Cost associated with hematopoietic stem cell transplantation: a retrospective claims data analysis in Germany
Abstract
Aim: Quantify hematopoietic stem cell transplantation (HSCT) costs in German patients with acute lymphoblastic leukemia (ALL), diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL). Methods: The primary outcome was direct and indirect costs in patients with ALL/DLBCL/FL who received HSCT between 2010 and 2014. Costs were evaluated two to four quarters before to eight quarters after HSCT. Results: Among 258 patients with HSCT, direct costs were €290,125/patient (pediatric ALL), €246,266/patient (adult ALL), €230,399/patient (DLBCL/FL allogeneic) and €107,457/patient (DLBCL/FL autologous). Indirect costs with HSCT were €52,939/patient (adult ALL), €20,285/patient (DLBCL/FL allogeneic) and €29,881/patient (DLBCL/FL autologous). Conclusion: Direct and indirect costs associated with HSCT are substantial for patients with ALL, DLBCL and FL. Novel therapies that reduce HSCT use could reduce medical costs.
Tumors of the hematopoietic and lymphatic systems, such as leukemia and lymphoma, constitute a major disease burden, with approximately 352,000 and 452,000 newly diagnosed cases of leukemia and lymphoma, respectively, worldwide in 2012 [1]. For patients with relapsed/refractory disease, hematopoietic stem cell transplantation (HSCT) is one of the treatment options. The goal of HSCT is to restore the patient's lymphohematopoietic system by replacing the malignant cell population and re-establishing normal blood cell production. HSCT can be autologous (using the patient's own stem cells) or allogeneic (using stem cells from a matched donor) [2].
Despite its potential medical benefit for patients with life-threatening diseases, HSCT is associated with certain clinical risks [3], and with high costs. In Germany, to the best of our knowledge, very limited data have been published on costs associated with HSCT treatment in patients with leukemia and lymphoma. The aim of this study is to fill this gap by investigating costs associated with HSCT based on claims data from a German study population. The following types of leukemia/lymphoma were investigated.
Acute lymphoblastic leukemia
Acute lymphoblastic leukemia (ALL) is a cancer of the blood characterized by an uncontrolled proliferation of lymphoblasts. It is the most common type of leukemia in children (with an incidence peak between 2 and 5 years of age). ALL is usually treated with chemotherapy, comprising an induction phase, a consolidation phase and a maintenance phase that can stretch over several years. For high-risk patients or patients with an early relapse, allogeneic HSCT is a treatment option. However, because of its serious side effects, allogeneic HSCT is generally not recommended for patients older than 65 years [4].
Diffuse large B-cell lymphoma
Diffuse large B-cell lymphoma (DLBCL) is the most common type of aggressive non-Hodgkin lymphoma. The average age at diagnosis is 65–70 years; however, there is considerable variation in patient age, and even children can be affected. DLBCL is usually treated with chemotherapy (often in combination with rituximab). For patients who are heavily pretreated, have refractory disease or are experiencing failure after autologous HSCT, allogeneic HSCT is the main treatment option [5].
Follicular lymphoma
Follicular lymphoma (FL) constitutes the most common type of slow-growing non-Hodgkin lymphoma. Its progression is often asymptomatic and may not require immediate treatment. However, overall survival for patients with FL is highly variable and can range from a few years to more than 30 years. FL can develop into more aggressive types of lymphoma such as DLBCL. Radiation therapy is a potentially curative treatment during the early stage of the disease. Systemic treatments generally involve chemotherapy in combination with rituximab. Autologous HSCT is a treatment option for relapsed chemosensitive patients after treatment with two to three lines of previous chemoimmunotherapies. For younger patients who relapse following autologous HSCT, allogeneic HSCT is a potential treatment option [5,6].
Given the lack of previously published results on HSCT-associated costs in patients with leukemia and lymphoma in Germany, this study aims to quantify costs associated with HSCT in patients with ALL, DLBCL and FL from a German study population. This information can inform policy makers about the burden of HSCT. As a reference, costs were also calculated for age- and sex-matched controls who were diagnosed with ALL, DLBCL or FL; received chemotherapy; and had no HSCT (this was an exploratory objective of the study).
Methods
Study design
This retrospective study was based on German administrative claims data of the Institut für angewandte Gesundheitsforschung Berlin (InGef), formerly known as the Health Risk Institute (HRI). The study was planned and executed following best practice recommendations for secondary data analyses [7,8]. All statistical analyses were conducted using SAS Enterprise Guide version 9.2.
Data sources
The InGef database is a complete, longitudinal claims dataset of approximately 6.7 million patients, comprising 10% of the German statutory health insured population between 2010 and 2015.
External validation of the database showed good accordance with the German population in terms of measures of morbidity, mortality and drug usage [9]. There is also a high persistence of insured persons within the database over time, indicating suitability of the data source for longitudinal epidemiological analyses [9]. The database has been accepted multiple times by official regulatory authorities in Germany as a valid data source [10–14].
The database includes information about utilization of services on a case-by-case level. The most important data elements included in the database are demographic information (including the date of death, if applicable); ambulatory services and ambulatory diagnoses; hospitalization information, including date of admission and discharge, diagnoses and procedures; supply of reimbursed drugs by pharmacies (including the corresponding date of prescribing); reimbursed remedies and aids; and information on times of inability to work as well as disability. To support claims, diagnoses (International Classification of Diseases, 10th Revision, German Modification [ICD-10-GM]) and procedure codes are provided together with costs. Indirect costs are calculated by analyzing inability to work (i.e., number of days a patient is absent from work due to illness) and costs due to productivity loss, which are estimated from the duration of the inability to work.
Study type, selection of study population & inclusion criteria
This was a retrospective cohort study. The index was the quarter when HSCT was performed. The following criteria were used to extract the study population for the cost analysis (Figure 1):
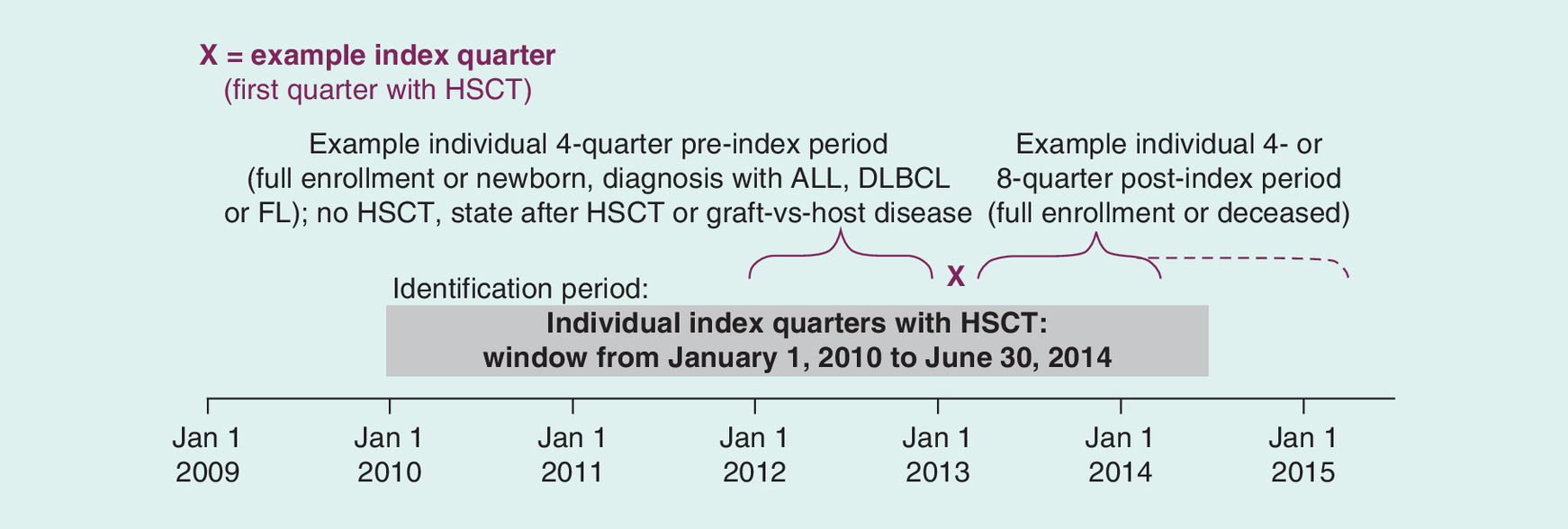
Figure 1. Study design.
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; HSCT: Hematopoietic stem cell transplantation.
Prevalent population inclusion criteria
Treatment with HSCT between January 1, 2010, and June 30, 2014 (identified based on the following OPS codes: 5-411.0*, 5-411.2*, 5-411.3*, 5-411.4*, 5-411.5*, 8-805.0*, 8-805.2*, 8-805.3*, 8-805.4*, 8-805.5*).
Continuous enrollment (or newborn) during the four quarters before the HSCT index quarter (preindex period).
Continuous enrollment (or deceased) during eight quarters after the HSCT index quarter (postindex period).
An ambulatory verified or a primary or secondary hospital diagnosis of ALL (ICD-10-GM C91.0*), DLBCL (ICD-10-GM C83.3) or FL (ICD-10-GM C82*) in the same hospital case as the HSCT. If a patient had diagnoses from more than one of these groups in the same hospital case as the HSCT, assignment was done following the same algorithm as described above for incident patients.
Patients diagnosed with ALL were subdivided into pediatric and adult groups. Patients younger than 18 years at the time of the index quarter were assigned to the pediatric patient group, whereas patients 18 years or older were assigned to the adult group.
To assess costs associated with HSCT as accurately as possible, patients who had already received a transplant in their history were excluded from this study. To achieve this, the following exclusion criteria were applied:
A preexisting diagnosis of HSCT, state after HSCT (ICD-10-GM Z94.80 and Z94.81) or a diagnosis of graft-versus-host disease (ICD-10-GM T86.0*) during 1 year before the index quarter.
Control groups
As a reference, costs were also calculated for age- and sex-matched control groups: a control group for ALL patients and a control group for DLBCL and FL patients combined. The control groups included patients diagnosed with ALL, DLBCL or FL who received chemotherapy treatment but who did not undergo treatment with HSCT. Patients were selected for the control group based on the following inclusion/exclusion criteria:
Control group inclusion criteria
Full enrollment between January 1, 2009, and June 30, 2015 (or newborn/deceased).
An ambulatory verified or primary or secondary hospital diagnosis of ALL, DLBCL or FL between January 1, 2010, and June 30, 2014.
A prescription or procedure code indicating chemotherapy treatment occurring between January 1, 2010, and June 30, 2014, occurring after the first diagnosis of ALL, DLBCL or FL.
Control group exclusion criteria
A pre-existing diagnosis of HSCT, state after HSCT (ICD-10-GM codes: Z94.80 and Z94.81) or a diagnosis of graft-versus-host disease (ICD-10-GM: T86.0*) between January 1, 2009, and June 30, 2015.
As the index quarter, a random quarter with a diagnosis of ALL, DLBCL or FL and an ATC or procedure code indicating chemotherapy was used. Moreover, control groups were constructed in such a way that, at the time of the index quarter, each person in the patient group had one person in the control group with the same indication (ALL or DLBCL/FL), age and sex. Similar to the patient group, costs for the control group were calculated for the index quarter and preindex and postindex periods.
Results
Cost analysis
The total number of patients with a diagnosis of ALL, DLBCL or FL diagnosis between January 1, 2010, and June 30, 2014, in the database was 2119 (713 pediatric ALL and 1406 adult ALL), 3357, and 3423, respectively. The number of patients with HSCT included in the cost analysis is shown in Figure 2. In the observation period, 1879 patients had HSCT, of whom 1687 fulfilled the additional inclusion requirements (no pre-existing diagnosis of HSCT, state after HSCT or diagnosis of graft-versus-host disease during 1 year before the index quarter). A total of 85% (1429 out of 1687) of the observable patients treated with HSCT had other malignant main discharge diagnoses (shown in Table 1) in the hospital where the HSCT took place and were not included in the study population. Analysis of cost was done on the remaining 258 patients with diagnoses under consideration for this study (ALL, DLBCL and FL) and HSCT.
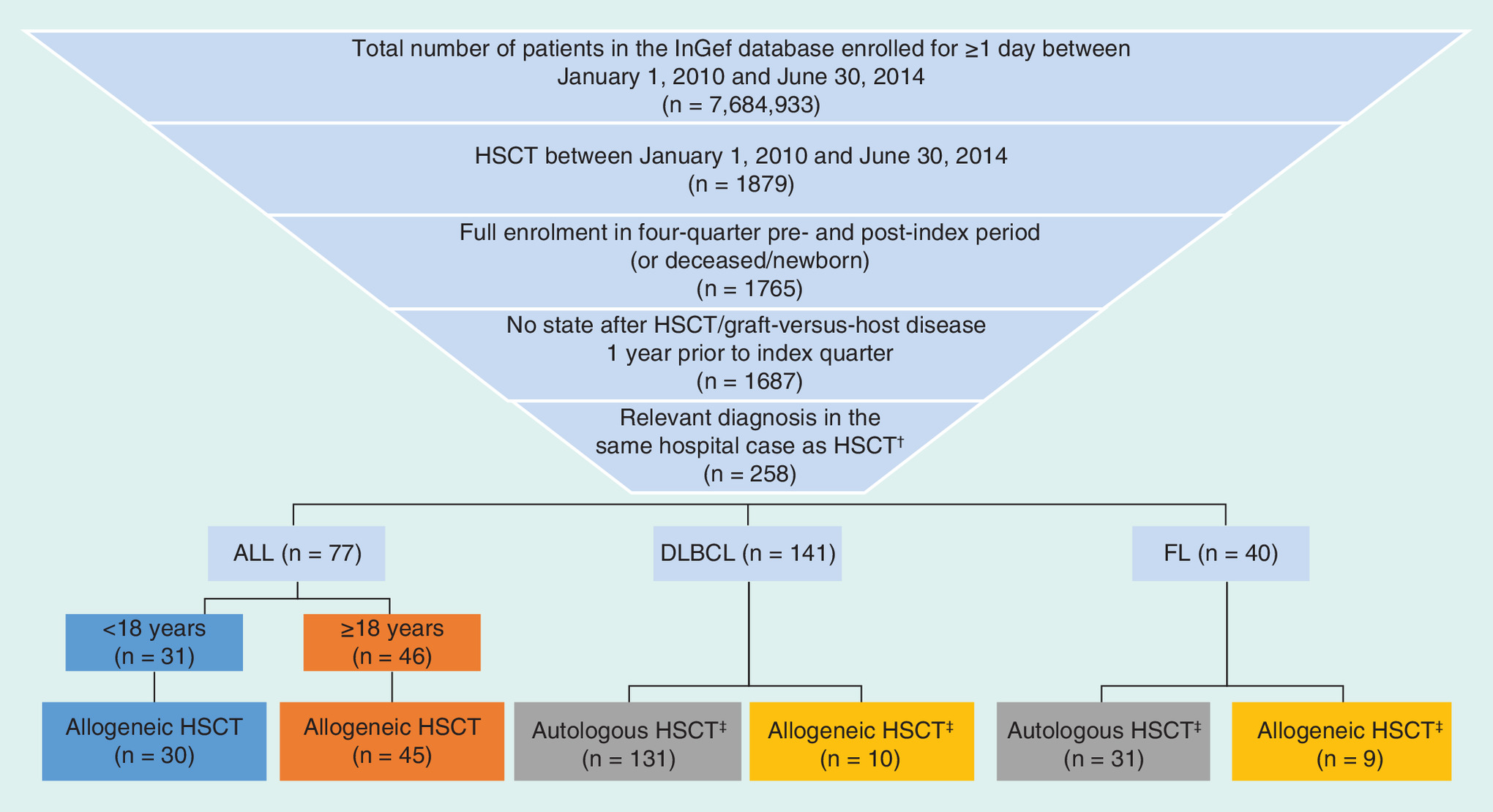
Figure 2. Number of patients evaluated.
†Patients with several diagnoses were assigned to the highest diagnosis group (ALL > DLBCL > FL).
‡For DLBCL/FL patients with an autologous and an allogeneic HSCT, the first HSCT was counted.
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; HSCT: Hematopoietic stem cell transplantation; InGef: Institut für angewandte Gesundheitsforschung Berlin.
| Diagnosis (ICD-10 Code) | N |
|---|---|
| Multiple myeloma and malignant plasma cell neoplasms (C90*) | 513 |
| Myeloid leukemia (C92*) | 340 |
| Anemia in chronic diseases classified elsewhere (D63*) | 318 |
| Myelodysplastic syndromes (D46*) | 71 |
| Hodgkin lymphoma (C81*) | 51 |
| Monocytic leukemia (C93*) | 35 |
| Malignant neoplasm of testis (C62*) | 34 |
| Mature T/NK-cell lymphomas (C84*) | 30 |
| Other | 37 |
| Total | 1429 |
NK: Natural killer.
The age distribution of patients with HSCT differs for the investigated disease entities (Table 2). HSCT is performed mostly in patients with ALL aged <60 years, whereas it is performed in patients aged >40 years in patients with DLBCL and FL.
| Patient group | Mean age, years (SD) | Median age, years | Male, n (%) | Female, n (%) |
|---|---|---|---|---|
| ALL | 26.12 (17.40) | 24 | 46 (60) | 31 (40) |
| – Pediatric | 9.13 (5.26) | 9 | 19 (61) | 12 (39) |
| – Adult | 37.57 (12.66) | 38 | 27 (59) | 19 (41) |
| DLBCL | 56.26 (12.20) | 59 | 94 (67) | 47 (33) |
| FL | 54.30 (8.17) | 54 | 24 (60) | 16 (40) |
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; SD: Standard deviation.
Depending on age and underlying disease, survival rates differed significantly in patients with HSCT. Over the follow-up period of eight quarters, the proportion of surviving patients was 73% (22/30) in pediatric ALL, 47% (21/45) in adult ALL, 32% (6/19) in DLBCL/FL with allogeneic HSCT and 50% (81/162) in DLBCL/FL with autologous HSCT (Figure 3).
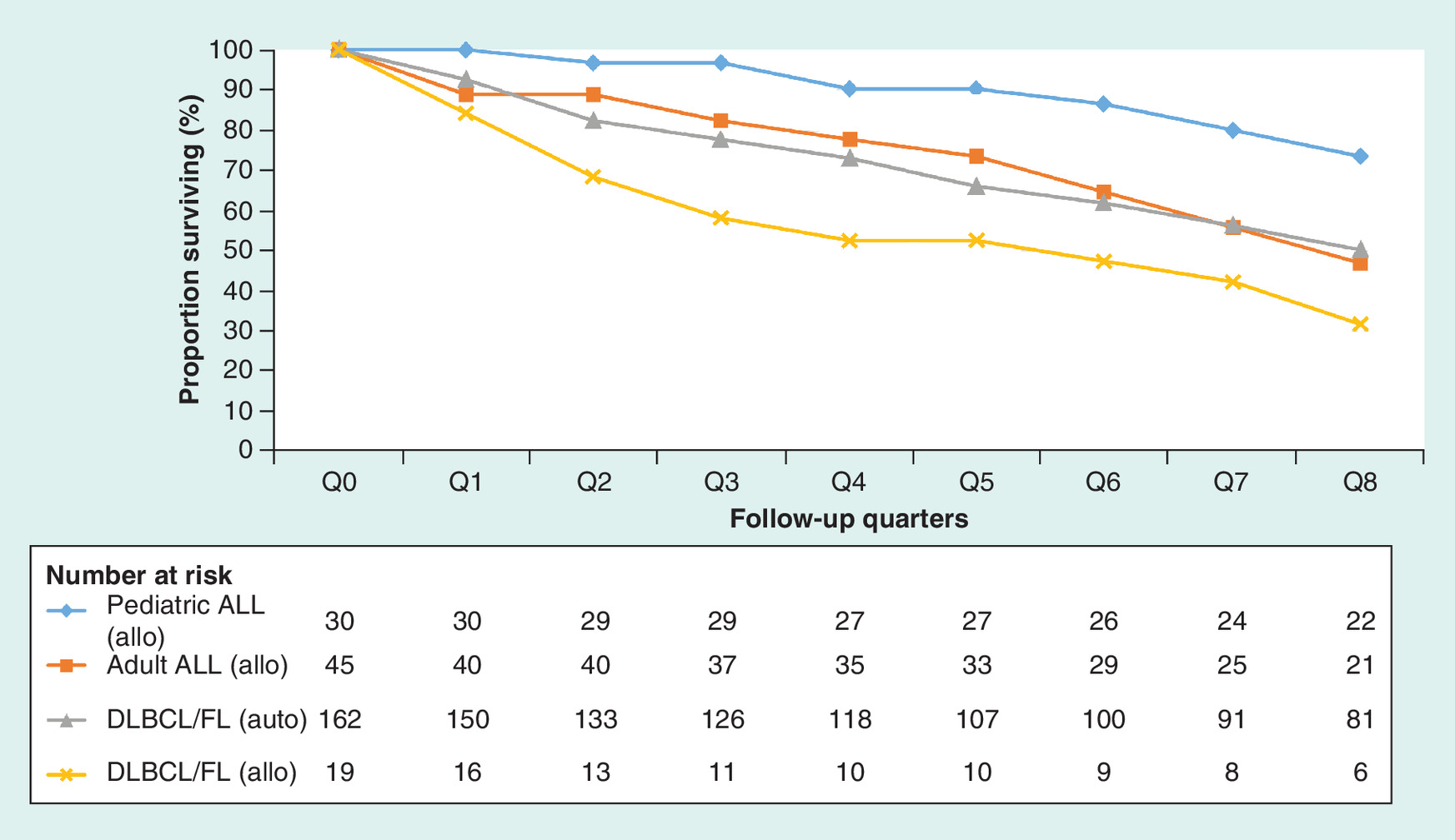
Figure 3. 2-year survival rates of acute lymphoblastic leukemia, diffuse large B-cell lymphoma and follicular lymphoma patients with hematopoietic stem cell transplantation.
ALL: Acute lymphoblastic leukemia; allo: Allogeneic; auto: Autologous; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; Q: Quarter.
Direct total costs for patients with HSCT in each study subpopulation and total costs for the corresponding control groups are shown in Table 3. Mean costs were calculated by dividing the sum of all costs generated within the observation period by the number of all patients with HSCT at the index date. In the period of two quarters before and eight quarters after HSCT, average direct healthcare costs were found to be €290,125 in pediatric ALL, €246,266 in adult ALL, €230,399 in DLBCL/FL with allogeneic HSCT and €107,457 in DLBCL/FL with autologous HSCT. Patients with HSCT had two- to four-times higher total healthcare cost within the observation period of two quarters before and eight quarters after HSCT compared with the age- and sex-matched control groups.
| Group | Mean | SD | 25th percentile | Median | 75th percentile | Min | Max |
|---|---|---|---|---|---|---|---|
| ALL pediatric (allogeneic) | 290,125 | 110,381 | 196,943 | 275,183 | 341,692 | 149,933 | 597,774 |
| – Control | 96,651 | 58,231 | 65,820 | 88,238 | 111,909 | 190 | 286,018 |
| ALL adult (allogeneic) | 246,266 | 107,765 | 171,390 | 215,150 | 282,315 | 92,425 | 497,411 |
| – Control | 85,674 | 74,097 | 33,314 | 78,094 | 115,667 | 159 | 304,039 |
| DLBCL/FL (allogeneic) | 230,399 | 129,136 | 131,195 | 204,896 | 333,734 | 56,701 | 576,534 |
| – Control | 55,201 | 31,701 | 43,929 | 51,277 | 68,127 | 147 | 120,926 |
| DLBCL/FL (autologous) | 107,457 | 54,679 | 74,491 | 91,403 | 115,753 | 34,235 | 328,123 |
| – Control | 54,732 | 37,961 | 34,147 | 47,048 | 64,729 | 64 | 266,919 |
†Data are from the period two quarters before to eight quarters after HSCT and for age- and sex-stratified control groups.
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; HSCT: Hematopoietic stem cell transplantation; Min: Minimum; Max: Maximum; SD: Standard deviation.
In addition to direct costs due to healthcare resource utilization, there are considerable indirect costs incurred by patients with malignant hematologic diseases (Figure 4). Indirect costs comprise sick pay and productivity loss and thus only occur in the adult working population. Productivity loss was estimated by multiplying the number of sick leave days by the average loss of gross value added provided by the German Federal Institute for Occupational Safety and Health (BAuA). Indirect costs in the period two quarters before HSCT to eight quarters after ranged from €20,258 in DLBCL/FL with allogeneic transplant (8.1% of overall cost) to €29,881 in DLBCL/FL with autologous transplant (21.8% of overall cost), and €52,939 in adult ALL patients (17.7% of overall cost).
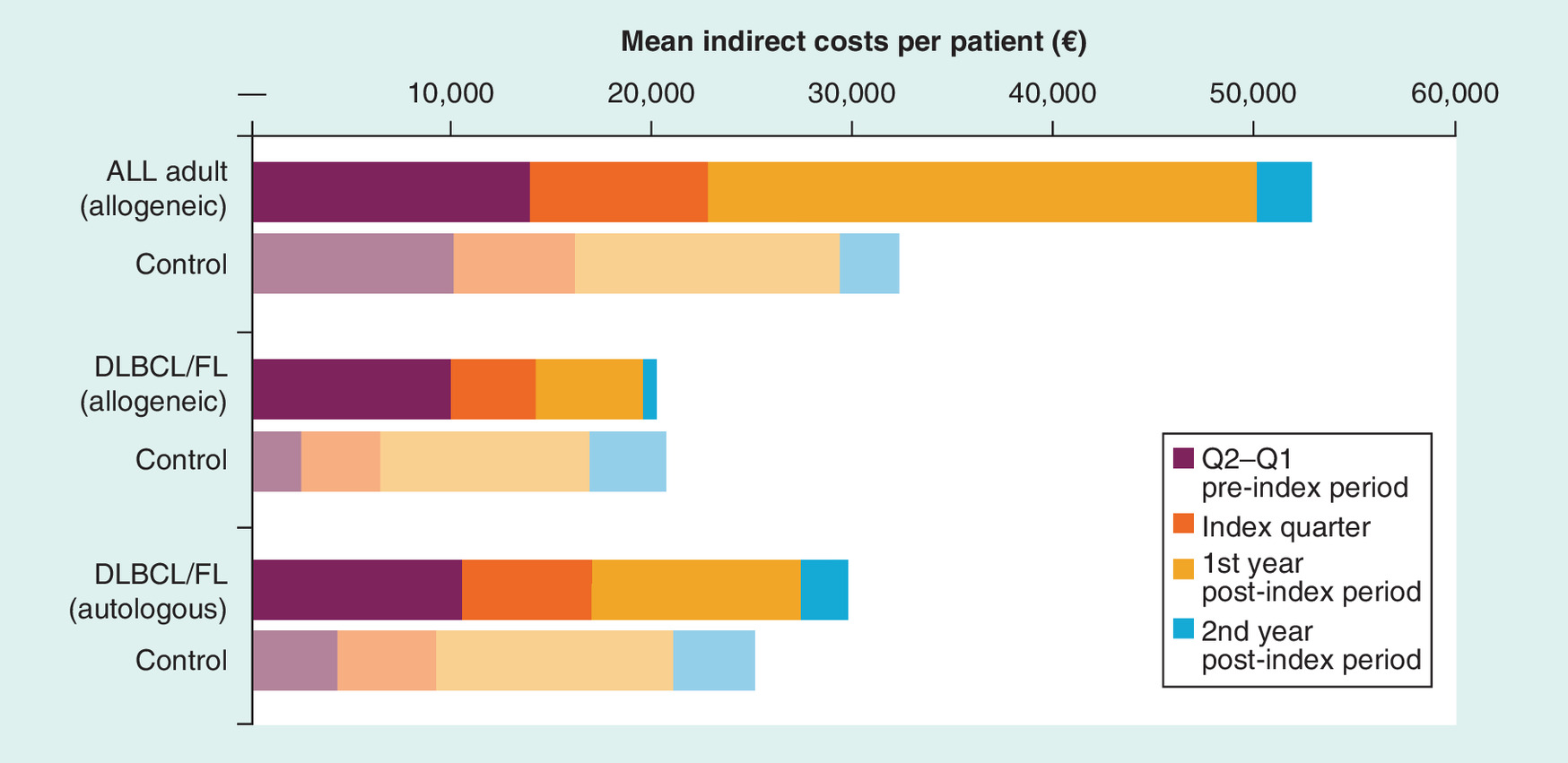
Figure 4. Mean indirect costs per patient (in €) with hematopoietic stem cell transplantation over time versus controls with chemotherapy.
Data are from the period two quarters before to eight quarters after HSCT and for age- and sex-stratified control groups.
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; HSCT: Hematopoietic stem cell transplantation; Q: Quarter.
Independent of the underlying diagnosis, most costs in HSCT patients were incurred from hospital treatment (80–90%), followed by cost for medication (7–14%) and ambulatory cost to a lesser extent (2–5%; Table 4).
| Sector | Mean | Percentage | SD | Median | Min | Max |
|---|---|---|---|---|---|---|
| ALL pediatric (allogeneic) | ||||||
| Hospital | 261,350 | 90.1 | 110,090 | 222,467 | 128,961 | 579,756 |
| Medication | 20,076 | 6.9 | 13,798 | 16,380 | 2902 | 54,886 |
| Ambulatory | 6685 | 2.3 | 5185 | 4824 | 93 | 20,889 |
| Remedies | 1358 | 0.5 | 1672 | 730 | 0 | 5478 |
| Technical aids | 656 | 0.2 | 1160 | 38 | 0 | 4355 |
| Total direct costs | 290,125 | 100.0 | 110,381 | 275,183 | 149,933 | 597,774 |
| ALL adult (allogeneic) | ||||||
| Hospital | 201,876 | 82.0 | 83,509 | 182,446 | 64,765 | 449,611 |
| Medication | 33,847 | 13.7 | 41,892 | 18,794 | 2754 | 224,839 |
| Ambulatory | 9196 | 3.7 | 5288 | 8874 | 1476 | 30,193 |
| Technical aids | 690 | 0.3 | 3207 | 13 | 0 | 21,616 |
| Remedies | 659 | 0.3 | 1307 | 168 | 0 | 7482 |
| Total direct costs | 246,266 | 100.0 | 107,765 | 215,150 | 92,425 | 497,411 |
| DLBCL/FL (allogeneic) | ||||||
| Hospital | 188,574 | 81.8 | 124,394 | 132,226 | 45,963 | 545,822 |
| Medication | 31,501 | 13.7 | 44,075 | 23,709 | 0 | 193,148 |
| Ambulatory | 7886 | 3.4 | 5035 | 7472 | 1453 | 19,273 |
| Technical aids | 1323 | 0.6 | 3006 | 0 | 0 | 9930 |
| Remedies | 1115 | 0.5 | 2130 | 0 | 0 | 7250 |
| Total direct costs | 230,399 | 100.0 | 129,136 | 204,896 | 56,701 | 576,534 |
| DLBCL/FL (autologous) | ||||||
| Hospital | 87,340 | 81.3 | 51,993 | 73,074 | 29,624 | 320,070 |
| Medication | 14,397 | 13.4 | 15,094 | 9080 | 189 | 76,185 |
| Ambulatory | 5077 | 4.7 | 3703 | 4447 | 103 | 22,299 |
| Remedies | 323 | 0.3 | 922 | 0 | 0 | 8963 |
| Technical aids | 320 | 0.3 | 707 | 0 | 0 | 6155 |
| Total direct costs | 107,457 | 100.0 | 54,679 | 91,403 | 34,235 | 328,123 |
†Data are from the period two quarters before to eight quarters after HSCT.
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; HSCT: Hematopoietic stem cell transplantation; Min: Minimum; Max: Maximum; SD: Standard deviation.
Mean direct healthcare costs in patients with HSCT rose in the two quarters before HSCT, building to a peak in the quarter of transplantation before falling again. In year 2 after HSCT in pediatric ALL and DLBCL/FL (autologous), costs were <€20,000. In adult ALL, healthcare costs in year 2 after HSCT were approximately €30,000. The highest average cost per patient in year 2 after HSCT was seen in patients with a diagnosis of DLBCL/FL who received allogeneic HSCT; these costs were higher than in year 1 after HSCT. Pediatric ALL was associated with the highest cost in the quarter of HSCT (€133,585) and lowest cost in year 2 after HSCT (€11,949) compared with the other three subpopulations evaluated (Figure 5).
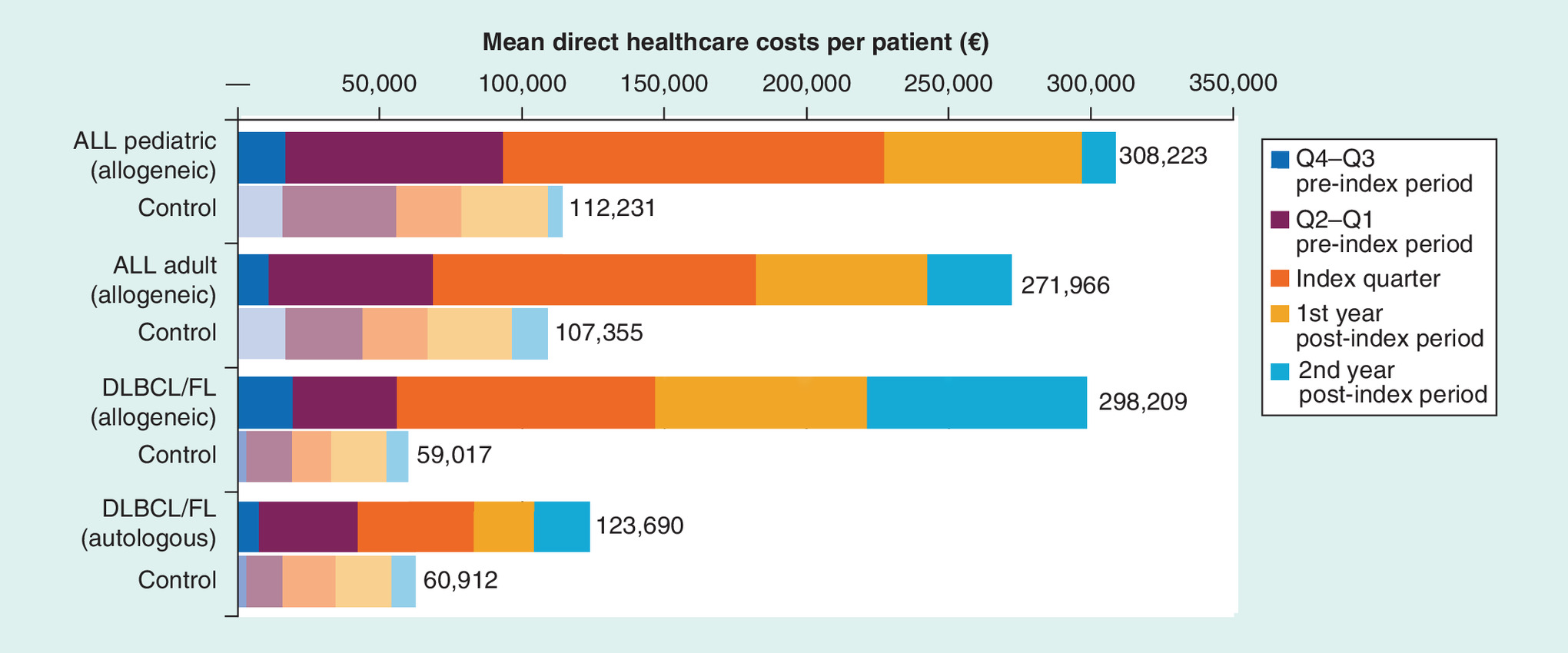
Figure 5. Mean direct healthcare costs per patient (in €) with hematopoietic stem cell transplantation in selected observation periods versus controls with chemotherapy.
ALL: Acute lymphoblastic leukemia; DLBCL: Diffuse large B-cell lymphoma; FL: Follicular lymphoma; Q: Quarter.
Discussion
To the best of our knowledge, this is the first study to investigate costs associated with HSCT in patients with ALL, DLBCL and FL. Results showed that HSCT in the treatment of ALL is associated with substantial healthcare costs. These findings are generally consistent with other recent investigations done in EU countries. Among patients with relapsed/refractory Philadelphia-negative B-cell relapsed/refractory ALL, costs associated with HSCT were €133,965 (including €26,337 for HSCT itself) in Belgium; estimated costs were €118,672 in the HSCT period and €68,344 during chemotherapy before HSCT in France [15,16]. Of note, there were differences in design between the studies. For example, in the French study, the index date was the diagnosis date for ALL, whereas in our study, the index was the HSCT quarter. The French study was based on chart review and separated the chemotherapy and HSCT periods, whereas our study was based on claims data and did not differentiate between the chemotherapy and HSCT periods. Additionally, there may be differences in measurement periods due to data limitations (differences in time to patient death or loss to follow-up). However, we found the results from these studies were generally consistent with our study.
Costs are even higher in the USA. In patients with DLBCL, the average total healthcare cost was estimated to be US$248,390 during the index hospitalization and $455,741 1 year after the index date [17]. In patients with ALL, during the first year following HSCT, the total cost was estimated to be US$683,099 based on two US nationally representative, large claims databases [18]. Consistent with our analysis, hospitalization represented the largest component of the overall cost. Another more recent US claims-based study estimated that the total cost of allogeneic HSCT for patients with ALL was US$669,711 (US$275,642 per patient for the index hospitalization period and US$394,069 during the year following the index period) [19]. In a US study that used a national private claims database (including patients across multiple diagnoses [ICD-9 diagnosis codes]), the median total cost reported for allogeneic HSCT was US$203,026, with the majority of costs incurred during the initial transplant hospitalization [20]. Consistent with our analysis, costs were higher for pediatric patients versus adults and for allogeneic HSCT versus autologous HSCT.
Within the first 2 years after transplantation, healthcare costs were two- to four-times higher compared with age- and sex-matched patients who did not receive HSCT for the same indication. In this study the cost impact of HSCT (i.e., the difference in cost utilized for patients with HSCT vs those without) observed in pediatric ALL was on average almost €200,000 covering an observation period of 1 year before and 2 years after transplant. The cost impact of allogeneic HSCT in adult ALL and DLBCL/FL was €160,000 and €175,000, respectively. Patients receiving autologous HSCT in DLBCL/FL were associated with additional costs of €50,000.
The highest healthcare costs and most intensive healthcare resource utilization in Germany were observed within the first year following the HSCT, which is consistent with results from other studies [18]. The main driver of high economic burden is hospitalizations, which accounted for more than 80% of direct healthcare costs. In addition to direct healthcare cost, the indirect cost in adult patients induced by sick pay and productivity loss add another 15–20% to the potential overall cost.
This analysis was subject to certain limitations. Retrospective claims data analyses are subject to potential coding errors or data omissions. Although the sample size was relatively small, our findings are likely to be representative of the economic burden of allogeneic HSCT in ALL, DLBCL and FL in Germany. To avoid underestimation of the overall economic burden, indirect cost was calculated in terms of sick pay and productivity loss. This calculation did not include further nonmedical and nonpharmacy costs incurred by patients or caregivers, such as temporary housing or transportation. Further research would be warranted to assess the nonmedical and nonpharmacy costs. Selection of patients for the control group was a further limitation of the study. Our control groups included patients diagnosed with ALL, DLBCL or FL who did not receive HSCT. Matching of controls was based on age and sex because the claims database did not include additional information that could be used to match cases with controls (e.g., disease characteristics, comorbidities, prior lines of therapy, time to remission/duration of remission). Because there may have been important differences between the control and study groups that have not been accounted for, the control groups should be regarded as descriptive.
Conclusion
Hematopoietic stem cell transplantation is associated with substantial cost in the treatment of malignant hematopoietic diseases. Indirect cost due to sick leave and consecutive productivity loss constitute relevant additional cost factors in Germany. Novel and effective therapies that reduce HSCT use could potentially reduce total medical costs.
This analysis investigated costs associated with hematopoietic stem cell transplantation (HSCT) (between January 1, 2010, and June 30, 2014) in patients with acute lymphoblastic leukemia (ALL), diffuse large B-cell lymphoma (DLBCL) and follicular lymphoma (FL), based on claims data from a German study population; costs were also calculated for age- and sex-matched controls.
Among 258 patients with HSCT, total direct costs per patient during the observation period were €290,125 (pediatric ALL), €246,266 (adult ALL), €230,399 (DLBCL/FL allogeneic) and €107,457 (DLBCL/FL autologous).
Direct costs in age- and sex-matched controls without HSCT were €96,651, €85,674, €55,201 and €54,732, respectively.
Indirect costs per patient with HSCT were €52,939 (adult ALL), €20,285 (DLBCL/FL allogeneic) and €29,881 (DLBCL/FL autologous).
Indirect costs in age- and sex-matched controls without HSCT were €38,059, €22,483 and €26,395, respectively.
Within the first 2 years after transplantation, healthcare costs are two- to four-times higher in patients who receive HSCT compared with age- and sex-matched controls who do not receive HSCT.
Indirect costs due to sick leave and productivity loss constitute additional costs.
Limitations of this study include the use of a retrospective claims database that could have resulted in data omissions and a relatively small sample size.
Novel therapies that reduce HSCT use could reduce medical costs.
Acknowledgments
A small portion of the research (in 30 pediatric patients with ALL) was presented at the 58th Annual Meeting of the American Society of Hematology in 2016 (Lehne M, Hickstein L, Salimullah T et al. Costs of allogeneic hematopoietic stem cell transplantation [HSCT] in pediatric patients with acute lymphoblastic leukemia [ALL] – an analysis of German claims data. Abstract #5932).
Authors’ contributions
All authors were involved in the conception and design, or analysis and interpretation of the data; L Mayerhoff and J Zhang were involved in the drafting of the paper or revising it critically for intellectual content; and all authors were involved in the final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Financial & competing interests disclosure
This study was financed by Novartis Pharmaceuticals Corporation. Elsevier Health Analytics has received consultancy fees from Novartis for this project. Novartis was involved in the study planning and interpretation of the results. Novartis was not involved in the execution of the analysis. T Salimullah is an employee of Novartis. SK Thomas was an employee of Novartis at the time of the study and is a current employee of Alexion Pharmaceuticals. J Zhang is an employee of and stock holder of Novartis. L Mayerhoff, M Lehne and S Prieur are employees of Elsevier Health Analytics (EHA). EHA received payment from Novartis for analyzing the study data. L Hickstein is an employee of the Health Risk Institute. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Editorial assistance was provided by Rozena Varghese, PharmD, of C4 MedSolutions, LLC (Yardley, PA, USA), a CHC Group company and was funded by Novartis Pharmaceuticals Corporation.
Ethical conduct of research
Anonymized SHI data were used for this research. The data are provided in accordance with paragraphs 287 SGB V and 75 Sozialgesetzbuch (SGB) X of German law. In accordance with German data protection requirements, data on patients and physicians are anonymized, as are the providers and the sickness funds. No regions smaller than federal states or cohorts with less than 100 patients are identified. The use of such data is not subject to ethics committee approval in Germany. All InGef studies need approval from the internal InGef Scientific Research Group, which considers both ethical and scientific aspects of the intended study.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
International Agency for Research on Cancer. GLOBOCAN 2012: estimated cancer incidence, mortality, and prevalence worldwide in 2012. Estimated age-standardised incidence and mortality rates: men (2012). http://globocan.iarc.fr/Pages/fact_sheets_population.aspx.
2.
Copelan EA. Hematopoietic stem-cell transplantation. N. Engl. J. Med. 354(17), 1813–1826 (2006).
• Review of hematopoietic stem cell transplantation (HSCT) and its role in treating hematological malignancies; provides background on costs and complications related to HSCT.
3.
Fielding AK, Richards SM, Chopra R et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 109(3), 944–950 (2007).
• Examined outcomes in adult patients with recurring acute lymphoblastic leukemia, including those who received HSCT; provides data on complications related to HSCT.
4.
Terwilliger T, Abdul-Hay M. Acute lymphoblastic leukemia: a comprehensive review and 2017 update. Blood Cancer J. 7(6), e577 (2017).
5.
Epperla N, Hamadani M. Hematopoietic cell transplantation for diffuse large B-cell and follicular lymphoma: current controversies and advances. Hematol. Oncol. Stem Cell Ther. 10(4), 277–284 (2017).
6.
Mendez M, Torrente M, Provencio M. Follicular lymphomas and their transformation: past and current research. Expert Rev. Hematol. 10(6), 515–524 (2017).
7.
Swart E, Schmitt J. [STandardized Reporting Of Secondary data Analyses (STROSA)-a recommendation]. Z Evid. Fortbild. Qual. Gesundhwes. 108(8–9), 511–516 (2014).
8.
International Society of Pharmacoepidemiology. Guidelines for good pharmacoepidemiology practices (GPP). Pharmacoepidemiol. Drug Saf. 17(2), 200–208 (2008).
9.
Andersohn F, Walker J. Characteristics and external validity of the German Health Risk Institute (HRI) Database. Pharmacoepidemiol. Drug Saf. 25(1), 106–109 (2016).
10.
Institute for Quality and Efficiency in Health Care. Ponatinib – assessment according to § 35a (para. 1, sentence 10) Social Code Book V (dossier assessment [G13-02] (2013). www.iqwig.de/en/projects-results/projects/health-economic/g13-02-ponatinib-assessment-according-to-35a-para-1-sentence-10-social-code-book-v-dossier-assessment.3691.html.
11.
Institute for Quality and Efficiency in Health Care. Brivaracetam – benefit assessment according to §35a Social Code Book V [dossier assessment A16-08] (2016). www.iqwig.de/en/projects-results/projects/drug-assessment/a16-08-brivaracetam-benefit-assessment-according-to-35a-social-code-book-v.7228.html.
12.
Institute for Quality and Efficiency in Health Care. Sacubitril/valsartan – benefit assessment according to §35a Social Code Book V [dossier assessment A15-60] (2016). www.iqwig.de/download/A15-60_Sacubitril-valsartan_Extract-of-dossier-assessment.pdf.
13.
Institute for Quality and Efficiency in Health Care. Secukinumab (plaque psoriasis) – benefit assessment according to §35a Social Code Book V [dossier assessment Nr. 515] (2016). www.iqwig.de/download/A17-08_Secukinumab_Nutzenbewertung-35a-SGB-V_V1-0.pdf.
14.
Institute for Quality and Efficiency in Health Care. Tasimelteon – benefit assessment according to §35a Social Code Book V [dossier assessment Nr. 454] (2016). www.iqwig.de/download/G16-08_Tasimelteon_Bewertung-35a-Abs1-Satz10-SGB-V.pdf.
15.
Dombret H, Thomas X, Chevallier P et al. Healthcare burden and reimbursement of hospitalization during chemotherapy for adults with Ph-negative relapsed or refractory B-cell precursor acute lymphoblastic leukemia in France: a retrospective chart review. J. Med. Econ. 19(11), 1034–1039 (2016).
•• Retrospective review of costs for adult patients with ALL in France; findings are generally consistent with the current analysis.
16.
Maertens J, Graux C, Breems D et al. Retrospective chart review of hospitalizations and costs associated with the treatment of adults with Philadelphia-negative B-cell relapsed or refractory acute lymphoblastic leukemia in Belgium. Acta Clin. Belg. 72(6), 429–433 (2017).
•• Retrospective review of costs for adult patients with ALL in Belgium; findings are generally consistent with the current analysis.
17.
Maziarz RT, Hao Y, Guerin A et al. Economic burden following allogeneic hematopoietic stem cell transplant in patients with diffuse large B-cell lymphoma. Leuk. Lymphoma 59(5), 1133–1142 (2018).
•• Study on costs for patients with DLBCL who received HSCT in the USA; findings show higher costs than observed in the current analysis.
18.
Maziarz RT, Guérin A, Gauthier G et al. Five-year direct costs of acute lymphoblastic leukemia pediatric patients undergoing allogeneic stem cell transplant. Int. J. Hematol. Oncol. 5(2), 63–75 (2016).
•• Study on costs for pediatric patients with ALL who received HSCT in the USA; findings show higher costs than observed in the current analysis.
19.
Zhang X, Song H, Lopez-Gonzalez L, Jariwala-Parikh K, Cong Z. Economic burden of hematopoietic stem cell transplantation (HSCT) in patients with acute lymphoblastic leukemia (ALL) in the US [abstract #3376]. American Society of Hematology 59th Annual Meeting & Exposition. GA, USA, December 9–12 2017.
•• Study on costs for patients with ALL who received HSCT in the USA; findings show higher costs than observed in the current analysis.
20.
Majhail NS, Mau LW, Denzen EM, Arneson TJ. Costs of autologous and allogeneic hematopoietic cell transplantation in the United States: a study using a large national private claims database. Bone Marrow Transplant. 48(2), 294–300 (2013).
Information & Authors
Information
Published In
Copyright
© 2018 Jie Zhang et al.
History
Received: 28 September 2018
Accepted: 29 October 2018
Published online: 5 December 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost associated with hematopoietic stem cell transplantation: a retrospective claims data analysis in Germany. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0100
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Jonas Wißkirchen, Nora S. Rogmann, Michael Greiling, Frederic Ries, Anke Ohler, Georg Hess, Julia Osygus, Healthcare resource utilization analysis in newly diagnosed mantle cell lymphoma: resource alleviation with adoption of the TRIANGLE ibrutinib regimen without autologous stem cell transplantation, Annals of Hematology, 10.1007/s00277-026-07139-1, 105, 8, (2026).
- Karin Berger, Bernhard Moertl, Michael von Bergwelt-Baildon, Dominik Obermüller, Dorota Pawlowska-Phelan, Martin Dreyling, Follicular lymphoma or diffuse large B-cell lymphoma: a population based analysis of epidemiological and health economic aspects in Germany, Annals of Hematology, 10.1007/s00277-025-06592-8, 104, 9, (4625-4635), (2025).
- Priyatesh Chandra Dwivedi, Yasam Venkata Ramesh, Raj Nagarkar, Shorting of existing conditioning regimen for relapsed/refractory gastric diffuse large B-cell lymphoma transplant and studying its related outcomes: A first of its kind case report, Iraqi Journal of Hematology, 10.4103/ijh.ijh_118_24, 14, 1, (131-134), (2025).
- Lynn Leppla, Klaus Kaier, Anja Schmid, Sabine Valenta, Janette Ribaut, Juliane Mielke, Alexandra Teynor, Robert Zeiser, Sabina De Geest, Evaluating the cost, cost-effectiveness and survival of an eHealth-facilitated integrated care model for allogeneic stem cell transplantation: Results of the German SMILe randomized, controlled implementation science trial, European Journal of Oncology Nursing, 10.1016/j.ejon.2024.102740, 74, (102740), (2025).
- Yinglin Liao, Wenxin Zhao, Jing Yang, Jing Li, Juejing Chen, Ziyan Chen, Ling Jin, Longyue Li, Fen Huang, Lingyi Liang, Delayed diagnosis of ocular graft-versus-host disease after allogeneic hematopoietic stem cell transplantation, The Ocular Surface, 10.1016/j.jtos.2024.05.002, 34, (1-8), (2024).
- Marina Hernández-Aliaga, Carlos Carretero-Márquez, Carlos Javier Peña, Enric Santacatalina-Roig, Rut Navarro-Martínez, At-Home Care Versus Total Hospital Care Model for Autologous Stem Cell Transplantation in Adult Lymphoma Patients, Cancer Nursing, 10.1097/NCC.0000000000001407, (2024).
- Nancy V. Kim, Gemma McErlean, Serena Yu, Ian Kerridge, Matthew Greenwood, Richard De Abreu Lourenco, Healthcare Resource Utilization and Cost Associated with Allogeneic Hematopoietic Stem Cell Transplantation: A Scoping Review, Transplantation and Cellular Therapy, 10.1016/j.jtct.2024.01.084, 30, 5, (542.e1-542.e29), (2024).
- Scarlette Pacis, Anna Bolzani, Alexander Heuck, Klaus Gossens, Mathias Kruse, Björn Fritz, Ulf Maywald, Thomas Wilke, Christian Kunz, Epidemiology and Real-World Treatment of Incident Diffuse Large B-cell Lymphoma (DLBCL): A German Claims Data Analysis, Oncology and Therapy, 10.1007/s40487-024-00265-8, 12, 2, (293-309), (2024).
- Karen Fitzner, June M. McKoy, Perspectives on the Cost and Value of Stem Cell and Emerging Therapies, Comprehensive Hematology and Stem Cell Research, 10.1016/B978-0-443-15717-2.00056-1, (446-460), (2024).
- Andrei B. Abrosimov, Dmitry S. Blinov, Ekaterina V. Blinova, Mikhail A. Maschan, RESULTS OF A COMPARATIVE PHRMACOECONOMICS ANALYSIS OF STRATEGIES FOR THE PREVENTION OF GRAFT-VERSUS-HOST DISEASE IN CHILDREN WITH HEMATOLOGICAL MALIGNANCES: A SINGLE CENTER EXPERIENCE, Acta medica Eurasica, 10.47026/2413-4864-2023-1-1-10, 1, (1-10), (2023).