Cost–effectiveness analysis of endoscopic eradication therapy for treatment of high-grade dysplasia in Barrett’s esophagus
Abstract
Aim: The aim was to evaluate the cost–effectiveness of endoscopic eradication therapy (EET) with combined endoscopic mucosal resection and radiofrequency ablation for the treatment of high-grade dysplasia (HGD) arising in patients with Barrett’s esophagus compared with endoscopic surveillance alone in the UK. Materials & methods: The cost–effectiveness model consisted of a decision tree and modified Markov model. A lifetime time horizon was adopted with the perspective of the UK healthcare system. Results: The base case analysis estimates that EET for the treatment of HGD is cost-effective at a GB£20,000 cost–effectiveness threshold compared with providing surveillance alone for HGD patients (incremental cost–effectiveness ratio: GB£1272). Conclusion: EET is likely to be a cost-effective treatment strategy compared with surveillance alone in patients with HGD arising in Barrett’s esophagus in the UK.
First draft submitted: 6 December 2016; Accepted for publication: 10 March 2017; Published online: 25 May 2017
Barrett’s esophagus (BE) is a precancerous state that can develop into esophageal adenocarcinoma (OAC). BE exists in most patients in a metaplastic state and carries a very low risk of progression to invasive neoplasia and OAC in the region of 0.12–0.5% per year [1,2]. The 2013 British Society of Gastroenterology (BSG) guidelines advise that, in those patients with BE in whom there is no neoplasia, surveillance is recommended for those fit for endoscopy [3]. This is based on existing evidence from published studies which show that surveillance correlates with early-stage cancer diagnosis and likely improved survival from other cancers [4–6]. Recent work from the ProBar study group examined data from the Dutch cancer registry. They compared survival of patients with BE with neoplastic progression during surveillance with those of patients without neoplastic progression and patients with OAC in the general population. They found that OAC was diagnosed at an earlier stage during BE surveillance than in the general population. However, the survival of patients with BE with neoplastic progression was not significantly worse than those of patients without neoplastic progression, and was similar to survival of patients with stage 0 or stage 1 OAC in the general population [7]. In patients with OAC, the prognosis is poor with just over 15% patients being alive at 5 years [8].
Current UK surveillance guidelines [3] recommend that patients with BE undergo endoscopy every 2–5 years. In some patients, no surveillance is recommended due to the negligible risk for cancer progression. The intervals are dependent on the length of BE and presence of intestinal metaplasia at the index endoscopy. However, in a minority of patients with BE there is a molecular and pathological transformation through various dysplastic stages to mucosal dysplasia and cancer and then finally invasive disease where it is desirable to treat early. High-grade dysplasia (HGD) and intramucosal cancer (IMC) (collectively referred to as BE-related neoplasia), arising from BE can carry a 40–60% risk of progressing to OAC [9]. In some series, the risk of patients with HGD in BE progressing to OAC is 16–59% within 5 years of diagnosis [10].
Traditionally, esophagectomy has remained the mainstay of managing those patients with early mucosal neoplasia in BE. This is not only because of the significant risk of progression to OAC but also because up to 40% of patients with HGD may already harbor occult cancer in the Barrett’s segment [11], although subsequent studies suggest this rate is much lower [12]. Even in specialist high-volume centers this operation carries a high mortality rate of 2–5% and subsequent morbidity of up to 40% [13,14]. Recent data from the National Oesophago-Gastric Cancer Audit (NOGCA) in the UK, indicated that 30-day mortality was 2.2% and there were significant postoperative complications and long-term morbidity in 40% of patients [15,16].
The introduction of minimally invasive endotherapies such as photodynamic therapy (PDT), radiofrequency ablation (RFA), cryotherapy and endoscopic mucosal and submucosal resection (EMR and ESD) over the past decade have seen a paradigm shift in the management of patients with BE-related neoplasia. Maximally invasive treatment for early esophageal cancer with esophagectomy continues to carry a significant mortality and morbidity. Surgery was previously reserved for patients with HGD or IMC arising in BE. As a result there has been a major emphasis toward targeting patients who are at risk of developing OAC, to try and intervene at a preneoplastic and early cancer stage of the aggressive disease process to improve outcomes.
In 2010 the UK National Institute for Health and Care Excellence (NICE), published guidelines on the use of RFA in HGD in BE. Subsequently, RFA and EMR are now NICE-approved treatments for HGD and IMC arising in BE. In 2013, the BSG [3] endorsed the use of minimally invasive endoscopic treatment for early Barrett’s neoplasia, together with combined endoscopic resection for lesions, followed by ablation with radio frequency. The American Gastroenterological Association and American College of Gastroenterology also support this approach to patients with BE-related neoplasia over surveillance or surgery with esophagectomy [17,18].
Societies worldwide now endorse the use of minimally invasive endoscopic therapy with endoscopic resection of visible lesions followed by RFA to treat patients with BE-related mucosal neoplasia [3,18]. The 2013 BSG guidelines advise that, for HGD arising in patients with BE that is confined to the mucosa, endoscopic therapy is preferred over esophagectomy or endoscopic surveillance. The use of endoscopic resection is considered to be the therapy of choice for dysplasia associated with visible lesions and T1a neoplasia. In the presence of HGD without visible lesions, these patients should be managed with an endoscopic ablative technique with the majority of the recent evidence base favoring the use of RFA. Several large volume studies have shown high rates of disease eradication with RFA in patients with HGD arising in BE [19–22]. The cost–effectiveness for endoscopic therapy for BE neoplasia remains an area of debate [16].
Cost–effectiveness analysis is used by decision makers to determine the allocation of scare resources. In cost–effectiveness analysis health outcomes are often measured using quality-adjusted life years (QALYs). This measure uses ‘utility’ – a scale in which health is measured from 0 to 1, with 1 being perfect health and 0 being dead or equivalent to being dead. The utility score is multiplied by the amount of time a patient spends in that health state and so accounts for both quality and quantity of life. The preferred method of presenting cost–effectiveness results is the incremental cost–effectiveness ratio (ICER), this ratio takes into account the extra cost and the extra benefit (in this case QALYs). An intervention can be considered cost-effective if the benefits gained are greater than the opportunity costs. ICERs under GB£20,000 up to GB£30,000 are usually considered to be ‘cost-effective’ in the UK [23].
This is the first UK study to evaluate the cost–effectiveness of endoscopic treatment of BE neoplasia versus endoscopic surveillance in a cohort of patients with HGD in BE. Previous UK studies in the same patient cohort have compared different treatment options in practice at the time (e.g., esophagectomy for HGD) [24].
The aim of this study was to evaluate the cost–effectiveness of endoscopic eradication therapy (EET) for the treatment of HGD in BE patients compared with endoscopic surveillance alone in the UK.
Materials & methods
The economic model was developed from the perspective of the National Health Service (NHS) and personal social services. The model adopted a lifetime time horizon; annual discount rates of 3.5% were applied to costs and benefits, as per the NICE reference case [23]. An annual cycle length was used in the model. A hypothetical cohort of BE patients following an initial diagnosis of HGD was modeled. In the intervention (EET) arm, patients with HGD were treated with EET. In the comparator arm, patients with HGD received surveillance only until esophageal cancer developed. In both arms, patients with no dysplasia Barrett’s esophagus (NDBE) or low-grade dysplasia (LGD) were assumed to have surveillance.
Model structure
The model structure is outlined in Figure 1A & B. The model structure consists of an initial decision tree, in which patients in the treatment arm were assumed to have EET. This determines which health state they moved into in the Markov component. After initial treatment all patients enter the natural history Markov model. Patients could move between health states as shown in the diagram (NDBE, LGD, HGD and OAC). In the treatment arm, when patients were ‘new’ to HGD, they went on to have EET. A patient was considered ‘new’ to a health state when they were not there in the last cycle of the model. For example, a patient could undergo EET at the start of the model and enter NDBE, they could then progress to LGD then HGD where they would be given RFA treatment again. As such, dependent on the treatment outcome, the patient re-enters the natural history section either in the health state they were in when they had treatment if the dysplasia was not eradicated, or NDBE. Patients who were not being treated underwent surveillance. If a patient progressed to OAC, they underwent an esophagectomy and the outcome of this treatment was either ‘cured’ with a lifelong lower quality of life (QOL) [13,14] or the patient dies. Costs and utilities were assigned to the number of patients in each health state.
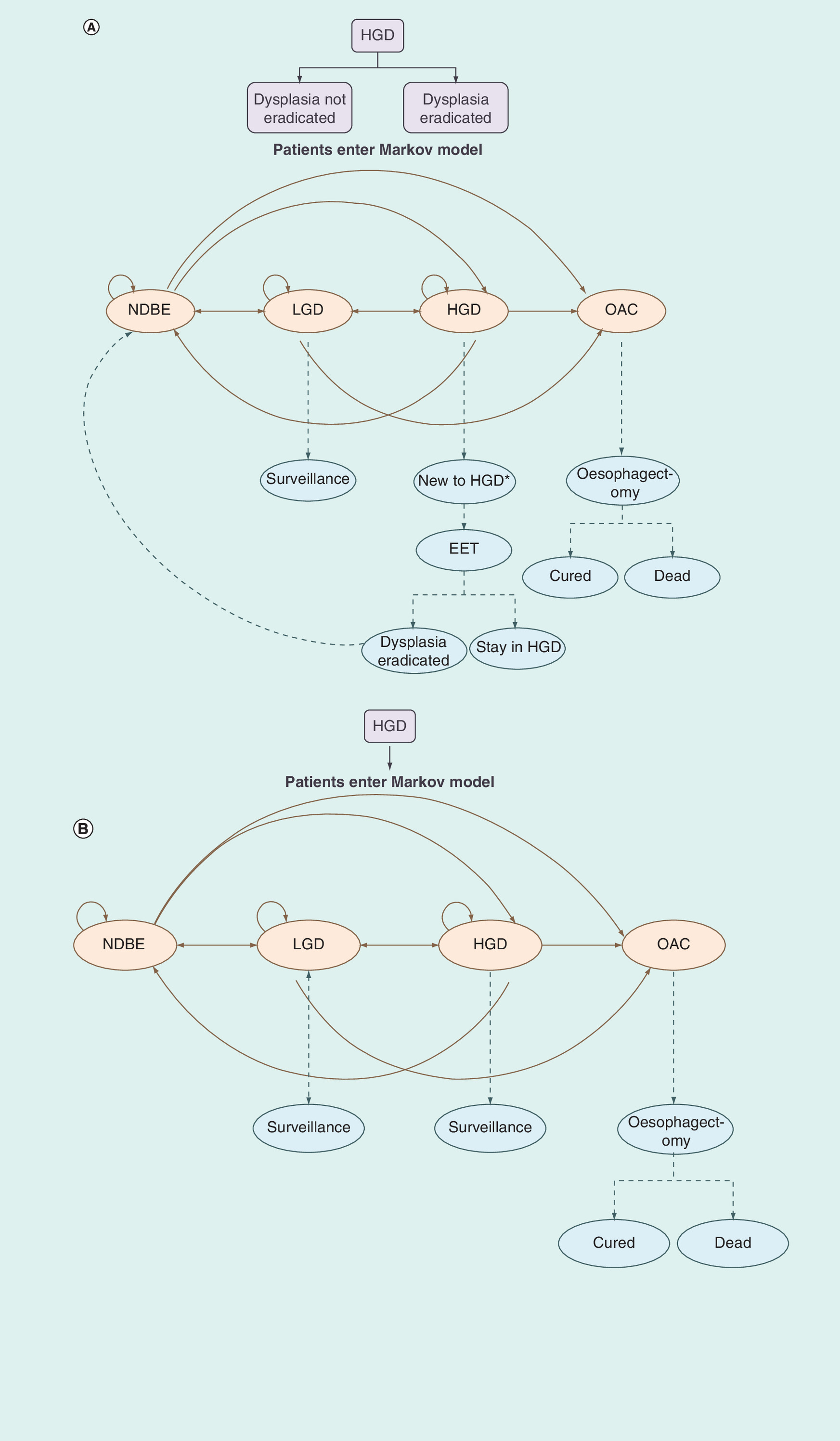
Figure 1. Model structure.
(A) Model structure – treatment arm. The model structure consists of an initial decision tree, in which HGD patients enter the model in the treatment arm and were assumed to have EET. This determines which health state they moved into in the Markov component. After initial treatment all patients enter the natural history Markov model. Patients could move between health states as shown in the diagram (NDBE, LGD, HGD and OAC). Patients in both NDME and LGD receive surveillance and patients in HGD received EET. Patients with OAC undergo esophagectomy. (B) Model structure – comparator arm. The model structure consists of Markov model in which HGD patients enter the model in the comparator arm. All patients enter the natural history Markov model. Patients could move between health states as shown in the diagram (NDBE, LGD, HGD and OAC). Patients in both LGD and HGD receive surveillance. Patients with OAC undergo esophagectomy.
EET: Endoscopic eradication therapy; HGD: High-grade dysplasia; LGD: Low-grade dysplasia; NDBE: Nondysplastic Barrett’s esophagus; OAC: Esophageal adenocarcinoma.
Model inputs
Effectiveness
Effectiveness inputs were derived from published literature and were used in both arms of the model (although applied slightly differently, as illustrated in Figure 1A & B). Three studies were identified that reported transition probabilities [25–27]. Many of the inputs reported were the same or similar. Das et al. [27] had some data missing (probability of movement from LGD to NDBE and LGD) necessary to populate the transition probability matrix. However, these data were mostly taken from Shaheen et al. [25] which is considered separately. Therefore, the options included in the model were two sets of probabilities from Inadomi et al. [26] and one from Shaheen et al. [25]. Inadomi et al. was selected for the base case input because this was the most up-to-date. In addition, Inadomi et al. carried out an analysis in which they altered the absolute values (based on the proportional relationships between transitions) to fit overall cancer incidence statistics. Inputs and sources are summarized in Table 1.
Cost
The unit costs in the model were derived from standard costs sources used in the UK (outlined in Table 1). The resource use was drawn from a variety of sources. Costs were limited to direct healthcare costs. Costs were calculated based on an annual cycle length. For NDBE, one surveillance session every 3–5 years was assumed, two sessions per year for LGD and three sessions per year for HGD, though this cost was only applied in the comparator arm in which HGD patients were not receiving treatment (a scenario analysis was carried out with four sessions per year for HGD). Drugs costs consisted of the average cost of acid suppression during and after the treatment phase with proton pump inhibitors (PPIs; omeprazole, lansoprazole, rabeprazole, pantoprazole and esomeprazole) [31]. Further to clinical expert advice, the dose was doubled for patients who were undergoing endoscopic treatment. The cost of double the dose of PPIs and H2 antagonist drugs was applied for 12 months following EET.
Quality of life
BE utilities were identified from published literature [29] (Table 1). However, the calculations used in the NICE model were based on a utility score of 1 for no BE. A utility of 1 represents perfect health, which is unlikely to be a realistic estimate. Instead, the average utility for a population of this age was included from the EuroQOL population norms [32]. The disutility that was applied to the utility value of 1 in the NICE guidance was applied to the EuroQOL population average instead. Additionally, disutility values were applied when any of the following events occurred: stricture, surgery for perforation, EET, esophagectomy surgery.
Outcomes
The primary outcome of the economic model was the ICER based on the total costs and QALYs for each arm. The additional cost per extra unit of health benefit gained is of key interest to policy and decision-makers. ICERs were calculated as follows:
The standard cost–effectiveness threshold used by NICE is GB£20,000–30,000, that is, an ICER below this threshold is considered ‘cost-effective’ [23].
Sensitivity analysis
Univariate sensitivity analysis was performed on key variables in the model. All input parameters were varied widely, between at least ±50%. Probabilistic sensitivity analysis (PSA) was also undertaken, exploring the impact upon the results when varying all parameters within the model. PSA involves specifying a probability distribution for each parameter. The model then draws a number from each input’s individual distribution and, for each iteration, a result is generated. The type of distribution applied for each input is summarized in Table 2. Due to a lack of data, the majority of standard errors applied were assumptions. However, an approximation of the standard errors for the cost of EMR was derived from the interquartile ranges reported in NHS reference costs [30] and the α and β for the effectiveness inputs were derived from the trial [28].
Results
Base case results
The model estimates that EET for HGD patients is cost-effective at a GB£20,000 threshold compared with providing surveillance alone. The disaggregated results are shown in Table 3. The results show that although there are additional costs associated with RFA at a 30-year time horizon, the QALYs accrued offset this additional cost with an estimated ICER of GB£1272. This translates to a net health benefit of 0.92 QALYs. Net health benefit is the value of the benefit minus the costs. Here it is the incremental QALYs minus the total costs divided by a GB£20,000 threshold (the health expected to be forgone elsewhere).
The results show the ‘per patient’ cost of each health state. These costs take into account the number and the time spent in each health state. The health state costs consist of the cost of surveillance and the cost of drugs. The costs relating to EET have been separated out for clarity. These costs include the cost of EMR, RFA, complications associated with RFA and any additional drugs that are prescribed as a result of RFA. It should be noted that these costs are incurred in the HGD health state explaining why the average per patient cost in HGD in the treatment arm is not higher.
Figure 2A shows the Markov cohort trace for the treatment and Figure 2B for the comparator arm. The Markov cohort trace helps to visualize the movement of patients through a fairly complex model structure.
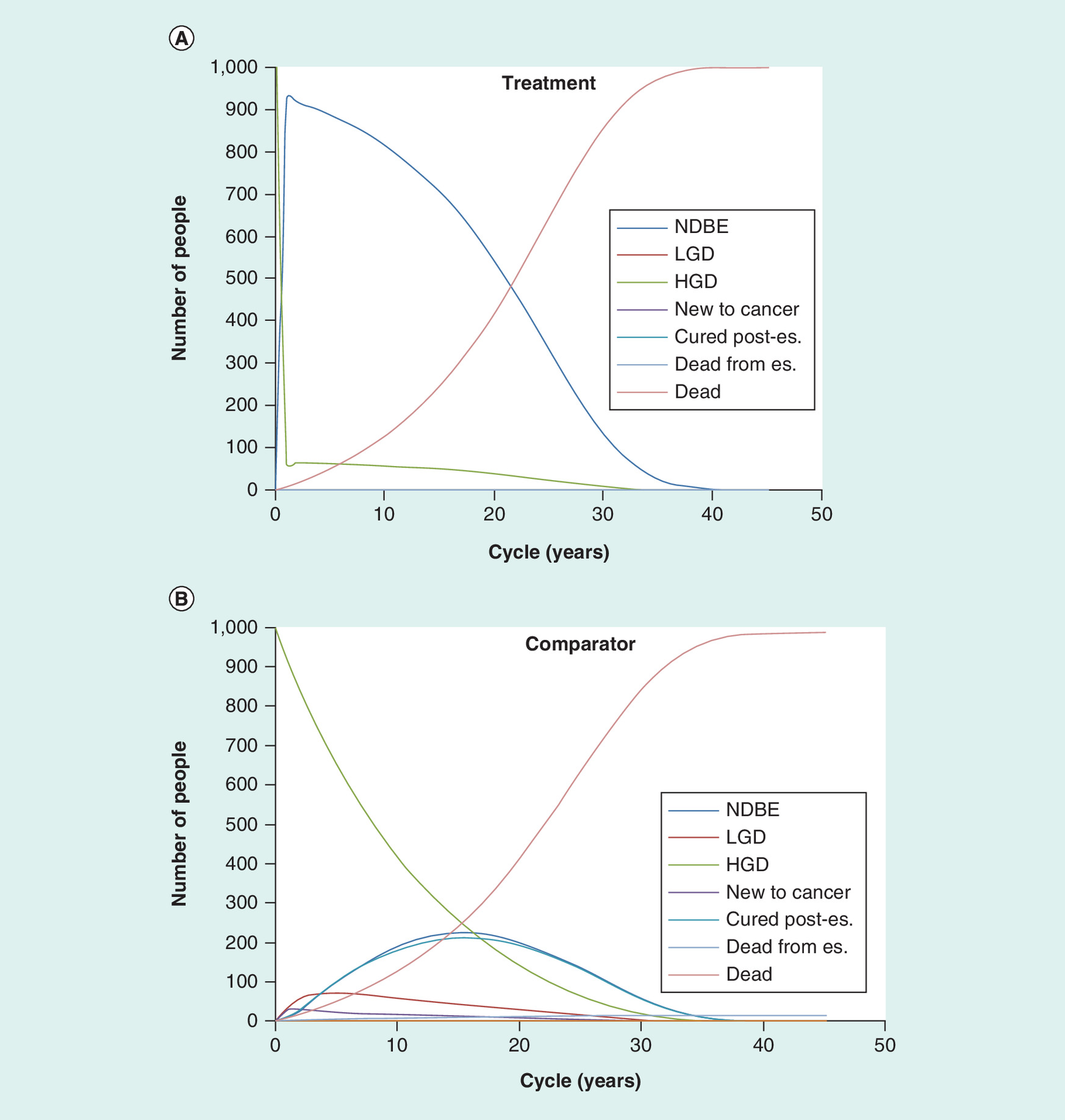
Figure 2. Cohort Traces.
(A) Cohort trace – treatment arm – number of people in each health state by time point. (B) Cohort trace – comparator – number of people in each health state by time point.
es.: Esophagectomy; HGD: High-grade dysplasia; LGD: Low-grade dysplasia; NDBE: Nondysplastic Barrett's esophagus.
Figure 2A shows that in the treatment arm patients are progressing more slowly (some of them have treatment and move back to NDBE where they re-enter the natural history model). Initially this is positive, because fewer patients are in the more serious health states in which higher costs are incurred and in which the patient has lower utility. However, because patients are progressing through the model more quickly in the comparator arm, more patients are undergoing esophagectomy. For the patients that undergo esophagectomy, the only outcomes are death, which incurs no cost and no utility or ‘cured’ in which no costs are incurred but the patient has a lower lifetime utility. While these patients are not incurring any costs (but are incurring reduced utility), patients in the treatment arm are continuing in the natural history model, incurring treatment costs and disutility associated with adverse events.
Figure 2B shows the Markov trace for the comparator arm. In the comparator arm, patients are progressing more quickly through the natural history model and there are more people in the ‘cured’ and ‘dead postesophagectomy’ because patients progress through the health states faster. There are also far more patients with HGD compared with the treatment arm in which more patients spend time in the NDBE health state.
Univariate sensitivity analysis
Extensive univariate sensitivity analyses have been carried out in which one parameter within the model is varied in isolation to assess its impact on the model’s results. Sensitivity analyses that have a significant impact on the model results (i.e., the ICER increased over GB£20,000) are reported here.
Figure 3A shows that, intuitively, as the proportion of patients who have residual dysplasia following treatment for HGD is decreased (treatment is more effective) the ICER increases.
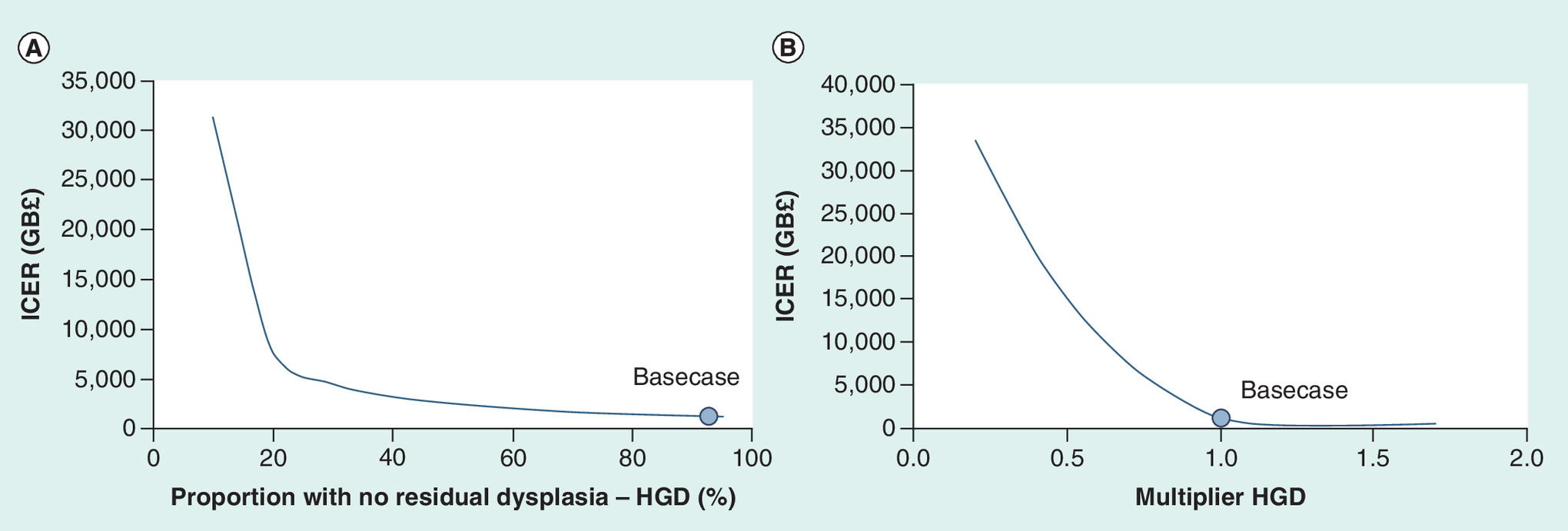
Figure 3. Deterministic Sensitivity Analyses.
(A) One-way sensitivity analysis – varying the proportion of patients with residual HGD after endoscopic eradication therapy. (B) One-way sensitivity analysis – HGD multiplier – varying the probability of patients staying in the HGD health state in each cycle.
HGD: High-grade dysplasia; ICER: Incremental cost–effectiveness ratio.
Figure 3B shows that as the HGD multiplier is increased (more people stay in the HGD state each cycle) the ICER decreases. When the multiplier is applied it changes the transition probability values (the probability of patients moving between health states in each cycle). When the HGD multiplier is increased, the probability of staying in HGD each cycle increases and the probability of staying in all the other health states is reduced proportionally. The graph levels out due to the proportion staying in HGD reaching 100%.
A scenario analysis was carried out in which ongoing costs were applied to patients postesophagectomy. This was not included in the base case due to a lack of data with which to populate this parameter. However, in the scenario analysis an assumption was applied that patients incur costs of GB£500 every year, for life after esophagectomy. As expected, the results showed that a higher cost associated with esophagectomy results in a lower ICER. The results of this scenario analysis did not change the direction of results.
A further scenario analysis was carried out in which the number of surveillance appointments in patients with HGD was increased from three per year to four per year. The results showed that the costs increased in the comparator arm for HGD patients. This resulted in a cost saving and, therefore, a dominant ICER.
Probabilistic sensitivity analysis
A visual inspection of a graphical representation of the mean of the estimates showed that reasonable stability in the estimates had been achieved by 2000 iterations; 65% of iterations were cost-effective using a GB£20,000 threshold, and 67% using a GB£30,000 threshold (Figure 4).
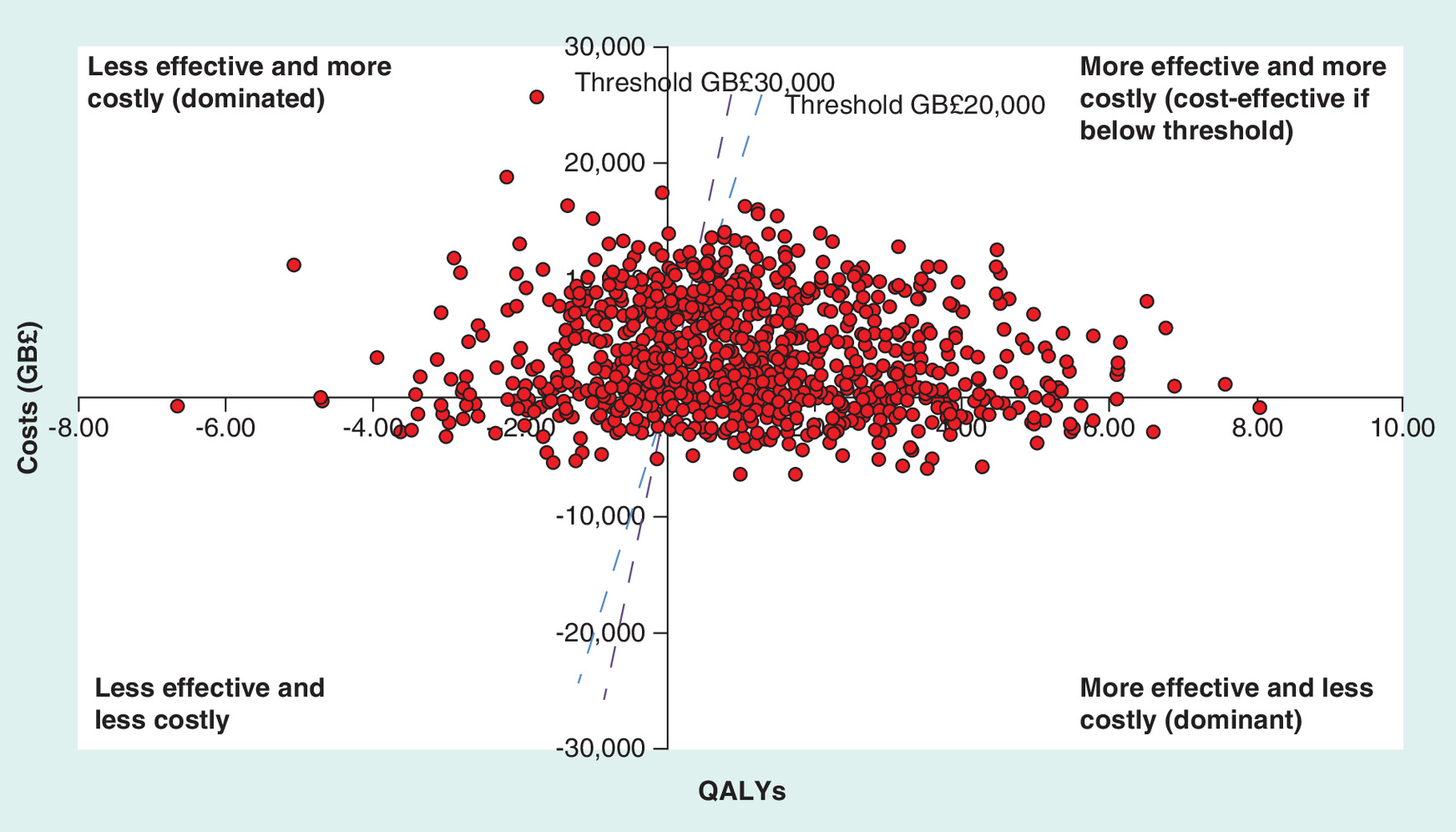
Figure 4. Results of probabilistic sensitivity analysis.
The blue dashed line represents the GB£20,000 cost–effectiveness threshold. The purple dashed line represents the GB£30,000 threshold. Each data point on the graph shows the model results for cost and effect for one iteration of the probabilistic sensitivity analysis. Any iterations that fall below the cost–effectiveness threshold (dashed line) represent iterations can be considered cost-effective.
QALY: Quality adjusted life year.
Discussion
Our analysis estimates that treating patients with BE and HGD with EET compared with endoscopic surveillance alone is cost-effective from a UK healthcare perspective. The results are in line with the findings of previous similar studies [24,26,34]. However, this is the first UK study to evaluate the cost–effectiveness of EET versus endoscopic surveillance in a cohort of HGD patients. The main aims of this study were to reflect current BSG recommendations for treating HGD with EET [3] and address the gap identified in the 2015 NOGCA [16] which suggested that over a quarter of patients with HGD were managed with surveillance alone.
Previous studies have been carried out from the US healthcare perspective, in which practice and resource use is likely to differ from the UK [26,34]. Previous UK studies in the same patient cohort have compared different treatment options in practice at the time (e.g., esophagectomy for HGD) [24], but this is no longer standard practice in the UK as evidenced by recent audit data showing that surgery for patients with HGD is performed only in a small minority of patients (6.3%) [16].
Univariate sensitivity analysis identified the key areas of uncertainty that were likely to affect the direction of results. The first parameter identified was the proportion of patients who had residual dysplasia following RFA treatment. The data input for this value was derived from a single landmark randomised control trial (RCT) of 119 patients with BE-related neoplasia receiving RFA and, therefore, we can be reasonably confident in this input value. For the results to cross the GB£20,000 threshold, the proportion of successful treatment would have to decrease below 20% (base case: 92.6%). Such a large change in the success of RFA treatment is unlikely based on the abundance of recent publications from around the world showing dysplasia eradication rates of over 80% [21,35].
The second parameter is the HGD multiplier. The relationship between inputs when changing the multiplier is complex (see Figure 1A & B). When there are fewer people within HGD, there are proportionally more people in the other three health states (NDBE, LGD, OAC). In order for the ICER to increase above GB£20,000, there would have to be less than half the proportion of patients that stay in the HGD health state each year in the natural history model. This would result in the other half of patients moving to the other health states because transition probabilities must add to 100% each cycle.
As with all models, the model structure reflects a simplification of reality. There may be some nuances in clinical practice that are not accounted for in the model structure which often reflects a lack of data to populate the necessary model parameters (such as, the distinction between early and late esophageal cancer and the fact that current practice is variable, with a small proportion of patients receiving surgery when HGD is present [16] and the fact that some patients with OAC may present too late for surgery and will receive palliation only). In addition, some patients may regress to LGD after RFA and carry on treatment, not including this in the model should not impact on the results given that the patient incur the same costs and it is likely they experience a similar QOL as HGD patients. There is an assumption that all patients with HGD are fit to undergo repeated procedures for EET and also the patients with HGD in the surveillance arm are fit for regular surveillance until they develop cancer. We also assume that being in an endoscopic surveillance program results in cancer detected at an early stage that will result in the likelihood of curative intervention with surgery. This has been the basis for all the international guidance on BE surveillance but recent data show that actually even though cancer may be detected early there may not actually be a difference in survival in these patients [7]. However, the model aims to capture mean inputs for the average patient and find a balance between a model structure that is too complex or simple dependent, in part, on the data available with which to populate the model.
Due to a lack of data, many of the model inputs relied on previous literature, some of which was not based in the UK [26] or relied on expert clinical opinion. For example, due to a lack of natural history data, the inputs used were from a previous model which calibrated the transition probabilities necessary for the model to the US annual incidence rates. The impact of varying these inputs on the model results was tested using univariate and PSA, discussed above.
Since April 2012, the NOGCA has been collecting data on patients with a new diagnosis of esophageal HGD in the UK. After 2 years of data collection, data on 930 cases of HGD were analyzed. The majority of these patients were offered EET and were managed nonsurgically, with EMR and RFA being used most frequently (67.5%). Only 6.3% of patients underwent a surgical resection which in young patients, those with multifocal HGD with nodules that would risk EET being unsuccessful remains an alternative in the minority. The data showed that 26.2% of patients were managed by endoscopic surveillance alone. It must be pointed out that data collection for this audit commenced in April 2012 some months prior to the BSG guidelines in 2013 recommending EET as first-line treatment for HGD patients. The data show that the proportion of HGD patients managed with surveillance alone increased with age, from 12.6% for patients aged under 60 years to 43.2% in patients aged 80 years or over (p < 0.001). This suggests that in some of the more elderly patients with comorbidity and other medical conditions precluding repeated endoscopic treatment surveillance until cancer developed was a more attractive option. Access to EET for patients with BE-related neoplasia is still limited to specialist cancer centers within the UK and, therefore, certain patients may have not had access, although with dissemination of national guidelines this is likely to change in the next round of audit.
Patients with BE-related neoplasia and HGD are at risk of developing OAC and suffer a poor prognosis once this occurs. Continuing advances in minimally invasive endoscopic therapy with advanced imaging to guide EMR followed by RFA mean that high rates of disease eradication are possible with a very good safety profile in these patients. International societies advise that the role of EET can be preferable to surgery or surveillance in these patients [3,18] and our results suggest that this minimally invasive approach might also be a cost-effective strategy and should help shape policy and resource planning locally.
| Parameter | Base case | Notes | Ref. |
|---|---|---|---|
| Effectiveness inputs | |||
| Success of RFA for HGD: | |||
| – Complete eradication of dysplasia | 92.6% | – | [28] |
| – Residual dysplasia | 7.4% | – | [28] |
| – Natural history transition probabilities | Full table available in reference | – | [26] |
| Cost inputs | |||
| RFA | GB£1509 per session | Average number of treatments = 3 | [29,30] |
| EMR | GB£702 per session | Average number of treatments = 1 | [29,30] |
| Stricture | GB£3931 | Average number of sessions to treat stricture is 1.3 (average) endoscopies and dilatations | [19,29–30] |
| Perforation | GB£7807 | Cc score of 2–3. 6-day stay | [30] |
| Esophagectomy | GB£9678 | Excess bed days included. Total stay 12 days | [29,30] |
| Surveillance | GB£681 | And expert opinion | [30] |
| PPI drug costs | Average annual cost = GB£61 | – | [31] |
| PPI additional following surgery | GB£61 | – | [31] |
| H2 antagonist drugs following surgery | GB£444.69 – ranitidine | – | [31] |
| Utility inputs | |||
| Cured (or no Barrett’s esophagus) | 0.80 | [32] | |
| NDBE | 0.71 | Calculated from the disutilities used in | [29] |
| LGD | 0.65 | Calculated from the disutilities used in | [29] |
| HGD | 0.57 | Calculated from the disutilities used in | [29] |
| OAC | 0.48 | Calculated from the disutilities used in | [29] |
| Cured – postesophagectomy | 0.774 | Calculated from | [26] |
| Stricture | -0.03 (applied for 0.25 months) | Calculated from | [29] |
| Surgery for perforation | -0.28 (applied for 0.5 months) | Calculated from | [29] |
| EMR and RFA surgery | -0.06 (applied for 0.5 months) | – | [24] |
| Esophagectomy surgery | -0.26 (applied for 9 months) | Calculated from | [29] |
| Safety inputs | |||
| Rate of stricture in RFA procedure | 9% | – | [19] |
| Rate of perforation in RFA procedure | 0.1% | Clinical expert opinion | – |
| Mortality from esophagectomy | 4.3% | – | [16] |
| All-cause mortality | Dependent on starting age and cycle in the model | – | [33] |
EMR: Endoscopic mucosal resection; HGD: High-grade dysplasia; LGD: Low-grade dysplasia; NDBE: No dysplasia Barrett’s esophagus; OAC: Esophageal adenocarcinoma; PPI: Proton pump inhibitor; RFA: Radiofrequency ablation.
| Parameter | Distribution |
|---|---|
| Utilities | β |
| Disutilities (QALYs lost) | γ |
| Costs | γ |
| Safety | β |
| Effectiveness | |
| HGD: No residual dysplasia | β |
| Multiplier NDBE, LGD, HGD | Lognormal |
HGD: High-grade dysplasia; LGD: Low-grade dysplasia; NDBE: No dysplasia Barrett’s esophagus; QALY: Quality-adjusted life year.
| Outcome | Treatment | Comparator | Incremental |
|---|---|---|---|
| Cost of EET (GB£)† | 6317 | 0 | 6317 |
| Cost of NDBE (GB£) | 2735 | 41 | 2694 |
| Cost of LGD (GB£) | 1074 | 357 | 718 |
| Cost of HGD (GB£) | 70 | 8047 | −7977 |
| Cost of OAC (GB£) | 573 | 1079 | −506 |
| Total cost (GB£) | 10,769 | 9524 | 1246 |
| Total QALYs | 10.041 | 9.062 | 0.979 |
| ICER (GB£) | – | – | 1272 |
| NMB | – | – | 0.92 |
EET: Endoscopic eradication therapy; HGD: High-grade dysplasia; ICER: Incremental cost–effectiveness ratio; LGD: Low-grade dysplasia; NDBE: No dysplasia Barrett’s esophagus; NMB: Net health benefit; OAC: Esophageal adenocarcinoma; QALY: Quality-adjusted life year.
†
Cost of EET includes all associated costs (EMR, complications and drug costs).
What is already known about this subject?
Current clinical recommendations are to treat patients with Barrett’s esophagus and high-grade dysplasia (HGD) with endoscopic eradication therapy (EET) before esophageal cancer develops.
The 2015 UK National Oesophago-Gastric Cancer Audit identified that over a quarter of patients with HGD were still managed with surveillance alone.
Previous studies have investigated the cost–effectiveness of different treatment strategies for HGD. However, there were no available studies in the UK comparing EET with surveillance alone in patients with HGD.
What are the new findings?
The base case economic model results estimate that EET is a cost-effective treatment strategy compared with surveillance alone for treating HGD patients in the UK.
The additional quality-adjusted life years that patients gained offset the costs associated with EET treatment.
Probabilistic sensitivity analysis showed a 61% probability of EET being cost-effective at a GB£20,000 threshold.
A scenario analysis, in which the number of surveillance appointments in patients with HGD was increased from three to four per year, resulted in a cost saving and, therefore, a dominant incremental cost–effectiveness ratio.
How might it impact on clinical practice in the foreseeable future?
International consensus supports EET for patients with Barrett’s esophagus-related neoplasia. In the UK, a significant proportion of patients with HGD still undergo surveillance alone. These data suggest that offering endoscopic therapy in those fit for treatment is an attractive and cost-effective approach.
Financial & competing interests disclosure
A Filby and M Taylor’s employer York Health Economics Consortium received funding for health economics consultancy from Medtronic (manufacturer of Barrx RF ablation products). R Haidry has received educational grants to support research from Medtronic.The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open Access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
References
Papers of special note have been highlighted as: • of interest
1.
Bhat S, Coleman HG, Yousef F et al. Risk of malignant progression in Barrett's esophagus patients: results from a large population-based study. J. Natl Cancer Inst. 103(13), 1049–1057 (2011).
2.
Hvid-Jensen F, Pedersen L, Drewes AM, Sorensen HT, Funch-Jensen P. Incidence of adenocarcinoma among patients with Barrett's esophagus. N. Engl. J. Med. 365(15), 1375–1383 (2011).
3.
Fitzgerald RC, di Pietro M, Ragunath K et al. British Society of Gastroenterology guidelines on the diagnosis and management of Barrett's oesophagus. Gut 63(1), 7–42 (2014).
4.
Corley DA, Mehtani K, Quesenberry C, Zhao W, de Boer J, Weiss NS. Impact of endoscopic surveillance on mortality from Barrett's esophagus-associated esophageal adenocarcinomas. Gastroenterology 145(2), 312–319 e311 (2013).
5.
Fountoulakis A, Zafirellis KD, Dolan K, Dexter SP, Martin IG, Sue-Ling HM. Effect of surveillance of Barrett's oesophagus on the clinical outcome of oesophageal cancer. Br. J. Surg. 91(8), 997–1003 (2004).
6.
Cooper GS, Yuan Z, Chak A, Rimm AA. Association of prediagnosis endoscopy with stage and survival in adenocarcinoma of the esophagus and gastric cardia. Cancer 95(1), 32–38 (2002).
7.
Kastelein F, van Olphen SH, Steyerberg EW, Spaander MC, Bruno MJ, ProBar-Study Group. Impact of surveillance for Barrett's oesophagus on tumour stage and survival of patients with neoplastic progression. Gut 65(4), 548–554 (2016).
8.
Oesophageal Cancer (C15), Age-Standardised One-, Five- and Ten-Year Net Survival, Adults (Aged 15–99), England and Wales, 2010–2011. www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/oesophageal-cancer/survival#A77uzhsT4OaPBkU5.99
9.
Buttar NS, Wang KK, Sebo TJ et al. Extent of high-grade dysplasia in Barrett's esophagus correlates with risk of adenocarcinoma. Gastroenterology 120(7), 1630–1639 (2001).
10.
Montgomery E, Goldblum JR, Greenson JK et al. Dysplasia as a predictive marker for invasive carcinoma in Barrett esophagus: a follow-up study based on 138 cases from a diagnostic variability study. Hum. Pathol. 32(4), 379–388 (2001).
11.
Fernando HC, Luketich JD, Buenaventura PO, Perry Y, Christie NA. Outcomes of minimally invasive esophagectomy (MIE) for high-grade dysplasia of the esophagus. Eur. J. Cardiothorac. Surg. 22(1), 1–6 (2002).
12.
Wang VS, Hornick JL, Sepulveda JA, Mauer R, Poneros JM. Low prevalence of submucosal invasive carcinoma at esophagectomy for high-grade dysplasia or intramucosal adenocarcinoma in Barrett's esophagus: a 20-year experience. Gastrointest. Endosc. 69(4), 777–783 (2009).
13.
Prasad GA, Wang KK, Buttar NS et al. Long-term survival following endoscopic and surgical treatment of high-grade dysplasia in Barrett's esophagus. Gastroenterology 132(4), 1226–1233 (2007).
14.
Fernandez FG, Meyers BF. Quality of life after esophagectomy. Semin. Thorac. Cardiovasc. Surg. 16(2), 152–159 (2004).
15.
Palser TR, Cromwell DA, Hardwick RH et al. Re-organisation of oesophago-gastric cancer care in England: progress and remaining challenges. BMC Health Serv. Res. 9, 204 (2009).
16.
Drehmer M, Pereira MA, Schmidt MI et al. Associations of dairy intake with glycemia and insulinemia, independent of obesity, in Brazilian adults: the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Am. J. Clin. Nut. 101(4), 775–782 (2015).
17.
Shaheen NJ, Falk GW, Prasad GA, Gerson L. ACG clinical guideline: diagnosis and management of Barrett’s esophagus. Am. J. Gastroenterol. 111(1), 30–50 (2015).
18.
American Gastroenterological A, Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ. American Gastroenterological Association medical position statement on the management of Barrett's esophagus. Gastroenterology 140(3), 1084–1091 (2011).
19.
Haidry RJ, Dunn JM, Butt MA et al. Radiofrequency ablation and endoscopic mucosal resection for dysplastic barrett's esophagus and early esophageal adenocarcinoma: outcomes of the UK National Halo RFA Registry. Gastroenterology 145(1), 87–95 (2013).
20.
Shaheen NJ, Sharma P, Overholt BF et al. Radiofrequency ablation in Barrett's esophagus with dysplasia. N. Engl. J. Med. 360(22), 2277–2288 (2009).
21.
Phoa KN, Pouw RE, Bisschops R et al. Multimodality endoscopic eradication for neoplastic Barrett oesophagus: results of an European multicentre study (EURO-II). Gut 65(4), 555–562 (2016).
22.
Phoa KN, Pouw RE, van Vilsteren FG et al. Remission of Barrett's esophagus with early neoplasia 5 years after radiofrequency ablation with endoscopic resection: a Netherlands cohort study. Gastroenterology 145(1), 96–104 (2013).
23.
Developing NICE Guidelines: The Manual. (Eds.) National Institute for Health and Care Excellence, 2014) www.nice.org.uk/media/default/about/what-we-do/our-programmes/developing-nice-guidelines-the-manual.pdf
24.
Boger PC, Turner D, Roderick P, Patel P. A UK-based cost-utility analysis of radiofrequency ablation or oesophagectomy for the management of high-grade dysplasia in Barrett's oesophagus. Aliment. Pharmacol. Ther. 32(11–12), 1332–1342 (2010).
25.
Shaheen NJ, Inadomi JM, Overholt BF, Sharma P. What is the best management strategy for high grade dysplasia in Barrett's oesophagus? A cost–effectiveness analysis. Gut 53(12), 1736–1744 (2004).
26.
Inadomi JM, Somsouk M, Madanick RD, Thomas JP, Shaheen NJ. A cost-utility analysis of ablative therapy for Barrett's esophagus. Gastroenterology 136(7), 2101–2114 e2101–e2106 (2009).
27.
Das A, Wells C, Kim HJ, Fleischer DE, Crowell MD, Sharma VK. An economic analysis of endoscopic ablative therapy for management of nondysplastic Barrett's esophagus. Endoscopy 41(5), 400–408 (2009).
28.
Shaheen NJ, Overholt BF, Sampliner RE et al. Durability of radiofrequency ablation in Barrett's esophagus with dysplasia. Gastroenterology 141(2), 460–468 (2011).
• This paper is of interest as the single landmark randomized controlled trial of 119 patients with Barrett's esophagus related neoplasia receiving radiofrequency ablation, the findings of which underpin the economic model.
29.
Li R, Zhang P, Barker LE, Chowdhury FM, Zhang X. Cost–effectiveness of interventions to prevent and control diabetes mellitus: a systematic review. Diabetes Care 33(8), 1872–1894 (2010).
30.
Givens DI. Dairy products: good or bad for cardiometabolic disease? Am.J. Clin. Nutr. 101(4), 695–696 (2015).
31.
Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 87(1), 4–14 (2010).
32.
Szende A, Janssen B, C J (Eds.). Self-reported population health: an international perspective based on EQ-5D. EuroQol. Springer (2014).
33.
Forouhi NG, Koulman A, Sharp SJ et al. Differences in the prospective association between individual plasma phospholipid saturated fatty acids and incident Type 2 diabetes: the EPIC-InterAct case-cohort study. Lancet Diabetes Endocrinol. 2(10), 810–818 (2014).
34.
Hur C, Choi SE, Rubenstein JH et al. The cost–effectiveness of radiofrequency ablation for Barrett's esophagus. Gastroenterology 143(3), 567–575 (2012).
35.
Haidry RJ, Butt MA, Dunn JM et al. Improvement over time in outcomes for patients undergoing endoscopic therapy for Barrett's oesophagus-related neoplasia: 6-year experience from the first 500 patients treated in the UK patient registry. Gut 64(8), 1192–1199 (2015).
Information & Authors
Information
Published In
Copyright
Rehan Haidry.
History
Published online: 25 May 2017
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
Cost–effectiveness analysis of endoscopic eradication therapy for treatment of high-grade dysplasia in Barrett’s esophagus. (2017) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2016-0089
Export citation
Select the citation format you wish to export for this article or chapter.
Citing Literature
- Massimiliano di Pietro, Nigel J Trudgill, Melina Vasileiou, Gaius Longcroft-Wheaton, Alexander W Phillips, James Gossage, Philip V Kaye, Kieran G Foley, Tom Crosby, Sophie Nelson, Helen Griffiths, Muksitur Rahman, Gill Ritchie, Amy Crisp, Stephen Deed, John N Primrose, National Institute for Health and Care Excellence (NICE) guidance on monitoring and management of Barrett’s oesophagus and stage I oesophageal adenocarcinoma, Gut, 10.1136/gutjnl-2023-331557, 73, 6, (897-909), (2024).
- Jin Lin Tan, Kingjin Heng, Mohamed Asif Chinnaratha, Norma B. Bulamu, Billingsley Kaambwa, Rajvinder Singh, Incidence rates of Barrett’s esophagus and esophageal adenocarcinoma: a systematic review and meta-analysis, iGIE, 10.1016/j.igie.2024.01.001, 3, 1, (92-103.e3), (2024).
- Mark Nuijten, Livia Dainelli, Bahareh Rasouli, Krysmaru Araujo Torres, Moreno Perugini, Agnieszka Marczewska, A Meal Replacement Program for the Treatment of Obesity: A Cost-Effectiveness Analysis from the Swiss Payer’s Perspective, Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 10.2147/DMSO.S284855, Volume 14, (3147-3160), (2021).
- Joel H. Rubenstein, John M. Inadomi, Cost-Effectiveness of Screening, Surveillance, and Endoscopic Eradication Therapies for Managing the Burden of Esophageal Adenocarcinoma, Gastrointestinal Endoscopy Clinics of North America, 10.1016/j.giec.2020.08.005, 31, 1, (77-90), (2021).
- John J. McGoran, Krish Ragunath, Endoscopic management of Barrett's esophagus: Western perspective of current status and future prospects, Digestive Endoscopy, 10.1111/den.13812, 33, 5, (720-729), (2020).
- Prateek Sharma, Nicholas J. Shaheen, David Katzka, Jacques J.G.H.M. Bergman, AGA Clinical Practice Update on Endoscopic Treatment of Barrett’s Esophagus With Dysplasia and/or Early Cancer: Expert Review, Gastroenterology, 10.1053/j.gastro.2019.09.051, 158, 3, (760-769), (2020).
- Vicki Pollit, David Graham, Catherine Leonard, Alexandra Filby, Jessica McMaster, Stuart J. Mealing, Laurence B. Lovat, Rehan J. Haidry, A cost-effectiveness analysis of endoscopic eradication therapy for management of dysplasia arising in patients with Barrett’s oesophagus in the United Kingdom, Current Medical Research and Opinion, 10.1080/03007995.2018.1552407, 35, 5, (805-815), (2019).