Gelatin tannate versus other antidiarrheal medication in children with acute gastroenteritis: a retrospective, observational study
Abstract
Aim: To evaluate the effectiveness and safety of gelatin tannate (GT) for acute gastroenteritis (AGE) in children. Materials & methods: In this retrospective, observational study, children admitted for AGE received GT ± oral rehydration solution (ORS; n = 46) or other antidiarrheal medications ± ORS (n = 46). Number and consistency of stools were recorded. Results: Children were aged 6 months to 7.9 years. GT ± ORS reduced diarrhea duration (29.0 vs 45.4 h, p < 0.0001) and normalized stool consistency at 72 h in significantly more patients (87.0 vs 30.4%; p = 0.026) compared with other antidiarrheal medications ± ORS. Differences in favor of GT were apparent from 12 h onward. Conclusion: GT is more effective than conventional treatment for managing AGE in children.
Acute gastroenteritis (AGE) is defined as a decrease in the consistency of stool leading to loose or liquid stools and/or an increase in the frequency of evacuations to ≥3 in 24 h, with or without fever or vomiting [1,2]. Acute diarrhea typically lasts less than 7 days [2,3].
AGE is very common in Europe, with an incidence ranging from 0.5 to 2 episodes/child/year in children aged ≤3 years [1]. Although AGE is rarely life-threatening in children residing in high-income countries, it is a frequent cause of medical consultations and hospitalizations, and thus represents a considerable healthcare and economic burden [2,4,5].
The most common cause of AGE in children in all European countries is rotavirus, although norovirus has become the leading cause of medically attended AGE in countries with high rotavirus vaccine coverage [1]. Other viral pathogens responsible for AGE are adenoviruses and sapoviruses, and the main bacterial agents include strains of Campylobacter, Salmonella, Shigella, etc [1,5]. In about 40% of cases, no causative agent can be identified [5].
The objectives of treating AGE are to prevent and correct dehydration, promote weight gain after rehydration using normal nutritional intake (early nutrition), and decrease the duration and severity of diarrhea and secondary morbidity [5]. Recommended first-line therapy is oral hypo-osmotic rehydration solution (ORS) [2]. Active oral pharmacological agents that may be used as an adjunct to ORS to reduce the duration and severity of diarrhea include specific probiotics, especially Lactobacillus GG and Saccharomyces boulardi, and also Lactobacillus reuteri DSM 17938 [2]. Diosmectite (adsorbant) and racecadotril (antisecretory) were options ‘to consider’ in the 2014 European guidelines for managing AGE in children [1], although their efficacy is currently under question [2].
Given this limited armamentarium, there is interest in identifying other effective, safe and low-cost interventions for treatment of AGE. Tasectan® (Noventure, Barcelona, Spain) is a medical device available in many European countries to control and reduce symptoms of diarrhea. The device is a complex of gelatin and tannic acid that is stable in the gastric acid environment and in the basic or neutral environment of the small and large bowel. Gelatin tannate (GT) belongs to a mucoprotectant class of compounds with barrier protective properties [6], which includes xyloglucan, also with antidiarrheal effect in children [7]. The GT is thought to act by forming a mechanical protective biofilm on the intestinal mucosa [8], thereby restoring normal function of the intestinal barrier and contributing to normal physiological homeostasis [9]. Other proposed mechanisms for its activity include preventing adhesion of Escherichia coli, Salmonella spp., toxins and other harmful substances (e.g., pro-inflammatory compounds) to the intestinal mucosa [10,11], and modulating the composition of microbiota [12].
An observational study from Spain [13] and three of four randomized controlled trials [14–17] of GT conducted to date in young children with AGE have reported better symptomatic improvement with ORS + GT than with ORS (± placebo). The aim of the current observational study in children with AGE was to compare the effectiveness and safety of GT (GT ± ORS) with that of conventional treatment for AGE under real-world clinical practice conditions.
Materials & methods
This retrospective, observational study involved children admitted for AGE to a single pediatric clinic in Cluj-Napoca, Romania. All children had been treated by the same pediatric gastroenterologist. This same investigator analyzed medical records for two groups of subjects: those who had been treated with GT ± ORS and those who had been treated with other antidiarrheal medication (OAM) ± ORS during hospitalization for AGE.
To be eligible for analyses, children had to fulfill the following criteria: 3 months to 12 years of age at the time of admission; diagnosis of AGE, with a maximum symptom duration of 72 h before admission; clinical signs of mild or moderate dehydration (modified Vesikari score) [18]; good compliance with study medication defined as ingestion of ≥75% of required doses depending on weight/age.
Patients who met any of the following criteria were ineligible for analyses: associated extraintestinal infectious diseases; severe AGE with sepsis; bloody diarrhea; severe malnutrition (Z score for BMI <3 SDs for patients aged >24 months; Z score <3 SDs for weight related to height for patients aged <24 months); known immune deficiency; known digestive disease associated with chronic diarrhea (e.g., food allergy, cystic fibrosis, celiac disease, inflammatory bowel disease, irritable bowel); digestive malformations; chronic intestinal pseudo-obstruction; intake of probiotics, antibiotics, racecadotril, diosmectite or GT within 7 days before presentation; administration of any medication other than study medication during hospitalization.
The ‘GT’ group received oral GT according to approved labeling (<3 years: 250 mg four-times daily; ≥3 years: 500 mg four-times daily) ± ORS. The ‘OAM’ group received one or more of the following products according to approved labeling: diosmectite ± racecadotril ± Saccharomyces boulardii or Lactobacillus GG ± ORS. Treatment began immediately after admission and was continued for a maximum duration of 72 h.
Data collected on patients at the time of admission were: day of admission, age and gender, duration of AGE before hospitalization (hours), number of stools and their consistency (according to the Bristol scale) [19] during the 24 h before hospitalization, number of vomiting episodes during the 24 h before hospitalization, weight and height, body temperature and severity of dehydration.
Data collected on patients after admission were: type of antidiarrheal therapy; number of liquid stools at 12, 24, 36, 48 and 72 h; number of total stools and consistency of all stools at 12, 24, 36, 48 and 72 h; number of vomiting episodes/day; weight at 72 h; type, number and severity of adverse reactions; and day of discharge.
Study end points
The primary end point was the duration of diarrhea, defined as the time to normalization of stool consistency (Bristol scale: 1–5).
Secondary efficacy measures were: time to normal stool consistency per day (with reference to the period before the diarrhea); number (%) of watery stools (Bristol scale: 6–7) and, respectively, number (%) of normal consistency stools (Bristol scale: 1–5) at 12, 24, 36, 48 and 72 h after the start of treatment; number (%) of patients with normal consistency stools at 12, 24, 36, 48 and 72 h; risk of diarrhea at 72 h; number (%) of patients with complete recovery (acute diarrhea and associated symptoms) at 48 h; patients’ weight difference at 72 h; and duration of hospitalization.
Safety was assessed by monitoring adverse reactions (disease worsening/complications) reported by patients or observed by the physician during treatment.
Ethical considerations
The study protocol was approved by the Institutional Review Board of the Emergency Clinical Hospital for Children. Only the investigator collected data from the medical records. Collected data did not include information that could identify subjects.
Statistical methods
Based on assumed treatment success rates of 90% in the treatment group and 70% in the control group, the sample size was calculated to ensure a statistical power of 80% to detect noninferiority between GT and OAM, at a significance level of 0.05. Assuming a dropout rate of 10%, 92 patients in total were required for evaluation.
Results are summarized using descriptive statistics: mean ± standard deviation (SD) for continuous variables and absolute (n) and relative (%) frequency counts for categorical variables. Standard statistical tests (Chi square/Fisher's exact or Student's t test/Mann-Whitney U test) were used to compare treatment groups depending on the distribution and number of subjects. Kaplan–Meier survival analysis was used to estimate the interval until disappearance of diarrhea after admission.
Statistical analyses were performed using IBM SPSS Statistics 20 and Microsoft Excel 2016 and XLSTAT.
Results
The study population comprised 92 subjects treated with GT ± ORS (n = 46) or OAM ± ORS (n = 46) between 1 December 2012 and 9 March 2018. Demographic and clinical characteristics of the treatment groups are summarized in Table 1. The mean age of analyzed patients was approximately 3 years, and the age range was 6 months to 7.9 years. The treatment groups were reasonably well matched for demographic and clinical characteristics. More than 90% of patients in each treatment group had a dehydration severity score of 1/2 or 2 at admission. AGE etiology was rotavirus in approximately 40% of patients in each group. No infectious agent was detected in approximately 50% of patients in each group.
| Characteristic | Gelatin tannate ± ORS (n = 46) | Other antidiarrheal medication ± ORS† (n = 46) | p-value |
|---|---|---|---|
| Gender, n (%) – Male – Female | 18 (39.1) 28 (60.9) | 27 (58.7) 19 (41.3) | 0.06 |
| Age (years) ± SD | 2.9 ± 2.1 | 2.8 ± 1.7 | 0.81 |
| Weight (kg) ± SD | 13.4 ± 5.1 | 13.5 ± 3.9 | 0.93 |
| Height (cm) ± SD | 92.1 ± 18.5 | 91.7 ± 15.0 | 0.90 |
| BMI (kg/m2) ± SD | 15.0 ± 1.7 | 15.3 ± 1.7 | 0.21 |
| Temperature (°C) ± SD | 37.1 ± 0.6 | 37.2 ± 0.7 | 0.42 |
| Duration of acute gastroenteritis before hospitalization, n (%) 0–24 h 24–48 h 48–72 h | 11 (23.9) 14 (30.4) 21 (45.7) | 18 (39.1) 13 (28.3) 15 (32.6) | 0.19 |
| Severity of dehydration, n (%) No dehydration 1 1/2 – 2 | 3 (6.5) 4 (8.7) 17 (37.0) 22 (47.8) | 0 4 (8.7) 21 (45.7) 21 (45.7) | 0.17 |
| Etiology, n (%) Rotavirus Adenovirus Negative Not tested | 18 (39.1) 3 (6.5) 23 (50.0) 2 (4.4) | 19 (41.3) 3 (6.5) 24 (52.2) 0 | 0.50 |
†Other antidiarrheal medications were one or more of diosmectite, racecadotril and Saccharomyces boulardii or Lactobacillus GG.
ORS: Oral rehydration solution; SD: Standard deviation.
GT was significantly superior to OAM in reducing the duration of diarrhea. The mean time to normalization of stool consistency (primary end point) was 29.0 ± 2.5 h in the GT group and 45.4 ± 1.1 h in the OAM group (p < 0.0001; Figure 1). At 36 h after the start of treatment, no patient in the GT group had more than 2 stools/day compared with 14 patients in the OAM group. Kaplan–Meier survival analysis of the time to disappearance of diarrhea indicated that the probability of a patient having a liquid stool at 72 h after the start of treatment was 8.7% in the GT group and 67.4% in the OAM group (p < 0.0001; Figure 2).


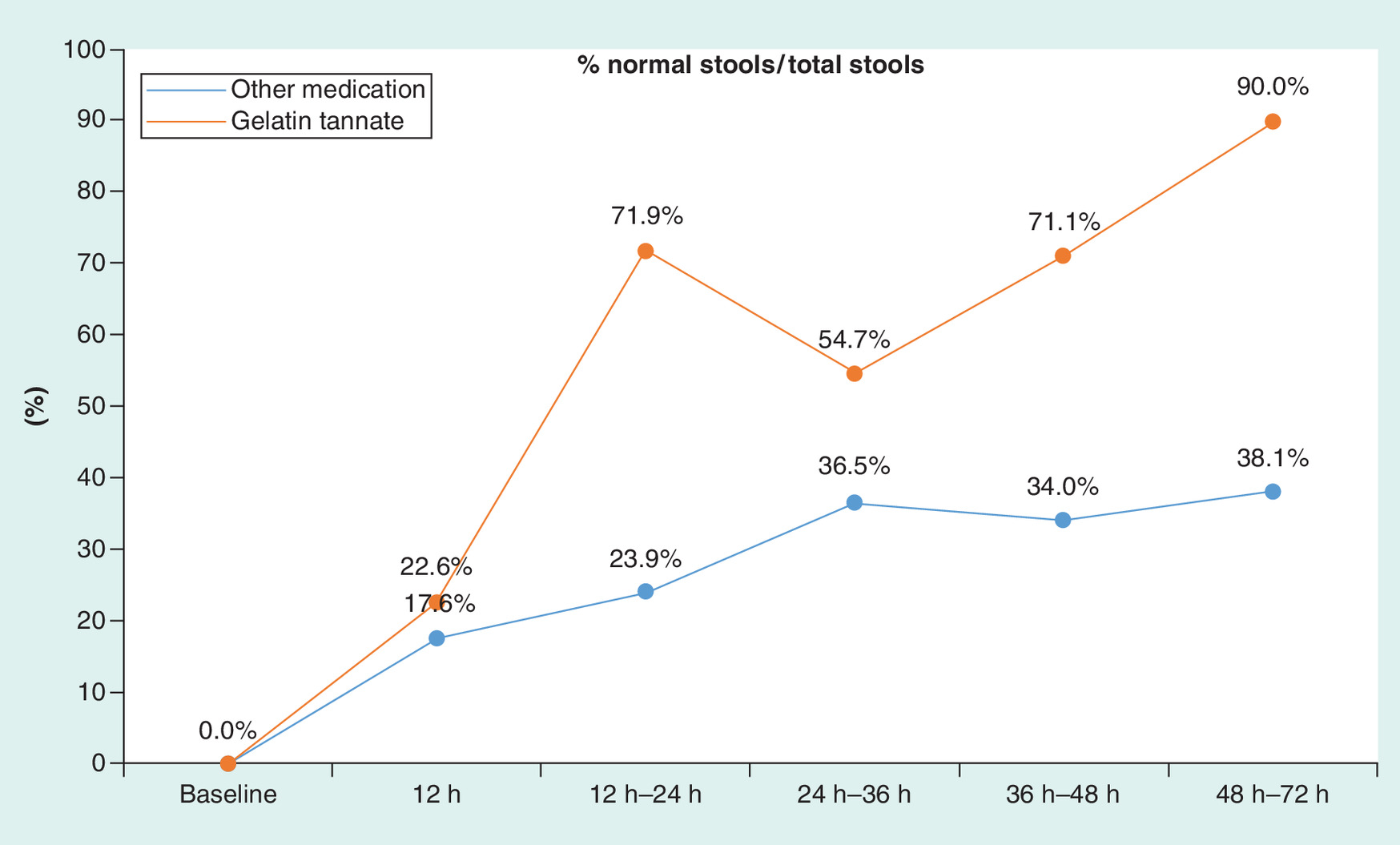
GT was more efficient than OAM in normalizing watery stools. At baseline, there were no normal stools in either group (GT group: 167 liquid stools; OAM group: 217 liquid stools). At 72 h after the start of treatment, 90.0% (36/40) and 38.1% (24/63) of total stools in the GT group and OAM group, respectively, were of normal consistency; a treatment effect in favor of GT was apparent from 12 h onward (Figure 3). At 72 h after the start of treatment, a significantly greater proportion of patients treated with GT than OAM had no stools or normal stools (87.0 vs 30.4%; p = 0.026).
At 48 h from the start of treatment, the proportion of patients with complete recovery from liquid stools was higher with GT than OAM (67.4 vs 15.2%), whereas treatments were equally effective with respect to the proportion of patients with no vomiting (95.7 vs 97.8%).
There were no differences between GT and OAM with regard to changes in bodyweight.
The average length of hospital admission was 5 days in both treatment groups.
No adverse events were reported in either treatment arm during the study.
Discussion
The current study, which involved retrospective review and analysis of medical records of children hospitalized for AGE at a single center in Romania and treated by the same physician, indicated that GT ( ± ORS) at the recommended daily dosage for patient age led to quicker and more effective symptomatic improvement than conventional therapy with one or more of disomectite, racecadotril, and specific probiotic agents (± ORS). The OAM group reflected standard of care treatment for AGE in children according to European guidelines current at the time of the study [1]. Mean duration to the last liquid stool, or stool normalization time, was 16.4 h shorter in the GT group compared with the OAM group (p < 0.0001). At each time point from 12 h onward, the number of normal stools and the number (and %) of patients with no stools or normal stools was greater in the GT group than in the OAM group.
The results are consistent with those of other studies investigating GT for treatment of AGE in young children. In an observational study reported in 2009, Esteban Carretero and colleagues demonstrated a significant reduction in the mean number of stools and improved stool consistency as early as 12 h after the onset of treatment with GT + ORS compared with ORS alone in 211 Spanish children (mean age 2.5 ± 2.4 years) with acute diarrhea [13]. Three of four randomized controlled trials of GT performed to date in children with AGE have reported significant symptomatic improvement with GT compared with control [14–17]. Similar to our own findings, Italian investigators reported a significant reduction in the mean duration of diarrhea with GT + ORS versus ORS alone (76.8 vs 108.0 h; p < 0.0001) in 60 children with AGE [14]. With regards to the efficiency of the treatment effect, two independent Turkish groups reported significant reductions in stool frequency in favor of GT over placebo within the first 12 [15] or 24 h [16] of treatment in children with AGE. Conversely, a recently reported randomized controlled trial from Poland comparing GT and placebo as an adjunct to standard ORS therapy in children with AGE failed to show differences between treatment arms for diarrhea duration or any other outcome measure [17]. These authors discuss in detail the methodological differences which may have led to the contradictory findings between their study and previous randomized studies of GT and call for ‘further well-designed and carefully conducted randomized controlled trials’ to provide a definitive answer about the efficacy of GT. Meanwhile, the weight of evidence suggests that GT may be of value in managing AGE in children.
The absence of adverse events observed with either treatment during the study aligns with the results of previous studies of GT in children with AGE in which either no or few adverse events were reported [14–17]. The risk of adverse events with GT is considered minimal due to lack of systemic absorption of the complex [8]. Safety is always a major consideration when evaluating medications indicated for use in children.
The study is limited by its retrospective observational design, which can introduce selection bias and by the single-center setting, which can limit generalizability of the results to other settings and geographic locations. Conversely, the fact that all children were treated by the same pediatric gastroenterologist, who was also responsible for extracting the data from the medical records, reduces interinvestigator variability. Although an observational study may not provide the same level of evidence as a randomized controlled trial, it offers valuable insight into the use of an intervention in the target patient population under usual clinical practice conditions.
Conclusion
This study adds to the evidence that GT, alone or in combination with ORS, can alleviate AGE-associated symptoms in children more effectively and more efficiently than conventional treatment (i.e., one or more of disomectite, racecadotril, and specific probiotic agents ± ORS). Although GT is not endorsed in current guidelines as an option for treating AGE in children [1,2], it offers an interesting alternative to standard pharmacological therapy.
Treatment of acute gastroenteritis (AGE) aims to prevent/correct dehydration, promote weight regain after rehydration, and decrease the duration/severity of diarrhea and secondary morbidity.
This retrospective, observational study involved children aged 6 months to 7.9 years in Romania who were hospitalized for AGE, with a maximum symptom duration of 72 h before admission.
Medical records were reviewed and compared for 46 patients treated with gelatin tannate (GT) ± oral rehydration solution (ORS) and 46 patients treated with other antidiarrheal medication (OAM) consisting of one or more of disomectite, racecadotril, and Saccharomyces boulardii or Lactobacillus GG ( ± ORS), between 1 December 2012 and 9 March 2018.
Patients were treated for a maximum of 72 h.
GT significantly reduced the time to last liquid stool: 29.0 ± 2.5 h versus 45.4 ± 1.1 h with OAM (p < 0.0001).
At 72 h, significantly more patients treated with GT presented no stools or normal consistency stools compared with patients treated with OAM (87.0 vs 30.4%; p = 0.026).
The probability of a patient having a liquid stool at 72 h after the start of treatment was 8.7% in the GT group and 67.4% in the OAM group (p < 0.0001).
No adverse events were reported with either treatment during the study.
GT presents an interesting alternative for treating AGE in children.
Author contributions
ED Serban was responsible for conception and design of the study, and performed the data acquisition and data interpretation. M Manolache performed the data analysis. ED Serban contributed substantially to drafting of the manuscript and revising it critically for important intellectual content. The authors provided final approval of the version to be published.
Financial & competing interests disclosure
ED Serban has participated as a clinical investigator and/or advisory board member and/or consultant and/or speaker for Abbvie, Montavit, Nestle, Noventure, Nutricia and Reckitt Benckiser. M Manolache is a full-time employee of CEBIS International (Bucharest, Romania). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Medical writing assistance was provided by Kerry Dechant of Content Ed Net. Financial support for the study and for medical writing assistance was provided by Noventure SL, Barcelona, Spain.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Data sharing statement
The authors certify that this manuscript reports original clinical trial data. The data will not be made publicly available.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Guarino A, Ashkenazi S, Gendrel D et al. European Society for pediatric gastroenterology, hepatology, and nutrition/european society for pediatric infectious diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J. Pediatr. Gastroenterol. Nutr. 59(1), 132–152 (2014).
2.
Guarino A, Lo Vecchio A, Dias JA et al. Universal recommendations for the management of acute diarrhea in non-malnourished children. J. Pediatr. Gastroenterol. Nutr. 67(5), 586–593 (2018).
•• New international clinical recommendations for the management of children with acute gastroenteritis.
3.
Lo Vecchio A, Vandenplas Y, Benninga M et al. An international consensus report on a new algorithm for the management of infant diarrhoea. Acta Paediatr. 105(8), e384–e389 (2016).
•• Evidence-based sequence of interventions to optimize management of acute diarrhea in infant.
4.
Farthing M, Salam MA, Lindberg G et al. Acute diarrhea in adults and children: a global perspective. J. Clin. Gastroenterol. 47(1), 12–20 (2013).
5.
Faure C. Role of antidiarrhoeal drugs as adjunctive therapies for acute diarrhoea in children. Int. J. Pediatr. 2013, 612403 (2013).
6.
Piqué N, Gómez-Guillén MDC, Montero MP. Xyloglucan, a plant polymer with barrier protective properties over the mucous membranes: an overview. Int. J. Mol. Sci. 19(3), pii: E673 (2018).
7.
Pleşea Condratovici C, Bacarea V, Piqué N. Xyloglucan for the treatment of acute gastroenteritis in children: results of a randomized, controlled, clinical trial. Gastroenterol. Res. Pract. 2016, 6874207 (2016).
8.
Bueno L, Sekkal S, Theodorou V, Dattilo M. Undissociated gelatin tannate reduces intestinal leakiness and mucosa inflammation by forming a protective biofilm: results from in vitro and in vivo studies. United European Gastroenterol. J. 1(Suppl 1.), A75–A76 (2013).
9.
Lopetuso LR, Scaldaferri F, Bruno G, Petito V, Franceschi F, Gasbarrini A. The therapeutic management of gut barrier leaking: the emerging role for mucosal barrier protectors. Eur. Rev. Med. Pharmacol. Sci. 19(6), 1068–1076 (2015).
10.
De Servi B, Moreira Da Silva R, Meloni M. New insights into the mechanism of action of gelatin tannate for acute diarrhoea. Part 2: antibacterial activity. Presented at: 33rd Congress of the Groupe Francophone d'Hépato-Gastroentérologie et Nutrition Pédiatriques. Nantes, France, 30 March 2012.
11.
Frasca G, Cardile V, Puglia C, Bonina C, Bonina F. Gelatin tannate reduces the proinflammatory effects of lipopolysaccharide in human intestinal epithelial cells. Clin. Exp. Gastroenterol. 5, 61–67 (2012).
12.
Scaldaferri F, Lopetuso LR, Petito V et al. Gelatin tannate ameliorates acute colitis in mice by reinforcing mucus layer and modulating gut microbiota composition: emerging role for ‘gut barrier protectors’ in IBD? United European Gastroenterol. J. 2(2), 113–122 (2014).
• In vivo evidence for the mechanisms of action of gelatin tannate.
13.
Esteban Carretero J, Durbán Reguera F, López-Argüeta Alvarez S, López Montes J. A comparative analysis of response to ORS (oral rehydration solution vs. ORS + gelatin tannate in two cohorts of pediatric patients with acute diarrhea. [Article in English, Spanish]. Rev. Esp. Enferm. Dig. 101(1), 41–48 (2009).
14.
Mennini M, Tolone C, Frassanito A, Midulla F, Cucchiara S, Aloi M. Gelatin tannate for acute childhood gastroenteritis: a randomized, single-blind controlled trial. Paediatr. Drugs 19(2), 131–137 (2017).
15.
Kara SS, Volkan B, Erten Ì. The therapeutic effect of gelatin tannate in acute diarrhea in children. Turkish J. Pediatr. 59, 531–536 (2017).
16.
Çağan E, Ceylan S, Mengi Ş, Çağan HH. Evaluation of gelatin tannate against symptoms of acute diarrhea in pediatric patients. Med. Sci. Monit. 23, 2029–2034 (2017).
17.
Kołodziej M, Bebenek D, Konarska Z, Szajewska H. Gelatine tannate in the management of acute gastroenteritis in children: a randomised controlled trial. BMJ Open 8(5), e020205 (2018).
18.
Freedman SB, Eltorky M, Gorelick M. Pediatric Emergency Research Canada Gastroenteritis Study Group. Evaluation of a gastroenteritis severity score for use in outpatient settings. Pediatrics 125(6), e1278–85 (2010).
19.
Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 32(9), 920–924 (1997).
Information & Authors
Information
Published In
Copyright
© 2019 Future Medicine Ltd.
History
Received: 6 August 2018
Accepted: 19 November 2018
Published online: 15 January 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Gelatin tannate versus other antidiarrheal medication in children with acute gastroenteritis: a retrospective, observational study. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0082
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Yu‐Rou Jiang, Ren‐Jie Liu, Jun Tang, Meng‐Qi Li, Ding‐Kun Zhang, Zhao‐Qing Pei, San‐Hu Fan, Run‐Chun Xu, Hao‐Zhou Huang, Jun‐Zhi Lin, The health benefits of dietary polyphenols on pediatric intestinal diseases: Mechanism of action, clinical evidence and future research progress, Phytotherapy Research, 10.1002/ptr.8218, 38, 7, (3782-3800), (2024).
- J. Esquena-Moret, A Review of Xyloglucan: Self-Aggregation, Hydrogel Formation, Mucoadhesion and Uses in Medical Devices, Macromol, 10.3390/macromol2040037, 2, 4, (562-590), (2022).
- Martin Gregora, Self-treatment of diarrheal diseases in children - what to recommend in the pharmacy, Praktické lékárenství, 10.36290/lek.2022.019, 18, 2, (92-95), (2022).
- Martin Gregora, Common and rare complications of gastroenteitis, Pediatrie pro praxi, 10.36290/ped.2021.023, 22, 2, (125-128), (2021).
- Carmen Alonso-Cotoner, Mar Abril-Gil, Mercé Albert-Bayo, John-P. Ganda Mall, Elba Expósito, Ana M. González-Castro, Beatriz Lobo, Javier Santos, The Role of Purported Mucoprotectants in Dealing with Irritable Bowel Syndrome, Functional Diarrhea, and Other Chronic Diarrheal Disorders in Adults, Advances in Therapy, 10.1007/s12325-021-01676-z, 38, 5, (2054-2076), (2021).