Estimating efficiency of Directive 2011/24/EU cross-border healthcare in member states
Publication: Journal of Comparative Effectiveness Research
Abstract
Aim: Directive 2011/24/EU on patients’ rights in cross-border healthcare facilitates EU citizens' access to and reimbursement for healthcare provided or prescribed in a member state other than the member state of affiliation. Materials & methods: The efficiency of cross-border healthcare policy is evaluated using data envelopment analysis of relevant items in Eurobarometer Survey on Safety and Quality of Care and Patients’ Rights in the EU. Results: Our study shows policy inefficiency in 52% of the 25 EU member states included in the analysis. Addressing difficulties patients encounter while seeking reimbursement from their national health service or health insurer and reducing the number of adverse events patients experience when receiving healthcare improves policy efficiency. Conclusion: Our findings confirm that there is country-level variation in cross-border healthcare policy efficiency.
Improving the health and promoting people’s wellbeing are among the key ambitions of the European Union (EU) and as Article 35 of the EU Charter of Fundamental Human Rights declares:
“A high level of human health protection shall be ensured in the definition and implementation of all Union policies and activities.”
Health in the EU is conceptualized as people’s right and safeguarded in all of the policies of the Union. Legislations in the form of Directives, Regulations and Rulings of the Court of Justice of the European Union are sources of policies in the EU.
Directive 2011/24/EU on patients’ rights in cross-border healthcare defines the conditions under which a patient may travel to another EU country to receive medical care and reimbursement [1] where medical care and reimbursement covers healthcare costs including prescriptions and delivery of medications and medical devices. The Directive prescribes creation of national contact points that provide accurate information to citizens, defines minimum required elements that should be included in medical prescriptions taken from one EU country to another and encourages development of networks of medical expertise, health technology assessments and e-health tools [1]. Directive 2011/24/EU is a critical step toward harmonizing principles in all EU health systems [2] and a wider cooperation in European healthcare. Protection of health across the EU member states can not only be attained with common health and health-related policies but also with similar commitment to their implementation.
Limited number of studies has addressed patient-centered factors related to quality and safety of healthcare services and their effect on policy efficiency. A number of studies have observed geographical, cultural and economic factors resulting in variation in policy implementation of tobacco and alcohol control policies and food policies across the member states [3–5]. Other studies, such as the study by Mackenbach and McKee [6], addressed national-level constructs to assess varied implementation of health policies across European countries. Mackenbach and McKee have identified that countries with high expression values which have rising demands for participation in decision-making in economic and political life compared with countries with high survival values that place emphasis on economic and physical securities differ in implementing policies. Mackenbach and McKee also suggested constructs representing government effectiveness, democracy, left-party participation in government and ethnic fractionalization may influence a state’s policy performance.
A number of common European values such as the welfare tradition and commitment to solidarity, liberalization, privatization, competition and consumer choice driven healthcare systems may help improve efficiencies of health policies [7]. Also, as Dixon and Polteiakhoff [8] proposed the evident convergence of the two main types of health systems in Europe – namely Bismark systems of social health insurance and Beveridge systems of tax-funded universal coverage in Europe make common health policies and their implementation a possibility. However, more research is needed to identify tangible and modifiable factors and predictors that influence policy implementation of states [9].
The European Parliament and Council enacted the Directive 2011/24/EU in the year 2011 and a deadline for its transposition into national legislation in all EU member states was set for the 25th October 2013. Patients move across the EU states for a number of reasons. Free movement in the EU, dissatisfaction with healthcare provision and deficiencies of health systems at home, search for specialist treatment may be some of these reasons explaining patient mobility across the EU [10,11]. Very few studies investigated the implementation of the Directive and the factors associated with its implementation. Greer [12] suggested that lack of patient awareness of the provisions of the Directive led to its low uptake, whereas Vasev and Vrangbæk [13] warned that certain features of the Directive such as the upfront payment of services by the patients and the level of coverage at the member state of affiliation would result in low uptake of the policy by economically disadvantaged citizens. Azzopardi-Muscat et al. report on a study that included seven member states.
With this study, we assess the uptake of the Directive by evaluating efficiency of each member state in implementing it from operational, financial and quality perspective. Efficiency analysis and measurement is a complex task, particularly when conceptual challenges, multiple objectives or great scope of error exist [14].
Organizational efficiency analysis has been pioneered by Farrell [15] to measure the efficiency of organizations or systems. Organizational efficiency refers to “the capacity of an organization, institution or business to produce desired results with a minimum expenditure of energy, time, money, personnel, material” [16]. Here, the countries are conceptualized as the institutions, the desired results are conceptualized as uptake of the Directive while improving quality of care received and reducing problems during reimbursement process. Quality of healthcare is accomplished when adverse events and harms are minimized while receiving healthcare both in the member state of affiliation and in any member state other than the member state of affiliation. Quality at of healthcare at home is critical for motivating inflow of patients, quality of healthcare at other member state other than the state of affiliation would encourage the outflow of patients. Efficiency of the Directive can only be optimized when the patients' mobility are in both directions.
For this study, we use data envelopment analysis (DEA) to measure efficiency [17]. DEA is a nonparametric method that has been previously used in a number of studies to evaluate efficiencies of public policies [18,19], health service evaluation and to inform policy [20–28]. The study evaluates the efficiency of Directive 2011/24/EU on patient’s rights in cross-border healthcare across member states using DEA and attempts to identify further determinants of policy efficiency.
Materials & methods
Data sources
To evaluate the efficiency of the Directive, this study used data from the special Eurobarometer 411 on patient safety and quality of care administered in 2013 and special Eurobarometer 425 on patients' rights in the EU administered in 2014. Items from the Eurobarometer surveys were used as quality and operational success indicators, respectively. The Eurobarometer is a series of public opinion surveys that are administered face-to-face in the appropriate national language to about 1000 persons per member state with residents who are 15 years and older. Number of interviews in Malta, Luxemburg and Republic of Cyprus are approximately 500. The Eurobarometer surveys use stratified random sampling technique in line with population density. The published reports contain no breakdown by gender, age or other characteristics by country. However, technical specifications of the surveys report that a multistage random sampling design has been used and stratified according to sex, age and region (European Commission. Patient Safety and Quality of Care. Special Eurobarometer 411.2014 and European Commission. Patient’s Rights in the EU. Special Eurobarometer 425.2015). The two surveys used in the study have been administered at two different time points and waves where Eurobarometer 411 was administered in 2013 and 425 in 2014. This constitutes one of the limitations of the study. Sample sizes for each wave were 27,919 and 27,868, respectively.
Data were also extracted from other publicly available data sources such as the European Society of Cardiology, World Bank Open Data, International Monetary Fund, World Economic Outlook and Eurostat. Complete data were available for 25 of the 28 EU member states, therefore, analyses were performed with only 25 member states. Lithuania, Luxemburg and Malta were excluded from analysis due to incomplete data. The year 2014 was taken as the reference year for all other publicly available data.
Analyses
Analysis was carried out in two stages. In the first stage, efficiency of the Directive was evaluated using DEA for each of the 25 member states. In the second stage of analysis, further determinants of policy efficiency were identified through multiple regression analysis.
Data envelopment analysis
The linear programming model [29] using WinQSB 2.0 software is used to evaluate efficiencies, where decision-making units (DMUs) are the 25 EU member states included in the study.
Efficiency analysis involves three main steps. In the first step, DEA is used to derive efficiencies of comparable units known as DMUs and identifies DMUs that perform the best. Here, the DMUs are the EU member states. DEA assigns an efficiency score of 1 (100%) to efficient DMUs, and a score less than 1 to inefficient ones [30]. First hyperbolic distance function (HDF) of Färe et al. [29] is used to calculate efficiencies and efficiency weights. Next, the HDF model is adapted to the hyperbolic ranking model of Johnson and McGinnis [31] to rank each country in terms of efficiency. In the final step of the analysis, using an efficiency improvement model and using UK’s efficiency as the target, as it is the most efficient and highest ranking country determined by the first steps of the analysis, the percentage reduction required for key quality and operational indicators (x1, 2 and 3) to reach efficiency for every country is calculated.
Inputs and outputs for DEA have been chosen based on the objectives of the Directive. Improving the quality of healthcare in the member state of affiliation and in any member state other than the member state of affiliation improves the implementation of the Directive. Therefore, improving quality by minimizing harm and adverse events or harm patients experience while receiving medicines (nonhospital care), diagnosis (nonhospital care) or treatment (hospital care) in their state of affiliation or in any other member states improves implementation of the Directive. Adverse events may be “healthcare-associated infections, medication-related errors, surgical errors, medical device failures, errors in diagnosis and failure to act on the results of tests” [32]. Also, operationally reducing problems during the reimbursement process for healthcare and medicines received in any other member state other than the member state of affiliation will improve uptake of the Directive. The efficiency model utilized here aims to minimize factors that discourage and maximize factors that promote implementation of the Directive. Table 1 describes the selected inputs and outputs used in efficiency analysis.
| Variables | Role | Indicator | Definition | Source |
|---|---|---|---|---|
| Harmed by hospital | Input (x1) | Quality | Percentage of people that answered yes, they think patients are most likely to be harmed by hospital care | QC6a (EB-411). How likely do you think patients could be harmed by hospital care in our country? |
| Harmed by nonhospital | Input (x2) | Quality | Percentage of people that answered yes, they think patients are most likely to be harmed nonhospital healthcare | QC6b (EB-411). How likely do you think patients could be harmed by nonhospital care in our country? |
| Reimbursement problem | Input (x3) | Operational | Number of people that answered yes, they encounter problems getting reimbursement from their national health service or health insurer | QD7 (EB-425). Thinking about the last you received treatment in another EU country, did you encounter any problems getting reimbursement from your national health service or health insurer? |
| Health expenditure | Input (x4) | Operational | Health expenditure per capita | World Bank |
| No. of adverse events | Output (y1) | Quality | Number of people that answered no, they did not experience any adverse events when receiving treatment in another EU country | QC7 (EB-411). Have you or your family member ever experienced adverse event when receiving healthcare in another EU country? |
| Medical treatment in another EU country | Output (y2) | Operational | Number of people that answered yes, they have received any medical treatment in another EU country | QD6 (EB-425). Have you received treatment in another EU country in the last 12 months? |
EU: European Union.
The quality indicators used in the efficiency evaluation are participant responses to QC6a and QC6b, which are considered as inputs (x1 and x2), and QC7 as output (y1) from the Eurobarometer 411 [32]. The operational indicators used in the efficiency evaluation are participant responses to QD7 (x3), which is considered as an input and QD6 (y2), which is considered as an output from the Eurobarometer 425 [33]. Health expenditure per capita has also been used as an input (x4) [34].
Multiple regression analysis
Multiple regression analysis was performed using IBM Statistics SPSS 20. Efficiency scores calculated in the DEA were used as the dependent variable while the number of civil society umbrella organizations working in the field of cross-border healthcare (data from European Patients Forum), number of specialist doctors (Eurostat), number of cardiovascular disease hospitals (European Society of Cardiology), gross domestic products (GDP; World Development Indicators) and the population (World Development Indicators) were the independent variables. The aim of the analysis was to identify further determinants of efficiency of the Directive.
These independent variables were chosen following a literature review on factors that may affect patient mobility. Patient mobility in the EU could be explained in a number of ways [35]. One of the reasons why patients decide to get services elsewhere is the absence of highly specialized services with specialist healthcare as these services might not be cost effective in smaller countries, therefore their existence could be associated with utilization of the Directive [36]. For this reason, number of specialist doctors, number of specialist hospitals specifically cardiovascular disease were chosen to be included in the analysis.
Evidence from the literature also indicates resources as playing a critical role affecting transposition and implementation of this Directive [13]. For this reason, GDP was included in the analysis.
The report on the Cross-border Healthcare Directive also indicated lack of awareness among European citizens about their right to choose healthcare in another country as an obstacle to the uptake of the Directive [37]. Smith et al. [38] emphasize civil society organizations’ role in ensuring right to health is enjoyed by all. Number of civil society umbrella organizations who were members of European Patients Forum working in the field of cross-border healthcare were seen as a proxy indicator of patient awareness and used in the analysis.
Results
DEA determined the average efficiency score as 0.93 (93%), suggesting overall inefficiency of the Directive (Table 2) in the EU countries. Only 12 (48%) of the members states had efficiency of the Directive. Further analysis with the hyperbolic ranking model of Johnson and McGinnis [31] determined United Kingdom, Austria and Romania ranking the highest in efficiency, while Netherlands, France and Republic of Cyprus ranking the lowest in efficiency. HDF identified the number of adverse events when receiving care in a member state other than the member state of affiliation and the number of patients who reported encountering problems getting reimbursed for cross-border treatments as the two factors (Table 3), contributing the most to efficiency of the Directive.
| Country | Efficiency (%) | Rank |
|---|---|---|
| Austria | 100 | 2 |
| Belgium | 83.5 | 22 |
| Bulgaria | 100 | 7 |
| Croatia | 100 | 8 |
| Cyprus | 73.3 | 25 |
| Czech Republic | 96.5 | 15 |
| Denmark | 87.2 | 20 |
| Estonia | 100 | 10 |
| Finland | 100 | 9 |
| France | 74.2 | 24 |
| Germany | 100 | 11 |
| Greece | 90.9 | 18 |
| Hungary | 100 | 4 |
| Ireland | 98.1 | 14 |
| Italy | 100 | 6 |
| Latvia | 100 | 11 |
| Netherlands | 78.7 | 23 |
| Poland | 100 | 5 |
| Portugal | 99.1 | 13 |
| Romania | 100 | 3 |
| Slovakia | 94.7 | 16 |
| Slovenia | 85.4 | 21 |
| Spain | 94.6 | 17 |
| Sweden | 90 | 19 |
| United Kingdom | 100 | 1 |
| Average | 93.8 |
| No. adverse event (y1) | Medical treatment in another EU country (y2) | Harmed by hospital care (x1) | Harmed by nonhospital (x2) | Problems getting reimbursement (x3) | Total health expenditure (x4) | |
|---|---|---|---|---|---|---|
| Average | 0.46318 | 0.1406 | 0.2744 | 0.2571 | 0.5313 | 0.1956 |
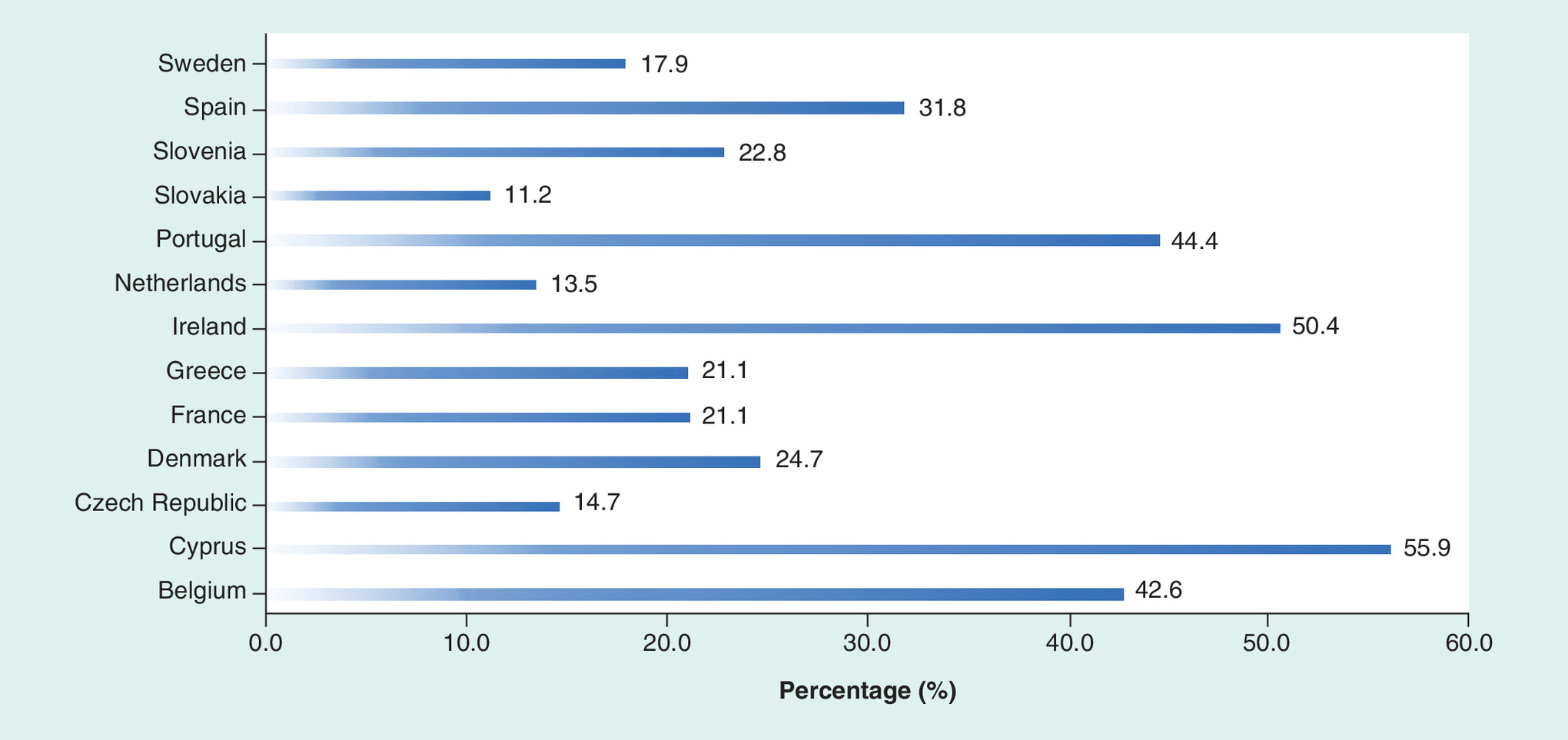
The results of the efficiency improvement model (Figure 1) indicate that Sweden is able to reach efficiency by making an improvement of 17.9% in quality and operation indicators by reducing hospital and nonhospital harm and number of patient encountering reimbursement problems. While Cyprus and Ireland need an improvement of 55.9 and 50.4%, respectively, in the quality and operational indicators to attain efficiency.
Multiple regression analysis was used to test if the number of civil society umbrella organizations working on health issues, number of specialist doctors, number of specialized hospitals, GDP or population size significantly predicted efficiency of the Directive. The evidence from the data failed to reject the null hypothesis, which states that the independent variables do not predict efficiency. This result could be due to small sample size [38].
Discussion & conclusion
Directive 2011/24/EU on patients' rights in cross-border healthcare facilitates EU citizens' access to and reimbursement for healthcare provided or prescribed in a member state other than the member state of affiliation. This study evaluates the efficiency of cross-border healthcare policy using DEA of relevant items in Eurobarometer survey on safety and quality of care and patient's rights in the EU. The study indicates that more than half of the EU member states included in the study attained efficiency of the Directive, however, variations in the uptake of the Directive are also evident. Countries with similar welfare traditions and close geographical proximity are expected to have well-established cross-border collaborations, therefore display similar trends in the uptake of the Directive [39]. While use of routine data for monitoring of efficiency proves advantages, the use of different populations might pose a limitation. However, the probability sampling strategy employed for data collection may have minimized this limitation. Differences in the uptake of the Directive were expected between older and newer members of the EU [13], findings of the study suggest that such trend is not evident. The study therefore demonstrates that explanations behind uptake of common policies might be complex and varied. The study demonstrates that the use of explorative approaches and tools commonly used in other disciplines to investigate the workings of policies and proposes how efficiency of policies could be improved.
Common health policies are needed to deal with common health challenges posed by aging populations, infectious diseases, antimicrobial resistance, shortage of blood products and humanitarian conflicts. Further studies are needed to better understand the emergence and implementation of EU norms and specifically common health policies.
Future perspective
Addressing uptake of common policies and practices requires multidisciplinary approaches. Explorative tools will be critical in furthering our understanding of efficiency of existing common policies and ways of improving implementation. Secondary analysis of readily available data is critical in exploratory studies specifically in policy analysis.
•
The study evaluated the efficiency of Directive 2011/24/EU on patient’s rights in cross-border healthcare using data envelopment analysis.
•
The study ranked 25 EU member states according to their respective efficiencies in implementation of Directive 2011/24/EU on patient’s rights in cross-border healthcare.
•
The study assessed the contribution of quality and operational inputs and other relevant factors to efficiency of the Directive 2011/24/EU on patient’s rights in cross-border health.
•
Quality of care is measured by the number of adverse events and harms reported Eurobarometer surveys on safety and quality of care and patient’s rights in the EU.
•
Problems encountered during reimbursement is a critical operational indicator contributing to efficiency of the Directive.
•
Reduction in number of adverse events experienced in and problems encountered during reimbursement for healthcare provided or prescribed in a member state other than the member state of affiliation contribute most to the efficiency of the Directive.
Author’s contributions
MD Ibrahim, MB Hocaoglu and B Numan conceptualized the study. MD Ibrahim and MB Hocaoglu extracted the data. MD Ibrahim and S Daneshvar performed the efficiency analysis. All the authors investigated the results and supervised the findings. All the authors discussed the results and contributed to the final manuscript.
Acknowledgements
The authors thank the reviewers for their invaluable feedback.
Financial & competing interests disclosure
The authors thank the Institute of Graduate Studies and Research, Research Advisory Board at Eastern Mediterranean University in Cyprus for providing us with the funding to partake in Europe in Discourse Conference where this study was presented. The draft version of this paper has been published in 1st Europe in Discourse Conference Proceedings. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest
1.
European Commission. Directive 2011/24/EU on patients’ rights in cross-border healthcare. https://ec.europa.eu/health/cross_border_care/overview_en
2.
Azzopardi-Muscat N, Baeten R, Clemens T et al. The role of the 2011 Patients' Rights in Cross-border Health Care Directive in shaping seven national health systems: looking beyond patient mobility. Health Policy 122(3), 279–283 (2018).
3.
Österberg EL. Alcohol tax changes and the use of alcohol in Europe. Drug Alcohol Rev. 30(2), 124–129 (2011).
• Identifies policy implementation gaps among EU countries with a subject of tax changes.
4.
Elmadfa I, Meyer A, Nowak V et al. European nutrition and health report. Forum Nutr. 62, 1–405 (2009).
5.
Gruning T, Gilmore AB, McKee M. Tobacco industry influence on science and scientists in Germany. Am. J. Public Health 96(1), 20–32 (2006).
6.
Mackenbach JP, McKee M. A comparative analysis of health policy performance in 43 European countries. Eur. J. Public Health 23(2), 195–201 (2013).
7.
Greer SL, Hervey TK, Mackenbach JP, McKee M. Health law and policy in the European Union. Lancet 381(9872), 1135–1144 (2013).
• Illustrates how health law and policy effects go beyond normal activities and affect almost every aspect of health and healthcare.
8.
Dixon A, Poteliakhoff E. Back to the future: 10 years of European health reforms. Health Econ. Policy Law 7(1), 1–10 (2012).
• Analyze health reforms in EU states that cross-borders will be shaped by the social and political institutions of a country, and also propose that policymakers should look at their neighbors in order to develop appropriate policy solutions.
9.
Walshe K, McKee M, McCarthy M et al. Health systems and policy research in Europe: Horizon 2020. Lancet 382(9893), 668–669 (2013).
10.
Wismar M, Busse R. Outcome-related health targets – political strategies for better health outcomes: a conceptual and comparative study (part 2). Health Policy 59(3), 223–241 (2002).
11.
Wismar M, Figueras J, Ernst K, Van Ginneken E. Cross-Border Health Care in the European Union: Mapping and Analysing Practices and Policies. European Observatory on Health Systems and Policies, UK (2011).
• Summary of the cross-border healthcare policy in Europe.
12.
Greer SL. Avoiding another directive: the unstable politics of European Union cross-border health care law. Health Econ. Policy Law 8(4), 415–421 (2013).
• Analyze the challenges relating to cross-border healthcare law and identifying the reimbursement problems.
13.
Vasev N, Vrangbæk K. Transposition and national-level resources: introducing the Cross-Border Healthcare Directive in Eastern Europe. West Eur. Politics 37(4), 693–710 (2014).
14.
Jacobs R, Smith PC, Street A. Measuring Efficiency in Health Care: Analytic Techniques and Health Policy. Cambridge University Press, Cambridge, UK (2006).
15.
Farrell MJ. The measurement of productive efficiency. J. R. Stat. Soc. 120, 253–290 (1957).
16.
NIH U.S. National Library of Medicine. Efficiency, Organizational MeSH descriptor data 2018. https://meshb.nlm.nih.gov/record/ui?ui=D017598
17.
Vincová K. Using DEA models to measure efficiency. Biatec 13(8), 24–28 (2005).
18.
Buleca J, Mura L. Quantification of the efficiency of public administration by data envelopment analysis. Procedia Economics Finance 15, 162–168 (2014).
19.
Begg I, Henry SGB. Applied Economics and Public Policy. Cambridge University Press, Cambridge, UK (1998).
20.
Zavras AI, Tsakos G, Economou C, Kyriopoulos J. Using DEA to evaluate efficiency and formulate policy within a Greek National Primary Health Care Network. J. Med. Syst. 26(4), 285–292 (2002).
• Presents how DEA was used to analyze and formulate policies within the Greek healthcare system.
21.
Varabyova Y, Müller J-M. The efficiency of health care production in OECD countries: a systematic review and meta-analysis of cross-country comparisons. Health Policy 120(3), 252–263 (2016).
• Presents how was used to analyze and formulate policies within the Greek healthcare system.
22.
Guerra M, De Souza AA, Moreira DR. Performance analysis: a study using data envelopment analysis in 26 Brazilian hospitals. J. Health Care Finance 38(4), 19–35 (2012).
• Understanding data envelopment analysis (DEA) in health context.
23.
Giancotti M, Guglielmo A, Mauro M. Efficiency and optimal size of hospitals: results of a systematic search. PLoS ONE 12(3), e0174533 (2017).
• Understanding DEA in health context.
24.
Narimatsu H, Nakata Y, Nakamura S et al. Applying data envelopment analysis to preventive medicine: a novel method for constructing a personalized risk model of obesity. PLoS ONE 10(5), e0126443 (2015).
• Understanding DEA in health context.
25.
Flokou A, Aletras V, Niakas D. A window-DEA based efficiency evaluation of the public hospital sector in Greece during the 5-year economic crisis. PLoS ONE 12(5), e0177946 (2017).
• Understanding DEA in health context.
26.
Pelone F, Kringos DS, Romaniello A, Archibugi M, Salsiri C, Ricciardi W. Primary care efficiency measurement using data envelopment analysis: a systematic review. J. Med. Syst. 39(1), 156 (2015).
• Understanding DEA in health context.
27.
Cordero Ferrera JM, Crespo Cebada E, Murillo Zamorano LR. The effect of quality and socio-demographic variables on efficiency measures in primary health care. Eur. J. Health Econ. 15(3), 289–302 (2014).
• Understanding DEA in health context.
28.
Pelone F, Kringos DS, Valerio L et al. The measurement of relative efficiency of general practice and the implications for policy makers. Health Policy 107(2), 258–268 (2012).
• Understanding DEA in health context.
29.
Färe R, Margaritis D, Rouse P, Roshdi I. Estimating the hyperbolic distance function: a directional distance function approach. Eur. J. Oper. Res. 254(1), 312–319 (2016).
30.
Charnes A, Cooper WW, Rhodes E. Measuring the efficiency of decision making units. Eur. J. Oper. Res. 2(6), 429–444 (1978).
31.
Johnson AL, McGinnis LF. The hyperbolic-oriented efficiency measure as a remedy to infeasibility of super efficiency models. J. Oper. Res. Soc. 60(11), 1511–1517 (2009).
32.
European Commission. Special Eurobarometer 411: patient safety and quality of care. (2014). https://data.europa.eu/euodp/data/dataset/S1100_80_2_411
33.
European Commission. Special Eurobarometer 425 patients' rights in cross-border healthcare in the European Union Report (2015). http://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_425_sum_en.pdf
34.
World Development Indicators, Health Expenditure. http://databank.worldbank.org/data/reports.aspx?source=world-development-indicators
35.
Legido-Quigley H, Glinos I, Baeten R, McKee M. Patient mobility in the European Union. BMJ 334(7586), 188 (2007).
36.
Muscat N, Grech K, Cachia JM, Xureb D. Sharing capacities – Malta and the United Kingdom. In: Patient Mobility in the European Union: Learning from Experience. Rosenmoller M, McKee M, Baeten R (Eds). The Cromwell Press, Trowbridge, UK, 119 (2006).
37.
European Comission, Consul JO. Member State Data on cross-border healthcare following Directive 2011/24/EU (2015). https://ec.europa.eu/health/sites/health/files/cross_border_care/docs/2015_msdata_en.pdf
38.
Smith J, Buse K, Gordon C. Civil society: the catalyst for ensuring health in the age of sustainable development. Global. Health 12(1), 40 (2016).
39.
Bobek J, Schmidt AE, Röhrling I et al. Study on Cross-Border Cooperation capitalising on existing initiatives for cooperation in cross-border regions. Cross-border.Care. (2018). https://ec.europa.eu/health/sites/health/files/cross_border_care/docs/2018_crossbordercooperation_frep_en.pdf
Information & Authors
Information
Published In
Pages: 827 - 834
PubMed: 29770704
Copyright
© 2018 Future Medicine Ltd.
History
Received: 2 April 2018
Accepted: 8 May 2018
Published online: 17 May 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Estimating efficiency of Directive 2011/24/EU cross-border healthcare in member states. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0027
Export citation
Select the citation format you wish to export for this article or chapter.