Real-world US healthcare costs of psoriasis for biologic-naive patients initiating apremilast or biologics
Abstract
Aim: Biologics and apremilast have advanced psoriasis management by adding treatment options. This study evaluated persistence, adherence and healthcare costs among biologic-naive patients receiving apremilast or biologics. Methods: Administrative claims data for adults starting apremilast or biologics from 1 January 2013 to 30 June 2016 were matched based on demographics. Results: Apremilast (n = 703) and biologics (n = 1378) had similar baseline characteristics. 12-month persistence and adherence rates were similar. Adjusted total healthcare costs were lower with apremilast versus biologics (p < 0.001) due to lower total outpatient pharmacy costs (p < 0.001). Conclusion: Real-world apremilast users had similar adherence and lower total healthcare costs versus biologic users. Apremilast's cost advantage was evident regardless of whether the patients were persistent or nonpersistent, or switched or did not switch treatments.
Psoriasis is a common systemic inflammatory disorder that affects more than seven million adults in the USA [1–3] and has an incidence of 0.6 new cases per 1000 person-years [4]. The relapsing, remitting condition is chronic in >90% of patients [5], nearly 20% of whom have moderate to severe psoriasis requiring systemic treatment [6]. Psoriasis has a substantial effect on quality of life [5] and is frequently associated with comorbidities, such as obesity, cardiovascular disease, metabolic syndrome and fatty liver, all of which contribute to reduced work capacity, anxiety, depression, sense of stigma and social isolation [1], reduced life expectancy [6], and an accrued socioeconomic burden on individuals and the healthcare system [3,7]. The estimated total annual direct cost to treat psoriasis in the USA (2015) is US$12.2 billion [1].
First-line treatments for mild psoriasis include over-the-counter or prescription topical corticosteroids, tazarotene and vitamin D analogs [8–10]. For patients with moderate to severe psoriasis, phototherapy and systemic medications may be used. Systemic psoriasis treatments include oral agents, such as apremilast, cyclosporine, acitretin and methotrexate [11–13], and biologic agents that target TNF-α, IL-12, IL-23 and IL-17A [6,12,14].
Unlike biologics, apremilast provides patients with an oral option that does not require laboratory monitoring. Based on published prices, apremilast is also less costly than biologics [1]. However, the current literature is relatively sparse with respect to real-world adherence to and cost of apremilast treatment. This study compares the persistence, adherence and healthcare costs of biologic-naive psoriasis patients treated with apremilast compared with biologic agents among commercially insured adults with psoriasis in the USA.
Methods
Study design & data source
This retrospective, observational cohort study used administrative claims data of patients identified from the IBM MarketScan® Commercial and Medicare Supplemental Databases (Truven Health Analytics, now IBM Watson Health, MA, USA). The study period extended from 1 January 2013 to 30 June 2016. The MarketScan databases contain the pooled healthcare experience of >100 million commercial and Medicare supplemental enrollees during the study period. The databases include medical claims for healthcare services performed in the inpatient and outpatient settings as well as enrollment data, including member demographic information, eligibility and benefits data. The medical claims files include service dates, provider reimbursement amounts, patient copayments and deductible amounts. All database records are deidentified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act (HIPAA) of 1996. The databases have been evaluated and certified by an independent third party to be in compliance with the HIPAA statistical deidentification standard. The databases were certified to satisfy the conditions set forth in Sections 164.514 (a)–(b)1ii of the HIPAA privacy rule regarding the determination and documentation of statistically deidentified data. Because the study used only deidentified patient records and did not involve the collection, use or transmittal of individually identifiable data, institutional review board approval to conduct this study was not required.
Patient selection criteria
Patients were identified if their index date for treatment initiation with apremilast or a biologic agent for psoriasis and/or psoriatic arthritis (PsA) was between 1 January 2014 and 30 June 2016. Biologic agents included adalimumab, certolizumab, etanercept, golimumab, infliximab, secukinumab or ustekinumab; medications that were approved after 30 June 2015 were not evaluated because the patient population initiating these medications would not have satisfied the study inclusion and exclusion criteria. Inclusion criteria were as follows: at least two medical claims with an International Classification of Diseases (ninth and tenth edition) Clinical Modification diagnosis of psoriasis and/or PsA during the 12 months prior to the index date; aged ≥18 years of age on the index date; continuous enrollment with medical and pharmacy benefits for the 12 months prior to the index date (preindex/baseline period); continuous enrollment with medical and pharmacy benefits during the 12 months following the index date (postindex/follow-up period); no evidence of other biologic-indicated autoimmune conditions in the 12-month pre-index period or 12-month post-index period (ulcerative colitis, Crohn's disease, rheumatoid arthritis and other inflammatory polyarthropathies, including ankylosing spondylitis and juvenile idiopathic arthritis); no evidence of a cancer diagnosis at any time during the study period (pre- or post-index period); and no evidence of multiple index medications on the index date. Analysis was limited to psoriasis patients who were naive to both apremilast and biologic agents; patients with PsA were excluded from this analysis.
Outcomes
The two primary outcomes analyzed in this study were treatment patterns (treatment persistence, persistence-based medication possession ratio [MPR], adherence) and all-cause healthcare costs. Treatment persistence was defined as the proportion of patients without discontinuation of the index medication based on a >60-day gap in therapy following the exhaustion of the previous days’ supply or a switch to apremilast or a biologic prior to the end of the 12-month postindex period. The postindex persistence period was defined as the total number of days from the index date to the earliest discontinuation of the index medication based on a >60-day gap in therapy, or a switch to apremilast or a biologic if the patient was nonpersistent on therapy, or the end of the 12-month postindex period if the patient was persistent on therapy. Persistence-based MPR was the sum of days’ supply for all prescription claims during the postindex persistence period divided by the total number of days in the postindex persistence period. Adherence was defined as a persistence-based MPR of ≥80%.
All-cause healthcare expenditures were reported by type of service (outpatient medical, outpatient pharmacy, total) and measured while patients were persistent on their index treatment per-patient per-month (PPPM) and during the 12-month postindex period. The total costs of 12 months of persistence were calculated among persistent apremilast initiators and among persistent biologic initiators. The total costs for nonpersistent switchers and nonpersistent nonswitchers were calculated among nonpersistent apremilast or biologic patients who switched treatments and among nonpersistent apremilast or biologic patients who did not switch treatments, respectively. Healthcare costs were based on paid amounts of adjudicated claims, including insurer and health plan payments as well as patient cost-sharing in the form of copayment, deductible and coinsurance. Cost for services provided under capitated arrangements were estimated using payment proxies that were computed based on paid claims at the procedure level using the MarketScan Commercial and Medicare Supplemental Databases. All dollar estimates were inflated to 2016 dollars using the medical care component of the Consumer Price Index.
Other measures/covariates
Covariates included age (18–24, 25–34, 35–44, 45–54, 55–64, 65–74, ≥75 years of age), sex, insurance plan type (comprehensive, exclusive provider organization, health maintenance organization, point of service, preferred provider organization, point of service with capitation, consumer driven health plan, other), US Census Bureau geographic region (Northeast, North, Central, South, West, or unknown), urban/rural residence and index year. Comorbid conditions identified during the baseline period included anxiety, cardiovascular disease, depression, headache, hepatotoxicity, hypertension, serious infections, moderate or severe renal disease, osteoarthritis, osteoporosis, postmenopausal symptoms and Type II diabetes mellitus. Concomitant medications were antidiabetics, antidepressants, atypical antipsychotics, benzodiazepines, bisphosphonates/selective estrogen receptor modulators and opioids. The Charlson Comorbidity Index, baseline total healthcare expenditures, psoriatic-related medications and procedures were also noted during the baseline period and while patients were persistent on the index therapy (phototherapy, nonsteroidal anti-inflammatory drugs/cyclooxygenase-2 inhibitors, corticosteroids, systemic agents [acitretin, cyclosporine, methotrexate, sulfasalazine, leflunomide]).
Statistical analysis
All variables were summarized descriptively as means (standard deviation) or counts (percentages). The t-tests/Wilcoxon rank-sum tests were used to test for significant differences between continuous variables and χ2 tests were used for categorical variables.
Apremilast and biologic users were 1:2 propensity score matched using the nearest neighbor matching with calipers (0.25 width) of the pooled standard deviation. The propensity score was calculated from logistic regression model predicting the probability of treatment assignment conditional on observed baseline patient demographics and clinical characteristics. The matching characteristics included in the model were age group, gender, health plan, payer, region, index year and urbanicity.
Generalized linear models (GLMs) with log link and γ-error distribution were used on the matched cohorts to estimate treatment effect on healthcare costs, adjusting for patient demographics, baseline clinical characteristics and baseline total costs. Models were fit separately by type of service (outpatient medical, outpatient pharmacy, total) while the patient was persistent on their index treatment and during the 12-month postindex period.
Results
Study sample
From the MarketScan Commercial and Medicare Supplemental Databases, 128,927 patients were identified as having initiated a new treatment episode with apremilast or a biologic agent for psoriasis and/or PsA between 1 January 2014 and 30 June 2016. After applying the inclusion and exclusion criteria, 8519 eligible patients were identified (Figure 1). The apremilast and biologic patients were then propensity score matched; of those successfully matched, the biologic-naive patients were retained to provide a final matched, apremilast- and biologic-naive sample composed of 703 psoriasis patients initiating apremilast and 1378 psoriasis patients initiating a biologic.
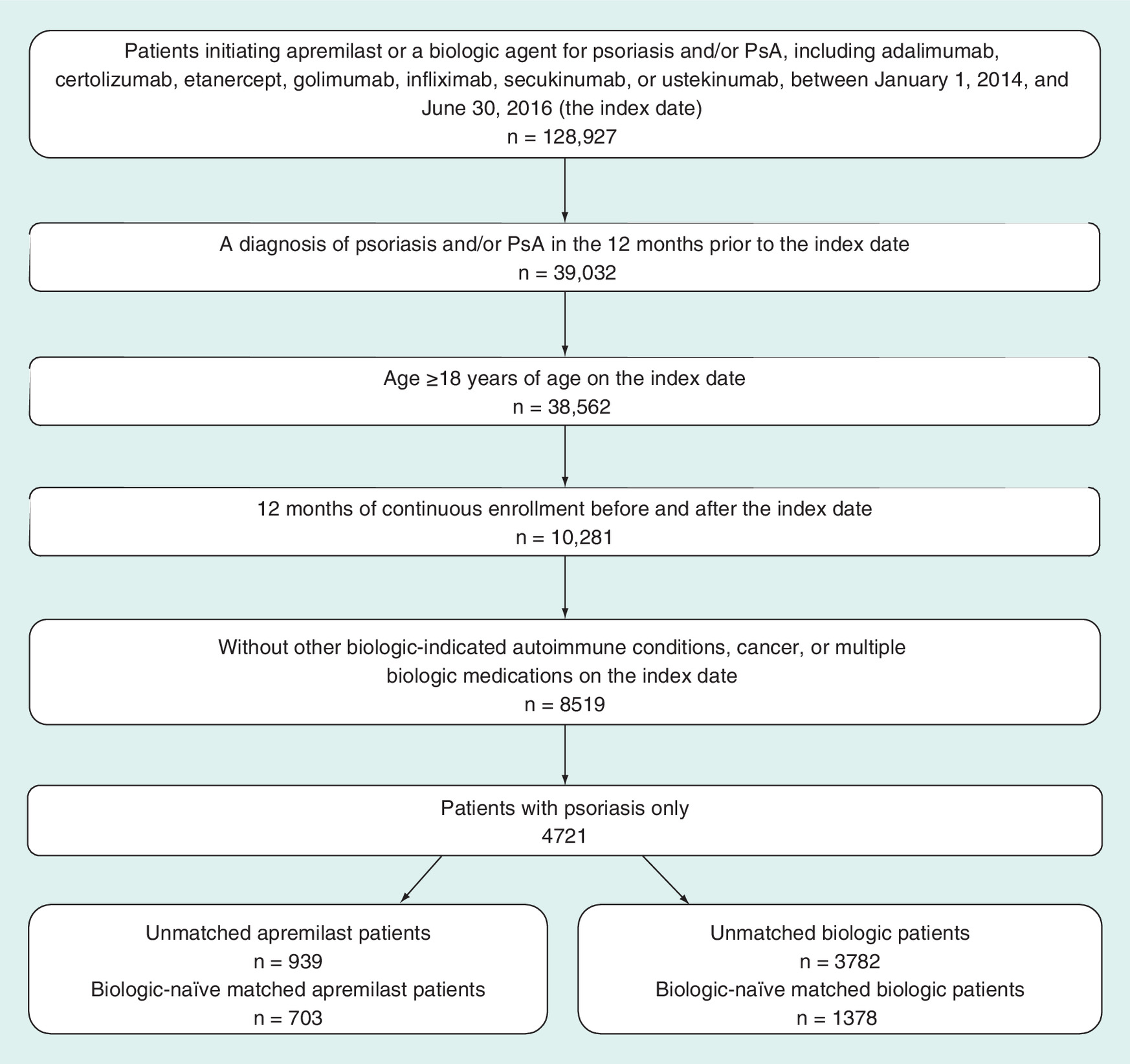
Figure 1. Selection and attrition of biologic-naive patients initiating apremilast or biologics.
PsA: Psoriatic arthritis.
After propensity score matching, the two biologic-naive study cohorts had similar patient demographics and clinical characteristics. The mean age was 49 years, 50% were female and the mean Charlson Comorbidity Index score was 0.4 (Table 1). Concomitant medication use, comorbid conditions and baseline healthcare costs were also similar; however, baseline medication history differed somewhat in that fewer patients initiating apremilast had prior methotrexate use in the 12-month pre-index period compared with those initiating a biologic (11.0 vs 18.7%; p < 0.001).
| Characteristics | Apremilast n = 703 | Biologics n = 1378 |
|---|---|---|
| Age (years) | 49.4 (12.98) | 49.0 (12.51) |
| Sex, n (%) | ||
| – Male | 336 (47.8) | 686 (49.8) |
| – Female | 367 (52.2) | 692 (50.2) |
| Insurance plan type (%) | ||
| – Health maintenance organization | 47 (6.7) | 102 (7.4) |
| – Preferred provider organization | 433 (61.6) | 833 (60.4) |
| – Consumer-directed health plan | 81 (11.5) | 168 (12.2) |
| – Other/unknown | 142 (20.2) | 275 (20.0) |
| Geographic region (%) | ||
| – Northeast | 180 (25.6) | 367 (26.6) |
| – North Central | 185 (26.3) | 347 (25.2) |
| – South | 265 (37.7) | 518 (37.6) |
| – West | 72 (10.2) | 145 (10.5) |
| Primary payer (%) | ||
| – Commercial | 635 (90.3) | 1273 (92.4) |
| – Medicare | 68 (9.7) | 105 (7.6) |
| Index year (%) | ||
| – 2014 | 194 (27.6)‡ | 890 (64.6) |
| – 2015 | 509 (72.4)‡ | 488 (35.4) |
| Charlson Comorbidity Index | 0.48 (1.07) | 0.42 (0.93) |
| Preperiod comorbid conditions (%) | ||
| – Cardiovascular disease | 82 (11.7) | 159 (11.5) |
| – Hypertension | 230 (32.7) | 457 (33.2) |
| – Serious infection | 197 (28.0) | 339 (24.6) |
| – Osteoarthritis | 58 (8.3) | 97 (7.0) |
| – Type II diabetes mellitus | 99 (14.1) | 212 (15.4) |
| Preperiod concomitant medications (%) | ||
| – Antidepressants | 179 (25.5) | 356 (25.8) |
| – Antidiabetics | 106 (15.1) | 217 (15.7) |
| – Benzodiazepines | 107 (15.2) | 222 (16.1) |
| – Opioids | 197 (28.0) | 417 (30.3) |
| Psoriatic-related therapies (%) | ||
| – Systemic agents | 124 (17.6)‡ | 347 (25.2) |
| – Acitretin | 34 (4.8) | 75 (5.4) |
| – Cyclosporine | 15 (2.1) | 35 (2.5) |
| – Methotrexate | 77 (11.0)‡ | 257 (18.7) |
| – Sulfasalazine | 3 (0.4) | 7 (0.5) |
| – Leflunomide | 3 (0.4)† | 0 (0.0) |
| – NSAIDs/COX-2s | 189 (26.9) | 358 (26.0) |
| – Corticosteroids | 646 (91.9)‡ | 1161 (84.3) |
| Preperiod total healthcare costs, mean (SD) | US$12,004 (US$19,279) | US$11,763 (US$24,327) |
Values expressed as mean (SD) or n (%).
†p < 0.05, apremilast vs biologics.
‡p < 0.001, apremilast vs biologics.
NSAID: Nonsteroidal anti-inflammatory drug; SD: Standard deviation.
Treatment persistence & adherence
Treatment persistence in the 12-month postindex period was similar for psoriasis patients initiating apremilast compared with patients initiating a biologic (44.4 vs 44.6%; p = 0.914). Persistence-based MPRs were similar for patients initiating apremilast compared with patients initiating a biologic (0.86 vs 0.86; p = 0.654), as were adherence rates (73 vs 74%; p = 0.516). The patients initiating apremilast were less likely to be nonpersistent because of switching compared with patients initiating biologics (Table 2).
| Variable | Apremilast n = 703 | Biologics n = 1378 | p-value |
|---|---|---|---|
| Persistent patients (%) | 312 (44.4) | 615 (44.6) | 0.914 |
| Nonpersistent patients (%) | 391 (55.6) | 763 (55.4) | 0.914 |
| Days in persistence period (all patients) | 224.3 (138.4) | 237.6 (131.2) | 0.032 |
| Reason for nonpersistence (%) | |||
| – >60-day gap | 369 (94.3) | 679 (88.9) | 0.003 |
| – >60-day gap with restart of index medication | 93 (23.8) | 267 (35.0) | <0.001 |
| – Switch to another biologic | 22 (5.6) | 84 (11.0) | 0.003 |
| Treatment to which a patient switches (%) | |||
| – Adalimumab | 0 (0.0) | 0 (0.0) | – |
| – Apremilast | 0 (0.0) | 17 (1.2) | 0.003 |
| – Certolizumab | 0 (0.0) | 1 (0.1) | 1.000 |
| – Etanercept | 5 (0.7) | 13 (0.9) | 0.589 |
| – Golimumab | 0 (0.0) | 1 (0.1) | 1.000 |
| – Infliximab | 0 (0.0) | 0 (0.0) | – |
| – Ixekizumab | 0 (0.0) | 0 (0.0) | – |
| – Secukinumab | 5 (0.7) | 13 (0.9) | 0.589 |
| – Ustekinumab | 12 (1.7) | 39 (2.8) | 0.117 |
| Adherence while persistent on index agent | |||
| – MPR | 0.86 (0.12) | 0.86 (0.13) | 0.654 |
| – Nonadherence, MPR of <80% (%) | 193 (27.5) | 360 (26.1) | 0.516 |
| – Adherence, MPR of ≥80% (%) | 510 (72.5) | 1018 (73.9) | 0.516 |
Values expressed as mean (SD) or n (%).
MPR: Medication possession ratio; SD: Standard deviation.
Healthcare costs
Unadjusted PPPM total healthcare costs while persistent on therapy were lower among apremilast patients compared with biologic patients (US$3426 vs US$5649; p < 0.001). Compared with biologic users, apremilast users had lower PPPM outpatient pharmacy costs (US$2478 vs US$4922; p < 0.001) and lower PPPM outpatient medical costs (US$407 vs US$640; p < 0.05). Differences in outpatient medical costs were due to lower PPPM costs for other outpatient services, which included services such as radiology, infusion administrations, rehabilitation and physical therapy (US$272 vs US$488; p < 0.05).
Unadjusted total healthcare costs during the 12-month follow-up period were lower among apremilast patients compared with biologics patients (US$32,304 vs US$49,875; p < 0.001); differences were driven by lower outpatient pharmacy costs (US$23,376 vs US$41,803; p < 0.001).
Adjustment for differences in baseline clinical characteristics with GLMs did not change the magnitude or the direction of the results: Apremilast users experienced lower costs while persistent on therapy and during the 12-month follow-up period compared with biologic users. PPPM total costs were US$2458 lower among apremilast patients while persistent on therapy (US$2484 vs US$4942; p < 0.001), which were driven by lower PPPM outpatient pharmacy costs and PPPM outpatient medical costs (Figure 2). During the 12-month postindex period, total healthcare costs were US$19,327 lower for apremilast patients compared with biologic patients (US$31,337 vs US$50,664; p < 0.001) because of lower total outpatient pharmacy costs (US$23,171 vs US$42090; p < 0.001; Figure 3).
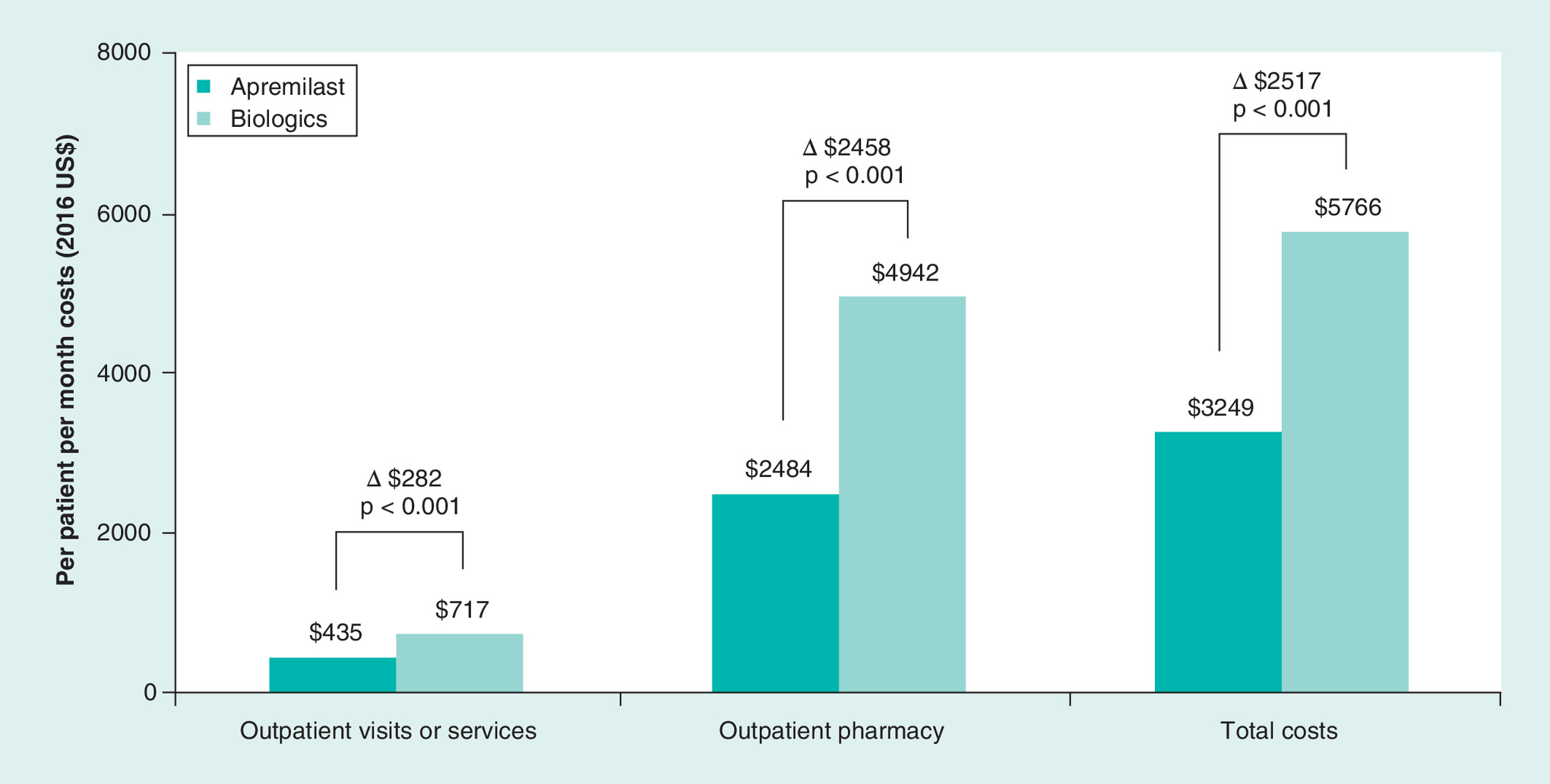
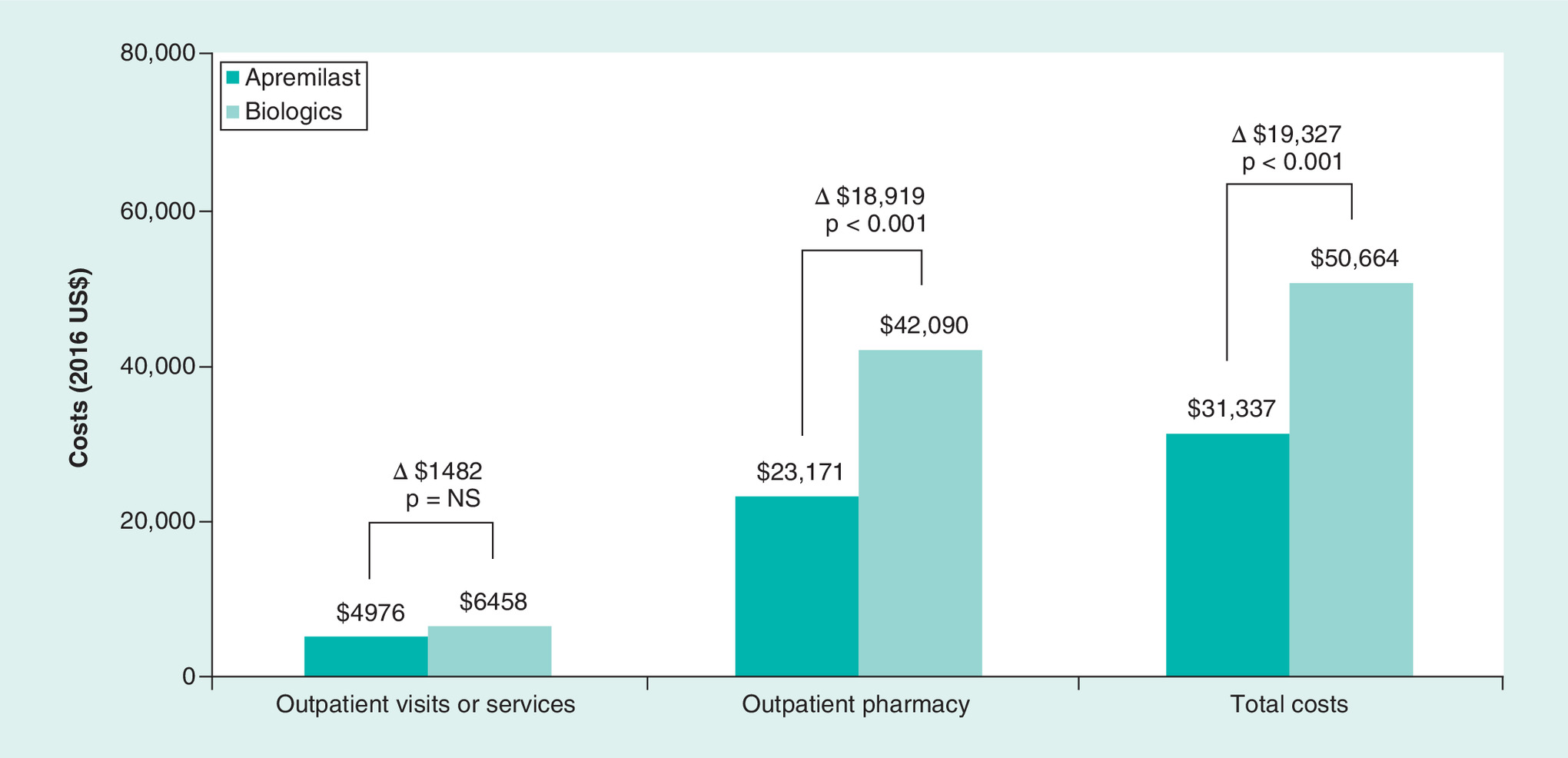
Figure 3. Adjusted total healthcare costs during the 12-month follow-up period.
NS: Not significant.
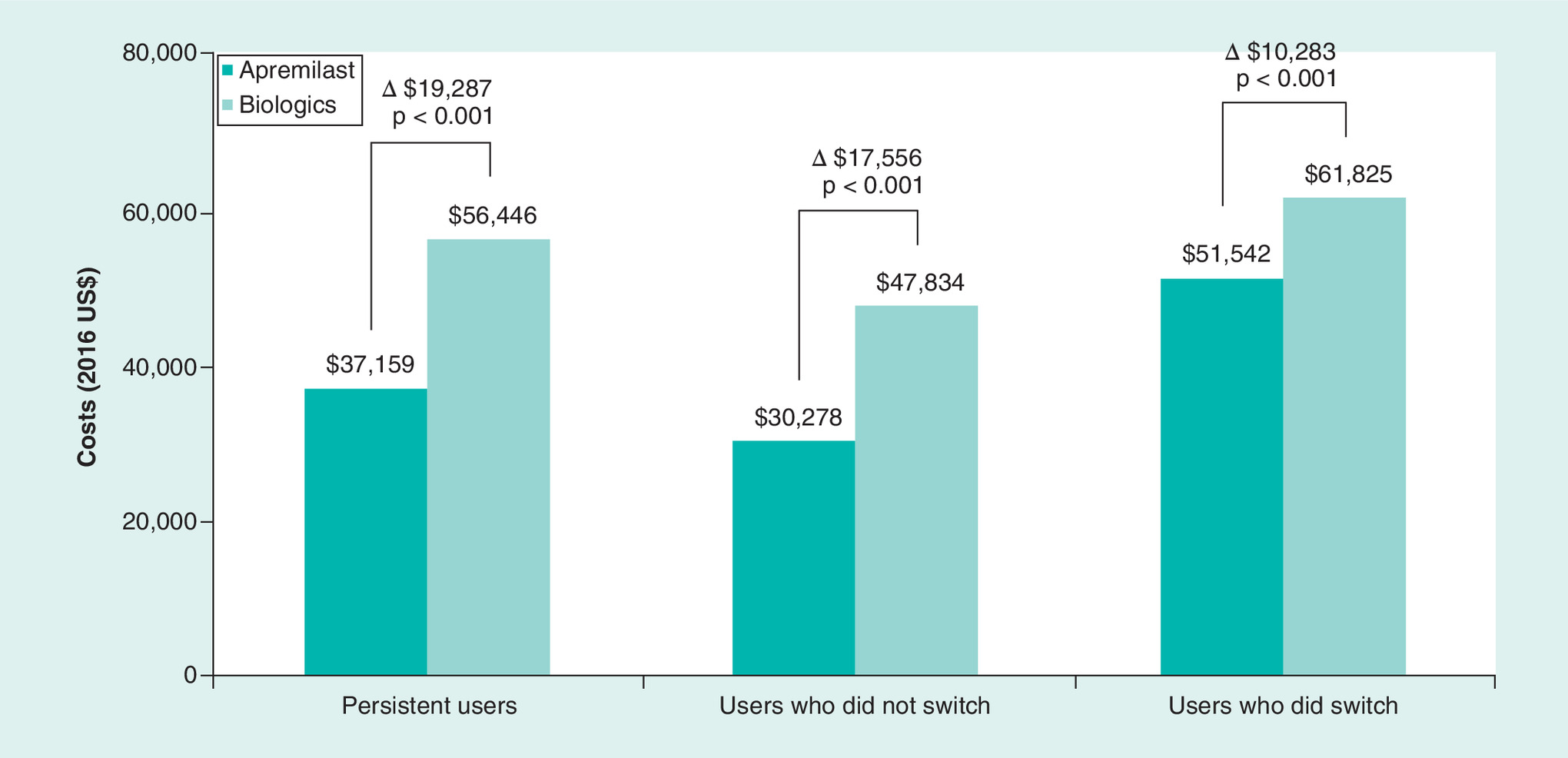
The total healthcare costs for 12 months of persistence were US$19,287 lower among persistent apremilast patients compared with persistent biologic patients (US$37,159 vs US$56,446; p < 0.001; Figure 4). The difference in total cost over 12 months decreased to US$17,556 among nonpersistent nonswitchers initiating apremilast compared with nonpersistent nonswitchers initiating a biologic (US$30,278 vs US$47,834; p < 0.001). Compared with persistent patients and nonpersistent nonswitchers, the total costs over 12 months were highest among the nonpersistent patients who switched treatments (apremilast: US$51,542, biologics: US$61,825; p < 0.001). The cost advantage among apremilast patients who switched treatments decreased to US$10,283 less than biologic initiators who switched treatments because of higher pharmacy costs.
Discussion
This administrative claims-based analysis investigated persistence, adherence and healthcare costs among biologic-naive patients initiating apremilast or a biologic in the real-world setting. After multivariable adjustment for differences in baseline clinical characteristics using GLMs, total healthcare costs in the first year after starting treatment were US$19,327 lower for apremilast patients compared with those initiating biologics (US$31,337 vs US$50,664). The cost advantage of over US$19,000 per year remained evident among apremilast patients persistent on treatment for 1 year (US$37,159 vs US$56,446) and remained approximately US$10,000 per year among nonpersistent patients who switched treatments (apremilast: US$51,542, biologics: US$61,825). Psoriasis patients initiating apremilast had comparable adherence, reduced likelihood of switching and lower overall total healthcare costs compared with those initiating biologics, suggesting that apremilast patients generally perceived continuing treatment to be worthwhile and exacerbations did not drive frequent inpatient admissions, outpatient visits or unanticipated pharmacy costs.
Apremilast is an oral systemic drug approved for the treatment of plaque psoriasis in 2014. Biologic therapies are delivered subcutaneously or intravenously, which may result in pain and discomfort for patients as well as adverse events such as injection site reactions [15]. By comparison, oral apremilast may be easier and more comfortable for some patients to administer [15]. Factors such as ease of administration, adverse effects and drug acquisition costs may contribute to patients’ preference for oral treatment.
These study findings provide a benchmark of the total healthcare costs in the first year after initiating apremilast treatment and an updated estimate of the total direct costs in the first year after initiating biologics for psoriasis. Our estimate of US$31,337 for the 1-year total direct costs for patients initiating apremilast and US$50,664 (2016 US dollars) for patients initiating biologics are similar to several previous costs analyses. A cost-per-responder model estimated that the 1-year pharmacy costs for psoriasis patients achieving a ≥75% reduction from baseline in Psoriasis Area and Severity Index score were US$34,472 for apremilast compared with US$44,791 for adalimumab, US$57,816 for etanercept and US$45,319 to US$87,378 for ustekinumab (2011 US dollars) [16]. Our cost estimates for biologics are similar to another study that reported the 1-year pharmacy costs related to induction and maintenance treatment for adalimumab, etanercept and ustekinumab ranged from US$39,041 to US$53,909 (2014 US dollars) [17].
Positioning new therapies in the armamentarium of treatment options is challenging, especially in a dynamic market with new agents and mechanisms of action being introduced in rapid succession [18,19]. Our results may be useful for providers as well as pharmacy and therapeutic committees seeking to optimize psoriasis care while reducing healthcare costs.
Results from this study may not be generalizable to psoriasis patients without commercial or private Medicare supplemental coverage. The potential for underdiagnosis of psoriasis among patients introduces selection bias into the study design by excluding psoriasis patients who were untreated or did not have a relevant diagnosis recorded on their medical claims; however, the omission of these patients should not alter the interpretation of findings. A second potential contributor to selection bias is the required 12 months of continuous enrollment before and after the index date. Patients who did not meet the continuous enrollment criteria were excluded from the study, including patients who no longer had health insurance or who expired during the postindex period. Therefore, the study population may appear to be healthier than the total population of patients in the database.
The MarketScan research databases rely on administrative claims data for clinical detail and, as such, these data are subject to data coding limitations and data entry error. Medication persistence and adherence measures were based on filled prescriptions and it was assumed that patients took the medication as prescribed. In addition, the treatment landscape changed during this study period; newer medications approved after 30 June 2015 could not be included as patients initiating these medications would not have satisfied the inclusion and exclusion criteria.
Unidentified systematic differences between the study cohorts may contribute to differences in treatment patterns, healthcare utilization and costs. For example, there may be significant age or gender differences between the cohorts, the influence of which we attempted to adjust for by GLM modeling; however, our ability to adjust was limited to those characteristics available in administrative claims. Finally, an emerging body of evidence suggests that multimodal treatment approaches may improve treatment adherence, patient quality of life and clinical outcomes by addressing comorbidities (cardiovascular conditions), lifestyle (smoking, obesity) and patient health literacy through education and mental health interventions [13,20,21]. We have no data regarding patient participation in any complementary programs to address modifiable risk factors for disease progression or to monitor and improve treatment adherence.
Conclusion
This novel real-world analysis compared patients initiating apremilast or biologics for the treatment of moderate to severe psoriasis. Apremilast users had lower total healthcare costs while persistent on treatment and during the 12-month postindex period. Moreover, the relative cost advantage for apremilast users over 12 months was highest for patients persistent on treatment and lowest for nonpersistent patients who switched to biologics. Given the wide variety of therapeutic options and difficulty of treating psoriasis, future research efforts should include clinically relevant characteristics not available in claims data that may be useful in optimizing treatment recommendations. Analyses should also identify potential predictors of switching from one systemic agent to another. These efforts will help to refine the empiric positioning of various therapeutic agents. Finally, measures to improve patients’ persistence and adherence may help to reduce the cost of psoriasis management while improving patients’ lives.
Background
Biologics and apremilast have revolutionized the treatment of psoriasis. However, there is little real-world information on persistence, adherence and cost of apremilast compared with biologics among commercially insured adults with psoriasis in the USA.
Methods
This analysis used administrative claims data to compare the persistence, adherence and healthcare costs of biologic-naive psoriasis patients treated with apremilast or biologic agents;
Generalized linear models were used on propensity score-matched cohorts to estimate the treatment effect on healthcare costs, adjusting for patient demographics, baseline clinical characteristics and baseline total healthcare costs.
Results
Treatment persistence and adherence rates are similar for psoriasis patients initiating apremilast compared with patients initiating a biologic;
After multivariable adjustment for differences in baseline clinical characteristics using generalized linear models, total healthcare costs in the first year after starting treatment are US$19,327 lower for apremilast patients compared with those initiating biologics (apremilast: US$31,337 vs biologics: US$50,664);
Total healthcare costs were higher among patients who were nonpersistent on treatment. However, apremilast's cost advantage was evident regardless of whether patients were persistent or were nonpersistent and switched or did not switch treatments.
Future perspective
Measures to improve patients’ persistence and adherence may help reduce the cost of psoriasis management.
Acknowledgments
The authors gratefully acknowledge the research and editorial contributions of A Krug, MPH.
Authors’ contributions
This study was conceived and designed by SR Feldman, CL Pelletier, KL Wilson, RK Mehta, MA Brouillette and MM Bonafede. Data collection and statistical analysis were done by KL Wilson, MA Brouillette, D Smith and MM Bonafede. All authors contributed to the data interpretation, drafting, revision and approval of the submitted report, and all authors had full access to all of the data.
Financial & competing interests disclosure
This study was funded by Celgene Corporation. SR Feldman has received research support from and served as a consultant and speaker for AbbVie, Celgene Corporation, Eli Lilly, Janssen, Novartis and Ortho Dermatology. CL Pelletier and RK Mehta are employees of Celgene Corporation. KL Wilson, MA Brouillette, D Smith and MM Bonafede are employees of IBM Watson Health. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct
The authors state that all database records are deidentified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996. Because only deidentified patient records were used in the study and no collection, use or transmittal of individually identifiable data occurred, institutional review board approval to conduct this study was not required.
References
Papers of special note have been highlighted as: • of interest
1.
Feldman SR, Goffe B, Rice G et al. The challenge of managing psoriasis: unmet medical needs and stakeholder perspectives. Am. Health Drug Benefits 9(9), 504–513 (2016).
• Describes how psoriasis is a complex, costly disease and how patients and healthcare providers manage the various psoriasis treatment options so patients can obtain optimal care.
2.
National Institute of Arthritis and Musculoskeletal and Skin Disease. Questions and answers about psoriasis (2017). www.niams.nih.gov/health-topics/psoriasis.
3.
World Health Organization. Global report on psoriasis (2016). http://apps.who.int/iris/bitstream/handle/10665/204417/9789241565189_eng.pdf;jsessionid=FA9000ED205E06CBB51120CECA4F1E6E?sequence=1.
4.
Bell LM, Sedlack R, Beard CM, Perry HO, Michet CJ, Kurland LT. Incidence of psoriasis in Rochester, Minn, 1980–1983. Arch. Dermatol. 127(8), 1184–1187 (1991).
5.
Pathirana D, Ormerod AD, Saiag P et al. European S3-guidelines on the systemic treatment of psoriasis vulgaris. J. Eur. Acad. Dermatol. Venereol. 23(Suppl. 2), 1–70 (2009).
6.
Vide J, Magina S. Moderate to severe psoriasis treatment challenges through the era of biological drugs. An. Bras. Dermatol. 92(5), 668–674 (2017).
7.
Brezinski EA, Dhillon JS, Armstrong AW. Economic burden of psoriasis in the United States: a systematic review. JAMA Dermatol. 151(6), 651–658 (2015).
8.
National Psoriasis Foundation. About psoriasis and psoriatic arthritis in children (2018). www.psoriasis.org/parents/about-psoriasis.
9.
National Psoriasis Foundation. Topical treatments (2018). www.psoriasis.org/about-psoriasis/treatments/topicals.
10.
National Psoriasis Foundation. Traditional systemic medications (2018). www.psoriasis.org/about-psoriasis/treatments/systemics.
11.
Zerilli T, Ocheretyaner E. Apremilast (Otezla): a new oral treatment for adults with psoriasis and psoriatic arthritis. PT 40(8), 495–500 (2015).
12.
Guerriero F, Orlando V, Monetti VM, Russo V, Menditto E. Biological therapy utilization, switching, and cost among patients with psoriasis: retrospective analysis of administrative databases in Southern Italy. Clinicoecon. Outcomes Res. 9, 741–748 (2017).
13.
Gisondi P, Del Giglio M, Girolomoni G. Treatment approaches to moderate to severe psoriasis. Int. J. Mol. Sci. 18(11), E2427 (2017).
14.
National Psoriasis Foundation. Moderate to severe psoriasis and psoriatic arthritis: biologic drugs (2018). www.psoriasis.org/about-psoriasis/treatments/biologics.
15.
Palfreeman AC, McNamee KE, McCann FE. New developments in the management of psoriasis and psoriatic arthritis: a focus on apremilast. Drug Des. Devel. Ther. 7, 201–210 (2013).
• Models the cost per responder for psoriasis patients receiving etanercept or ustekinumab treatment, and the article provides an older estimate of the costs of psoriasis patients treated with select biologics.
16.
Martin S, Feldman SR, Augustin M, Szapary P, Schenkel B. Cost per responder analysis of ustekinumab and etanercept for moderate to severe plaque psoriasis. J. Dermatolog. Treat. 22(3), 138–143 (2011).
• Reports the average wholesale cost of biologics over time, which serves as an estimate of the price of biologics for patients with psoriasis.
17.
Cheng J, Feldman SR. The cost of biologics for psoriasis is increasing. Drugs Context 3, 212266 (2014).
18.
Reed M, Crosbie D. Apremilast in the treatment of psoriatic arthritis: a perspective review. Ther. Adv. Musculoskelet. Dis. 9(2), 45–53 (2017).
19.
Goldenberg G, Lanoue J, Dong J. New oral therapies for psoriasis: a comprehensive review. J. Clin. Aesthet. Dermatol. 9(8), 25–28 (2016).
20.
Thorneloe RJ, Griffiths CEM, Emsley R, Ashcroft DM, Cordingley L. Intentional and unintentional medication non-adherence in psoriasis: the role of patients’ medication beliefs and habit strength. J. Invest. Dermatol. 138(4), 785–794 (2018).
21.
Singh SM, Narang T, Vinay K et al. Clinic-based group multi-professional education causes significant decline in psoriasis severity: a randomized open label pilot study. Indian Dermatol. Online J. 8(6), 454–459 (2017).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 19 September 2018
Accepted: 19 October 2018
Published online: 2 November 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Real-world US healthcare costs of psoriasis for biologic-naive patients initiating apremilast or biologics. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0097
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Andreas Pinter, Marcus Schulte, Nils Kossack, Marc Pignot, Michael Schultze, Andrea Feldhus, Real-world psoriasis treatment patterns and disease burden in Germany, with a focus on biologics and apremilast: data from a German statutory health insurance database, Journal of Medical Economics, 10.1080/13696998.2025.2452054, 28, 1, (207-220), (2025).
- Celine Miyazaki, Junya Masuda, Phiona I-Ching Tsai, Hidehisa Saeki, Factors Affecting Treatment Persistence in Japanese Patients with Psoriasis Prescribed Biologics: A Real-World Study Using an Insurance Claim Database, Dermatology and Therapy, 10.1007/s13555-024-01274-1, 14, 11, (2999-3015), (2024).
- Dominic Pilon, Timothy Fitzgerald, Maryia Zhdanava, Amanda Teeple, Laura Morrison, Aditi Shah, Patrick Lefebvre, Risk of Treatment Discontinuation among Patients with Psoriasis Initiated on Ustekinumab and Other Biologics in the USA, Dermatology and Therapy, 10.1007/s13555-022-00707-z, 12, 4, (971-987), (2022).
- Masayuki Tanaka, Yasushi Ozeki, Fujio Matsuyama, Tatsunori Murata, Shinichi Imafuku, Taichi Nakamura, Apremilast Prolongs the Time to First Biologic Therapy in Japanese Patients with Psoriasis, Dermatology and Therapy, 10.1007/s13555-021-00659-w, 12, 2, (451-466), (2021).
- Andrea Picchianti-Diamanti, Francesca Romana Spinelli, Maria Manuela Rosado, Fabrizio Conti, Bruno Laganà, Inhibition of Phosphodiesterase-4 in Psoriatic Arthritis and Inflammatory Bowel Diseases, International Journal of Molecular Sciences, 10.3390/ijms22052638, 22, 5, (2638), (2021).
- Shammy Jindal, Rajendra Awasthi, Dhananjay Singhare, Giriraj T. Kulkarni, Topical delivery of Tacrolimus using liposome containing gel: An emerging and synergistic approach in management of psoriasis, Medical Hypotheses, 10.1016/j.mehy.2020.109838, 142, (109838), (2020).
- Jashin J Wu, Corey Pelletier, Brian Ung, Marc Tian, Ibrahim Khilfeh, Jeffrey R Curtis, Real-world switch patterns and healthcare costs in biologic-naive psoriasis patients initiating apremilast or biologics, Journal of Comparative Effectiveness Research, 10.2217/cer-2020-0045, 9, 11, (767-779), (2020).
- David L Kaplan, Brian L Ung, Corey Pelletier, Chuka Udeze, Ibrahim Khilfeh, Marc Tian,
Switch Rates and Total Cost of Care Associated with Apremilast and Biologic Therapies in Biologic-Naive Patients with Plaque Psoriasis
, ClinicoEconomics and Outcomes Research, 10.2147/CEOR.S251775, Volume 12, (369-377), (2020). - Yves Poulin, Catherine Beauchemin, Catherine Royer, Anne-Julie Gaudreau, Clarabella Yim, Fei Fei Liu, Jean Lachaine, Real-World Experience With Apremilast in the Treatment of Adults With Moderate to Severe Plaque Psoriasis in Québec: A Claims-Based Analysis of Drug Utilization and Healthcare Resource Utilization, Journal of Cutaneous Medicine and Surgery, 10.1177/1203475420936652, 24, 6, (573-587), (2020).
- Eran Shavit, Neil H. Shear, An update on the safety of apremilast for the treatment of plaque psoriasis, Expert Opinion on Drug Safety, 10.1080/14740338.2020.1744562, 19, 4, (403-408), (2020).