Health benefits and economic advantages associated with increased utilization of a smoking cessation program
Publication: Journal of Comparative Effectiveness Research
Abstract
Rationale, aim & objective: The goal of this study was to examine the health and economic impacts related to increased utilization of the Duke Smoking Cessation Program resulting from the addition of two relatively new referral methods – Best Practice Advisory and Population Outreach. Materials & methods: In a companion paper ‘Comparison of Referral Methods into a Smoking Cessation Program’, we report results from a retrospective, observational, comparative effectiveness study comparing the impact of three referral methods – Traditional Referral, Best Practice Advisory and Population Outreach on utilization of the Duke Smoking Cessation Program. In this paper we take the next step in this comparative assessment by developing a Markov model to estimate the improvement in health and economic outcomes when two referral methods – Best Practice Advisory and Population Outreach – are added to Traditional Referral. Data used in this analysis were collected from Duke Primary Care and Disadvantaged Care clinics over a 1-year period (1 October 2017–30 September 2018). Results: The addition of two new referral methods – Best Practice Advisory and Population Outreach – to Traditional Referral increased the utilization of the Duke Smoking Cessation Program in Primary Care clinics from 129 to 329 smokers and in Disadvantaged Care clinics from 206 to 401 smokers. The addition of these referral methods was estimated to result in 967 life-years gained, 408 discounted quality-adjusted life-years saved and total discounted lifetime direct healthcare cost savings of US$46,376,285. Conclusion: Health systems may achieve increased patient health and decreased healthcare costs by adding Best Practice Advisory and Population Outreach strategies to refer patients to smoking cessation services.
The impact of smoking
Smoking is the leading preventable cause of morbidity and mortality in the USA [1]. Smoking causes approximately 480,000 deaths per year [2] and 28.6% of all cancer deaths [3]. Smoking has been shown to cause lung disease, heart disease, peripheral vascular disease, stroke, thromboembolic disease, diabetes, bone fractures, cataracts, dementia and developmental disorders, [4] and in the USA, smoking incurs a financial burden of over US$300 billion per year [5]. As evidence mounts on the health and financial costs of smoking, there is an urgent need to provide smokers with access to effective tobacco use treatment.
Changes in the smoking population
The rate of smoking in the USA has decreased from 43% in 1964 [6] to 15.7% today [7]. With this decreased rate in smoking, there has been a change in the demographics of those who smoke. On average, smokers today have relatively low education, [8] low income [9] and high rates of psychiatric illness [10,11]. Each of these challenges makes it less likely that a smoker will be successful when trying to quit [12–14]. When today’s average smoker makes an unassisted quit attempt, their success rate in quitting is only 3–5% [15].
Changes in healthcare
With these changes in the smoking population, there has also been a change in the nature of healthcare. Fifty years ago, most healthcare in the USA was provided by general practitioners working in small practices with minimal cohesion or integration [16]. Today, 91.2% of Americans receive care within a health system, [17,18] and these health systems adhere to specific patient care objectives and communicate preferred treatment pathways to health system providers [19]. A widely recognized health system objective is the provision of effective smoking cessation services to health system patients [20].
The key evolutionary transition is that referral to smoking cessation services is no longer driven solely at an individual patient level by medical providers. Rather it is driven at a population level by health system objectives [20–22]. In 2014, the CDC published ‘Best Practices for Comprehensive Tobacco Control Programs’ with recommendations for all healthcare systems, clinics, hospitals, dental offices, pharmacies and emergency departments to ask, advise and refer patients to evidence-based tobacco treatment [21,22]. Each year, 80% of all smokers see a medical provider [23] and each of these contacts is an opportunity to provide treatment or referral to evidence-based tobacco treatment services. Smoking abstinence rates for specialized treatment programs (e.g., Mayo Clinic, MD Anderson, Duke) are in the range of 27–39% – nine- to ten-times that of an unassisted quit attempt [24–26].
Emergence of the electronic health record
One of the most significant changes in healthcare in the last 20 years has been the wide-scale proliferation of the electronic health record (EHR) [27]. In 2007, only 35% of office-based physicians used an EHR; by 2015, EHR use increased to 90% in clinics [28] and 96% in hospitals [29]. This means that a large majority of US smokers who have seen a physician are registered within an EHR [23]. Furthermore, in many health systems, smoking status is recognized as a vital sign, [30] such that providers are required to obtain smoking status on every patient over the age of 13 [31]. Although imperfect, [32] the EHR has become an effective tool for identification of smokers within a health system.
Patient referral methods
In this paper and in our companion paper, ‘Comparison of Referral Methods into a Smoking Cessation Program’, we assess the effects of three referral methods – Traditional Referral, Best Practice Advisory (BPA) and Population Outreach. Traditional Referral is an informal term used for our purposes here to denote the default method of patient referral used by providers everywhere for hundreds of years; it refers to the general situation in which a provider sees a patient and then, for a multitude of potential reasons, sends the patient to be seen by another provider. A key concept underlying Traditional Referral is that it is motivated and initiated by the medical provider who sees the patient. BPA and Population Outreach are categorically different from Traditional Referral because they are not solely driven by the medical provider, but instead are driven in part or whole by health system objectives. BPA refers to a referral method in which the EHR alerts the provider during a clinic visit that their patient may benefit from a specific treatment [33]. At selected Duke clinics, a BPA alert occurs during a clinic visit if the EHR recognizes the patient as current smoker. There were limited data describing the incidence of BPA use in the USA, but at least 90% of US physicians use an EHR, [28] and alerts are a common component of the EHR [34]. Population Outreach is a referral method in which a ‘pursuit list’ is generated containing all patients across a population who meet a specified set of criteria. These patients are then contacted proactively by phone, text, email, mail or other methods and offered services [35]. In the Duke Smoking Cessation Program (DSCP), Population Outreach occurs by running a pursuit list that includes all current smokers who have a medical appointment within the next 30 days. DSCP staff then calls these patients on the phone and offers them DSCP services. To our knowledge, at the time of this study, there are only a small number of health systems that utilize Direct Outreach to refer patients to smoking cessation services [36,37].
Sample population
Our companion paper reported utilization of DSCP services at Primary Care, Disadvantaged Care, Pulmonology, Infectious Disease and Cancer Care clinical sites. The analysis in this current paper was limited to Primary Care and Disadvantaged Care clinics because patients in our other clinics with chronic obstructive pulmonary disorder, HIV and cancer showed high morbidity and mortality and did not easily generalize to the wider population (unpublished data, 2019). Duke Primary Care clinics are staffed by Family Practice or Internal Medicine physicians and provide a medical home where patients receive routine care and referrals to services when needed. Disadvantaged Care refers to a type of primary care clinic that provides additional services to assist people with financial challenges. The majority of DSCP patients in the Duke Disadvantaged Care clinics report an annual income of under US$10,000 per year.
Materials & methods
Objective
The goal described in our companion paper ‘Comparison of Referral Methods into a Smoking Cessation Program’ was to compare three referral methods (Traditional Referral, BPA and Population Outreach) on utilization of DSCP services. In this study, we took the next step and assessed the economic and health outcomes of increased program utilization that occurred when BPA and Population Outreach were added to Traditional Referral. Data collection occurred over a 1-year period between 1 October 2017 and 30 September 2018. This was a retrospective, observational, comparative effectiveness study and, as such, patients were not randomized. Instead, data collection occurred within a natural treatment environment, with the goal that outcomes might reflect real-world practice.
Model development methods
We developed Markov models designed to estimate population changes over time and integrate information from multiple sources including prospective and retrospective data and information from the literature [38]. Our methodology was guided by the recommendations of the two Panels on Cost–Effectiveness in Health and Medicine [39,40]. The Markov models simulated yearly transitions in current smoking, smoking abstinence, smoking relapse and smoking-related and all-cause mortalities of adult smokers (Figure 1). Costs were assessed from the medical provider’s perspective. Because many of the model parameters differ by gender, separate models were developed for males and females. Also, because recruitment rates and treatment methods differed by clinic type, separate models were developed for Primary Care and Disadvantaged Care clinic patients. The model parameters were derived from analysis of DSCP clinic data or from the most current literature available. Table 1 provides details on Markov model parameters.
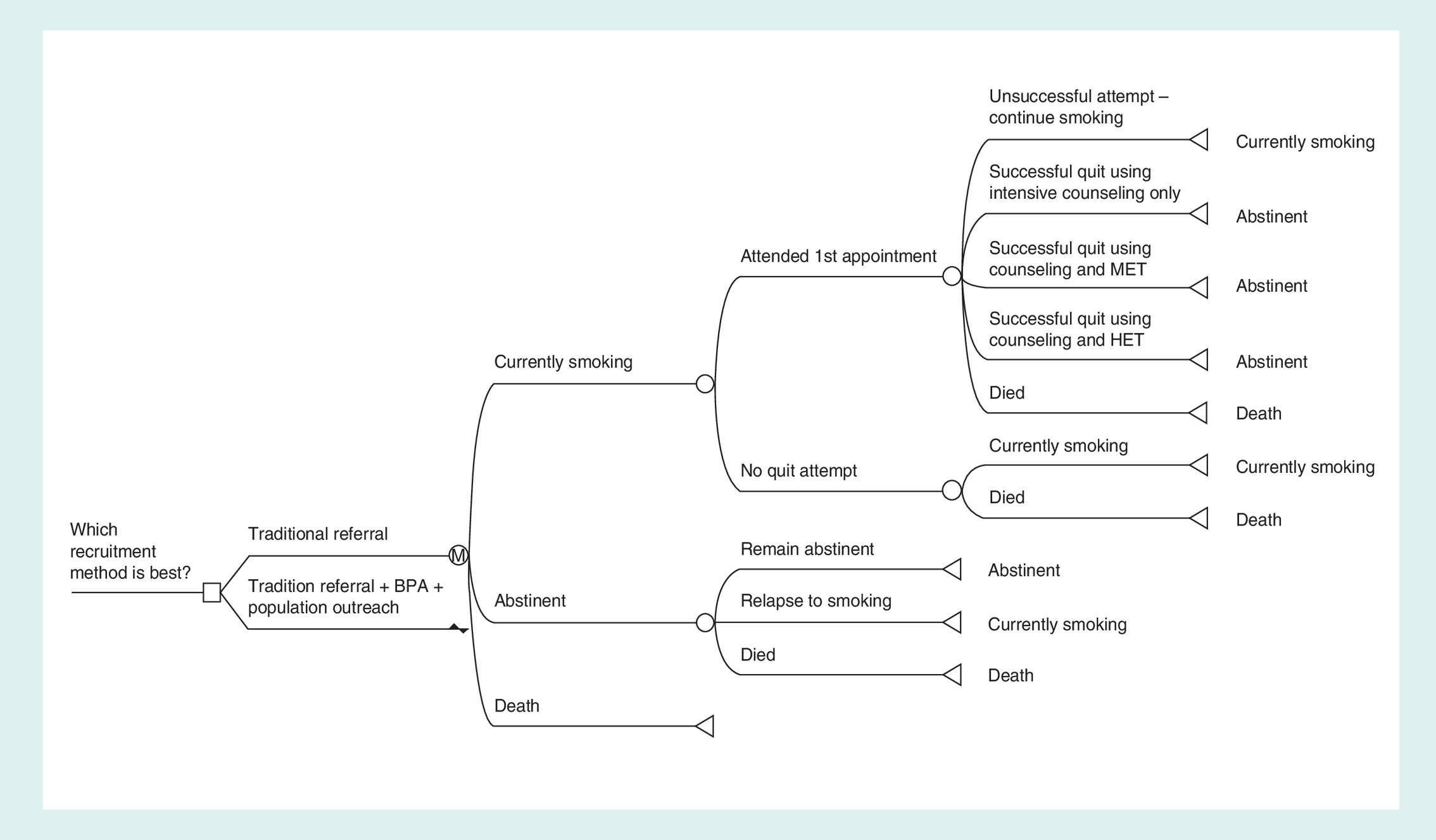
Figure 1. Markov model diagram.
MET: nicotine replacement monotherapy (patch, gum, lozenge, spray, inhaler) or bupropion; HET: varenicline or combination nicotine replacement therapy.
BPA: Best Practice Advisory; HET: Highly effective treatment; MET: Moderately effective treatment.
| Parameter | Values | Ref. | |
|---|---|---|---|
| 1st appointment attendance | Primary care | Disadvantaged care | [41] |
| – Traditional | 4.6% | 7.4% | |
| – BPA | 0.8% | 0.7% | |
| – Population-based | 6.3% | 6.3% | |
| Quit attempt method proportions | [41] | ||
| – Behavioral counseling | 6% | 5% | |
| – Moderately effective treatment† | 6% | 20% | |
| – Highly effective treatment‡ | 88% | 75% | |
| Acquisition cost (US$) | [42] | ||
| – Behavioral counseling | 71 | ||
| – Moderately effective treatment | 320 | ||
| – Highly effective treatment | 932 | ||
| Dispensing cost (US$) | [43] | ||
| – Triangular§ | 2,970, 20 | ||
| Annual quit rates | [44–49] | ||
| – Unassisted | 4.3% | ||
| – Behavioral counseling | RR = 1.57 (95% CI, 1.40–1.77) | ||
| – Moderately effective treatment | RR = 1.61 (95% CI, 1.49–1.76) | ||
| – Highly effective treatment | RR = 2.27 (95% CI, 2.02–2.55) | ||
| Annual relapse rates | [50,51] | ||
| – Year 1 | 0.10 (95% CI: 0.05–0.17) | ||
| – Years 2–5 | 0.063 | ||
| – Years 6–10 | 0.020 | ||
| – Years 10+ | 0.010 | ||
| Mortality hazard ratios¶ | Smoking | Abstinent | [44] |
| – Female, age 18–23 | 1.185 | 1.105 | |
| – Female, age 24–54 | 1.369 | 1.214 | |
| – Female, age 55–74 | 2.533 | 1.666 | |
| – Female, age 75+ | 1.411 | 1.111 | |
| – Male, age 18–23 | 1.743 | 1.037 | |
| – Male, age 24–54 | 2.486 | 1.074 | |
| – Male, age 55–74 | 2.55 | 1.992 | |
| – Male, age 75+ | 1.326 | 1.074 | |
| – COPD multiplier | 2.14 | 2.0 | |
| Medical care costs (US$) | [52] | ||
| – Female, age 18–34 | 262 | 51 | |
| – Female, age 35–54 | 1503 | 192 | |
| – Female, age 55–64 | 4285 | 1191 | |
| – Female, age 65–74 | 8931 | 2781 | |
| – Female, age 75+ | 17,253 | 4906 | |
| – Male, age 18–34 | 318 | 102 | |
| – Male, age 35–54 | 1601 | 402 | |
| – Male, age 55–64 | 5415 | 1443 | |
| – Male, age 65–74 | 10,924 | 3117 | |
| – Male, age 75+ | 17,896 | 5192 | |
| Utility weights | [53] | ||
| – Female, age 18–24 | 0.8952 | 0.9084 | |
| – Female, age 25–34 | 0.8835 | 0.8988 | |
| – Female, age 35–44 | 0.8716 | 0.8872 | |
| – Female, age 45–54 | 0.8317 | 0.8479 | |
| – Female, age 55–64 | 0.7648 | 0.7827 | |
| – Male, age 18–24 | 0.9211 | 0.9342 | |
| – Male, age 25–34 | 0.9166 | 0.9306 | |
| – Male, age 35–44 | 0.8899 | 0.9058 | |
| – Male, age 45–54 | 0.8422 | 0.8596 | |
| – Male, age 55–64 | 0.7815 | 0.802 | |
| Discount rate | 3% (range 0–8%) | [39] | |
†
Moderately effective treatments include nicotine replacement monotherapy (patch, gum, lozenge, spray and inhaler) or bupropion.
‡
Highly effective treatments are varenicline or combination NRT.
§
For triangular distributions, the three values represent the minimum, most likely and maximum of the range of parameter values.
¶
Because mortality hazard ratios were not available for age group 18–23, we assumed that they were half that of the 24–54 age group.
BPA: Best Practice Advisory; NRT: Nicotine replacement therapy; RR: Relative risk.
Markov model health states
We analyzed data stratified by clinic type and recruitment method to determine the proportion of patients who attended their first appointment. Those who made a quit attempt transitioned between three health states – ‘currently smoking’, ‘abstinent’ and ‘death’. All individuals began in the health state defined as ‘currently smoking’. During each one-year cycle, a smoker may or may not have made a quit attempt; if they did make a quit attempt and they were successful, they transitioned to the ‘abstinent’ health state. Those who transitioned to the ‘abstinent’ health state remained in this state unless they relapsed. If they relapsed, they transitioned back to the ‘currently smoking’ health state where they, again, may or may not make a quit attempt the following year. The final health state, ‘death’, was the absorbing health state. Those in the ‘currently smoking’ or ‘abstinent’ health state may transition to the ‘death’ health state at various rates depending on smoking status, age and gender [44].
Smoking cessation abstinence rates
The probability of transitioning from the ‘currently smoking’ state to the ‘abstinent’ state depended on the method used to quit smoking. In the DSCP, all smokers who attended a visit received intensive behavioral counseling and most but not all received pharmacotherapy. Quit attempts then fell into three categories, each with an associated abstinence rate: counseling only; counseling plus moderately effective medication treatment (nicotine replacement monotherapy (patch, gum, lozenge, spray, inhaler) or bupropion and; counseling plus highly effective medication treatment (varenicline or combination nicotine replacement), as defined by Cochrane Reviews [45,46,54]. The probability of a successful quit attempt was derived by applying hazard ratio multipliers provided in Cochrane Reviews [45,46,54] to an unassisted smoking abstinence rate of 4.3% [44]. The proportion of quit attempts using each of these three approaches was then derived using clinic-level data on medication use by DSCP patients.
Relapse rate
After quitting, there was a risk of relapsing back to the ‘currently smoking’ health state. We modeled risk of relapse as a function of time based on relapse survival curves in which the risk of relapse decreases over time [50]. While relapse rates differ by intervention in the short term (<1 year), these differences do not significantly predict long-term relapse. Thus, relapse rate was modeled as a distribution during the first year [50] and as point estimates thereafter [51].
Costs
Most health systems now use an EHR and alerts such as BPA are common, [28,34] such that implementing BPA-based referral constitutes a one-time, relatively small fixed cost. Because of this, these technology costs of BPA development were not included in the analysis. To estimate cost of wages, we observed that patient treatment within the DSCP required an average of 30 min with a distribution of 5–45 min depending on patient complexity. To account for this, a per minute wage rate for DSCP medical providers, including fringe benefits, was applied to visit time. Smoking cessation pharmacotherapy costs were calculated to include the medication acquisition plus the cost of dispensing, which covers a pharmacy’s operating costs. We derived medication acquisition costs from the US federal government’s Federal Supply Schedule, available from the Veterans Administration’s Pharmacy Benefits Management agency [55]. Because each medication treatment can have varying regimens, we used mean dosing and treatment length for medication acquisition cost. For dispensing cost, we used a distribution of reimbursement rates for dispensing cost paid by state Medicaid programs [56]. To estimate the cost of smoking cessation counseling, we referenced Medicare reimbursement codes used within the DSCP (CPT 99407 and 99406) [57]. Finally, we incorporated the medical care costs incurred by current smokers and former smokers [52]. Medical care costs for current smokers are highest, followed by former smokers, followed by never smokers.
Life expectancy & quality-adjusted life-years gained
To calculate life expectancy, simulated smokers accrued a value of 1 while in all health states other than ‘death’. Life expectancy estimates were not discounted. Because former smokers enjoy a higher quality of life than current smokers, we also calculated quality-adjusted life-years (QALYs) gained, weighting life expectancy by age-, gender- and smoking status-stratified utility weights [53].
Model simulations
Markov modeling was conducted using the simulation software TreeAge Pro 2018. Probabilistic sensitivity analysis via 10,000 iterations of second-order Monte Carlo simulation was used to derive mean cost, life expectancy and QALY estimates, as well as respective 95% CIs [38]. The CIs were compared for overlap to determine statistical significance of group mean differences. Costs and QALYs were discounted at 3%, as recommended by the Panel [58]. For each iteration, quit attempts began at the mean age of the patients seen at each clinic and continued annually until the patient died or until they reached age 100. At last, we conducted one-way sensitivity analyses to assess the robustness of the impacts each model parameter had on results. This was conducted using the tornado diagram feature of TreeAge Pro. For each parameter, cost and effectiveness were calculated for each value in the respective range of values. The range of cost and effectiveness results estimated by the range of values for each parameter were compared with each other to determine which parameters had the greatest impact on the results as well as at which parameter values the results were no longer cost saving or cost effective. For those parameters, where a range was not provided in the literature, a range was created by using ±25% of the point estimate.
Results
Program utilization
During the 1-year data collection period, there were 2816 smokers seen for primary care services within the two Primary Care clinics. Among these, 4.6% attended a DSCP appointment via Traditional Referral and 0.8% via BPA. During this period, there were 2789 smokers seen within the two Disadvantaged Care clinics. Among these, 7.4% attended an appointment via Traditional Referral and an additional 0.7% via BPA. As discussed in our companion paper, Population Outreach was pilot tested and showed an increase in DSCP utilization of 6.3%. Combining all three referral methods, DSCP utilization was 11.7% in Primary Care and 14.4% in Disadvantaged Care clinics. The mean age of smokers seen was 57 in Primary Care and 55 in Disadvantaged Care clinics. Highly effective pharmacotherapy was provided to 88% of Primary Care and 75% of Disadvantaged Care patients. Moderately effective pharmacotherapy was given to 6% of Primary Care and 20% of Disadvantaged Care patients. Behavioral counseling alone was provided to 6% of Primary Care and 5% of Disadvantaged Care patients.
Quality-adjusted life-years
Using Markov modeling, the increase in DSCP utilization resulted in an improvement in health outcomes and a decrease in medical costs. Across both clinic types and sex, the addition of new referral methods – BPA and Population Outreach – to Traditional Referral resulted in per person QALY gains of 0.07–0.08 (26–28 QA days; QALY results in Table 2). In Primary Care clinics, males gained 98 QALYs and females gained 103 QALYs. In Disadvantaged Care clinics, males gained 79 QALYs and females gained 128 QALYs. Among the 5605 smokers seen in the two Primary Care and two Disadvantaged Care clinics, the addition of BPA and Population Outreach to Traditional Referral was associated with 27 quality-adjusted days per person and 408 QALYs gained.
| Clinic type (smokers seen) | Recruitment method | |||||
|---|---|---|---|---|---|---|
| Traditional | Traditional + EHR | QALYS gained | ||||
| Per person | Total | Per person | Total | Per person (QA days) | Total | |
| Males | ||||||
| – Primary Care (n = 1408) | 10.41 | 14,655 | 10.48 | 14,753 | 0.07 (26) | 98 |
| – Disadvantaged Care (n = 1171) | 10.94 | 12,814 | 11.01 | 12,893 | 0.07 (25) | 79 |
| – Male subtotal | 10.65 | 27,469 | 10.72 | 27,647 | 0.07 (26) | 177 |
| Females | ||||||
| – Primary Care (n = 1408) | 11.49 | 16,168 | 11.56 | 16,271 | 0.07 (27) | 103 |
| – Disadvantaged Care (n = 1618) | 12.07 | 19,528 | 12.15 | 19,656 | 0.08 (29) | 128 |
| – Female subtotal | 11.80 | 35,696 | 11.88 | 35,926 | 0.08 (28) | 231 |
| – Total (N = 5605) | 11.27 | 63,165 | 11.34 | 63,573 | 0.07 (27) | 408 |
All of the QALYs gained are statistically significant at α ≤0.05.
EHR: Electronic health record; QALY: Quality-adjusted life-year.
Life expectancy
Life-years remaining are presented in Table 3 with removal of utility weights. Analysis showed that the addition of BPA and Population Outreach referral methods to Traditional Referral was associated with male smokers attending either clinic types gaining a mean of 0.15 years (55 days) of life. Among men, the addition of BPA and Population Outreach to Traditional Referral led to a total of 211 years gained for Primary Care smokers and 177 years gained for Disadvantaged Care smokers.
| Clinic type (smokers seen) | Recruitment method | |||||
|---|---|---|---|---|---|---|
| Traditional | Traditional + EHR | LYs gained | ||||
| Per person | Total | Per person | Total | Per person (days) | Total | |
| Males | ||||||
| – Primary Care (n = 1408) | 19.67 | 27,680 | 19.82 | 27,891 | 0.15 (55) | 211 |
| – Disadvantaged Care (n = 1171) | 20.91 | 24,496 | 21.06 | 24,670 | 0.15 (55) | 174 |
| – Male subtotal | 20.23 | 52,176 | 20.38 | 52,561 | 0.15 (55) | 385 |
| Females | ||||||
| – Primary Care (n = 1408) | 23.07 | 32,470 | 23.25 | 32,727 | 0.18 (67) | 257 |
| – Disadvantaged Care (n = 1618) | 24.59 | 39,777 | 24.79 | 40,102 | 0.20 (73) | 325 |
| – Female subtotal | 23.88 | 72,247 | 24.07 | 72,829 | 0.19 (69) | 582 |
| Total (N = 5605) | 22.20 | 124,423 | 22.38 | 125,391 | 0.18 (67) | 967 |
All of the life-years gained are statistically significant at α ≤0.05.
EHR: Electronic health record; LY: Life-year.
Female smokers in Primary Care clinics gained 0.18 years (67 days) of life and 0.20 years (73 days) of life in Disadvantaged Care clinics. Female Primary Care smokers gained 257 years and female Disadvantaged Care smokers gained 325 total years. Among the 5605 smokers seen in the Primary and Disadvantaged Care clinics, there was a gain of 967 years of life expectancy or 67 days per person.
Healthcare costs
Lifetime direct healthcare costs are provided in Table 4. The key findings are that Traditional Referral plus EHR-based referral led to total lifetime healthcare cost savings of US$11,396,528 among male Primary Care clinic smokers or US$8097 per male smoker. Among males in Disadvantaged Care clinics, the total and per person savings were US$8,957,543 and 7647, respectively. Among female smokers utilizing the Primary Care clinics, the total lifetime healthcare cost savings were US$11,868,040 or 8432 per female smoker. Disadvantaged Care clinic female smokers accrued a lifetime healthcare cost savings of US$14,154,175 or 8750 per person. Among smokers in both clinics, the addition of BPA and Patient Outreach to Traditional Referral led to an estimated savings of US$8,276 per smoker and a total of US$46,376,285.
| Clinic type (by gender) | Recruitment method | |||||
|---|---|---|---|---|---|---|
| Traditional | Traditional + EHR | Cost savings | ||||
| Per person (US$) | Total (US$) | Per person (US$) | Total (US$) | Per person (US$) | Total (US$) | |
| Males | ||||||
| Primary Care (n = 1408) | 166,145 | 233,849,088 | 158,048 | 222,452,560 | 8097 | 11,396,528 |
| Disadvantaged Care (n = 1171) | 158,135 | 185,236,176 | 150,488 | 176,278,633 | 7647 | 8,957,543 |
| Male subtotal | 162,507 | 419,085,264 | 154,614 | 398,731,193 | 7892 | 20,354,071 |
| Females | ||||||
| Primary Care (n = 1408) | 173,878 | 244,733,285 | 165,446 | 232,865,245 | 8432 | 11,868,040 |
| Disadvantaged Care (n = 1618) | 165,062 | 267,007,592 | 156,312 | 252,853,417 | 8750 | 14,154,175 |
| Female subtotal | 169,164 | 511,740,877 | 160,562 | 485,718,662 | 8602 | 26,022,215 |
| Total (N = 5605) | 166,100 | 930,826,141 | 157,825 | 884,449,856 | 8276 | 46,376,285 |
All of the above cost savings are statistically significant at α≤ 0.05.
EHR: Electronic health record.
Sensitivity analyses
The parameter discount rate, with a range of 0–8%, had the largest range of cost and effectiveness results. Probability of relapse, with a range from 0.05 to 0.15 annually, also had a substantial spread of results. However, the combination of Traditional Referral, BPA and Population Outreach still maintained dominance – that is, lower cost and also increased effectiveness – over the Traditional only arm across respective ranges. The only variable for which dominance was not maintained by the no cost-sharing policy was for the annual probability of death if a current smoker (range 0.003–0.004); however, the spread of results was small and still highly cost effective. All other model parameters only had small changes in overall results over their respective ranges.
Discussion
Main findings
Traditional Referral was associated with DSCP utilization of 4.6% among Primary Care smokers and 7.4% among Disadvantaged Care smokers. The addition of referral through BPA and Population Outreach substantially increased DSCP utilization to 11.7 and 14.4%, respectively. The health outcomes of adding these referral methods led to an increase of 0.07 QALYs (27 quality-adjusted days) saved per person and 408 total QALYs saved and 0.18 years (67 days) and 967 total life-years saved. The lifetime cost savings per person was US$8276, with total cost savings for the Primary Care and Disadvantaged Care clinics of US$46,376,285. Cost savings was higher among female smokers because they live approximately 2 years longer than male smokers.
Comparison of outcomes to existing literature
Our findings appear to be somewhat similar to findings in the existing literature on the BPA and Population Outreach when used as referral methods to smoking cessation services. Regarding BPA, one study shows that BPA generated a total of 3.4 referrals per clinic per year to a phone-based smoking cessation program [59]. This outcome is quite low and similar to our BPA outcomes. Population Outreach was studied in a randomized controlled trial using an automated phone-based outreach; program utilization from population outreach was 6.1%, [36] similar to the 7% we found in our study. Another study compared health and economic outcomes of Population Outreach to the use of no referral to a smoking cessation program. Outcomes showed 0.005 additional QALYs, with an expected incremental cost–effectiveness ratio of US$4231 per QALY [60]. Our outcomes were somewhat high, which may be related to differences in smoking cessation programs. The program that was tested was non-intensive, producing lower abstinence rates, whereas DSCP provides intensive face-to-face, treatment with individualized medication and behavioral strategies, an approach that leads to higher rates of smoking abstinence.
Limitations
As with all model-based studies, there are parameter-based limitations due to simplifying assumptions. We based quit attempts on attendance of first clinic visit and we did not account for unassisted quits. However, this is true for both of the comparison arms and thus did not affect the incremental results. For quit attempts, the model assumed that only one quit attempt was made per year. However, this leads to a conservative bias in our results because multiple quit attempts would improve the chances of quitting, thereby accruing the cost savings and effectiveness gains from quitting. We could not model switching between smoking cessation interventions. Switching interventions may potentially lead to a more or less effective intervention and some may argue that switching to a less effective regimen is more likely. At the least, the possibility of switching medications adds uncertainty to our estimates. Much of the literature-based evidence we relied upon for the model parameter values were reported as point estimates, with no information regarding their distributions. This limited our ability to derive confidence intervals for the cost and effectiveness results. However, one-way sensitivity analyses indicated that only a few parameters could have a large impact on the estimates and only with highly unlikely outlier values.
In terms of model-based limitations, we identified two limitations: BENESCO and harm reduction. When modeling smoking cessation, two general strategies are taken: either a successful quit-based approach as we and others [54] have taken or a smoking-related attributable risk approach, such as the BENESCO model [49]. A limitation of the quit-based approach is that limited information is gained – we simply estimate what costs and effectiveness are likely to be if they quit versus if smokers do not quit. However, for clinical practice decision-making from the provider perspective, that may be the only two essential pieces of information necessary for decision making. In the latter approach, smokers are modeled to transition to a limited number of smoking-related health states: lung cancer or chronic obstructive pulmonary disease, coronary heart disease or stroke, asthma and death. Thus information is gained regarding which diseases contribute what portion of the costs and effectiveness gains. However, while these five health states capture the majority of the smoking-related disease burden, the authors themselves acknowledge that smoking is known to affect health in more than 50 different ways, at least 20 of which can be fatal. Thus, the smoking-attributable risk has its own limitation of not capturing all of the smoking-related costs and underestimating the benefits of smoking cessation.
An abstinence-based approach is also limiting in that the model only accrues benefit if the smoker is able to quit successfully. However, the smoking cessation interventions may also provide benefit or cost savings if they lead to harm reduction from fewer cigarettes smoked. We chose to exclude harm reduction from the models because harm reduction is a controversial public health issue – the goal should be totally quitting – and there is limited information regarding the health and cost effects of reducing the number of cigarettes smoked but not quitting. Also, accounting for harm reduction in the models would only improve the cost savings and health gains presented in this study. We were also limited to using first visit attendance as a proxy for a quit attempt. Of course, it is quite likely that some smokers attempted to quit on their own, but this could not be observed.
Conclusions
Today, smokers have very low success rates when they try to quit on their own; however, most smokers receive services through health systems that offer smoking cessation programs with highly effective treatment. A key to making a health system smoking cessation program successful is developing methods to increase utilization of services. Our study showed that newer methods of referral – BPA and Population Outreach – led to substantial increases in service utilization. Our modeling shows that this in turn resulted in improved health outcomes and lower healthcare costs. Other institutions may similarly benefit from the use of these referral methods for smoking cessation services.
•
Smoking remains the leading cause of preventable morbidity and mortality in the USA.
•
Smoking cessation interventions have been shown to be among the most effective intervention programs available.
•
Traditional referral (common provider-driven referral) alone has resulted in suboptimal utilization of smoking cessation services.
•
Health systems have now adopted best practice care pathways, including pathways for the treatment of smokers. With the emergence of electronic health records, a health system is able to identify patients who smoke and drive referral to evidence-based treatment for these patients.
•
Two relatively new referral methods show promise for increasing utilization of smoking cessation services – Best Practice Advisory (an alert that occurs in the electronic health record and guides treatment) and Population Outreach (a list of patients generated through the electronic health record that is then contacted to offer treatment).
•
This study found that Best Practice Advisory and Population Outreach substantially increased utilization of a smoking cessation program over using Traditional Referral alone.
•
The analysis in this paper showed that the increases in program utilization from using these forms of referral resulted in an increase in life expectancy, quality-adjusted life-years and lifetime cost savings.
Author contributions
S Datta performed Markov modeling, researched the background on population-based information and is the primary author of the manuscript. PA Dennis performed supporting statistical analysis and is a contributing author of the manuscript. J Davis researched background information, assisted in data review and analysis, provided expertise on tobacco science and is the senior author of the manuscript.
Acknowledgments
J Greyber edited and formatted the manuscript for publication. A Pratt developed the figures.
Financial & competing interests disclosure
J Davis, PA Dennis, A Pratt and J Greyber are employees of Duke University, which received financial support from Pfizer, Inc., in connection with the development of this manuscript. S Datta was employed by Duke University (which received financial support from Pfizer, Inc. in connection with the development of this manuscript) at the time this study was conducted and the manuscript was written. S Datta, PA Dennis and J Davis declare research funding from Pfizer Inc. and Axsome Therapeutics Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval.
Data sharing statement
Data collected for this study contain protected health information for patients seen at the Duke Smoking Cessation Program and as such cannot be made publicly available.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
United States Surgeon General. The Health Consequences of Smoking – 50 years of progress (2014). www.ncbi.nlm.nih.gov/books/NBK179276/pdf/Bookshelf_NBK179276.pdf
2.
Centers for Disease Control and Prevention. Smoking and tobacco use; electronic cigarettes (2018). www.cdc.gov/tobacco/basic_information/e-cigarettes/
3.
Lortet-Tieulent J, Sauer AG, Siegel RL et al. State-level cancer mortality attributable to cigarette smoking in the United States. JAMA Intern. Med. 176(12), 1792–1798 (2016).
4.
Centers for Disease Control and Prevention. Smoking and Tobacco use; smokeless tobacco (2014). www.cdc.gov/tobacco/data_statistics/fact_sheets/smokeless/index.htm
5.
Centers for Disease Control and Prevention. Economic trends in tobacco (2019). www.cdc.gov/tobacco/data_statistics/fact_sheets/economics/econ_facts/index.htm
6.
National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. Fifty years of change 1964–2014 (2014). www.ncbi.nlm.nih.gov/books/NBK294310/
7.
Centers for Disease Control and Prevention. Current cigarette smoking among adults in the United States (2019). www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm
8.
Centers for Disease Control and Prevention. Cigarette smoking and tobacco use among people of low socioeconomic status (2018). www.cdc.gov/tobacco/disparities/low-ses/
9.
Centers for Disease Control and Prevention. Burden of tobacco use in the US: current cigarette smoking among us adults aged 18 years and older (2019). www.cdc.gov/tobacco/campaign/tips/resources/data/cigarette-smoking-in-united-states.html
10.
Centers for Disease Control and Prevention. Tobacco use and quitting among individuals with behavioral health conditions (2019). www.cdc.gov/tobacco/disparities/mental-illness-substance-use/index.htm
11.
National Alliance on Mental Illness. Tobacco and smoking. www.nami.org/learn-more/mental-health-public-policy/tobacco-and-smoking
12.
Christiansen B, Reeder K, Hill M, Baker TB, Fiore MC. Barriers to effective tobacco-dependence treatment for the very poor. J. Stud. Alcohol Drugs 73(6), 874–884 (2012).
13.
Stewart DW, Adams CE, Cano MA et al. Associations between health literacy and established predictors of smoking cessation. Am. J. Public Health 103(7), e43–e49 (2013).
14.
Trainor K, Leavey G. Barriers and facilitators to smoking cessation among people with severe mental illness: a critical appraisal of qualitative studies. Nicotine Tob. Res. 19(1), 14–23 (2017).
15.
Hughes JR, Keely J, Naud S. Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction 99(1), 29–38 (2004).
16.
McDonough JE. The United States health system in transition. Health Syst. Ref. 1(1), 39–51 (2015).
17.
Institute of Medicine (US) Committee for the Study of the Future of Public Health. The Future of Public Health, Appendix A: Summary of the Public Health System in the United States. National Academies Press (US), www.ncbi.nlm.nih.gov/books/NBK218212/
18.
US Census Bureau. Health insurance coverage in the United States (2016). www.census.gov/library/publications/2017/demo/p60-260.html
19.
Committee on the Learning Health Care System in America, Institute of Medicine. A Continuously Learning Health Care System. Smith M, Saunders R, Stuckhardt Let al et al. (Eds). National Academies Press (US), www.ncbi.nlm.nih.gov/books/NBK207218/
20.
Curry SJ, Keller PA, Orleans CT, Fiore MC. The role of health care systems in increased tobacco cessation. Annu. Rev. Public Health 29, 411–428 (2008).
21.
Centers for Disease Control and Prevention. Smoking and tobacco use; state and community resources. www.cdc.gov/tobacco/stateandcommunity/index.htm
22.
Centers for Disease Control and Prevention. Best practices for comprehensive tobacco control programs – 2014 (2018). www.cdc.gov/tobacco/stateandcommunity/best_practices/index.htm
23.
Centers for Disease Control and Prevention. Tobacco use screening and counseling during physician office visits among adults – National Ambulatory Medical Care Survey and National Health Interview Survey, United States, 2005–2009. https://www.cdc.gov/mmwr/preview/mmwrhtml/su6102a7.htm
24.
Karam-Hage M, Oughli HA, Rabius V et al. Tobacco cessation treatment pathways for cancer patients: 10 years in the making models for smoking cessation practice. J. Natl Compr. Canc. Netw. 14(11), 1469–1477 (2016).
25.
Hays JT, Croghan IT, Schroeder DR et al. Residential treatment compared with outpatient treatment for tobacco use and dependence. Mayo Clin. Proc. 86(3), 203–209 (2011).
26.
Davis JM, Goldberg SB, Angel KS, Silver RH, Kragel EA, Lagrew DJ. Observational study on a mindfulness training for smokers within a smoking cessation program. Mindfulness (NY) 8(6), 1698 (2017).
27.
Atherton J. Development of the electronic health record. AMA J. Ethics 13(3), 186–189 (2011).
28.
Centers for Disease Control and Prevention. National Health Statistics Reports Number 115. 115, 9 (2018).
29.
Adoption of Electronic Health Record Systems among U.S. Non-federal acute care hospitals: 2008–2015 (2016). https://dashboard.healthit.gov/evaluations/data-briefs/non-federal-acute-care-hospital-ehr-adoption-2008-2015.php
30.
Fiore MC, Jorenby DE, Schensky AE, Smith SS, Bauer RR, Baker TB. Smoking status as the new vital sign: effect on assessment and intervention in patients who smoke. Mayo Clinic Proc. 70(3), 209–213 (1995).
31.
EHR Incentive Program. Eligible professional meaningful use core measures measure 9 of 13 stage 1(2014 definition) (2014). www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/9_Record_Smoking_Status.pdf
32.
Polubriaginof F, Salmasian H, Albert DA, Vawdrey DK. Challenges with collecting smoking status in electronic health records. AMIA Annu. Symp. Proc. 2017, 1392–1400 (2018).
33.
Lurio J, Morrison FP, Pichardo M et al. Using electronic health record alerts to provide public health situational awareness to clinicians. J. Am. Med. Inform. Assoc. 17(2), 217–219 (2010).
34.
Perri-Moore S, Kapsandoy S, Doyon K et al. Automated alerts and reminders targeting patients: a review of the literature. Patient Educ. Couns. 99(6), 953–959 (2016).
35.
Simon GE, Beck A, Rossom R et al. Population-based outreach versus care as usual to prevent suicide attempt: study protocol for a randomized controlled trial. Trials 17(1), 452 (2016).
36.
Haas JS, Linder JA, Park ER et al. Proactive tobacco cessation outreach to smokers of low socioeconomic status: a randomized clinical trial. JAMA Intern. Med. 175(2), 218–226 (2015).
37.
Danan ER, Fu SS, Clothier BA et al. the equity impact of proactive outreach to smokers: analysis of a randomized trial. Am. J. Prev. Med. 55(4), 506–516 (2018).
38.
Briggs A, Sculpher M, Claxton K. Decision Modelling for Health Economic Evaluation. Oxford University Press, Oxford, UK (2006).
39.
Neumann PJ, Ganiats TG, Russell LB, Sanders GD, Siegel JE. (Eds). Cost–Effectiveness in Health and Medicine. Oxford University Press, Oxford, UK (2016).
40.
Sanders GD, Neumann PJ, Basu A et al. Recommendations for conduct, methodological practices and reporting of cost–effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA 316(10), 1093–1103 (2016).
• A useful resource for conducting state-of-the-art cost–effectiveness economic analyses.
41.
Duke Smoking Cessation Program. Duke smoking cessation program clinic data. NC, USA
42.
US Department of Veterans Affairs. Pharmacy benefits management services (2020). www.pbm.va.gov/
43.
Centers for Medicare and Medicaid Services (2019). www.cms.gov/
44.
Barnett PG, Wong W, Jeffers A, Hall SM, Prochaska JJ. Cost-effectiveness of smoking cessation treatment initiated during psychiatric hospitalization: analysis from a randomized, controlled trial. J. Clin. Psych. 76(10), e1285–e1291 (2015).
• An important source for the Markov model strategy and some of the parameter values used in the model.
45.
Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst. Rev. 5, CD009329 (2013).
•• An important source for the relative effectiveness of various smoking cessation interventions.
46.
Hartmann-Boyce J, Stead LF, Cahill K, Lancaster T. Efficacy of interventions to combat tobacco addiction: cochrane update of 2013 reviews. Addiction 109(9), 1414–1425 (2014).
47.
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 3, CD001292 (2017).
48.
Siu AL. Behavioral and pharmacotherapy interventions for tobacco smoking cessation in adults, including pregnant women: US Preventive Services Task Force recommendation statement. Ann. Intern. Med. 163(8), 622–634 (2015).
49.
Patnode CD, Henderson JT, Thompson JH, Senger CA, Fortmann SP, Whitlock EP. Behavioral counseling and pharmacotherapy interventions for tobacco cessation in adults, including pregnant women: a review of reviews for the US Preventive Services Task Force. Ann. Intern. Med. 163(8), 608–621 (2015).
50.
Hughes JR, Peters EN, Naud S. Relapse to smoking after 1 year of abstinence: a meta-analysis. Addict. Behav. 33(12), 1516–1520 (2008).
51.
Howard P, Knight C, Boler A, Baker C. Cost-utility analysis of varenicline versus existing smoking cessation strategies using the BENESCO Simulation model: application to a population of US adult smokers. Pharmacoeconomics 26(6), 497–511 (2008).
52.
Maciosek MV, Xu X, Butani AL, Pechacek TF. Smoking-attributable medical expenditures by age, sex and smoking status estimated using a relative risk approach. Prev. Med. 77, 162–167 (2015).
•• An important source of medical care costs of current versus former smokers.
53.
Vogl M, Wenig CM, Leidl R, Pokhrel S. Smoking and health-related quality of life in English general population: implications for economic evaluations. BMC Public Health 12(1), 203 (2012).
54.
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 3, CD001292 (2017).
55.
Office of Procurement, Acquisition and Logistics (OPAL). Pharmaceutical prices (2020). www.va.gov/opal/nac/fss/pharmPrices.asp
56.
Medicaid covered outpatient prescription drug reimbursement information by state (2020). www.medicaid.gov/medicaid/prescription-drugs/state-prescription-drug-resources/drug-reimbursement-information/index.html
57.
Quick guide: billing for smoking cessation counseling 99406 and 99407 (2016). https://capturebilling.com/how-bill-smoking-cessation-counseling-99406-99407/
58.
Sanders GD, Neumann PJ, Basu A et al. Recommendations for conduct, methodological practices and reporting of cost–effectiveness analyses: second panel on cost–effectiveness in health and medicine. JAMA 316(10), 1093–1103 (2016).
59.
Adsit RT, Fox BM, Tsiolis T et al. Using the electronic health record to connect primary care patients to evidence-based telephonic tobacco quitline services: a closed-loop demonstration project. Transl. Behav. Med. 4(3), 324–332 (2014).
60.
Thao V, Nyman JA, Nelson DB et al. Cost–effectiveness of population-level proactive tobacco cessation outreach among socio-economically disadvantaged smokers: evaluation of a randomized control trial. Addiction 114(12), 2206–2216 (2019).
Information & Authors
Information
Published In
Pages: 817 - 828
PubMed: 32815740
Copyright
© 2020 James Davis and co-authors. This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License
History
Received: 10 January 2020
Accepted: 5 June 2020
Published online: 20 August 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Health benefits and economic advantages associated with increased utilization of a smoking cessation program. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2020-0005
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Olivia Allen, Lindsey Fields, Maura Sweeney, Shontel Als, William Seiple, Anurag Shrivastava, The Impact of Workflow Modifications in an Electronic Medical Record on Tertiary Service Referrals for Patients with Visual Impairment in New York City, Clinical Ophthalmology, 10.2147/OPTH.S532586, Volume 19, (3693-3702), (2025).
- Seyedeh Samaneh Miresmaeeli, Davoud Khorasani Zavareh, Hesam Seyedin, A comparative study: Accreditation of universities' disaster risk management for health promotion, Journal of Education and Health Promotion, 10.4103/jehp.jehp_590_22, 12, 1, (2023).