Impact of cytoreductive surgery on outcomes of metastatic appendiceal carcinoma: a real-world, population-based study
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To evaluate the impact of cytoreductive surgery on the outcomes of patients with metastatic appendiceal carcinoma. Methods: Surveillance, Epidemiology and End Results (SEER) database was accessed and patients with metastatic appendiceal carcinoma diagnosed (2010–2015) were reviewed. Kaplan–Meier survival estimates/log-rank testing were then used to assess overall survival outcomes according to cytoreductive surgery. Multivariable Cox regression analysis was then used to evaluate factors affecting cancer-specific survival. Factors included in this model were age, race, sex, stage and histology and cytoreductive surgery. Results: A total of 1339 patients with metastatic appendiceal carcinoma were included in the current study. Using Kaplan–Meier survival estimates to evaluate overall survival, patients with surgery for metastatic disease have better overall survival compared with patients without surgery for metastatic disease (p < 0.001). Stratifying survival analysis according to histology, the overall survival benefit from surgery for the metastases seems to be limited to patients with mucinous adenocarcinoma (p = 0.002) rather than patients with nonmucinous adenocarcinoma (p = 0.401). Multivariable Cox regression analysis was then conducted to evaluate factors predicting cancer-specific survival. The following factors were associated with worse cancer-specific survival: African-American race (hazard ratio [HR]: 1.356; 95% CI: 1.036–1.774; p = 0.026), more advanced stage (HR: 3.910; 95% CI: 2.735–5.588; p < 0.001), nonmucinous adenocarcinoma (HR for signet ring carcinoma vs mucinous adenocarcinoma: 2.119; 95% CI: 1.674–2.683; p < 0.001) and no surgical resection of metastatic disease (HR: 1.273; 95% CI: 1.067–1.519; p < 0.001). Conclusion: The current study suggests that among patients with metastatic appendiceal carcinoma, surgical cytoreduction of metastatic disease is associated with improved outcomes for patients with mucinous adenocarcinoma but not in patients with nonmucinous adenocarcinoma.
Appendiceal neoplasms represent a rare entity of digestive neoplasms with an incidence of approximately 2.6 per million people in the United States per year [1,2]. The most common two histological types of appendiceal tumors are epithelial tumors and neuroendocrine tumors [3].
Based on a number of retrospective reports, surgical cytoreduction (with or without intraperitoneal chemotherapy) has been advocated as a treatment strategy for patients with metastatic appendiceal carcinoma (particularly those with pseudomyxoma peritonei) [4,5]. However, there is generally a lack of updated studies which evaluate this intervention in the era of recent updates in systemic therapy options for metastatic colorectal carcinoma.
While randomized controlled trials are the gold standard for assessing the value of different interventions among cancer patients, there are known logistic challenges surrounding the design and conduct of such trials to evaluate surgical interventions [6]. Moreover, recruitment into such trials would become even more challenging for rare disease entities like appendiceal carcinoma [7]. Therefore, well-designed population-based studies remain an invaluable source to assess the value of surgical interventions in rare diseases.
Surveillance, Epidemiology and End Results (SEER) database is one of the largest population-based cancer registries in the world with rigorous quality assurance procedures and relatively large sample size (even for less common cancer types). Therefore, it makes a perfect sense to mine this database to answer questions regarding the impact of cytoreductive surgery on the outcomes of patients with metastatic appendiceal carcinoma. Results of the current study would inform surgical teams (as well as other members of the multidisciplinary team) regarding the role of surgery in this clinical scenario.
Objective
To evaluate the impact of cytoreductive surgery on the outcomes of patients with metastatic appendiceal carcinoma.
Methods
The current study was derived from SEER-18 registries (November 2018 submission). Patients within this submission were followed until December 2016 [8].
Cohort selection
The following eligibility criteria were used to select patients for inclusion into the current study: microscopically confirmed diagnosis with metastatic appendiceal carcinoma (including low-grade appendiceal mucinous neoplasms (LAMN); diagnosed 2010–2015 (in order to ensure relevance of the results of the study with current oncological and surgical practice and because a separate AJCC/TNM staging system for appendiceal carcinoma was first introduced in 2010). Inclusion of the study was limited to 2015 in order to allow at least 1 year of survival follow-up for all included patients (this SEER submission included patients up to December 2019 only). This study was conducted in accordance with STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) guidelines [9] (Supplementary Table 1).
Data collection
Where available and for each included patient, the following data were collected: age at diagnosis, sex, race, histology, grade, stage group, T stage, N stage and M stage (as per TNM 7th staging system), nonperitoneal sites of metastasis, treatment with surgery, chemotherapy and/or radiation therapy. Within the TNM seventh staging system for appendiceal carcinoma, M1a stage is defined as intraperitoneal metastasis beyond the right lower quadrant, including pseudomyxoma peritonei while M1b is defined as nonperitoneal metastasis. Likewise, within the TNM seventh stage grouping system, stage IVA is defined as (M1a N0 and grade 1); stage IVB is defined as (M1a N0 and grade 2–3 OR M1a N+ [any grade]) and stage IVC is defined as M1b [10]. Although TNM staging system for appendiceal carcinoma has been updated to the eighth edition since 2017 [11], the updated staging system cannot be incorporated in the current study because it was not reported in the SEER database yet.
The SEER variable ‘RX Summ–Surg Oth Reg/Dis’ was used to identify cases who have or have not been treated with cytoreductive surgery/surgery for metastatic disease. Information about the extent of surgical cytoreduction, perioperative morbidity/mortality as well as co-administration of intraperitoneal chemotherapy is not available in the SEER database.
Primary end points of the current study include overall survival (defined as the time from diagnosis till death of any cause) and cancer-specific survival (defined as the time from diagnosis till death of appendiceal cancer).
Statistical analysis
Descriptive statistics including frequencies and percentages were used to describe baseline and treatment characteristics of the study cohort. Chi-squared testing was used to compare baseline characteristics between patients who did or did not have surgery for the metastases. Kaplan–Meier survival estimates/log-rank testing were then used to assess overall survival outcomes according to cytoreductive surgery. Multivariable Cox regression analysis was then used to evaluate factors affecting cancer-specific survival. All relevant clinicopathological and treatment factors were included in this model, including age, race, and sex, stage, histology and cytoreductive surgery. Histological grade was not included in this model because it is part of the AJCC/TNM stage grouping system included in the same model. Chemotherapy and radiotherapy were not included in this model because of uncertainty surrounding the accuracy of reporting of chemotherapy and radiotherapy within the SEER database. SPSS statistical software was used in the current study (Version 20.0, IBM, NY, USA).
Results
Patients’ characteristics
A total of 1339 patients with metastatic appendiceal carcinoma were included in the current study. Within this cohort of patients, the majority have an age of 40–69 years (70.3%), female sex (58.7%), white race (81.5%), mucinous adenocarcinoma (63.4%), well-moderately differentiated histology (50%), stage IVC (53.4%), T4 disease (70.7%), N0 disease (62.3%) and M1b disease (53.4%). A total of 47.7% of patients were treated with surgery for the metastases, 70% of patients were treated with chemotherapy and 1.4% of patients were treated with radiation therapy (Table 1). Mean follow-up duration of the study cohort was 27.48 months (SD: 20.96).
| Parameter | N (%) |
|---|---|
| Age – 40 years – 40–69 years – ≥70 years | 102 (7.6%) 941 (70.3%) 296 (22.1%) |
| Sex – Males – Females | 553 (41.3%) 786 (58.7%) |
| Race – White – Black – Others – Unknown | 1091 (81.5%) 129 (9.6%) 114 (8.5%) 5 (0.4%) |
| Histology – Mucinous adenocarcinoma – Signet ring carcinoma – Other adenocarcinoma variants | 849 (63.4%) 197 (14.7%) 293 (21.9%) |
| Grade – Well differentiated – Moderately differentiated – Poorly differentiated – Undifferentiated – Unknown | 303 (22.6%) 367 (27.4%) 283 (21.1%) 59 (4.4%) 327 (24.4%) |
| Stage group (AJCC 7th edition)† – IVA – IVB – IVC – IVNOS | 325 (24.3%) 187 (14%) 715 (53.4%) 112 (8.4%) |
| T stage – T0 – T1 – T2 – T3 – T4 – Tx | 20 (1.5%) 43 (3.2%) 15 (1.1%) 119 (8.9%) 946 (70.7%) 196 (14.6%) |
| N stage – N0 – N1 – N2 – Nx | 834 (62.3%) 185 (13.8%) 163 (12.2%) 157 (11.7%) |
| M stage – M1a‡ – M1b‡ – M1NOS§ | 554 (41.4%) 715 (53.4%) 70 (5.2%) |
| Nonperitoneal sites of metastases – Liver – Lung – Bone – Brain | 190 (14.2%) 46 (3.4%) 24 (1.8%) 3 (0.2%) |
| Surgical treatment of the primary – Limited resection – Radical surgery (partial, hemi-, subtotal or total colectomy) – None – Unknown | 35 (2.6%) 962 (71.8%) 280 (21%) 62 (4.6%) |
| Surgical treatment of metastatic disease – Yes – No – Unknown | 639 (47.7%) 694 (51.8%) 6 (0.5%) |
| Chemotherapy – Yes – No/unknown | 949 (70.9%) 390 (29.1%) |
| Radiotherapy – Yes – No | 19 (1.4%) 1720 (98.6%) |
†
IVA: M1a N0 and grade 1; IVB: M1a N0 and grade 2–3 OR M1a N+ (any grade); IVC: M1b.
‡
M1a: Intra-peritoneal metastasis beyond the right lower quadrant, including pseudomyxoma perironei; M1b: Nonperitoneal metastasis.
§
NOS: Not otherwise specified.
AJCC: American Joint Committee on Cancer.
Comparing patients who had surgery for metastatic disease versus those who did not have, patients with surgery for the metastases were more likely to have male sex (54.3 vs 38.3%; p < 0.001), well-differentiated histology (p = 0.009) and mucinous histology (p = 0.024). There was no difference between both groups with regards to age group (p = 0.304) or race (p = 0.916).
Survival outcomes
Using Kaplan–Meier survival estimates to evaluate overall survival according to surgery for metastatic disease, patients with surgery for metastatic disease have better overall survival compared with patients without surgery for metastatic disease (median survival 40 vs 27 months; p < 0.001; Figure 1). Stratifying survival analysis according to histology, the overall survival benefit from surgery for the metastases seems to be limited to patients with mucinous adenocarcinoma (median overall survival 73 vs 43 months; p = 0.002) rather than patients with nonmucinous adenocarcinoma (median overall survival 20 vs 17 months; p = 0.401; Figure 2A & B). When the survival analysis of patients with nonmucinous adenocarcinoma was further stratified into those with signet ring carcinoma versus those with other variants of nonmucinous adenocarcinoma, there was no benefit from surgery for the metastases in both subgroups (p for signet ring carcinoma subgroup = 0.984; p for other nonmucinous variants = 0.227; data not shown).
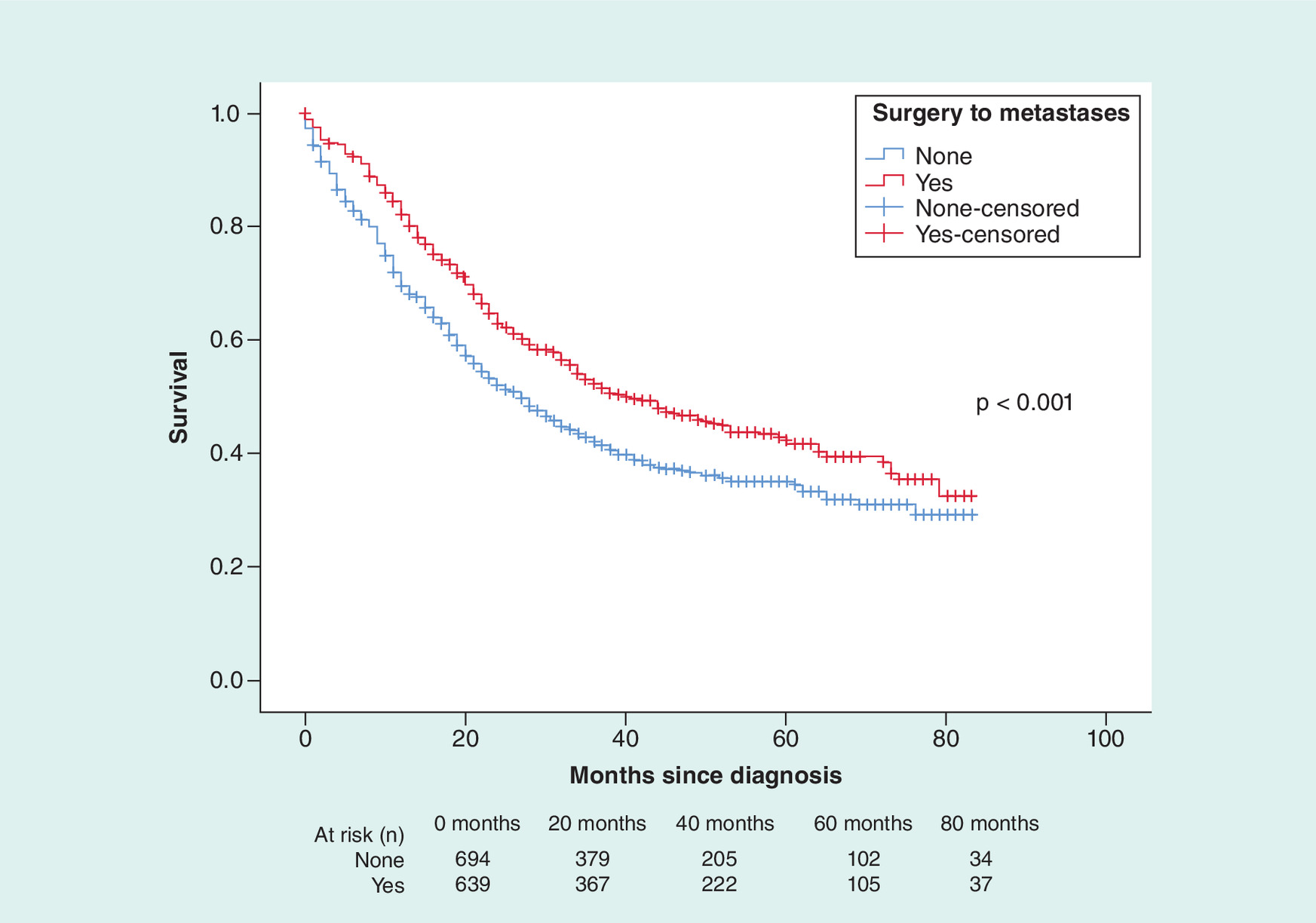
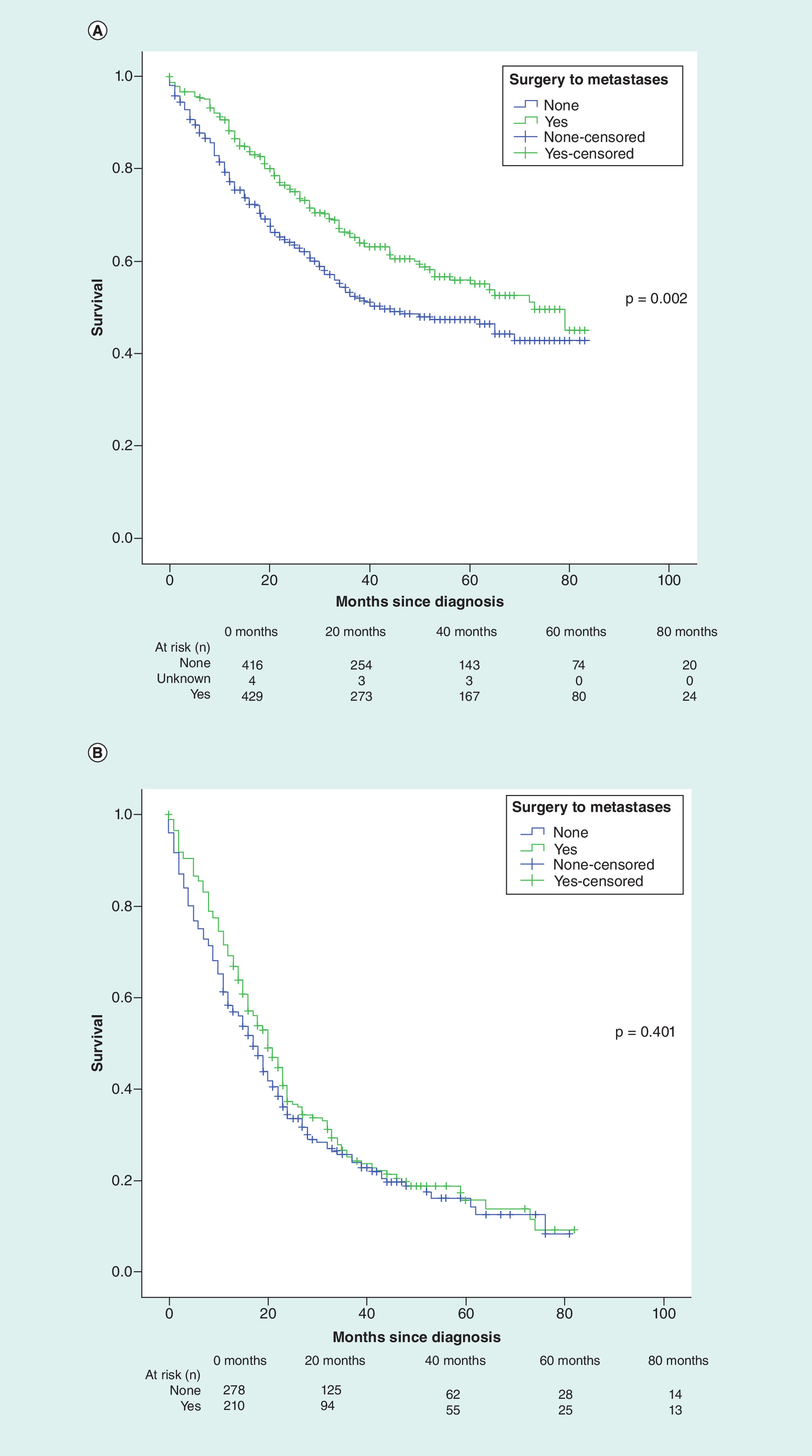
Figure 2. Surgery for metastases.
Kaplan–Meier survival curve for the impact of surgery for the metastases on overall survival among (A) patients with mucinous adenocarcinoma; (B) patients with nonmucinous adenocarcinoma.
Multivariate Cox regression analysis was then conducted to evaluate factors predicting cancer-specific survival. The following factors were associated with worse cancer-specific survival: African-American race (hazard ratio [HR]: 1.356; 95% CI: 1.036–1.774; p = 0.026), more advanced stage (HR: 3.910; 95% CI: 2.735–5.588; p < 0.001), nonmucinous adenocarcinoma (HR for signet ring carcinoma vs mucinous adenocarcinoma: 2.119; 95% CI: 1.674–2.683; p < 0.001) and no surgical resection of metastatic disease (HR: 1.273; 95% CI: 1.067–1.519; p < 0.001; Table 2).
| Parameters | HR (95% CI) | p-value |
|---|---|---|
| Age – 40–69 years – <40 years – ≥70 years | Reference 0.826 (0.583–1.170) 1.126 (0.912–1.388) | 0.282 0.269 |
| Sex – Males – Females | Reference 0.860 (0.720–1.028) | 0.098 |
| Race – White – Black – Others | Reference 1.356 (1.036–1.774) 0.883 (0.638–1.222) | 0.026 0.454 |
| Stage group (AJCC 7th edition) – IVA – IVB – IVC | Reference 3.910 (2.735–5.588) 2.991 (2.169–4.125) | <0.001 <0.001 |
| Histology – Mucinous adenocarcinoma – Signet ring carcinoma – Other adenocarcinoma variants | Reference 2.119 (1.674–2.683) 2.452 (1.993–3.016) | <0.001 <0.001 |
| Surgical treatment of metastatic disease – Yes – No | Reference 1.273 (1.067–1.519) | 0.007 |
†
Patients with unknown race, stage or surgical resection were included in the analysis but they were not reported here.
AJCC: American Joint Committee on Cancer; HR: Hazard ratio.
Discussion
The current study evaluates the impact of surgical resection of metastatic disease on the outcomes of patients with metastatic appendiceal carcinoma. It indicates that among patients with metastatic appendiceal carcinoma, surgical cytoreduction of metastatic disease is associated with improved outcomes for patients with mucinous adenocarcinoma but not in patients with nonmucinous adenocarcinoma. This differential effect based on histology might be related to the poor outcomes of patients with nonmucinous adenocarcinoma (a considerable proportion of those patients have signet ring carcinoma) which made cytoreductive surgery a rather futile intervention in their case.
Findings from the current study are in line with prior population-based studies confirming the beneficial role of surgery for metastatic disease among patients with gastrointestinal cancers and distant metastases [12–14]. This study also gives an insight into the impact of race on the outcomes of this rare digestive cancer. Similar to the findings from other digestive cancers, patients with African-American race have unfortunately worse cancer-specific survival. Possible reasons might include biological differences but also socioeconomic differences in healthcare access [13]. Failure to be referred to specialist centers to have surgery with or without intraperitoneal chemotherapy (this is a rare neoplasm for which there is still limited awareness in the surgical community) might be playing a role as well here [15,16,17].
A recent US randomized study evaluated hematologic toxicities after hyperthermic intraperitoneal chemotherapy (HIPEC) with oxaliplatin or mitomycin in patients with appendiceal tumors. It suggested that both mitomycin and oxaliplatin are associated with minor hematologic toxicity. However, mitomycin has slightly lower quality of life and higher hematologic toxicity [14]. Another French study (PRODIGE-7) has evaluated specifically the impact of cytoreductive surgery with or without HIPEC in the management of peritoneal carcinomatosis from colorectal cancer. It showed a median overall survival of 41.2 months in the non-HIPEC arm and 41.7 months in the HIPEC arm; thus, suggesting that HIPEC did not influence survival in this cohort of patients [18]. Although the survival numbers in this study are a bit impressive for patients with metastatic colorectal cancer to the peritoneum; it is certainly applicable only to a highly selected subgroup of patients with excellent performance, limited comorbidity, and limited peritoneal disease. It is also unclear if these results can be extrapolated to patients with appendiceal carcinoma who generally have different biology and different clinical course of their disease compared with colorectal cancer patients.
Limitations & strengths
Several limitations need to be acknowledged in the current study. First: there was a lack of information in the current study regarding performance status and comorbidity of included patients. To limit the impact of this confounder, both overall and cancer-specific survivals were used as study end points. While noncancer morbidity might affect overall survival outcomes; it is less likely to impact cancer-specific survival outcomes. Second: lack of detailed information about the extent of surgical cytoreduction as well as details of co-administration of intraperitoneal or intravenous chemotherapy is likely to decrease the veracity of the results of the current study. Surgical treatment has to be performed in well-selected patients (peritoneal only disease, good performance status, responding to chemotherapy) and complete/optimal resection is essential (just like for any metastatic disease e.g., liver resection for metastatic colon cancer). This detailed set of information is not available from SEER. These limitations need to be assessed versus the strengths of the current study including the up-to-date nature of data collection and a relatively large number of included patients for such a rare disease entity.
Implications on practice
Because of the rarity of metastatic appendiceal carcinoma and the lack of level I evidence to guide treatment recommendations, management of these cases is usually debated in multidisciplinary tumor boards. Results of the current study should inform therapeutic decision making particularly with regards to the role of cytoreductive surgery for metastatic mucinous adenocarcinoma of the appendix. Metastatic nonmucinous adenocarcinoma of the appendix seems to carry a particularly bad prognosis and – based on the small-sized cohort in the current study – cytoreductive surgery does not appear to improve the outcomes. In the view of the author of this paper, management of metastatic nonmucinous adenocarcinoma of the appendix should be along the general lines of management of metastatic colorectal cancer (although strong evidence is lacking for this viewpoint).
Future perspective
Because of the rarity of this disease entity, multi-institutional and multinational collaboration is fundamental in informing the therapeutic decision making for metastatic appendiceal carcinoma. Research questions that need to be answered include biological differences between appendiceal carcinoma and colorectal carcinoma (and the potential implications of these biological differences on systemic therapy choices), and differences between mucinous and nonmucinous adenocarcinomas of the appendix in terms of biology, clinical presentation and treatment responsiveness.
Conclusion
In conclusion, the current study suggests that among patients with metastatic appendiceal carcinoma, surgical cytoreduction of metastatic disease is associated with improved outcomes for patients with mucinous adenocarcinoma but not in patients with nonmucinous adenocarcinoma. Weaknesses of the current study might however limit its external validity.
•
Surveillance, Epidemiology and End Results (SEER) database was accessed and patients with metastatic appendiceal carcinoma diagnosed 2010–2015 were reviewed.
•
Kaplan–Meier survival estimates/log-rank testing were then used to assess overall survival outcomes according to cytoreductive surgery.
•
Multivariable Cox regression analysis was then used to evaluate factors affecting cancer-specific survival. Factors included in this model were age, race, sex, stage and histology and cytoreductive surgery.
•
A total of 1339 patients with metastatic appendiceal carcinoma were included in the current study.
•
Using Kaplan–Meier survival estimates to evaluate overall survival, patients with surgery for metastatic disease have better overall survival compared with patients without surgery for metastatic disease (p < 0.001).
•
Stratifying survival analysis according to histology, the overall survival benefit from surgery for the metastases seems to be limited to patients with mucinous adenocarcinoma (p = 0.002) rather than patients with nonmucinous adenocarcinoma (p = 0.401).
•
Multivariable Cox regression analysis was then conducted to evaluate factors predicting cancer-specific survival.
•
The following factors were associated with worse cancer-specific survival: African-American race (hazard ratio [HR]: 1.356; 95% CI: 1.036–1.774; p = 0.026), more advanced stage (HR: 3.910; 95% CI: 2.735–5.588; p < 0.001), nonmucinous adenocarcinoma (HR for signet ring carcinoma vs mucinous adenocarcinoma: 2.119; 95% CI: 1.674–2.683; p < 0.001) and no surgical resection of metastatic disease (HR: 1.273; 95% CI: 1.067–1.519; p < 0.001).
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_file.pdf)
- Download
- 511.12 KB
References
Papers of special note have been highlighted as: • of interest
1.
Nutu OA, Marcacuzco Quinto AA, Manrique Municio A et al. Mucinous appendiceal neoplasms: incidence, diagnosis and surgical treatment. Cir. Esp. 95(6), 321–327 (2017).
2.
Smeenk RM, van Velthuysen ML, Verwaal VJ, Zoetmulder FA. Appendiceal neoplasms and pseudomyxoma peritonei: a population based study. Eur. J. Surg. Oncol. 34(2), 196–201 (2008).
3.
Benedix F, Reimer A, Gastinger I, Mroczkowski P, Lippert H, Kube R. Primary appendiceal carcinoma – epidemiology, surgery and survival: results of a German multi-center study. Eur. J. Surg. Oncol. 36(8), 763–771 (2010).
4.
Mirnezami R, Moran BJ, Harvey K et al. Cytoreductive surgery and intraperitoneal chemotherapy for colorectal peritoneal metastases. World J. Gastroenterol. 20(38), 14018–14032 (2014).
5.
El-Nakeep S, Rashad N, Oweira H et al. Intraperitoneal chemotherapy and cytoreductive surgery for peritoneal metastases coupled with curative treatment of colorectal liver metastases: an updated systematic review. Expert Rev. Gastroenterol. Hepatol. 11(3), 249–258 (2017).
6.
Yu J, Chen W, Chen S et al. Design, conduct, and analysis of surgical randomized controlled trials: a cross-sectional survey. Ann. Surg. 270(6), 1065–1069 (2018).
7.
Panageas KS. Clinical trial design for rare cancers: why a less conventional route may be required. Expert Rev. Clin. Pharmacol. 8(6), 661–663 (2015).
8.
Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Incidence - SEER 18 Regs Custom Data (with additional treatment fields), Nov 2018 Sub (1975–2016 varying) - Linked To County Attributes - Total U.S., 1969–2017 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2019, based on the November 2018 submission (2018). www.seer.cancer.gov
9.
von Elm E, Altman DG, Egger M et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ 335(7624), 806–808 (2007).
10.
Edge SB, Compton CC. The American joint committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 17(6), 1471–1474 (2010).
11.
Amin MB, Greene FL, Edge SB et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 67(2), 93–99 (2017).
12.
Oweira H, Petrausch U, Helbling D et al. Prognostic value of site-specific metastases in pancreatic adenocarcinoma: a surveillance epidemiology and end results database analysis. World J. Gastroenterol. 23(10), 1872–1880 (2017).
13.
Abdel-Rahman O. Outcomes of non-metastatic colon cancer patients in relationship to socioeconomic status: an analysis of SEER census tract-level socioeconomic database. Int. J. Clin. Oncol. 24(12), 1582–1587 (2019).
14.
Levine EA, Votanopoulos KI, Shen P et al. A multicenter randomized trial to evaluate hematologic toxicities after hyperthermic intraperitoneal chemotherapy with oxaliplatin or mitomycin in patients with appendiceal tumors. J. Am. Coll. Surg. 226(4), 434–443 (2018).
15.
Oweira H, Petrausch U, Helbling D et al. Prognostic value of site-specific extra-hepatic disease in hepatocellular carcinoma: a SEER database analysis. Expert Rev. Gastroenterol. Hepatol. 1(7), 695–701 (2017).
16.
Oweira H, Mehrabi A, Reissfelder C, Abdel-Rahman O. A real-world, population-based analysis of the outcomes of colorectal cancer patients with isolated synchronous liver or lung metastases treated with metastasectomy. World J. Surg. (2020) (Epub ahead of print).
• Evaluates the impact of metastatectomy on survival of metastatic colorectal cancer.
17.
Abdel-Rahman O. A real-world, population-based study of the outcomes of patients with metastatic colorectal cancer to the peritoneum treated with or without cytoreductive surgery. Int J Colorectal Dis. (2020).
18.
Quenet F, Elias D, Roca L et al. A UNICANCER Phase III trial of hyperthermic intra-peritoneal chemotherapy (HIPEC) for colorectal peritoneal carcinomatosis (PC): PRODIGE 7. J. Clin. Oncol. 36, LBA3503–LBA3503 (2018).
Information & Authors
Information
Published In
Pages: 431 - 439
PubMed: 32253936
Copyright
© 2020 Future Medicine Ltd.
History
Received: 27 November 2019
Accepted: 10 February 2020
Published online: 7 April 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Impact of cytoreductive surgery on outcomes of metastatic appendiceal carcinoma: a real-world, population-based study. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0179
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Rennie Xinrui Qin, Tilisi Puloka, Jia Hui Lim, Caro Staheli, Jesse Fischer, Simione Lolohea, Jasen Ly, Treatment of peritoneal disease arising from mucinous vs. non-mucinous appendiceal neoplasms with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy, Pleura and Peritoneum, 10.1515/pp-2025-0007, 10, 3, (137-145), (2025).
- Wolfgang B. Gaertner, Shaun R. Brown, Michael Deutsch, Mehraneh D. Jafari, Mukta K. Krane, Vlad V. Simianu, Michael A. Valente, Amy L. Lightner, Daniel L. Feingold, Ian M. Paquette, The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Appendiceal Neoplasms, Diseases of the Colon & Rectum, 10.1097/DCR.0000000000003796, 68, 7, (815-834), (2025).
- Yuqian Tian, Carrie Luu, Danielle H. Carpenter, Grace Montenegro, A Unique Presentation of Metastatic Gallbladder Carcinoma, Case Reports in Surgery, 10.1155/2021/6455540, 2021, (1-5), (2021).