Crizotinib versus chemotherapy: a real-world cost–effectiveness study in China
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: To assess the cost–effectiveness of crizotinib verses platinum-based doublet chemotherapy as the first-line treatment for anaplastic lymphoma kinase (ALK)-positive non-small-cell lung cancer (NSCLC) in the real-world setting. Methods: Data from 163 advanced ALK positive NSCLC patients were collected from West China Hospital, Sichuan University (Chengdu, China). They were categorized into two groups as treated with crizotinib (n = 83) or chemotherapy (n = 80) as a first-line therapy. The progression-free survival (PFS) as the primary clinical outcome, and the direct medical costs were collected from hospital information systems. Incremental cost–effectiveness ratio (ICER) was calculated with costs, quality-adjusted life-years, as well as the costs discounted at 3% annually. Additionally, two different kinds of medical insurance (MI) for pharma-economic assessment were considered. Results: Crizotinib improved PFS versus chemotherapy in ALK positive patients (median PFS 19.67 m vs 5.47 m; p < 0.001). Moreover, crizotinib obtained an ICER of US$36,285.39 before the end of 2016, when crizotinib, pemetrexed and anti-angiogenesis drugs were not MI covered. This is more than the willingness to pay threshold (three-times of gross domestic product per capita in mainland China or Sichuan Province). However, ICER was US$7321.16, which is less than willingness to pay, when crizotinib and all chemotherapy drugs were covered by MI from the end of 2016. Sensitivity analysis demonstrated a 99.7% probability for crizotinib to be more cost-effective than chemotherapy, when crizotinib and all anticancer drugs were MI covered. One-way sensitivity analysis for the reimbursement ratio of crizotinib indicated that cost-effective tendency for crizotinib increased as reimbursement ratio increased. Conclusion: Crizotinib could be an effective, and cost-effective first-line treatment for ALK positive advanced NSCLC with the MI coverage currently available in Chengdu, Sichuan Province, China.
Among all of the cancers, lung cancer is the most relevant problem in society, because it has the highest worldwide mortality rate. Eighty percent of all cases are non-small-cell lung cancer (NSCLC). The previous therapeutic treatments for advanced NSCLC are mainly based on traditional chemotherapy agents. These traditional anticancer drugs tend to have low efficacy, which is confirmed by the fact that the mortality rate is still high [1]. However, targeted therapies are generating a revolution in therapeutic treatment by blocking specific enzymes, and growth factor receptors involved in cancer cell proliferation. Although target drugs are very expensive and appear to increase healthcare costs, vital socio-economic clinical consequences should be discussed [2]. For instance, considering opportunity costs, including day-hospital costs, costs for treating adverse effects or costs for clinicians may be reduced when target therapies are used [1]. In addition, the continuous evolution of technological change in medicine should be associated with a far-sighted health policy. An important challenge by policy makers is to design a fruitful health policy that should provide good quality healthcare at low cost to population. Hence, the vital characteristics to design and implement a far-sighted policy for healthcare that can trigger clinical/cost–effectiveness of target therapies should be discussed [2].
Anaplastic lymphoma kinase (ALK) rearrangement is present in 3–5% of NSCLCs [3,4]. Crizotinib is an orally administered ALK tyrosine kinase inhibitor, it displays remarkable efficacy as first generation targeted agents. Compared with chemotherapy, crizotinib therapy improved survival and response rate, as well as a better quality of life [5–7]. It initiates significant shrinking of tumors in approximately 90% of patients with ALK-positive NSCLC [8]. Crizotinib has a 75% response rate versus 45% for chemotherapy in a first-line setting [6,9]. The results from the Profile 1014 study showed that the median progression-free survival (PFS) of crizotinib was 10.9 months. This is significantly longer than PFS with pemetrexed plus platinum chemotherapy [6], and also provides a new benchmark for overall survival, highlighting the benefit of crizotinib for prolonging survival [10].
There are some studies about the assessment of the economic value of crizotinib. Djalalov et al. reported crizotinib first-line therapy is not cost-effective, by using a Markov model from the Canadian public health, due to the high-drug cost and a low biomarker frequency in the population [11]. Crizotinib was approved for ALK-positive advanced NSCLC in mainland China in 2013. The crizotinib patient assistance program (PAP) was implemented for Chinese patients who tested ALK positive to help them afford it. It was reported that in the PAP setting, crizotinib therapy is a cost-effective alternative, compared with pemetrexed plus platinum chemotherapy by PROFILE 1014 trial data analysis [12]. However, it is difficult to ascertain response in the real-world situation. First, PFS in the real-world is longer than it would be in randomized clinical trials because, some patients can benefit from continuing crizotinib treatment beyond disease progression (CBPD) [13–16]. Second, the chemotherapy regimen used in clinical practice in the real-world is not just the pemetrexed platinum scheme, but also other schemes, or chemotherapy combined with anti-angiogenesis drugs. Finally, most chemotherapeutic drugs were covered by medical insurance (MI) since 2010 [17]. Pemetrexed and anti-angiogenesis drugs were included in MI since 2017 [18,19]. Crizotinib has been covered by the critical disease insurance in Chengdu, Sichuan Province, China since 2016 [20].
We carried out this real-world study to assess the cost–effectiveness of first-line crizotinib versus chemotherapy for ALK positive metastatic NSCLC under the different MI situations. The analysis of this research provides evidence for crizotinib’s socio economic consequences on the healthcare system, and supports clinical and economic-effectiveness of personalized medicines.
Methods
Data & sources
From June 2010 to June 2016, a total of 163 advanced ALK positive NSCLC patients with no systemic treatment were collected from West China Hospital, Sichuan University (Chengdu, China), with a median follow-up of 27.67 months. The data were retrieved from the hospital information system of West China Hospital, which can guarantee the completeness and the quality of the data. In addition, due to the treatment requirement for advanced NSCLC patients, the quality of follow-up could be ensured in this study. Eligible patients were aged at least 18 years old, with histologically or cytopathologically confirmed newly diagnosed stage IIIB/IV, and with the presence of at least one documented ALK rearrangement, with the treatment of crizotinib or platinum-based chemotherapy as the first-line therapy. Patients were ineligible if they received crizotinib and platinum-based chemotherapy at the same time during the study period. Patients were categorized into two groups as treated with crizotinib (n = 83) or chemotherapy (n = 80) as a first-line therapy.
Measures of the study
The primary clinical outcome was the PFS and the main economic outcome is the incremental cost–effectiveness ratio (ICER). The PFS of chemotherapy was defined as: the time from initiation of treatment to RECIST-defined disease progression (PD), or death from any cause. The total PFS of crizotinib was defined as: from initiation of treatment, to the end of treatment or death from any cause. If the patient was last known to be progression-free, then the study period end date was used for censoring. Adverse events (AE) were classified and graded according to Common Terminology Criteria for Adverse Events, version 4.0.
This analysis used the perspective of the Chinese healthcare, only direct medical costs data were considered. Costs data were collected from the hospital information system. The total direct medical costs for each patient were calculated as the sum of all cost categories. Since the end of 2016, the price of crizotinib has fallen 10% in Sichuan, Chengdu. Crizotinib was covered by the critical disease insurance. Mean cost per patient over the entire period was calculated by summing the totals and then dividing the sum by the sample size in each arm. Costs were discounted at an annual rate of 3%, in line with Chinese guidelines for pharmacoeconomic evaluations. The costs are shown in 2017 US dollars (1USD = 6.74 RMB). Since health utility measurements were not available in the real-world setting, literature-based utility weights were used [5].
In China, Pfizer and the China Primary HealthCare Foundation are currently implementing a PAP. PAP allows ALK-positive NSCLC patients that received crizotinib to pay US$31750.74 for the first year of treatment and US$15875.37 for the second year until to PD with the doctor’s assessment. When crizotinib costs were partly paid by public healthcare payers in Chengdu, the patients need to pay US$21364.9 for the first year and US$14243.32 for the second year until to PD.
For the residents living in Chengdu, reimbursement was provided by the universal government-sponsored insurance plan. The detailed reimbursement ratio of the drugs referred to the Sichuan Drug Catalog for Basic Medical Insurance, Work-Related Injury Insurance, and Maternity Insurance (2010 Edition) before the end of 2016 [18]. According to the MI policy, Drugs of class A and B were covered by 100 and 80% separately. The new reimbursement rules referred to the National Drug Catalog for Basic Medical Insurance, Work-Related Injury Insurance and Maternity Insurance (2017 Edition) [19]. Pemetrexed, bevacizumab and endostatin were included into drug catalog of Medical Insurance as class B from 2017 [18]. Crizotinib was included into Medical Insurance for Major Diseases in Chengdu at the end of 2016 and reimbursement ratio was calculated as 70% [20]. In addition, for the other costs besides the drug cost, reimbursement ratio was calculated as 70% referring to Chengdu medical service and price item (announced by the Ministry of Human Resources and Social Security of Chengdu, 2016 version) [21].
The main economic outcome is the ICER. Health benefits were expressed as life years (LYs), and quality-adjusted life-years (QALYs) gained. The ICER was calculated by dividing the incremental cost difference between the two strategies, by the incremental difference in health outcomes (LYs and QALYs). We used 3× the per capita gross domestic product (GDP) of Sichuan in 2017 (US$6607.83) as the cost–effectiveness threshold according to the WHO recommendations.
Data analysis & procedure
For statistical methods included in this study, continuous variables are presented as mean, standard deviation, median and range per group. Categorical variables are expressed as percentage. For the comparison test, two-tailed Student’s t-test for the continuous variables, and Fisher's exact test, or Chi-square test were used for the categorical variables as appropriate. Survival curves for PFS were plotted using the Kaplan–Meier method. Medians and the associated 95% CIs were computed. The differences were assessed by the log-rank test. All tests were two-sided, with statistical significance at p < 0.05. In addition, propensity score matching (PSM) was used to adjust significant differences in patient characteristics and reduce the influence of possible confounding factors. Logistic regression was calculated with the covariates, age, gender, disease period, smoking status, histopathology, ECOG performance status, metastatic status and ALK-rearranged test methods. A total of eight variables were included, and one-to-one nearest-neighbor matching without replacement was performed with a caliper of width equal to 0.2. Analyses were conducted with the R statistical package v.2.13.1 (R Foundation for Statistical Computing, Vienna, Austria).
Probabilistic Sensitivity Analysis (PSA) was performed to assess the impact of uncertainty around the key parameters of the model on the ICER. A second-order Monte Carlo simulation with 1000 iterations was used to run replicated outcomes. The normal distributions used for costs, utility and reimbursement ratio were carried to the specific limits. The results are presented as an Incremental cost–effectiveness scatter plot. In addition, one-way sensitivity analysis for the reimbursement ratio of crizotinib and three chemotherapy drugs (pemetrexed, bevacizumab and endostatin) was also examined.
Results
Patient characteristics
Patients’ characteristics were summarized in Table 1. Except for a little difference in age, it was almost balanced in patients characteristics between crizotinib group and chemotherapy group. The patients in crizotinib group were younger than control group (p = 0.042). PSM was used to adjust for the age differences, and the results were unchanged after PSM (Supplementary Table 4).
| Characteristics | All patients (n = 163) | Crizotinib (n = 83) | Chemotherapy (n = 80) | p-value |
|---|---|---|---|---|
| Age | 0.042 | |||
| – Median (range) | 50 (24.79) | 48 (24.69) | 51.5 (28.79) | |
| – Mean ± standard deviation | 49.82 ± 11.31 | 48.02 ± 11.54 | 51.69 ± 10.83 | |
| – Male Gender -no(%) | 70 (42.9%) | 32 (38.6%) | 38 (47.5%) | 0.320 |
| Stage | 1.000 | |||
| – IIIB | 11 (6.7%) | 6 (7.2%) | 5 (6.2%) | |
| – IV | 152 (93.3) | 77 (92.8%) | 75 (93.8%) | |
| No Smoking status – no (%) | 132 (81.0%) | 67 (80.7%) | 65 (81.2%) | 1.000 |
| Histopathology – no (%) | 0.127 | |||
| – Adenocarcinoma | 150 (92.0%) | 79 (95.2%) | 71 (88.8%) | |
| – Non-adenocarcinoma | 13 (8%) | 4 (4.8%) | 9 (11.2%) | |
| ECOG performance status no (%) | 1.000 | |||
| – 0 or 1 | 146 (89.6%) | 71 (85.5%) | 75 (93.8%) | |
| – 2 or 3 | 17 (10.4%) | 12 (14.5%) | 5 (6.2%) | |
| Metastatic status | ||||
| – Brain metastases present | 47 (28.8%) | 26 (31.3%) | 21 (26.3%) | 0.588 |
| – Bone metastases present | 60 (36.8%) | 31 (37.3%) | 29 (36.3%) | 1.000 |
| – Extra-pulmonary metastases present | 66 (40.5%) | 34 (41.0%) | 32 (40%) | 1.000 |
| ALK rearranged test | 0.159 | |||
| – Ventana IHC | 65 (39.9%) | 38 (45.8%) | 27 (33.8%) | |
| – FISH | 98 (60.1) | 45 (54.2%) | 53 (66.2%) |
ALK: Anaplastic lymphoma kinase; ECOG: Eastern Cooperative Oncology Group; FISH: Fluorescent in situ hybridization; IHC: Immunohistochemistry.
Base-case analysis
In this study, crizotinib was administered at a dose of 250 mg orally, twice per day, with proper adjustments as needed. Conventional chemotherapy as the first-line treatment regimen was as follows: 55% were pemetrexed plus platinum chemotherapy, 12.5% were paclitaxel plus platinum chemotherapy, 3.8% were etoposide plus platinum chemotherapy, 12.5% were combined chemotherapy with anti-angiogenesis like bevacizumab and endostatin. There was a significant improvement in objective response rate and disease control rate for the crizotinib group compared with the chemotherapy group (objective response rate: 48.2 vs 7.5%, respectively; p < 0.001; disease control rate: 95.2 vs 81.3%, respectively; p = 0.011; Supplementary Table 1). The median-PFS in the crizotinib group was significant longer than it was in chemotherapy (13.9 vs 5.47 m, respectively; p < 0.001; Supplementary Figure 1). At the data cut off, 67 patients who received crizotinib had primary PD and 30 patients were decided by physicians to continue CBPD, where 56.7% of the patients were brain metastasis. The results in survival analysis showed that the patients taking crizotinib prolonged total median PFS compared with the chemotherapy group (19.67 vs 5.47 m, respectively; p < 0.001; Figure 1).
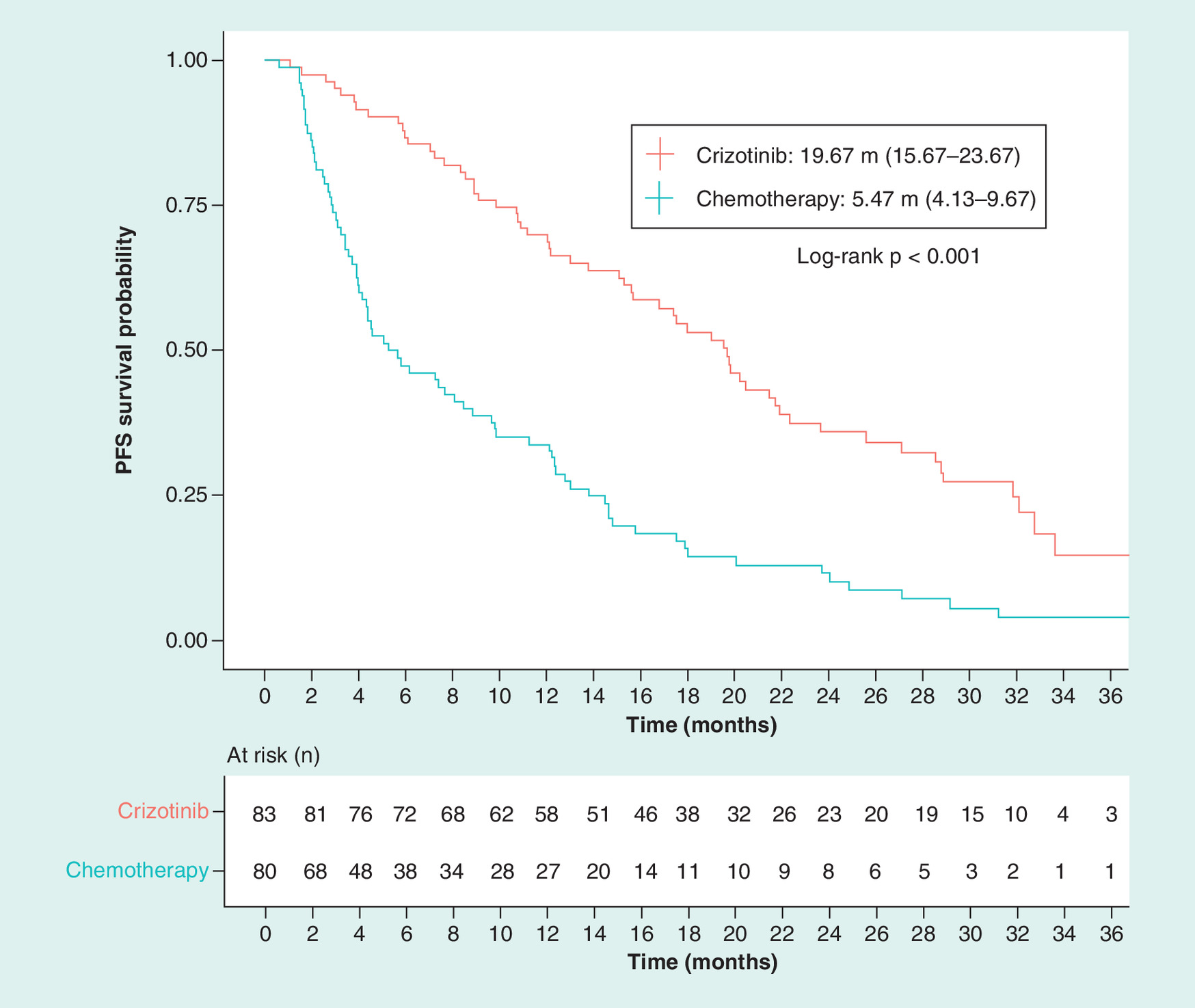
Figure 1. Kaplan–Meier analysis comparing total progression-free survival between the patients treated with crizotinib and chemotherapy as first-line therapy for anaplastic lymphoma kinase positive non-small-cell lung cancer.
PFS: Progression-free survival.
The related AE were summarized in Supplementary Table 2. The most common AE with crizotinib was hepatic toxicity, with 2.4% of the patients reaching 3 grade. The most common AE with chemotherapy was hematologic toxicity, with 8% of patients at 3 grade.
The costs were summarized in Table 2. The cost of crizotinib is higher than the anticancer drug cost in chemotherapy group. However for the other costs, including costs for AE Management, Examination and Hospitalization in crizotinib were less than in chemotherapy. The majority of the total cost was the anticancer cost for both groups. Due to crizotinib, pemetrexed, bevacizumab and endostatin being covered by MI after the end of 2016, the total cost for patients’ perspective decreased significantly.
| Cost/patient (95% CI) | Before the end of 2016 | After the end of 2016 | ||||
|---|---|---|---|---|---|---|
| Crizotinib (n = 83) | Chemotherapy (n = 80) | p-value | Crizotinib (n = 83) | Chemotherapy (n = 80) | p-value | |
| Anticancer drug | 44942.5 (43159.06, 46725.94) | 8146.12 (5918.71, 10373.53) | <0.05 | 9846.06 (9367.18, 10324.94) | 1724.29 (1280.59, 2167.99) | <0.05 |
| Adverse event management | 20.53 (9.56, 31.5) | 35.13 (23.2, 47.06) | <0.05 | 20.53 (9.56, 31.5) | 35.13 (23.2, 47.06) | <0.05 |
| Radiotherapy | 239.76 (143.37, 336.1) | 384.87 (231.68, 538.06) | 0.85 | 239.76 (143.37, 336.15) | 384.87 (231.68, 538.06) | 0.85 |
| Hospitalization | 111.25 (42.03,180.47) | 190.15 (146.88, 233.42) | <0.05 | 111.25 (42.03, 180.47) | 190.15 (146.88, 233.42) | <0.05 |
| Examination | 904.32 (786.85, 1021.79) | 1161.9 (1011.73, 1312.07) | <0.05 | 904.32 (786.85, 1021.79) | 1161.9 (1011.73, 1312.07) | <0.05 |
| Other costs† | 495.59 (342.34, 648.84) | 873.22 (646.44, 1100) | <0.05 | 495.59 (342.34, 648.84) | 873.33 (646.44, 1100) | <0.05 |
| Total cost‡ | 46713.94 (44788.08, 48639.8) | 10791.4 (8351.65, 13231.15) | <0.05 | 11617.51 (10953.93, 12281.09) | 4369.56 (3624.05, 5115.07) | <0.05 |
†
Other costs were included materials, support solution and so on.
‡
Total costs were calculated from the patient’s perspective.
The results of cost–effectiveness are reported in Table 3. The base-case results indicate that crizotinib would result in a longer PFS, more LYs (1.18 years) and QALYs (0.99 years) for the clinical benefit. Before the end of 2016, the ICER was US$30442.83 per LYs gained, and US$36285.39 per QALYs gained, and both of them were more than willingness to pay (WTP; 3 × GDP). After the end of 2016, the ICER dropped notably considering the new MI policy. Not only the ICER was US $6142.33 per LYs gained, which was less than 1 × GDP for Sichuan province, China, but also the ICER was US$7321.16 per QALYs, which was less than 1 × GDP for China. Both of them were less than WTP. Based on these findings, crizotinib can be considered a cost-effective option for advanced ALK positive patients comparing with chemotherapy, even after all the chemotherapy drugs were covered by MI.
| Group | Strategy | Cost (US$) | PFS LYs | ICER/LYs | PFS QALYs | ICER/QALYs |
|---|---|---|---|---|---|---|
| Before the end of 2016 | – Crizotinib without MI | 46713.94 | 1.64 | 1.31 | ||
| – Chemotherapy with partly MI | 10791.40 | 0.46 | 30442.83† | 0.32 | 36285.39† | |
| After the end of 2016 | – Crizotinib with MI | 11617.51 | 1.64 | 1.31 | ||
| – Chemotherapy with MI | 4369.56 | 0.46 | 6142.33‡ | 0.32 | 7321.16§ |
†
>3 × GDP of China.
‡
<1 × GDP of Sichuan Province China.
§
<1 × GDP of China.
GDP: Gross domestic product; ICER: Incremental cost–effectiveness ratio; LY: Life Year; MI: Medical insurance; PFS: Progression-free survival; QALY: Quality-adjusted life year.
Sensitivity analysis
To drive robust estimations of incremental LYs, QALYs and costs, the PSA was performed using a second-order Monte Carlo simulation with 1000 iterations to run replicated outcomes. The setting of all parameters in PSA were listed in Supplementary Table 3. The probability sensitivity analysis revealed that all the simulation results for ICER fell within the first, and fourth quadrants. More than 90% of the results were located in the first quadrant (Figure 2). Moreover, more than 99% of sampled ICERs were below a threshold of WTP. These results indicated that compared with chemotherapy, crizotinib showed cost–effectiveness in more than 99% of probability, considering a cost–effectiveness threshold of a 3 × GDP per capita in 2017 in Sichuan when crizotinib and all the anticancer drugs were covered by MI. In addition, one-way sensitivity analysis for reimbursement ratio of crizotinib and three chemotherapy drugs which were covered by MI from 2017 was also assessed (Figure 3). First, six reimbursement ratios of crizotinib including 0%, 60–100% were assessed as three chemotherapy drugs (pemetrexed, bevacizumab and endostatin) 80% MI covered (green circle). Second, three chemotherapy drugs 60, 80 and 100% MI covered were analyzed as crizotinib 70% MI covered (blue triangle line). The results indicated that the cost-effective tendency for crizotinib increases as the reimbursement ratio increases.

Figure 2. Incremental cost–effectiveness scatter plot for probabilistic sensitivity analyses.
Each point represents the mean incremental cost and effectiveness of crizotinib compared with chemotherapy as first-line therapy for anaplastic lymphoma kinase positive non-small-cell lung cancer.
WTP: Willingness to pay.
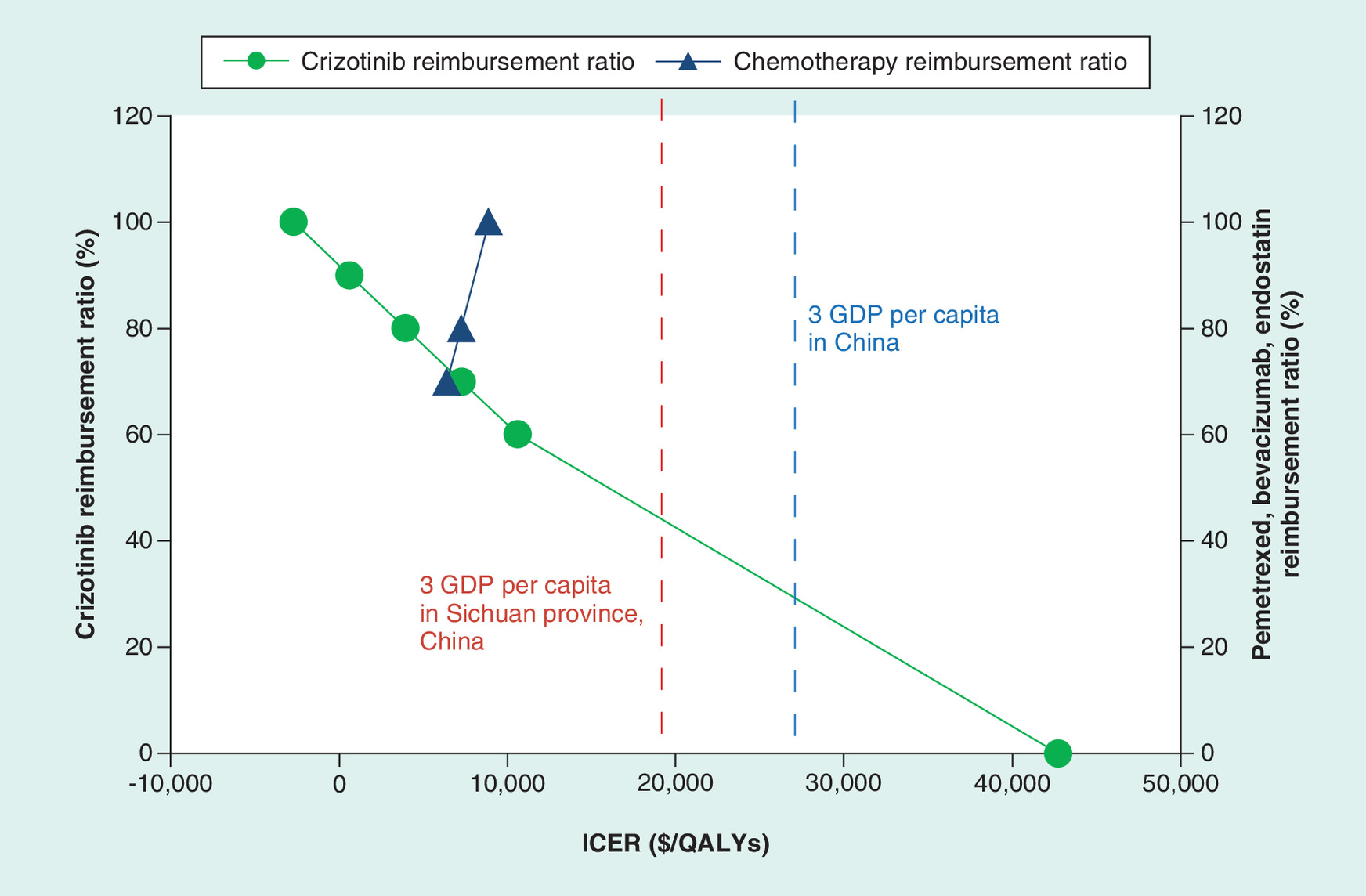
Figure 3. One-way sensitivity analysis for reimbursement ratio of crizotinib and chemotherapy.
QALY: Quality-adjusted life year; GDP: Gross domestic product; ICER: Incremental cost effectiveness ratio.
Discussion
To our knowledge, this is the first study using patient-level real-world data to investigate the cost–effectiveness of crizotinib versus chemotherapy as first-line treatment for ALK-positive advanced NSCLC patients, which is likely to better reflect effectiveness, and resource use than RCT evidence. There are three points to consider. First of all, we reported a median total PFS of 19.67 m after crizotinib treatment, which is more than the PFS of 10.9 m in Profile 1014. Among 67 crizotinib-treated patients with RECIST-defined PD, 30 (45%) continued CBPD. These patients responded to, and exhibited extended PFS from initial crizotinib treatment, and had a site of PD particularly amenable to local therapy (brain). Second, the chemotherapy regimen is not limited to a pemetrexed platinum scheme, but other schemes, or chemotherapy combined with anti-angiogenesis drug were also used. Finally, the change of MI policy was considered in the study. We found crizotinib is a cost-effective choice for ALK-positive NSCLC in comparison with chemotherapy with Chengdu, Sichuan Province MI coverage after 2016.
Dajlalov [11] reported crizotinib first-line therapy was not cost-effective using a Markov model. However, Chouaid provided different comments [22]. The standard first-line treatment strategy was cisplatin-gemcitabine doublet. However, the recommendations for first-line treatment of NSCLC also included other regimens such as pemetrexed concurrently with cisplatin, or at the patients discretion, bevacizumab combined with chemotherapy. If some patients received these high-cost drugs, such as pemetrexed or bevacizumab, it will probably significantly impact the ICER. In our real-world study, 55% were pemetrexed plus platinum chemotherapy, 12.5% were combined chemotherapy with bevacizumab and endostatin. We found crizotinib first-line treatment could be cost-effective compared with chemotherapy with the MI coverage and PAP.
Compared with a recent published model-based economic analysis using PROFILE 1014 trial data analysis [12], the study focused on the assessment of three ALK rearrangement testing methods in combination with crizotinib versus a traditional regimen, as well as the impact of crizotinib PAP. Both of the two studies suggest crizotinib is an effective, and cost-effective first-line treatment for ALK-positive advanced NSCLC compared with chemotherapy.
Although crizotinib has been approved in China since 2013, the clinical practical use was limited due to the high price. What’s more, most chemotherapeutic drugs were covered by MI. Pemetrexed and anti-angiogenesis drugs were also included in MI later. At the end of 2016, crizotinib was covered by MI in Chengdu, Sichuan Province. It caused a major change for the treatment strategy for ALK-positive NSCLC. Our study indicates that crizotinib could be a cost-effective alternative if it is covered by MI. Since the end of 2018, crizotinib has been covered by MI in some other regions of China. This study could benefit healthcare systems in further regions of China currently considering coverage of crizotinib.
Given its retrospective nature, this study had several limitations. First, the results might be limited because of the small sample size in this study. We implemented quality controls to make sure that a consistent conclusion was achieved between the patients diagnosed at different years in the study. We randomly screened 10% of the patients who were diagnosed at different year, and ICER was calculated for these patients respectively. The results showed that the consistent conclusion was obtained. Second, there was selection bias in patient characteristics because the median age for the patients in the crizotinib group is 3 years younger than the patients in chemotherapy group in this study. It suggested that young patients may have a stronger desire for treatment. PSM was used to adjust for significant differences, and similar results were obtained (Supplementary Tables 4–9 and Figures 2–4). Third, since the utility data for Chinese are very limited currently, the utilities included in this study were extracted American utility scores from the literature based on the PROFILE 1007 study [7]. Moreover, sensitivity analysis was performed for the utilities to make sure the conclusions were not influenced by varying the values. Finally, it is difficult to collect all cost data in a real-world situation. We estimated the examination cost based on the routine clinical practice. It is our desire that further study can be based on multicenter randomized trial, or registration study.
In summary, the present study provides valuable real-world evidence that with the Chengdu, Sichuan province MI coverage, crizotinib could be an effective and cost-effective first-line treatment for ALK positive advanced NSCLC compared with chemotherapy.
•
Crizotinib as first generation of anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor, displays remarkable efficacy, improving survival and response rate, as well as a better quality of life compared with chemotherapy. However, the expensive price limited the wide use in clinical practice.
•
This study assessed the cost–effectiveness of crizotinib verses platinum based doublet chemotherapy as the first-line treatment for ALK-positive non-small-cell lung cancer in the real-world setting.
•
The progression-free survival (PFS) was the primary clinical outcome, and the direct medical costs were collected from hospital information systems.
•
Incremental cost–effectiveness ratio (ICER) was calculated with costs and quality-adjusted life years.
•
The results demonstrated that crizotinib improved PFS versus chemotherapy in ALK-positive patients (median PFS 19.67 vs 5.47 m; p < 0.001).
•
Moreover, crizotinib obtained an ICER of US$36,285.39 before the end of 2016, when crizotinib, pemetrexed and anti-angiogenesis drugs were not medical insurance (MI) covered. This is more than the willingness to pay threshold (three-times of gross domestic product per capita in mainland China or Sichuan Province).
•
However, ICER was US$7321.16, which is less than willingness to pay, when crizotinib and all chemotherapy drugs were covered by MI from the end of 2016.
•
These findings suggest that crizotinib could be an effective, and cost-effective first-line treatment for ALK positive advanced non-small-cell lung cancer with the MI coverage currently available in Chengdu, Sichuan Province, China.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Acknowledgments
This work was supported by National Key Research and Development Program of China (No. 2018YFC1311400/2018YFC1311402). The authors would like to thank D Kang in the Department of EBM and Clinical Epidemiology, West China Hospital for professional guidance, and helpful suggestions. Our sincere thanks also, to F Liu of Pfizer Medical for support with the literature review.
Financial & competing interests disclosure
The funding for the data analysis of this study was sponsored by Pfizer China. The study sponsor did not interfere with the study design, data collection or writing of this manuscript. L Li is an employee of Palan DataRx Co. Ltd, a research consulting company receiving industry funds to conduct health economics, and outcomes research in China. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations.
Supplementary Material
File (suppl_file.doc)
- Download
- 557.00 KB
References
1.
Coccia M. Evolutionary growth of knowledge in path-breaking targeted therapies for lung cancer: radical innovations and structure of the new technological paradigm. Int. J. Behav. Healthcare Res. 3(3/4), 273–290 (2012).
2.
Coccia M. Path-breaking target therapies for lung cancer and a far-sighted health policy to support clinical and cost–effectiveness. Health Pol. Technol. 3(1), 74–82 (2014).
3.
Soda M, Choi YL, Enomoto M et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature 448(7153), 561–566 (2007).
4.
Rikova K, Guo A, Zeng Q et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell 131(6), 1190–1203 (2007).
5.
Ou SH, Bartlett CH, Mino-Kenudson M et al. Crizotinib for the treatment of ALK-rearranged non-small cell lung cancer: a success story to usher in the second decade of molecular targeted therapy in oncology. Oncologist 17(11), 1351–1375 (2012).
6.
Solomon BJ, Mok T, Kim DW et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 371(23), 2167–2177 (2014).
7.
Blackhall F, Kim DW, Besse B et al. Patient-reported outcomes and quality of life in PROFILE 1007: a randomized trial of crizotinib compared with chemotherapy in previously treated patients with ALK-positive advanced non-small-cell lung cancer. J. Thorac. Oncol. 9(11), 1625–1633 (2014).
8.
Hamidaddin MA, AlRabiah H, Darwish IA. Development and comparative evaluation of two immunoassay platforms for bioanalysis of crizotinib: a potent drug used for the treatment of non-small cell lung cancer. Talanta 201, 217–225 (2019).
9.
Molnar TF, Szipocs A, Szalai Z. Neoadjuvant crizotinib for ALK re-arranged NSCLC? J. Thorac. Oncol. 14(4), 574–576 (2019).
10.
Solomon BJ, Kim DW, Wu YL et al. Final overall survival analysis from a study comparing first-line crizotinib versus chemotherapy in ALK-mutation-positive non-small-cell lung cancer. J. Clin. Oncol. 36(22), 2251–2258 (2018).
11.
Djalalov S, Beca J, Hoch JS et al. Cost–effectiveness of EML4-ALK fusion testing and first-line crizotinib treatment for patients with advanced ALK-positive non-small-cell lung cancer. J. Clin. Oncol. 32(10), 1012–1019 (2014).
12.
Lu S, Zhang J, Ye M et al. Economic analysis of ALK testing and crizotinib therapy for advanced non-small-cell lung cancer. Pharmacogenomics 17(9), 985–994 (2016).
13.
Ou SH, Janne PA, Bartlett CH et al. Clinical benefit of continuing ALK inhibition with crizotinib beyond initial disease progression in patients with advanced ALK-positive NSCLC. Ann. Oncol. 25(2), 415–422 (2014).
14.
Lei YY, Yang JJ, Zhong WZ et al. Clinical efficacy of crizotinib in Chinese patients with ALK-positive non-small-cell lung cancer with brain metastases. J. Thorac. Dis. 7(7), 1181–1188 (2015).
15.
Hong X, Chen Q, Ding L et al. Clinical benefit of continuing crizotinib therapy after initial disease progression in Chinese patients with advanced ALK-rearranged non-small-cell lung cancer. Oncotarget 8(25), 41631–41640 (2017).
16.
Duruisseaux M, Besse B, Cadranel J et al. Overall survival with crizotinib and next-generation ALK inhibitors in ALK-positive non-small-cell lung cancer (IFCT-1302 CLINALK): a French nationwide cohort retrospective study. Oncotarget 8(13), 21903–21917 (2017).
17.
Sichuan Provincial Human Resources and Social Security Department. Sichuan drug catalog for basic medical insurance work-related injury insurance, and maternity insurance 2010 (2018). http://www.sc.hrss.gov.cn/bsfw/shbx/ylbx_1/xgzc/201311/t20131106_12903.html
18.
Sichuan Provincial Human Resources and Social Security Department. National drug catalog for the basic medical insurance, work-related injury insurance, and maternity insurance 2017 (2018). http://www.sc.hrss.gov.cn/zwgk/zcwj/201710/t20171010_64835.html
19.
Sichuan Provincial Human Resources and Social Security Department. Thirty-six negotiated drugs included in medical insurance drug list 2017 (2018). http://www.sc.hrss.gov.cn/zwgk/zcwj/201710/t20171010_64835.html
20.
Chendu Human Resources and Social Security Bureau. Critical illness insurance program in Chengdu (2019). http://cdhrss.chengdu.gov.cn/cdrsj/c113823/2016-11/18/content_f48facef6c884ad8a86297d3359ca88d.shtml
21.
Ministry of Human Resources and Social Security of Chengdu. Chengdu medical service and price item 2016 (2019). http://cddrc.chengdu.gov.cn/cdfgw/c120782/201604/06/content_560db5ac065e4e84b7d9c4856918468a.shtml
22.
Chouaid C, Borget I, Vergnenegre A. Targeted therapies in non-small-cell lung cancer management: no cost-effective strategies? J. Clin. Oncol. 32(31), 3577 (2014).
Information & Authors
Information
Published In
Pages: 93 - 102
PubMed: 31958984
Copyright
© 2020 Future Medicine Ltd.
History
Received: 12 June 2019
Accepted: 22 October 2019
Published online: 21 January 2020
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Crizotinib versus chemotherapy: a real-world cost–effectiveness study in China. (2020) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2019-0075
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Ruimin Liu, Chunrong Su, Hang Su, Lisen Wang, Prognostic analysis and development of a prognostic model for EML4-ALK-positive lung cancer patients treated with ALK-TKIs, Frontiers in Medicine, 10.3389/fmed.2026.1760300, 13, (2026).
- Ruijuan Liu, Huihui Liu, Haoyang Chen, Ke An, Jingyao Wei, Ji Zhang, Yue Du, Yueqin Wang, Xin Tian, N6-methyladenosine reader YTHDF3-mediated Lcn2 mRNA stability promotes the hepatotoxicity of crizotinib , Toxicological Sciences, 10.1093/toxsci/kfaf154, 209, 1, (2025).
- Wanjie Zhang, Yuqiong Lu, Zhanjing Dai, Linning Wang, Yang Zhou, Yun Lu, Feng Chang, Cost-effectiveness of iruplinalkib versus crizotinib in first-line anaplastic lymphoma kinase-positive advanced non-small-cell lung cancer patients in China, Frontiers in Pharmacology, 10.3389/fphar.2025.1651463, 16, (2025).
- Lara Chayab, Natasha B. Leighl, Mina Tadrous, Christine M. Warren, William W. L. Wong, Trends in Real-World Clinical Outcomes of Patients with Anaplastic Lymphoma Kinase (ALK) Rearranged Non-Small Cell Lung Cancer (NSCLC) Receiving One or More ALK Tyrosine Kinase Inhibitors (TKIs): A Cohort Study in Ontario, Canada, Current Oncology, 10.3390/curroncol32010013, 32, 1, (13), (2024).
- Yajie Gu, Bing Liu, Xiaonan Lin, Jinjin Chen, Xin Chen, Yingshuo Jiang, Yifan Zhu, Xin Li, Sheng Lou, Junrong Zhu, Assessing the cost-effectiveness of replacing antimetabolites with mTOR inhibitors in heart transplant immunosuppression in China: a network meta-analysis-based economic evaluation, International Journal of Clinical Pharmacy, 10.1007/s11096-024-01793-z, 46, 6, (1472-1481), (2024).
- Jing Wang, Xiao-yu Xu, Xin-yue Li, Jian-chao Luo, Zhe-yan Zhang, Jing Chen, Jian-ping Cai, Li-kang Zhang, Jian-chang Qian, The impact of CYP3A4 genetic polymorphism on crizotinib metabolism and drug-drug interactions, Toxicology and Applied Pharmacology, 10.1016/j.taap.2024.117016, 489, (117016), (2024).
- Dharna Gupta, Nidhi Gupta, Navneet Singh, Shankar Prinja, Economic Evaluation of Targeted Therapies for Anaplastic Lymphoma Kinase– and ROS1 Fusion–Positive Non–Small Cell Lung Cancer in India, JCO Global Oncology, 10.1200/GO.23.00260, 10, (2024).
- Zixuan He, Xianqin Huang, Dingyi Chen, Guoan Wang, Yuezhen Zhu, Huangqianyu Li, Sheng Han, Luwen Shi, Xiaodong Guan, Sponsorship bias in published pharmacoeconomic evaluations of national reimbursement negotiation drugs in China: a systematic review, BMJ Global Health, 10.1136/bmjgh-2023-012780, 8, 11, (e012780), (2023).
- Linjun Xie, Leyun Ding, Lian Tang, Zuming Yang, Dan Wu, Wenjuan Wang, Juehui Mao, Lu Shi, Chun Liu, Lufen Duan, Jinhui Xu, Qin Zhou, Jiantong Sun, Xinyuan Ding, A real-world cost-effectiveness study of vancomycin versus linezolid for the treatment of late-onset neonatal sepsis in the NICU in China, BMC Health Services Research, 10.1186/s12913-023-09628-9, 23, 1, (2023).
- Lara Chayab, Natalia Konstantelos, Natasha B. Leighl, Mina Tadrous, William W. L. Wong, A Systematic Review of the Cost-Effectiveness Analyses of Anaplastic Lymphoma Kinase (ALK) Inhibitors in Patients with Locally Advanced or Metastatic Non-small Cell Lung Cancer (NSCLC), PharmacoEconomics, 10.1007/s40273-023-01279-2, 41, 8, (945-980), (2023).