Bridging the gap: Enabling equitable access to rare disease therapies through strategic evidence planning

Developing therapies for rare diseases demands foresight and precision at every stage of evidence generation. In this Guest Column, we explore how strategic evidence planning, from early discovery to post-launch, can bridge persistent access gaps. We highlight why early alignment with regulators, health technology assessment (HTA) bodies and payers is vital to sustaining equitable access. Our analysis underscores that in rare disease development success depends not only on innovation but on planning for evidence that endures.
Why strategic evidence planning matters
Rare disease drug development is high risk and high reward, where each early decision shapes a therapy’s long-term trajectory. Because patient populations are small and unmet need is urgent, developers must plan evidence strategies not only for regulatory approval but also for reimbursement and sustained access. With frameworks such as the EU’s Joint Clinical Assessment (JCA), evolving national HTAs, and demanding US payer standards, strategies must be global and proactive from discovery onward.
Sponsors need to anticipate what regulators, HTA bodies and payers will require across all stages, from preclinical work and Phase 1 studies through to pivotal trials and into the post-launch era of real-world evidence (RWE) collection. In rare disease drug development, the traditional distinctions between clinical trial phases are increasingly blurred. Phase 1 is not only about safety, but also about laying the foundation for demonstrating value. Phase 2/3 serves as the essential stage for generating evidence that supports earlier access for patients with high unmet need. Lastly, in post-launch, ongoing evidence generation becomes critical to determining whether access can be sustained.
Without such strategic planning, access gaps will persist, leaving patients with rare diseases at a disadvantage compared to those with more common conditions. This not only delays or denies life-changing treatments for underserved populations, but also deepens systemic health inequities by reinforcing disparities in those who benefit from innovation and investment in healthcare.
Discovery and Phase 1: building the foundation
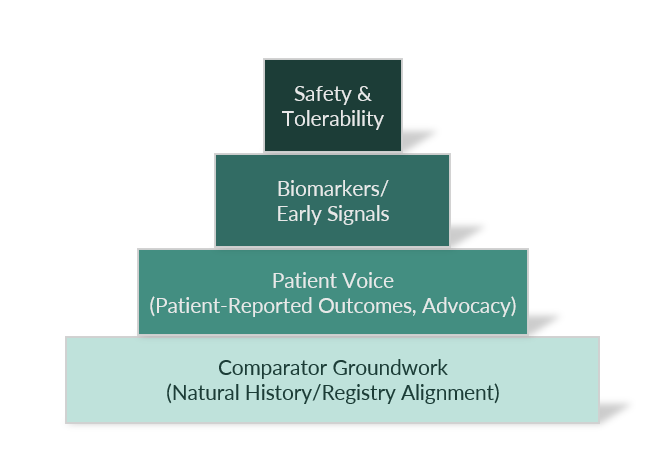
The earliest stages of development that include discovery, preclinical, and first-in-human Phase 1 trials lay the evidence foundation for a rare disease therapy. Phase 1 traditionally focuses on safety, tolerability, pharmacokinetics, pharmacodynamics, and dose-finding. In rare diseases, the small patient populations and limited natural history data make each data point especially critical. Careful planning is essential to enhance the ability to detect meaningful treatment effects and guide later-phase efficacy studies.
“Early studies should be designed with the end goals of approval, reimbursement, and patient access in mind. Choosing the right endpoints that reflect outcomes meaningful to patients, such as functional ability or quality of life, is critical.”
Exploratory biomarkers, patient stratification, and carefully defined inclusion/exclusion criteria may further optimize early-phase signal detection, but only if they are validated against clinical outcomes. The European Medicines Agency (EMA) and the US Food and Drug Administration (FDA) provide qualification pathways, but this work must begin early. For gene and enzyme therapies, demonstrating a plausible link between biomarker shifts and patient benefit strengthens later regulatory and payer arguments.
Comparator strategy is another element to address; even if Phase 1 is uncontrolled, teams can start building a natural-history dataset or external control cohort. Laying this groundwork in Phase 1 ensures that later Phase results will be interpretable and credible to both regulators and HTA agencies.
Early stakeholder engagement is a hallmark of a strong Phase 1 strategy. This means involving not just regulators, but also payers, HTA agencies, and even patients in the trial design stage. Early scientific advice meetings in Europe, which may include HTA input, and US programs, such as Fast Track or Regenerative Medicine Advanced Therapy (RMAT), offer opportunities to align trial design with both regulators and payers. Patients and advocacy groups can also highlight outcomes that matter most, supporting inclusion of patient-reported outcomes (PROs) from the start.
“From a health equity perspective, this ensures that the voices of those directly affected are heard early, helping to shape trials around real-world needs, improve relevance, and support better adherence and access for underserved populations.”
Another challenge is manufacturing consistency. For complex therapies like gene or cell therapies, ensuring early consistency in production prevents later challenges around comparability, which could raise doubts about real-world effectiveness.
One notable example of the importance of early Phase 1 evidence planning comes from DFT383, a gene therapy for the rare disease cystinosis. The early trial was designed to assess safety, tolerability and preliminary efficacy in a carefully selected pediatric population. By employing multiple, complementary endpoints and identifying early biomarkers, the study generated critical data that informed dosing, optimized patient selection, and guided the design of subsequent trials. This robust early-phase evidence strengthened the clinical rationale for later studies, supported regulatory interactions, facilitating FDA and EMA designations, and provided HTA bodies with early signals of potential clinical benefit.
Janssen’s nipocalimab program, which targets the neonatal Fc receptor (FcRn), also shows disciplined early-phase development. First-in-human studies in healthy adults established safety, pharmacokinetics/pharmacodynamics, and dose-dependent IgG reductions. The company then produced positive randomized patient data in Phase 2 and a registrational Phase 3 study. In September 2025, EMA’s Committee for Medicinal Products for Human Use (CHMP) issued a positive opinion and offered a parallel regulator–HTA consultation route. The case highlights how early alignment and creative use of real-world data (RWD) can streamline rare disease therapy development. By designing early trial stages as a strategic foundation for later stages, companies will be in a much stronger position.
Phase 2/3: Bridging to approval and market
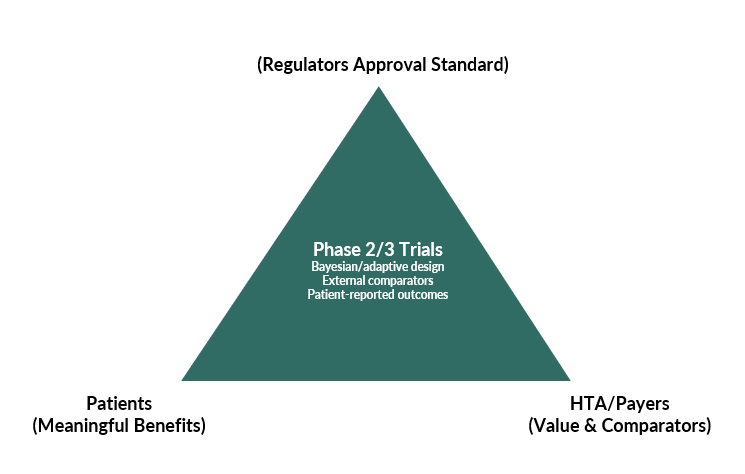
For most rare-disease therapies, Phase 2 and 3 studies play a vital role in turning small and often heterogeneous datasets into evidence that persuades regulators and HTA bodies. The practical lesson for developers is to plan early for uncertainty that will persist at launch, and to build credible solutions that keep patients moving toward access while more data is gathered.
In Phase 2 and 3, design choices should account for the challenges of working with small sample numbers and short follow-up periods. Having multiple endpoints, patient-reported outcomes, and prespecified subgroup analyses help to triangulate treatment effect and show consistency across measures. From a statistical perspective, Bayesian and adaptive features can be appropriate in Phase 2 and sometimes in Phase 3. For example, borrowing prior information, response adaptive randomization, or sample size re-estimation, provided decision rules and error control are prespecified. When a randomized placebo control is infeasible or follow up is short, mitigating solutions include high-quality external comparators such as natural history cohorts or registries with rigorous curation, sensitivity analyses, and transparent reporting. Extension studies and long-term registries are typically post-approval activities, but the design and set-up can begin during Phase 2 and 3 study planning so that RWD collection can start promptly after marketing authorization.
Access planning should progress alongside evidence generation. Preparing managed access agreements in parallel to Phase 2 and 3 allows reimbursement to be tied to further data collection and, where appropriate, to outcomes-based payments after approval. This may include developing approaches to selecting appropriate real-world outcome measures that could inform the outcome-based agreement. This approach creates room for timely patient access while durability, generalizability, and long-term safety are confirmed in routine care.
Recent examples show the risks and the opportunities. Amylyx’s AMX0035 achieved early approval on modest signals that were not replicated in a confirmatory Phase 3 trial, leading to its withdrawal. This underlines the need for Phase 2 and 3 evidence that is confirmatory and durable. By contrast, Zolgensma gained approval (even in very small populations) because early outcomes were striking when viewed against historical experience, and because the program coupled authorization with post-approval commitments and managed access.
“It is clear – careful design in Phase 2 and 3, transparent use of external evidence, and planned post-launch learning can carry a therapy to market while uncertainty continues to be addressed.”
Future developers should view uncertainty as a design input from the outset. During Phase 2 and 3, it is sensible to embed methods that make small studies work harder and to prespecify how external evidence will be used and tested. In parallel, plans for extension studies, registries, and RWD flows should be in place before approval so that post-authorization learning can begin immediately. At the same time, a managed entry strategy prepared in step with the clinical plan can align decision points with payer needs and link access to ongoing evidence generation.
“Taken together, early planning for anticipated uncertainty and well-prepared managed entry options make it more likely that regulators and HTA bodies will regard the totality of evidence as credible and actionable."
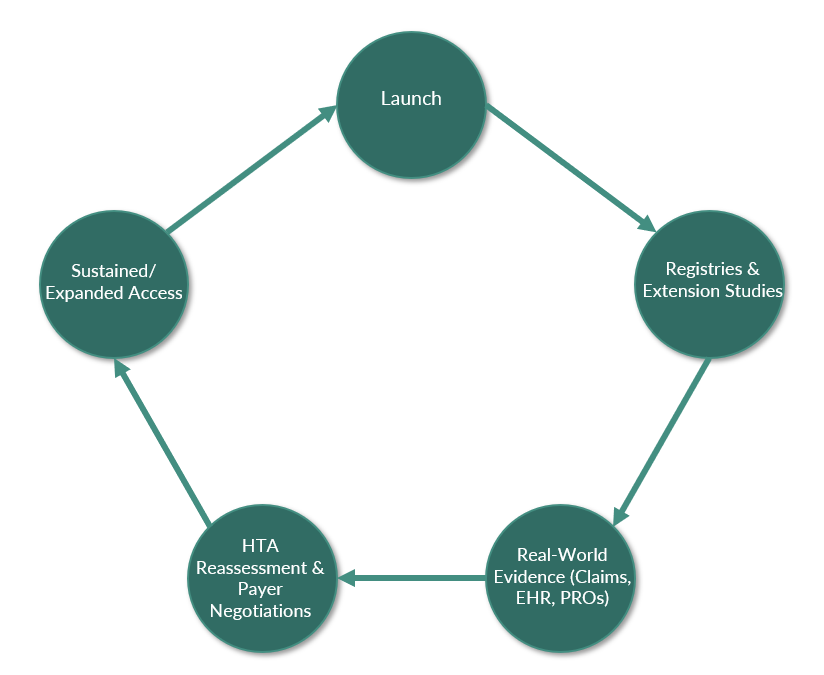
Post-launch: Sustaining access with RWE
In short, approval is not the finish line. Reassessment is common within 1–3 years in Europe and is ongoing in the US. Sustaining access requires continued demonstration of value.
Registries and extension studies are crucial for monitoring durability of benefit and long-term safety. Gene therapies often come with 15-year follow-up requirements. Confirmatory Phase 4 trials and post-authorization commitments are increasingly tied to conditional approvals. On real-world effectiveness, observational studies using claims or electronic health record (EHR) data can reveal whether trial outcomes are matched in clinical practice. RWE methods range from prospective patient registries and disease-specific natural history cohorts to retrospective studies using insurance claims databases, EHRs, or hybrid designs combining multiple sources. Analytic approaches in RWE studies include statistical methods such as propensity-score matching, inverse-probability weighting, or synthetic control arms that help mitigate confounding when direct comparators are lacking. While RWE studies may carry inherent biases, transparent design, pre-registration of protocols, and comparison across sources can strengthen their validity. Wearables and digital health tools are emerging as valuable ways to capture continuous outcomes, especially in rare diseases with small samples.
Managed entry and outcomes-based agreements also are critical in the post-launch phase. Because of high prices and uncertainty, payers increasingly link reimbursement to performance. For example, Italy’s AIFA (Agenzia Italiana del Farmaco), the Italian Medicines Agency, is known to pioneer web-based outcome tracking with automatic refunds if patients fail to meet milestones. US payers use outcomes-based rebates and pay-over-time models. Such arrangements make robust follow-up mechanisms indispensable. Regular reassessments of cost-effectiveness ensure pricing and reimbursement remain aligned with accumulating evidence.
In the UK, Spinraza (nusinersen for spinal muscular atrophy [SMA]) entered the UK market under a managed access agreement in 2019, restricted to certain patients. By 2021, registry and extension study data showed benefits in older children, leading NICE to expand access. This success reflected proactive evidence generation and stakeholder collaboration. In contrast, Glybera (alipogene tiparvovec), the first gene therapy approved in Europe for the treatment of familial lipoprotein lipase deficiency (LPLD), faced limited uptake following its launch. With only one patient treated and no RWE generated, payers saw no justification for its cost of >€1 million. Marketing authorization was not renewed in 2017, underscoring that approval without usage and evidence leads to a challenging market environment. Glybera’s lack of patient uptake despite regulatory approval illustrates a deep inequity in rare disease treatment. The lack of RWE meant that payers had no compelling data to justify reimbursement even though patients with familial LPLD faced serious health risks. Even the singular treated patient had to undertake extensive paperwork and negotiate directly with insurers.
This case underscores how regulatory approval alone is not enough.
“Without equitable access pathways, robust evidence generation, and sustainable delivery models, innovative therapies risk deepening disparities, leaving rare disease patients behind while others benefit from medical advances.”
Collaboration and transparency are also key factors in the post-launch phase. Working with clinicians, HTAs, and patients in data collection builds trust and ensures evidence reflects real-world experience. Publishing results, either positive or negative, reinforces credibility and helps secure long-term access by identifying gaps and providing evidence. Global coordination and equity of access are essential so that benefits extend beyond major markets and reach underserved patient populations.
The path to sustainable and equitable access
From discovery to post-launch, rare disease drug development is defined by evidence generation. Success depends on early alignment with regulators, HTAs bodies and patients; careful design of trials that maximize insights from limited data; and robust post-launch evidence strategies that sustain access.
The examples referenced illustrate how evidence choices at each stage reverberate. Missteps in endpoints or underpowered trials can derail approval, while strong external comparisons and patient engagement can transform modest results into compelling narratives. Post-launch, ongoing RWE generation and outcomes-based agreements determine whether access is maintained. Continuing lifecycle evidence generation, through label expansion, new subgroups, or earlier-line use, ensures patients continue to access impactful therapies.
Across all Phases, several principles stand out:
- Collaborate early and often. Regulators, HTA bodies, payers, patients, and clinicians must all shape the evidence strategy.
- Design for value. Endpoints, comparators, and biomarkers should reflect what matters to patients and payers, not just regulators.
- Plan for uncertainty. Bayesian designs, survival modeling, and outcomes-based agreements acknowledge and manage inevitable gaps.
- Commit to the long term. Evidence generation cannot stop at approval; sustained access requires continuous demonstration of benefit.
- Optimally communicate product value. Evidence and strategy alone are not enough to ensure success. A clear narrative tailored to the needs of the audience helps to optimally position a product. In rare diseases this may be even more important, as payers for example may be unfamiliar with the condition and its broader impact to the “health economy”.
In rare diseases, every data point is precious, and every phase of development is interconnected. By building a strong evidence foundation early, maximizing and contextualizing pivotal trial data, and executing vigilant post-market studies, biopharma teams can ensure that their therapies not only attain approval but remain available and make a lasting difference for patients. Early conversations and collaboration with HTA bodies and payers are invaluable.
At LCP Health Analytics, our work convening the first-of-its-kind collaboration between HTA bodies and industry to explore how health equity can be embedded into HTA decision-making shows that early, intentional dialogue is critical not just for aligning evidence expectations, but for ensuring that access planning reflects the needs of underserved populations. By engaging stakeholders early, developers can design trials that are more inclusive, relevant, and more likely to support equitable access.
The landscape is certainly challenging (small populations, evolving standards, high uncertainties) but as we have seen, it is navigable with strategic foresight.
“The reward for getting it right is immense. It creates the opportunity to deliver life-altering treatments to patients who have no other options and to sustain access in a way recognized as valuable by healthcare systems worldwide.”
In short, the path to success in rare disease drug development is not only paved by evidence, but also how you leverage the existing, sometimes challenging evidence base to optimal effect. With every step the goal remains the same, which is to transform hope for patients with rare diseases into tangible, lasting benefit, supported by evidence at every stage.
Authors
Sreenidhi Venkatesh
Associate Consultant Market Access, LCP Health Analytics

Sreenidhi Venkatesh is an Associate Consultant in LCP's Health Analytics team. She has a strong foundation in data science and programming, specializing in the healthcare and life sciences sectors. She brings hands-on experience from projects focused on rare diseases across market access and evidence generation. With a keen interest in health equity, she is passionate about leveraging data-driven insights to support more inclusive and impactful healthcare solutions.
Liz Rozin
Analyst, LCP Health Analytics

Liz Rozin is an Analyst in LCP's Health Analytics team. Her key areas of expertise include programming and database management. She has experience in using data science and machine learning techniques to analyze complex healthcare datasets, as well as uncovering insights on disease burden, treatment patterns, and healthcare outcomes.
Pei-Yu Lee
Associate Consultant Epidemiologist, LCP Health Analytics

Pei-Yu is an Associate Consultant in LCP's Health Analytics team. Pei-Yu’s academic background is in statistics and epidemiology. She has extensive experience in health research in both communicable and non-communicable diseases, with critical areas including Alzheimer's disease and heart diseases.
Catrin Treharne
Health Economics Lead, LCP Health Analytics

Catrin Treharne is a Partner and Health Economics Lead in LCP’s Health Analytics team, with more than 13 years’ experience in health economics and health technology assessment. Catrin’s experience spans the product lifecycle, from early economic models to global models suited for health technology assessment, as well as models developed for use in local payer negotiations. In her work, Catrin advances the application of methods to quantify health inequalities and reflect the broader value of health in decision-making.
Jasim Uddin
Market Access Lead, LCP Health Analytics

Jasim Uddin is a Principal and Market Access Practice Lead in the Health Analytics team, with over 20 years of experience in the biopharmaceutical and allied industries. As a seasoned market access consultant, Jasim has significant experience in navigating client market access challenges, with a track record of delivery on a range of global market access strategy and communication projects, including manuscript, global value dossier, landscape, payer insight, value story, and other cross-collaborative market access and HEOR projects. He has experience of working with products across a diverse range of therapy areas and a wide range of healthcare product types, including pharmaceuticals, medical devices, diagnostics, and digital prescription therapeutics. He has a specific interest in payer value communications, particularly how to optimally translate evidence into meaningful communications and tools that aim to facilitate optimal patient access.
Disclaimer
The opinions expressed in this feature are those of the authors and do not necessarily reflect the views of The Evidence Base® or Becaris Publishing Ltd.

Sponsorship for this Guest Column was provided by LCP Health Analytics.