M-bioscore: proposing a new statistical model for prognostic factors in metastatic breast cancer patients
Abstract
Aim: The current study aims to propose and internally validate ‘M-bioscore’, which is a model to help predict the outcomes of untreated metastatic breast cancer patients. Methodology: Surveillance, epidemiology and end results (SEER) database (2010–2013) was accessed. Patients were divided into two groups: a training set and a validation set. Through a Cox proportional model, multivariate analysis for potential prognostic factors was performed. M-bioscore was calculated for all patients. Survival analyses were conducted through Kaplan–Meier analysis/log-rank testing. Results: A total of 6655 metastatic breast cancer patients were analyzed. In the training set, the following factors were linked to better cancer-specific survival in multivariate analysis: estrogen receptor positivity, isolated distant nodal metastases, progesterone receptor positivity, lower nuclear grade and HER2 neu positivity (p < 0.01). Cancer-specific survival was then assessed according to M-bioscore. Adjusted Cox regression cause-specific hazard (using breast cancer death as the event of interest) was evaluated in the validation cohort. Pairwise hazard ratio comparisons between different scores were significant (p < 0.05) except for the comparison between score 6 and 7. C-index for the validation cohort was 0.665 (Standard error (SE): 0.010; 95% CI: 0.646- 0.685).Conclusion: M-bioscore can predict the outcomes of untreated metastatic breast cancer patients. Validation of external datasets is needed.
As the second most common cancer and the most common cancer among females, breast cancer represents a global health issue. More than one and half million patients were estimated to be affected with breast cancer in 2012 [1].
Approaches for the management of advanced breast cancer were based on a number of factors, which include tumor-related factors (biology, extent/distribution of metastases) and patient-related factors (performance and co-morbidity) [2]. Notably, the Tumor/Node/Metastasis (TNM) system (which is the commonly used staging system for breast cancer) deals with M1 breast cancer as one group [3]. The different editions of this staging system did not provide any further subclassification of M1 disease according to extent of metastatic disease in spite of clear evidence of differences in survival among patients with M1 disease based on the distribution of metastatic disease [4]. Moreover, until the most recent edition (8th Ed.), there was no incorporation of biological markers into the stage groups despite progress in our understanding of breast cancer biology and its impact on outcomes [5]. Thus, development of a reliable prognostic index that incorporates anatomy and biology, and that can be applied easily in different settings is an unmet need.
A new staging paradigm for patients with breast cancer who are nonmetastatic and treated with upfront surgery was proposed in 2011 [6]. It included estrogen receptor (ER) and grade. It was then updated recently to incorporate ER, HER2neu and nuclear grade in addition to pathological stage [7,8]. In the meantime, a similar model ‘Neo-bioscore’ was proposed and validated in order to predict the outcomes of neoadjuvantly treated patients [9,10]. Till now, no comparable model has been proposed or validated for metastatic disease. In the current study, a model for patients with metastatic breast cancer ‘M-bioscore’ is proposed for the first time and validated from a surveillance, epidemiology and end results (SEER) database cohort of patients. The candidate factors evaluated for inclusion into this model are similar to those evaluated in the previous models for nonmetastatic disease including anatomy-related factors (i.e., site and extent of metastases) and biology-related factors (i.e., ER, progesterone receptor [PR], HER2neu and nuclear grade).
Patients & methods
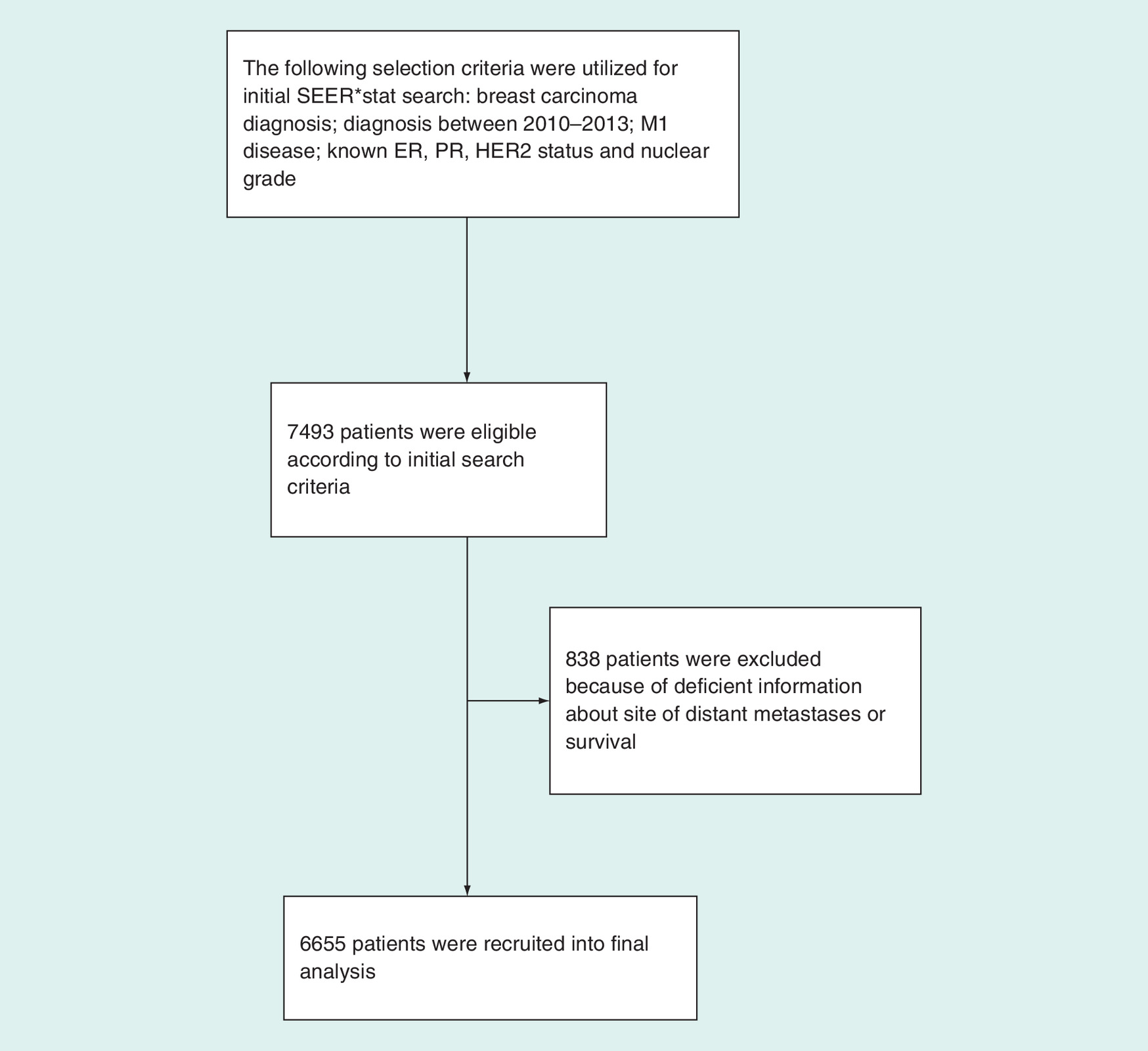
SEER*Stat software (Version 8.3.4) was used for accessing the SEER database [11]. The search was from 2010 to 2013 (because HER2 status and details of bone, brain, liver or lung metastases were not available for cases diagnosed before 2010). To identify suitable patients, the ICD-O-3/WHO 2008 category of ‘breast’ was selected and patients with M1 disease were chosen. Inadequate information about site of distant metastases, ER, nuclear grade, PR, survival or HER2 neu led to exclusion of some cases and this is detailed in Figure 1.
Data collection
Information of interest that was collected included: sites of distant metastases (including bone, brain, liver, lung, distant nodal deposits or skin metastases qualifying as M1), breast cancer subtype, HER2 neu, ER, PR, nuclear grade and histological subtype.
Baseline demographics like age at diagnosis, race and gender were also collected. Surgical treatment of the primary tumor, radiotherapy, survival status, cause of death and survival duration was also collected.
Statistical considerations
The study cohort was separated into two groups (through an SPSS-verified randomization procedure): training set (half of the cohort) for building the model and an internal validation set (the other half of the cohort) for validating the model. Cox proportional model was performed to conduct multivariate analyses of variables affecting cancer-specific survival. Building on the results of the multivariate analysis, the M-bioscore points were allocated. The lowest category of each risk factor was assigned a score of 0. A score was then produced for each case by summing the scores from each risk factor. It has to be noted that these scores are ordinal and not continuous scale. Thus, the resulting score should be handled as a categorical variable. Kaplan–Meier analysis/log-rank testing was then used for survival analyses according to M-bioscore. An ad-hoc Bonferroni adjustment of p-value was disregarded because, with a huge number of pairwise comparisons (28 pairwise comparisons), there was a risk of aggravating a type II error through this adjustment. An additional cumulative incidence function was conducted according to the M-bioscore in the validation set. Cox cause-specific hazard ratio with pairwise hazard ratio comparisons was also assessed in the validation cohort.
Cancer-specific survival was defined in the current analysis as time from diagnosis till death from breast cancer. Concordance index was then utilized to assess the predictor ability of the model [12]. SPSS Statistics 20.0 and Stata statistics 14.0 were employed for statistical comparisons. A two-tailed p-value < 0.05 was necessary to declare statistical significance.
Results
Patients, characteristics
6655 untreated metastatic breast cancer patients were identified from 2010 to 2013, and were included. Baseline characteristics of included patients including histology, age, race and distribution of sites of distant metastases were reported in Table 1. A single site of metastases was reported in 63.3%; while multiple sites of metastases were reported in 36.7%. Positive ER status in 75.6% of cases, positive PR status in 61.7% and positive HER2 neu status in 24.9% were reported. Breast cancer subtype distribution was also detailed in Table 1. Nuclear grade was: grade 1 in 11%, grade 2 in 44.1% and grade 3 in 44.9%. Breast surgery was conducted in 32.6% of cases and radiotherapy was received in 33.9%. Technical details about radiotherapy dose or technique were not available. Data about systemic therapy were not available. 3327 patients were randomly allocated to the training set and 3328 patients were randomly allocated to the validation set. Median follow-up time was 13 months and it ranged from 1 to 47 months and 10% of patients were followed for >3 years (36 months).
| Parameters | All patients (n = 6655) | Training cohort (n = 3327) | Validation cohort (n = 3328) |
|---|---|---|---|
| Age <40 years 40–69 years >69 years | 485 (7.3%) 4428 (66.5%) 1742 (26.2%) | 232 (7%) 2217 (66.6%) 878 (26.4%) | 253 (7.6%) 2211 (66.4%) 864 (26%) |
| Race White Black Others Unknown | 5093 (76.5%) 1040 (15.6%) 499 (7.5%) 23 (0.4%) | 2538 (76.3%) 526 (15.8%) 250 (7.5%) 13 (0.4%) | 2555 (76.8%) 514 (15.4%) 249 (7.5%) 10 (0.3%) |
| Gender Female Male | 6584 (98.9%) 71 (1.1%) | 3287 (98.8%) 40 (1.2%) | 3297 (99.1%) 31 (0.9%) |
| Histology IDC, NOS Lobular carcinoma, NOS Other variants | 5093 (76.5%) 654 (9.8%) 908 (13.7%) | 2546 (76.5%) 339 (10.2%) 442 (13.3%) | 2547 (76.5%) 315 (9.5%) 446 (14%) |
| Estrogen receptor Positive Negative | 5028 (75.6%) 1627 (24.4%) | 2522 (75.8%) 805 (24.2%) | 2506 (75.3%) 822 (24.7%) |
| HER2neu Positive Negative | 1655 (24.9%) 5000 (75.1%) | 805 (24.2%) 2522 (75.8%) | 850 (25.5%) 2478 (74.5%) |
| Breast subtype HR+/Her2- HR+/Her2+ HR-/Her2+ Triple negative | 4049 (60.8%) 1082 (16.3%) 573 (8.6%) 951 (14.3%) | 2035 (61.2%) 536 (16.1%) 269 (8.1%) 487 (14.6%) | 2014 (60.5%) 546 (16.4%) 304 (9.1%) 464 (13.9%) |
| Nuclear grade 1 2 3 | 735 (11%) 2934 (44.1%) 2986 (44.9%) | 372 (11.2%) 1472 (44.2%) 1483 (44.6%) | 363 (10.9%) 1462 (43.9%) 1503 (45.2%) |
| Distribution of metastases Isolated bone Isolated distant lymph nodes Isolated skin Isolated lung Isolated liver Isolated brain Multiple sites | 2431 (36.5%) 533 (8%) 36 (0.5%) 672 (10.1%) 475 (7.1%) 68 (1%) 2440 (36.7%) | 1240 (37.3%) 277 (8.3%) 16 (0.5%) 363 (10.9%) 213 (6.4%) 30 (0.9%) 1181 (35.7%) | 1191 (35.8%) 256 (7.7%) 20 (0.6%) 309 (9.3%) 262 (7.9%) 38 (1.1%) 1252 (37.6%) |
| Breast surgery None Yes Unknown | 4464 (67.1%) 2167 (32.6%) 24 (0.4%) | 2238 (67.3%) 1077 (32.4%) 12 (0.4%) | 2226 (66.9%) 1090 (32.8%) 12 (0.4%) |
| Radiotherapy Yes No Unknown | 2258 (33.9%) 4187 (62.9%) 210 (3.2%) | 1118 (33.6%) 2115 (63.6%) 94 (2.8%) | 1140 (34.3%) 2072 (62.3%) 116 (3.5%) |
| Events Cancer-specific deaths Overall deaths | 1835 2478 | 910 1220 | 925 1258 |
IDC: Infiltrating duct carcinoma; NOS: Not otherwise specified.
Survival outcomes of the training cohort
Multivariate analysis of variables potentially affecting cancer-specific survival was performed among the training cohort (evaluating the following: site/distribution of metastasis, ER, PR, HER2neu and nuclear grade). The following variables were linked to better cancer-specific survival (ER positivity, isolated distant nodal metastases, PR positivity, lower nuclear grade and HER 2 neu positivity) (p < 0.01) (Table 2).
| Parameter | Training set | |
|---|---|---|
| HR (95% CI) | p-value | |
| Site of metastases | ||
| Isolated bone | Reference | |
| Isolated distant LN | 0.602 (0.442–0.819) | 0.001 |
| Isolated skin | 0.165 (0.023–1.180) | 0.073 |
| Isolated liver | 1.119 (0.835–1.499) | 0.453 |
| Isolated lung | 1.063 (0.838–1.349) | 0.613 |
| Isolated brain | 1.937 (1.056–3.552) | 0.033 |
| Multiple sites | 1.798 (1.538–2.101) | < 0.0001 |
| Estrogen receptor | ||
| Positive | Reference | |
| Negative | 1.529 (1.262–1.850) | < 0.0001 |
| Progesterone receptor | ||
| Positive | Reference | |
| Negative | 1.631 (1.363–1.951) | < 0.0001 |
| Her2 neu | ||
| Positive | Reference | |
| Negative | 1.683 (1.427–1.985) | < 0.0001 |
| Nuclear grade | ||
| III | Reference | |
| I | 0.694 (0.544–0.886) | 0.003 |
| II | 0.789 (0.680–0.916) | 0.002 |
HR: Hazard ratio; LN: Lymph node.
Building on the results of the multivariate analysis, the M-bioscore was formulated (Table 3). An M-bioscore point is given for each of negative ER, negative PR, negative HER2 neu and nuclear grade >2. The metastatic site is given the following points: 0 for distant lymph nodes (isolated) (because it has a statistically significant lower HR compared with bone), 1 for bone/skin deposits (isolated), 2 for liver/lung deposits (isolated), 3 for brain deposits (isolated) or multiple sites of metastases. An M-bioscore was constructed for each case (may range from 0 to 7).
| Factor | M-bioscore points assigned |
|---|---|
| Site of distant metastasis Isolated distant LN Isolated bone/skin Isolated liver/lung Isolated brain/multiple sites | 0 1 2 3 |
| Estrogen receptor Positive Negative | 0 1 |
| Progesterone receptor Positive Negative | 0 1 |
| Her2 neu Positive Negative | 0 1 |
| Nuclear grade 1 2 3 | 0 0 1 |
LN: Lymph node.
Distribution of patients according to the overall score of each case of the training cohort was described in Table 4. The 4-year cancer-specific survival rate for each score was also described in Table 4. The 4-year cancer-specific survival rate was determined through the life tables’ function of the SPSS.
| Score | All cases | Training set (3327 patients) | Validation set (3328 patients) | |||
|---|---|---|---|---|---|---|
| n (%) | 4-year CSS rates | n (%) | 4-year CSS rates | n (%) | 4-year CSS rates | |
| 0 | 22 (0.3%) | 95% | 10 (0.3%) | 100% | 12 (0.4%) | 91% |
| 1 | 273 (4.1%) | 81% | 139 (4.3%) | 68% | 134 (4%) | 82% |
| 2 | 1567 (23.5%) | 69% | 816 (24.5%) | 59% | 751 (22.6%) | 70% |
| 3 | 1202 (18.1%) | 60% | 599 (18%) | 54% | 603 (18.1%) | 56% |
| 4 | 1680 (25.2%) | 52% | 829 (24.9%) | 47% | 851 (25.6%) | 45% |
| 5 | 1038 (15.6%) | 35% | 503 (15.1%) | 29% | 535 (16.1%) | 29% |
| 6 | 590 (8.9%) | 26% | 290 (8.7%) | 22% | 300 (9%) | 20% |
| 7 | 283 (4.3%) | 17% | 141 (4.2%) | 16% | 142 (4.3%) | 19% |
CSS: Cancer-specific survival.
Survival outcomes of the validation cohort
Table 4 shows the distribution and 4-year cancer-specific survival among the three cohorts according to M-bioscore. Table 5 shows median overall and cancer-specific survival for the overall cohort according to M-bioscore.
| Score | Overall survival (months) | Cancer-specific survival (months) |
|---|---|---|
| 0 | Not reachable | Not reachable |
| 1 | Not reachable | Not reachable |
| 2 | Not reachable | Not reachable |
| 3 | 39 | Not reachable |
| 4 | 33 | 43 |
| 5 | 22 | 28 |
| 6 | 13 | 15 |
| 7 | 9 | 12 |
Cox regression cause-specific hazard (using breast cancer death as the event of interest) adjusted for age, race, surgery and radiation therapy was evaluated in the validation cohort (Figure 2A). Pairwise hazard ratio comparisons between different scores were significant (p < 0.05) with the exception of the comparison between score 6 and 7. Subdistribution hazard ratio (using the primary failure end point of breast cancer death and using other causes of death as competing causes of death) adjusted for age, race, surgery and radiotherapy in the validation set for the M-bioscore was: 1.449 (95% CI: 1.389–1.511; p < 0.0001) indicating increasing risk of death from breast cancer with increasing score. The cumulative incidence function (according to different scores) was also displayed in Figure 2B.

Figure 2. Survival outcomes for the validation set.
(A) Adjusted cancer-specific hazard according to M-bioscore among validation set. (B) Cumulative incidence function according to the M-bioscore among validation set.
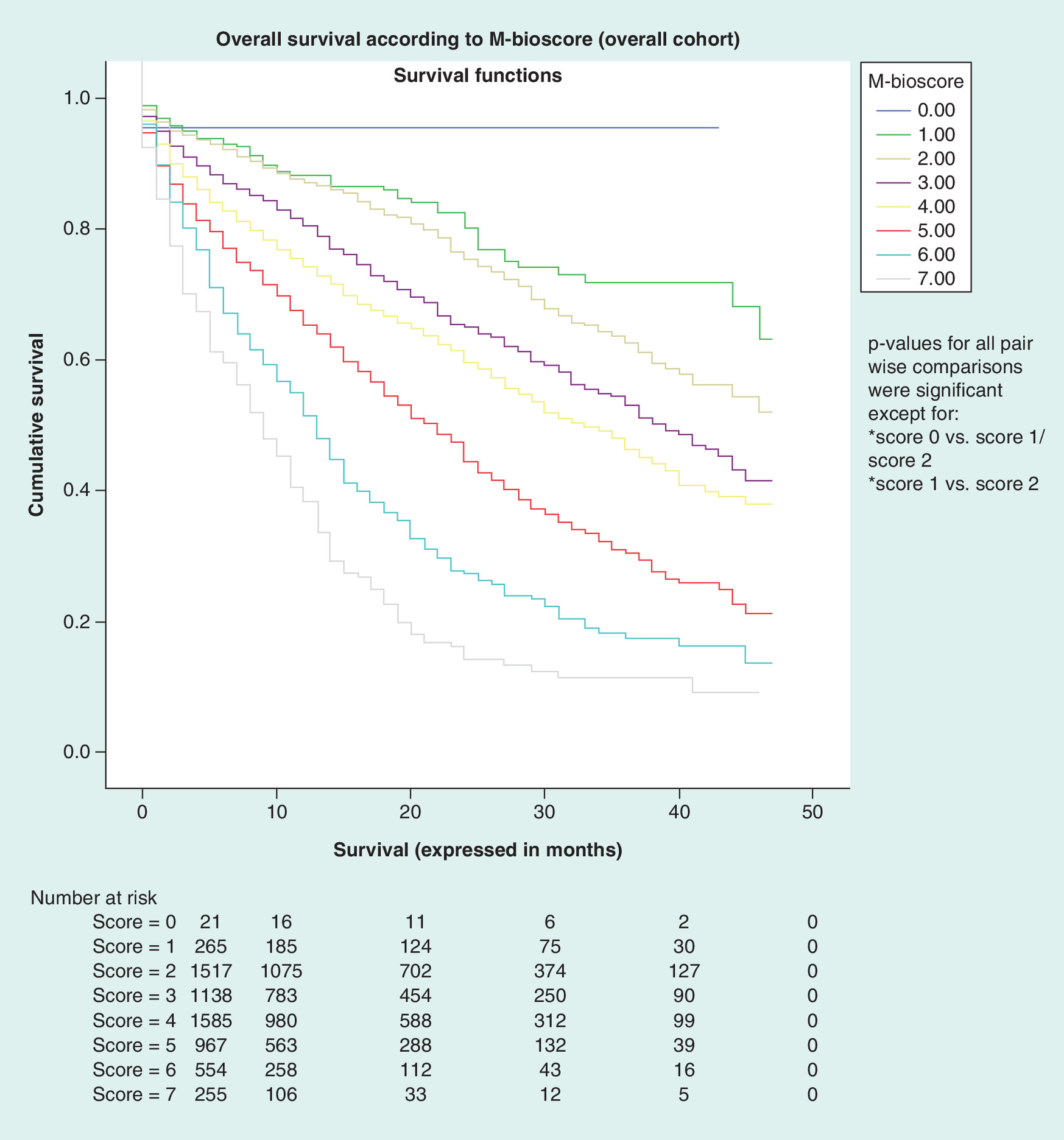
Overall survival was assessed according to M-bioscore model in the overall cohort, and p-values for comparisons among different score points were significant (p < 0.05) with the exception of the comparisons between score 0 and score 1/score 2 and the comparison between scores 1 and 2 (Figure 3).
Concordance index was also assessed using death from breast cancer as the dependent variable; and the finding for the validation cohort was 0.665 (SE: 0.010; 95% CI: 0.646– 0.685).
Discussion
The current study proposes an M-bioscore for previously untreated metastatic breast cancer and internally validates its performance in a group of patients registered within the SEER database. The current analysis supports the discriminating utility of the M-bioscore model and suggests it may be included in patient counseling and decision-making models for metastatic breast cancer.
Potential setbacks in this analysis may include: data about Charlson co-morbidity index or performance status are not available; therapeutic data (particularly systemic therapy) are insufficient in the SEER database; data about other potential prognostic molecular markers are not available (e.g., gene expression profiling [GEP]); the follow-up period is relatively short (2010–2013); and this may have obscured some long-term differences between different score categories; M-bioscore is formulated based on a cohort of US patients. Therefore, before it can be globally adopted, its prognostic performance should be externally validated within other ethnicities and treatment settings. Additionally, it is not exactly known if the biopsy for biological markers was taken from the primary tumor or metastatic disease in each patient.
Given the simplicity and accessibility of the markers used in the current prognostic scoring system (ER, PR, grade, Her2 and site of metastases) and given the fact that these markers are part of the routine workup of every newly diagnosed metastatic breast cancer patient, M-bioscore seems an easily affordable model for patients with breast cancer. It has, however, to be noted that M-bioscore should be handled in practice as a categorical variable.
Together with the baseline clinicopathological factors discussed in the current study, proper selection of treatments as well as proper sequencing of therapeutic strategies was shown to impact the outcomes of metastatic breast cancer patients [13]. This illustrates the important role played by expert and multidisciplinary oncological evaluation of each case of metastatic breast cancer.
Age, breast surgery and radiation therapy were not entered into the multivariate analysis and subsequently the model. The rationale behind this was that younger patients, who were referred to surgery or radiation therapy, are more likely to have a good performance and receive more aggressive therapy. In the context of absence of performance status and co-morbidity data from the SEER database, this might have created a bias in the model (i.e., younger patients would have better outcomes not because of an indolent disease but rather because of more aggressive treatment). Thus, these factors were not elaborated in the model. Besides, factors like age and treatment were not included in the previously proposed bioscore and Neo-bioscore models for early stage breast cancer. Thus, it was deemed appropriate to keep the structure of the M-bioscore model similar to previously published bioscore models in other treatment settings.
Despite the comparably impressive 4-year cancer-specific survival rate for patients with score 0 (95%), p-values for pairwise hazard ratio comparisons were insignificant for some comparisons. This may be interpreted by the small number of patients in some validation cohort subgroups, which may have precluded statistical significance in these comparisons.
The prognostic impact of the metastatic site and metastatic pattern in breast cancer was recognized and reported by some population-based studies [14]. What is new in the current analysis is the integration of these findings together with other relevant and easily accessible biomarkers to form a comprehensive prognostic model for this subset of patients.
Although positive HER2 status was considered a marker of more aggressive disease in adjuvant and metastatic settings [15], data from MD-Anderson group [7] as well as the current analysis indicate better outlook for patients with HER2-positive disease. One important context for this finding is that the majority of HER2-positive patients in both analyses were mostly offered and received anti-HER2 therapy.
The current analysis indicates that in the metastatic setting, the hormone receptor positive, HER2-positive phenotype is the most favorable phenotype. This goes in line with previous population-based data which were also notably published in the era of anti-HER2 therapy [16]. However, given that the impact of choice of systemic treatment on clinical outcome remains unclear, the above conclusion should be taken cautiously.
The eighth American Joint Committee on Cancer (AJCC) breast cancer stage groups presented – for the first time – a dual staging approach, including prognostic stage groups and anatomical stage groups [7]. The prognostic stage groups included some biomarkers (like ER, nuclear grade, PR, Oncotype DX recurrence score and HER2 neu). However, in the AJCC 8th Ed., these prognostic groups were not extended to patients with M1 disease. The current analysis offered an integrated M-bioscore incorporating both anatomy and biology for M1 patients and it may guide future revisions to the AJCC stage groups.
Multiple studies suggested that utilization of GEP tests improves the predictability of anatomical staging for nonmetastatic ER-positive/HER2-negative disease [17,18]. Similarly, it has been suggested that these tests may play a role in metastatic disease [19]. It remains to be seen if there is an added predictive value for combining GEP to the M-bioscore model.
Conclusion
M-bioscore can predict the outcomes of untreated metastatic breast cancer patients. Validation through the use of external datasets is needed.
The current study aims to propose and internally validate ‘M-bioscore’, which is a model to help predict the outcomes of untreated metastatic breast cancer patients.
Surveillance, epidemiology and end results (SEER) database (2010–2013) was accessed. Patients were divided into two groups: a training set and a validation set.
Through a Cox proportional model, multivariate analysis for potential prognostic factors was performed. M-bioscore was calculated for all patients. Survival analyses were conducted through Kaplan–Meier analysis/log-rank testing.
A total of 6655 metastatic breast cancer patients were analyzed. In the training set, the following factors were linked to better cancer-specific survival in multivariate analysis: ER positivity, isolated distant nodal metastases, PR positivity, lower nuclear grade and HER 2 neu positivity (p < 0.01).
Cancer-specific survival was then assessed according to M-bioscore. Adjusted Cox regression cause-specific hazard (using breast cancer death as the event of interest) was evaluated in the validation cohort. Pairwise hazard ratio comparisons between different scores were significant (p < 0.05) except for the comparison between scores 6 and 7.
Concordance index for the validation cohort was 0.665 (SE: 0.010; 95% CI: 0.646–0.685).
Financial & competing interests disclosure
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
As this study is based on a publicly available database without identifying patient information, informed consent was not needed.
References
Papers of special note have been highlighted as: • of interest
1.
The GLOBOCAN project. www.globocan.iarc.fr.
2.
Jackisch C, Lammers P, Jacobs I. Evolving landscape of human epidermal growth factor receptor 2-positive breast cancer treatment and the future of biosimilars. Breast 32, 199–216 (2017).
3.
Amin MB, Greene FL, Edge SB et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more ‘personalized’ approach to cancer staging. CA Cancer J. Clin. 67(2), 93–99 (2017).
4.
Nguyen DH, Truong PT, Walter CV, Hayashi E, Christie JL, Alexander C. Limited m1 disease: a significant prognostic factor for stage IV breast cancer. Ann. Surg. Oncol. 19(9), 3028–3034 (2012).
5.
Abdel-Rahman O. Validation of the 8th AJCC prognostic staging system for breast cancer in a population-based setting. Breast Cancer Res. Treat. (2017) (Epub ahead of print).
6.
Yi M, Mittendorf EA, Cormier JN et al. Novel staging system for predicting disease-specific survival in patients with breast cancer treated with surgery as the first intervention: time to modify the current American Joint Committee on Cancer staging system. J. Clin. Oncol. 29(35), 4654–4661 (2011).
7.
Giuliano AE, Connolly JL, Edge SB et al. Breast cancer – major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 67(4), 290–303 (2017).
• Reviews major changes in the American Joint Committee on Cancer system for breast cancer.
8.
Abdel-Rahman O. Assessment of the prognostic and discriminating value of the novel bioscore system for breast cancer; a SEER database analysis. Breast Cancer Res. Treat. (2017) (Epub ahead of print).
9.
Mittendorf EA, Vila J, Tucker SL et al. The neo-bioscore update for staging breast cancer treated with neoadjuvant chemotherapy: incorporation of prognostic biologic factors into staging after treatment. JAMA Oncol. 2(7), 929–936 (2016).
10.
Vila J, Teshome M, Tucker SL et al. Combining clinical and pathologic staging variables has prognostic value in predicting local-regional recurrence following neoadjuvant chemotherapy for breast cancer. Ann. Surg. 265(3), 574–580 (2017).
11.
Surveillance, Epidemiology and End Results program. About the SEER program. http://seer.cancer.gov/about.
12.
Metz CE. Basic principles of ROC analysis. Semin. Nucl. Med. 8(4), 283–298 (1978).
13.
Mestres JA, Imolins AB, Martínez LC et al. Defining the optimal sequence for the systemic treatment of metastatic breast cancer. Clin. Transl. Oncol. 19(2), 149–161 (2017).
14.
Miao H, Hartman M, Bhoo-Pathy N et al. Predicting survival of de novo metastatic breast cancer in Asian women: systematic review and validation study. PLoS One 9(4), e93755 (2014).
15.
Figueroa-Magalhaes MC, Jelovac D, Connolly RM, Wolff AC. Treatment of HER2-positive breast cancer. Breast 23(2), 128–136 (2014).
16.
Yardley DA, Tripathy D, Brufsky AM et al. Long-term survivor characteristics in HER2-positive metastatic breast cancer from registHER. Br. J. Cancer 110(11), 2756–2764 (2014).
17.
Sorlie T, Perou CM, Tibshirani R et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl Acad. Sci. USA 98(19), 10869–10874 (2001).
18.
Gluz O, Nitz UA, Christgen M et al. West German study group Phase III planB trial: first prospective outcome data for the 21-gene recurrence score assay and concordance of prognostic markers by central and local pathology assessment. J. Clin. Oncol. 3 4(20), 2341–2349 (2016).
19.
Mostert B, Sieuwerts AM, Kraan J et al. Gene expression profiles in circulating tumor cells to predict prognosis in metastatic breast cancer patients. Ann. Oncol. 26(3), 510–516 (2015).
Information & Authors
Information
Published In
Copyright
© 2018 Future Medicine Ltd.
History
Received: 11 January 2018
Accepted: 15 May 2018
Published online: 7 September 2018
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
M-bioscore: proposing a new statistical model for prognostic factors in metastatic breast cancer patients. (2018) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2018-0006
Export citation
Select the citation format you wish to export for this article or chapter.