Quality-adjusted life year difference in patients with predominant negative symptoms of schizophrenia treated with cariprazine and risperidone
Abstract
Aim: Our study aimed at estimating differences in quality-adjusted life year (QALY) gain for patients with predominant negative symptoms of schizophrenia treated with cariprazine compared with risperidone. Materials & methods: A Markov model was built, based on the Mohr–Lenert approach and data derived from clinical trials, to estimate potential QALY gains of patients. Results: Patients had higher probability of reaching better health states treated with cariprazine compared with risperidone. In the model, this resulted in an estimated QALY gain of 0.029 per patient, after 1 year of treatment. Conclusion: Cariprazine, which showed clinically meaningful improvement in the symptoms, and personal and social performance, can also provide significant QALY gain in the treatment of patients with predominant negative symptoms of schizophrenia compared with risperidone.
First draft submitted: 5 April 2017; Accepted for publication: 3 May 2017; Published online: 17 May 2017
Schizophrenia is a chronic mental disorder that affects more than 21 million people worldwide [1]. It is characterized by hallucinations, abnormal social behavior and other cognitive difficulties. Patients with schizophrenia may have difficulties making distinction between reality and delusions; may be unresponsive and have difficulty expressing emotions properly in social situations [1]. The health, social and economic burden of schizophrenia is tremendous, not only for patients but also for families, caregivers and the wider society. Recent estimations for annual costs for the schizophrenia population in the USA alone varied between US$25 billion [2] and US$156 billion [3].
Schizophrenia is characterized by a diverse set of symptoms based on the presence of positive or negative symptoms of the disease [4]. Positive symptoms can include delusions, hallucinations and other phenomena that individuals did not experience before the onset of the condition. Negative symptoms, such as lack of motivation, lack of need for human relationships and absence or deficit of normal emotional responses, reflect that the condition removes aspects of life that the patient previously experienced [5]. In the case of negative symptoms, patients’ response to medications is usually limited compared with positive symptoms [6].
Cariprazine is an orally active and potent dopamine D2 (DRD2) and D3 receptor (DRD3) partial agonist with preferential binding to DRD3, which has demonstrated efficacy in treating various symptoms of schizophrenia in short- and long-term treatment trials. Cariprazine is approved in the USA for the treatment of schizophrenia and manic or mixed episodes associated with bipolar I disorder in adults. In a clinical trial, cariprazine has been shown significant improvement both in the symptoms and social performance of patients with predominant negative symptoms (PNS) of schizophrenia compared with a representative of second-generation antipsychotics [7–9].
Cariprazine was tested against risperidone in a randomized, double-blind, active controlled, monotherapy treatment clinical trial (EudraCT 2012–005485–36) conducted by Gedeon Richter Plc. on a subpopulation of patients with schizophrenia showing PNS. The study was a two-arm superiority trial. Details of study design, inclusions and exclusions criteria were described in detail by Németh et al. [8]. The study had a sufficiently long treatment period (26 weeks) to judge and score patients’ symptoms severity after a cross-titration period of 2 weeks and randomized 231 patients into the risperidone and 230 patients into the cariprazine treatment arms. Change from baseline in the primary efficacy parameter, the positive and negative syndrome scale (PANSS) factor score for negative symptoms was statistically significant greater in the cariprazine group than in the risperidone group at week 26. Based on data derived from the clinical trial, patients also showed greater improvement in the personal and social performance total score as well as in three of the four personal and social performance subdomains with cariprazine compared with risperidone.
The purpose of the analysis reported in this paper was to estimate the gain in quality-adjusted life years (QALYs) that could be achieved over 54 weeks by the use of cariprazine in the treatment of schizophrenia for patients with PNS compared with the widely used second-generation antipsychotic drug, risperidone, based on the PANSS data from the Németh et al. clinical trial [8]. The approach has been taken to use trial results to identify how patients move from initial PANSS states to other states over time, dependent on whether they are being treated with risperidone or cariprazine and to use a previously developed algorithm for converting PANSS scores to utility estimates to allow the calculation of QALYs. This information is combined together in a Markov state transition model with states defined by PANSS scores to facilitate determining the added value of cariprazine.
Methods
Comparator
In accordance with the comparator treatment assessed in the Németh et al. clinical trial [8], the Markov state transition model compares cariprazine with risperidone.
Cycle length
Considering the pharmacokinetic properties of cariprazine [10–12], transition probabilities and clinical efficacy in the first 4–6 weeks of cariprazine treatment may not be fully representative for the consecutive time period. In accordance with this, the model was constructed with weekly cycles in the initial 6-week time period and 12-week long cycles for the latter periods, therefore the use of different transition probabilities was necessary for the first 6 weeks and for the subsequent model time period.
The model is able to run on different time horizons from 54 to 522 weeks (in concordance with the 12-week cycle length used in the model), that are approximately equivalent to 1–10 years. The results presented here are for 54 weeks.
Health states & quality of life data
PANSS is a 30-item scale to categorize patients with schizophrenia [13]. It has 7 positive symptom subscale items, 7 negative symptom subscale items and 16 general psychopathology items. The 7 items of positive symptom subscale are marked as P1–P7; the 7 negative symptom subscale items are marked as N1 to N7; and the remaining 16 items are referred to as G1 to G16. PANSS scores can also be divided into five factors based on Mohr et al. [14] (Table 1).
Mohr et al. defined eight health states for schizophrenia in 2004 [14] based on the positive factor score, negative factor score and cognitive factor score subscales of the PANSS scale. Lenert et al. [15] defined the thresholds of the three factor scores to determine health states. After reviewing the thresholds, Lenert and his co-authors issued a corrigendum [16] to the definitions of the original health states by Mohr et al. [14]. The final set of cut-off values to define the health states used in our analysis is included in Table 2. The eight Mohr–Lenert health states were the basis of the model structure with the addition of the health state ‘Death’ (Figure 1).
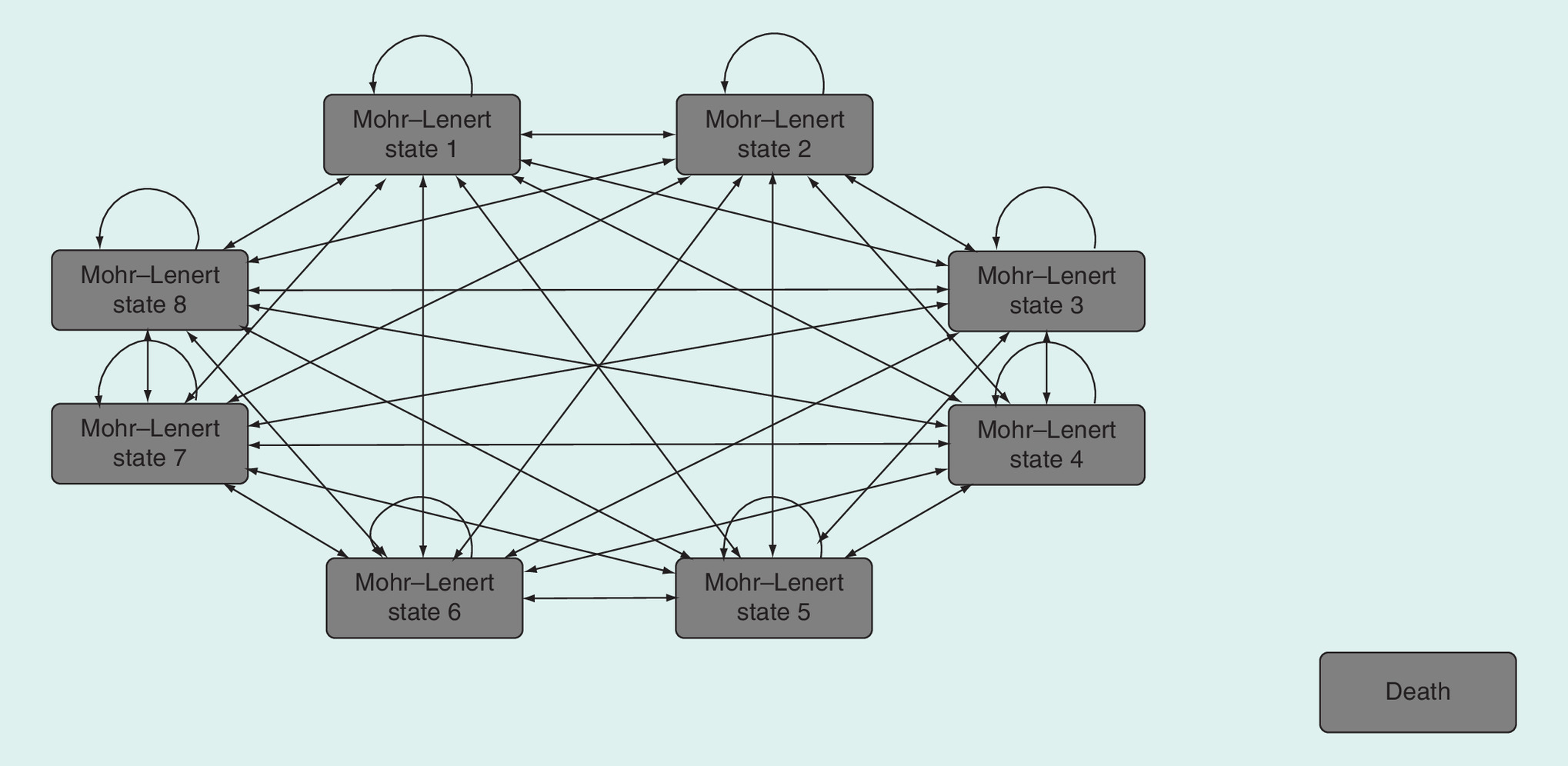
Figure 1. Structure of the cost–effectiveness model.
Patients can move from any health states to the ‘Death’ health state.
The authors calculated and assigned utility values to the previously defined eight Mohr–Lenert health states based on data gathered from an internet survey panel's standard gamble and visual analog scale ratings. The weighted means of the utility values associated with Mohr–Lenert health states range from 0.88 to 0.42 [15]. The utility value associated with the health state of ‘Death’ is zero.
Transition probabilities
The weekly transition probabilities (i.e., the numerical likelihoods of patients moving from one PANSS state to another) for both the cariprazine and the risperidone arm were acquired from the first 4 weeks of the Németh et al. clinical trial [8]. For the latter periods, transition probabilities were acquired from the cases where the time period between any two PANSS assessments was between 11 and 13 weeks (77–93 days). All the transition probability matrices are included in the Supplementary Appendix.
The transition probability matrices acquired from the clinical trial were not adequately populated for all possible transitions between health states, as the number of observations was considered to be too low in many cases. In order to complete the transition probability matrices, expert interviews were conducted with three experts from Hungary who had decades of experience in treating patients with schizophrenia. One of the experts is a leading psychiatrist in Hungary, one is from a university psychiatry clinic and one treats patients with schizophrenia at a day care service having many years of experience. Their estimates were not cross-checked with empirical data.
Experts were asked to give their opinion about the probabilities of patients with PNS of schizophrenia moving from a certain Mohr–Lenert health state to another when treated with a second-generation antipsychotic drug, like risperidone. Data from the expert interviews were gathered using the Prior Elicitation Graphical Software which is capable of modeling opinions about multinomial probabilities by a Dirichlet prior distribution, implementing methodology for assessing a subjective (personal opinion) distribution for the parameters of a multinomial model [18] using Bayesian mathematics.
During the Bayesian analysis, the influence of the prior probabilities on the posterior probabilities was kept minimal in order to ensure that the empirical data would determine mostly the estimated value of the transitional probability in case of transitions which occurred in the clinical trial. The same weights were assigned to the matrices obtained from the three expert interviews. The number of subjects moving from a state to the seven others or staying in the current one was set at the value of 1 in case of the priors. Consequently, when clinical trial data were available, the posterior was mainly influenced by the likelihood and not by the prior. The same priors were used for both the cariprazine and risperidone arms of the model.
Adverse events
The analysis of adverse events (AEs) in the Németh et al. clinical trial [8] were done based on the patients reported AEs at the visits. In the trial, the number of reported cases of all examined AEs was low on both arms (Table 3). Differences between the cariprazine and risperidone arms could be observed but none of those were statistically significant.
The AE incidence rates for the second-generation antipsychotics after switching were calculated from the AE rates of risperidone using the relative AE rates of second-generation antipsychotics published by Glick et al. [19]. The calculation was based on a conservative approach using the relative safety and tolerability profiles compared with risperidone.
Utility decrements were assigned to the AEs based on published analyses [15]. The mean disutilities associated with orthostatic hypotension, weight gain, tardive dyskinesia, pseudo-Parkinsonism and akathisia were 0.058, 0.031, 0.095, 0.074 and 0.059, respectively in a subtractive model.
Switching possibility analysis
Local experts strongly suggested that the model should include the possibility of switching between therapies, because in real life, patients with schizophrenia are not treated by the same antipsychotic drug for many years. This is in concordance with other published models of schizophrenia [20–22].
The model allows one-way switching from both treatment arms to second-generation antipsychotics. It is assumed that they have the same efficacy (transition probabilities between health states) as risperidone, but have different AE profiles.
Patients switch was analyzed in relation of two factors in the model. In the first case, switching is tied to AEs and is intended to model patients’ real-life therapy switching patterns driven by intolerability or safety problems. In the second case, it is linked to the health states and includes all other reasons of real-life therapy switch, such as switching due to lack of efficacy, personal decision, other reasons and AEs not captured by the model.
To capture the importance of switching due to lack of efficacy, higher switching probabilities are attributed to more severe health states (health states 7 and 8); that means that patients switch to another therapy when the current treatment becomes ineffective. Lieberman et al. [23] published discontinuation rates for risperidone. The health state related switching rates of risperidone were applied on the cariprazine arm as well. Combining switching due to patient’s decision, AEs other than extrapyramidal symptoms or clinically significant weight gain or sedation and switching due to other causes resulted in a base-case value of annual switching rate of 32%, thereby encompassing two of the four reasons listed in the Lieberman study. In the case of the two most severe Mohr–Lenert health states (7 and 8), the switching rate was estimated to be 54%, as a result of considering switching due to lack of efficacy, in addition to switching due to patient’s decision, AEs other than extrapyramidal symptoms or weight gain or sedation and other causes, thereby encompassing three out of the four reasons listed in the Lieberman study. The reason of intolerability from the Lieberman study was linked to the occurrence of AEs directly, as explained above. Internal checks were applied to assess the face validity of the switching rates.
Model settings
The analysis was conducted assuming that 50% of patients start from Mohr–Lenert health state 4, and 50% of patients start from Mohr–Lenert health state 6, in accordance with the characteristics of the patient population of the Németh et al. clinical trial [8]. The average starting age of patients was set to 40 years, and the proportion of males was set to 50%. These base-case settings were evaluated during the sensitivity analyses.
The time horizon of the model was set to 54 weeks (∼1 year) that is the combination of the 6-week initial titration period and four 12-week cycles. The annual discount rate for health outcomes was set to 5% as this value is among the generally accepted discount rates [24]. For an analysis conducted on a longer time horizon, the local discount rates will be used in the model. Results were calculated and presented both with and without allowing switching in the model. Mortality rates were gathered from the data published by the Hungarian Central Statistical Office [25].
Results
Based on the transition relative frequency matrices derived from the Németh et al. clinical trial [8], patients had a higher probability of reaching better health states on the cariprazine arm compared with the risperidone arm of the trial.
The highest quality of life value is associated with Mohr–Lenert health state 1. In the model, 43% of patients were in Mohr–Lenert health state 1 on the cariprazine arm and 23% of patients were in this health state on the risperidone arm after the first modeled year (54 weeks) when switching was not considered. When switching was allowed, 38% of patients were in Mohr–Lenert health state 1 on the cariprazine arm and 23% of patients were in this health state on the risperidone arm after the first modeled year (54 weeks). These changes can be attributed to the fact that patients were more likely to move to health states with higher quality of life values when treated with cariprazine. After switching, the utility is affected in two ways: the person gets rid of the disutility of the side effect but will not gain the relative efficacy of cariprazine anymore. As the utility decrements associated with the side effects are relatively small compared with the utility gain due to being in a better health state, this explains that when switching is considered, there is less QALY gain over a longer time horizon.
Patients on the cariprazine arm of the model gained 0.758 QALYs throughout the first year without therapy switching and 0.754 QALYs when therapy switch was considered. Patients on the risperidone arm of the model gained 0.729 QALYs throughout the first year without therapy switching and 0.729 QALYs when therapy switch was considered.
In the Markov model, the final results showed an estimated QALY gain of 0.029 per patient comparing cariprazine with risperidone after 1 year of treatment when therapy switch was not considered. The model showed an estimated QALY gain of 0.025 per patient comparing cariprazine with risperidone after 1 year of treatment when therapy switch was allowed.
To assess the robustness of these findings, deterministic and probabilistic sensitivity analyses (DSA and PSA) were conducted. Transition probabilities, utility values associated with health states, utility decrements associated with AEs, AE occurrence rates and switching rates were included in the analysis.
The DSA were conducted by changing the values of each input parameter listed above with ±10%. The DSA was performed both with and without therapy switching. According to the results of the DSA, the model was most sensitive to the changes in the utility values associated with Mohr–Lenert health states 1, 2 and 4 (Figures 2 & 3). Histograms were compiled to visualize the results of 1000 model runs of the PSA (Figures 4 & 5).
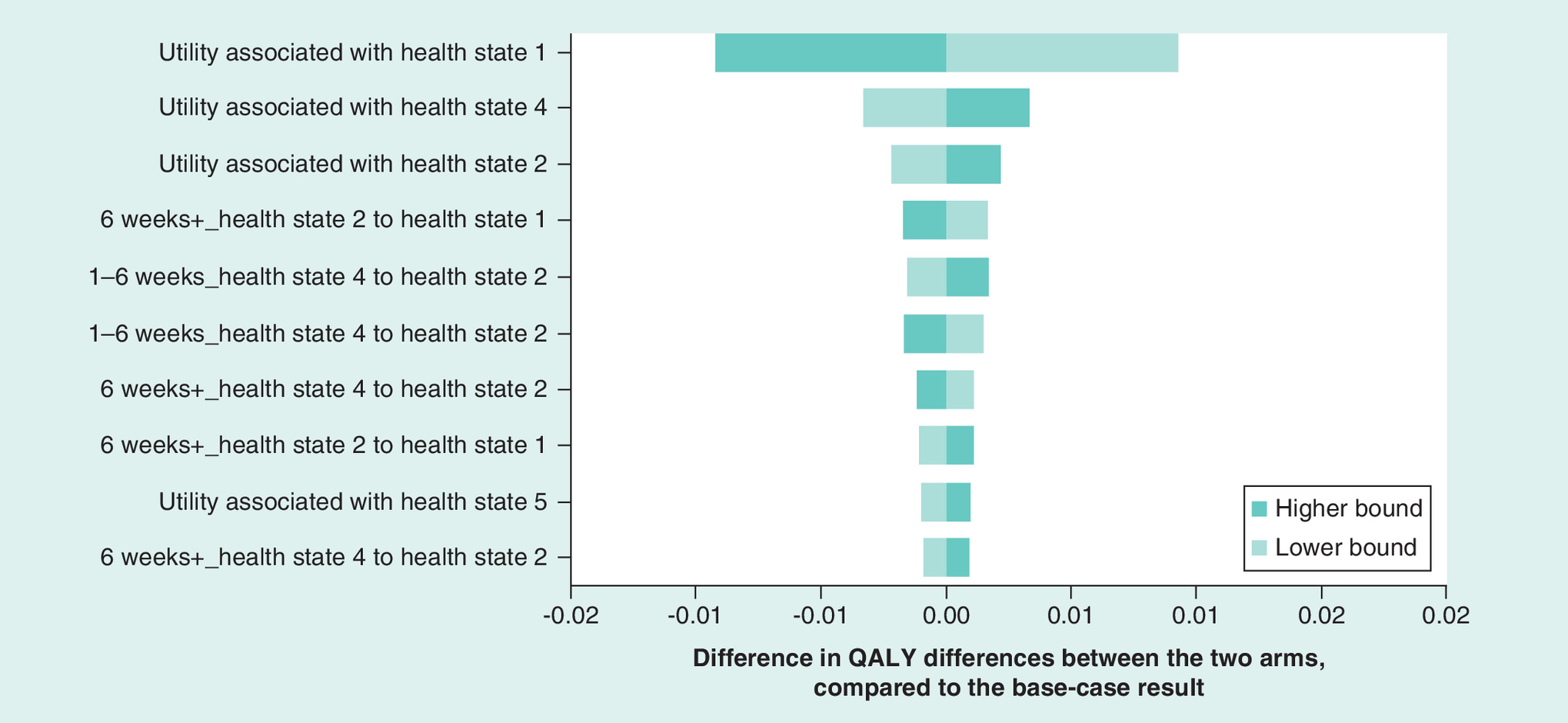
Figure 2. Results of a deterministic sensitivity analysis after one modeled year with switching.
QALY: Quality-adjusted life year.
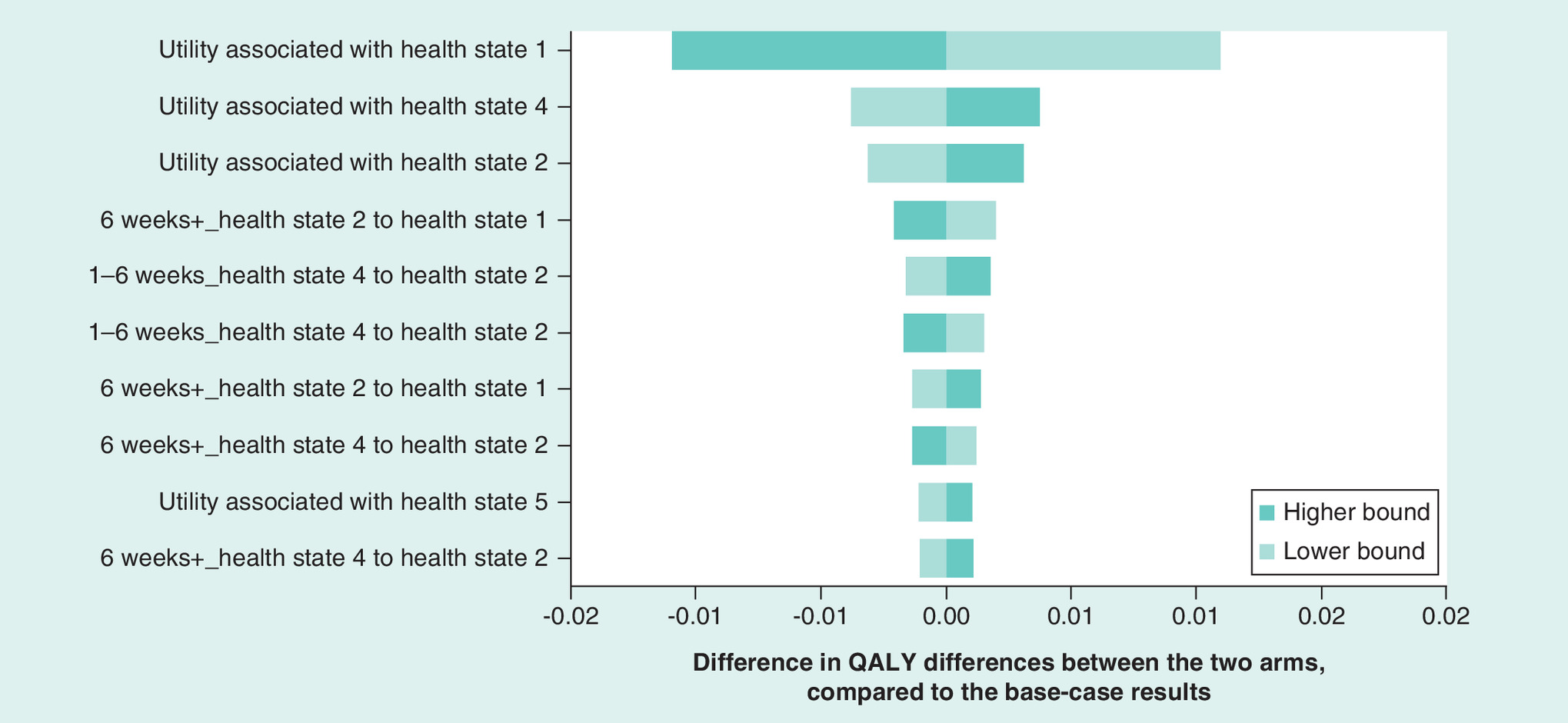
Figure 3. Results of a deterministic sensitivity analysis after one modeled year without switching.
QALY: Quality-adjusted life year.
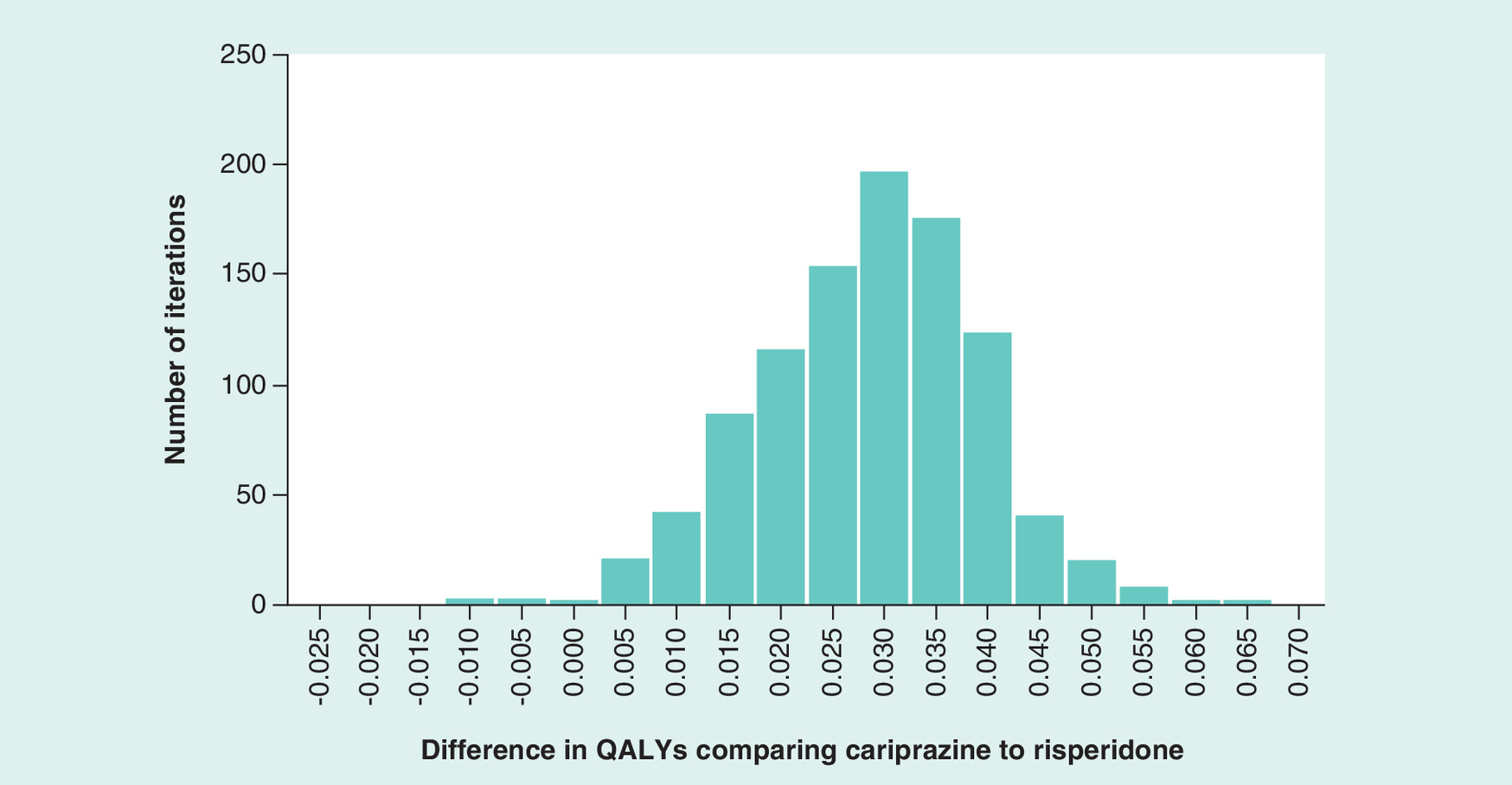
Figure 4. Results of a probabilistic sensitivity analysis after one modeled year with switching.
QALY: Quality-adjusted life year.
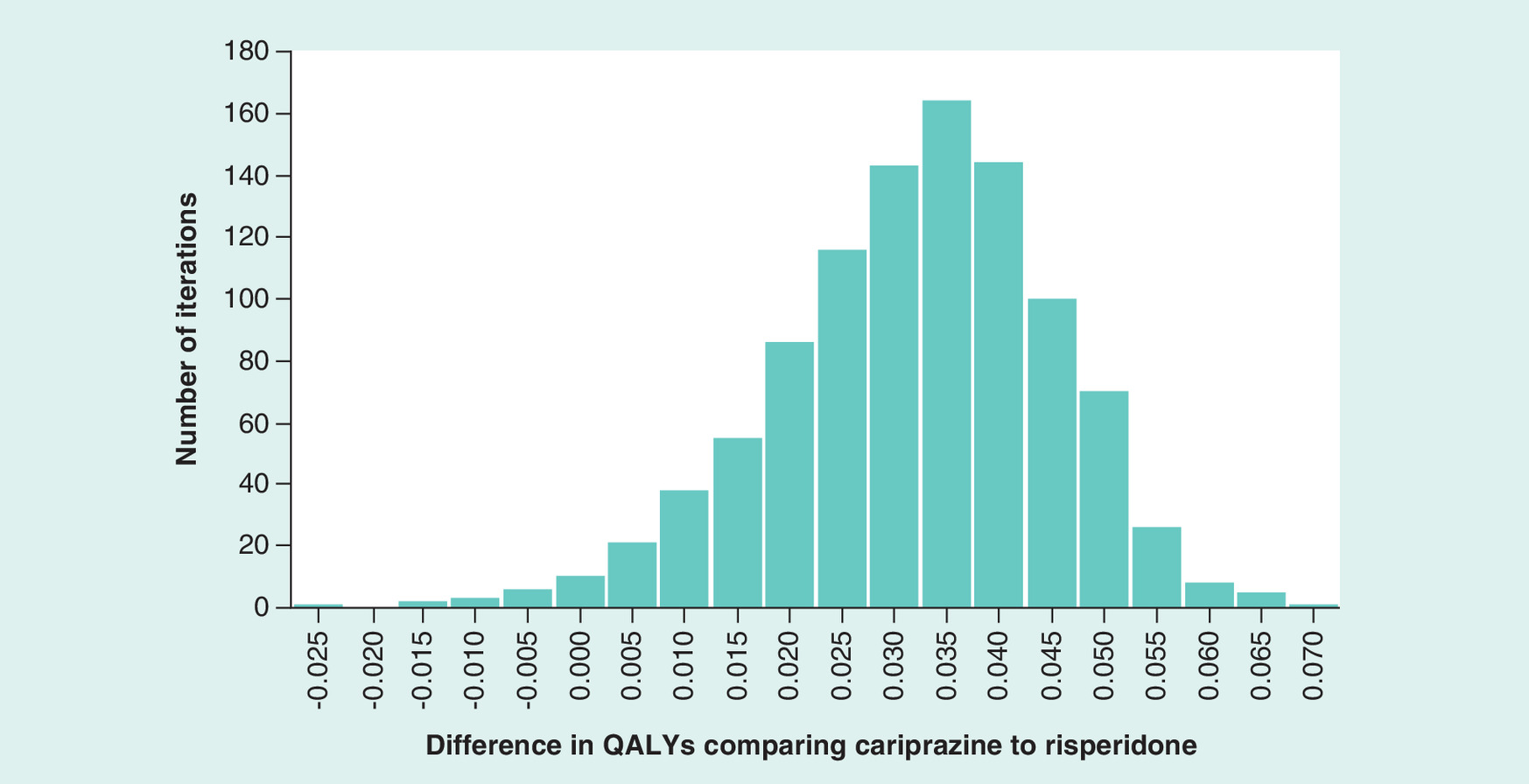
Figure 5. Results of a probabilistic sensitivity analysis after one modeled year without switching.
QALY: Quality-adjusted life year.
When switching was considered, the probabilistic sensitivity analysis showed that cariprazine treatment resulted in more QALYs than risperidone in 99.5% of all model runs. The mean of these QALY differences between the two treatment arms was 0.026 with a standard deviation of 0.011 after 1000 model runs.
When switching was not allowed, the probabilistic sensitivity analysis showed that cariprazine resulted in more QALYs than risperidone in 97.7% of all model runs. The mean of the incremental QALYs was 0.029 with a standard deviation of 0.014 after 1000 model runs.
Discussion
The differences in efficacy in the primary and secondary end points in the Németh et al. clinical trial [8] can be attributed to the fact that previous clinical studies with cariprazine were not focusing on patients with PNS and that most of the earlier clinical trials had a time horizon of only 6 weeks, thus not exceeding the initial titration period. It is also the first large randomized controlled trial that reports significant difference between two compared antipsychotics.
Our analysis demonstrated that cariprazine provides additional QALY gains for PNS patients compared with risperidone. These findings are important as many health technology assessment agencies, like the National Institute for Health and Care Excellence in England, require health benefits to be translated to QALYs for the evaluation of cost–effectiveness [26]. The findings are in line with the results of the Németh et al. clinical trial [8]. The importance of this QALY gain can be thoroughly evaluated after assessing cost and resource utilization data, and calculating an incremental cost–effectiveness ratio.
Switching was built into the model in order to make it suitable for reflecting to the real-life treatment patterns of patients with schizophrenia. When switching was allowed, it slightly decreased the added QALY benefit of cariprazine, however the results still showed higher values on the cariprazine arm compared with the risperidone arm. Applying switching changed the QALYs gained on the risperidone arm to a lesser extent than on the cariprazine arm. It was assumed that other second-generation antipsychotics have the same efficacy as risperidone, therefore the same transition probability matrices were used after a therapy switch on the risperidone arm. After switching occurs on the cariprazine arm, patients move according to the same transition probabilities as on the risperidone arm. The different safety profiles of these pharmaceuticals were taken into account which led to a marginal increase in QALYs on the risperidone arm after therapy switching.
In the DSA, even the most influential input parameters did not change the difference of QALYs between the two arms by more than 0.01, thereby confirming the robustness of the results.
The PSA confirmed the robustness of the base-case analysis results, as the overwhelming majority of model runs resulted in positive incremental QALY values comparing cariprazine with risperidone.
The modeling process was in accordance with standard methodology, data were obtained from the Németh et al. clinical trial [8], all necessary assumptions were of conservative nature and the sensitivity of the results was tested in DSA and PSA. Therefore, this methodology was suitable for providing evidence that the patients with PNS of schizophrenia can have a higher quality of life with cariprazine compared with risperidone.
Potential further steps include analyzing cost–effectiveness of cariprazine treatment after gathering cost and resource utilization data from a specific country and development of an individual-level simulation model based on the structure and the inputs of the Markov state transition model.
Limitations of the study include the following:
As no literature is available describing switching rates related to Mohr–Lenert health states, the switching feature of the model is based on the comprehensive data published by Lieberman [23] on reasons of discontinuation of risperidone treatment. These data were used for estimating the switching rates for both treatment arms, as similar data are not available for cariprazine;
The transition probability matrices derived from the Németh et al. clinical trial [8] lacked transitions between many health states in an extent that it was considered unrealistic to apply the transition probability matrices without adjustment. Additional data were gathered from three expert interviews and were combined with the clinical trial data in a Bayesian analysis;
AEs were assumed not to be dependent on health state, which is a conservative assumption as more patients tend to be in better health states on the cariprazine arm, therefore the occurrence of AEs can be overestimated on this arm;
The Németh et al. clinical trial provided no data on mortality [8] in connection with the eight Mohr–Lenert health states. Therefore, as a conservative assumption, the mortality rates of the general population were used in the model; it was assumed that there is no significant difference in the mortality between the two treatment groups. Neither disease-specific nor health state specific mortality was assumed;
The estimations based on expert interviews, that were conducted to fill the gaps of the transition probability matrices, were not cross-checked with empirical data.
Conclusion
Cariprazine can provide additional QALY gain in the treatment of patients with PNS of schizophrenia compared with risperidone. The robustness of the results was tested and confirmed by deterministic and PSA.
| Name of factor score | Positive factor score | Negative factor score | Cognitive factor score | Mood factor score | Hostility factor score |
|---|---|---|---|---|---|
| Abbreviation | PFS | NFS | CFS | MFS | HFS |
| Positive symptom subscale items included | P1, P3, P5, P6 | – | P2 | – | P4, P7 |
| Negative symptom subscale items included | – | N1–N4, N6 | N5, N7 | – | – |
| General psychopathology symptoms included | G9 | G7, G16 | G5, G10, G11, G12, G13, G15 | G1, G2, G3, G4, G6 | G8, G14 |
P1, P2, P7: items of the positive symptom subscale of the Positive and Negative Syndromes Scale.
N1, N2, N7: items of the negative symptom subscale of the Positive and Negative Syndromes Scale.
G1, G2, G16: items of the general symptom subscale of the Positive and Negative Syndromes Scale.
| Health state | Negative factor score | Positive factor score | Cognitive factor score |
|---|---|---|---|
| Mohr–Lenert health state 1 | <2.1 | <2.7 | <2.9 |
| Mohr–Lenert health state 2 | 2.1–3.4 | <2.7 | <2.9 |
| Mohr–Lenert health state 3 | <3.4 | 2.7–3.9 | <2.9 |
| Mohr–Lenert health state 4 | >3.4 | <3.9 | <2.9 |
| Mohr–Lenert health state 5 | <3.4 | <3.9 | >2.9 |
| Mohr–Lenert health state 6 | >3.4 | <3.9 | >2.9 |
| Mohr–Lenert health state 7 | <3.4 | >3.9 | Any value |
| Mohr–Lenert health state 8 | >3.4 | >3.9 | Any value |
| Adverse event full name | 28-day incidence | |
|---|---|---|
| Cariprazine arm | Risperidone arm | |
| Dyskinesia | 0.40% | 0.54% |
| Pseudo-Parkinsonism | 0.87% | 1.54% |
| Akathisia | 2.07% | 1.07% |
| Orthostatic hypotension | 0.20% | 0.07% |
| Sedation and somnolence | 1.20% | 2.34% |
| Clinically significant weight gain | 0.38% | 1.02% |
Our study aimed at estimating differences in quality-adjusted life year (QALY) gain for schizophrenic patients with predominant negative symptoms treated with cariprazine compared with risperidone.
A data analysis was conducted on individual patient level data derived from the RGH-188–005 clinical trial.
The 30 items of the positive and negative syndrome scale were used to categorize patients into eight different health states.
A Markov state transition model was built with eight health states, to estimate the potential gains in QALYs of patients for 1 year.
The option of therapy switching was also considered in the model.
Patients had higher probability of reaching better health states treated with cariprazine compared with risperidone.
The Markov model showed an estimated QALY gain of 0.029 per patient when therapy switch was not considered and a QALY gain of 0.025 per patient when therapy switch was considered, comparing cariprazine with risperidone after 1 year of treatment.
Cariprazine can provide additional QALY gain in the treatment of schizophrenia for patients with predominant negative symptoms compared with risperidone.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: Supplementary Material
Authors’ contributions
All authors conceived the study. Z Vokó, B Németh, M Horváth and K Kóczián developed the study concept. Z Vokó and B Németh conducted the statistical analysis with support from A Molnár. B Németh and A Molnár wrote the manuscript and Z Vokó contributed substantially to the revision of the earlier drafts. The accuracy of the analysis was checked by R Akehurst, M Horváth, K Kóczián, G Németh and A Götze. All authors have read and approved the final manuscript.
Financial & competing interests disclosure
This study has received funding from Gedeon Richter Plc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Supplementary Material
File (suppl_appendix.docx)
- Download
- 35.39 KB
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
World Health Organization. Schizophrenia Fact sheet (2016). www.who.int/mediacentre/factsheets/fs397/en/
2.
Desai PR, Lawson KA, Barner JC, Rascati KL. Estimating the direct and indirect costs for community-dwelling patients with schizophrenia. J. Pharm. Health Serv. Res. 4(4), 187–194 (2013).
3.
Cloutier M, Aigbogun MS, Guerin A et al. The economic burden of schizophrenia in the United States in 2013. J. Clin. Psychiatry 77(6), 764–771 (2016).
4.
Tandon R, Nasrallah HA, Keshavan MS. Schizophrenia, “just the facts” 4. Clinical features and conceptualization. Schizophr. Res. 110(1–3), 1–23 (2009).
5.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th Edition). American Psychiatric Publishing, VA, USA (2013).
6.
Chue P, Lalonde JK. Addressing the unmet needs of patients with persistent negative symptoms of schizophrenia: emerging pharmacological treatment options. Neuropsychiatr. Dis. Treat. 10, 777–789 (2014).
7.
Debelle M, Németh G, Szalai E et al. Cariprazine as monotherapy for the treatment of schizophrenia patients with predominant negative symptoms: a double-blind, active controlled trial. Eur. Neuropsychopharmacol. 25, S510 (2015).
8.
Németh G, Laszlovszky I, Czobor P et al. Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial. Lancet 389(10074), 1103–1113 (2017).
•• Summarizes the results of the clinical trial that served as the basis of the calculations of the model.
9.
Németh G, Debelle M, Laszlovszky I et al. Monotherapy treatment with cariprazine for the treatment of predominant negative symptoms of patients with schizophrenia: a double-blind, active comparator-controlled trial. Eur. Psychiatry 33, S256–S257 (2016).
10.
Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin. Drug Metabol. Toxicol. 9(2), 193–206 (2013).
11.
Nakamura T, Kubota T, Iwakaji A, Imada M, Kapas M, Morio Y. Clinical pharmacology study of cariprazine (MP-214) in patients with schizophrenia (12-week treatment). Drug Design Dev. Ther. 10, 327–338 (2016).
12.
Pásztor Mészáros G, Kapás M, Borsos M et al. Pharmacokinetics of RGH-188, a new dopamine D3/D2 antagonist/partial agonist atypical antipsychotic, in healthy subjects. Eur. Neuropsychopharmacol. 17, S451–S452 (2007).
13.
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13(2), 261–276 (1987).
14.
Mohr PE, Cheng CM, Claxton K et al. The heterogeneity of schizophrenia in disease states. Schizophr. Res. 71(1), 83–95 (2004).
•• One of the three publications that explain the foundations of the Mohr–Lenert method, which was the basis of the Markov model structure.
15.
Lenert LA, Sturley AP, Rapaport MH, Chavez S, Mohr PE, Rupnow M. Public preferences for health states with schizophrenia and a mapping function to estimate utilities from positive and negative symptom scale scores. Schizophr. Res. 71(1), 155–165 (2004).
•• One of the three publications that explain the foundations of the Mohr–Lenert method, which was the basis of the Markov model structure.
16.
Lenert LA, Rupnow MF, Elnitsky C. Application of a disease-specific mapping function to estimate utility gains with effective treatment of schizophrenia. Health Qual. Life Outcomes 3(1), 57 (2005).
•• One of the three publications that explain the foundations of the Mohr–Lenert method, which was the basis of the Markov model structure.
17.
Lenert LA, Sturley AP, Rapaport MH, Chavez S, Mohr PE, Rupnow M. Corrigendum to Public preferences for health states with schizophrenia and a mapping function to estimate utilities from positive and negative symptom scale scores [Schizophr. Res. 71(1) (2004) 155–165]. Schizophr. Res. 80, 135–136 (2005).
18.
Elfadaly FG, Garthwaite PH. Eliciting Dirichlet and Gaussian copula prior distributions for multinomial models. Stat. Computing 27(2), 449–467 (2017).
19.
Glick ID, He X, Davis JM. First-generation antipsychotics: current status. Primary Psychiatry 13(12), 51–58 (2006).
20.
Furiak NM, Ascher-Svanum H, Klein RW et al. Cost-effectiveness model comparing olanzapine and other oral atypical antipsychotics in the treatment of schizophrenia in the United States. Cost Eff. Resour. Alloc. 7, 4 (2009).
21.
García-Ruiz AJ, Pérez-Costillas L, Montesinos AC, Alcalde J, Oyagüez I, Casado MA. Cost-effectiveness analysis of antipsychotics in reducing schizophrenia relapses. Health Econ. Rev. 2, 8 (2012).
22.
Park T, Kuntz KM. Cost-effectiveness of second-generation antipsychotics for the treatment of schizophrenia. Value Health 17(4), 310–319 (2014).
23.
Lieberman JA, Stroup TS, Mcevoy JP et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N. Engl. J. Med. 353(12), 1209–1223 (2005).
• Basis of the calculations regarding switching rates.
24.
Severens JL, Milne RJ. Discounting health outcomes in economic evaluation: the ongoing debate. Value Health 7(4), 397–401 (2004).
25.
Hungarian Central Statistical Office. Demographic Yearbook 2012. Hungarian Central Statistical Office, Budapest, Hungary (2013).
26.
National Institute for Health and Clinical Excellence. Guide to the methods of technology appraisal 2013 (2013). www.nice.org.uk/process/pmg9/chapter/foreword
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 17 May 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Quality-adjusted life year difference in patients with predominant negative symptoms of schizophrenia treated with cariprazine and risperidone. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2017-0024
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Shivam Tyagi, Ajeet Sidana, Sushmita Bhattacharya, Antipsychotics and their Impact on Biopsychosocial Outcomes in Schizophrenia: A Randomized Comparative Study, Indian Journal of Social Psychiatry, 10.4103/ijsp.ijsp_371_25, 42, 1, (33-40), (2026).
- František Petrovič, František Murgaš, Anna Tirpáková, Marie Hubálovská, György Molnár, Roman Králik, Ján Zozuľak, Enikő Nagy, Marek Nocoń, Zoltán Balogh, Measuring the quality of life university students and its predictors as a basis for its applied research. Cross-country evidence, Sustainable Futures, 10.1016/j.sftr.2025.101214, 10, (101214), (2025).
- Keyuri Adhikari, Khalid Kamal, Ki Jin Jeun, David Nolfi, Mohammed Ashraf, Christopher Zacker, Real-World Effectiveness, Economic, and Humanistic Outcomes of Selected Oral Antipsychotics in Patients with Schizophrenia: A Systematic Review Evaluating Global Evidence, ClinicoEconomics and Outcomes Research, 10.2147/CEOR.S469024, Volume 16, (621-645), (2024).
- S.G. Sukiasyan, ANTIPSYCHOTIC DRUGS: THREE GENERATIONS OF ANTIPSYCHOTICS, ARMENIAN JOURNAL OF MENTAL HEALTH, 10.55436/10.54436/1829202X-15.2024.1-3, (3-26), (2024).
- Andrea de Bartolomeis, Mariateresa Ciccarelli, Giuseppe De Simone, Benedetta Mazza, Annarita Barone, Licia Vellucci, Canonical and Non-Canonical Antipsychotics’ Dopamine-Related Mechanisms of Present and Next Generation Molecules: A Systematic Review on Translational Highlights for Treatment Response and Treatment-Resistant Schizophrenia, International Journal of Molecular Sciences, 10.3390/ijms24065945, 24, 6, (5945), (2023).
- David Taylor, Ramalingam Chithiramohan, Jasdev Grewal, Avirup Gupta, Lars Hansen, Gavin P. Reynolds, Sofia Pappa, Dopamine partial agonists: a discrete class of antipsychotics, International Journal of Psychiatry in Clinical Practice, 10.1080/13651501.2022.2151473, 27, 3, (272-284), (2022).
- Sofia Pappa, Arturas Kalniunas, Hitendra Sharma, Ali Raza-Syed, Manzar Kamal, Fintan Larkin, Efficacy and safety of cariprazine augmentation in patients treated with clozapine: a pilot study, Therapeutic Advances in Psychopharmacology, 10.1177/20451253221132087, 12, (2022).
- Richard Dodel, Christopher Kruse, Annette Conrads-Frank, Uwe Siebert, Pharmacoeconomics, NeuroPsychopharmacotherapy, 10.1007/978-3-030-62059-2_381, (101-234), (2022).
- David Bruhn, Steve Hwang, Ana Howarth, Sanjay Dubé, The burden of illness for patients with schizophrenia and primary negative symptoms: A systematic literature review, Schizophrenia Research, 10.1016/j.schres.2022.09.017, 248, (341-344), (2022).
- Michael Davidson, Jay Saoud, Corinne Staner, Nadine Noel, Sandra Werner, Elisabeth Luthringer, David Walling, Mark Weiser, Philip D Harvey, Gregory P Strauss, Remy Luthringer, Efficacy and Safety of Roluperidone for the Treatment of Negative Symptoms of Schizophrenia, Schizophrenia Bulletin, 10.1093/schbul/sbac013, 48, 3, (609-619), (2022).