The comparative effectiveness of antiretroviral therapies for HIV: evidence to inform precision public health
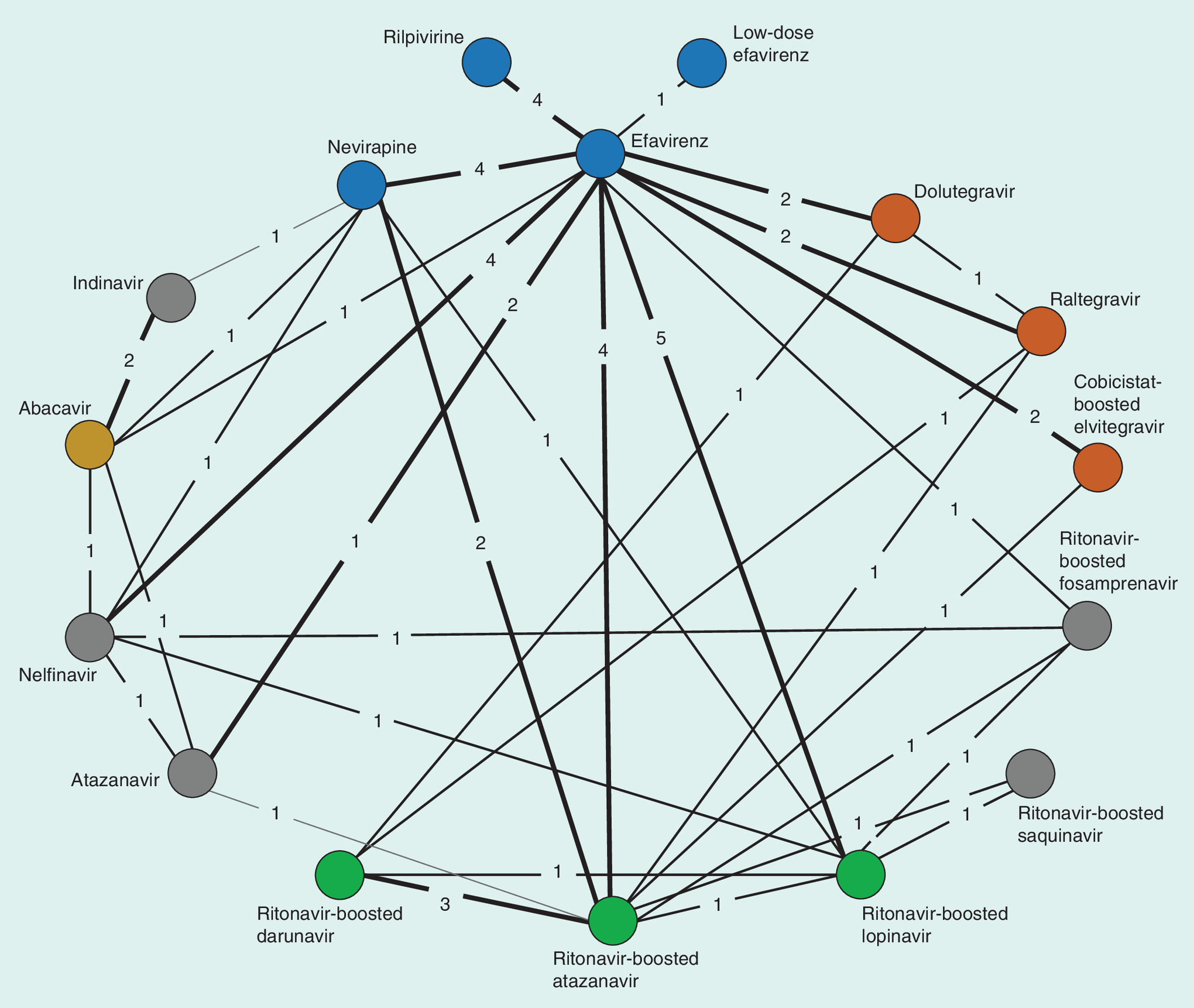
Figure 1. Network of all 71 trials included in the principal analyses.
Circles (nodes) in the diagrams represent individual treatments, lines between circles represent availability of head-to-head evidence between two treatments and the numbers on the lines are the number of randomized clinical trials informing each head-to-head comparison. The colors represent antiretroviral therapy classes, with gray representing older protease inhibitors included in the network as connectors.
First draft submitted: 14 December 2016; Accepted for publication: 16 December 2016; Published online: 25 January 2017
The HIV/AIDS epidemic represents one of the greatest public health challenges of the past century. Since its discovery in 1981, an estimated 35 million people have died and an estimated 37 million people currently live with this viral infection [1,2]. The effects of this pandemic have devastated relationships, households and economies. While the disease disproportionately affects people in low-income settings, particularly Africa, research related to the effectiveness of interventions has predominantly been conducted in low endemic settings, such as the western world [3]. Until the roll-out of antiretroviral therapy (ART) under the direction of the President's Emergency Plan for AIDS Response (PEPFAR) in 2003, few policy-makes expected to be able to provide lifelong ART to patients in poor settings, including Africa and Asia. However, using a simple public health approach based on treating the sickest patients and the most vulnerable (typically mothers to avoid vertical transmission to babies) first, the expansion of ART in developing settings has had remarkable success and now provides lifelong ART to an estimated 18.2 million patients [4]. These successes were built on a framework that provides simplified therapy using a choice of ART that minimizes adverse events and resistance and is associated with negotiated price reductions according to the payers.
As the epidemic now approaches a less emergency-like scenario, there have been increasing efforts to stratify services and choice of drugs according to the needs of patients, the healthcare system and the evidence supporting choice of ART combination. Given that more than 40 different ART regimens exist, the choice of regimen is challenging for decision-makers as most ART regimens include a combination of at least two (and more typically three) drugs. In more developed settings, the choice of ART is often based on local clinical guidelines, physician experience and the history of the patients exposure to ART in an effort to reduce adverse events and resistance [5]. The International Antiviral Society, USA, that produces US relevant guidance, uses systematic searches and supplements this with expert consensus to derive guidance [5]. In low-income settings, the choice of ART is more challenging as the cost of drug regimens can vary importantly and access to the specific drugs may be limited. As a result, major international policy organizations, such as PEPFAR, the WHO and the Clinton Health Initiative, have been involved in advocacy related to price negotiation and access to regimens with both drug developers and generic developers. Determining the choice of regimen that these policy-makers would advocate for has historically been driven by expert advisory panels and has not included a formal comparative effectiveness approach. We were most recently involved in the 2015 guideline development for WHO to determine recommended ART regimens related to low-income settings [6].
Working with WHO, we advocated for a Health Economics and Outcomes Research (HEOR) approach to use a formal comparative effectiveness analysis and, in particular, to apply a network meta-analysis for both first- and second-line ART regimens for adults, adolescents and children. The previous 2013 WHO ART guidelines recommended (for adults and adolescents) a first-line ART consisting of two nucleos(t)ide reverse transcriptase inhibitors (NRTIs) and a non-nucleoside reverse transcriptase inhibitor (NNRTI) [7]. In the presence of contraindications, other NRTI or NNRTI are considered based on availability. Where available, a ritonavir-boosted protease inhibitor (PI/r) based regimen could be considered. The comparative effectiveness of these interventions was unknown.
Since the 2013 WHO ART guidelines [8], several studies had reported results on new first-line regimens, including some using different ART classes and dose optimization strategies. Specifically, newer trials suggest that among ART-naive patients, integrase inhibitor regimens using the currently recommended two-NRTI backbone have favorable efficacy, yet appear to have more favorable safety profiles [9–11]. Also, a low dose efavirenz (an NNRTI) regimen appeared to offer better clinical outcomes than standard dose, but with a better safety profile. Yet placing these new and desireable interventions in the context of the many other combinations was challenging. Thus there was a need for evidence synthesis to determine if current recommended therapies are still the best available options. We therefore employed a network meta-analysis based on all published evidence up to July 2015 [12].
Figure 1 displays the network of evidence for all included trials. Details and exact results of the analysis can be found in the published manuscript [13]. The network is well-connected and centered by standard dose efavirenz. For viral suppression, integrase inhibitor based regimens were found to be more effective than other regimens. For example at 48 weeks, dolutegravir had an odds ratio (OR) of 1.87 in comparison to efavirenz (95% credibility [CrI]: 1.34–2.64) followed by raltegrevir (OR: 1.40; 95% CrI: 1.02 – 1.96). Low-dose efavirenz, was comparable to all other treatments. Estimates were similar across time points. Evidence for the comparisons of interest with respect to viral suppression were considered moderate to strong. These findings were replicated for the analysis examining adolescents, babies and second-line treatments using a similar approach. While some have argued that implementing integrase inhibitor-based regimens as first line in low-income settings is not cost effective [14], others, such as the Rwandan Ministry of Health, have used the evidence to bargain with drug manufacturers for reduced pricing on integrase inhibitor based therapies, thus hoping to achieve better clinical outcomes for their populations and a new era of first-world healthcare in the developing world.
Our current understanding of the comparative effectiveness of ART regimens represents an important precedent for both WHO and the use of Health Economics and Outcomes Research approaches to inform global decision-making for important diseases. This demonstrates a strategy about utilizing and implementing Precision Public Health decision-making to move beyond simplified therapies to medical decision-making informed by the best available evidence that is defensible beyond expert opinion [15].
Acknowledgements
EJ Mills was commissioned by the WHO to conduct the work that this editorial is based on.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
1.
Wang H, Wolock TM, Carter A et al. Estimates of global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2015: the Global Burden of Disease Study 2015. Lancet HIV 3(8), E361–E387 (2016).
2.
Murray CJ, Ortblad KF, Guinovart C et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9947), 1005–1070 (2014).
3.
Kent DM, Mwamburi DM, Bennish ML et al. Clinical trials in sub-Saharan Africa and established standards of care: a systematic review of HIV, tuberculosis, and malaria trials. JAMA 292(2), 237–242 (2004).
4.
UNAIDS. Fact sheet, November 2016. www.unaids.org/en/resources/fact-sheet
5.
Gunthard HF, Saag MS, Benson CA et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2016 recommendations of the International Antiviral Society-USA Panel. JAMA 316(2), 191–210 (2016).
6.
Kanters S, Ford N, Druyts E et al. Use of network meta-analysis in clinical guidelines. Bull. WHO 94(10), 782–784 (2016).
7.
WHO. Global update on HIV treatment 2013: results, impact and opportunities (2013). www.who.int/hiv/pub/progressreports/update2013/en/
8.
Doherty M, Ford N, Vitoria M et al. The 2013 WHO guidelines for antiretroviral therapy: evidence-based recommendations to face new epidemic realities. Curr. Opin. HIV AIDS 8(6), 528–534 (2013).
9.
Mesplède T, Quashie PK, Zanichelli V et al. Integrase strand transfer inhibitors in the management of HIV-positive individuals. Ann. Med. 46(3), 123–129 (2014).
10.
Raffi F, Jaeger H, Quiros-Roldan E et al. Once-daily dolutegravir versus twice-daily raltegravir in antiretroviral-naive adults with HIV-1 infection (SPRING-2 study): 96 week results from a randomised, double-blind, non-inferiority trial. Lancet Infect. Dis. 13(11), 927–935 (2013).
11.
Walmsley SL, Antela A, Clumeck N et al. Dolutegravir plus abacavir–lamivudine for the treatment of HIV-1 infection. N. Engl. J. Med. 369(19), 1807–1818 (2013).
12.
Mills EJ, Thorlund K, Ioannidis JP. Demystifying trial networks and network meta-analysis. BMJ 346, f2914 (2013).
13.
Kanters S, Vitoria M, Doherty M et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: a systematic review and network meta-analysis. Lancet HIV 3(11), E510–E520 (2016).
14.
Pozniak AL, Hill AM. First-line integrase inhibitors for HIV-prices versus benefits. Lancet HIV 3(11), E500–E501 (2016).
15.
Dowell SF, Blazes D, Desmond-Hellman S. Four steps to precision public health. Nature 540, 189–191 (2016).
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 25 January 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
The comparative effectiveness of antiretroviral therapies for HIV: evidence to inform precision public health. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0093
Export citation
Select the citation format you wish to export for this article or chapter.