Use of echocardiograms in the Medicare population: a diagnostic tool in the fight against severe aortic stenosis
Abstract
Aim: To estimate undiagnosed aortic stenosis (AS) in the Medicare population. Methods: Patients enrolled (2011–2014) were eligible. After criteria were applied, time zero was the first record of an echocardiogram (ECHO) for the ECHO-AS cohort and randomly assigned for the no-ECHO cohort. The ECHO-AS cohort was propensity matched to patients in the no-ECHO cohort, and survival analysis was performed. Results: Of the 854,493 (25%) patients who received an ECHO, 1 in 4 were diagnosed with AS. After propensity matching, the no-ECHO cohort who died, almost half (49%) had a record of a cardiovascular event prior to their death. The no-ECHO cohort had statistically significant (p = 0.003) higher risk of death than their ECHO-AS counterparts. Conclusion: In the Medicare population, patients aged 65 years or older, with increased risk factors for and symptoms common in AS patients, should be considered for diagnostic ECHOs.
Moderate-to-severe valvular heart disease (VHD) is common in developed countries. VHD is present in about 5 million Americans, or 2.5% of the US population, and increases with age, affecting 4–9% of people aged 65–74 years and 12–13% of people aged 75 years and older [1–3]. Aortic stenosis (AS), defined as a narrowing of the aortic valve opening that restricts blood flow from the left ventricle to the aorta, is the most prevalent VHD in western populations [4]. It is estimated to be present in 12.4% of the population aged 75 years and above in Europe and North America, and its prevalence is expected to increase as the population ages, thereby increasing the healthcare burden of VHD [2,4,5].
Missed diagnoses, undertreatment and high mortality rates, all contribute to the growing healthcare burden associated with AS. Patients with VHD are often underdiagnosed because the disease may be asymptomatic, underlying chronic conditions may mask symptoms, or, as is sometimes the case with elderly patients, physical examinations may appear normal due to the effects of aging on the cardiovascular system [1,6]. Even if diagnosed, many patients with severe, symptomatic AS do not undergo aortic valve replacement (AVR) [2,7–9]. Those patients with severe AS who do not get an AVR have survival rates as low as 50% at 2 years and 20% at 5 years [10].
Physical examination does allow for the detection of asymptomatic VHD; but, an echocardiogram (ECHO) is the gold standard diagnostic tool used to assess the severity and evaluate the prognosis of VHDs [4]. However, not all Medicare patients receive an ECHO, making it difficult to diagnose and evaluate the severity of VHD. The objective of this study was twofold. First, investigators aimed to examine the rate of diagnostic ECHO testing in the Medicare population. The second objective was to quantify the occurrence of potentially undiagnosed AS by comparing outcomes of patients who were diagnosed with AS and received an ECHO to patients who did not receive an ECHO nor had a diagnosis of VHD, but had similar comorbidity and symptom profiles to patients with AS who received an ECHO. Analyses were conducted using the Medicare fee-for-service (FFS) database. Coding for both transthoracic ECHOs and transesophageal ECHOs was used for the analysis (Supplementary Table 1).
Methods
Data source
Data were derived from the Medicare Limited Dataset Standard Analytic Files for beneficiaries enrolled in FFS Medicare from 1 January 2011, to 31 December 2014. These data contain detailed information from claims submitted by providers, which include, but are not limited to, an encrypted beneficiary identifier, the identity of the provider of the services, Medicare program payments and beneficiary responsibility, from and through dates, and, where appropriate, admission and discharge dates. The data also contain information on the following for institutional providers: the source of admission and discharge destinations (including death), International Classification of Disease (ICD)-9 and ICD-10 diagnosis and procedure codes, revenue centers, Current Procedural Terminalogy (CPT) and Healthcare Common Procedure Coding System (HCPCS) codes, and charges associated with those services. A separate file provides annual demographic and enrollment information for all Medicare beneficiaries.
Services that are covered by Medicare FFS Parts A and B are reported by hospitals (inpatient and outpatient basis), nursing facilities (postacute skilled services only), home health agencies, freestanding clinics, ambulatory surgical centers, physicians and nonphysician practitioners, and medical equipment suppliers. Unfortunately, while the Medicare claims database offers great coding detail, it does not provide electronic medical record detail, only Medicare claims. Therefore, researchers did not have access to ECHO data. They could see if a patient had an ECHO and what diagnoses they received but could not determine the severity of the diagnosis.
Defining the cohorts
Patients were considered for this study if they were enrolled in Medicare part A and B (5% Standard Analytic Files Medicare FFS) from 1 January 2011 to 31 December 2014. First, patients were divided into two cohorts: those with a record of one or more ECHOs and a diagnosis of AS; and those with no record of an ECHO anytime in the database and no diagnosis of VHD. Patients were excluded if any of the following criteria applied: a patient was aged <65 years old at time zero; a patient had no record of an ECHO, but a diagnosis of VHD, valve procedure or heart failure; a patient had an ECHO, but no diagnosis of valve disease; or a patient was enrolled <6 months before time zero (see Supplementary Data for coding detail).
Next, researchers used propensity matching to refine the original two cohorts into two equally sized, comparable groups. The ECHO-AS cohort was propensity matched to patients with no record of an ECHO using the baseline characteristics, comorbid conditions and clinically relevant symptoms (syncope, dyspnea, angina, edema, fatigue and palpitations) that were recorded at time zero. Time zero for the ECHO-AS cohort was defined as the first record of a patient's ECHO. Investigators used a Gaussian distribution of the mean and standard deviation of days from enrollment to the record of the first ECHO from the ECHO-AS cohort to randomly assign time zeros for patients in the no-ECHO cohort. After matching, patients from the two new, comparable cohorts of equal populations and similar clinical profiles were followed in the database until a record of death; end of enrollment; or end of the database.
Statistical analyses
This study is a descriptive, retrospective database analysis designed to quantify the rate of ECHO testing and the occurrence of undiagnosed AS in the Medicare population. After propensity matching, a survival analysis was performed using a Cox proportional hazards regression analysis, which calculated hazard ratios for time-to-death as well as model covariates of interest: cardiac-related symptoms, age, sex and the Elixhauser Comorbidity Index [11]. Sample selection and creation of analytic variables were performed using the Instant Health Data platform (BHE, MA, USA). Statistical analyses were undertaken with R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria). This research involved secondary analyses of deidentified data and was therefore exempted from institutional review.
Results
Of the total Medicare 5% FFS sample from 1 January 2011, through 31 December 2014 (3,383,990 patients), 2,529,497 (75%) had no record of receiving an ECHO anytime in the database (see attrition diagram in Figure 1). For the 854,493 (25%) patients who had a record of one or more ECHOs, 136,672 (16%) met the additional inclusion criteria of a diagnosis of AS; 6 months of continuous enrollment before time zero (the first instance of their AS diagnosis); and being aged 65 years or older at the time of AS diagnosis (Figure 1). Notably, only 7644 (5.6%) patients with a diagnosis of aortic valve disease had aortic valve replacement (AVR [surgical or transcather]) after diagnosis. The final sample size for each of the two cohorts of interest before matching was 136,672 patients for the ECHO-AS cohort and 1,173,299 patients for the no-ECHO cohort.
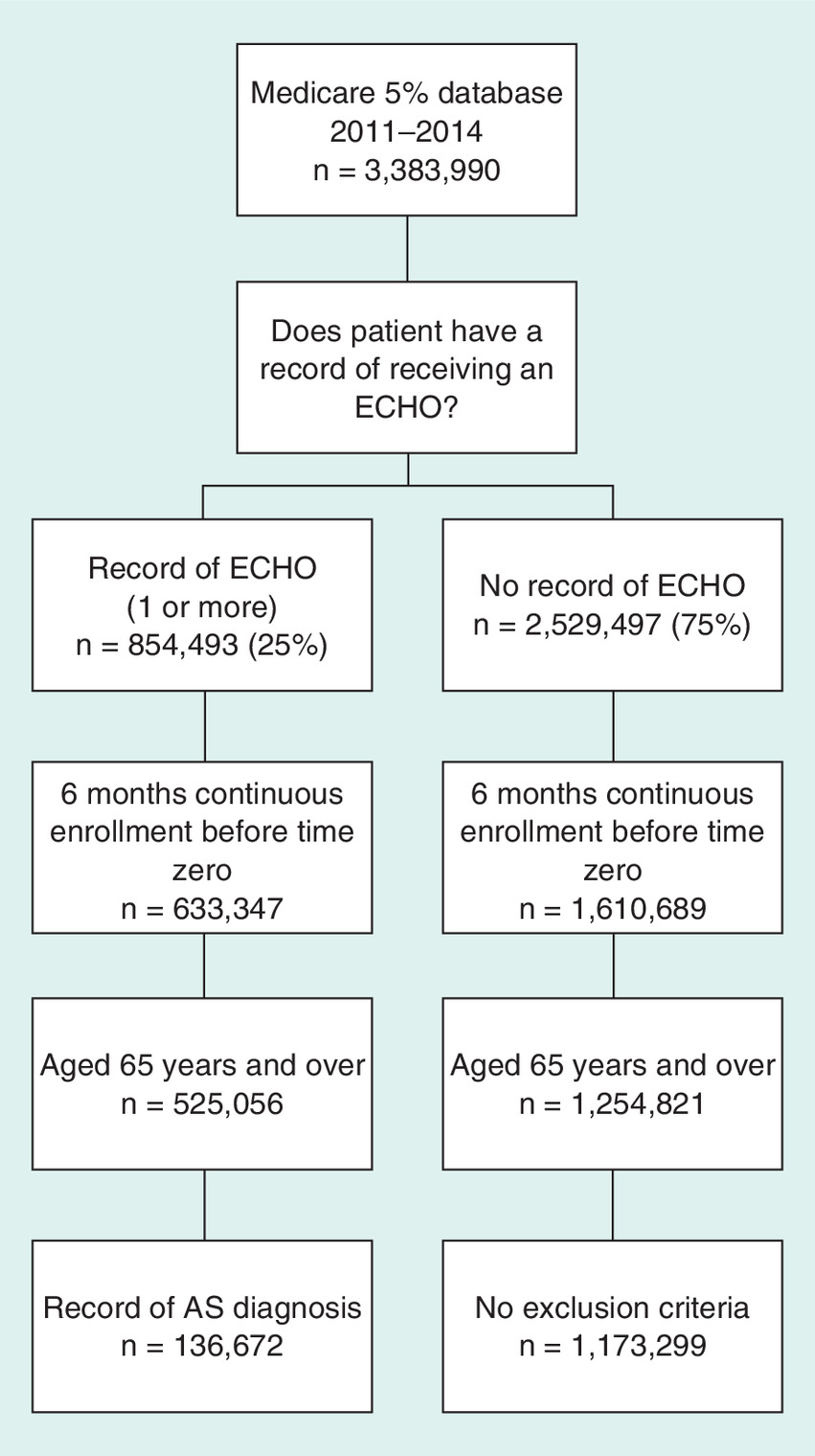
Figure 1. Attrition diagram.
AS: Aortic stenosis; ECHO: Echocardiogram.
For both cohorts, patients’ baseline characteristics before matching are provided in Table 1. Patients who received an ECHO and had AS were older (average age of 78 years) and sicker (Elixhauser score of 5.97) than patients without a record of an ECHO (average age of about 74 years; Elixhauser score of 1.34). Patients from the ECHO-AS cohort also had a much higher rate of symptoms than the no-ECHO cohort (Table 2). ECHO-AS patients experienced dyspnea more than any other symptom (61,686 [45.1%]), followed by fatigue (55,869 [40.9%]). Conversely, patients with no-ECHO experienced fatigue more than any other symptom (136,684 [11.7%]), followed by dyspnea (65,735 [5.6%]). Angina was experienced the least by both cohorts (only 4.1% [5614] of ECHO-AS patients and 0.3% of no-ECHO patients). As expected, the ECHO-AS cohort had higher rates for all of the symptoms. Patients from the ECHO-AS cohort also had higher rates of atrial fibrillation, chronic obstructive pulmonary disease (COPD), hypertension and stroke than their no-ECHO–no-AS counterparts. Over half of the patients without a record of an ECHO (before matching) had no record of COPD, diabetes, stroke, heart failure, hypertension or hyperlipidemia.
| Characteristic | ECHO-AS (n = 136,672) | No-ECHO (n = 1,173,299) |
|---|---|---|
| Age, y, mean (SD) | 78.0 (7.8) | 73.6 (7.3) |
| Sex, no. (%): | ||
| – Female | 73,175 (53.5) | 661,479 (56.4) |
| – Male | 63,496 (46.5) | 511,820 (43.6) |
| Region, no. (%): | ||
| – Midwest | 28,294 (22.3) | 253,425 (22.3) |
| – Northeast | 28,367 (22.3) | 212,771 (18.8) |
| – South | 49,108 (38.7) | 396,144 (34.9) |
| – West | 21,286 (16.8) | 272,247 (24.0) |
| Elixhauser score, mean (SD) | 5.97 (3.1) | 1.34 (2.0) |
AS: Aortic stenosis; ECHO: Echocardiogram; SD: Standard deviation.
| Symptoms, no. (%) | ECHO-AS (n = 136,672) | No-ECHO (n = 1,173,299) |
|---|---|---|
| Angina | 5614 (4.1) | 2986 (0.3) |
| Dyspnea | 61,686 (45.1) | 65,735 (5.6) |
| Edema | 29,467 (21.6) | 46,179 (3.9) |
| Fatigue | 55,869 (40.9) | 136,684 (11.6) |
| Palpitations | 14,480 (10.6) | 18,852 (1.6) |
| Syncope | 18,643 (13.6) | 19,317 (1.7) |
AS: Aortic stenosis; ECHO: Echocardiogram.
After propensity matching, 21,609 patients were assigned to each cohort. Patient demographics, clinical symptoms and the Elixhauser scores for each cohort after matching are shown in Table 3. Although the cohorts were similar, small differences persisted; therefore, variables that remained significant after matching were included as covariates in the Cox regression model. Of the 5291 (24.5%) patients in the no-ECHO cohort who died in the post period, almost half (49%) had a record of a cardiovascular event before their death in the post period (Figure 2). Results of the Cox regression are shown in Table 4. The no-ECHO cohort is statistically significant (p = 0.003) with patients in the no-ECHO cohort at higher risk of death than their ECHO-AS counterparts. Statistically significant symptoms, which increase the risk of death are also shown.
| Variables | ECHO-AS (n = 21,609) | No-ECHO (n = 21,609) |
|---|---|---|
| Age, y, mean (SD) | 76.8 (7.12) | 74.6 (7.22) |
| Sex, no. (%): | ||
| – Female | 11,198 (51.8) | 11,657 (53.9) |
| – Male | 10,411 (48.2) | 9952 (46.1) |
| Region, no. (%): | ||
| – Midwest | 4774 (22.1) | 5296 (24.5) |
| – Northeast | 4373 (20.2) | 4212 (19.5) |
| – South | 8449 (39.1) | 8386 (38.8) |
| – West | 4013 (18.6) | 3715 (17.2) |
| Symptoms, no. (%): | ||
| – Angina | 692 (3.2) | 652 (3.0) |
| – Dyspnea | 8386 (38.8) | 8363 (38.7) |
| – Edema | 3657 (16.9) | 3683 (17.0) |
| – Fatigue | 8165 (37.8) | 8639 (40.0) |
| – Palpitations | 2368 (11.0) | 2632 (12.1) |
| – Syncope | 2692 (12.5) | 2817 (13.0) |
| Average Elixhauser (SD) | 4.46 (2.57) | 4.62 (2.71) |
AS: Aortic stenosis; ECHO: Echocardiogram; SD: Standard deviation.
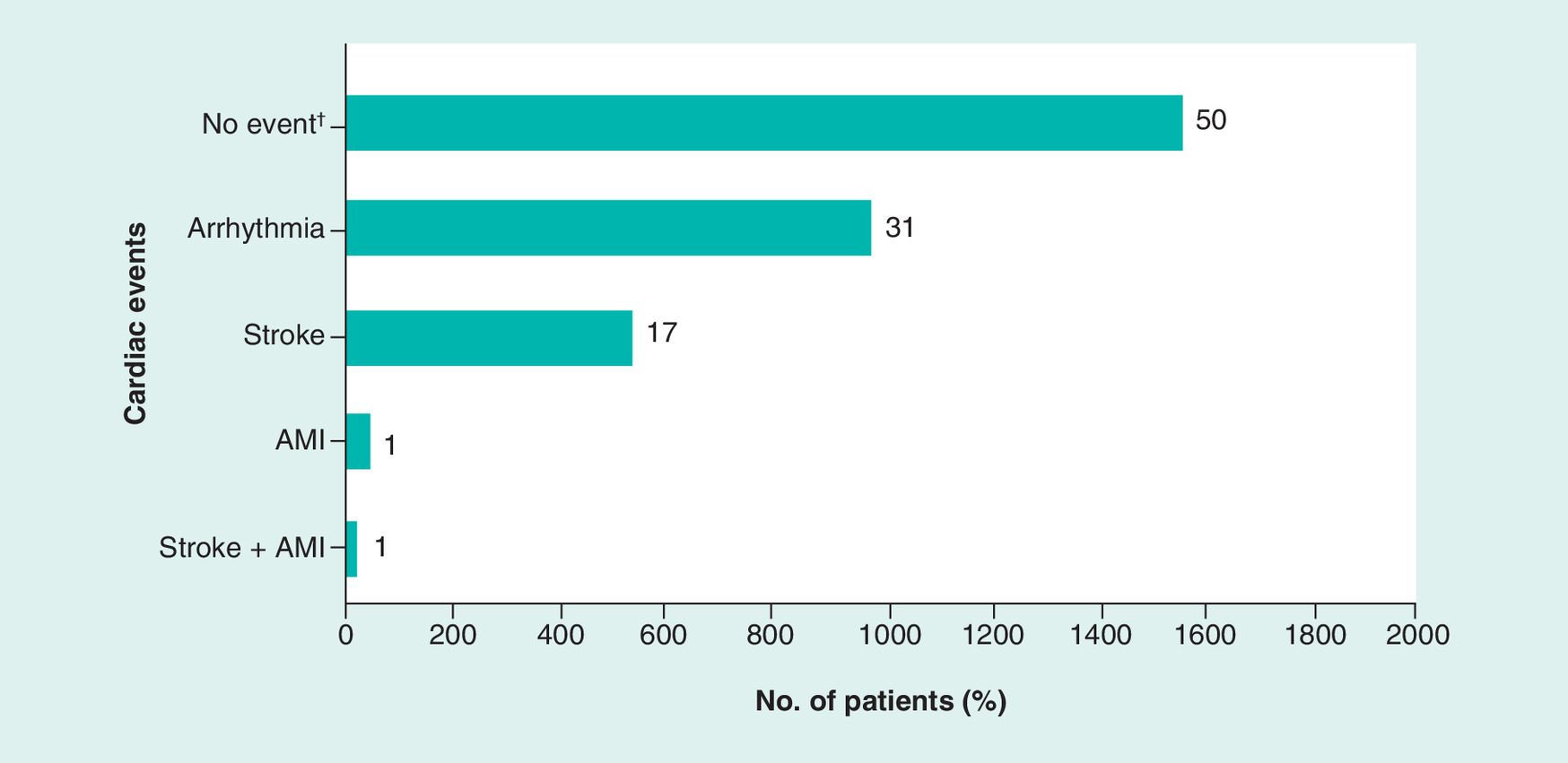
Figure 2. The rate of acute cardiac events in the postperiod for no-echocardiogram patients who died.
†No event means that patients who did not receive an echocardiogram and died did not have a record of arrhythmia, stroke, or AMI at any time in the post period. Of 3128 patients who did not receive an echocardiogram and died in the post period, 1563 had no record of an acute cardiac event such as arrhythmia, stroke or AMI; 977 had an arrhythmia; 530 had a stroke; 40 had an AMI; and 18 had both a stroke and an AMI.
AMI: Acute myocardial infarction.
| Variable | HR | CI |
|---|---|---|
| No-ECHO | 1.07† | 1.03–1.12 |
| Age | 1.08 | 1.08–1.09 |
| Sex, male | 1.36 | 1.31–1.42 |
| Dyspnea | 1.21 | 1.16–1.27 |
| Edema | 1.20 | 1.14–1.26 |
| Fatigue | 1.08 | 1.04–1.13 |
| Elixhauser | 1.19 | 1.19–1.20 |
†Hazard ratio is of interest.
CI: Confidence interval; ECHO: Echocardiogram; HR: Hazard ratio.
Discussion
This study found that only 25% of patients from the Medicare 5% FFS sample aged 65 years and above from 2011 to 2014 received an ECHO. AS is associated with a large, growing healthcare burden [2,6], and ECHOs are a key diagnostic tool when evaluating AS [4]. Baseline characteristics before matching indicated that patients who received an ECHO and had AS were older and sicker than patients without a record of an ECHO, which is a possible explanation for why the younger, healthier population did not receive ECHOs. However, AS is often asymptomatic [6]. Of elderly patients in the USA aged 75 years and above with severe AS, 24.4% are asymptomatic [2]. Patients may go years without developing symptoms; alternatively, mild or generic symptoms may be mistaken for respiratory disease [6]. ECHOs can help differentiate respiratory conditions like COPD from structural heart disease; and, exercise testing and stress echocardiography are also helpful when evaluating patients with VHD [12]. These supplemental tests are recommended to get a more complete picture of the disease and uncover otherwise masked symptoms in patients with asymptomatic AS [12]. Most patients with asymptomatic AS will develop symptoms within 5 years [13]; and, once symptoms like exertional angina, syncope and dyspnea develop, average survival rates for patients with severe AS decrease substantially, ranging from 2 to 5 years [9].
AVR has been shown to improve survival rates [14,15] and is indicated for patients with moderate and severe AS [1]; however, waiting too long to intervene may put excessive risk on patients. Unfortunately, a substantial number of patients do not have valve replacements, even though AVR is indicated for patients with severe AS [2,7,8,15]. The literature suggests that patients may not undergo AVR or opt for a more conservative treatment path because of comorbidities or patient preference, but more commonly, patients do not receive appropriate or timely care because physicians under recognize symptoms, misappropriate symptoms (e.g., mistake AS for a respiratory illness), or overestimate operative risks (including advanced age or left ventricular dysfunction) [7,9,15]. One study by Freed et al. [7] found that of 106 patients with severe AS, only 33 (31%) had undergone AVR and that the main reason that patients with symptomatic severe AS did not have AVR was their symptoms were thought to be unrelated to AS. Of the 73 patients who did not have AVR, 42 patients (58%) were asymptomatic but only 4% had undergone exercise stress testing (another common diagnostic tool for recognizing symptoms related to AS). Freed et al. also found that within 15 months, 15 (14%) of the 73 patients who did not undergo AVR died.
Moreover, a multicenter survey by Bach [8] in 2011 found that, overall, many patients who would potentially benefit from AVR were not evaluated properly for AS. Bach found that only about half of the patients with severe AS were referred to a cardiothoracic surgeon (referrals were more likely if patients had angina, which this study found to be an uncommon symptom) and only about 40% had AVR. Of the remaining patients who did not have surgery, about a fourth were asymptomatic.
This study supports a theme in the literature that patients with VHD are commonly underdiagnosed and undertreated because of a lack of testing [7] and timely referrals [8]. While physical examinations and auscultation do allow for the detection of asymptomatic VHD, ECHOs remain a key diagnostic tool in identifying VHD; yet, only about 25% of Medicare FFS patients had an ECHO, and of the 5291 patients in the no-ECHO cohort who died in the post period, almost half (49%) had a record of a cardiovascular event before their death in the post period (Figure 2). While it is not possible to confirm that these patients had AS, they had cardiovascular disease, which may have been treated correctly if those patients had received an ECHO.
The total Medicare parts A and B population in 2017 aged 65 years and older was estimated to be 49.8 million [16]. Of the 3,383,990 patients in the Medicare 5% FFS Database from 2011 through 2014, the initial sample for this study, 74.7% (2,529,497) did not receive ECHOs. If that percentage is applied to the total aged Medicare population, then 37,224,977 people did not receive ECHOs. Table 2 shows that the most common clinical symptom at baseline before matching among patients in the no-ECHO cohort is fatigue, affecting 11.6% (136,684/1,173,299) of patients (fatigue is also common in the ECHO-AS cohort; only dyspnea affects a slightly higher percentage of people). The least common symptom (in both cohorts) is angina, which is observed in 0.3% (2986) of no-ECHO patients. So, at the most, 11.6% of the no-ECHO group would have a reason to have an ECHO and, at the least, 0.3% should have an ECHO. Taking 0.3 and 11.6% of the total aged Medicare population who did not receive ECHOs yields a minimum and maximum of 94,736 and 4,336,541 patients, respectively. This range represents patients who, based on their symptoms, perhaps should have received ECHOs, but did not.
AS is most prevalent in the Medicare population, affecting 12.4% of people aged 75 years and above [2]. Increasing the frequency in which Medicare patients receive ECHOs will likely improve patient outcomes and help diagnose AS more accurately and efficiently. The ability to effectively diagnose AS will become increasingly relevant as the overall US population ages and the burden of disease increases [2,5]. Utilizing key diagnostic techniques like ECHOs more frequently and effectively will help identify severe AS in the Medicare population, broadening treatment options and improving clinical outcomes. If AS can be diagnosed earlier and more effectively, treatment options and survival rates will improve, and the future impact on public health and healthcare-resource utilization will likely decrease.
Data limitations
The limitations of this study are those that are inherent in retrospective claims-based data analyses, including lack of generalizability to noninsured populations, clinical outcomes being imputed from data not prepared for research purposes, and the under reporting of certain events and diagnoses. Administrative claims data are collected for billing and reimbursement, not for coordinating medical care or conducting outcomes research. The data are subject to coding errors and under reporting of clinical conditions that do not trigger a billable event. For example, ICD-9 diagnosis codes have a specific code for rheumatic AS; however, physicians typically code for AS under the code for aortic valve disease. Therefore, both codes are incorporated into this analysis, which may introduce some overlap with aortic valve diseases.
Additionally, we did not have electronic medical record detail, including laboratory results and physician notes. We only had access to Medicare claims, which also meant that we could not assess ECHO data and the severity of the diagnosis. We only knew if a patient received an ECHO and what diagnoses they received. Therefore, specific medical details could not be determined. This study was not a prospective randomized controlled clinical trial and therefore may have confounding variables and inherent biases. Despite these shortcomings, administrative data have been widely used to evaluate the association between treatments and clinical outcomes, particularly when a portrayal of patient experience outside the controlled setting of the clinical trial is useful.
Conclusion
About 25% of patients in the Medicare population receive an ECHO, and aortic valve disease is diagnosed in about one in four of those patients. After matching, almost 50% of patients without a record of an ECHO who died also had a record of an acute cardiovascular event before their death. In the Medicare population, patients aged 65 years or older with increased risk factors for AS like hypertension, diabetes, COPD and stroke should be considered for a diagnostic ECHO.
This research title utilized data from January 2011 to December 2014 to evaluate the utilization of echocardiograms (ECHO) in the Medicare population.
Patients who received an ECHO and had a subsequent aortic stenosis (AS) diagnosis (ECHO-AS cohort) were propensity matched to patients who did not receive an ECHO (no-ECHO cohort) but had similar comorbidities, demographics and clinically relevant symptoms.
ECHO-AS patients experienced dyspnea more than any other symptom (61,686 [45.1%]), followed by fatigue (55,869 [40.9%]).
Patients from the ECHO-AS cohort had higher rates of atrial fibrillation, chronic obstructive pulmonary disease, hypertension and stroke than their no-ECHO counterparts.
Of the patients in the no-ECHO cohort, who died in the post period, nearly half (49%) had a record of a cardiovascular event prior to their death and the no-ECHO cohort had statistically significant (p = 0.003) higher risk of death than their counterparts in the ECHO-AS cohort.
In the Medicare population, patients aged 65 years or older, with increased risk factors for and symptoms common in AS patients, should be considered for a diagnostic ECHO to detect AS.
Increasing the frequency in which Medicare patients receive ECHOs will help diagnose AS more accurately and efficiently.
Identifying AS in the Medicare population more frequently and efficiently will likely broaden treatment options and improve clinical outcomes.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Financial & competing interests disclosure
This study was sponsored by Edwards Lifesciences. EA Grossi is a consultant to and holds intellectual property with Edwards Lifesciences and Medtronic. KA Moore is an employee of Edwards Lifesciences. C Gunnarsson is a consultant to Edwards Lifesciences. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Material
File (supplementarydata.docx)
- Download
- 40.78 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Nishimura RA, Otto CM, Bonow RO et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 135(25), e1159–e1195 (2017).
•• The US guidelines that drive the diagnosis of treatment of valvular heart disease.
2.
Osnabrugge RL, Mylotte D, Head SJ et al. Aortic stenosis in the elderly: disease prevalence and number of candidates for transcatheter aortic valve replacement: a meta-analysis and modeling study. J. Am. Coll. Cardiol. 62(11), 1002–1012 (2013).
• Highlights the undertreatment and underdiagnosis of severe symptomatic aortic stenosis.
3.
Benjamin EJ, Blaha MJ, Chiuve SE et al. Heart disease and stroke statistics – 2017 update: a report from the American Heart Association. Circulation 135(10), e146–e603 (2017).
• A current update on the prevalence of valvular heart disease.
4.
Vahanian A, Alfieri O, Andreotti F et al. Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. J. Cardiothorac. Surg. 42(4), S1–S44 (2012).
•• The European guidelines, similar to the US guidelines, drive the diagnosis and treatment of valvular heart disease.
5.
Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet 368(9540), 1005–1011 (2006).
•• The original research is the most frequently cited data looking at the prevalence of valvular heart disease.
6.
Helms AS, Bach DS. Heart valve disease. Prim. Care 40(1), 91–108 (2013).
7.
Freed BH, Sugeng L, Furlong K et al. Reasons for nonadherence to guidelines for aortic valve replacement in patients with severe aortic stenosis and potential solutions. Am. J. Cardiol. 105(9), 1339–1342 (2010).
• Provides clarity around the reasons for underdiagnosis and undertreatment of aortic stenosis.
8.
Bach DS. Prevalence and characteristics of unoperated patients with severe aortic stenosis. J. Heart Valve Dis. 20(3), 284–291 (2011).
9.
Varadarajan P, Kapoor N, Bansal RC, Pai RG. Clinical profile and natural history of 453 nonsurgically managed patients with severe aortic stenosis. Ann. Thorac. Surg. 82(6), 2111–2115 (2006).
10.
Otto CM. Timing of surgery in mitral regurgitation. Heart 89(1), 100–105 (2003).
• The original research includes mortality data for valvular heart disease.
11.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med. Care 36(1), 8–27 (1998).
12.
Picano E, Pibarot P, Lancellotti P, Monin JL, Bonow RO. The emerging role of exercise testing and stress echocardiography in valvular heart disease. J. Am. Coll. Cardiol. 54(24), 2251–2260 (2009).
13.
Pellikka PA, Sarano ME, Nishimura RA et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 111(24), 3290–3295 (2005).
• The original research examines the progression of aortic stenosis.
14.
Brennan JM, Edwards FH, Zhao Y et al. Long-term survival after aortic valve replacement among high-risk elderly patients in the United States: insights from the Society of Thoracic Surgeons Adult Cardiac Surgery Database, 1991 to 2007. Circulation 126(13), 1621–1629 (2012).
15.
van Geldorp MW, van Gameren M, Kappetein AP et al. Therapeutic decisions for patients with symptomatic severe aortic stenosis: room for improvement? Eur. J. Cardiothorac. Surg. 35(6), 953–957; discussion 957 (2009).
16.
US Centers for Medicare and Medicaid Services. CMS Fast Facts. US Centers for Medicare and Medicaid Services, MD, USA (2018).
Information & Authors
Information
Published In
Copyright
© 2019 EA Grossi, KA Moore & C Gunnarsson.
History
Received: 16 July 2018
Accepted: 10 December 2018
Published online: 14 January 2019
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Use of echocardiograms in the Medicare population: a diagnostic tool in the fight against severe aortic stenosis. (2019) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0071
Export citation
Select the citation format you wish to export for this article or chapter.