What clinicians should know about differential placebo effects
Abstract
Research is inconclusive as to whether placebo interventions can result in clinical improvement. A number of methodological concepts must be taken into consideration when estimating differential effects of placebo interventions. Using network meta-analysis, researchers can move beyond the lack of direct comparisons available between different placebo interventions by making multiple pairwise comparisons. This design allows us to account for several components of the placebo effect. The additive effects of placebos may be beneficial in clinical practice if physicians can utilize them in a non-deceptive manner to optimize patient care. Researchers and clinicians should be aware of the existence of differential placebo responses when considering selecting appropriate placebo controls in the design of future clinical trials and when formulating treatment regimens.


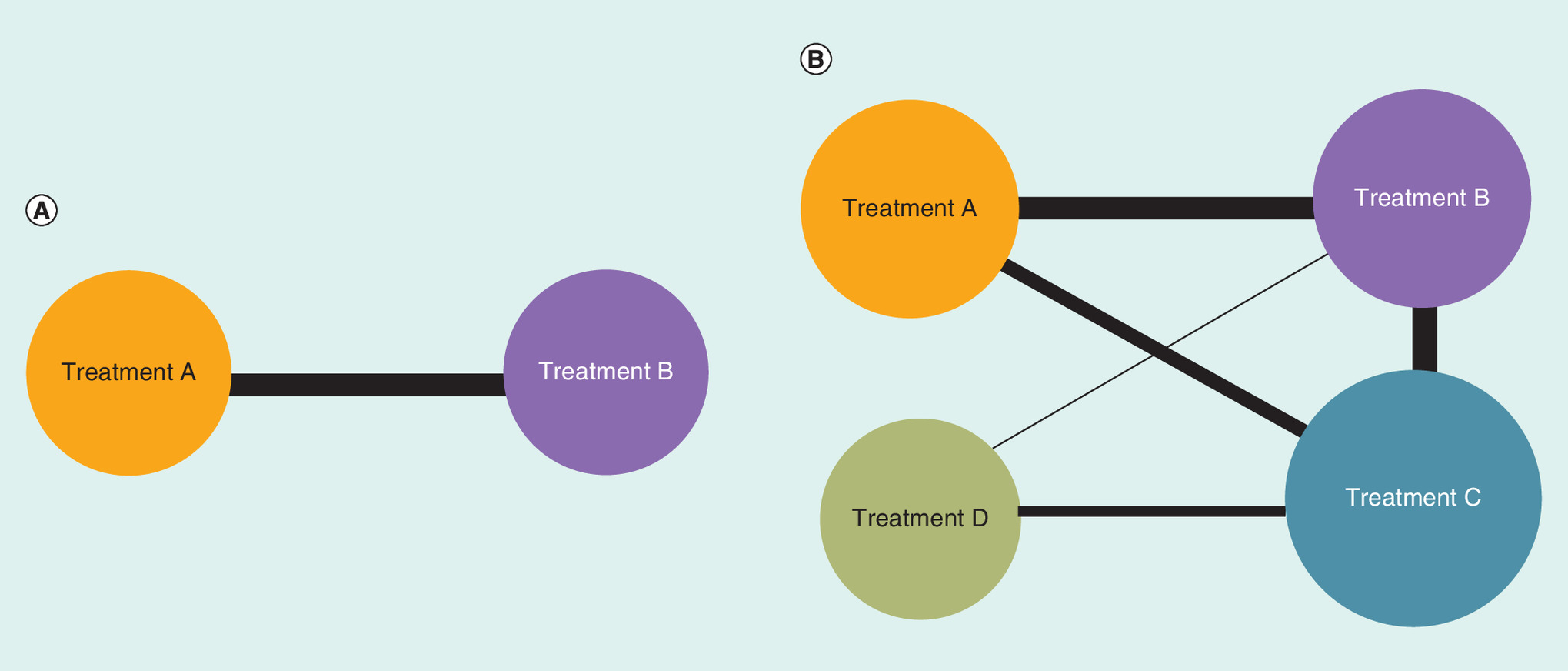
Figure 3. Representation of traditional and network meta-analysis methods.
(A) Diagram of traditional meta-analysis method. (B) Diagram of network meta-analysis method. Circle size reflects the total number of participants receiving a treatment and the line width reflects the number of trials comparing two treatments. No connecting line between two circles indicates no direct comparison between the two treatments.


Figure 5. Demonstration of differential placebo effects.
IA: Intra-articular; SMD: Standardized mean difference.
First draft submitted: 13 October 2015; Accepted for publication: 26 February 2016; Published online: 19 April 2016
The ‘placebo effect’, or the observed clinical effect of treatments which are assumed to be ineffectual, is a subject of methodological, ethical, and clinical debates. Placebo research up to the present has spanned a vast range of psychological and physiological conditions and has involved many different treatment modalities. While some experts have described the placebo as ‘powerful’ and have proposed that it has the ability to go so far as to elicit clinical effects characteristic of the active treatment [1,2], others have found that the effects of placebos in clinical trials are generally weak or not present at all [3]. Though consensus is far from being reached as to the strength, clinical applicability, and cross-disciplinary variation of the placebo effect, a deeper understanding of its impact on observed treatment effects would be valuable to clinicians in their interpretation of clinical trial findings. Evidence of differential placebo effects could be of particular value to clinicians when developing treatment regimens in real-world clinical practice.
Estimation of placebo effects: methodological considerations
Components of treatment effect
In order to appreciate the clinical impact of placebos, it is essential to understand the concepts of overall treatment effect and specific treatment effect. Overall treatment effect refers to the total benefit a patient experiences from a treatment, including associated placebo effects. Specific effect refers to the treatment benefit that extends beyond placebo effects. The specific effect is essentially the overall effect minus placebo effects, and it is representative of the treatment's intended therapeutic action. For example, if we have a treatment with an effect size of 5 points and a placebo with an effect size of 2 points, the specific effect of this treatment is 5 minus 2, which is 3 points, whereas the overall effect of the same treatment is 5 points (Figure 1). In real-world clinical practice, all observed effects are overall treatment effects.
Participant expectation
Participant expectation and regression to the mean are methodological concerns that may impact the magnitude of the placebo effects observed in individual trials. Participant expectation, a key mechanism of placebo effect, is a psychological phenomenon which relates to a trial participant's assumptions of a treatment's effect [4]. Participants enrolled in clinical trials tend to disproportionately recall positive results as treatment progresses due to their expectations of the treatment's effect, regardless of receiving active treatment or placebo, while simultaneously downplaying negative effects or not acknowledging a complete lack of effect [5]. Often described as Hawthorne effects, the overestimation of intervention effects due to clinical trial participation is one of many manifestations of patient expectation [6]. The manner in which investigators introduce treatments to participants at the initiation of a clinical trial, the characteristics of active treatments, and the measures taken to blind patients to treatment allocation heavily influence participant expectation; these qualities can vary widely between trials. Expectation on the part of participants can ultimately obscure or amplify the specific effects of active treatments and the effects of placebo interventions [7]. When synthesizing the results of multiple clinical trials to ascertain a comprehensive treatment effect, it is important for researchers to bear the impact of patient's expectation in mind. Similarly, it is essential for clinicians to be aware of the inherent patient expectation associated with clinical trial participation and its resulting impact on observed treatment effects when applying clinical trial data to real-world treatment decisions. Oftentimes, the efficacy of treatments does not entirely translate into clinical practice, as the expectation of a new drug effect which is observed in a clinical trial is no longer at play.
Regression to the mean
Regression to the mean refers to a phenomenon in which outcomes that produce extreme values upon the baseline measurement are statistically more likely to produce values which fall closer to the mean of the sample upon the final measurement [8]. Sample and outcome characteristics can influence the extent to which values will regress to the mean, although control over these characteristics is limited. Regression to the mean has been erroneously attributed, according to some researchers, to the placebo effect, particularly when measuring subjective pain [9]. Under this assumption, the placebo effect observed in clinical trials may actually be significantly smaller than it appears to be due to regression to the mean and other nonspecific effects. The ‘true placebo effect’ is defined as the effect that remains after nonspecific effects have been subtracted from the ‘perceived placebo effect’ (Figure 2) [10].
Network meta-analysis: a solution to scarcity of evidence
In light of the methodological challenges described, it would be ideal to examine the effects of different placebo interventions in the most direct way possible, either in comparison with each other or against an untreated study arm in a randomized controlled trial (Figure 3A). However, due to ethical concerns, these types of trials are extremely rare. Consequently, conducting a traditional meta-analysis using direct comparisons is not an option, and indirect comparison methods such as network meta-analysis must be undertaken. In a traditional meta-analysis, two treatments are compared against each other. Network meta-analysis is an extension of traditional meta-analysis that compares multiple interventions, even in the absence of randomized trials which directly compare these interventions with each other (Figure 3B). In doing so, network meta-analysis allows researchers to estimate relative effects of all available treatments and to develop a hierarchy of treatments based on their effect sizes [11,12]. Our own research in this field explored the strength of the placebo effect in a network of clinical trials in patients with knee osteoarthritis (OA) [13]. Knee OA was ideal for our study due to its high prevalence, well-defined diagnostic criteria, validated outcome measures and extensive clinical research involving a variety of therapeutic approaches. One of the key assumptions of a network meta-analysis is that all included trials should share similar characteristics, and the characteristics of knee OA trials in particular provided us with an excellent opportunity for studying the placebo effect and assessing the different impacts various types of placebos may have on pain [11,12].
The efficacy paradox
In a network meta-analysis comparing many interventions involving different types of placebo comparators, the assumption is often made that various placebos can be categorized as a single group on the basis of having the same null effects. Combining placebos that differ in route of administration or in other characteristics could be problematic if they are not completely ineffectual and if variations in efficacy do exist between the different types. The differential placebo effect leads to a phenomenon called ‘efficacy paradox’, a concept that has the potential to influence clinicians’ decision-making in real-world clinical practice. The efficacy paradox refers to a scenario in which a treatment whose overall effect appears moderately superior to a placebo counterpart may be more efficacious than a different treatment which shows a greater superiority over its placebo, if the placebo effects of the two treatments vary (Figure 4) [14]. This scenario can be seen when treatments with different routes of administration are compared. In clinical practice, choosing a more effective oral treatment by examining randomized trials that compare separate oral treatments against a similar oral placebo is reasonable. However, if choosing between a topical and an oral treatment, it would be erroneous to base the clinical decision on separate trials comparing these treatments against their respective placebos. For example, an oral treatment with an overall effect size of 5 points compared against an oral placebo with an effect size of 2 points will have a specific effect of 3 points. A topical treatment with an overall effect size of 6 points compared against a topical placebo with an effect size of 4 points will have a specific effect of 2 points. Thus, even though the specific effect of the topical treatment is inferior to that of the oral treatment, a patient would perceive a greater overall benefit (6 vs 5 points) using the topical preparation (Figure 4).
Estimation of differential placebo effects
Most of the published meta-analytic studies that measure the strength of placebo effects do so by employing a single-group analytic design. Single-group analysis breaks randomization by selecting only treatment arms of interest from each trial, making it difficult to control for participant expectation and/or regression to the mean and to segregate them from the perceived placebo effect. In utilizing network meta-analysis methodology, we are able to preserve randomization by analyzing both active and placebo groups in all of the included studies. Maintaining randomization allows us to account for regression to the mean and other nonspecific effects and to negate them from the overall placebo effect, which in turn allows us to measure the ‘true placebo effect’.
In this study, we compared placebo treatments of varying routes of administration among clinical trials specifically focused on knee OA patients [13]. We included only randomized controlled trials of adults with knee osteoarthritis which compared leading pharmaceutical products against oral, intra-articular or topical placebos. We applied limitations to both the population and to the placebo administration types included in order to reduce heterogeneity in our sample. We included 149 trials including 39,814 participants and performed network meta-analysis using a Bayesian random effects model. Additionally, we performed another network meta-analysis in which we assumed equivalency of all placebos and compared the results of both network meta-analyses in order to assess the impact of ignoring differential placebo effects. We calculated the standardized mean differences between placebo types using the changes in pain scores from baseline to 3 months. Our analysis provided strong evidence toward the existence of differential placebo effects attributable to treatment administration route. It was shown that intra-articular and topical placebos were more effective when compared with oral placebo, with effect sizes of 0.29 (95% CI: 0.09–0.49) and 0.20 (95% CI: 0.20–0.38), respectively.
The comparison between intra-articular corticosteroids (IACS) and various placebo administration types clearly illustrated differential placebo effects. Against their typical intra-articular placebo comparator, IACS demonstrated an effect size of 0.29 (95% CI: 0.15–0.44). When compared with topical placebo, the effect size of IACS increased to 0.38 (95% CI: 0.09–0.67), and in comparison with oral placebo, the original effect size was nearly doubled (0.58 [95% CI: 0.34–0.82]). Conversely, we found that comparison of active treatments with matching placebos can produce positive effects for some active treatments which are diminished when compared with a placebo that has a different route of administration. When compared with oral placebo, oral celecoxib (COX-2 inhibitor) showed a statistically significant benefit of 0.34 (95% CI: 0.27–0.42). The effect size decreased dramatically, however, and was no longer statistically significant, when celecoxib was compared with topical placebo (0.14 [95% CI: -0.04–0.32]) or intra-articular placebo (0.05 [95% CI: -0.15–0.32]). These results provide an example of the efficacy paradox, demonstrating that comparing active treatments with placebo treatments can potentially lead to a misinterpretation of a treatment's specific effect, particularly if one or both of the treatments involves a route of administration associated with strong placebo effects (Figure 5). In addition to the evidence from this network meta-analysis, differential efficacy of placebo interventions has also been demonstrated in previously published meta-analyses, as well as in direct comparisons in prior clinical trials [15–18]. These trials spanned a variety of patient populations and included an assortment of placebo procedures.
One of the limitations in employing a network meta-analysis method for studying placebo effects is the scarcity of direct evidence available for comparisons between different placebo interventions. Our study, for example, had only one randomized trial of oral versus topical placebo among 149 randomized controlled trials [13,19]. The results from network meta-analyses should be interpreted with caution, and the amount of indirect evidence contributing to the analysis should be carefully considered. Despite the limitations, network meta-analysis continues to be the best possible method for differentiating between placebo interventions in the absence of direct comparisons by a randomized trial. Though indirect treatment comparisons are subject to bias, carefully conducted indirect treatment comparisons can, in tandem with the existing body of evidence provided by randomized controlled trials, provide a more detailed and informative profile of treatment effects and their relationship to placebo effects [12].
Discussion: placebo effects in a real-world clinical setting
Isolation and assessment of placebo effects can be clinically applicable in a variety of conditions and contexts, especially for patients suffering from conditions for which clinical outcomes are predominantly measured subjectively. A 6-week randomized controlled trial in patients with irritable bowel syndrome (IBS) performed by Kaptchuk et al. aimed to distinguish and assess three components of the placebo effect specific to clinical settings: patient's response to observation, patient's response to administration of a therapeutic regimen and patient's response to the patient/caregiver interaction. Out of three study arms, one received no treatment, one received sham acupuncture treatment and one received sham acupuncture treatment which was ‘augmented’ by a focus on caregiver warmth. At 6 weeks, patients receiving ‘augmented’ placebo treatment reported statistically significantly better results with regard to IBS symptom severity and quality of life scales. The authors concluded that focus on a warm patient/practitioner interaction could lead to a placebo effect which results in significant clinical improvement [20]. This trial is an example of one way that clinicians can apply the beneficial effects of placebos to clinical practice in an ethical way. IBS was chosen by the authors of this study because it has demonstrated a very high placebo response in randomized controlled trials. Similarly, sham acupuncture was selected as the placebo treatment for this trial because it is known to elicit strong placebo effects. Such choices can branch beyond clinical trial design, and it may be possible for practitioners to tailor their patients’ treatment based not only on the specific placebo response of a particular disease, but also based on the strength of placebo effects elicited by a particular route of administration.
The findings from studies measuring placebo effects have great potential to be applicable in real-world clinical practice. However, clinicians should be aware of the fact that the observed placebo effects are reported by patients enrolled in blinded randomized controlled trials. When patients are not blinded to treatment, as is the case in clinical practice, it is difficult to determine the extent to which the observed placebo effect would translate into the real world. In practice, it may be a challenge to harness placebo effects without deceiving or misinforming patients about their treatment regimen. Deceiving patients about their treatment raises ethical concerns by violating informed consent and the standards of transparency currently set in place for clinical care, and as such it is not currently acceptable to use placebos as standalone treatments [4]. It might also be impractical to commercialize the usage of placebos as standalone treatments because marketing a drug is not permitted without disclosing its active contents, and upon disclosure there would be no certainty if the benefits associated with placebos could still be observed. Despite these challenges, placebo effects can be harnessed at least partially, for example, when choosing to administer either a topical or intra-articular treatment for osteoarthritis.
Conclusion
In conclusion, clinicians should be cognizant of the notion that placebos are not null in efficacy, nor are they equivalent to one another. Understanding differential placebo effects is the first step to gaining a deeper comprehension of the efficacy paradox. Knowledge about how route of administration impacts patient response to treatment could be invaluable to clinicians when deciding on the most effective treatment regimens. The additive effects of placebos may be beneficial in clinical practice if physicians can utilize them in a nondeceptive manner to optimize patient care. Researchers should also be aware of differential placebo responses and consider selecting appropriate placebo controls in the design of future clinical trials and network meta-analyses.
Background
Research thus far is inconclusive as to whether or not placebo interventions can result in clinical improvement. Understanding placebo effects involves many nuances and methodological challenges. Our goal is to present some of the most important concepts involved in placebo research.
Estimation of placebo effects: methodological considerations
Components of treatment effect:
Overall treatment effect refers to the overall benefit a patient gets from treatment. It is comprised of ‘specific treatment effect’ and the ‘placebo effect’;
Specific treatment effect refers to the effects which result directly from administered treatments; it is essentially equal to the overall treatment effect minus placebo and nonspecific effects.
Participant expectation
Participant expectation refers to a patient's assumptions of a treatment's effect.
Patient expectation can lead to misrepresentation of specific effects of active treatments, and can obscure or amplify placebo effects.
Regression to the mean
Refers to the tendency of extreme baseline values to fall closer to the mean of the sample upon the final assessment.
Failure to account for regression to the mean can lead to an overestimated placebo effect.
Network meta-analysis: a solution to scarcity of evidence
It is rare, if impossible, to find a randomized controlled trial directly comparing placebo interventions against each other or against an untreated study arm.
Using network meta-analysis, researchers can move beyond the lack of direct comparisons by making pairwise comparisons between multiple treatments that are not directly compared within clinical trials. This allows for estimation of the relative effects of all treatments involved, ultimately enabling researchers to develop a hierarchy of treatments.
The efficacy paradox
A scenario in which a treatment whose overall effect appears moderately superior to a placebo counterpart may be more efficacious than a different treatment which shows a greater superiority over its placebo, if the placebo effects of the two treatments vary.
Estimation of differential placebo effects
Using indirect comparisons, we can estimate the relative effects of placebo interventions. Since Network Meta-Analysis method does not break trial randomization, we can account for regression to the mean and negate it from the overall placebo effect, leaving us with a more accurate representation of the placebo effect.
Discussion: placebo effects in a real-world clinical setting
An randomized controlled trial by Kaptchuk et al. demonstrated that placebo treatments can produce statistically significant clinical effects, particularly in diseases with a documented large placebo response.
The additive effects of placebos may be beneficial in clinical practice if physicians can utilize them in a nondeceptive manner to optimize patient care.
Conclusion
Researchers and clinicians should be aware of the existence of differential placebo responses, when considering selecting appropriate placebo controls in the design of future clinical trials and when formulating treatment regimens.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
1.
Zhang W, Robertson J, Jones AC et al. The placebo effect and its determinants in osteoarthritis: meta-analysis of randomised controlled trials. Ann. Rheum. Dis. 67(12), 1716–1723 (2008).
2.
Wampold BE, Minami T, Tierney SC et al. The placebo is powerful: estimating placebo effects in medicine and psychotherapy from randomized clinical trials. J. Clin. Psychol. 61(7), 835–854 (2005).
• A re-analysis of a meta-analysis by Hróbjartsson et al. which demonstrated a robust placebo effect and highlighted that placebo effects can be hidden or even diminished based on meta-analysis design and based on heterogeneous disease characteristics.
3.
Hróbjartsson A, Gotzsche PC. Placebo interventions for all clinical conditions. Cochrane Database Syst. Rev. (1), CD003974 (2010).
• Systematic review and meta-analysis examining the effects of placebo treatments in 156 trials encompassing 46 different clinical conditions. Authors found that placebo treatments had a weak, if nonexistent effect.
4.
Finniss DG, Kaptchuk TJ, Miller F, Benedetti F. Biological, clinical, and ethical advances of placebo effects. Lancet 375(9715), 686–695 (2010).
•• A review that details the biological and clinical background of the placebo effect and expands upon the ethical considerations involved with applying placebo treatment to real-world clinical practice.
5.
Price DD, Finniss DG, Benedetti F. A comprehensive review of the placebo effect: recent advances and current thought. Annu. Rev. Psychol. 59, 565–590 (2008).
6.
Holden JD. Hawthorne effects and research into professional practice. J. Eval. Clin. Pract. 7(1), 65–70 (2001).
7.
Vase L, Riley JL 3rd, Price DD. A comparison of placebo effects in clinical analgesic trials versus studies of placebo analgesia. Pain 99(3), 443–452 (2002).
8.
Delgado-Rodriguez M, Llorca J. Bias. J. Epidemiol. Community Health 58(8), 635–641 (2004).
9.
Whitney CW, Von Korff M. Regression to the mean in treated versus untreated chronic pain. Pain 50(3), 281–285 (1992).
10.
Ernst E, Resch KL. Concept of true and perceived placebo effects. BMJ 311(7004), 551–553 (1995).
11.
Salanti G. Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3(2), 80–97 (2012).
12.
Jansen JP et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health 14(4), 417–428 (2011).
13.
Bannuru RR et al. Effectiveness and implications of alternative placebo treatments: a systematic review and network meta-analysis of osteoarthritis trials. Ann. Intern. Med. 163(5), 365–372 (2015).
•• A systematic review and network meta-analysis exploring the differential placebo effects and their implications on the effects of active treatments in randomized controlled trials (RCTs) involving osteoarthritis patients.
14.
Walach H. The efficacy paradox in randomized controlled trials of CAM and elsewhere: beware of the placebo trap. J. Altern. Complement. Med. 7(3), 213–218 (2001).
15.
Traut EF, Passarelli EW. Placebos in the treatment of rheumatoid arthritis and other rheumatic conditions. Ann. Rheum. Dis. 16(1), 18–22 (1957).
16.
Grenfell RF, Briggs AH, Holland WC. A double-blind study of the treatment of hypertension. JAMA 176, 124–128 (1961).
17.
Morison RA, Woodmansey A, Young AJ. Placebo responses in an arthritis trial. Ann. Rheum. Dis. 20, 179–185 (1961).
18.
Kaptchuk TJ et al. Sham device v inert pill: randomised controlled trial of two placebo treatments. BMJ 332(7538), 391–397 (2006).
•• Single-blind RCT comparing the placebo counterparts for two different active interventions for persistent arm pain. Sham accupuncture was directly compared to an oral placebo. Authors concluded that the sham device had greater effects than oral placebo on self-reported outcomes over the longer course of treatment, but not during the 2-week run-in period.
19.
Conaghan PG et al. A multicentre, randomized, placebo- and active-controlled trial comparing the efficacy and safety of topical ketoprofen in Transfersome gel (IDEA-033) with ketoprofen-free vehicle (TDT 064) and oral celecoxib for knee pain associated with osteoarthritis. Rheumatology (Oxford) 52(7), 1303–1312 (2013).
20.
Kaptchuk TJ et al. Components of placebo effect: randomised controlled trial in patients with irritable bowel syndrome. BMJ 336(7651), 999–1003 (2008).
•• Single-blind RCT directly comparing two different placebo treatments with a group receiving no treatment in patients with irritable bowel syndrome, which found that nonspecific effects of certain treatments can reach statistical and clinical significance.
Information & Authors
Information
Published In
Copyright
© Future Medicine Ltd.
History
Published online: 19 April 2016
Keywords:
Topics
Authors
Metrics & Citations
Metrics
Article Usage
Article usage data only available from February 2023. Historical article usage data, showing the number of article downloads, is available upon request.
Citations
How to Cite
What clinicians should know about differential placebo effects. (2016) Journal of Comparative Effectiveness Research. DOI: 10.2217/cer-2015-0005
Export citation
Select the citation format you wish to export for this article or chapter.