-grade spondylolisthesis: percutaneous endoscopic or oblique lumbar interbody fusion
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To compare the clinical and radiographic outcomes of percutaneous endoscopic-assisted lumbar interbody fusion (PELIF) versus oblique lumbar interbody fusion (OLIF) for the treatment of symptomatic low-grade lumbar spondylolisthesis. Material & methods: The clinical and radiographic records of 48 patients underwent single-level minimally invasive lumbar fusion with a PELIF (n = 16) or OLIF (n = 32) were reviewed. Results: The clinical and radiographic outcomes were similar in both groups. PELIF procedure exhibited superior capability of the enlargement of foraminal width, but inferior capability of the restoration of foraminal height than OLIF procedure. Conclusion: PELIF minimizes the iatrogenic damages and perioperative risks to a great extent, and seems to be a promising option for the treatment of symptomatic low-grade lumbar spondylolisthesis.
Degenerative lumbar spondylolisthesis is an important cause of low-back pain and radicular pain [1]. Surgery is steadily acquiring acceptance among patients in whom optimal medical management has failed, typically entails decompression with fusion [2,3]. Open surgeries are considered to be the gold standard with reliable improvement in ameliorating patients function and quality of life [4]. However, supporting structures such as the paraspinal muscles and facet joints might be further destabilized. On the other hand, minimally invasive (MI) surgeries, including anterior, lateral or posterior lumbar interbody fusion are evolving and seeking to minimize collateral damage with the purported advantage of preventing iatrogenic instability and progression associated with open techniques [5]. Previous studies arrived at differing conclusions about the optimal fusion strategy, with studies that focused exclusively on the population with low-grade lumbar spondylolisthesis favoring the MI surgery [6].
Oblique lumbar interbody fusion (OLIF) as an MI retroperitoneal approach for intervertebral fusion, has increased in popularity since 2012. Though promising results from OLIF for low-grade lumbar spondylolisthesis have been reported [7,8], protesters of OLIF have criticized for the relatively high incidence of intra- and postoperative complications of 9.5 and 19.9%, respectively [4,9,10]. Moreover, insufficient decompression is not uncommon, and remedial decompressive procedure might be performed through the posterior approach. Recently, percutaneous endoscopic-assisted lumbar interbody fusion technique (PELIF) as a more MI technique, has been attempted for the treatment of degenerative lumbar diseases including low-grade spondylolisthesis [11–13]. So far, there are scant reports directly comparing the outcomes of PELIF and OLIF based on clinical and radiographic criteria.
To this end, we conducted this retrospective study to compare the clinical and radiographic outcomes following PELIF and OLIF for symptomatic, single-level low-grade degenerative lumbar spondylolisthesis.
Materials & methods
Subjects
Consent was obtained from each patient and the local Institutional Review Board approved the study. We retrieved the medical records of 143 patients diagnosed as symptomatic low-grade lumbar spondylolisthesis and surgically treated between January 2017 and October 2018 at our institution. The surgical indications of PELIF included: predominant back pain with or without radiating leg pain; corresponding flexion and extension x-rays, computed tomography (CT) and magnetic resonance images showing low-grade spondylolisthesis (no more than Meyerding grade II) with degenerated discs and endplates; and refractory to nonsteroidal anti-inflammatory medications combined with bedrest for at least 2 months. Patients with clinical symptoms related to intraspinal pathology, bony fracture and diseases that impair bone quality (e.g., osteoporosis, other metabolic diseases, neoplasm, infection or systemic diseases) were excluded. A total of 16 patients (Group PELIF) who met the inclusion criteria were identified, including nine males and seven females. The mean age of the patients was 61.2 ± 8.9 years (range, 49–75 years).
The surgical indications of OLIF included: back pain with radiating leg pain; corresponding radiographic images showing low-grade spondylolisthesis with decreased intervertebral height and foraminal height; and refractory to conservative treatment for at least 2 months. Patients treated with OLIF (Group OLIF) during the same period who were suitable matches to the PELIF participants with respect to pathology level, sex and age were identified and matched at a 1:2 ratio. To be specific, the pathology level and sex should be the same, and the age gap should be within 5 years. Patients assigned to group OLIF were selected by an independent observer not involved in this study, so the patients in group OLIF were not necessarily consecutive. No factors other than those listed above were taken into account during the matching process. A total of 32 patients who met the inclusion criteria were identified, including 18 males and 14 females. The mean age of the patients was 63.9 ± 7.6 years (range, 55–73 years).
Surgical procedures
Percutaneous endoscopic lumbar interbody fusion
As described in our previous study, the patient was kept awake through the surgery. Local anesthesia supplemented with standard epidural anesthesia was mandatory for PELIF procedure. Epidural anesthesia tube was placed at least two segments above the surgical segment. A total of 1% lidocaine 3 ml was applied initially, and 0.25% ropivacaine was added to adjust the sensory level and achieve the aim of sensory-motor separation. The patient was placed in the prone position on the operating table and draped aseptically. After identifying and marking the skin entry point with the guidance of a C-arm, an 18-G spinal needle was inserted and navigated toward the intervertebral foramen under image intensifier, and then replaced by a 0.8-mm blunt-tipped guidewire. A series of blunt-tapered obturators (TESSYS Endoscopic System [Joimax GmbH, Germany]) were inserted over the guidewire under image intensifier control, then a beveled working cannula (8.5 mm of outer diameter, 7.5 mm of inner diameter) was passed over the obturator. After the obturator was withdrawn, a working channel endoscope (7.3 mm of outer diameter, 3.5 mm of working channel) was then introduced and placed diagonally on the spinal canal. The facet joint osteotomy and neurological decompression were performed as percutaneous endoscopic lumbar discectomy (PELD) procedure.
After a 2.0 mm wire was inserted, the channel was withdrawn gently and replaced by the working sheath (11.1 mm of inner diameter, Aaxter Co., Ltd, Taiwan, China) used for endoscopic interbody fusion. A series of endoscopic reamers and curettes (220 mm of length) were introduced into the disc space under image intensifier. Adequate disc space and endplate preparation were manipulated under fluoroscopic guidance and inspected through endoscopic visualization (Figure 1A). Autologous bone was harvested from the contralateral posterior superior iliac spine and placed into the frontal and contralateral area of disc space through the working sheath (Figure 1B, Supplementary Video 1). Then the expandable cage (9 mm of height, 22 mm of length, bullet shaped) was fixed on the cage holding rod and placed into the disc space under fluoroscopic guidance (Figure 1C & D, Supplementary Video 2). Again, inspected the disc space and ventral side of the dura under endoscopic visualization before withdrawing the working sheath.
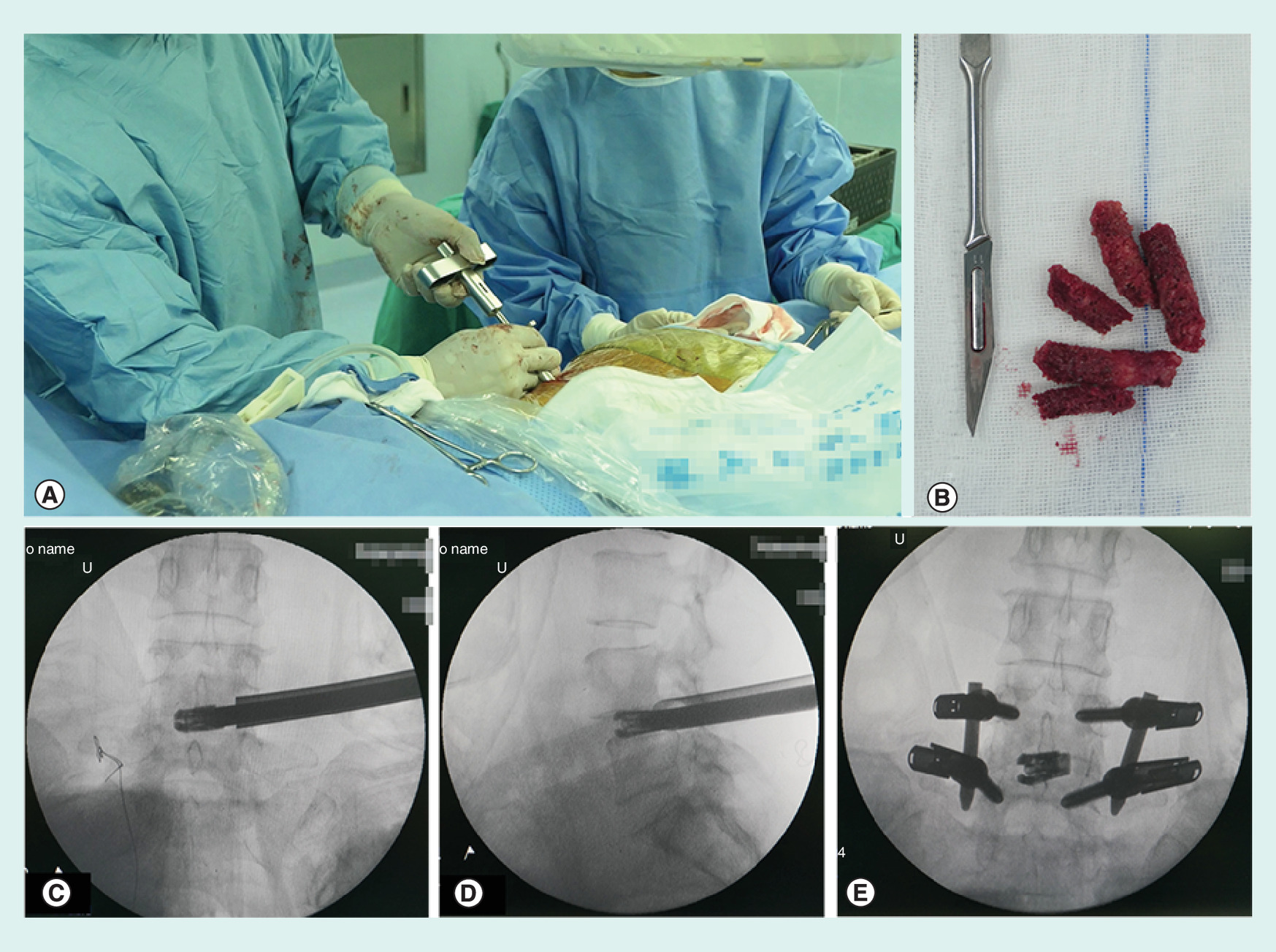
Figure 1. The surgical procedure of percutaneous endoscopic-assisted lumbar interbody fusion.
(A) The disc space and endplate preparation are prepared under image intensifier. (B) Autologous bone is harvested from the contralateral posterior superior iliac spine and placed into the frontal and contralateral area of disc space through the working sheath. (C & D) The cage is placed into the disc space under fluoroscopic guidance. (E) The pedicle screws are inserted and two rods are attached to the screws subfascially.
The percutaneous pedicle screw fixation was performed routinely. A total of 1% lidocaine was administered to the skin and evenly along the tracts of percutaneous pedicle screw. The Jamshidi needles were inserted followed by the placement of K-wires through the hollow of needles under image intensify. A series of obturator (7.5, 13.2 and 15 mm of outer diameter) were placed along with the K-wires. The awl and ball handle probe were introduced after withdrawing the outer working obturator. Then the pedicle screws (6.5 mm of diameter, 45 or 50 mm of length) were inserted and two rods were attached to the screws subfascially (Figure 1E). Removed all the instrument after final tightening of the screw extenders. Finally, closed all five incisions (about 1-cm in length) layer by layer.
Oblique lumbar interbody fusion
The patient was placed in the lateral decubitus position after general anesthesia. The target disc space was located and marked under image intensifier. A 4–6 cm skin incision was made in the lateral abdominal region, which was in the same horizontal plane as the target disc. External oblique, internal oblique and transverse abdominal muscles were then dissected along the direction of their fibers in this muscle-splitting approach. The retroperitoneal space was accessed by blunt dissection, then the peritoneal content was mobilized anteriorly and psoas was retracted posteriorly. A guidewire was placed into the target disc and confirmed by a radiograph. Sequential dilators were placed along the guidewire, then a lighted retractor was placed over the dilators and fixed to the vertebral body with a pin. Discectomy was manipulated through the operation window with nucleus pulposus clamp, then subchondral bone was exposed after sufficient vertebral endplate preparation. Autologous bone was harvested from the ipslateral posterior superior iliac spine through the skin incision intended for pedicle screw placement. A lordotic cage (Medtronic, Inc, MN, USA) packed with autologous bone was inserted into the exposed disc spaces with the guidance of a C-arm. Then, the abdominal wall muscles and the incision were closed sequentially after a drainage tube was placed [7,14]. The patient was changed to the prone position and draped aseptically, posterior percutaneous pedicle screw fixation was performed as aforementioned.
Postoperative protocol
The drainage tube was removed within 24 h after surgery in the OLIF group. All patients were mobilized 1 day postoperatively. Then, they were advised to wear a lumbosacral corset and to avoid strenuous activity for 3 months. Radiographs were taken 2 days after surgery as quality control. Analgesic medication was adapted to the severity of the back pain.
Clinical outcomes
Clinical outcomes were assessed by an independent experienced clinical research coordinator with a visual analogue scale for back pain (VAS-B) and leg pain (VAS-L), Oswestry Disability Index (ODI) and 36-Item Short Form Health Survey (SF-36). These data were collected before surgery and at each follow-up interval. In addition, perioperative data including operation time blood loss, length of hospital stay and perioperative complications were recorded as well.
Radiographic assessment
Radiographs were taken preoperatively and immediate postoperatively, as well as at each follow-up interval. Assessments were done for forward displacement for anterolisthesis (DA), disc height (DH), foraminal height (FH), foraminal width (FW) segmental lordotic angle (SLA), lumbar lordotic angle (LLA) and cage location on x-ray images (Figure 2). The DA was measured from the cortex of the posterior aspect of the caudal slipped vertebrae to the cortex of the posterior aspect of the rostral slipped vertebrae using the sagittal cut with the greatest amount of displacement [15]. The DH was measured by averaging the anterior and posterior disk heights on the lateral radiograph in neutral position. The FH was measured as the maximum distance between the inferior margin of the pedicle of the superior vertebra and the superior margin of the pedicle of the inferior vertebra. The FW was measured as the maximum distance between the posterior margin of disc and the facet joint [16]. The SLA was obtained by the angle between superior endplate of rostral vertebrae and inferior endplate of caudal vertebrae. LLA was measured as the angle between upper endplate of L1 and superior endplate of the sacrum. According to the disc center, the cage location was classified as anterior 1/3, middle 1/3 and posterior 1/3 [16]. Moreover, the inter-vertebral disc of the fusion level was evaluated for degeneration and stratified into five grades based on Pfirrmann classification [17]. The criteria used to define bone union were defined as follows: no radiolucency between the graft and the vertebral body, the presence of bridging osseous trabeculae on CT images [18].

Figure 2. Sagittal balance parameters measured on lateral x-rays.
(A) Disc height [(A + B)/2]; foraminal height (C); foraminal width (D); forward displacement for anterolisthesis (E). (B) Segmental lordotic angle (F); lumbar lordotic angle (G).
We computed the improvement rate in each outcome measure at final follow-up compared with preoperative values. The improvement rate for all parameters was calculated as (final follow-up score – preoperative score)/(preoperative score) × 100 (%).
Statistical analysis
Descriptive statistics were reported as means and standard deviations and frequencies and percentages where appropriate. SPSS 17.0 software (SPSS Inc, IL, USA) was used to conduct all statistical analysis. The Fisher exact test or chi-squared test was used to compare qualitative variables between groups, and the independent t-test or Wilcoxon rank-sum test was used to compare quantitative variables between groups. p < 0.05 was considered statistically significant.
Results
The demographic and baseline characteristics of the patients in each group are shown in Table 1. No statistical differences were found between groups in regard to the incidence of low back pain (14/16 vs 25/32; p = 0.179), the incidence of radiculopathy (13/16 vs 28/32; p = 0.835), duration of pain at index surgery (14.4 ± 4.0 vs 15.6 ± 7.3; p = 0.551), distribution of disc degeneration (p = 0.685), hospital length of stay (4.9 ± 1.2 days vs 4.3 ± 1.6 days; p = 0.298) and follow-up duration (22.6 ± 5.7 months vs 24.2 ± 7.1 months; p = 0.378). The mean operative time for the PELIF procedure was 155.2 ± 10.1 min (range 138.0–171 min), which was slightly shorter than that of OLIF procedure (160.3 ± 19.7 min, range 139.0–181 min; p > 0.05). The mean blood loss was 35.0 ± 8.5 ml (range 25.0–40.0 ml) for PELIF, which was statistically lesser than that of OLIF procedure (80.0 ± 16.9 ml, range 50–200 ml; p < 0.05).
| Variable | PELIF | OLIF | t-value | p-value |
|---|---|---|---|---|
| No. of patients (male/female) | 16 (9/7) | 32 (18/14) | N/A | N/A |
| Age in years | 61.2 ± 8.9 | 63.9 ± 7.6 | 0.948 | 0.350 |
| Low back pain | 14 | 25 | 2.102 | 0.179 |
| Radiculopathy (left/right) | 13 (4/9) | 28 (11/17) | 0.440 | 0.835 |
| Duration of pain at index surgery (months) | 14.4 ± 4.0 | 15.6 ± 7.3 | 0.602 | 0.551 |
| Pathology level | ||||
| – L3/4 | 3 | 6 | N/A | N/A |
| – L4/5 | 13 | 26 | N/A | N/A |
| Disc degeneration (Pfirrmann classification) | 0.700 | 0.685 | ||
| – Grade III | 3 | 8 | ||
| – Grade IV | 9 | 19 | ||
| – Grade V | 4 | 5 | ||
| Operation time (min) | 155.2 ± 10.1 | 160.3 ± 19.7 | 1.747 | 0.092 |
| Intraoperative blood loss (ml) | 35.0 ± 8.5 | 80.0 ± 16.9 | 2.297 | 0.033† |
| Hospital length of stay (days) | 4.9 ± 1.2 | 4.3 ± 1.6 | 1.703 | 0.298 |
| Follow-up duration (months) | 22.6 ± 5.7 | 24.2 ± 7.1 | 1.139 | 0.378 |
†
Values were compared between PELIF and OLIF groups, and the result were statistically significant (p < 0.05).
N/A: Patients were selected proportionally, and not compared between two groups.
OLIF: Oblique lumbar interbody fusion; PELIF: Percutaneous endoscopic-assisted lumbar interbody fusion.
Changes in regard to displacement for anterolisthesis, disc height, foraminal height and foraminal width indicated a significant difference in the immediate postoperative period but not at final follow-up in both groups (Table 2). The OLIF procedure provided better FH restoration than PELIF procedure after surgery (22.3 ± 4.7 mm vs 19.4 ± 3.8 mm; p < 0.01) and at the final follow-up (21.5 ± 3.9 mm vs 19.6 ± 2.4 mm; p < 0.01). However, the PELIF procedure provided better FW enlargement than OLIF procedure after surgery (11.3 ± 1.4 mm vs 9.7 ± 1.2 mm; p < 0.01) and at the final follow-up (10.9 ± 1.6 mm vs 9.5 ± 0.9 mm, 45.3 vs 10.5%, both p < 0.01). In the PELIF group, the DA at baseline, after surgery and at final follow-up were 5.7 ± 0.9 mm, 1.6 ± 0.4 mm and 1.6 ± 0.8 mm, respectively. The corresponding values in the OLIF group were 6.1 ± 2.2 mm, 2.0 ± 1.6 mm, 1.9 ± 1.4 mm, respectively. The DH in the PELIF group was 6.9 ± 1.1 mm preoperatively, 12.9 ± 1.4 mm postoperatively and 12.1 ± 1.7 mm at final follow-up, while DH in the OLIF group was 8.0 ± 2.0 mm preoperatively, 13.2 ± 1.7 mm postoperatively and 13.2 ± 2.1 mm at final follow-up. Though the DH was higher in the OLIF group at final follow-up, but the PELIF group exhibited slightly better improvement rate of DH. As listed in Table 2, except marginally better correction rate of LLA immediately after surgery in OLIF group, obvious improvements were not observed in both group in terms of SLA and LLA.
| Radiographic parameters | PELIF | OLIF | t-value | p-value |
|---|---|---|---|---|
| Displacement for anterolisthesis (mm) | ||||
| – Pre-operation | 5.7 ± 0.9 | 6.1 ± 2.2 | 1.559 | 0.052 |
| – Post-operation | 1.6 ± 0.4‡ | 2.0 ± 1.6‡ | 1.703 | 0.102 |
| – Final follow-up | 1.6 ± 0.8‡ | 1.9 ± 1.4‡ | 0.981 | 0.334 |
| – Improvement ratio (%) | 71.9% | 68.9% | 0.762 | 0.141 |
| Disc height (mm) | ||||
| – Pre-operation | 6.9 ± 1.1 | 8.0 ± 2.0 | 1.672 | 0.285 |
| – Post-operation | 12.9 ± 1.4‡ | 13.8 ± 1.7‡ | 1.553 | 0.130 |
| – Final follow-up | 12.1 ± 1.7‡ | 13.2 ± 2.1‡ | 1.419 | 0.166 |
| – Improvement ratio (%) | 75.3% | 66.0% | 4.713 | 0.041† |
| Foraminal height (mm) | ||||
| – Pre-operation | 15.3 ± 2.5 | 16.9 ± 3.1 | 1.485 | 0.062 |
| – Post-operation | 19.4 ± 3.8‡ | 22.3 ± 4.7‡ | 5.949 | 0.000† |
| – Final follow-up | 19.6 ± 2.4‡ | 21.5 ± 3.9‡ | 3.252 | 0.003† |
| – Improvement ratio (%) | 28.1% | 22.5% | 2.547 | 0.056 |
| Foraminal width (mm) | ||||
| – Pre-operation | 7.5 ± 1.4 | 8.6 ± 1.0 | 2.670 | 0.012† |
| – Post-operation | 11.3 ± 1.4‡ | 9.7 ± 1.2‡ | 1.511 | 0.034† |
| – Final follow-up | 10.9 ± 1.6‡ | 9.5 ± 0.9‡ | 1.633 | 0.046† |
| – Improvement ratio (%) | 45.3% | 10.5% | 7.571 | 0.000† |
| Segmental lordotic angle (°) | ||||
| – Pre-operation | 13.7 ± 4.5 | 15.0 ± 5.5 | 1.184 | 0.245 |
| – Post-operation | 15.4 ± 4.1 | 16.8 ± 4.0 | 0.982 | 0.336 |
| – Final follow-up | 15.7 ± 5.2 | 16.5 ± 4.8 | 0.542 | 0.592 |
| – Improvement ratio (%) | 14.5% | 10.9% | 2.033 | 0.061 |
| Lumbar lordotic angle (°) | ||||
| – Pre-operation | 48.3 ± 8.4 | 47.4 ± 9.6 | 0.802 | 0.600 |
| – Post-operation | 49.3 ± 10.3 | 52.6 ± 6.2‡ | 3.101 | 0.004† |
| – Final follow-up | 49.8 ± 9.6 | 50.2 ± 9.7 | 1.798 | 0.802 |
| – Improvement ratio (%) | 3.1% | 5.6% | 2.948 | 0.012† |
†
Values were compared between PELIF and OLIF groups, and the result were statistically significant (p < 0.05).
‡
Values were compared with preoperative ones, and the result were statistically significant (p < 0.05).
OLIF: Oblique lumbar interbody fusion; PELIF: Percutaneous endoscopic-assisted lumbar interbody fusion.
Patients in either PELIF group (Figure 3) or OLIF group showed significant improvement from preoperative score at postoperative period and final follow-up interval in all functional metrics (Table 3). For patients in the PELIF group, the VAS-B scores were 4.2 ± 1.5 at baseline, 1.3 ± 0.4 immediately after surgery, and 1.1 ± 0.6 at final follow-up, respectively. The corresponding values were 4.7 ± 1.7, 2.0 ± 0.7 and 1.2 ± 0.7 in the OLIF group, which depicted less satisfactory outcomes immediately after surgery than the PELIF procedure. As for SF-36 PCS, significantly better improvements were observed in the OLIF group than those of PELIF group immediately after surgery (50.5 ± 2.7 vs 45.6 ± 3.0; p < 0.01) and at final follow-up (56.0 ± 6.2 vs 53.8 ± 4.9; p = 0.035). Other functional metrics including VAS-L, ODI and SF-36 MCS demonstrated equivalent improvements immediately after surgery and during follow-up period (p > 0.05). The improvement ratios concerning all functional parameters at final follow-up were not statistically significant.
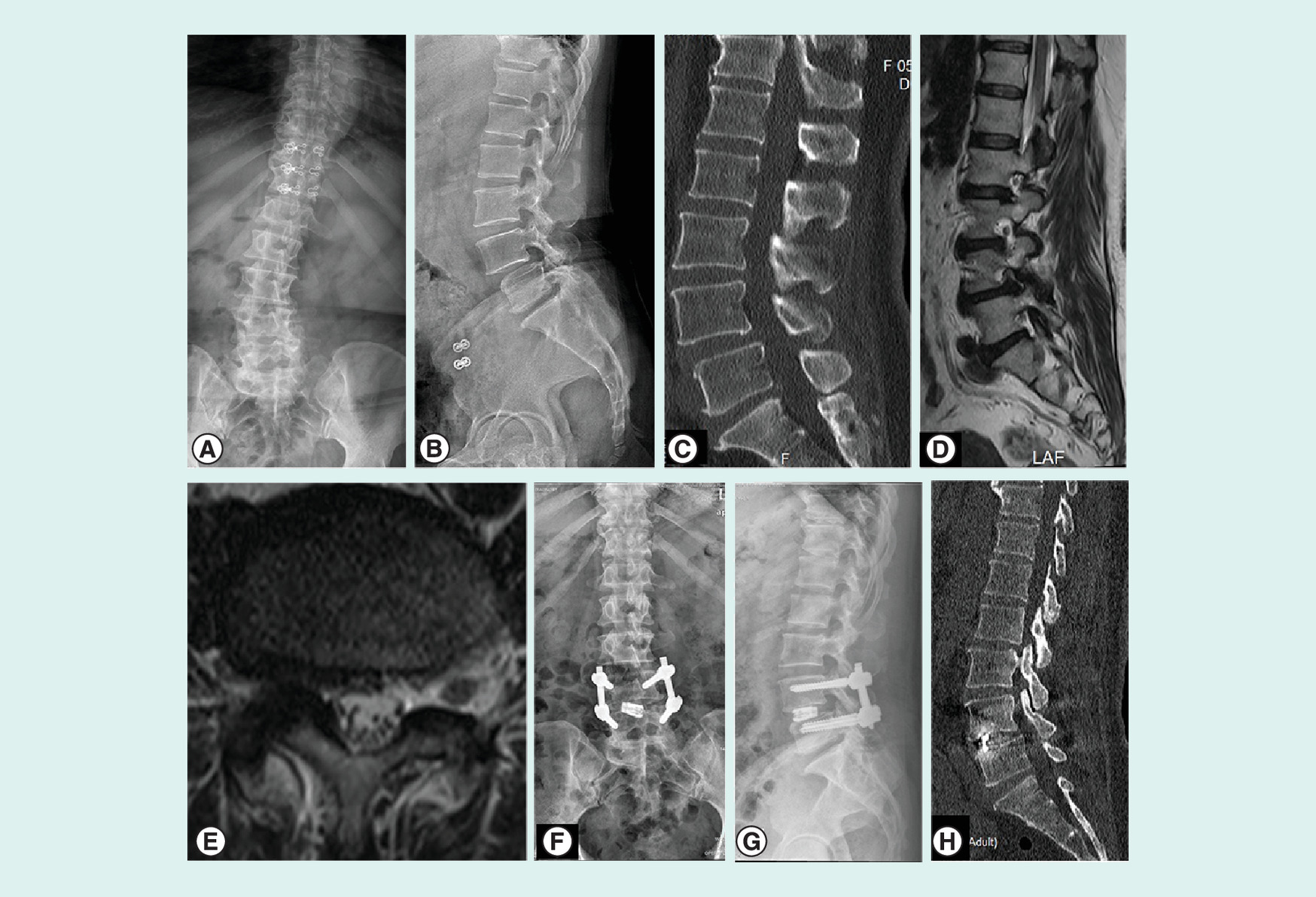
Figure 3. A 67-year-old woman was admitted to our institution due to severe low back pain, right lower extremity pain and numbness for 3 months.
Grade I spondylolisthesis was revealed on preoperative x-rays and computed tomography scans (A–C). Disc collapse and herniation on the partial right side at L4/5 was seen on magnetic resonance imaging images (D & E). The patient underwent single-level percutaneous endoscopic-assisted lumbar interbody fusion at L4/5 (F & G). Sagittal computed tomography images at 25 months postoperatively revealed solid interbody fusion (H).
| Functional assessment | PELIF | OLIF | t-value | p-value |
|---|---|---|---|---|
| VAS-B | ||||
| – Pre-operation | 4.2 ± 1.5 | 4.7 ± 1.7 | 0.892 | 0.379 |
| – Post-operation | 1.3 ± 0.4‡ | 2.0 ± 0.7‡ | 2.913 | 0.006† |
| – Final follow-up | 1.1 ± 0.6‡ | 1.2 ± 0.7‡ | 0.347 | 0.731 |
| – Improvement ratio (%) | 73.8% | 74.4% | 0.571 | 0.219 |
| VAS-L | ||||
| – Pre-operation | 6.0 ± 1.2 | 5.8 ± 1.4 | 0.442 | 0.661 |
| – Post-operation | 1.9 ± 0.6‡ | 1.8 ± 0.5‡ | 0.142 | 0.888 |
| – Final follow-up | 1.1 ± 0.5‡ | 0.9 ± 0.6‡ | 0.514 | 0.711 |
| – Improvement ratio (%) | 81.6% | 84.4% | 0.392 | 0.103 |
| ODI (%) | ||||
| – Pre-operation | 41.7 ± 4.8 | 43.3 ± 3.0 | 1.054 | 0.304 |
| – Post-operation | 16.9 ± 4.9‡ | 17.5 ± 3.2‡ | 1.066 | 0.295 |
| – Final follow-up | 11.9 ± 3.3‡ | 11.4 ± 2.6‡ | 0.938 | 0.355 |
| – Improvement ratio (%) | 71.4% | 73.6% | 0.724 | 0.401 |
| SF-36 PCS | ||||
| – Pre-operation | 33.7 ± 4.5 | 35.9 ± 3.8 | 2.973 | 0.063 |
| – Post-operation | 45.6 ± 3.0‡ | 50.5 ± 2.7‡ | 4.865 | 0.000† |
| – Final follow-up | 53.8 ± 4.9‡ | 56.0 ± 6.2‡ | 2.199 | 0.035† |
| – Improvement ratio (%) | 59.6% | 56.0% | 1.365 | 0.221 |
| SF-36 MCS | ||||
| – Pre-operation | 40.5 ± 2.4 | 38.9 ± 4.2 | 1.184 | 0.245 |
| – Post-operation | 50.6 ± 3.6‡ | 44.1 ± 5.7‡ | 0.982 | 0.336 |
| – Final follow-up | 55.7 ± 8.2‡ | 53.8 ± 7.9‡ | 0.542 | 0.592 |
| – Improvement ratio (%) | 37.5% | 38.3% | 0.727 | 0.491 |
†
Values were compared between PELIF and OLIF groups, and the result were statistically significant (p < 0.05).
‡
Values were compared with preoperative ones, and the result were statistically significant (p < 0.05).
MCS: Mental component score; ODI: Oswestry disability index; OLIF: Oblique lumbar interbody fusion; PCS: Physical component score; PELIF: Percutaneous endoscopic-assisted lumbar interbody fusion; SF-36: Short form-36 health surgery questionnaire; VAS-B: Visual analogue scale for back pain; VAS-L: Visual analogue scale for leg pain.
In the PELIF group, one patient complained about ipsilateral leg numbness that was transient in nature and improved with observation at the 4-month follow-up. In the OLIF group, two cases of leg numbness occurred in two patients. Specifically, one female patient complained about unrelieved pain and numbness in her calf. Magnetic resonance imaging scans demonstrated remnant disc fragment in the lateral recess. A PELD surgery was suggested to the patient, and she received the surgery 4 days after index surgery. The symptoms were successful diminished immediately after surgery. Another female patient experienced immediate symptom relief after index surgery. But she suffered from progressively intermittent claudication, and complained about pain and numbness in her calf at her 13-month return visit. Radiographic data demonstrated ligamentum flavum hypertrophy and spinal canal stenosis. The patient received open laminectomy with posterolateral fusion, and her symptoms were relieved gradually. No other perioperative complications including dural tear, infection, or implant loosening occurred. According to the CT scans at the final follow-up visit, the presence of bridging bone through the cage or external to it was observed in all cases, which was assessed as denoting a successful fusion.
Discussion
The initial management of low-grade lumbar spondylolisthesis with neurogenic symptoms is typically conservative. For patients who do not experience relief, the current standard of care for surgical management is decompression and fusion, which is recognized to considerably improve clinical outcomes [19]. Various surgical techniques have been described to achieve fusion in the management of spondylolisthesis, from the classic posterolateral fusion, to posterior lumbar interbody fusion (PLIF), and transforaminal lumbar interbody fusion (TLIF). No particular method has been shown to be superior in terms of clinical outcomes [20].
OLIF, as a modification of the retroperitoneal approach for microsurgical anterolateral lumbar interbody fusion, has gained its popularity in the treatment of lumbar spondylolisthesis [7]. Despite dispute remains over the extent of decompression due to its indirect decompressive nature, there is an abundance of descriptive studies favoring this technique for satisfying reduction [7,21–23]. The advent of percutaneous endoscopic lumbar interbody fusion, pioneered by Osman [11], represents the latest technical advancement in the surgical management of symptomatic low-grade lumbar spondylolisthesis [11,24,25]. However, the clinical and radiographic outcomes of PELIF are still hang in doubt. To obtain the comparable outcomes of mainstream MI techniques such as OLIF, PELIF procedures need to be as effective as OLIF in terms of achieving the intended goals of surgery (e.g., pain and functional improvement, decompression of the spinal canal and the foramen and restoration of regional and global alignment). As demonstrated in the current study, PELIF with direct decompression and OLIF with indirect decompression both have their merits in the treatment at symptomatic low-grade lumbar spondylolisthesis.
Given the stricter access, concerns have been raised about the capacity of PELIF to offer sufficient reduction of spondylolisthesis; and to date, it has not been directly compared with OLIF in that regard. [26] Castellvi et al. [27] mentioned the ability of single-level OLIF in terms of sagittal balance correction. Significant improvement was seen in all radiographic parameters, with increases of 61% in DH, 16% in contralateral FH and 18% in ipsilateral FH. Sparse data exist regarding the sagittal balance correction of PELIF technique, with only one study reporting a mean of 3 mm correction in DH. [28] In the present study, expandable cages were applied in the PELIF procedure, and comparable outcomes regarding the restoration of DH were observed between the two group after surgery. We referred to the radiographic data of MI-TLIF, which was direct decompression through the posterior approach as well. Isaacs et al. [29] reported comparative radiographic outcomes of MI-lateral and MI-TLIF in the treatment of degenerative spondylolisthesis. The results showed that the magnitudes of both ipsilateral and contralateral foraminal height increase were significantly greater in the MI-lateral group, which was verified by the present study. Ahn et al. [30] conducted quantitative assessment of the foraminal parameters after endoscopic lumbar foraminotomy. The most prominent increase was observed in FW, with a 44.2% increase, while FH increased by 18.6%. In the present study, the improvement ratio of FW was considerably better in the PELIF group than that of OLIF group (50.7 vs 12.8%). This may be explained by the fact that the decompression procedure of PELIF focuses more in the anteroposterior direction at level of redundant disc and the tip of the hypertrophic superior facet rather than in the craniocaudal direction. Partial resection of the upper or lower pedicle as well as soft tissue removal with endoscopic instruments could increase FH.
This study demonstrated similar results of sagittal balance correction in both groups. SLA didn't indicate a significant improvement in the immediate postoperative period and at final follow-up in both groups. But, OLIF corrected LLA slightly more effectively than PELIF immediately after surgery, which was consistent with the trend among previous comparative studies favoring the superiority of lateral approach over posterior approach in regard to restoration of lumbar lordosis. This phenomenon might be attributed to the feature of the case; a 12° cage was used in OLIF and the 0° expandable cage was used in PELIF. In addition, both SLA and LLA were not changed obviously from preoperative to long-term follow-up in neither group. Champagne et al. [31] compared three widely used interbody fusion approaches in regard to their ability to correct sagittal balance, including pelvic parameters. Minor impacts on global sagittal alignment and pelvic parameters were observed among patients surgically treated on single level excluding L5-S1. Only one level manipulated minimized the impact on focal and segmental alignment. Moreover, LLA was essentially within range of normal preoperative values and remained as same postoperatively in both groups. Thus, we could not draw conclusions on the relationship between the sagittal alignment and surgical approaches including PELIF and OLIF.
A number of recent studies documented comparatively clinical results of indirect and direct MI decompression [4,16,20,23,27]. Lin et al. [32] reported paralleling clinical outcomes of 104 patients treated with OLIF and 144 patients treated with MI-TLIF. Improvement of 33.56 points in ODI, 4.56 points in VAS-B and 6.84 points in VAS-L was observed in the OLIF group, while improvement of 30.27 points in ODI, 4.68 points in VAS-B and 6.48 points in VAS-L was observed in the MI-TLIF group. Previous studies have also suggested that a minimally clinically important change of at least 10 points regarding ODI and at least 2.5 points for VAS could be determined as clinically relevant improved [33]. The evaluation of clinical outcomes in the present study indicated excellent improvement in both groups. Noteworthy, there was a greater decrease in VAS-B in patients treated by PELIF as compared with those treated by OLIF immediately after surgery (1.3 ± 0.4 vs 2.0 ± 0.7), which might be owing to the lesser iatrogenic violation of PELIF procedure. In the PELIF group, 73.8% decrease in VAS-B, 81.7% decrease in VAS-L, 71.4% decrease in ODI and 37.5% improvement in SF-36 MCS were observed at final follow-up. In the OLIF group, a similar trend was observed representing 74.4% decrease in VAS-B, 84.4% decrease in VAS-L, 73.7% decrease in ODI and 38.3% improvement in SF-36 MCS at final follow-up. These findings were in line with those documented in previous studies. Thus, despite of better improvement of SF-36 PCS in OLIF group, there was no significant difference between the two groups in clinical outcomes regarding the patient's recovery at last follow-up in this study. Overall, compared with OLIF technique, PELIF could offer patients with equivalent clinical outcomes but lesser iatrogenic damage.
Our results were also within the acceptable range in terms of complication rates, as compared with similar studies. In the PELIF group, one patient complained about ipsilateral leg numbness that was transient in nature and improved with observation at the 4-month follow-up. Moreover, bone fusion was achieved in all cases. In 2013, Jacquot et al. [12] reported the clinical and radiological results of 57 patients treated with PELIF. The surgical outcome was not promising as mentioned by themselves, since cage migrations were observed among 15 cases, and 13 (22.8%) symptomatic cases accepted remedial operation. According to our preliminary experience, complete decompression, sufficient and adequate disc space preparation, utilization of autogenous bone instead of allograft, and complementary posterior fixation are key factors for the successful implementation of PELIF technique. In the OLIF group, 6.3% (2/32) of patients suffered leg numbness postoperatively and during follow-up period, depicting a lower complication rate than an average of 9.5% as documented in literature [34].
The current study presents various limitations. First, this is a retrospective series of highly selected cases and selection bias is unavoidable. But, we have kept the consistency of demographic data at baseline, including number of patients, age and pathology level. Second, relatively small sample size limits the validity of the drawn solid conclusions. The global sagittal alignment assessment is restricted to the parameters chosen, given that other parameters such as the sagittal vertical axis, pelvic index, pelvic tilt and sacrum slope were not accounted for. Third, this study also focuses on short-term outcomes, with no long-term radiological follow-up to confirm whether the results were sustained.
Conclusion
PELIF could achieve equivalent clinical and radiographic outcomes compared with OLIF when the spondylolisthesis is mild. Furthermore, PELIF enables solid lumbar interbody fusion with minimal iatrogenic damage and avoidance of general anesthesia, which may enhance the recovery of patients with high expectations or old patients with concomitant diseases. It seems that PELIF could be considered as acceptable surgical option for the treatment of symptomatic low-grade lumbar spondylolisthesis.
•
This was the first comparative study concerning the surgical outcomes between percutaneous endoscopic-assisted lumbar interbody fusion (PELIF) and oblique lumbar interbody fusion (OLIF).
•
The PELIF could be manipulated without general anesthesia.
•
Extremely less iatrogenic damage of PELIF enhanced the recovery of patients.
•
The PELIF might be friendly to patients with severe concomitant diseases.
•
When compared with OLIF technique, the PELIF exhibited superiority in the enlargement of foraminal width, but inferiority in the improvement of foraminal height.
•
The functional outcomes were almost equivalent in both PELIF and OLIF technique.
•
Satisfactory bone fusion could be obtained by PELIF technique.
•
The PELIF might be a promising surgical alternative to the treatment of symptomatic mild spondylolisthesis.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Author contributions
M Jin and T Shen conceived the study design and performed the manuscript drafting. T Zhao, Jun Zhang, H Shao and J Liu contributed toward the interpretation and the collection of the data. Y Huang and G Xu were responsible for the supervision and critical revision of the manuscript. All authors have read and approved the final manuscript.
Acknowledgments
We appreciate the contribution of all patients, their families, the investigators and the medical staff. We are grateful to all authors.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Data sharing statement
The data used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical conduct of research
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Supplementary Material
References
1.
Kalichman L, Kim DH, Li L, Guermazi A, Berkin V, Hunter DJ. Spondylolysis and spondylolisthesis: prevalence and association with low back pain in the adult community-based population. Spine (Phila PA 1976) 34(2), 199–205 (2009).
2.
Seng C, Siddiqui MA, Wong KP et al. Five-year outcomes of minimally invasive versus open transforaminal lumbar interbody fusion: a matched-pair comparison study. Spine (Phila PA 1976) 38(23), 2049–2055 (2013).
3.
Zigler J, Ferko N, Cameron C, Patel L. Comparison of therapies in lumbar degenerative disc disease: a network meta-analysis of randomized controlled trials. J. Comp. Eff. Res. 7(3), 233–246 (2018).
4.
Lu VM, Kerezoudis P, Gilder HE, Mccutcheon BA, Phan K, Bydon M. Minimally invasive surgery versus open surgery spinal fusion for spondylolisthesis: a systematic review and meta-analysis. Spine (Phila PA 1976) 42(3), E177–E185 (2017).
5.
Alimi M, Hofstetter CP, Pyo SY, Paulo D, Hartl R. Minimally invasive laminectomy for lumbar spinal stenosis in patients with and without preoperative spondylolisthesis: clinical outcome and reoperation rates. J. Neurosurg. Spine 22(4), 339–352 (2015).
6.
Mummaneni PV, Bisson EF, Kerezoudis P et al. Minimally invasive versus open fusion for Grade I degenerative lumbar spondylolisthesis: analysis of the Quality Outcomes Database. Neurosurg. Focus 43(2), E11 (2017).
7.
Silvestre C, Mac-Thiong JM, Hilmi R, Roussouly P. Complications and morbidities of mini-open anterior retroperitoneal lumbar interbody fusion: oblique lumbar interbody fusion in 179 patients. Asian Spine J. 6(2), 89–97 (2012).
8.
Sheng SR, Geng YB, Zhou KL, Wu AM, Wang XY, Ni WF. Minimally invasive surgery for degenerative spondylolisthesis: transforaminal or oblique lumbar interbody fusion. J. Comp. Eff. Res. 9(1), 45–51 (2020).
9.
Abe K, Orita S, Mannoji C et al. Perioperative complications in 155 patients who underwent oblique lateral interbody fusion surgery: perspectives and indications from a retrospective, multicenter survey. Spine (Phila PA 1976) 42(1), 55–62 (2017).
10.
Woods KR, Billys JB, Hynes RA. Technical description of oblique lateral interbody fusion at L1-L5 (OLIF25) and at L5-S1 (OLIF51) and evaluation of complication and fusion rates. Spine J. 17(4), 545–553 (2017).
11.
Osman SG. Endoscopic transforaminal decompression, interbody fusion, and percutaneous pedicle screw implantation of the lumbar spine: a case series report. Int. J. Spine Surg. 6, 157–166 (2012).
12.
Jacquot F, Gastambide D. Percutaneous endoscopic transforaminal lumbar interbody fusion: is it worth it? Int. Orthop. 37(8), 1507–1510 (2013).
13.
Wang MY, Grossman J. Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: initial clinical experience with 1-year follow-up. Neurosurg. Focus 40(2), E13 (2016).
14.
Zhu G, Hao Y, Yu L, Cai Y, Yang X. Comparing stand-alone oblique lumbar interbody fusion with posterior lumbar interbody fusion for revision of rostral adjacent segment disease: a STROBE-compliant study. Medicine (Baltimore) 97(40), e12680 (2018).
15.
Alvi MA, Sebai A, Yolcu Y et al. Assessing the differences in measurement of degree of spondylolisthesis between supine MRI and erect x-ray: an institutional analysis of 255 cases. Oper. Neurosurg. (Hagerstown) 18(4), 438–443 (2019).
16.
Jin J, Ryu KS, Hur JW, Seong JH, Kim JS, Cho HJ. Comparative study of the difference of perioperative complication and radiologic results: MIS-DLIF (minimally invasive direct lateral lumbar interbody fusion) versus MIS-OLIF (minimally invasive oblique lateral lumbar interbody fusion). Clin. Spine Surg. 31(1), 31–36 (2018).
17.
Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila PA 1976) 26(17), 1873–1878 (2001).
18.
Choudhri TF, Mummaneni PV, Dhall SS et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 4: radiographic assessment of fusion status. J. Neurosurg. Spine 21(1), 23–30 (2014).
19.
Martin CR, Gruszczynski AT, Braunsfurth HA, Fallatah SM, O'Neil J, Wai EK. The surgical management of degenerative lumbar spondylolisthesis: a systematic review. Spine 32(16), 1791–1798 (2007).
20.
Abdu WA, Lurie JD, Spratt KF et al. Degenerative spondylolisthesis: does fusion method influence outcome? Four-year results of the spine patient outcomes research trial (SPORT). Spine 34(21), 2351 (2009).
21.
Tay KS, Bassi A, Yeo W, Yue WM. Intraoperative reduction does not result in better outcomes in low-grade lumbar spondylolisthesis with neurogenic symptoms after minimally invasive transforaminal lumbar interbody fusion–a 5-year follow-up study. Spine J. 16(2), 182–190 (2016).
22.
Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 1(1), 2 (2015).
23.
Ohtori S, Orita S, Yamauchi K et al. Mini-open anterior retroperitoneal lumbar interbody fusion: oblique lateral interbody fusion for lumbar spinal degeneration disease. Yonsei Med. J. 56(4), 1051–1059 (2015).
24.
Youn MS, Shin JK, Goh TS, Lee JS. Full endoscopic lumbar interbody fusion (FELIF): technical note. Eur. Spine J. 27(8), 1949–1955 (2018).
25.
Wu J, Liu H, Ao S et al. Percutaneous endoscopic lumbar interbody fusion: technical note and preliminary clinical experience with 2-year follow-up. Biomed. Res. Int. 2018, 5806037 (2018).
26.
Videbaek TS, Bunger CE, Henriksen M, Neils E, Christensen FB. Sagittal spinal balance after lumbar spinal fusion: the impact of anterior column support results from a randomized clinical trial with an eight-to thirteen-year radiographic follow-up. Spine 36(3), 183–191 (2011).
27.
Castellvi AE, Nienke TW, Marulanda GA, Murtagh RD, Santoni BG. Indirect decompression of lumbar stenosis with transpsoas interbody cages and percutaneous posterior instrumentation. Clin. Orthopaed. Rel. Res. 472(6), 1784–1791 (2014).
28.
Lee SH, Erken HY, Bae J. Percutaneous transforaminal endoscopic lumbar interbody fusion: clinical and radiological results of mean 46-month follow-up. Biomed. Res. Int. 2017, 3731983 (2017).
29.
Isaacs RE, Sembrano JN, Tohmeh AG. Two-year comparative outcomes of MIS lateral and MIS transforaminal interbody fusion in the treatment of degenerative spondylolisthesis: Part II: radiographic findings. Spine (Phila PA 1976) 41(Suppl. 8), S133–S144 (2016).
30.
Ahn Y, Kim WK, Son S, Lee SG, Jeong YM, Im T. Radiographic assessment on magnetic resonance imaging after percutaneous endoscopic lumbar foraminotomy. Neurol. Med. Chir. (Tokyo) 57(12), 649–657 (2017).
31.
Champagne P-O, Walsh C, Diabira J et al. Sagittal balance correction following lumbar interbody fusion: a comparison of the three approaches. Asian Spine J. 13(3), 450–458 (2019).
32.
Lin G-X, Akbary K, Kotheeranurak V et al. Clinical and radiologic outcomes of direct versus indirect decompression with lumbar interbody fusion: a matched-pair comparison analysis. World Neurosurg. 119, e898–e909 (2018).
33.
Ostelo RW, De Vet HC. Clinically important outcomes in low back pain. Best. Pract. Res. Clin. Rheumatol. 19(4), 593–607 (2005).
34.
Li HM, Zhang RJ, Shen CL. Radiographic and clinical outcomes of oblique lateral interbody fusion versus minimally invasive transforaminal lumbar interbody fusion for degenerative lumbar disease. World Neurosurg. 122, e627–e638 (2019).
Information & Authors
Information
Published In
Pages: 639 - 650
PubMed: 32551889
Copyright
© 2020 Future Medicine Ltd.
History
Received: 8 February 2020
Accepted: 16 April 2020
Published online: 18 June 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Minimally invasive surgery for low-grade spondylolisthesis: percutaneous endoscopic or oblique lumbar interbody fusion. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0022
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Miguel de Pedro Abascal, Teresa Bas, Paloma Bas, Ghassan Elgeadi Saleh, Alberto Caballero García, Joint Halley Guimbard Perez, Amparo Ortega Yago, Miguel Ángel Castillo Soriano, Endoscopic Spine Surgery vs. Conventional Approaches for Lumbar Spondylolisthesis: Systematic Review and Meta-Analysis, Journal of Clinical Medicine, 10.3390/jcm15124751, 15, 12, (4751), (2026).
- Katsuhisa Yamada, Ken Nagahama, Hisataka Suzuki, Yuichiro Abe, Shigeto Hiratsuka, Yohei Sodeyama, Daisuke Ukeba, Hiroyuki Tachi, Tsutomu Endo, Takashi Ohnishi, Yuichi Hasegawa, Hideki Sudo, Takahiko Hyakumachi, Norimasa Iwasaki, Comparative Study between Full-Endoscopic Transforaminal Approach Lumbar Interbody Fusion (TF-LIF) Using PETLIF System and Minimally Invasive TLIF for Degenerative Lumbar Spine Disorders, Spine Surgery and Related Research, 10.22603/ssrr.2024-0254, 9, 4, (460-468), (2025).
- Xijian Hu, Lei Yan, Jing Chai, Xiaofeng Zhao, Haifeng Liu, Jinhuai Zhu, Huo Chai, Yibo Zhao, Bin Zhao, Comparison of the Outcomes of Endoscopic Posterolateral Interbody Fusion and Lateral Interbody Fusion in the Treatment of Lumbar Degenerative Disease: A Systematic Review and Network Meta‐Analysis, Orthopaedic Surgery, 10.1111/os.14371, 17, 5, (1287-1297), (2025).
- Wenhao Zhao, Chuanli Zhou, Hao Zhang, Jianwei Guo, Jialuo Han, Antao Lin, Yan Wang, Xuexiao Ma, Clinical, Radiographic and Fusion Comparison of Oblique Lumbar Interbody Fusion (OLIF) stand-alone and OLIF with posterior pedicle screw fixation in patients with degenerative spondylolisthesis, BMC Musculoskeletal Disorders, 10.1186/s12891-023-06985-8, 24, 1, (2023).
- Koichiro Ono, Daisuke Fukuhara, Ken Nagahama, Yuichiro Abe, Kenji Takahashi, Tokifumi Majima, Percutaneous Endoscopic Transforaminal Lumbar Interbody Fusion (PETLIF): Current Techniques, Clinical Outcomes, and Narrative Review, Journal of Clinical Medicine, 10.3390/jcm12165391, 12, 16, (5391), (2023).
- Xu Shen, Yu-cheng Gao, Pei Zhang, Peng Song, Zan-li Jiang, Feng Wang, Wen-bin Xuan, Zeng-xin Gao, Is unilateral-approach full-endoscopic lumbar fusion effective for single-level lumbar spondylolisthesis with bilateral symptoms? A preliminary report of 43 CT analysis, European Spine Journal, 10.1007/s00586-023-07667-8, 33, 2, (409-416), (2023).
- Huan Ma, Fanyi Zhang, Qijie Ying, Baoze Pan, Yuting Li, Hongping Ge, Yu Cao, Tingfei Jiang, Meifen Dai, Conghua Ji, Long‐Term Clinical and Imaging Results of Oblique Lateral Interbody Fusion for Degenerative Lumbar Spondylolisthesis: A Systematic Review and Meta‐Analysis, Orthopaedic Surgery, 10.1111/os.13588, 15, 2, (400-412), (2022).